There’s a BIG advancement that was just unveiled this week regarding nutrition and IBD. Nutritional Therapy for IBD, a non-profit dedicated to improving the lives and health outcomes of patients with Crohn’s disease and ulcerative colitis through evidence-based adjunctive nutritional therapy, launched their The IBD Nutrition Navigator™ to the public yesterday.
It’s a project that’s been in the works for two years and it’s the first nutritional tool of its kind! This FREE resource allows patients, caregivers, and healthcare professionals to work together to find the best nutritional approach on a personal level. This week on Lights, Camera, Crohn’s we hear from Kim S. Beall, Pharm. D., co-founder of Nutritional Therapy for IBD and Dr. Ashwin N. Ananthakrishnan MD, MPH, FACG, AGAF. These two, in collaboration with dozens of healthcare providers, designers, patients and volunteers, made this resource a reality for the IBD community.
What is the Nutrition Navigator™?
The design was led by Dr. Ananthakrishnan, Harvard graduate, Director of the Crohn’s and Colitis Center at Massachusetts General Hospital and one of the top GI clinicians.
“The IBD Nutrition Navigator™ is a groundbreaking algorithm-based tool designed to assist healthcare providers and patients in determining a personalized approach to using nutritional therapy alongside medication to optimize care,” he says.
“The tool is based on discussions that Dr. Ananthakrishnan has with his patients about nutrition and how it can be used in conjunction with medications and surgery to improve health outcomes. The IBD Nutrition Navigator™ is interactive and walks providers and patients step by step through six questions to assess not only the patient’s individual disease state and goalsbut also their interest in resources for nutritional therapy,” explains Kim.
The tool is designed for healthcare providers and patients to use together in shared decision making. Once completed, the tool recommends the best fit for an evidence based nutritional therapy. These recommendations are geared 100% to the individual based on how they answer the questions. As we all know, there is not a one-size-fits-all answer when it comes to IBD nutrition, and the recommendation is never nutrition vs medication. It’s using nutrition as another tool alongside medication and other therapies.
The inspiration behind the IBD Nutrition Navigator™
Dr. Ananthakrishnan, an esteemed member of Nutritional Therapy for IBD’s medical advisor board, is the inspiration behind the IBD Nutrition Navigator™.
“He discusses nutrition with his patients and uses nutritional therapy alongside medication as part of his regular practice. “What should I eat?” is the most common question for patients after an IBD diagnosis. But because every patient is different, there is not a “one size fits all” answer to that question,” says Kim. “Weeding through the abundance of nutrition information available can be confusing and time-consuming. Dr. Ananthakrishnan felt that we should provide more guidance to healthcare professionals in a simple, evidence-based, clinical manner. And thus, the idea for the IBD Nutrition Navigator™ was born.”
A closer look at nutrition and IBD
Nutritionaltherapies used alongside medication and/or surgery can help manage symptoms, aid healing, and reduce inflammation in IBD patients.
“For a long time, it was thought that diet didn’t even matter when it comes to managing IBD. We now have growing evidence that suggests that food does indeed matter as both a risk factor and a therapeutic option,” says Kim. “Patients struggle, however, with the abundance of nutritional information AND misinformation available. They may want to incorporate nutrition into their IBD management but don’t know where to start.”
Another very prevalent struggle is malnutrition. Patients are often afraid to eat new or certain foods for fear that those foods may cause pain or other symptoms. I know in my nearly 20 years living with Crohn’s disease I was considered malnourished during my initial diagnosis and hospitalization and was watched closely when I was losing weight unintentionally prior to acute flares in the past.
At a baseball game with my brother days before my Crohn’s disease diagnosis in 2005. Little did I know I was malnourished here.
Cool features of the IBD Nutrition Navigator™ to highlight
Years of planning went into the development of the IBD Nutrition Navigator’s clinical algorithm, so the information you will find on the tool is all evidence-based and thoroughly reviewed by medical advisors.
“There are so many thoughtful features of this practical tool. First, while the development of the IBD Nutrition Navigator™ was quite complex, the result is a very straightforward, simple-to-use, interactive questionnaire. Because the tool is so concise, it can be easily used during a regular appointment with a healthcare provider. Two of the six questions gauge the patient’s interest and resources in using nutritional therapy. These questions evaluating the feasibility of and readiness for change are what makes the tool particularly unique and comprehensive. As patients and healthcare providers progress through the IBD Nutrition Navigator™, the suggested nutritional approaches appear on the screen and will adjust in real time. You can see how your answers to the questions may modify the dietary options.” says Kim.
Finally, once the recommended nutritional approach is selected, there are links to extensive resources from Nutritional Therapy with IBD to help you learn about incorporating that approach and even a recipe database with diet-specific dishes.
Tips for taking the information learned and discussing it with a registered dietitian/GI
The IBD Nutrition Navigator™ is designed to facilitate nutrition conversations between patients and healthcare providers, including registered dietitians who play a significant role in this process.
“Before using the tool, patients and healthcare providers must acknowledge that a full clinical assessment—including screening for malnutrition and eating disorders—is the necessary first step. The addition of or changes to nutritional therapy should always be made through shared decision-making between the patient and healthcare provider,” adds Kim.
Patients or caregivers interested in nutritional therapy can print this flyer to take to their provider. The QR code provides a link to Nutritional Therapy for IBD’s website where you will find the IBD Nutrition Navigator™ and many other evidence-based nutritional resources.
Final Thoughts
The IBD Nutrition Navigator™ aims to provide healthcare professionals and patients with a tool that helps us choose the right, individualized nutritional therapy to use alongside medication and/or surgery and optimize care. Once you discover the best nutritional fit, patients can gain confidence in their food choices and ultimately improve their overall health and healing.
I wish when I was diagnosed with Crohn’s in 2005 that I had a tool like this at my fingertips. A dietitian (who was not well-versed on IBD) told me I would never eat raw fruit or vegetables again and it felt like doomsday. I was overwhelmed, and at age 21, days after being given a chronic illness diagnosis, that advice devastated me. Our community is incredibly fortunate to have a tool like this so we can feel more in control and more empowered to make appropriate dietary changes that are personalized to our care and tailored to fit our ever-changing treatment plan. In addition to the IBD Nutrition Navigator™, this volunteer-led organization provides a wealth of information and resources about nutrition and IBD on its website. Click here to learn more.
Everybody copes and has their own unique tips and tricks for undergoing an MRE. I received more than 100 messages with recommendations, there was some overlap and similar advice—but I know our community could benefit from this information and find comfort in it. One of the most challenging aspects of undergoing medical scans and procedures is the mental health aspect—the wait, the wondering. Oftentimes these results do not go in our way and may indicate we are in a serious flare or need surgery. So, while the actual process of drinking contrast and dealing with claustrophobia can be intense, the challenges are often amplified by the dread of finding out the story behind our symptoms. Understand you are not alone in that. I try and just prepare myself for the worst, while hoping for the best. Nobody wants “bad” news, but once you go through the scan and have a better idea of what is going on and then you can go after the flare and get to feeling better.
Here’s the link to Part 1 of “Everything You Need to Know Before an MRE with IBD” in case you missed it.
Advice from the community to ease the MRE experience
“Whether it’s laying there saying prayers (like the Rosary) or focusing on doing something (like walking through Sun salutations or walking through doing something you love to do) that has helped me.”
“As a pediatric patient, my mom was allowed into the MRE room, and she held my foot (the only thing she could reach). Just feeling she was physically there helps my anxiety a lot. Ask for goggles that let you watch a movie are gamechangers because you can’t see anything but the movie, even if you tried!”
“I close my eyes and pretend that I’m lying on a beach and listening to country music. I feel comfortable knowing I can see my feet at the other end, and they can communicate with me. Honestly, I close my eyes and sing my heart out!”
“I listen to the loud banging noises and try to find melodies or patterns. Then, I repeat them back in my head and by the time I’ve done it a few times I’m in a meditative state or the test is over.”
“I try to look up/behind me if I start to feel claustrophobic and you can see outside! I also find it almost relaxing to count the loud clips and beeps. It gets your mind distracted.”
“Picture yourself someone you like; use deep breathing to help soothe your vagus nerve.”
“I know it’s not ideal, but if you are extremely overwhelmed you can always get the test under general anesthesia.”
“I focus on my breathing and imagine I’m in my favorite place.”
“Eye mask with no metal clasps and ear plugs (or music) helps to reduce the sensory overload for me.”
“Before you get in the tube, ask for a towel. Put it over your eyes and do not take it off until they let you out.”
“Deep breaths. Visualize you’re in your favorite place and ask for music. Ask your GI if moving forward Intestinal Ultrasound can replace getting an MRE.”
“I’m normally able to tilt my head up to see out the end of the tube. It helps me so much!”
“Breathing exercises can help.”
“Ask if there is a bariatric imaging machine so you have more room.”
“Slow deep breathing helps me prepare for it and calm down.”
“I close my eyes and envision being on a bench or somewhere hard but with open space for me.”
“Gadolinium has a high allergic reaction. Even if you have not had it before. Communicate with your care team and ask about taking Benadryl.”
“Meditation and Guided Imagery.”
“I take deep breaths and remind myself I am going to be ok. It was quicker than I had expected.”
“Take extra Xanax! I take it for flying and always need more than I think.”
“If they let you pick the music, pick it! Having my music really helps me.”
“See if an Open MRI is available. Otherwise, a big dose of benzos.”
“I’ve been Twilight sedated before, it’s the only way to go!”
“I took Zofran. I also wear MRI safe clothes, so I don’t have to change. I make sure there’s no metal in my bra.”
“Focus on breathing. Close your eyes before being rolled in. Think of something like planning a party or a holiday.”
“I hate it. Hate it. Hate it. Someone told me just don’t open your eyes and it worked.”
“I take Ativan and do breathing exercises.”
“Always ask for a towel or wash cloth to cover your eyes.”
“Keep your eyes closed the whole time. Do not peek. And ask for your favorite music to play.”
“I keep my mind focused on other topics and talk to God.”
“Take anxiety meds! If I have to do this again, I will take something.”
“Let your care team know before you enter the room that you’re claustrophobic.”
“Say Affirmations or imagine being on a vacation on a sunny beach. Anything to divert your mind.”
“Last time my nurse gave me an orange smelling strip that helped so much.”
“I close my eyes and pray or sing songs I like the most in my mind.”
“Slow breathing and counting (in for 4 seconds and out for 4 seconds) or listening to music while in the tube.”
“I always have a Life Saver candy between the contrast drinks.”
“I asked them to bring me back far enough so I could tip my head back and see the ceiling.”
“My sister needs to take 3 anxiety pills for the MRE.”
“Try to find your happy place and go to that in the tube.”
“Have all the good and happy plans run through your mind and ponder them. Daydreams! Mantras!”
“I write stories in my head—like manifestations.”
“Think of a beach on a sunny day.”
“Make lists in your head.”
“Definitely have anxiety meds on hand.”
“Bring a personal blanket. This always helps me.”
