When something traumatic happens—like the mass shooting in Uvalde that left 19 children and two adults dead last week, the stress, sadness, and overwhelming grief can cause IBD to spiral out of control. You are not alone if the heavy nature of what’s happening in the world causes your mind to race and your GI symptoms to be amplified. As May (Maternal Mental Health month) comes to an end, a look at how we can best navigate these emotions and how our thoughts impact the gut-brain connection.
Looming threat of flares and violence
With the constant news cycle that bombards us, added into our reliance on social media, and seeing everyone’s opinions and posts, it’s the perfect storm for feeling suffocated by sadness. Life with IBD, whether you are in remission or not, is living with the looming thought of when your next flare or hospitalization is going to be. You know in your heart of hearts that it’s not a matter of if, but when your IBD is going to rear its ugly head. These days with violence happening left and right, it’s a challenge not to wonder and worry when you’re out in public if you’re going to be in the wrong place at the wrong time or if your children are in harm’s way.
The anxiety of worrying about the “what if” and the pain of grieving can often correlate to actual physical pain in our bodies that are already fighting an uphill battle. It’s difficult to try and make sense of what’s going on in the world. It’s impossible to try and wrap your brain around how people can be so evil. As a mom, I found myself crying putting each of my kids to sleep last week. Snuggling them a little longer. Worrying about their wellbeing and praying as hard as I could over them.
As a former news anchor and journalist, I vividly recall the moment the news of Sandy Hook broke. I was standing in the newsroom, about to head out to the studio to anchor the Midday show, when the heartbreaking news came over the newsfeed. It was incomprehensible then and it’s even worse now as a mom of three. I have only been able to watch the news in short snippets right now because I felt like the sadness of it all was consuming me in an unhealthy way. There’s a guilt that comes with trying to tune out the coverage and feeling like you’re not giving the reality of other peoples’ heartbreak the attention it deserves, while trying to protect your own mental state and heart.
Dr. Lindsay Hallett (Zimmerman), PsyD, is a clinical psychologist in Indiana. Here is her advice for coping:
Give yourself half the grace you give to others. This can make a significant difference in your overall well-being and stress level.
Reach out. If connection feels like what you truly need, enlist a friend or relative. The higher the level of personal connection, the better- seeing a friend is preferable to FaceTime, a phone call is preferable to texting, etc. But also, any connection is better than none.
Make time to move. Time is a premium to everyone and even 15 minutes will do. Listen to your body and give it what it needs – stretching, a walk, an intense workout, gardening… any kind of movement that respects your body’s own capabilities.
Give yourself permission to check out. If everything feels to be “too much,” avoidance can be healthy. Communicate healthy boundaries with others that you can’t talk about topic XYZ right now.
Seek therapy. Your emotional house doesn’t have to be “on fire” to benefit. Ask your primary care doctor, contact your insurance company, or research PsychologyToday.com to find a therapist. In-person with occasional virtual supplementation is best, but online therapy platforms can be helpful if you aren’t having luck otherwise.
Give yourself permission to unplug and stop doom scrolling. While there is no “right way” to cope with traumatic events like what happened in Uvalde and so many times before, give yourself permission to feel whatever complex emotions you are experiencing while also giving yourself space and time to take breaks and turns off screens. When you have IBD, being cognizant of what triggers you and recognizing how your symptoms speak to you, can allow you to stay one step ahead of the game in managing your illness. Focus on what’s tangible, what’s right in front of you, and what you are able to control.
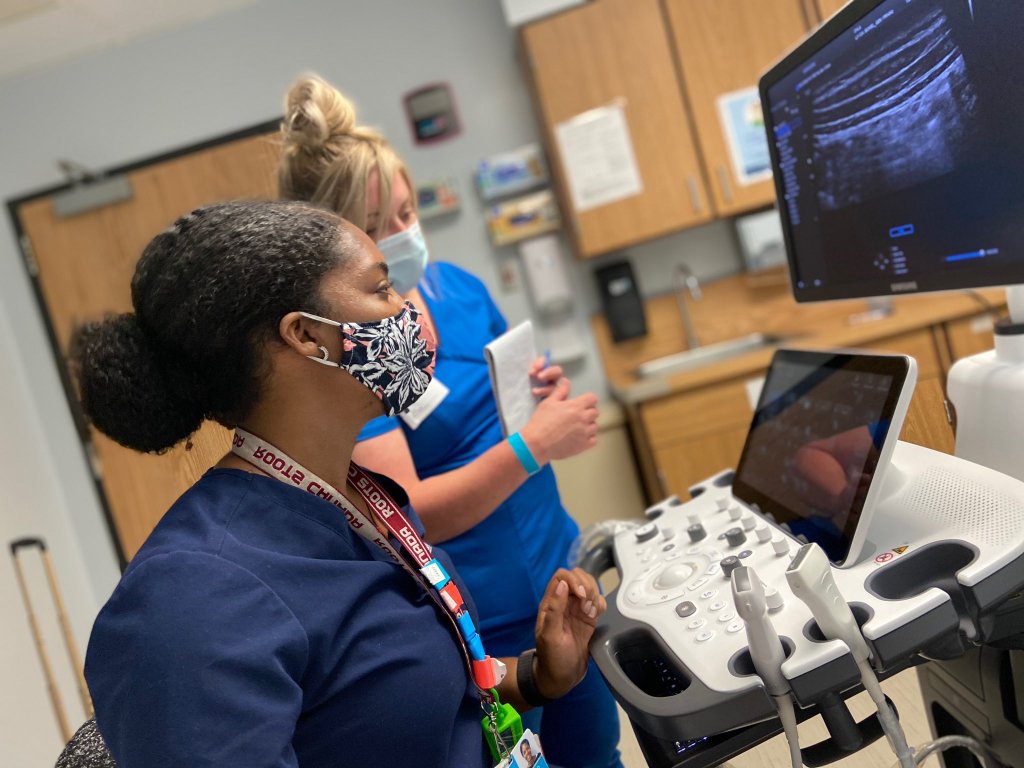
Innovation and changes in healthcare are propelled by patients and caregivers speaking up about improvements that can change the way IBD is treated and managed. This week on Lights, Camera, Crohn’s we hear from pediatric gastroenterologists Dr. Michael Dolinger, MD, MBA, Advanced Pediatric Inflammatory Bowel Disease Fellow, Ichan School of Medicine at Mount Sinai and Dr. Mallory Chavannes, MD, MHSc, FRCPC, Pediatric Gastroenterology, Hepatology and Nutrition, Children’s Hospital Los Angeles about the benefits of Intestinal Ultrasound (IUS) becoming a part of routine care, regardless of age.
