The article discusses how teenage girls and young women post upsetting footage and commentary on social media about their “invisible illnesses” to gain attention and “likes” and bashes “Spoonies” for giving people a behind-the-scenes look at the reality of their chronic condition. Hold UP. As someone who has lived with Crohn’s disease for more than 17 years, who is patient advocate, and works tirelessly to empower and educate others about life with inflammatory bowel disease, by candidly sharing on social media and through my blog, I find it incredibly disheartening and worrisome that a story of this nature is in circulation.
The ableist mentally shines bright
How disappointing that a “news outlet” takes the time to belittle people who are battling debilitating and unpredictable illnesses and sharing their struggles not for attention, but for support and camaraderie. Unless you have a chronic illness, you don’t have the slightest clue about what it’s like to wake up each day and not know what the next hour is going to bring. Unless you have a chronic illness, you can’t begin to imagine the stress, worry, and anxiety that comes along with diseases that limit us and often set us up for failure when it comes to trying to keep up with the rest of society. Unless you have a chronic illness, you have no idea how isolating and overwhelming it can be to be young and unhealthy, different than your peers, while fearing what your future is going to hold. Unless you have a chronic illness, you can’t fathom what it’s like to juggle multiple specialists, appointments, medications, insurance, specialty pharmacies, and screening tests… just to survive. It’s imperative those with invisible chronic illnesses share their stories and show others that what they are going through.
Articles like this are extremely damaging and triggering to those who suffer in silence, the newly diagnosed, and furthers the fear of what could happen if you decide to come out of the “proverbial closet” publicly and share about your health struggles.
Patient communities NEED you to share
When I was diagnosed with Crohn’s disease at age 21 in July 2005, Facebook hadn’t even been out for a year. No one was going on social media and sharing they had a disease. I felt like I was on a desert island, all alone with a diagnosis that flipped my world as I knew it upside down. As an aspiring TV journalist, two months out of college graduation, I had no idea how I was going to function and follow my dreams. Nobody wants a chronic illness diagnosis. Nobody asks for this. Nobody wants to suffer so they can have “likes” and attention on social media, trust me. Never in my life have I seen people encouraging others to lie to their doctors about getting the diagnosis that they want.
With diseases like inflammatory bowel disease, this is not something you can fake. A diagnosis is received after scopes, scans, and labs, reflect that this is in fact the case. You don’t just walk into a doctor’s office and say you aren’t feeling well and exaggerate abdominal pain. It’s not a competition of who is “sickest,” people are sharing what they are going through for a variety of reasons. When someone is in a hospital bed, they may share for support, advice, and prayers. When someone is gearing up for a colonoscopy, they may share so they can get tips for easing the prep or coping with the worry of the unknown. When someone is pregnant and flaring, they may share to hear from other IBD moms who have been there before. The examples are endless. Patients are not haphazardly concocting up social media content and lies about their medical struggles to see who is going to get more attention. This is not “attention” people want.
By claiming we share for attention it goes against everything we stand for and belittles the lifechanging work patient advocates are doing to support and comfort their peers. As a patient advocate myself, I do so much behind the scenes “work” to guide those in the IBD community and help them every step of the way. It’s about helping others from the bottom of your heart and being the voice you needed to hear upon diagnosis and through milestones in life. It’s genuinely finding connections with those who are not just strangers on the internet, but quickly become your closest confidantes and resources. Since coming out and sharing I had Crohn’s disease in 2015, I went from having family and friends who didn’t have Crohn’s offering me support, to an army of thousands of members in the IBD family I can rely on who “get it” and are available right at my fingertips. THIS IS PRICELESS.
Sorry not sorry for the “upsetting content”
The article states “thousands of teens are banding together on social media as part of the movement” to support the Spoon theory. Imagine what it’s like to be living this reality versus just having to view a post on social media. Can you pause and put yourself in the hospital bed or on the operating table or on the couch about to do a painful injection and think about the pain and suffering those with chronic illness are forced to endure just to survive like the rest of society? It’s privileged to lash out against those who are doing all they can to show others what their lives consist of rather than bottling everything up—THAT is damaging, THAT is not healthy. Must be nice to have the privilege to keep scrolling and living your healthy life and only see a few seconds on your screen.
Should chronic illness patients be smiling as they’re suffering in hospital beds? Is it not normal to be crying when you’re worried and scared and can’t help but get emotional with all that’s on your shoulders? No one is complaining. It’s the stark reality. It’s heavy. It’s no surprise that more than 30% of people with IBD also deal with mental health issues and anxiety because life with the disease is so heavy.
It’s not about the money
Can we all pause and laugh about the fact the article claims those with chronic illness post on social media for the money. Hilarious. Get a grip. Even as a well-established and trusted “health influencer” within the IBD community, when companies reach out to me, it’s often to try products, not get a paycheck. When I am paid for my advocacy work it’s working diligently like your job as a journalist to write articles, create social media copy, and educate others about what my life is like with Crohn’s. I get compensated like any other human for using my skills and expertise, along with my precious time and energy, to sit on advisory boards and offer input and perspective for marketing and awareness campaigns. My job is not to be a patient, my “job” is to take what I’ve learned and use it to make a difference and help others.
This is not for show. Digging up past medical trauma and flare ups is not enjoyable. If businesses and pharmaceutical companies want to collaborate with chronic illness patients, they should be paying us for our invaluable intel and understanding. The article states patients have adopted “victim mentalities” …wow…and “communities of grievances” … when medical professionals are out of line or treat patients without respect, you better believe your ass they should be called out. How is change going to happen and life for chronic illness patients going to improve if we sit quietly. Be loud, my friends. Don’t allow articles like this to stop you from sharing. We NEED your valid experiences. You deserve to be heard. You matter. Even though the rest of society may be rolling their eyes or trying to stop us, they won’t, and they can’t.
