
Innovation and changes in healthcare are propelled by patients and caregivers speaking up about improvements that can change the way IBD is treated and managed. This week on Lights, Camera, Crohn’s we hear from pediatric gastroenterologists Dr. Michael Dolinger, MD, MBA, Advanced Pediatric Inflammatory Bowel Disease Fellow, Ichan School of Medicine at Mount Sinai and Dr. Mallory Chavannes, MD, MHSc, FRCPC, Pediatric Gastroenterology, Hepatology and Nutrition, Children’s Hospital Los Angeles about the benefits of Intestinal Ultrasound (IUS) becoming a part of routine care, regardless of age.


The goal of IUS is to utilize a non-invasive method to monitor disease activity over time and it’s considered to be more precise than endoscopy in identifying both disease location and characterizing the severity of IBD. The IBD community—both patients and caregivers—can help fuel the adoption of IUS and gain access to receiving more information about their disease activity than ever before.
What is Intestinal Ultrasound (IUS)?
Intestinal Ultrasound (IUS) is an abdominal ultrasound performed during a routine clinic visit without preparation, fasting, or contrast to assess both the colon and the small intestine (terminal ileum most frequently) for the presence of disease activity. Probes are placed over the abdomen and the provider looks at images of the small and large bowel.
“The beauty is that, unlike procedures and other image modalities available to assess disease activity of inflammatory bowel disease, IUS can be performed without any preparation or fasting,” said Dr. Chavannes. “In the setting of active disease, patients can have a thickened appearance of the wall of the bowel (termed increased bowel wall thickness) in both the small intestine and the colon, which can be detected via ultrasound.”
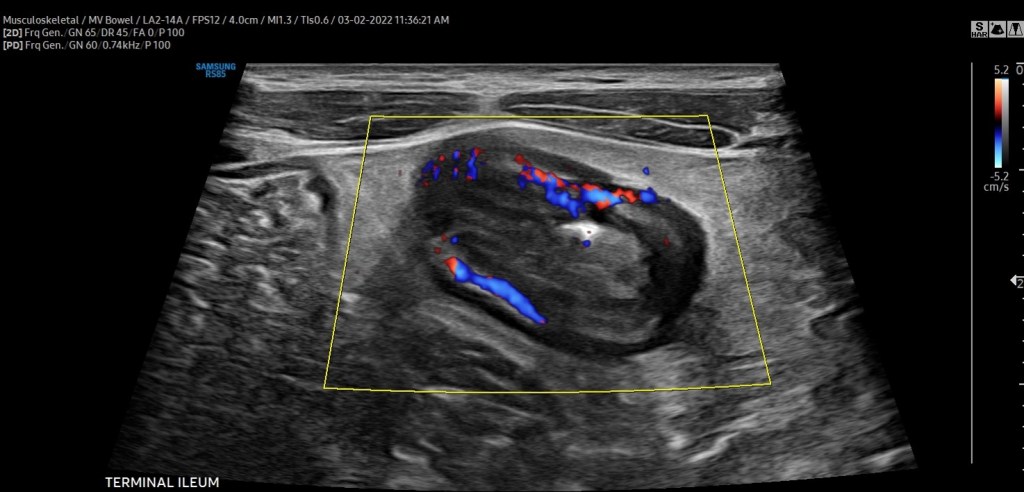
In addition, by using color Doppler, a feature that assesses the velocity of blood flow within and around the bowel wall, gastroenterologists can demonstrate inflammatory activity in the bowel wall. IUS can also detect IBD complications, such as fistulas, abscesses, or strictures (narrowing) of the bowel.
“Our expectation is that, with effective therapies, the aforementioned features of disease activity should improve or even disappear over subsequent clinic visits. If they do not, we now have an objective tool available in the clinic that can assist clinical decisions, such as ordering further investigations or even optimizing or changing therapy. Improvement of bowel wall thickening or decrease in color Doppler signaling is a reassuring sign that treatment is working. Lack of improvement signifies that optimization or changes in therapy should be considered,” explained Dr. Chavannes.
“Intestinal ultrasound is precise, we monitor bowel wall thickness down to the 0.1 mm. We are now able to make informed decisions with patients together, assessing their disease objectively in real-time so we can be aligned with our treatment goals. This reduces misunderstanding and may lead to better treatment adherence and improved outcomes,” said Dr. Dolinger.