“Bring ear plugs in case they don’t have some for you.”
“Use a wedge pillow for your legs (ask for it).”
“Visualize the best vacation, start to finish. Try to remember every detail. Distract your mind!”
“Ask for a heated blanket, it can be chilly in there.”
“When your mind wanders, count. Count breaths in (5) and out (5) and focus on the numbers.”
“Some MRI machines offer a mirror, almost like a periscope. It shows you the outside!”
“Fast paced work out music helps me.”
“I ask before we start that they give me a time update every 15 minutes.”
“It makes me less anxious when I hear the weird and terrible sounds the machine makes if I have NSYNC playing. Have them play music you like that’s also light and funny. (As in 90’s boy bands!)
“My office gives lavender stickers to help calm you to place on the robe. It helped me!”
“I’m SO claustrophobic but I always self-talk “I’m a mother and set the example for my kids.”
“Tell the tech you are nervous. Ask them to check in with you more than they usually would.”
“Remember you can squirm out of the bottom if you need to. Knowing that makes me feel less trapped.”
“Lavender essential oil.”
“I took half a Xanax and enjoyed every second…haha.”
“Take the meds and extra, if possible. I’ve taken up to 4-5 mg of Ativan!”
“They let you choose your radio station or podcast, which can help.”
“I’ve listened to the Hamilton soundtrack. I struggle more with getting the contrast down.”
“Meditation! I always do it before, during, and after.”
“Prepare a playlist or an audiobook and ask if the tech can play it over the speaker.”
“I pray the entire time, so I don’t panic.”
“Try not to investigate too much about the details, it may worry you too much.”
“It’s easier to go in feet first, I don’t know why…but it is.”
“Use the help/panic button and take a break midway through if needed.”
“Be prepared to hold your breath a lot—the tech will guide you.”
“Request a helmet with a mirror. It’ll help you see out of the tube.”
“Try and see how many song lyrics you can remember.”
“Tell them you are nervous. They are more understanding and will talk you through it more.”
“Make sure you give the anxiety meds at least 30 minutes to work their magic.”
“The pills help tremendously, but I also bring an eye mask.”
“Thank you for doing this article, I’ve canceled my MRE twice now out of fear.”
This post is sponsored by Corra. All thoughts and opinions shared are my own.
For as long as Elya Lane can remember she had signs and symptoms of a health condition. It wasn’t until college that she received her official diagnosis of Ehlers Danlos Syndrome and POTS. She says her poor health started to spiral with other comorbidities popping up, the worst of which was chronic UTIs that left her whole body in crippling, burning pain and weak from the antibiotics. Elya’s personal journey with chronic illness inspired her to create the Corra App. This week on Lights, Camera, Crohn’s we learn about how she made her dream a reality and how she hopes to improve peoples’ lives.
The breaking point
“I was constantly plagued with fears of antibiotic resistance, infection complications, or complications from long term antibiotic use. I got to the point where I was so sick that I wrote letters to my kids and my family in case something happened to me. I started tracking all our passwords and making videos for my husband on where our important files were, how different things were stored, all the kids’ data, etc. While I tried to face this potential outcome bravely, I was devastated imagining my kids growing up without a mom,” said Elya.
As she navigated these dark and daunting days, the despair caused her to think about how she could fight back and regain control of her health.
“I started to religiously track my health in journals before transferring to Excel spreadsheets. I was so frustrated by how exhausting and impossible it felt to crunch that much data, so I turned to searching for a symptom track and correlative software to help me. I downloaded and tried every single one I could find – but none met my needs. Some even gave me back faulty data which made me angry. That’s when I decided to create a solution myself,” she explained.
In 2020, after losing access to all her healthcare management tools, and with her health declining rapidly, she decided to create Corra.
The meaning of Corra
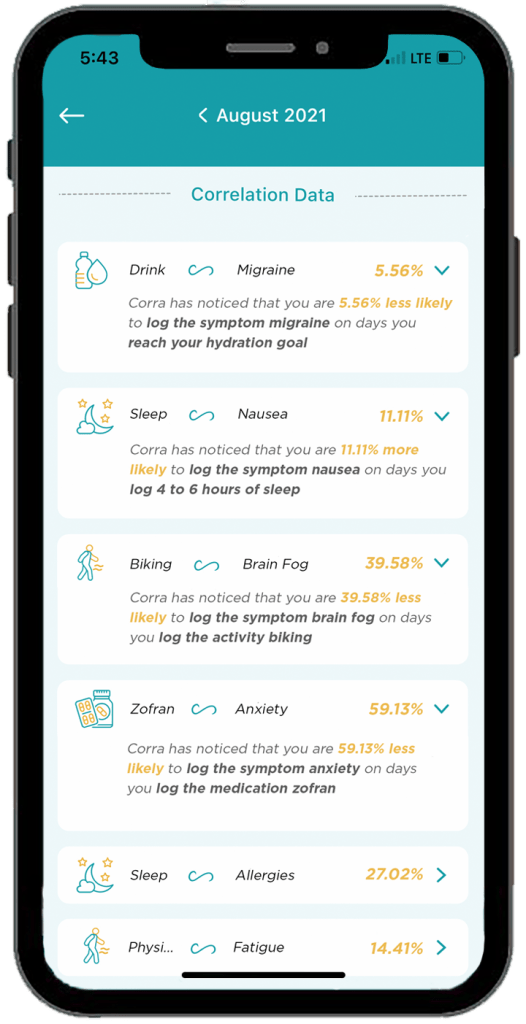
There are quite a few chronic illness apps on the market, some that even attempt to offer correlative insights. Corra is short for correlations. Elya wanted to identify correlations in her health so that she could find her triggers and optimize her lifestyle.
Here’s what sets Corra apart from other chronic illness apps on the market:
The algorithm was custom built by Corra’s chief data scientist, Simeon Wilson, who has a master’s in quantitative economics from UCLA. “We are not aware of any software that exists that compares to what Corra is currently offering with our correlative algorithm.”
Corra was designed by individuals with chronic illness. “Not just me! While the idea and original designs are all mine, we brought on more than 200 beta testers with various chronic illnesses to provide their feedback and help us tailor the app to the needs of the chronic illness community. Even now, we continue to rely on the insights and feedback from the community to enhance and adjust the app. I want Corra to always be designed by and created for our community.”
We correlate with nutrition in an accurate and helpful way. “I believe nutrition plays a massive role in our health so one of our key focuses with our algorithm was to be able to correlate seamlessly with nutrition inputs.”
Corra does not sell user’s data. “We don’t scrape your data from your device or browsing history, we don’t use your data to sell you anything, we don’t share your data with third parties. Your data is yours alone. As an individual with a chronic illness who often feels more like a commodity than a person, making sure people can receive personalized insights into their health without signing away their privacy is incredibly important to me.”
Corra’s bells and whistles to check out
The ability to track health data in one place without having to use five different apps to log information. “My favorite part of Corra is of course the correlations, because getting detailed insights like that about my health is equivalent to having a team of data scientists run extensive tests on my health and provide me reports. It’s life changing to be able to learn about my health overtime and create a custom-built lifestyle that caters to my future.”
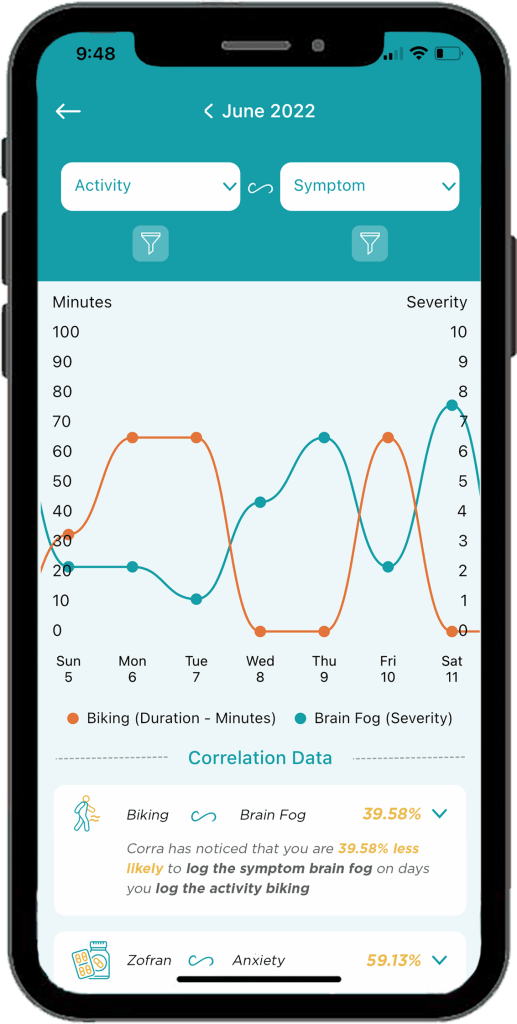
Discovering positive and negative correlations. “You may receive insight that something has x% chance of increasing or decreasing a symptom. I think being able to get data on the things that are helping is just as important as being able to identify triggers.”
The ability to log appointments, download PDFs of your data to share with my doctor, track medications and supplements, track mood and stress levels, etc. “I’m also extremely excited about all the upcoming integrations we have in the works! Soon we will be connected to Fitbit and Apple Health with Garmin, Cronometer, Weather data, and hopefully Oura coming shortly after! Over time we will continue to integrate with as many devices and apps as possible so users can have all their data in one location!”
A promising future
Elya says being able to learn what foods, activities, supplements, and medications help or cause symptoms has enabled her to have a much better understanding of how best to manage her health conditions.
“I’ve been told to go vegan, cut out red meat, don’t eat dairy, sugar, gluten, eat paleo, try a carnivore diet, go vegetarian, and try cutting out leafy greens… what I found with Corra is that I didn’t need to make these drastic nutrition changes, I only needed to cut out some foods in each of those categories. For example, I discovered that I have a high trigger correlation with ground beef. I can eat steak and other red meat, but not ground beef. Similarly, chicken thighs are a trigger for me, but chicken breast is not. Same with gluten, there are some gluten products that are triggering for me, but not all gluten triggers me. Being able to identify exactly which foods to cut out, rather than willy nilly cutting out entire food groups or going on drastic diet changes, has been an absolute game changer.”
Elya has also discovered that cold and flu medications like Mucinex are major triggers for her. This helped her realize why she would get a horrible flare a few days after coming down with a cold or flu.
“Now, I try to manage my colds and flus with other medicine to try to prevent the flare on top of the cold. It’s also important to note that I’m not cured! I have to manage my diet and my activities and my supplements every day. The difference is, I’m no longer throwing shots in the dark, I now have the information I need to manage my condition to the best of my ability.”
Information really is power, and it has given Elya control over her life and reduced her anxiety. Because of Corra, she is now coming up on two years without the need for daily antibiotics. It’s been over 2 years since she visited the emergency room.
“I’ve found that medical providers are far more willing to accept unbiased data from an algorithm than trust my verbal expression of my experience, so in that way Corra becomes my advocate and backs up my statements,” said Elya.