I don’t want to go back to 2005 when I was all alone in my struggles with Crohn’s disease. I want to stay in 2022 when I can post whatever I want, whenever I want about my trials and triumphs as a woman, mother, and wife with Crohn’s disease and not fear judgement. Sometimes I’m thriving, sometimes I’m struggling. It’s vital that those with chronic illness continue to honestly share their stories on social media to provide clarity, education, and connection to those who relate wholeheartedly.
So, dear Emma, from one journalist to another, please start sharing stories that matter—don’t go after stories for attention or follow the adage, “it bleeds, it leads.” Seems like you are the one going after the likes. You should know better.
Sign the Petition
There has been outrage in the chronic illness community about this article—many feeling triggered and upset by the accusations and the claims made about Spoonies. An online petition has been created to have this Daily Mail article taken down—you can sign the petition by clicking here.
They call themselves “Propellers.” They’re a team of volunteers, made up of IBD patients and caregivers who created a non-profit called Propel a Cure for Crohn’s in 2016. They are laser focused on preventing and curing Crohn’s disease and, on the heels of their first research project funded at Stanford University in the world-renowned lab of Professor Mark Davis, they’re now determined to make a meaningful difference through their Roadmap to a Cure for Crohn’s effort. During this month (September 2022), they’re aiming to raise $50,000 to help get their latest project off the ground and to provide a solid foundation to bring their global team together.
This is a grassroots effort fueled by patient and parent volunteers. Patients and caregivers have an opportunity right now to directly influence a brighter future without Crohn’s! This is a peer-to-peer fundraiser—it’s not just about the monetary donations, but also sharing the message with others far and wide. Not only are international researchers involved, there are people all over the globe participating. In addition to the English-language campaign, there are also Swedish and Portuguese online campaigns running as well.
The Patient/Caregiver Perspective
Ildiko Mehes recalls what it was like when her 9-year-old daughter received her lifechanging Crohn’s disease diagnosis in 2017.
“As a parent, a serious diagnosis like Crohn’s is a huge shock, and it’s absolutely devastating and heartbreaking. Even during periods of remission, we are always on high alert and waiting for the other shoe to drop. At diagnosis, my whole world stopped, literally and figuratively. As irrational as it sounds, as a parent, you wish the rest of the world stopped with you to help you address the crisis. You wish that all of modern medicine rolled up their sleeves and urgently worked together to precisely diagnose the problem and bring her back to long-term health.”
As a caregiver, Ildiko has a unique sense of urgency and determination. She feels we need and can do better for IBD patients.
“When an otherwise healthy child, with no prior medical history, suddenly presents with IBD symptoms during a routine winter virus, you ask yourself “what caused this switch to be flipped?” Not having any answers to the underlying mechanism of disease onset or perpetuation, having a trial-and-error approach to disease management, and being forced to consider serious immunosuppressive medications with modest clinical trial benefits feels unacceptable as a parent. This is what drives me.”
As a pharmaceutical executive with more than 20 years of experience, Ildiko uses that unique skill set to go after complex and difficult goals with Propel a Cure and feels a deep sense of obligation to help our community.
“While there is excellent research ongoing in IBD, it happens in silos. It lacks global coordination and a plan. We don’t yet understand many basic things about Crohn’s. We are all just hoping for a “eureka moment” that hasn’t come over the last 100 years. We are continuously enticed with headlines of a “promising” new pathway or new drug candidate, usually in mice. And then that great idea sits there, with no progress made, a decade or more later. I know we can do better,” she said.
Natalie Muccioli Emery was diagnosed with Crohn’s disease in 2011 and she’s also a Propel a Cure Board member. She started dealing with abdominal issues 26 years ago. Being a veteran patient has provided her with perspective about how far treating and managing IBD has come and how far we still have to go.
“Propel a Cure was the first organization whose mission resonated with me. I appreciate their mission to cure Crohn’s Disease, but I even more appreciate the fact that they have laid out a plan as to what the areas of knowns and remaining unknowns are in their Roadmap to a Cure for Crohn’s project. Complex issues like Crohn’s Disease will take a collaborative and systematic approach to address, and this cause has captured that,” said Natalie.
Not only is Natalie an IBD mom, she’s also an IBD aunt!
“I believe that as an adult with IBD, the way I embody the role of a “Crohn’s Warrior” is not for myself it is for the next generation. I have “been there and done all that” with Crohn’s. But just because I did it with Crohn’s doesn’t mean the next generation should have to. I grow increasingly concerned when I see the rising rates of IBDs like Crohn’s in younger people. I believe the rising rates of Crohn’s should create a sense of urgency and a desire for a better future.”
Putting the puzzle pieces together
The Roadmap to a Cure is an ambitious project but one that is needed to drive real progress toward cures and prevention of IBDs, not just talk about “cures” in some very distant future. Ildiko says the brilliant clinicians and scientists she has gotten to know all tell her that getting to a cure will take a grassroots effort, global collaboration, and involvement of patients and caregivers.
“We at Propel a Cure are deeply committed to doing exactly that. The first step in our project is to systematize what we already know about Crohn’s today. We know a great deal, thanks to research. But when we are talking about complex fields like genetics, epigenetics, immunology, microbiology, epidemiology, multi-omics platforms and artificial intelligence, etc. there is no way any one person or group can know everything. We need a large global group of dedicated and brilliant experts to put all the puzzle pieces we already have on one table so we can begin to then put the pieces together,” she explained.
Grabbing the attention of medical professionals and researchers
Propel a Cure grabbed the attention of Dr. Bram Verstockt, MD, PhD, Department of Gastroenterology and Hepatology, University Hospitals Leuven, on social media.
“I truly like the concept of joined forces across various stakeholders, including patients and caregivers. As clinicians and scientists, we can have ideas about how to move forward based on experiences and interactions with patients on a daily basis. However, the next step really is to involve patients actively in many of these projects, as is currently the case with Propel a Cure,” said Dr. Verstockt.
The “Roadmap to a Cure” aims to bring together expertise across many different fields and niches in IBD.