The goal of IUS is to utilize a non-invasive method to monitor disease activity over time and it’s considered to be more precise than endoscopy in identifying both disease location and characterizing the severity of IBD. The IBD community—both patients and caregivers—can help fuel the adoption of IUS and gain access to receiving more information about their disease activity than ever before.
What is Intestinal Ultrasound (IUS)?
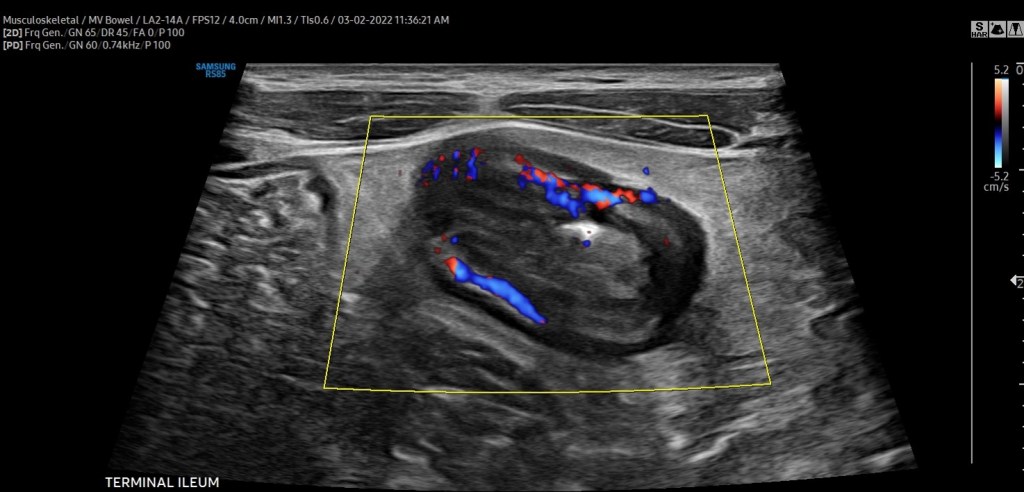
Intestinal Ultrasound (IUS) is an abdominal ultrasound performed during a routine clinic visit without preparation, fasting, or contrast to assess both the colon and the small intestine (terminal ileum most frequently) for the presence of disease activity. Probes are placed over the abdomen and the provider looks at images of the small and large bowel.
“The beauty is that, unlike procedures and other image modalities available to assess disease activity of inflammatory bowel disease, IUS can be performed without any preparation or fasting,” said Dr. Chavannes. “In the setting of active disease, patients can have a thickened appearance of the wall of the bowel (termed increased bowel wall thickness) in both the small intestine and the colon, which can be detected via ultrasound.”
In addition, by using color Doppler, a feature that assesses the velocity of blood flow within and around the bowel wall, gastroenterologists can demonstrate inflammatory activity in the bowel wall. IUS can also detect IBD complications, such as fistulas, abscesses, or strictures (narrowing) of the bowel.
“Our expectation is that, with effective therapies, the aforementioned features of disease activity should improve or even disappear over subsequent clinic visits. If they do not, we now have an objective tool available in the clinic that can assist clinical decisions, such as ordering further investigations or even optimizing or changing therapy. Improvement of bowel wall thickening or decrease in color Doppler signaling is a reassuring sign that treatment is working. Lack of improvement signifies that optimization or changes in therapy should be considered,” explained Dr. Chavannes.
“Intestinal ultrasound is precise, we monitor bowel wall thickness down to the 0.1 mm. We are now able to make informed decisions with patients together, assessing their disease objectively in real-time so we can be aligned with our treatment goals. This reduces misunderstanding and may lead to better treatment adherence and improved outcomes,” said Dr. Dolinger.