She says her health conditions have caused her to go through depression, isolation, and hopelessness. But her hope for Corra is two-fold.
“First, I believe it can help others identify their triggers and optimize their life so that their conditions can become more manageable, but I also hope that Corra can be a beacon of light for those struggling to see they are not alone. There are so many steps between the start of symptoms and any kind of treatment let alone cure (depending on if your condition is even curable)… and I want to be the one that goes into the trenches and helps people who are suffering the most. So many people in the chronic illness community get forgotten or left with “your test results are normal” when they know there is something wrong with them. I want to create a company that comes alongside them and lifts them up and allows them to have their voices heard.”
Downloading Corra
You can download Corra directly from the App store or the Android playstore. There is a free version as well as premium access. The premium version is $7.99/month or $24.99 if you enroll for a 6-month subscription. Elya is looking for Corra Insiders who are interested in getting free access to the app. By joining the Insiders group, you get a first look at upcoming features. This provides you the opportunity to share feedback on what you do/don’t like or would like to see improved or added in the future. Sign up for the Corra Insiders program here.
When you hear the word “Skyrizi,” you may think people are referring to an up-and-coming rapper or something fun, but in case you didn’t know, Skyrizi (risankizumab-rzaa) is a biologic drug that was approved to treat Crohn’s disease in June 2022. With the medication only being around for IBD less than 13 months, finding patient experiences wasn’t as “easy” as previous articles I have covered on Lights, Camera, Crohn’s about biologics, but I learned a lot writing this and I think you will gain a better understanding of Skyrizi after reading this, too.
Some background on Skyrizi
Skyrizi was previously approved for moderate to severe plaque psoriasis and active psoriatic arthritis. It’s worth noting that Skyrizi is the first treatment for Crohn’s that targets the interleukin-23 (IL-23) protein, which is responsible for inflammation in our bodies. By going after IL-23, Skyrizi helps reduce inflammation that can contribute to Crohn’s symptoms.
When it comes to dosing, patients receive an intravenous (IV) infusion that lasts about an hour at week 0, week 4, and week 8, followed by a self-administered subcutaneous injection with an on-body injector (OBI) at week 12 and every 8 weeks after that. This whole OBI situation is incredibly intriguing to me. I’ve been doing Humira injections for 15 years (!) this week, so I’m used to self-injecting, but knowing technology like the OBI exists gives hope to people who are fearful of needles and having to give themselves a shot. We’ll get into more about the OBI and what fellow patients have to say later in the article.
As far as safety, prior to starting Skyrizi, it’s advised that your GI order lab work that looks at your liver function. If results come back abnormal, this may not be the right drug for you. If you are in the family planning stages, pregnant, or breastfeeding, speak to your doctor. You can also enroll in the ongoing PIANO study, which looks at the safety and efficacy of IBD medications during pregnancy and beyond. Since Skyrizi is so new to the game, research is needed to help pave the way for IBD moms and their children.
Let’s hear from the patient perspective
Prior to starting Skyrizi in February (2023), Stelara failed Stéphane. I’m always careful with how I word this—and I wish all patients and healthcare providers would be conscious of not saying “the patient failed” anything—at the end of the day, it’s the drug that fails us. Stéphane says he didn’t start feeling a response until this month (July)—just before his second OBI (on-body injection). Although his calprotectin started to respond positively in May.
“The good is that I’ve responded and feel better. The bad is that we don’t know how long my response will last or how much it’ll stop inflammation and the formation of strictures. I’ve responded to Remicade, Entyvio, Stelara, but I’ve also developed strictures and had surgeries on all of them. I can hope that Skyrizi won’t continue this dire and disappointing record.”
Megan says before she started Skyrizi she was on the path to an ostomy. Entyvio had failed her, and she was experiencing perianal Crohn’s symptoms that were keeping her from being the mom, wife, and employee she wanted to be.
“My medical team and I decided to start Skyrizi and plan for a temporary ostomy to help my symptoms while we waited for the medication to take effect. After my second Skyrizi infusion, I noticed significant improvement in my symptoms! My bowel movements were more regular, there was a decrease in drainage from my setons, and I had less pain overall. Given my positive response to the medication, we were able to table ostomy surgery. I was extremely relieved and grateful that I had such a quick response to Skyrizi.”
Maha went on Skyrizi after the biologic she was on failed her after six years. As she was reeling from the reality that the biologic that had put her into clinical remission could suddenly not work anymore, she was hesitant and nervous about how to decide the next treatment options.
“After reviewing all of my options with my doctor, I chose Skyrizi based on data and evidence, and also on a gut feeling that this might be the right next step. I’m happy to report that I was right, and in the time that I’ve been on Skyrizi, I’ve achieved a state of remission I could only dream of, with no side effects!”
Elizabeth was in the clinical trial for Skyrizi. She says the biologic “changed her life.” After fighting a Crohn’s flare for seven years, it’s been the only medication that’s wrangled her disease under control.
Kelly started to flare last Fall, because of a loss of response to Remicade (infliximab). Her gastroenterologist suggested Skyrizi as an option that aligned with her drug priorities: namely safety and efficacy.
“The drug has very good data behind it, and she had heard of excellent response in the clinical trials. But it was very new to GIs across the US. It was a gamble, but one that we both thought was worth trying.”
Unfortunately, Kelly dealt with significant problems and delays with her prior authorization and needed to use the AbbVie Bridge Program to get her first infusion dose covered.
“My insurance company used my participation in the Bridge Program as a reason to deny my coverage for the drug. But AbbVie anticipated this issue and has several support programs that cover longer use of the drug and help with deductibles until insurance companies change their policies about drug coverage. I strongly believe that the months of stress and anxiety and daily hours-long phone calls to try to get this drug covered and delivered seriously exacerbated my flare symptoms,” said Kelly.
This cat and mouse game is something far too many of us can relate to. It’s sickening and ridiculous what chronic illness patients have to go through month after month, just to receive medication on time. Kelly was constantly anxious and worried about whether her Skyrizi would be covered.
Kelly tells me her first two infusions were easy and that she had almost zero side effects aside from very mild fatigue, like her normal Crohn’s baseline.
Kelly’s final Skyrizi induction infusion
“My third infusion was a little heavier hitting, like how Remicade infusions felt: a pronounced bit of fatigue, headache and brain fog that lasted less than a day. It was very tolerable. I didn’t have to premedicate before the infusions either, although my doctor had started me on budesonide to try to control the inflammation and keep the flare from getting worse while we waited for the Skyrizi to kick in.”
Cassandra says this is her third biologic and the whole experience in and of itself has been a bit nerve wracking. She lives in Canada and was the first to receive Skyrizi in her city.
“I didn’t love being the first, having the nurses learn on me, not knowing what to expect was difficult as I typically try finding online forums where others share their experiences. So far, I feel ok with it. Skyrizi hasn’t gotten me into remission, but we will see how it goes!”
The OBI (On-Body Injector)
Like anything new, getting used to a new medication and the mode of delivery can have a bit of an adjustment period. You wear the device on your thigh or abdomen for 5 minutes while the medication gets into your skin.
Kelly – “The neat thing about Skyrizi is the Obi, or on-body injector. It’s a brand-new device that is halfway between an infusion and an injection. It’s a small rectangular device with adhesive on the whole back that sticks to your leg. The needle in the device is tiny and I had zero sensation or pain. The button to trigger the needle is large and doesn’t have the same kind of chunky CLICK that the Humira pens do, which was nice and felt less aggressive and intimidating. Because the device infuses the medication into your body over several minutes, it uses an electronic pump. This means you cannot wear your fitness device or Apple watch or have your phone anywhere near it while you’re doing the injection.”
Kelly says she expected to have difficulty with the adhesive since it covered such a large area of skin and was strong. Other than mild discomfort while peeling it off (like taking off a band-aid), her skin didn’t have any other reaction.
Stéphane-“The written instructions for Skyrizi make the self-administering with the on-body injection unnecessarily complicated. I counted 33 warnings of what not to do, something that just generates anxiety. In fact, it’s simple and easy and the Skyrizi video they provide on the website is far more confidence-inspiring and useful.”
Stéphane says it’s helpful to watch the video after reading the instructions. He says the video is good at stripping the process down to essentials and showing that the injection process is in fact easy.
“The front of the thigh is simpler than the stomach because it naturally offers the flat, smooth, easily accessible space you need to place the injector. You clean the small end of the vial, stick it into the injector so it clicks, close injector door, clean area of skin, take the two strips off the back (top first), place it on your thigh and press down the adhesive, then press forcefully on button of injector,” he said.
Jessica made the switch to Skyrizi after being on Stelara. So far, she hasn’t experienced side effects and the medication has kept her Crohn’s in remission.
“The new on-body injector technology is weird and takes some getting used, but overall, it’s painless. It’s just been a little complicated to learn. If there’s a lump on your skin after you take the injector off. She says it goes away. While the needle doesn’t hurt, Jessica feels as the medicine goes into your system you start to feel more pressure.”
So far, Megan has completed two OBIs at home. She says the OBI is extremely easy to use. She’s done Humira, Stelara, Cimzia, and methotrexate in the past and says the OBI for Skyrizi is the easiest and least painful.
“I like to head to a secluded area, so I don’t chance my son trying to wrestle or play and accidentally knock it out of place. (IBD mom hack!) While I still have hard days and I’m not symptom-free, my hard days are much less frequent than before starting Skyrizi!”
Cassandra-“The OBI is amazing. I have been getting IVs monthly/every other month for 9 years, so to not have to get an IV has been wonderful. I have grown to really hate them and have had some bad experiences getting IVs so to not have to face that has made a world of difference. The OBI is so simple, so quick, and relatively painless (though I have felt some slight pinching/stinging). All in all, it’s very simple and I find the mechanism very innovative and cool! I haven’t had any side effects yet, aside from injection site swelling and redness the day of.”
Maha-“The best part is the ease with which I can do my Skyrizi injections via the on-body injector: it’s painless, quick, and honestly I forget that I have to do them until my next injection rolls around.”
Benefits of utilizing the Nurse Ambassador Program Much like other biologics on the market, patients can tap into the free Nurse Ambassadors on hand to help ease the transition to Skyrizi. These nurses provide invaluable guidance and comfort every step of the way. Not only is utilizing these programs beneficial for patients, but also caregivers who may be helping to administer medication.
Kelly-“The device is so new, and the instructions can be long and a little complicated, but AbbVie has a nurse ambassador program that is free for all patients. I cannot recommend the program enough. My nurse ambassador came to my house before I even received the first infusion dose and answered all my hundreds of questions about the expected side effects, the rate of response, and showed me a demonstration with the OBI. It was helpful to get comfortable with the training device. My nurse ambassador also showed up to my house for my first injection and walked me through each step and was excellent at providing support.”
Natalie started Skyrizi infusions in May, 2 infusions down, 1 more to go before she starts with the OBI. She says while she hasn’t experienced huge benefits yet, she’s still hopeful. This is her first biologic and she’s appreciative of how helpful the AbbVie nurse has been through the process.