“Over the past decades, a lot of scientific evidence has been generated in multiple domains of Crohn’s disease, so now it’s time to bring all that evidence together and truly connect the dots. Only by doing so, one might unravel knowns and unknowns and highlight where the remaining key gaps are, and we can define the priorities and strategies of how to fill these gaps to significantly advance the field, to improve the lives of patients with Crohn’s disease,” said Dr. Verstockt.
Where the roadmap can take us
After the initial step of putting together the state of the art, the next step is identifying gaps in our knowledge: what puzzle pieces do we still need? The third step is to develop the plan, or the Research Roadmap, to get from what we know today to developing cures and prevention strategies.
“We truly believe in a future where we can prevent and cure Crohn’s and eliminate so much patient and family suffering,” said Ildiko.
The reason this requires a grassroots effort and all of us patients and caregivers to fund it, is that otherwise the current system largely doesn’t provide incentives for new ideas or cures or global collaborative efforts of this magnitude. A recent paper discusses how the same ideas have been funded for decades, with limited progress and that we urgently need new directions.
Ildiko believes the current research incentive model is broken. “If we want true progress and cures for Crohn’s and other IBDs, we need a new collaborative model among IBD foundations/nonprofits, patients, caregivers, researchers, clinicians, and others. I believe this can become a model for other chronic and immune-mediated diseases.”
Click here to watch a video where Ildiko explains the Roadmap to a Cure project further.
Hopes for the future
“I would really like to see more key opinion leaders be brave about acknowledging the risks and limitations of current therapies, avoid putting lipstick on a pig when discussing some newer drug candidates in trials with lackluster results and the same mechanisms, dispense with biased headlines like “safe and effective” when the data is much more nuanced or unclear, and openness to “outside-the-box” ideas, like microbiome manipulation, including via diet, infectious triggers like Epstein-Barr virus in Multiple Sclerosis, vagus nerve stimulation, Fecal Microbiota Transplant (FMT), hyperbaric oxygen, etc. and also adopt routine monitoring via intestinal ultrasound for many patients,” said Ildiko.
As of now (September 12, 2022)—more than $26,609 has been raised!
“I have been overwhelmed by the response so far, as has the entire Propel team. People are really connecting with our mission. We are getting donations from so many states and countries! We have received more messages of profound thanks and hope than I can recount. This fuels us so much,” said Ildiko.
Natalie feels a wide range of emotions each time she sees a donation come in or the campaign shared across social media.
“I go from feeling hopeful, to introspective, to sad. I truly wish we did not have to do this campaign and that in 2022 we knew what the underlying cause(s) of Crohn’s are, and that safe, effective, reliable treatments were available for all Crohn’s patients. But here we are. Crohn’s is still very much part of the lives of patients and caregivers, and we need to take action to change that. I am so grateful for the outpouring of support we have received so far, but there is more work to be done!”
Propel a Cure has virtually no overhead fees or salaries, so every single dollar donated to Roadmap for a Cure goes to research.
“We are all volunteers who work out of our homes. The donations will be put towards collaborative research teams worldwide. Each team will lead a contributing area to the development of Crohn’s Disease (environment, microbiome, immune system etc.) and highlight where the gaps in knowledge remain,” said Natalie.
“The ultimate dream obviously would be to cure and if not, to significantly improve the quality of life for millions of patients worldwide,” said Dr. Verstockt.
Click here to donate to this incredible cause or to join their team.
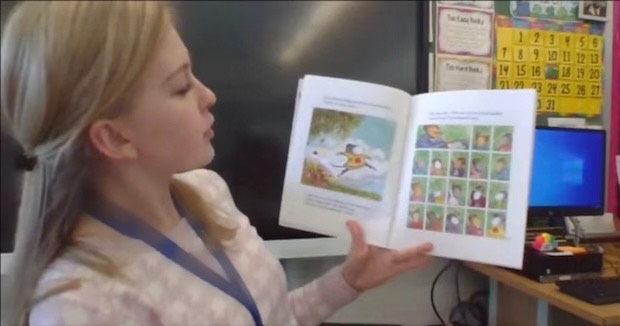
Life with IBD impacts our careers in many ways. Our disease can often dictate what path our future takes. As students, teachers, and families gear up for another school year, I thought it would be interesting to hear from educators who have IBD about what it’s like to lead a classroom while living with an unpredictable chronic illness. This week on Lights, Camera, Crohn’s hear the inspiring stories and perspectives of four unsung heroes who don’t allow their IBD to rob them of their career aspirations.
Sarah Rife has been a teacher for seven years, she’s also an IBD mom and an ostomate. She’s currently teaching eighth grade math in the Chicagoland area, but previously taught high school Geometry and Algebra.
“I have taught through many highs and lows Crohn’s wise. For the first 5 years, there wasn’t a single year that I didn’t use every single sick day I had (and then some unpaid days). I believe four out of five of those first years, I had at least one hospitalization where I missed consecutive days, as well. In this time, I was on four different medications and tried a clinical trial.”
While this was going on Sarah says she rarely ate at school and if she did, she stuck to 3-4 “safe foods” to help get through the day.
“I constantly taught with an escape plan in the back of my mind. You can’t just leave a room full of 28-32 kids sitting unsupervised, so I constantly had to think about things like ‘Who will I have cover my class?’ ‘What if I am gone more than 5-10 minutes?’ ‘What can they work on that they will know how to do if I have to step out in the middle of teaching them something new?”
Sarah is open about her IBD with students and their families and says having IBD has made her a more compassionate educator since she understands when students need to miss school.
“When I was younger, I was the student missing multiple days of school. I remember the things that some of my favorite teachers did that helped me to not stress when I felt like I had mountains of missing work. Whenever I have a student gone for health reasons, physical or mental, my standard answer when they come back is “Worry about everything else first, and then I’ll talk to you about what we can do to bring you up to speed in math class. Don’t stress, I will work with you on it.”
One year while being evaluated by her principal during a drop-in visit. He walked into her room, sat down, and started typing. He was aware of her Crohn’s, but Sarah panicked when she knew she needed to make a mad dash to the bathroom while he was in her classroom observing her.