Why the delay in the United States?
While IUS isn’t the standard of care across the world, it is used in several Canadian IBD centers and in Europe (Germany, Italy, Norway, the Netherlands, and Australia to name a few). However, there are still many areas of Canada and countries in Europe where this is not used as part of routine IBD care.
“There have been several barriers to adoption in the USA, the biggest of which are reimbursement and the lack of training/expertise. However, that is changing, as there is a tremendous amount of interest from most major academic centers,” said Dr. Dolinger. “Through the International Bowel Ultrasound Group (IBUS) there is now a formal training, while intensive, that can be completed by anyone willing in the USA, which did not exist 5 years ago.”
IUS fits perfectly in the treat-to-target algorithm by adopting a monitoring strategy that helps to prevent flares and bowel damage.
“There is no other test for patients to see their disease dynamically with a gastroenterologist in real-time, which enhances shared understanding and informs decision making like never before. All of this will help break the barrier in the USA and around the rest of the world,” said. Dr. Dolinger.
A study conducted in 2016 explored why IUS is not standard of care in the United States. The
authors surveyed nearly 350 physicians, of which 40% were pediatric gastroenterologists. Although a minority of gastroenterologists were using ultrasound to assess and monitor IBD (either bedside or within the radiology department), over three-quarters expressed interest in using it more.
“The main limitation identified or perceived by gastroenterologists who responded to this survey was a concern for inter-observer variability, a lack of familiarity with ultrasound indications and techniques, and a lack of interest and access to pursuing additional specialized training. In addition, the survey identified a common message that I have received previously from some radiologists; that other modalities are more precise or effective in assessing IBD. All these reasons can hinder interest and implementation,” said Dr. Chavannes.
However, considering the multi-center effort in disseminating training, knowledge, and engagement that has been ongoing in the USA in recent years, Dr. Chavannes is hopeful that IUS will rapidly become the standard of care nationwide.
How Children’s Hospital in LA and Mount Sinai in New York Use the Technology
The Henry and Elaine Kaufman Intestinal Ultrasound Program at Mount Sinai is one of the first in the country to employ the training of gastroenterologists and regular use of intestinal ultrasound for both children and adults routinely in the IBD center for non-invasive disease activity monitoring.
“This would not be possible without the leadership of Dr. Marla Dubinsky, who has worked painstakingly hard to bring this to patients at Mount Sinai, overcoming every barrier to lead the way in the USA. We would like patients everywhere in the USA to be able to have tight control non-invasive monitoring with intestinal ultrasound and in turn, are working with International Bowel Ultrasound Group (IBUS) to host the first hands-on training in the USA at Mount Sinai in the fall. We have faculty from around the country signed up to learn and this will hopefully begin to fuel further adoption,” said Dr. Dolinger.
Intestinal Ultrasound was introduced at Children’s Hospital in LA in the summer of 2020. This was incredibly helpful during the pandemic when access to endoscopy time was difficult, considering cancellations due to active COVID infection and decreased daily procedures to allow for intensive cleaning protocols.
“We integrated using IUS for all patients coming to the pediatric IBD clinic. We have seen an immediate benefit in how we approach patient care and how timely clinical decisions can be made right at the time of the clinical encounter. One example is for patients presenting for a second opinion; these patients usually present with ongoing symptoms of varying degrees, yet incomplete or dated documentation of endoscopy, fecal calprotectin (a stool test helpful in indicating inflammation), and blood work,” said Dr. Chavannes.
During the visit, IUS gives an opportunity to understand the source of the symptoms experienced by patients and the degree of ongoing inflammation. Then, clinical decisions can be made that day, eliminating the need for additional testing. Dr. Chavannes says IUS even helps ease the discussions she has with parents and families.
“Many parents are stunned by the images they see and the changes over time. At the same time, they also notice when there is little difference from one appointment to the next, understanding the reason we are making the changes to the management plan that follows,” said Dr. Chavannes. “IUS has been invaluable for children under 6 years of age. This vulnerable population needs frequent objective reassessments, which is not possible otherwise. Using MR-Enterography would require general anesthesia, and access can be difficult. Similarly, for endoscopy, the prep can be poorly tolerated, and it also requires general anesthesia. IUS is non-invasive, painless, very well tolerated in young children, and available in real-time. Therefore, both parents and children are quite satisfied with their experience with IUS.”
Targeting treatment through IUS
Monitoring symptoms alone is not effective in reaching deep healing of disease in IBD, as many patients feel well despite having ongoing intestinal inflammation. IUS evaluates the inflammation that occurs within the thickness of the bowel wall (transmural inflammation).
“We often find that ultrasound is the only tool that shows continued inflammation when patients are in remission and labs have normalized. Optimizing therapies based on persistent inflammation seen on ultrasound may prevent us from falling into the trap of thinking our medications are working when our patients feel better and thus lead to better outcomes by not missing persistent inflammation that we have continued to miss with traditional monitoring strategies,” said Dr. Dolinger.
Although there are no fully established algorithms for the frequency of monitoring IBD using IUS, the best approach appears to have a baseline IUS at the time of IBD diagnosis or in the context of active symptoms or elevated inflammation markers on blood work (a flare).