“I am still pretty new to this myself, but talking with the Skyrizi nurse has helped a great deal, especially getting their co-pay program and just having someone to check in on you.”
Jessica– “AbbVie has an amazing support system, and you can always have a nurse ambassador visit you in person or Facetime you. When I FaceTime the nurse, she guides me through it. Just talking to her while the injector is on for five minutes has made a difference.”
Cassandra-“I live in Canada, so things may be different elsewhere, but Skyrizi is the first biologic where I was sent a “Welcome package” which had a little health/wellness goal setter, appointment tracking sheets, a large needle disposable cartridge for my used injectors, and a mini cooler with reusable ice packs. I was super impressed, and it was fun and cute to receive. I have used the nurse ambassador a few times, especially at the beginning. It’s nice to ask questions or voice concerns with them. Having a nurse ambassador gives me peace of mind.”
Maha-“I really appreciate AbbVie’s commitment to patient education and support through their Skyrizi Hub which provides insurance specialists, nurse ambassadors, and an on-call line to help with any medical or financial concerns! My nurse ambassador walked me through my first injection and has followed up with me regularly to check on my progress both in terms of clinical symptoms and also quality of life!”
Struggling with the “newness” of being a biologic the first year it’s approved for IBD
Kelly ended up flaring badly between her third induction infusions and the fourth dose (her first at home injection). She met with her GI several times, discussing what to do. Since Skyrizi is such a new IBD drug, there really isn’t any extensive anecdotal evidence or patient stories about whether it be worth it to continue the drug, or if she would be considered a “primary non-responder.”
“We struggled with what criteria to use to determine if I just needed to wait longer or if I needed to switch drugs. My GI reached out to the Skyrizi sales rep for their practice and was told not to give up on the drug before 24-26 weeks because clinical trials did show that a non-trivial number of outliers did capture response to the drug later than the expected 8-12 weeks that was seen with most primary responders. At 14 weeks, I could tell that I wasn’t seeing any response to the drug because I was tracking my symptoms, daily bowel movements and pain. It was helpful to have that data to show us in black and white that I wasn’t doing well.”
Looking at the reality of the data and watching her symptoms escalate and her inflammation creep higher and higher despite the steroids and Skyrizi, Kelly and her care team made the decision to discontinue Skyrizi and move to another drug.
“It’s hard to hear from so many medical professionals that a drug with only about a 40% response rate is considered a raving success in the GI community. For me, that’s an enormous number of people who did not respond to this drug. I wish very much I had been one of them, because it’s scary and upsetting when you burn through a drug and cannot go back to it in the future because of possible antibody development.” says Kelly.
Ultimately, the decision to try a medication is a highly personal decision, one that should be made well-informed and jointly with your GI healthcare provider.
Maha says, “My experience with Skyrizi has affirmed that there is hope in all the new therapeutic modalities that are coming out, and that they can offer patients a strong quality of life while delivering treatment as minimally invasive as possible.”
Interested in reading previous Light’s Camera Crohn’s Patient Experience articles about other biologics?
Raise your hand if you’ve ever been blindsided by an IBD flare. My Crohn’s has landed me in the hospital with zero warning on several occasions. The unpredictability of IBD is a huge challenge we all face. But what if a wearable device could signal when our disease course is going off the tracks? What if we had warnings long before we were face to face with our next flare?
An ongoing “Stress in Crohn’s” study out of Mt. Sinai’s IBD Center in New York and The John Radcliffe Infirmary/Oxford University in the United Kingdom has been investigating this since February 2021, with the help of 200 participants. The study wrapped up in June 2022 and was conducted in partnership with 4YouandMe and funded by a grant from The Leona M. and Harry B. Helmsley Charitable Trust to 4YouandMe.
The goal? To empower those with Crohn’s to monitor stress responses and early signs of impending illness worsening in between clinic visits, while providing a means to navigate life and mitigate the consequences stress has on our disease journey. While stress has long been known to somehow affect our IBD, the details of the relationship are poorly understood.
This week on Lights, Camera, Crohn’s we hear from an IBD mom and educator who recently participated in the Stress in Crohn’s study in hopes of taking action to help advance our knowledge of diseases like Crohn’s and ulcerative colitis.
The mission of the Stress in Crohn’s study
Wearables such as smart rings, smart watches, and smart scales, along with our phones, can collect information emanating from us. They can record our physiology and our routines that we are learning to weave together into “clinical symptoms”- such as fatigue, sleep, and stress.
“The main mission of 4YouandMe (nonprofit) is to empower individuals to navigate their own health by using wearables and apps while sharing their own health related data and insights for the benefit of all. This desire was birthed after working at Apple on their Special Projects team and grew out of asking “why can’t the data that emanates from each of us come back and help each person improve their health on a daily basis”,” said Stephen Friend, President 4YouandMe(nonprofit) , Visiting Professor of Connected Medicine, Oxford University.
Tina Aswani-Omprakash, MPH, Wearables Research Coordinator at Mount Sinai’s Susan & Leonard Feinstein IBD Center & Patient Advocate/Founder of the blog ‘Own Your Crohn’s’ says the promise of wearable devices in the prediction of IBD flares and drug response is real and something she’s excited about.
“As we know, IBD can be a progressive disease and it is important to shut down inflammation quickly to prevent complications. The wearable studies at Mount Sinai’s Susan & Leonard Feinstein IBD Center are looking to develop algorithms using measures such as heart rate variability, sleep duration & quality, essentially autonomic/ parasympathetic nervous system fluctuations via data collected through wearable devices. The hope is to help predict IBD flares and showcase drug response utilizing wearable device signatures,” said Tina.
Meet Nicole, Stress in Crohn’s study participant
Nicole Pavlin became a patient at the Mount Sinai IBD Center in New York and received an official diagnosis of Crohn’s disease of the ileum and jejunum in 2021, but her symptoms began more than 16 years prior. At the time Nicole was just beginning her teaching career and she was focused on raising her family. Once Nicole received her IBD diagnosis, she would often search GI research publications to better understand Crohn’s, along with the treatments and procedures available to patients.
“By educating myself about the disease, I’ve been able to communicate more efficiently with my healthcare team and advocate for my needs. The opportunity to participate in IBD research is always exciting to me, especially since the results could potentially help patients in the future,” said Nicole.
Nicole chose to participate in the “Stress in Crohn’s Study” from July 2021 to May 2022, which captured a period of time when her IBD symptoms took a turn for the worse. Nicole had bowel resection surgery that involved the removal of 6 inches of her ileum, including her Meckel’s diverticulum.
Getting recruited for the Stress in Crohn’s study
You may be wondering how Nicole got involved with this study. A Clinical Research Coordinator from the Mt. Sinai IBD Center reached out to Nicole to see if she’d be interested in participating. The researcher told her digital devices were being used to learn the relationship between Crohn’s disease symptoms and stress to try and predict the onset of flares.
“I was given detailed information about the study and instructions on downloading the app. The researchers provided me with an Oura ring, an Empatica EMBRACE wristband, and a Bodyport scale. I completed various surveys and tasks within the Stress Study app each day. Whenever I had a bowel movement, I would note the characteristics of the stool on the Pooply app based on the Bristol stool scale. The Rescue Time app was optional, and I chose not to use that one,” Nicole explained.
Daily points were awarded for wearing the Oura ring and Empatica wristband, using the Bodyport scale, answering survey questions, and completing tasks on the study app. Nicole received extra “boost points” for using the devices multiple days in a row.
“Every two weeks I gained points for completing a video diary and a cognition task. About five times during the study, I completed a Calprotectin stool sample at home through the IBDoc app. I had a support team and check-in calls each month to answer questions about my mental health and medications. There was also a study visit every three months to complete additional surveys about my health and Crohn’s disease.”
By the end of the study, Nicole earned more than 20,000 points for completing these tasks and eventually received 5 stars for being a “Groundbreaking Contributor” to science. She says the point system was a big motivator and a fun challenge. The study lasted 9 months. Nicole was compensated $400, and she got to keep the Oura ring.
Wearables provide a “new voice of objective data”
Up till now, those with chronic diseases have had to use their memory and feelings to convey their diseases. The wearables offer a new voice of objective data for themselves and for their physicians about what precisely occurred.
“In this study of Crohn’s disease, we were more interested in unlocking the link between stress and flares in Crohn’s. This is part of a larger set of feasibility studies to build for individuals a “Stress Load Navigator” for we note a tight connection between not just inflammatory bowel disease, but also diseases as diverse as diabetes, heart attacks, arthritis and even Alzheimer’s,” said Dr. Friend.
Marco Altini, Founder of HRV4Training, advisor at Oura, and Guest Lecturer at VU Amsterdam, says recent advancements in wearable technology are making it possible to move away from the lab and monitor our physiology continuously, in real life, when and where it really matters.
“In the context of many chronic conditions, the ability to monitor our own, individual changes in resting physiology over long periods of time, and in relation to symptoms or other makers, could finally help us better manage our health,” said Marco.Devices such as the Oura ring can monitor accurately resting heart rate and heart rate variability over time. These signals are tightly coupled to our stress response, which is often an important part of the picture when managing our health.
Participating in research as an IBD mom
Since there is a genetic component to IBD, Nicole says she worries that her children could show signs of the disease in the future. She’s been very open with her children about the challenges she’s faced with the disease.
“I want to model resilience for them so they can see how to navigate difficult situations. By participating in research, I want to show them that we have a chance to use these challenges to help others and make a difference in the future.”
Nicole says it’s encouraging that wearable devices could potentially predict the onset of flares, which might offer faster treatment to prevent the escalation of inflammation and disease progression.
The importance of contributing to IBD research
Nicole’s hope is that by sharing her experience, it will inspire others to participate in IBD research and encourage more funding for these types of initiatives.
“Our research contributions as chronic illness patients have so much potential to benefit others in the future. This study was fascinating, and it was truly a pleasure to participate in the research.”
She says by taking the daily surveys and performing the tasks, it made her feel like someone was paying attention to her struggles.
“It gave me an incentive to be strong, thinking that my challenges could be helpful to IBD research!”