“I ended up going over to him and asking “I really need to step out and use the bathroom. Do you want me to grab someone like I usually do, or do you just want to watch them since you are here” He agreed to watch them, and I ran out to go to the bathroom. Whenever I had to step out, I was also conscious of what time it was. This time, there were about 30 minutes of class left. In my head, I needed to get back ASAP because THE PRINCIPAL was in there and he was supposed to be observing me. When I heard the bell ring and I was still on the toilet, I panicked – I’m talking instant tears. I was able to finish and tried to hurry back to my room. My path crossed his on the way back and I started to say, “I’m sorry, I didn’t know I would be that long.”
Sarah says her mind was racing with crazy thoughts about her abilities as a teacher and what she was capable of. The principal could see she had been crying and more tears were starting to fall, and he interrupted her and said, “Sarah, I am not worried about it. This is your third year here and we know this happens. I am worried about what I see when you are able to be in the classroom and what I saw meets and exceeds our expectations. Please don’t worry about it.” – This reassured her so much more than even he will ever know, but the story replays in her head every time an administrator pops in her room for an unannounced observation – even 4 years later.
When Sarah taught high school, she was nowhere near remission, forcing her to be extremely transparent with her students.
“I told them that I had a disease called Crohn’s and that in a nutshell, my immune system was attacking itself, specifically my intestines. They knew that me having to step out of class and disappear to the bathroom was a possibility and witnessed it multiple times a week, sometimes in the same class period. They were also aware that often these bathroom breaks would result in pain, nausea, and exhaustion.”
Whenever Sarah would have an episode, she says the students went above and beyond to be empathetic and understanding.
“I had students volunteer to work out examples on the board so I could sit down, and they were extremely good at switching gears and changing the plan if I needed to do something with less walking around, standing, or talking – for example work on a worksheet instead of doing notes or bringing questions to me at my desk over me walking around offering help. I really do think high school students are more resilient and compassionate than people give them credit for.”
Since her ostomy surgery, Sarah’s life in the classroom has changed for the better.
“I feel like a completely different teacher. My energy isn’t nearly as much of an issue, I can teach without constantly having an escape plan or worrying how long I’ll be stuck in the bathroom, I can eat lunch at school like a normal person, without worry or only packing the same 3 things, and for the first time in my teaching career, I had paid sick days left at the end of the year. I had a chance to worry about the content I was teaching first and my health second, which I had never been able to do in the past.”
Sadly, this past week, Sara’s ostomy leaked while she was in the middle of teaching 30 thirteen-year-old students. Luckily, she works less than one mile from home so she yanked her shirt down as far as it could go and told the admin she’d be back in 15 minutes.
Sara Margolin of New York has been a professor of psychology for 15 years, with a focus on neuropsychology, cognition, and aging. She says her experience with ulcerative colitis and two other autoimmune conditions has made her more understanding toward her students. Sara says, “Robin Roberts said it best, “everybody has something.” And she’s right. I’m not the only person with a chronic illness. Many of my students struggle or someone they love struggles. Understanding that they deserve the compassion that I wish to have has only made me a better professor.”
Sara has had to leave the classroom on multiple occasions to urgently use the bathroom.
“I will either quickly show a film if I have one at hand or pretend to get a call from my children’s school and “need to leave to take it.” But in my smaller classes, where the discussion leads us there — in the discussion of medical trials, medications for chronic illness, or psychological issues stemming from chronic illness, I’ve discussed my condition. And there have been a handful of students over the years who have been diagnosed while in my class, and I share with them that I understand what they are going through. We bond over that.”
Now that classes are back to in person this fall, she has some concerns knowing she is not fully in remission and not able to teach remotely anymore.
“When I was teaching at home, I had a time or two where I turned my camera off and taught from the bathroom…. EEK! … and knowing that I may be in the position to need to do that but not be able to is nerve wracking. But I know that my colleagues will fill in for me if I do need them to.”
Madison Laspisa of New York has taught fourth grade for four years. She was diagnosed with Crohn’s disease in June 2020, during her first year of having her own classroom. Not only were schools shutting down when her severe symptoms began, but she was dealing with school closures and remote teaching, on top of being diagnosed with a chronic illness.
“My life was flipped completely upside-down to say the least. I was truly devastated at everything that was happening around me and to me. My first year in my own classroom should have been the most memorable part of my career (in a good way), but I sadly cannot say that. My life changed before I had a minute to truly process what was happening. However, since we were forced to stay home because of the Covid-19 pandemic I had the availability to see doctors and get procedures done as needed. Had it been a normal school year I would have had to take a leave of absence during my very first year of teaching.”
Since then, Madison says her IBD has impacted her experience as an educator in more ways than she’d like to admit.
“Aside from needing to take days off to receive my infusion, there have been days where I needed to take a last-minute half day because I desperately needed to see my doctor. At times, this can leave the main office scrambling to find a substitute for my class with an already existing shortage. Not to mention the schedule change my students have to now adjust to with their teacher leaving mid-day.”
Madison says the toughest challenge for her is the amount of time she needs to take off to receive her medication and meet with her care team. She does her best to schedule doctor appointments after school hours, but sometimes it’s not realistic. Right now, she receives her biologic every four weeks, which was changed from every eight weeks.
“This required change in my treatment plan will now require me to miss time in my classroom with my students twice as often. It’s not as simple as “taking a day off” as it is very time consuming to create thorough substitute plans on the days, I am absent. It makes me feel like I’m a “bad teacher” because I have to take time away from my students and classroom. I feel guilty when I’m making substitute plans because I know I am going to be absent the next day and my students have no idea.”
Madison says the weight of the unpredictability of her Crohn’s makes her anxious. She worries about waking up one morning and not being physically able to go into work and do her job.
“I love what I do with a passion and anything that can hinder my ability to do my job to the fullest breaks me. Having the summer months off allows me to slow down and take a break from my rigorous work schedule. In a sense, it provides me with some relief because I know being home, I don’t have to worry about missing work because of my IBD.”