“Then, the clinician can understand the features to follow over time. A repeat IUS can be performed at the end of induction treatment to assess how effective the management is. It would represent 6-8 weeks after the treatment was started. Provided that there is a marked improvement, the subsequent evaluations with IUS can be done every 3-6 months unless there are new concerns, with the closer timeline early in the disease course,” explained Dr. Chavannes.
In pediatric patients, this routine ends up matching most routine clinic visits. Therefore, as IUS becomes standard practice, and depending on how a patient is doing, their symptoms, and last assessed disease activity, patients can expect IUS as often as with each clinic visit. This modality would complement blood work and calprotectin stool tests in informing about disease activity and for complications of disease or flares.
What the future holds
Since a few IBD centers in the United States have already implemented regular IUS in their practice and have been disseminating knowledge about this technique, there is growing interest from pediatric providers to join the movement as well.
“Considering the challenges pediatric providers face in access to complementary imaging, operating room time, anesthesia exposure to endoscopy, and even the tolerance drinking contrast for radiology studies, IUS offers a fantastic way to assess disease activity in the pediatric IBD population. I am excited about the number of pediatric centers that have reached out about getting expertise in this field. The key is to promote buy-in from leaders in each institution to get the time and resources required for training and implementation,” said Dr. Chavannes.
Advice for patients and caregivers
It doesn’t hurt to bring up IUS at your next clinic appointment to gauge where your care team stands and if anything is in the works.
“If your provider is unaware of IUS and its benefit, it would be great to talk to them about the International Bowel Ultrasound Group. The curriculum for getting training involves three modules: an introductory module, a 4-week hands-on training at an expert center, and a concluding module and examination part of the European Crohn’s Colitis Congress,” said Dr. Chavannes.
She went on to say that hearing this request from patients may motivate administrators to provide the necessary time clinicians who are interested in getting expertise to implement the tool at their center would need.
Dr. Dolinger believes most major academic IBD centers in the United States will rely on IUS in the next 3-5 years.
“I would like to remind patients to be patient with their providers. Ensuring correct training and standardization is essential for adoption in the USA and this takes time and rigor to be done right and change the monitoring algorithm which has not been done in many years,” said Dr. Dolinger. “I began training in 2019 and it wasn’t until the second half of 2021 that we began using it very routinely for decision making, taking 2 years to become an expert. So, this will happen, but it will take some time.”
Patients and parents are big fans
The safety and efficacy of IUS can’t be matched. It’s also a big-time saver for everyone involved. A bedside ultrasound can be performed in a range of 20 minutes for the first thorough assessment, while an even more focused exam in a known patient can take less than 10 minutes.
“Both parents and children have been quite satisfied after their experience, as children can go back to school after the clinic despite undergoing this examination. Furthermore, the time saved in skipping additional appointments with the radiology department or procedures can be invaluable,” said Dr. Chavannes.
For parents, the imaging provides reassurance when there are improvements or when there are non-specific symptoms, yet the IUS is normal. IUS also bring validation when there are abnormal findings and helps to provide an explanation for why children are feeling a certain way.
“Children appreciate that it does not hurt and takes little time in addition to their clinic visits. In addition, they may not require additional appointments in radiology or endoscopy. Parents who had an opportunity of experiencing an ultrasound often request it afterward as part of their clinic visits. These families are more engaged and participate in shared decision-making. I am pleased and impressed at the engagement that actually “seeing” the disease together brings from families,” said Dr. Chavannes.
While the push is for IUS to be available to all IBD patients, both children and adults, it’s specifically beneficial for the management of pediatrics as it provides the unique opportunity to prevent bowel damage for a person’s entire life and reduce the need for invasive procedures, anesthesia, and sedation. IUS has the potential to alter scoping schedules in the future. While it will not replace the need for colon cancer screening or the assessment of mucosal and histologic healing, IUS can reduce the need for further follow-up scopes once those targets are achieved in between the need for cancer screening.