Nicole’s final thoughts on wearable devices
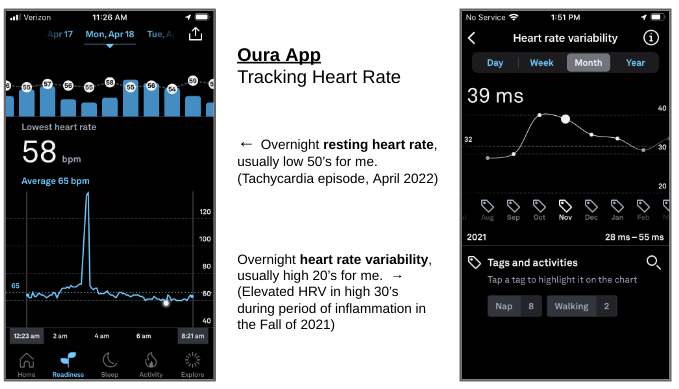
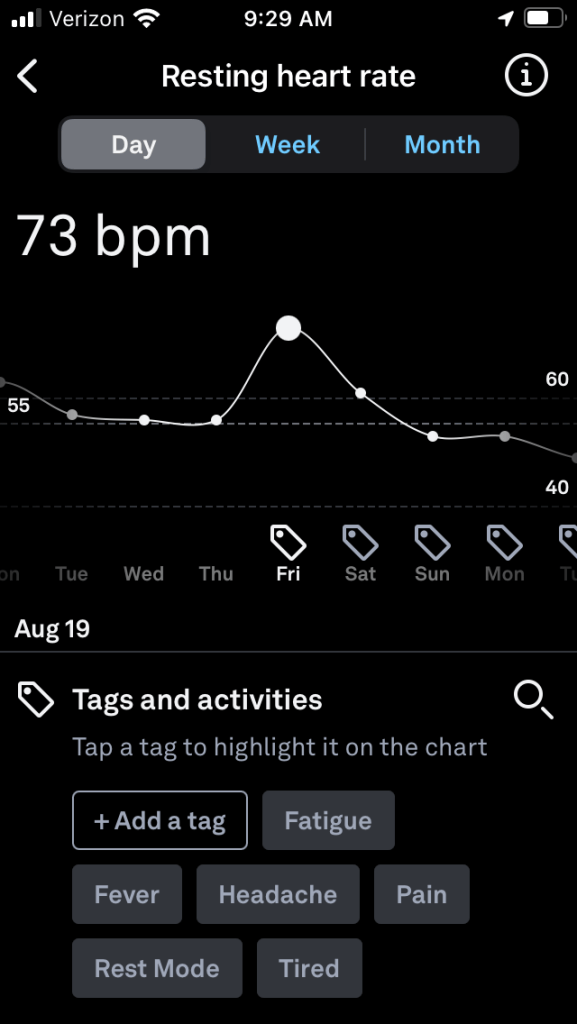
Wearable devices present a great opportunity for patients to monitor their health and provide feedback to healthcare professionals. “Since the study, I’ve continued to wear the Oura ring, and it’s been especially helpful to follow my progress as I rebuild and strengthen my body. Each morning I can check my readiness level to see how my heart has recovered from various activity levels. My sleep analysis has also been helpful for establishing a healthy sleep routine.”
The Oura ring has captured periods of strain on my body, and I can often tell when I’m getting sick with slight elevations in body temperature and resting heart rate. “During my Covid infection, the ring app even showed a fever spike along with elevated heart rate. I’ve also been able to monitor episodes of tachycardia with the help of the Oura ring and a KardiaMobile device, which is a single-lead portable EKG connected to a phone app. In addition, we have a pulse oximeter at home to monitor heart rate and oxygen saturation.”
With so much information to collect on our health, these devices can be overwhelming and anxiety provoking. “During the study, I was constantly monitoring my symptoms which led to a hyperfocus on my disease. Weighing myself each day also contributed to anxiety. Each time my weight dropped a little bit, I got worried and discouraged. The constant focus on weight can also contribute to issues with body image, and I’ve since decided to just weigh myself at medical appointments. For anyone considering wearable devices, it’s very important to keep moderation in mind.”
When we step out into the world, we need navigation tools. The same goes with wearable technologies. Soon, we’ll be able to use the data taken directly from our own bodies, during our day-to-day lives, to follow what is happening and help us to better navigate our own health paths. According to Dr. Friend, last year almost half of American adults were wearing some form of smart watch, and as of Spring 2022 more than 90% of smart watch users state they use health related apps to follow their health.
Interested in becoming a citizen scientist like Nicole? Learn about additional research opportunities:
In the future, Nicole plans to contribute to the Mount Sinai Million Health Discoveries Program which aims to understand how to treat different diseases in patients of all races, ages, and genders. She has also been invited to collaborate with Nutritional Therapy for IBD whose mission is to improve the lives and outcomes of patients with Crohn’s disease and ulcerative colitis through evidence-based nutrition.
Closing thoughts
The information collected from wearables can be a gamechanger for us as patients. Many of us call our doctors or go to the ER based on symptoms, but if we have remote monitoring via such devices, we could perhaps prevent this disease from spiraling. Kudos to Nicole and the many other research participants who are helping to push the needle and change the future of what it means to live with IBD.
“To me, that’s not just hope. That’s the future of managing this disease better and truly owning our Crohn’s or ulcerative colitis,” said Tina.
This article was sponsored by ImYoo. All thoughts and opinions shared are my own.
Precision medicine is a common term we hear when it comes to treating IBD now and into the future. But have you heard about citizen science as it relates to IBD? Citizen science gives everyone a chance to play an active role in research. Whether that’s coming up with research ideas or taking part in the experiments themselves, citizen science makes it possible for you to have a direct impact. A company spun out of Caltech is taking citizen science to a whole new level. ImYoo is debugging the human immune system by using at-home blood collection kits and single RNA sequencing to discover insights about autoimmune diseases.
Tatyana Dobreva and her co-founder, David Brown, worked at NASA prior to switching gears from space to focus on biotech.
“The COVID-19 pandemic accelerated the process and highlighted for us what was missing. Since the pandemic, people are paying more attention to their immune systems. Immunology is still as much a mystery as outer space, so that was the next frontier we wanted to get involved in. We feel that the best way to take on that challenge is by building a database across time, for every individual – that is what can make personalized medicine possible and that is why we’re so focused on making this research accessible.”
Since IBD presents uniquely in each person and changes over time, it’s a rollercoaster journey of highs to lows, flares to remission. With all the twists, turns, and complexities that ulcerative colitis and Crohn’s create for each of us in the patient community, following a roadmap can seem impossible.
“Precision medicine tries to apply scientific tools to take out some of this guesswork. A lot of those tools look at the genetic material you inherited from your parents. We’re adding another tool to that kit by looking at the expression of those genes. For IBD, we want to figure out which genes and cells are acting up during a flare,” said Tatyana.
By answering these key questions, clinicians have told Tatyana that it will help gastroenterologists make more informed decisions when it comes to treating and managing IBD and patients can feel more empowered every step of the way. While making the decision to start a biologic can be overwhelming for patients, precision medicine is a way to have powerful data to support the choice to move forward with that treatment plan.
Tracking the immune system over time
ImYoo’s focus is tracking a person’s immune system over time. Researchers do this by looking at RNA expression. Tatyana shared a fantastic analogy with me. She said that DNA is like the menu you get at a restaurant, RNA is your order, and proteins are your final meal.
“There are a lot of companies that look at your blueprint, or in this case your menu – all the possibilities. Our team at ImYoo looks at your cells’ orders over time. That way we can capture how the different immune cells in your blood are changing,” said Tatyana.
IBD flareups are of specific interest to both clinicians and patients. Even after living with Crohn’s disease for more than 17 years, the unpredictability of the disease is still one of my main struggles. The looming thoughts of a flare are always with you.
“There is not much literature on what happens in the immune system during a flare, and we think there are a lot of powerful biomarkers that could be discovered if IBD patients could track themselves during flares and when they feel “normal.”Our IBD study will ask IBD warriors to sample themselves both during and outside of flares,” said Tatyana.
ImYoo built a solid foundation for studying autoimmunity because researchers were able to build a database of “normal” immune systems.
“Being the first to do this for single-cell data means we can provide a helpful reference to enable more single-cell studies for the future. By having a large database of “healthy” immune systems, we can provide more context as to what having a flare means with respect to dysfunctional immune systems.”
How IBD Patients Can Participate
ImYoo’s IBD study was inspired by conversations researchers had across Reddit and in a Facebook group. Patients in the community offered invaluable insights about what to research.
Emily Harari works as a liaison between the scientific team at ImYoo and the patient community. She says if a person demonstrates interest in participating in the study, a screening process will take place to determine eligibility.
If you qualify, you are enrolled under an ethics-approved study protocol and sent a kit that includes a virtually painless capillary blood self-collection device called TAP II. The device allows you to participate in immune studies in the comfort of your home and send capillary blood samples directly to the ImYoo lab. The TAP II is placed on the upper arm and sticks with the help of a gentle adhesive, it barely penetrates the inner layer of your skin and feels like a suction cup.
“For the IBD study, we ask you to collect a few samples when you’re feeling well and a few samples when you’re flaring. The TAP II device is virtually painless and takes just a couple minutes to use. You’ll mail us the tube of your sample with the packaging we provide. After several weeks we’ll report updates from the lab and several weeks after that we’ll release our study’s findings to the community. Since the community is crowdsourcing the study for us, the least we can do is share what we discover. For example, we may find a new gene or an immune cell marker that helps your doctor better treat your flares,” said Emily.
The Power of Crowdsourcing
The best part about a crowdsourced study is that anyone can make a difference. By visiting the ImYoo crowdsourcing page and selecting “Participate in this Study!” you are making a powerful impact. The more people with IBD who join, the more attention we can attract for crowdfunding.
“If you’re eligible for the IBD study, we’ll reach out after we’ve hit our crowdfunding goal. To help us reach our goal, you can express an interest to participate or pitch in a donation to one of our Champions’ campaigns. There’s a network effect we’re going for, one person tapping into their community can open so many doors.”
If you’ve ever been told your labs or scopes look normal or there’s nothing more to do when you’re suffering through IBD, it’s simply not true. Everyone is on their own health journey and deserves a chance to take control of it.
“That’s why ImYoo is excited to put innovative science in peoples’ hands. This research isn’t possible without the IBD community, which is why we invite IBD Warriors to pitch in however they can – skip a coffee and donate $5, express interest to participate, or simply share to your network,” said Emily.
“Our goal is to empower the IBD community with more powerful tools. One of the biggest questions we hear from IBD folks is, “Am I in remission yet?” You might be feeling fine and think you’re good, meanwhile your immune system could be attacking your colon,” explained Tatyana. “We hope to help people track their immune systems when they are most vulnerable.”
By enabling the IBD community to crowdsource our own studies, the power is in our hands. ImYoo wants to explain their research findings every step of the way and keep people engaged, because it really is a partnership. From this IBD study, the ImYoo team wants to prove that the IBD community can make their own research happen. By studying flares, the hope is that sequencing the state of individual immune cells will uncover predictors and targets for more accessible precision medicine.
Connect with ImYoo, Follow and Participate in the Research
They call themselves “Propellers.” They’re a team of volunteers, made up of IBD patients and caregivers who created a non-profit called Propel a Cure for Crohn’s in 2016. They are laser focused on preventing and curing Crohn’s disease and, on the heels of their first research project funded at Stanford University in the world-renowned lab of Professor Mark Davis, they’re now determined to make a meaningful difference through their Roadmap to a Cure for Crohn’s effort. During this month (September 2022), they’re aiming to raise $50,000 to help get their latest project off the ground and to provide a solid foundation to bring their global team together.