Madison hopes that if someone reading this article aspires to work in education, that they don’t allow their IBD to deter them from taking the leap.
“Teaching and being with my students is my escape from my reality with IBD sometimes. IBD has robbed me of so much and I refuse to let it rob me of my dream job. Do not let IBD dictate what you can and cannot do. Being a teacher and having IBD are both full-time jobs and can be extremely overwhelming at times but loving what you do makes all the difference.”
Krista Deveau has been a teacher in Canada for seven years, she recently became a mom and is an ostomate. She currently teaches kindergarten but has also taught third grade and worked as an intervention specialist helping students with literacy and numeracy. She started her teaching career three months after having a bowel resection surgery. She ended up landing back in the hospital three months later, weighing under 100 pounds, in one of the worst flares of her life.
“My GI team told me that I had to work part time if I was able to or else my chances of being back in a hospital bed were quite high. Working part time has really given me a work- life balance where I can take care of my health and myself and also focus on my career.”
Prior to receiving her ostomy, Krista tells me it was difficult to teach, as she was having accidents almost daily and was vomiting in a garbage can outside of her classroom. During her first year of teaching, she had a meeting with an administrator after school and happened to have an accident. Krista had forgotten to bring a change of clothes.
“I was so embarrassed that I stayed behind my desk all afternoon so students couldn’t smell me. I cleaned up at recess as best as I could. After school I went to meet with admin and told them I had to leave because I had had an accident and didn’t have a change of clothes. I had already told them about my situation and how I was experiencing incontinence, so it wasn’t a big deal, but I was humiliated.”
Krista says teaching is a stressful and demanding job—and that it’s important to be honest with your admin team so there are no surprises along the way.
“Make sure to take care of yourself. Don’t stay late every day. Work smarter, not harder. Collaborate and share plans with other teachers so you aren’t reinventing the wheel. Lean on your coworkers. Find one good coworker friend that will have your back. Don’t work on weekends. Don’t take on too much of the extras, it’s okay to say no. Try to have a healthy work life balance. And find a school/school board that’s a good fit for you and where you feel supported.”
Helpful Tips for Educators with IBD
Be flexible and rework plans, not just in terms of being absent, but also what you can do instead if your energy level is too low to actively teachon your feet or if you need to talk for an hour straight multiple times a day.
For example: Create PowerPoint slides where every single step of a math problem animates itself with the click of a button so you can be sitting instead of standing up, exerting energy.
Teaching is a pleasant distraction. Teaching enables you to get your mind off your IBD and do what you love. Regardless of what you do professionally, your IBD is going to be a part of you, why let it take more from you than it already has? Enjoy the thing you can enjoy.
Make the appropriate accommodations for yourself. Once you are hired or work in a school district, provide school administrators with medical documentation as to why you are unable to work on a certain date. At the start of the school year, it can be helpful to turn in a letter stating your treatment plan along with a request to use the bathroom when needed stating your medical condition. Typically, teachers use the bathroom on their scheduled breaks, but this accommodation allows that in the event you need emergency use of a bathroom, someone will need to cover your class at any given time. This type of documentation for my district must be renewed every school year.
For example, if a typical teacher instructs five classes with an hour to plan and a 25-minute lunch, split with a 25-minute study hall, inquire about keeping your schedule consistent year after year and teaching two classes, then having a plan period, teaching two more classes, and then a ‘duty-free lunch’—meaning you get the entire 56 minutes for lunch, instead of having a study hall to give you a buffer for a bathroom trip along with minimal interruption to other classes.
Request a classroom close to a bathroom and department office so that there are people nearby in case you need someone to cover your class on a moment’s notice.
Try not to fear the worst. Being hospitalized is beyond your control and whether you have a chronic illness like IBD or not, life happens, and co-workers will need help from time to time. Rather than stress about who gave up what time to help you, focus on how to pay it forward and help other teachers when you feel well and when someone else is in need.
Teaching takes a village. Everyone is more than willing to help you out if you let them. Besides, it all becomes so much easier when you don’t feel like you must hide such a huge part of who you are. The sooner you realize people are willing to help you and you don’t have to try and keep it hidden, the easier teaching with IBD becomes.
This blog was sponsored by Mahana Therapeutics. All thoughts and opinions shared are my own.
Did you know that two thirds of people with inflammatory bowel disease (IBD) also meet the criteria for a functional GI disorder? Dr. Aline Charabaty, Dr. John Damianos, and Dr. Katie Dunleavy recently presented a paper at the 2022 Guild Conference addressing the substantial overlap between Crohn’s and ulcerative colitis and the gut-brain interaction. You may wonder what constitutes a functional GI disorder, irritable bowel syndrome (IBS) is the most common.
“What we know is that up to 30-40% of patients with IBD in remission (absence of gut inflammation) continue to have GI symptoms such as abdominal pain, bloating, diarrhea, constipation, and fecal urgency, due to disorders of gut-brain interaction (DGBIs, also known as functional gastrointestinal disorders),” explained Dr. Aline Charabaty, director of the IBD Center at Sibley Memorial Hospital.
As someone who was diagnosed with Crohn’s disease more than 17 years ago, I’ve been told by multiple gastroenterologists that I have IBS as well. At one point I was told, “you have a touch of IBS” …whatever that’s supposed to mean. I know I am not alone in believing I have both IBD and IBS, especially since having 18 inches of my small intestine removed for bowel resection surgery in 2015.
Dr. Charabaty says this is the case for many patients because of the following:
Structural damage to the gut caused by IBD. Crohn’s disease can lead to small bowel stricture, which can cause cramps and constipation (by blocking or slowing down the stool flow); Long standing UC can create a “lead pipe colon” (where the colon loses its normal twists and turns that typically slow the stool flow down and become like a straight tube which makes the stool “fall” straight down), which can cause diarrhea and urgency. Resection of part of the small bowel and colon decreases the surface of the bowel that can absorb the water and solidify stools, which leads to loose stool. Finally change in bowel anatomy from stricture or resection, abdominal adhesions from prior inflammation, abscess, or surgery, can lead to small bowel bacterial overgrowth (SIBO) which can cause bloating, pain, diarrhea, or constipation.
