
This post is sponsored by Corra. All thoughts and opinions shared are my own.
For as long as Elya Lane can remember she had signs and symptoms of a health condition. It wasn’t until college that she received her official diagnosis of Ehlers Danlos Syndrome and POTS. She says her poor health started to spiral with other comorbidities popping up, the worst of which was chronic UTIs that left her whole body in crippling, burning pain and weak from the antibiotics. Elya’s personal journey with chronic illness inspired her to create the Corra App. This week on Lights, Camera, Crohn’s we learn about how she made her dream a reality and how she hopes to improve peoples’ lives.

The breaking point
“I was constantly plagued with fears of antibiotic resistance, infection complications, or complications from long term antibiotic use. I got to the point where I was so sick that I wrote letters to my kids and my family in case something happened to me. I started tracking all our passwords and making videos for my husband on where our important files were, how different things were stored, all the kids’ data, etc. While I tried to face this potential outcome bravely, I was devastated imagining my kids growing up without a mom,” said Elya.
As she navigated these dark and daunting days, the despair caused her to think about how she could fight back and regain control of her health.

“I started to religiously track my health in journals before transferring to Excel spreadsheets. I was so frustrated by how exhausting and impossible it felt to crunch that much data, so I turned to searching for a symptom track and correlative software to help me. I downloaded and tried every single one I could find – but none met my needs. Some even gave me back faulty data which made me angry. That’s when I decided to create a solution myself,” she explained.
In 2020, after losing access to all her healthcare management tools, and with her health declining rapidly, she decided to create Corra.
The meaning of Corra
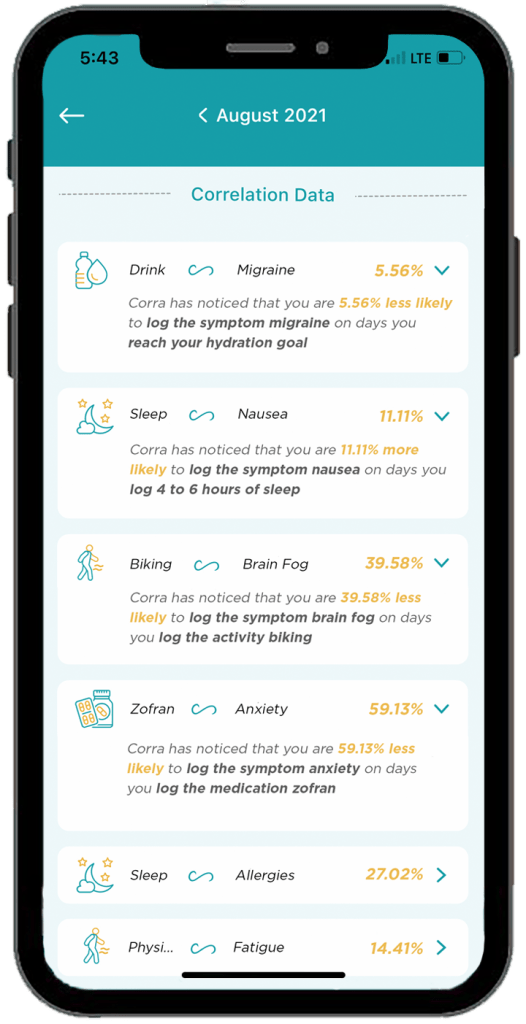
There are quite a few chronic illness apps on the market, some that even attempt to offer correlative insights. Corra is short for correlations. Elya wanted to identify correlations in her health so that she could find her triggers and optimize her lifestyle.