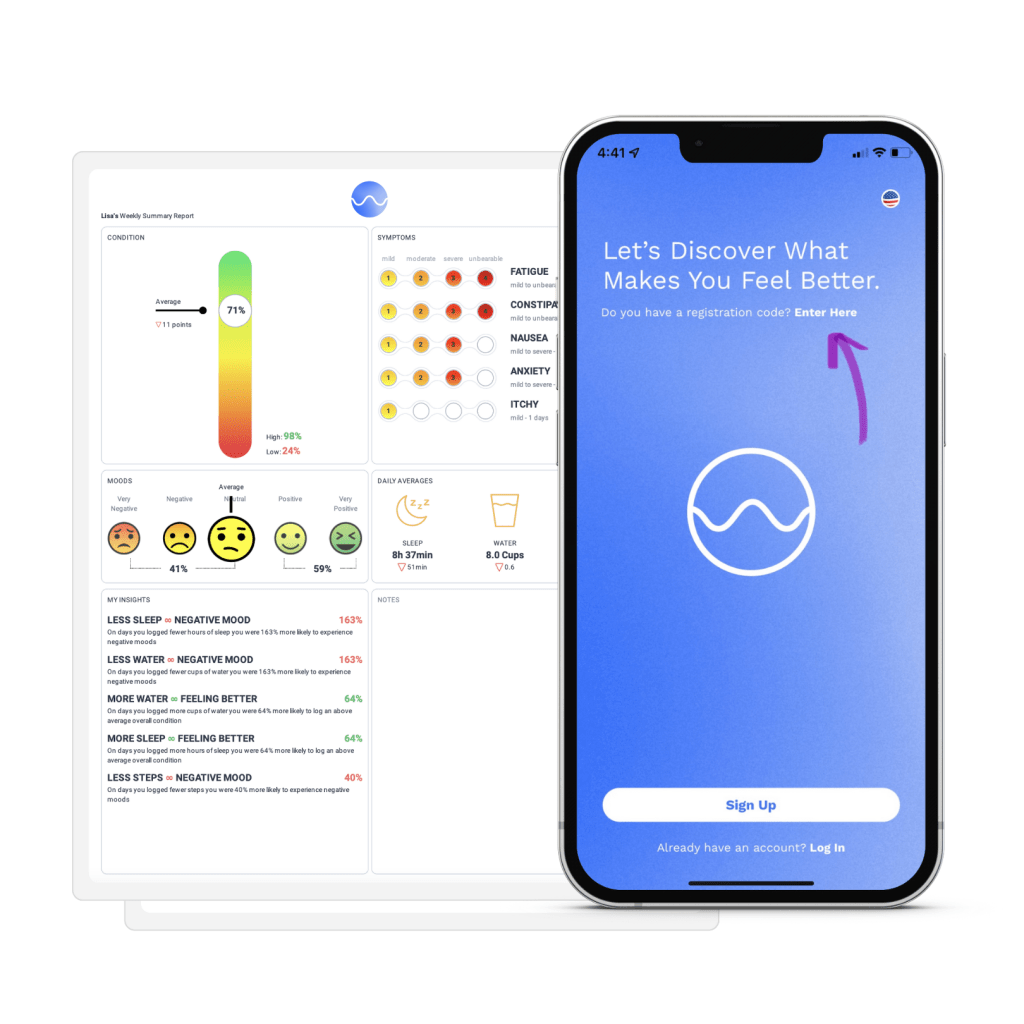
This blog post is sponsored by Wave Health. Thoughts and information shared are my own.
What started as an app designed for cancer patients in 2019, now spans more than 250 chronic health conditions, including inflammatory bowel disease. Wave Health is a free, easy-to-use, comprehensive tool that empowers patients to use their daily health data in practical and effective ways, while enabling those in our community to be more involved in their care and treatment decisions. This week on Lights, Camera, Crohn’s a look at the story behind how Wave Health came to be what it is today and how the app can be a transformative tool in how you take on your IBD.
Hear what Claudia Zhao, the Marketing and User Engagement lead at Wave, has to say about the inspiration behind their mission.
“Wave Health App was inspired by a personal patient experience. In 2013, one of Wave’s founding partners was diagnosed with non-Hodgkin’s lymphoma. During his treatment, Ric’s partner, Matt (now the CEO of Wave Health) began to record extensive data by hand — things like his diet, hydration, exercise, mental engagement — anything that might impact the side effects Ric faced during his chemo and drug therapy. With this information, they were able to provide their doctor with real-time, individualized information, and identify relationships between what Ric was doing and the side effects he was experiencing. Protocols were shifted and Ric began to feel better,” said Claudia.
Matt transformed his data analytics system into chemoWave, an app for cancer patients like Ric. Soon, they realized that anyone with a chronic illness would benefit from a health management and insights tool like chemoWave, and they created Wave Health App.
“Wave’s mission is simple: to help every patient take control of their own journey. Wave serves to empower patients to use their everyday data in ways that allow them to be better partners with their care team and ultimately improve their at-home and treatment decisions.”
What sets Wave apart from other IBD-related apps
Most IBD-related apps focus on tracking symptoms and a few other activities such as meals, bowel movements, and medications. Wave Health is different in that it serves as an all-in-one health diary.
“In addition to the more obvious activities to track in IBD management, Wave also lets you track vitals, sleep, menstruation, and even mindfulness activities like meditation and breathing. Wave then gives you personal insights, not only about your symptoms, but also about what’s impacting your moods and wellbeing. Wave helps you manage your IBD-related symptoms, but it also acts as your overall health companion.”
Having a companion to help guide the way you manage and treat your IBD can help ease the isolating nature of our disease. Often life gets busy, and we forget how much our Crohn’s disease or ulcerative colitis takes a toll on our day-to-day activities. It’s easy to generalize or downplay the struggle when it comes time to share how you’re feeling to your care team. Wave takes that guesswork out of picture and is a win-win for everyone involved.
A systemic review out of Cedars-Sinai Medical Center recently found the app to be the highest rated symptom and PRO tracker for cancer patients.
“This speaks to the fact that Wave is easy-to-use, while also providing real, tangible benefits to the patient journey. In addition to being rated the highest overall PRO tracking app, Wave also received the highest individual scores for both engagement and aesthetics, two very important pillars for any type of user experience. Since the review in 2020, Wave has also done a complete UI/UX redesign. With a more intuitive interface and new features that make health tracking even easier, the experience of using Wave is only getting better,” explained Claudia.