People living with IBD can become intolerant to certain foods or modify their diet. This can lead to change in gut flora that affect gut functioning and lead to GI symptoms.
Recurrent flares or previous severe inflammation can lead to change in the gut sensation. Visceral hypersensitivity, gut motility, gut microbiome, intestinal permeability, and how someone perceives and tolerates all the sensations (pain, discomfort) that come from the gut.
IBD affects people’s emotional and mental health and is associated with a higher incidence of depression and anxiety. We know that depression and anxiety can affect the gut functioning and lead to IBS symptoms.
“All these changes are similar to what we see in people living with IBS and can cause IBS and IBS symptoms in people living with IBD. Sometimes the way I explain it to patients with IBD, is that IBS is like the PTSD of the gut. The gut has been inflamed, traumatized, manipulated, changed from prior flare and now it can’t go back to functioning properly, even if it’s healed and it looks normal,” said Dr. Charabaty.
This is where Mahana IBS comes in. The main mission? To empower people with chronic conditions to lead fuller lives through digital therapeutics. That’s why they debuted their new prescription digital therapeutic app, Mahana IBS, in the fall of 2021. Their wish is to destigmatize IBS and bring hope and meaningful solutions to patients like you and me.
Steven Basta is the CEO of Mahana Therapeutics. He says the app is safe, FDA-cleared, and has been clinically proven in the world’s largest trial of its kind to reduce IBS symptom severity.
“Cognitive Behavioral Therapy (CBT) has long been recommended in clinical guidelines as a safe and effective treatment for IBS. Access to traditional CBT with a therapist has been a huge challenge due to the limited number of IBS-trained therapists (less than 300 in the US). Now patients can access CBT and learn the skills it provides to help a patient manage their disease by using Mahana IBS on their smartphone, with great results: 3 out of 4 patients find relief and results for most patients are lasting. Mahana users can complete the program in 90 days or less at their own pace with daily lessons on their phone to create a healthy brain-gut connection and live life more fully.”
Both IBD and IBS negatively impact our quality of life. Our mental health, our psychosocial health, and our financial health (increased health care utilization, missing days of work, medications to treat symptoms).
“Beyond treating the inflammation of IBD, and preventing IBD-associated complications, it is important to recognize and treat IBS when it is present, so people can recover and optimize their quality of life. CBT is an effective therapy for IBS and reduces or eliminates symptoms of abdominal pain, diarrhea, constipation, and bloating,” said Dr. Charabaty.
Unfortunately, access to a therapist who can provide gut-directed CBT can be limited: lack of therapists trained in CBT in someone’s geographical area, limited time availability (many therapists are not taking new patients, or have long waits to see someone; or from an IBD patients’ standpoint—lack of “extra” health care time available, when we often juggle many health appointments), deal with lack of insurance coverage, additional costs related to taking time off work and the expenses related to travel and participate in CBT sessions. Which makes the app even more useful and beneficial for the patient community.
Bringing up digital therapy to your GI provider
Digital therapy is new, and Mahana Therapeutics is working hard to spread awareness in the clinical and patient community to ensure everyone who could benefit, has access, and knows about Mahana IBS.
“It’s important for patients living with IBD to ask their doctor whether Mahana IBS is suitable for them and discuss how it can work with their treatment plan,” said Steve.
As a gastroenterologist who specializes in IBD, Dr. Charabaty says, “Having an FDA-cleared prescription app that provides CBT right at the patient’s fingertips is pure gold! Easy and effective access to CBT at a time that is convenient for the patient, in the privacy of their home, without the added extra time and cost burden of a visit to a clinician. I believe that with this technology/app, which removes many barriers to accessing therapy for IBS, that many more people living with IBS (whether they have IBD or not) will benefit from what CBT has to offer and will be able to improve their symptoms and regain their quality of life.”
Patients who are in IBD remission experiencing IBS Symptoms may want to ask:
“If my IBD is in remission and my symptoms are IBS related, could a digital therapy treatment such as Mahana IBS gut-directed CBT be suitable for me?”
GIs who want to understand more about the clinical evidence and indications for use for Mahana IBS can head this website to check out the medical provider welcome pack which contains all the clinical information they need to get started and to prescribe Mahana IBS.
While the app is a prescription, patients can also download the app on their own and show their gastroenterologist in clinic. But to gain access to the full program, patients need to get a prescription to unlock the benefits.
How the app is tailored to each patient
People experience IBS differently which is why Mahana IBS provides a personalized approach, regardless of type of IBS. In the early sessions of the app, patients create an IBS symptoms profile, take an IBS Symptom Severity Score assessment, and create their personalized model.
“This means people get to identify and capture their own symptoms and associated thoughts, behaviors and actions that arise as a result of these. As patients progress through the app and unlock tools and content, exercises are provided that are tailored to people’s individual IBS symptoms. Progress is recorded through the IBS Symptoms Severity Score at the beginning, the middle, and at the end of the program to measure results,” explained Steven.
Reframing thought process to reduce IBS symptoms
We can all relate to how feeling anxious can leave our ‘stomach in knots’ but in IBS there is a disorder of the brain-gut communication which causes and perpetuates symptoms. For example, our guts can release hormones that change our mood, and the brain in turn sends a signal to our guts to change our bowel functions which then sends more signals to the brain.
“Patients may develop habits or use ‘coping’ techniques that perpetuate the vicious cycle of brain-gut miscommunication without knowing it. The Mahana IBS app uses a gut-directed CBT program that was researched and developed over several decades. It is designed so you can understand your personalized patterns and then learn skills to help support a healthier brain-gut interaction. The program delivers a combination of education and exercises so that patients identify and reframe thoughts, feelings, and actions related to IBS. Through the Mahana IBS program, patients can gain tools and habits for managing symptoms long-term,” said Steven.