Here’s what sets Corra apart from other chronic illness apps on the market:
- The algorithm was custom built by Corra’s chief data scientist, Simeon Wilson, who has a master’s in quantitative economics from UCLA. “We are not aware of any software that exists that compares to what Corra is currently offering with our correlative algorithm.”
- Corra was designed by individuals with chronic illness. “Not just me! While the idea and original designs are all mine, we brought on more than 200 beta testers with various chronic illnesses to provide their feedback and help us tailor the app to the needs of the chronic illness community. Even now, we continue to rely on the insights and feedback from the community to enhance and adjust the app. I want Corra to always be designed by and created for our community.”
- We correlate with nutrition in an accurate and helpful way. “I believe nutrition plays a massive role in our health so one of our key focuses with our algorithm was to be able to correlate seamlessly with nutrition inputs.”
- Corra does not sell user’s data. “We don’t scrape your data from your device or browsing history, we don’t use your data to sell you anything, we don’t share your data with third parties. Your data is yours alone. As an individual with a chronic illness who often feels more like a commodity than a person, making sure people can receive personalized insights into their health without signing away their privacy is incredibly important to me.”
Corra’s bells and whistles to check out
- The ability to track health data in one place without having to use five different apps to log information. “My favorite part of Corra is of course the correlations, because getting detailed insights like that about my health is equivalent to having a team of data scientists run extensive tests on my health and provide me reports. It’s life changing to be able to learn about my health overtime and create a custom-built lifestyle that caters to my future.”
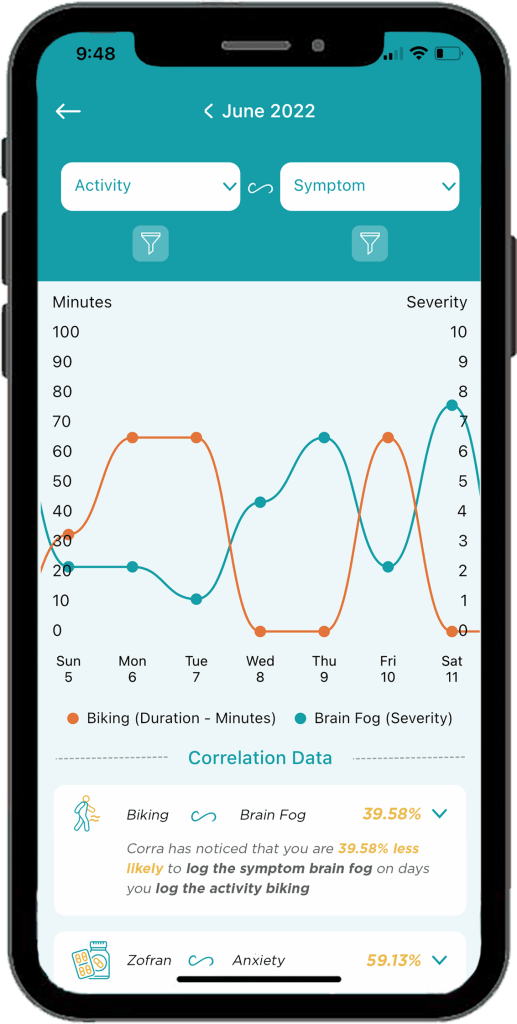
- Discovering positive and negative correlations. “You may receive insight that something has x% chance of increasing or decreasing a symptom. I think being able to get data on the things that are helping is just as important as being able to identify triggers.”
- The ability to log appointments, download PDFs of your data to share with my doctor, track medications and supplements, track mood and stress levels, etc. “I’m also extremely excited about all the upcoming integrations we have in the works! Soon we will be connected to Fitbit and Apple Health with Garmin, Cronometer, Weather data, and hopefully Oura coming shortly after! Over time we will continue to integrate with as many devices and apps as possible so users can have all their data in one location!”
A promising future
Elya says being able to learn what foods, activities, supplements, and medications help or cause symptoms has enabled her to have a much better understanding of how best to manage her health conditions.
“I’ve been told to go vegan, cut out red meat, don’t eat dairy, sugar, gluten, eat paleo, try a carnivore diet, go vegetarian, and try cutting out leafy greens… what I found with Corra is that I didn’t need to make these drastic nutrition changes, I only needed to cut out some foods in each of those categories. For example, I discovered that I have a high trigger correlation with ground beef. I can eat steak and other red meat, but not ground beef. Similarly, chicken thighs are a trigger for me, but chicken breast is not. Same with gluten, there are some gluten products that are triggering for me, but not all gluten triggers me. Being able to identify exactly which foods to cut out, rather than willy nilly cutting out entire food groups or going on drastic diet changes, has been an absolute game changer.”


Elya has also discovered that cold and flu medications like Mucinex are major triggers for her. This helped her realize why she would get a horrible flare a few days after coming down with a cold or flu.
“Now, I try to manage my colds and flus with other medicine to try to prevent the flare on top of the cold. It’s also important to note that I’m not cured! I have to manage my diet and my activities and my supplements every day. The difference is, I’m no longer throwing shots in the dark, I now have the information I need to manage my condition to the best of my ability.”
Information really is power, and it has given Elya control over her life and reduced her anxiety. Because of Corra, she is now coming up on two years without the need for daily antibiotics. It’s been over 2 years since she visited the emergency room.
“I’ve found that medical providers are far more willing to accept unbiased data from an algorithm than trust my verbal expression of my experience, so in that way Corra becomes my advocate and backs up my statements,” said Elya.


She says her health conditions have caused her to go through depression, isolation, and hopelessness. But her hope for Corra is two-fold.
“First, I believe it can help others identify their triggers and optimize their life so that their conditions can become more manageable, but I also hope that Corra can be a beacon of light for those struggling to see they are not alone. There are so many steps between the start of symptoms and any kind of treatment let alone cure (depending on if your condition is even curable)… and I want to be the one that goes into the trenches and helps people who are suffering the most. So many people in the chronic illness community get forgotten or left with “your test results are normal” when they know there is something wrong with them. I want to create a company that comes alongside them and lifts them up and allows them to have their voices heard.”
Downloading Corra
You can download Corra directly from the App store or the Android playstore. There is a free version as well as premium access. The premium version is $7.99/month or $24.99 if you enroll for a 6-month subscription. Elya is looking for Corra Insiders who are interested in getting free access to the app. By joining the Insiders group, you get a first look at upcoming features. This provides you the opportunity to share feedback on what you do/don’t like or would like to see improved or added in the future. Sign up for the Corra Insiders program here.