How Wave expanded beyond the cancer community
Beginning exclusively as a cancer app, Wave was expanded to serve all chronic illnesses because of the underlying challenges that patients face regardless of their specific health issue.
“The nature of most treatments is that they are standardized — protocols shift only after periods of trial and error. Wave identifies relationships effectively and quickly, so that treatments can be tweaked, and side effects can be alleviated or avoided more promptly.”
Another key focus of Wave is on filling the gap between doctor’s visits. Most of the patient experience occurs at home, not in the doctor office, and currently there is no sufficient system or way for patients to easily report their symptoms and other outcomes during these critical periods.
“Wave helps patients fill in their care team, whether it’s about how their symptoms have been improving or how many days they’ve missed their medications. With a comprehensive record of patients’ daily and treatment activities, doctors have a more complete picture of the patient and their journey and are enabled to make more-informed decisions from there.”
Wave can help anyone
You also don’t have to be “chronically ill” to use Wave and see its benefits. Tracking and getting Wave’s A.I. insights can help anyone improve how they feel. Wave is a health management tool for anyone looking to take control.
“The app empowers patients to take control of their own journey. Just by harnessing their own daily health data, they can get powerful information into what helps them feel better or worse and then adjust their at-home activities to optimize their wellbeing. Second, Wave helps patients communicated better with their doctors on what they’re experiencing between visits. Patients can share/email their logged data directly through the app, or they can receive easily shareable Wave Pro PDF reports,” said Claudia.
How Wave Pro Works and a 6-month FREE discount code
The reports summarize a patient’s important health data and insights from the week, allowing them to see both short-term and long-term trends and changes. Users can download these reports and bring them into their doctor’s visits. Wave Pro is available through a monthly ($10.99) or annual ($54.99) subscription, with a free 30-day trial at sign-up.
Enter the code LIGHTS right away at sign-up and receive 6 months of FREE Wave Pro reports.
This week I was feeding my 9-month-old a smoothie in his highchair before I had to run to grab my older two from preschool. I realized it was an injection day, so I figured I would do my shot while the baby was in the highchair to get it out of the way. It seemed like no big deal in the moment. But as I sat there and saw the baby food next to my Humira on the kitchen table I started thinking about how life as an IBD mom may feel normal to us, but what we do each day goes above and beyond.
Then my mind started wondering. I thought about how I had taken my oldest to his outdoor fieldtrip last week and refrained from having my morning coffee or eating breakfast so I could curb my Crohn’s from causing me problems. I thought about how my 3-year-old is so intuitive if she thinks I’m in pain, she grabs my belly and pretends to put the pain into her belly, telling me “I love you mama, take a breath.”
Take a breath. Boy oh boy do mothers in general need to stop and take that advice or what? Motherhood whether you have IBD or not is the most beautiful, exhausting, and rewarding challenge. No matter what season you are in it comes with triumphs and challenges it comes with happy tears and sad ones, too. It’s a constant game of trying to manage your emotions and tap into your patience, or whatever is left of it each day. We come to forget that we are also growing up in many ways, just as our kids do.
Motherhood and IBD is a balance of wanting to be all the things but knowing that at any given moment your body can throw your life and plans upside down. There are unspoken limitations.
It’s silently worrying and praying what will happen to your family if you go down and end up in the hospital.
It’s trying to stand tall when all you may want to do is rest on the couch.
It’s seeing your children thrive and feeling so much pride you constantly feel like you can cry tears of joy at any moment.
It’s getting scared when your little one randomly says their tummy hurts.
It’s knowing that your disease robbed you of a great deal—physically, mentally, emotionally, but it didn’t rob you of the greatest gift of all, being a mom.
It’s recognizing all that is still possible, even with this grueling disease.
It’s showing up each day, not only for yourself but for your family.
It’s taking the pain and feel-good days and focusing on one moment in time that feels slow but is going by in a flash.
Take a breath. You deserve it. We weren’t meant to mother alone. Lean on your village. Voice your struggles. Cry if you want to cry. But also, don’t put yourself to unattainable expectations. You have a chronic illness and you’re a mom. Don’t push yourself to the brink. Some days will be adventure-filled, others will be spent on the couch—and that’s OK. Your children are learning from you and gaining innate intuition, and that’s a gift. They’re witnessing that health is not something to be taken for granted. They’re watching you even when you think they are not. What may feel mundane to you, is not. As an IBD mom you are juggling countless extra balls in the air that healthy mothers don’t have to think about. Give yourself credit where credit is due and take a breath.
Moving away for school. A future career. Relationships. Discovering your identity. Switching from a pediatric IBD care team to adult providers. All while living with a chronic illness. This is the stark reality for young adults living with Crohn’s disease and ulcerative colitis. Juggling all these major life milestones and having to get acclimated to new physicians while taking the lead on disease management is often met with anxiety and worry from young patients, their parents, and caregivers. IBD is a family disease. Even if only one person in the household personally lives with the issue, the disease impacts each person.
This week on Lights, Camera, Crohn’s we hear from patients and caregivers who have lived through the experience and from pediatric GI’s about how best families can be supported through the changes to make them as seamless as possible for everyone involved.