Along with learning to reframe our thoughts, the app also features visceral relaxation exercises like diaphragmatic breathing or belly breathing, which can reduce visceral pain and improve GI function. Mahana IBS has easy to follow animations to help patients learn and practice these techniques.
While Mahana IBS is a treatment program designed to be completed in 90 days or less with lasting results, Steve tells me some patients may experience relief from their functional GI disorder within a matter of weeks.
“Patients go at their own pace, so they may complete the program more quickly. Once the 90 days have elapsed, patients can still access their personal data (for example goal setting, IBS-SSS score or their personal IBS Model). Patients can return to the app at any time to find support in any of the lessons, tools, and exercises they have completed.”
Accessing Mahana IBS
Mahana is committed to affordable access. Some patients may be reimbursed by insurance. For those patients who are not covered by insurance, there is a subsidized program to ensure patients will pay no more than $90 out of pocket for prescription cost. That’s less than a single session with a therapist ($120/session) for the complete 10-session program.
Steven says it’s incredibly rewarding and a huge privilege to lead the Mahana team transforming access to treatments like this through digital therapy.
“As CEO of Mahana Therapeutics I am inspired by so many amazing patients with IBS. One patient who had struggled for years with IBS symptoms that made her feel truly hopeless expressed that Mahana IBS changed her life. With the lessons and skills she learned, she no longer avoids the food she loves, and the way she thinks about IBS has altered so completely, it no longer limits her life. Our team’s mission is to make this story a reality for millions of IBS patients.”
Mahana IBS is available for download directly from the Apple App store and Google Play store—and the first session is free to try! To unlock all the specific features and benefits, you’ll want to get a prescription from your GI. Once you’ve been prescribed the app by your doctor, you will get a message from Blink Pharmacy with instructions to get started.
**Disclaimer: This article is in no way meant to offer medical advice or guidance. Medication to treat and manage IBD is NOT a failure. Please understand this is one person’s experience and journey. Prior to going off medication, consult with your gastroenterologist and care team.**
She was diagnosed with Crohn’s disease in 1991 at 19 years old. As a veteran patient and IBD mom of two teenagers, Kelli Young says the COVID-19 pandemic, along with turning 50, inspired her to dig deeper into her health journey and look beyond the “cookie cutter” approach to treating IBD. After multiple surgeries and decades of biologics and other medications, she was determined to try a different approach.
Much like many of us in the IBD community, we often choose to hide our disease from others. Kelli says 15 years of that strategy often left her feeling misunderstood. Once she started sharing and opening herself up to support, her world changed for the better. Anytime someone is sympathetic and says, “you poor thing,” Kelli reminds them that Crohn’s disease molded her in the person she is today and that everyone has problems, hers just happens to be IBD.
“Having lived more than half my life as an IBD patient, I knew I didn’t want to live the second half of my life the way I did the first half.”
Taking a closer look into food sensitivities
It’s no surprise the importance of diet has become a larger part of treating IBD in recent years, but there’s still a lot of gray area.
“Diet is often the one thing that the medical profession overlooks or provides the same generic diet to everyone, assuming everyone is the same. Diet is the #1 factor that affects your health in every way imaginable. Your energy, sleep, weight, sex drive, bowel movements, heart rate, and mood, just to name a few.”
Prior to changing her diet, Kelli connected with her longtime friend of more than 20 years, Dr. Sean Branham, a chiropractor who specializes in functional medicine. Dr. Branham ordered the Oxford Food Sensitivity Test. The test measures inflammation in the body on a cellular level. Food sensitivities are unique to each person, so it’s impossible to determine what your sensitivities are without getting tested. Reactions can also be delayed or be dose dependent.
Kelli says, “The Oxford Food Sensitivity Test looks at all types of white blood cells (Neutrophils, Lymphocytes, Monocytes and Eosinophils) and measures release of all pro-inflammatory chemicals like Cytokines, Histamines, Prostaglandins and Leukotrienes. Certain groups of foods are pro-inflammatory to humans because we may not contain all the enzymes to thoroughly break them down (like dairy). Other foods are pro-inflammatory because of their processing, like many different forms of sugar. Some are inflammatory due to genetic modification like gluten. Some healthy foods can create inflammation once digestive damage has been done and these partially digested foods leak across the digestive barrier and trigger an immune response.”
Customizing diet with Food Sensitivity results
Kelli’s tests results showed mushrooms, cashews, trout, mangos, green peas, coconut, among other foods, triggered an immune reaction. Once Kelli had her Food Sensitivity results in hand, her and Dr. Branham started to customize her diet.
“We first started by removing the bigger classes of pro-inflammatory foods like; dairy, sugar, gluten and soy and then assessed specific foods that were causing a problem for me individually.”
Along with removing these food groups from her diet, Kelli did a whole-body digestive cleanse that involved a specific diet with supplements, a shake, and a cream to rid the body the body of toxins, decrease inflammation, and cleanse the liver and digestive tract.
“Testing revealed that there were more than just digestive issues going on. I also had a blood sugar regulation problem, Estrogen dominance, nutrient deficiencies, a need for: digestive enzymes, immune support, and microbiome support. Once I completed the cleanse, we customized a supplement regimen specific to me based on my test results. We started with what Dr. Branham considered the most important things first and then as we corrected those issues, we moved on and tackled the next issue and so on.”
Celebrating a “new way of life”
As a single mom of a 19-year-old and a 16-year-old who have supported her through her IBD journey every step of the way, Kelli calls these lifestyle changes her “new way of life”.
“When my son was between the ages of 8-12 years old, he was showing IBD symptoms, but he didn’t have IBD, he was experiencing empathic pains. He watched me, a single mother, battle with the daily struggles. I tried to hide it, but he saw right through me. Today he is 16, growing, thriving, and enjoying his healthy mother. My daughter, 19, the age at which I was diagnosed, is thriving as well. I am now able to truly be present in both of their lives.”
When Kelli and her husband divorced, her children were only 8 and 5 years old. As an IBD mom it made an already challenging time that much more complicated. She never dreamed she’d be at this place in her life health-wise.