Why the delay in the United States?
While IUS isn’t the standard of care across the world, it is used in several Canadian IBD centers and in Europe (Germany, Italy, Norway, the Netherlands, and Australia to name a few). However, there are still many areas of Canada and countries in Europe where this is not used as part of routine IBD care.
“There have been several barriers to adoption in the USA, the biggest of which are reimbursement and the lack of training/expertise. However, that is changing, as there is a tremendous amount of interest from most major academic centers,” said Dr. Dolinger. “Through the International Bowel Ultrasound Group (IBUS) there is now a formal training, while intensive, that can be completed by anyone willing in the USA, which did not exist 5 years ago.”
IUS fits perfectly in the treat-to-target algorithm by adopting a monitoring strategy that helps to prevent flares and bowel damage.
“There is no other test for patients to see their disease dynamically with a gastroenterologist in real-time, which enhances shared understanding and informs decision making like never before. All of this will help break the barrier in the USA and around the rest of the world,” said. Dr. Dolinger.
A study conducted in 2016 explored why IUS is not standard of care in the United States. The
authors surveyed nearly 350 physicians, of which 40% were pediatric gastroenterologists. Although a minority of gastroenterologists were using ultrasound to assess and monitor IBD (either bedside or within the radiology department), over three-quarters expressed interest in using it more.
“The main limitation identified or perceived by gastroenterologists who responded to this survey was a concern for inter-observer variability, a lack of familiarity with ultrasound indications and techniques, and a lack of interest and access to pursuing additional specialized training. In addition, the survey identified a common message that I have received previously from some radiologists; that other modalities are more precise or effective in assessing IBD. All these reasons can hinder interest and implementation,” said Dr. Chavannes.
However, considering the multi-center effort in disseminating training, knowledge, and engagement that has been ongoing in the USA in recent years, Dr. Chavannes is hopeful that IUS will rapidly become the standard of care nationwide.
How Children’s Hospital in LA and Mount Sinai in New York Use the Technology
The Henry and Elaine Kaufman Intestinal Ultrasound Program at Mount Sinai is one of the first in the country to employ the training of gastroenterologists and regular use of intestinal ultrasound for both children and adults routinely in the IBD center for non-invasive disease activity monitoring.
“This would not be possible without the leadership of Dr. Marla Dubinsky, who has worked painstakingly hard to bring this to patients at Mount Sinai, overcoming every barrier to lead the way in the USA. We would like patients everywhere in the USA to be able to have tight control non-invasive monitoring with intestinal ultrasound and in turn, are working with International Bowel Ultrasound Group (IBUS) to host the first hands-on training in the USA at Mount Sinai in the fall. We have faculty from around the country signed up to learn and this will hopefully begin to fuel further adoption,” said Dr. Dolinger.

Intestinal Ultrasound was introduced at Children’s Hospital in LA in the summer of 2020. This was incredibly helpful during the pandemic when access to endoscopy time was difficult, considering cancellations due to active COVID infection and decreased daily procedures to allow for intensive cleaning protocols.
“We integrated using IUS for all patients coming to the pediatric IBD clinic. We have seen an immediate benefit in how we approach patient care and how timely clinical decisions can be made right at the time of the clinical encounter. One example is for patients presenting for a second opinion; these patients usually present with ongoing symptoms of varying degrees, yet incomplete or dated documentation of endoscopy, fecal calprotectin (a stool test helpful in indicating inflammation), and blood work,” said Dr. Chavannes.
During the visit, IUS gives an opportunity to understand the source of the symptoms experienced by patients and the degree of ongoing inflammation. Then, clinical decisions can be made that day, eliminating the need for additional testing. Dr. Chavannes says IUS even helps ease the discussions she has with parents and families.
“Many parents are stunned by the images they see and the changes over time. At the same time, they also notice when there is little difference from one appointment to the next, understanding the reason we are making the changes to the management plan that follows,” said Dr. Chavannes. “IUS has been invaluable for children under 6 years of age. This vulnerable population needs frequent objective reassessments, which is not possible otherwise. Using MR-Enterography would require general anesthesia, and access can be difficult. Similarly, for endoscopy, the prep can be poorly tolerated, and it also requires general anesthesia. IUS is non-invasive, painless, very well tolerated in young children, and available in real-time. Therefore, both parents and children are quite satisfied with their experience with IUS.”
Targeting treatment through IUS
Monitoring symptoms alone is not effective in reaching deep healing of disease in IBD, as many patients feel well despite having ongoing intestinal inflammation. IUS evaluates the inflammation that occurs within the thickness of the bowel wall (transmural inflammation).
“We often find that ultrasound is the only tool that shows continued inflammation when patients are in remission and labs have normalized. Optimizing therapies based on persistent inflammation seen on ultrasound may prevent us from falling into the trap of thinking our medications are working when our patients feel better and thus lead to better outcomes by not missing persistent inflammation that we have continued to miss with traditional monitoring strategies,” said Dr. Dolinger.
Although there are no fully established algorithms for the frequency of monitoring IBD using IUS, the best approach appears to have a baseline IUS at the time of IBD diagnosis or in the context of active symptoms or elevated inflammation markers on blood work (a flare).
“Then, the clinician can understand the features to follow over time. A repeat IUS can be performed at the end of induction treatment to assess how effective the management is. It would represent 6-8 weeks after the treatment was started. Provided that there is a marked improvement, the subsequent evaluations with IUS can be done every 3-6 months unless there are new concerns, with the closer timeline early in the disease course,” explained Dr. Chavannes.