Input from those who have made the switch
Aging out of pediatric doctors can be a stressful time for everyone involved. Let’s start with input from those with IBD who have made the switch along with what some parents and caregivers had to say.
Start researching doctors early. Do your homework and see what insurance providers accept and what hospitals they are affiliated with.
Ask your current pediatric doctors for recommendations/referrals.
Before the first visit make sure the adult GI has received copies of medical records.
Have healthcare proxy and power of attorney papers on file.
“I just turned 20, but I’m still in pediatrics and plan on staying until I graduate from college, as that is the norm at my hospital. However, as an adult in peds, I found it important to have healthcare proxy and power of attorney papers on file so my mom can still help me and if something were to happen like while I’m away at school she is able to get information. I broke my arm this past fall and my body went into such shock that I couldn’t give the hospital any information. My friends were with me and contacted my mom, but because I was 19, the hospital couldn’t even confirm to her that I was in the building. This was a wake-up call. We started thinking about, “what if this was my IBD?” and decided it was necessary to have the papers on file just in case. I still ask my mom to be involved in my care, but we both have the understanding that I have the final say.”- Anna
Navigating the switch through college
Heidi was diagnosed with Crohn’s when she was 9. She’s now 41. When she reflects on the transition from a pediatric doctor to one who treats adults, she recalls the process being fairly simple and a change she welcomed with open arms.
“The best thing was being talked to directly and my opinions mattered more in my later teenage years with the new doctor. Of course, my parents had my best interests at heart, but appointments were so frustrating as a young girl. Another reason for the seamless transition was that my new doctors were amazing. I switched at 18 and then again at 22 when I graduated college and moved away from home. My care team listened to me and saved my life. I know I’m lucky to have found such a wonderful team of doctors.”
Katie wishes there had been a support group (even online) for teenagers back when she was phased into an adult GI. She says when she was diagnosed with IBD at age 15, she often felt uncomfortable discussing her symptoms and didn’t feel her pediatric GI was that great with kids.
“I felt detached from my GI until I was in my 20s and had the confidence to advocate for myself. I was so lost and refused to tell classmates what was wrong with me for fear of being made fun of. I ended up missing so much school I decided to drop out, get my GED, and go straight to college. It was a terrible time to be honest.”
The difference in pediatric vs. adult care
“The transition happened quite fast as I was being referred to an adult surgeon for my complications that the pediatric team were not experienced or educated enough to treat for Crohn’s. I was thrown in the water with no guidance when I started seeing physicians who treated adults with Crohn’s. The pediatric GI team would dumb some things down for me and make my problems not seem “as bad.” As soon as complications started arising, they threw the towel in and basically told me they couldn’t help me anymore and would be better off seeing a care team with more experience with my symptoms and complications.”-Chrissy
Natasha experienced the transition about 13 years ago. Her pediatric team helped her choose an adult GI. And the guidance didn’t stop there.
“My pediatric GI told me who she wanted for me and then went with me to interview the doctors in the adult team. Once I chose, my pediatric GI attended every appointment with me until we all agreed I was ready to move into the next step of my care, which luckily was quickly. And the two doctors stayed in communication. My advice—be open with your doctor.”
Natasha recommends asking yourself the following questions to help streamline the process and make it less nerve-wracking.
What are you looking for in your next step of care?
What are you looking for during the transition process?
What is important to you in a physician?
Do your own research
“I had an AMAZING pediatric GI when I switched, and I just went with who she recommended. Looking back, I wish I did my research because he is not who I would have chosen for myself. I would recommend doing your own research and make sure whoever you find is willing to work with you and thoroughly go through your medical history and all your results. Too many doctors seem to just think they know everything, but we know our bodies best and need to have a medical team who lets us advocate for ourselves.”-Danielle
Jennie has lived with IBD for nearly 20 years. She has a PhD, works in IBD care, and recognizes she has the privilege of a strong support network and insurance. As an IBD psychologist she recognizes how difficult the system and transition can be for everyone involved.
“I was diagnosed with IBD at 12 and transitioned to adult care around age 18. I was extremely sick at the time and ended up having a proctocolectomy within months of transitioning. I think the biggest things for me were the notable shift in culture between the peds and adult world, and the insurance pieces. It’s so much for kids and families. Lastly. I’ve noticed the transition is nuanced for my parents who were so good at being my advocates, they will still offer to call the doctor if I tell them I am not feeling well, and they have a tough time not having the same significant role they did when I was younger.”
Allie was diagnosed with Crohn’s disease when she was 12. Her mom attended all her appointments until she turned 18, and only stopped going then because she was out of state for college and seeing a pediatric GI there until she turned 22. Allie’s mom kept a medical binder of all her procedures, lab results, and details about her patient journey. She says when she phased out of pediatrics and started taking matters into her own hands, she found the binder her mom made to be beneficial—Allie found herself referring to it when she couldn’t remember everything.
“What helped the transition the most was going to appointments on my own when I turned 18. I felt more prepared to speak for myself when I switched to an adult GI.”
Allie’s mom also inspired her to ask the tough questions. After witnessing how her mom spoke up to doctors it empowered her to speak up and stop minimizing her struggles. By watching how her mom handled appointments, it inspired Allie to write down all her questions and concerns before doctor appointments, so she doesn’t forget anything.