This is a grassroots effort fueled by patient and parent volunteers. Patients and caregivers have an opportunity right now to directly influence a brighter future without Crohn’s! This is a peer-to-peer fundraiser—it’s not just about the monetary donations, but also sharing the message with others far and wide. Not only are international researchers involved, there are people all over the globe participating. In addition to the English-language campaign, there are also Swedish and Portuguese online campaigns running as well.
The Patient/Caregiver Perspective
Ildiko Mehes recalls what it was like when her 9-year-old daughter received her lifechanging Crohn’s disease diagnosis in 2017.
“As a parent, a serious diagnosis like Crohn’s is a huge shock, and it’s absolutely devastating and heartbreaking. Even during periods of remission, we are always on high alert and waiting for the other shoe to drop. At diagnosis, my whole world stopped, literally and figuratively. As irrational as it sounds, as a parent, you wish the rest of the world stopped with you to help you address the crisis. You wish that all of modern medicine rolled up their sleeves and urgently worked together to precisely diagnose the problem and bring her back to long-term health.”
As a caregiver, Ildiko has a unique sense of urgency and determination. She feels we need and can do better for IBD patients.
“When an otherwise healthy child, with no prior medical history, suddenly presents with IBD symptoms during a routine winter virus, you ask yourself “what caused this switch to be flipped?” Not having any answers to the underlying mechanism of disease onset or perpetuation, having a trial-and-error approach to disease management, and being forced to consider serious immunosuppressive medications with modest clinical trial benefits feels unacceptable as a parent. This is what drives me.”
As a pharmaceutical executive with more than 20 years of experience, Ildiko uses that unique skill set to go after complex and difficult goals with Propel a Cure and feels a deep sense of obligation to help our community.
“While there is excellent research ongoing in IBD, it happens in silos. It lacks global coordination and a plan. We don’t yet understand many basic things about Crohn’s. We are all just hoping for a “eureka moment” that hasn’t come over the last 100 years. We are continuously enticed with headlines of a “promising” new pathway or new drug candidate, usually in mice. And then that great idea sits there, with no progress made, a decade or more later. I know we can do better,” she said.
Natalie Muccioli Emery was diagnosed with Crohn’s disease in 2011 and she’s also a Propel a Cure Board member. She started dealing with abdominal issues 26 years ago. Being a veteran patient has provided her with perspective about how far treating and managing IBD has come and how far we still have to go.
“Propel a Cure was the first organization whose mission resonated with me. I appreciate their mission to cure Crohn’s Disease, but I even more appreciate the fact that they have laid out a plan as to what the areas of knowns and remaining unknowns are in their Roadmap to a Cure for Crohn’s project. Complex issues like Crohn’s Disease will take a collaborative and systematic approach to address, and this cause has captured that,” said Natalie.
Not only is Natalie an IBD mom, she’s also an IBD aunt!
“I believe that as an adult with IBD, the way I embody the role of a “Crohn’s Warrior” is not for myself it is for the next generation. I have “been there and done all that” with Crohn’s. But just because I did it with Crohn’s doesn’t mean the next generation should have to. I grow increasingly concerned when I see the rising rates of IBDs like Crohn’s in younger people. I believe the rising rates of Crohn’s should create a sense of urgency and a desire for a better future.”
Putting the puzzle pieces together
The Roadmap to a Cure is an ambitious project but one that is needed to drive real progress toward cures and prevention of IBDs, not just talk about “cures” in some very distant future. Ildiko says the brilliant clinicians and scientists she has gotten to know all tell her that getting to a cure will take a grassroots effort, global collaboration, and involvement of patients and caregivers.
“We at Propel a Cure are deeply committed to doing exactly that. The first step in our project is to systematize what we already know about Crohn’s today. We know a great deal, thanks to research. But when we are talking about complex fields like genetics, epigenetics, immunology, microbiology, epidemiology, multi-omics platforms and artificial intelligence, etc. there is no way any one person or group can know everything. We need a large global group of dedicated and brilliant experts to put all the puzzle pieces we already have on one table so we can begin to then put the pieces together,” she explained.
Grabbing the attention of medical professionals and researchers
Propel a Cure grabbed the attention of Dr. Bram Verstockt, MD, PhD, Department of Gastroenterology and Hepatology, University Hospitals Leuven, on social media.
“I truly like the concept of joined forces across various stakeholders, including patients and caregivers. As clinicians and scientists, we can have ideas about how to move forward based on experiences and interactions with patients on a daily basis. However, the next step really is to involve patients actively in many of these projects, as is currently the case with Propel a Cure,” said Dr. Verstockt.
The “Roadmap to a Cure” aims to bring together expertise across many different fields and niches in IBD.
“Over the past decades, a lot of scientific evidence has been generated in multiple domains of Crohn’s disease, so now it’s time to bring all that evidence together and truly connect the dots. Only by doing so, one might unravel knowns and unknowns and highlight where the remaining key gaps are, and we can define the priorities and strategies of how to fill these gaps to significantly advance the field, to improve the lives of patients with Crohn’s disease,” said Dr. Verstockt.
Where the roadmap can take us
After the initial step of putting together the state of the art, the next step is identifying gaps in our knowledge: what puzzle pieces do we still need? The third step is to develop the plan, or the Research Roadmap, to get from what we know today to developing cures and prevention strategies.
“We truly believe in a future where we can prevent and cure Crohn’s and eliminate so much patient and family suffering,” said Ildiko.
The reason this requires a grassroots effort and all of us patients and caregivers to fund it, is that otherwise the current system largely doesn’t provide incentives for new ideas or cures or global collaborative efforts of this magnitude. A recent paper discusses how the same ideas have been funded for decades, with limited progress and that we urgently need new directions.
Ildiko believes the current research incentive model is broken. “If we want true progress and cures for Crohn’s and other IBDs, we need a new collaborative model among IBD foundations/nonprofits, patients, caregivers, researchers, clinicians, and others. I believe this can become a model for other chronic and immune-mediated diseases.”
Click here to watch a video where Ildiko explains the Roadmap to a Cure project further.
Hopes for the future
“I would really like to see more key opinion leaders be brave about acknowledging the risks and limitations of current therapies, avoid putting lipstick on a pig when discussing some newer drug candidates in trials with lackluster results and the same mechanisms, dispense with biased headlines like “safe and effective” when the data is much more nuanced or unclear, and openness to “outside-the-box” ideas, like microbiome manipulation, including via diet, infectious triggers like Epstein-Barr virus in Multiple Sclerosis, vagus nerve stimulation, Fecal Microbiota Transplant (FMT), hyperbaric oxygen, etc. and also adopt routine monitoring via intestinal ultrasound for many patients,” said Ildiko.
As of now (September 12, 2022)—more than $26,609 has been raised!
“I have been overwhelmed by the response so far, as has the entire Propel team. People are really connecting with our mission. We are getting donations from so many states and countries! We have received more messages of profound thanks and hope than I can recount. This fuels us so much,” said Ildiko.
Natalie feels a wide range of emotions each time she sees a donation come in or the campaign shared across social media.
“I go from feeling hopeful, to introspective, to sad. I truly wish we did not have to do this campaign and that in 2022 we knew what the underlying cause(s) of Crohn’s are, and that safe, effective, reliable treatments were available for all Crohn’s patients. But here we are. Crohn’s is still very much part of the lives of patients and caregivers, and we need to take action to change that. I am so grateful for the outpouring of support we have received so far, but there is more work to be done!”
Propel a Cure has virtually no overhead fees or salaries, so every single dollar donated to Roadmap for a Cure goes to research.
“We are all volunteers who work out of our homes. The donations will be put towards collaborative research teams worldwide. Each team will lead a contributing area to the development of Crohn’s Disease (environment, microbiome, immune system etc.) and highlight where the gaps in knowledge remain,” said Natalie.
“The ultimate dream obviously would be to cure and if not, to significantly improve the quality of life for millions of patients worldwide,” said Dr. Verstockt.
Click here to donate to this incredible cause or to join their team.
This blog was sponsored by Mahana Therapeutics. All thoughts and opinions shared are my own.
Did you know that two thirds of people with inflammatory bowel disease (IBD) also meet the criteria for a functional GI disorder? Dr. Aline Charabaty, Dr. John Damianos, and Dr. Katie Dunleavy recently presented a paper at the 2022 Guild Conference addressing the substantial overlap between Crohn’s and ulcerative colitis and the gut-brain interaction. You may wonder what constitutes a functional GI disorder, irritable bowel syndrome (IBS) is the most common.
“What we know is that up to 30-40% of patients with IBD in remission (absence of gut inflammation) continue to have GI symptoms such as abdominal pain, bloating, diarrhea, constipation, and fecal urgency, due to disorders of gut-brain interaction (DGBIs, also known as functional gastrointestinal disorders),” explained Dr. Aline Charabaty, director of the IBD Center at Sibley Memorial Hospital.
As someone who was diagnosed with Crohn’s disease more than 17 years ago, I’ve been told by multiple gastroenterologists that I have IBS as well. At one point I was told, “you have a touch of IBS” …whatever that’s supposed to mean. I know I am not alone in believing I have both IBD and IBS, especially since having 18 inches of my small intestine removed for bowel resection surgery in 2015.
Dr. Charabaty says this is the case for many patients because of the following:
Structural damage to the gut caused by IBD. Crohn’s disease can lead to small bowel stricture, which can cause cramps and constipation (by blocking or slowing down the stool flow); Long standing UC can create a “lead pipe colon” (where the colon loses its normal twists and turns that typically slow the stool flow down and become like a straight tube which makes the stool “fall” straight down), which can cause diarrhea and urgency. Resection of part of the small bowel and colon decreases the surface of the bowel that can absorb the water and solidify stools, which leads to loose stool. Finally change in bowel anatomy from stricture or resection, abdominal adhesions from prior inflammation, abscess, or surgery, can lead to small bowel bacterial overgrowth (SIBO) which can cause bloating, pain, diarrhea, or constipation.
People living with IBD can become intolerant to certain foods or modify their diet. This can lead to change in gut flora that affect gut functioning and lead to GI symptoms.
Recurrent flares or previous severe inflammation can lead to change in the gut sensation. Visceral hypersensitivity, gut motility, gut microbiome, intestinal permeability, and how someone perceives and tolerates all the sensations (pain, discomfort) that come from the gut.
IBD affects people’s emotional and mental health and is associated with a higher incidence of depression and anxiety. We know that depression and anxiety can affect the gut functioning and lead to IBS symptoms.
“All these changes are similar to what we see in people living with IBS and can cause IBS and IBS symptoms in people living with IBD. Sometimes the way I explain it to patients with IBD, is that IBS is like the PTSD of the gut. The gut has been inflamed, traumatized, manipulated, changed from prior flare and now it can’t go back to functioning properly, even if it’s healed and it looks normal,” said Dr. Charabaty.
This is where Mahana IBS comes in. The main mission? To empower people with chronic conditions to lead fuller lives through digital therapeutics. That’s why they debuted their new prescription digital therapeutic app, Mahana IBS, in the fall of 2021. Their wish is to destigmatize IBS and bring hope and meaningful solutions to patients like you and me.