In pediatric patients, this routine ends up matching most routine clinic visits. Therefore, as IUS becomes standard practice, and depending on how a patient is doing, their symptoms, and last assessed disease activity, patients can expect IUS as often as with each clinic visit. This modality would complement blood work and calprotectin stool tests in informing about disease activity and for complications of disease or flares.
What the future holds
Since a few IBD centers in the United States have already implemented regular IUS in their practice and have been disseminating knowledge about this technique, there is growing interest from pediatric providers to join the movement as well.
“Considering the challenges pediatric providers face in access to complementary imaging, operating room time, anesthesia exposure to endoscopy, and even the tolerance drinking contrast for radiology studies, IUS offers a fantastic way to assess disease activity in the pediatric IBD population. I am excited about the number of pediatric centers that have reached out about getting expertise in this field. The key is to promote buy-in from leaders in each institution to get the time and resources required for training and implementation,” said Dr. Chavannes.
Advice for patients and caregivers
It doesn’t hurt to bring up IUS at your next clinic appointment to gauge where your care team stands and if anything is in the works.
“If your provider is unaware of IUS and its benefit, it would be great to talk to them about the International Bowel Ultrasound Group. The curriculum for getting training involves three modules: an introductory module, a 4-week hands-on training at an expert center, and a concluding module and examination part of the European Crohn’s Colitis Congress,” said Dr. Chavannes.
She went on to say that hearing this request from patients may motivate administrators to provide the necessary time clinicians who are interested in getting expertise to implement the tool at their center would need.
Dr. Dolinger believes most major academic IBD centers in the United States will rely on IUS in the next 3-5 years.

“I would like to remind patients to be patient with their providers. Ensuring correct training and standardization is essential for adoption in the USA and this takes time and rigor to be done right and change the monitoring algorithm which has not been done in many years,” said Dr. Dolinger. “I began training in 2019 and it wasn’t until the second half of 2021 that we began using it very routinely for decision making, taking 2 years to become an expert. So, this will happen, but it will take some time.”
Patients and parents are big fans
The safety and efficacy of IUS can’t be matched. It’s also a big-time saver for everyone involved. A bedside ultrasound can be performed in a range of 20 minutes for the first thorough assessment, while an even more focused exam in a known patient can take less than 10 minutes.
“Both parents and children have been quite satisfied after their experience, as children can go back to school after the clinic despite undergoing this examination. Furthermore, the time saved in skipping additional appointments with the radiology department or procedures can be invaluable,” said Dr. Chavannes.
For parents, the imaging provides reassurance when there are improvements or when there are non-specific symptoms, yet the IUS is normal. IUS also bring validation when there are abnormal findings and helps to provide an explanation for why children are feeling a certain way.
“Children appreciate that it does not hurt and takes little time in addition to their clinic visits. In addition, they may not require additional appointments in radiology or endoscopy. Parents who had an opportunity of experiencing an ultrasound often request it afterward as part of their clinic visits. These families are more engaged and participate in shared decision-making. I am pleased and impressed at the engagement that actually “seeing” the disease together brings from families,” said Dr. Chavannes.
While the push is for IUS to be available to all IBD patients, both children and adults, it’s specifically beneficial for the management of pediatrics as it provides the unique opportunity to prevent bowel damage for a person’s entire life and reduce the need for invasive procedures, anesthesia, and sedation. IUS has the potential to alter scoping schedules in the future. While it will not replace the need for colon cancer screening or the assessment of mucosal and histologic healing, IUS can reduce the need for further follow-up scopes once those targets are achieved in between the need for cancer screening.
Additional Resources on Intestinal Ultrasound
Intestinal Ultrasound Ushers in New Era of IBD Treatment
Intestinal ultrasound and management of small bowel Crohn’s disease
Propel A Cure Zoom Interview: Intestinal Ultrasound Discussion with Dr. Michael Dolinger