“My mom asked me what fights I wanted her to fight for me and what I wanted to do myself. She guided me on what I might need to ask about when I had no clue—even as an adult she still offers to help call insurance companies to fight authorization battles. She gave me space to live my life when I turned 18. She worried, but she never hounded me for updates (are you taking your medication?, how are you feeling? Are you eating ok?”…but she always conveyed support (both my parents did) when I needed it most she showed up.”
Sari recommends young adults with IBD to ease into taking control of their care as early as possible.
“Things like refilling your own meds, scheduling your own appointments, and driving yourself to appointments goes a long way when it comes to learning how to stay organized and advocate for yourself. You don’t want to be doing all those things for the first time when you go to college or a start a new job—too many scary or unknown things at once!”
Check out what pediatric GI’s have to say about bridging the gap and ensure continuation of care.
Dr. Sandra Kim, MD, Associate Professor of Pediatrics, Director, Inflammatory Bowel Disease Center, UPMC Children’s Hospital of Pittsburgh, says, “Transition is the preparation process while the young adult/teens are still under the care of the pediatric team. Transfer of care is the actual “handoff” when the young adult moves from the pediatric GI team to the adult GI providers. Teens want independence but struggle with disease knowledge and self-management skills. Therefore, the pediatric GI team needs to help the teen (and the family, too!) by being active listeners, communicators, and educators. The healthcare team also should utilize things like transition tools.”
Dr. Kim went on to say that GI doctors need to assess how teens are doing on the road to greater independence and that shared decision-making helps build partnerships between adult and pediatric GI providers.
For the adult GI team:
Collaborate with the peds team in the initial stages of care transfer.
Anticipate existing gaps of knowledge and self – management skills
Prepare for more time during appointments for questions, additional education, and working with the family. Parents need help during this time of care transfer, too!
Woman patient signing medical documents discussing medication treatment with african american practitioner in hospital office during clinical consultation. Doctor physician explaining disease symptoms
Dr. Jonathan D. Moses, Assistant Professor of Pediatrics, Director, Pediatric Inflammatory Bowel Disease Program, UH Rainbow Babies and Children’s Hospital, explained how his hospital has a multidisciplinary pediatric IBD team that engages patients in a Health Maintenance Education Clinic as early as 11 years old.
“This allows them to build up the self-management skills needed for a successful transition to adult GI, when they are ready. In lieu of this resource, parents can engage their health care providers about ways to get their child more involved in their care and provide them with the autonomy, and support, to take over aspects of their care over a period of time.”
Dr. Hilary Michel, MD, Assistant Professor of Clinical Pediatrics, Nationwide Children’s Hospital, says a successful transition from pediatric to adult care requires that young folks have developed the knowledge and skills needed to understand and manage their disease independently.
“This knowledge and skill is not gained overnight, and ideally should be obtained gradually. Transfer to adult care should be planned in advance, when a patient is feeling well and has a good grasp on their disease management, so there are no gaps between peds and adult care. Parents and families can help the process by allowing teens to speak with their healthcare providers alone, gradually share care responsibilities, encourage them to learn about their disease, and highlight their successes.”
How this works in real time:
Patients can listen and participate in their visits.
Set goals with your healthcare team and work toward them, ask questions and share your opinions.
Healthcare teams can help by providing a non-judgmental space, listening attentively, encouraging young people’s success, engaging patients in decisions, checking for understanding, getting to know patients as people (talk about school, friends, activities), and connecting patients with resources
Dr. Whitney Marie Sunseri, MD, Pediatric Gastroenterologist, Assistant Professor of Pediatrics, UPMC Children’s Hospital of Pittsburgh, says “I always encourage a step-wise approach to transitioning to the adult world. I encourage patients to know their diagnosis, what medications they take and when, to recall their last scopes, and to be able to report all of their symptoms without the assistance of their parents. Then as they get older, and closer to the time of transition, I encourage them to look into different adult doctors. I give recommendations as well.”
Dr. Sunseri advises caregivers and patients to be proactive and look at reviews of doctors and who is in their insurance network. She says the most important visit is the one where patients follow up with her after their first adult visit to make sure it was a good fit and that they are in good hands.
“It’s bittersweet watching these children grow in so many ways and head off into the hands of another provider. Your heart swells with pride and breaks at the same time.”
Resources and Communities of Support
Sneha was diagnosed with Crohn’s at age six. She’s now 23 and still figuring out what her future will look like with IBD. As she grew up, she couldn’t find a community of young adults. This inspired her to create Generation Patient and the Crohn’s and Colitis Young Adults Network.
“Peer support during this transition is critical, so we host seven virtual community meetings. We have hosted over 250 of these peer support meetings over the last two years. I think peer support should be seen as essential during this transition period and it has been the best thing to come out of living with IBD.”
Generation Patient: Instagram–@generationpatient
CCYN: Instagram–@ccyanetwork
Join the American College of Gastroenterology Thursday, May 4, 2022 at Noon and 8 pm ET for a discussion about “Empowering Patients Through the Transition of Care in IBD”. Click here to register.