Steven Basta is the CEO of Mahana Therapeutics. He says the app is safe, FDA-cleared, and has been clinically proven in the world’s largest trial of its kind to reduce IBS symptom severity.
“Cognitive Behavioral Therapy (CBT) has long been recommended in clinical guidelines as a safe and effective treatment for IBS. Access to traditional CBT with a therapist has been a huge challenge due to the limited number of IBS-trained therapists (less than 300 in the US). Now patients can access CBT and learn the skills it provides to help a patient manage their disease by using Mahana IBS on their smartphone, with great results: 3 out of 4 patients find relief and results for most patients are lasting. Mahana users can complete the program in 90 days or less at their own pace with daily lessons on their phone to create a healthy brain-gut connection and live life more fully.”
Both IBD and IBS negatively impact our quality of life. Our mental health, our psychosocial health, and our financial health (increased health care utilization, missing days of work, medications to treat symptoms).
“Beyond treating the inflammation of IBD, and preventing IBD-associated complications, it is important to recognize and treat IBS when it is present, so people can recover and optimize their quality of life. CBT is an effective therapy for IBS and reduces or eliminates symptoms of abdominal pain, diarrhea, constipation, and bloating,” said Dr. Charabaty.
Unfortunately, access to a therapist who can provide gut-directed CBT can be limited: lack of therapists trained in CBT in someone’s geographical area, limited time availability (many therapists are not taking new patients, or have long waits to see someone; or from an IBD patients’ standpoint—lack of “extra” health care time available, when we often juggle many health appointments), deal with lack of insurance coverage, additional costs related to taking time off work and the expenses related to travel and participate in CBT sessions. Which makes the app even more useful and beneficial for the patient community.
Bringing up digital therapy to your GI provider
Digital therapy is new, and Mahana Therapeutics is working hard to spread awareness in the clinical and patient community to ensure everyone who could benefit, has access, and knows about Mahana IBS.
“It’s important for patients living with IBD to ask their doctor whether Mahana IBS is suitable for them and discuss how it can work with their treatment plan,” said Steve.
As a gastroenterologist who specializes in IBD, Dr. Charabaty says, “Having an FDA-cleared prescription app that provides CBT right at the patient’s fingertips is pure gold! Easy and effective access to CBT at a time that is convenient for the patient, in the privacy of their home, without the added extra time and cost burden of a visit to a clinician. I believe that with this technology/app, which removes many barriers to accessing therapy for IBS, that many more people living with IBS (whether they have IBD or not) will benefit from what CBT has to offer and will be able to improve their symptoms and regain their quality of life.”
Patients who are in IBD remission experiencing IBS Symptoms may want to ask:
“If my IBD is in remission and my symptoms are IBS related, could a digital therapy treatment such as Mahana IBS gut-directed CBT be suitable for me?”
GIs who want to understand more about the clinical evidence and indications for use for Mahana IBS can head this website to check out the medical provider welcome pack which contains all the clinical information they need to get started and to prescribe Mahana IBS.
While the app is a prescription, patients can also download the app on their own and show their gastroenterologist in clinic. But to gain access to the full program, patients need to get a prescription to unlock the benefits.
How the app is tailored to each patient
People experience IBS differently which is why Mahana IBS provides a personalized approach, regardless of type of IBS. In the early sessions of the app, patients create an IBS symptoms profile, take an IBS Symptom Severity Score assessment, and create their personalized model.
“This means people get to identify and capture their own symptoms and associated thoughts, behaviors and actions that arise as a result of these. As patients progress through the app and unlock tools and content, exercises are provided that are tailored to people’s individual IBS symptoms. Progress is recorded through the IBS Symptoms Severity Score at the beginning, the middle, and at the end of the program to measure results,” explained Steven.
Reframing thought process to reduce IBS symptoms
We can all relate to how feeling anxious can leave our ‘stomach in knots’ but in IBS there is a disorder of the brain-gut communication which causes and perpetuates symptoms. For example, our guts can release hormones that change our mood, and the brain in turn sends a signal to our guts to change our bowel functions which then sends more signals to the brain.
“Patients may develop habits or use ‘coping’ techniques that perpetuate the vicious cycle of brain-gut miscommunication without knowing it. The Mahana IBS app uses a gut-directed CBT program that was researched and developed over several decades. It is designed so you can understand your personalized patterns and then learn skills to help support a healthier brain-gut interaction. The program delivers a combination of education and exercises so that patients identify and reframe thoughts, feelings, and actions related to IBS. Through the Mahana IBS program, patients can gain tools and habits for managing symptoms long-term,” said Steven.
Along with learning to reframe our thoughts, the app also features visceral relaxation exercises like diaphragmatic breathing or belly breathing, which can reduce visceral pain and improve GI function. Mahana IBS has easy to follow animations to help patients learn and practice these techniques.
While Mahana IBS is a treatment program designed to be completed in 90 days or less with lasting results, Steve tells me some patients may experience relief from their functional GI disorder within a matter of weeks.
“Patients go at their own pace, so they may complete the program more quickly. Once the 90 days have elapsed, patients can still access their personal data (for example goal setting, IBS-SSS score or their personal IBS Model). Patients can return to the app at any time to find support in any of the lessons, tools, and exercises they have completed.”
Accessing Mahana IBS
Mahana is committed to affordable access. Some patients may be reimbursed by insurance. For those patients who are not covered by insurance, there is a subsidized program to ensure patients will pay no more than $90 out of pocket for prescription cost. That’s less than a single session with a therapist ($120/session) for the complete 10-session program.
Steven says it’s incredibly rewarding and a huge privilege to lead the Mahana team transforming access to treatments like this through digital therapy.
“As CEO of Mahana Therapeutics I am inspired by so many amazing patients with IBS. One patient who had struggled for years with IBS symptoms that made her feel truly hopeless expressed that Mahana IBS changed her life. With the lessons and skills she learned, she no longer avoids the food she loves, and the way she thinks about IBS has altered so completely, it no longer limits her life. Our team’s mission is to make this story a reality for millions of IBS patients.”
Mahana IBS is available for download directly from the Apple App store and Google Play store—and the first session is free to try! To unlock all the specific features and benefits, you’ll want to get a prescription from your GI. Once you’ve been prescribed the app by your doctor, you will get a message from Blink Pharmacy with instructions to get started.
This blog article is sponsored by Portal Instruments. All opinions and experiences shared are my own.
I’ll always remember how I felt the moment I was told I needed to go on a biologic drug to try and manage and control my Crohn’s disease. It was Fourth of July weekend 2008. My gastroenterologist walked into my hospital room and told me it was time to “break out the big guns,” meaning starting to get medication through an infusion or through a self-injection. I was a morning news anchor at the time in Wisconsin, three years into my patient journey. I knew without a doubt, for privacy reasons, and keeping my chronic health issue under the radar, that doing an injection in the comfort of my apartment was the best choice. As I watched the fireworks reflect off the hospital room window with my mom, tears flowed down my face. I didn’t know how on God’s green Earth I was ever going to be able to give myself an injection for the rest of my life.
I was never a huge fan of needles prior to my diagnosis. Once you have Inflammatory Bowel Disease, needles unfortunately are all part of it. While we may get desensitized, patients would give anything to be able to treat their disease without needles. When I started on my biologic, my mom and I went to my gastroenterologist office and a nurse told me I needed to do four, painful injections in my thighs because at the time I didn’t have enough fat on my stomach. I was shaking like a leaf. I had no idea what to expect, I was about to inflict pain on myself, the injector felt so foreign in my sweaty palms, and I was scared about not only how much it was going to hurt, but also the long-term side effects the medication could cause to my body.
I did the first injection and it felt like liquid fire burning through my skin. I couldn’t believe I had to sit there and do three more, back…to back…to back. The experience was traumatizing. When I finally did all four, my mom and I walked into the hallway and I embraced her, crying because of my reality, and knowing that in two weeks I would need to inject two more needles into my thighs for the final loading dose. Since July 2008, I’ve done a self-injection every other Monday and for a short time weekly, while I was flaring. That’s more than 2,600 shots.
Dreading “shot day”
The first few years I would absolutely dread my “shot day” and deal with the looming dread each week. Early on I would get emotional during the process and feel bad for myself. I was only 25 years old. It made me feel like I was a sickly person. My peers couldn’t relate. It was isolating and overwhelming. Every time I open my fridge, the box of injections is staring back at me as a constant reminder of what’s to come.
Doing my injections as an IBD mom
Fast forward to present day, I’m now a 38-year-old mom of three. Luckily, the formula for the medication was changed in 2018, making the drug virtually “pain-free”, but there are times I still feel the needle. Even though I have my medication process down to a science, I still wish I didn’t have to do it and I usually wait until Monday nights to do it. The timing is moreso out of habit, because when I was a morning news anchor there was no way I was going to deal with an injection at 2 a.m. I started a tradition of doing my injection while watching the Bachelor/Bachelorette, and that’s carried over now that I have three young children, often waiting until after their bedtimes. Each time after I’m done with my shot, I text my mom to let her know how it went. She’s a nurse and has been my greatest support with my IBD since the day I was diagnosed.
Sometimes my 5-year-old and 3-year-old watch me do my injection and each time they are intrigued. I’m sure my 11-month-old will be the same once he starts to gain an understanding of what I’m doing. It makes me sad that they often witness me doing my injection, but they are also my greatest motivation to be strong and smile through it. Watching me doing injections has made my kids incredibly brave at the pediatrician when it’s time for them to get their immunizations. Because I have little ones, I have to be mindful of disposing of my medication properly and keeping the Sharps disposal container out of harm’s way. We keep Sharps Containers up high in a cubby hole in our laundry room and I dispose of the injector pen immediately.
As an IBD mom, my greatest fear is passing along my Crohn’s to my children. While the risk is low, it’s there. I hope and pray my children won’t ever need to receive a biologic medication whether it’s through self-injection or infusion. For me, there’s no end in sight, I’m expected to be on my medication (if it remains therapeutic) for the rest of my life. Thinking of my babies having to deal with needles and being forced to inflict pain on them would be difficult for me and only add to the guilt.
The future holds so much promise when it comes to drug delivery without a needle. My hope is that in the years to come, other people won’t have to succumb to the same anxiety, pain, and worry I’ve had to deal with for more than a decade.
Innovation and changes in healthcare are propelled by patients and caregivers speaking up about improvements that can change the way IBD is treated and managed. This week on Lights, Camera, Crohn’s we hear from pediatric gastroenterologists Dr. Michael Dolinger, MD, MBA, Advanced Pediatric Inflammatory Bowel Disease Fellow, Ichan School of Medicine at Mount Sinai and Dr. Mallory Chavannes, MD, MHSc, FRCPC, Pediatric Gastroenterology, Hepatology and Nutrition, Children’s Hospital Los Angeles about the benefits of Intestinal Ultrasound (IUS) becoming a part of routine care, regardless of age.
The goal of IUS is to utilize a non-invasive method to monitor disease activity over time and it’s considered to be more precise than endoscopy in identifying both disease location and characterizing the severity of IBD. The IBD community—both patients and caregivers—can help fuel the adoption of IUS and gain access to receiving more information about their disease activity than ever before.
What is Intestinal Ultrasound (IUS)?
Intestinal Ultrasound (IUS) is an abdominal ultrasound performed during a routine clinic visit without preparation, fasting, or contrast to assess both the colon and the small intestine (terminal ileum most frequently) for the presence of disease activity. Probes are placed over the abdomen and the provider looks at images of the small and large bowel.
“The beauty is that, unlike procedures and other image modalities available to assess disease activity of inflammatory bowel disease, IUS can be performed without any preparation or fasting,” said Dr. Chavannes. “In the setting of active disease, patients can have a thickened appearance of the wall of the bowel (termed increased bowel wall thickness) in both the small intestine and the colon, which can be detected via ultrasound.”
In addition, by using color Doppler, a feature that assesses the velocity of blood flow within and around the bowel wall, gastroenterologists can demonstrate inflammatory activity in the bowel wall. IUS can also detect IBD complications, such as fistulas, abscesses, or strictures (narrowing) of the bowel.
“Our expectation is that, with effective therapies, the aforementioned features of disease activity should improve or even disappear over subsequent clinic visits. If they do not, we now have an objective tool available in the clinic that can assist clinical decisions, such as ordering further investigations or even optimizing or changing therapy. Improvement of bowel wall thickening or decrease in color Doppler signaling is a reassuring sign that treatment is working. Lack of improvement signifies that optimization or changes in therapy should be considered,” explained Dr. Chavannes.
“Intestinal ultrasound is precise, we monitor bowel wall thickness down to the 0.1 mm. We are now able to make informed decisions with patients together, assessing their disease objectively in real-time so we can be aligned with our treatment goals. This reduces misunderstanding and may lead to better treatment adherence and improved outcomes,” said Dr. Dolinger.
Why the delay in the United States?
While IUS isn’t the standard of care across the world, it is used in several Canadian IBD centers and in Europe (Germany, Italy, Norway, the Netherlands, and Australia to name a few). However, there are still many areas of Canada and countries in Europe where this is not used as part of routine IBD care.
“There have been several barriers to adoption in the USA, the biggest of which are reimbursement and the lack of training/expertise. However, that is changing, as there is a tremendous amount of interest from most major academic centers,” said Dr. Dolinger. “Through the International Bowel Ultrasound Group (IBUS) there is now a formal training, while intensive, that can be completed by anyone willing in the USA, which did not exist 5 years ago.”
IUS fits perfectly in the treat-to-target algorithm by adopting a monitoring strategy that helps to prevent flares and bowel damage.
“There is no other test for patients to see their disease dynamically with a gastroenterologist in real-time, which enhances shared understanding and informs decision making like never before. All of this will help break the barrier in the USA and around the rest of the world,” said. Dr. Dolinger.
A study conducted in 2016 explored why IUS is not standard of care in the United States. The
authors surveyed nearly 350 physicians, of which 40% were pediatric gastroenterologists. Although a minority of gastroenterologists were using ultrasound to assess and monitor IBD (either bedside or within the radiology department), over three-quarters expressed interest in using it more.
“The main limitation identified or perceived by gastroenterologists who responded to this survey was a concern for inter-observer variability, a lack of familiarity with ultrasound indications and techniques, and a lack of interest and access to pursuing additional specialized training. In addition, the survey identified a common message that I have received previously from some radiologists; that other modalities are more precise or effective in assessing IBD. All these reasons can hinder interest and implementation,” said Dr. Chavannes.
However, considering the multi-center effort in disseminating training, knowledge, and engagement that has been ongoing in the USA in recent years, Dr. Chavannes is hopeful that IUS will rapidly become the standard of care nationwide.
How Children’s Hospital in LA and Mount Sinai in New York Use the Technology
The Henry and Elaine Kaufman Intestinal Ultrasound Program at Mount Sinai is one of the first in the country to employ the training of gastroenterologists and regular use of intestinal ultrasound for both children and adults routinely in the IBD center for non-invasive disease activity monitoring.
“This would not be possible without the leadership of Dr. Marla Dubinsky, who has worked painstakingly hard to bring this to patients at Mount Sinai, overcoming every barrier to lead the way in the USA. We would like patients everywhere in the USA to be able to have tight control non-invasive monitoring with intestinal ultrasound and in turn, are working with International Bowel Ultrasound Group (IBUS) to host the first hands-on training in the USA at Mount Sinai in the fall. We have faculty from around the country signed up to learn and this will hopefully begin to fuel further adoption,” said Dr. Dolinger.
Intestinal Ultrasound was introduced at Children’s Hospital in LA in the summer of 2020. This was incredibly helpful during the pandemic when access to endoscopy time was difficult, considering cancellations due to active COVID infection and decreased daily procedures to allow for intensive cleaning protocols.
“We integrated using IUS for all patients coming to the pediatric IBD clinic. We have seen an immediate benefit in how we approach patient care and how timely clinical decisions can be made right at the time of the clinical encounter. One example is for patients presenting for a second opinion; these patients usually present with ongoing symptoms of varying degrees, yet incomplete or dated documentation of endoscopy, fecal calprotectin (a stool test helpful in indicating inflammation), and blood work,” said Dr. Chavannes.
During the visit, IUS gives an opportunity to understand the source of the symptoms experienced by patients and the degree of ongoing inflammation. Then, clinical decisions can be made that day, eliminating the need for additional testing. Dr. Chavannes says IUS even helps ease the discussions she has with parents and families.
“Many parents are stunned by the images they see and the changes over time. At the same time, they also notice when there is little difference from one appointment to the next, understanding the reason we are making the changes to the management plan that follows,” said Dr. Chavannes. “IUS has been invaluable for children under 6 years of age. This vulnerable population needs frequent objective reassessments, which is not possible otherwise. Using MR-Enterography would require general anesthesia, and access can be difficult. Similarly, for endoscopy, the prep can be poorly tolerated, and it also requires general anesthesia. IUS is non-invasive, painless, very well tolerated in young children, and available in real-time. Therefore, both parents and children are quite satisfied with their experience with IUS.”
Targeting treatment through IUS
Monitoring symptoms alone is not effective in reaching deep healing of disease in IBD, as many patients feel well despite having ongoing intestinal inflammation. IUS evaluates the inflammation that occurs within the thickness of the bowel wall (transmural inflammation).
“We often find that ultrasound is the only tool that shows continued inflammation when patients are in remission and labs have normalized. Optimizing therapies based on persistent inflammation seen on ultrasound may prevent us from falling into the trap of thinking our medications are working when our patients feel better and thus lead to better outcomes by not missing persistent inflammation that we have continued to miss with traditional monitoring strategies,” said Dr. Dolinger.
Although there are no fully established algorithms for the frequency of monitoring IBD using IUS, the best approach appears to have a baseline IUS at the time of IBD diagnosis or in the context of active symptoms or elevated inflammation markers on blood work (a flare).
“Then, the clinician can understand the features to follow over time. A repeat IUS can be performed at the end of induction treatment to assess how effective the management is. It would represent 6-8 weeks after the treatment was started. Provided that there is a marked improvement, the subsequent evaluations with IUS can be done every 3-6 months unless there are new concerns, with the closer timeline early in the disease course,” explained Dr. Chavannes.
In pediatric patients, this routine ends up matching most routine clinic visits. Therefore, as IUS becomes standard practice, and depending on how a patient is doing, their symptoms, and last assessed disease activity, patients can expect IUS as often as with each clinic visit. This modality would complement blood work and calprotectin stool tests in informing about disease activity and for complications of disease or flares.
What the future holds
Since a few IBD centers in the United States have already implemented regular IUS in their practice and have been disseminating knowledge about this technique, there is growing interest from pediatric providers to join the movement as well.
“Considering the challenges pediatric providers face in access to complementary imaging, operating room time, anesthesia exposure to endoscopy, and even the tolerance drinking contrast for radiology studies, IUS offers a fantastic way to assess disease activity in the pediatric IBD population. I am excited about the number of pediatric centers that have reached out about getting expertise in this field. The key is to promote buy-in from leaders in each institution to get the time and resources required for training and implementation,” said Dr. Chavannes.
Advice for patients and caregivers
It doesn’t hurt to bring up IUS at your next clinic appointment to gauge where your care team stands and if anything is in the works.
“If your provider is unaware of IUS and its benefit, it would be great to talk to them about the International Bowel Ultrasound Group. The curriculum for getting training involves three modules: an introductory module, a 4-week hands-on training at an expert center, and a concluding module and examination part of the European Crohn’s Colitis Congress,” said Dr. Chavannes.
She went on to say that hearing this request from patients may motivate administrators to provide the necessary time clinicians who are interested in getting expertise to implement the tool at their center would need.
Dr. Dolinger believes most major academic IBD centers in the United States will rely on IUS in the next 3-5 years.
“I would like to remind patients to be patient with their providers. Ensuring correct training and standardization is essential for adoption in the USA and this takes time and rigor to be done right and change the monitoring algorithm which has not been done in many years,” said Dr. Dolinger. “I began training in 2019 and it wasn’t until the second half of 2021 that we began using it very routinely for decision making, taking 2 years to become an expert. So, this will happen, but it will take some time.”
Patients and parents are big fans
The safety and efficacy of IUS can’t be matched. It’s also a big-time saver for everyone involved. A bedside ultrasound can be performed in a range of 20 minutes for the first thorough assessment, while an even more focused exam in a known patient can take less than 10 minutes.
“Both parents and children have been quite satisfied after their experience, as children can go back to school after the clinic despite undergoing this examination. Furthermore, the time saved in skipping additional appointments with the radiology department or procedures can be invaluable,” said Dr. Chavannes.
For parents, the imaging provides reassurance when there are improvements or when there are non-specific symptoms, yet the IUS is normal. IUS also bring validation when there are abnormal findings and helps to provide an explanation for why children are feeling a certain way.
“Children appreciate that it does not hurt and takes little time in addition to their clinic visits. In addition, they may not require additional appointments in radiology or endoscopy. Parents who had an opportunity of experiencing an ultrasound often request it afterward as part of their clinic visits. These families are more engaged and participate in shared decision-making. I am pleased and impressed at the engagement that actually “seeing” the disease together brings from families,” said Dr. Chavannes.
While the push is for IUS to be available to all IBD patients, both children and adults, it’s specifically beneficial for the management of pediatrics as it provides the unique opportunity to prevent bowel damage for a person’s entire life and reduce the need for invasive procedures, anesthesia, and sedation. IUS has the potential to alter scoping schedules in the future. While it will not replace the need for colon cancer screening or the assessment of mucosal and histologic healing, IUS can reduce the need for further follow-up scopes once those targets are achieved in between the need for cancer screening.