“Back then I wondered how I was going to give myself my own shots, how I was going to care for two small children 50% of the time when I was always sick. Being a single mother with IBD forced me to take a good hard look at my life, not only for me, but for the sake of my children. My motto used to be “expect the unexpected” and “no expectations.” Today, I no longer worry about the future bad days or wonder if I’m going to be around to be a grandmother someday. Yes, it’s difficult at times to follow such a structured lifestyle, but it’s even more difficult living a life being chronically ill.”
Going off all meds
Kelli has been off all IBD medication since May 2021. She says her GI of 30 years is reluctantly supporting her decision to go this route on her patient journey. Kelli had a colonoscopy in June 2022, and after the scope in recovery he said, “Well Kelli, your new way of life is working. I’ve never seen your scope results look this good.”
While this lifestyle may seem “extreme” to some or difficult to follow, Kelli says she was sick and tired of being sick and tired.
“The definition of “remission” varies depending on who you ask. I am celebrating three years of a “disease free” diagnosis. The Crohn’s will ALWAYS be very much part of my life, but now, the only time I have a “bad day” is when I cheat on my new way of life, eating something I shouldn’t be eating, not getting enough sleep, not exercising, and not managing my stress.”
Take yourself back to your most vulnerable moments as an IBD patient. There’s a good chance you’ve experienced an upsetting situation that involves getting an IV or a blood draw on more than one occasion. What may seem simple, can be complicated and traumatic. Back in December 2020 I shared an article on Lights, Camera, Crohn’s entitled, “Sticking to your guns: How to Speak up During Blood Draws and IVs”. This past week, I received a reader comment that quite honestly, made me angry.
The comment read, “Phlebotomists are only allowed 2 sticks anyways. After 2 unsuccessful attempts they should be getting someone else. No need to tell them they only get 2 tries lol. “I’m a hard stick” ok cool lol like we’re not going to figure that out while looking for a vein. Don’t be this annoying patient that everyone arguing who’s turn it is to deal with every time they walk in lol. Try being nice! Healthcare workers have to deal with too many shitty people. We only wanted to be in healthcare to help people! Not to hurt them!”
This comment inspired me to connect with the IBD community to hear firsthand what it’s like from our side, the patient experience. Shocker—we’re not “annoying patients” or “shitty people” …many of us have dealt with unimaginable pain and suffering related to our diseases. We’re tougher than nails because what we’ve been forced to endure, but that doesn’t mean we should be proverbial pin cushions made to feel guilty for making someone’s job a bit more difficult. It’s not a matter of placing blame or pointing fingers, it comes down to basic human decency, showing empathy to the person who is sick, trying to manage a complicated, unpredictable disease, who needs help.
In an Instagram poll I asked, “Has it ever taken more than two tries for a blood draw/IV? In a 24-hour period, 530 patients responded. 85 percent voted YES, 15% voted no. I followed up by asking “Do you share ahead of time that you have tough veins?” 76% of people voted YES, 24% voted NO.
In my own 17-year journey with Crohn’s disease, I’m your textbook patient with “bad veins”. It’s always an ordeal to get an IV started, blood draws often take multiple tries. I’m no stranger to this patient struggle, but I’ve learned to speak up respectfully in the moment and offer guidance rather than suffer in silence.
During a hospitalization for an abscess the size of a tennis ball in my small intestine in 2008 it took EIGHT tries to get my IV started. That moment still rocks my world when I think about it. Two nurses, rapid response nurses, and finally an anesthesiologist got the job done. That hospitalization I was told I needed to start a biologic—the only options back in 2008 were Remicade (an infusion) and Humira (a self-injection). One of the main reasons I chose Humira was because of my newfound fear of IVs.
Prior to an MRE in 2015 to see if I needed bowel resection surgery, I was so sick and rather than attempting to re-start an IV mid-hospitalization, the nurses brought in the vein finder—it was a game changer during an already stressful time.
In the recovery room after my colonoscopy in 2021 I had a nightmare of an experience with a nurse that I later reported to the hospital. My GI had asked for them to do labs through my IV (which is always a nightmare and never works because I’m so dehydrated from the prep). They decided to wait until after the procedure to get the labs. I was out of it and woke up to a nurse poking me SIX times. I kept pleading with her to let me go to a lab and to stop. She didn’t even respond to me; it was like I was invisible. Instead, she was ripping my well-respected GI apart and complaining to other nurses loudly about being asked to draw labs on dehydrated scope patients. I asked for my husband, she rolled her eyes. When he came back and told him I needed time to “calm down” before we left. I was hysterically crying. When I reported her unprofessional and heartless behavior, by the response on the other line, pretty sure I had the last laugh. Moving forward this fall with my colonoscopy I won’t be allowing labs to be drawn prior to or after the procedure. I’m more than happy to go to a lab at a different time and save us both the headache.
Let’s hear what fellow patients have to say about it
I was overwhelmed by the response from our community regarding this issue. I’m not able to share all the input but appreciate everyone taking the time to share.
When healthcare professionals say the darndest things
“I have so many memories of nurses/lab techs ignoring me when I say I’m a hard stick and dismissing me when I point them to the tried-and-true vein. I’ve heard everything from “I never miss” to “I used to work in the NICU, if I can get an IV started on a newborn, I can get one started on you.” And still, my veins will blow, and they’ll take more than three times to get it. These experiences have made me regret choosing Inflectra infusions as my first Crohn’s medication, as it forces blood draws and an IV every 8 weeks.”
“Some healthcare workers have rolled their eyes at me and were like “Well, let me just see what I can find” and then act irritated with me in the end when they need to ask me where to stick me anyway.”
“Usually they tell me something like, “I like a challenge!” or most recently, “Do I look like the kind of nurse who would be afraid of veins?”
“Nurses will always tell me “They’re the best” …yet they’re usually the ones who can’t find the veins. Then it’s almost like a disappointment in the patient because they always get everyone’s veins but can’t get yours?! It creates so much hoopla over nothing.”
“One hospitalization a nurse asked me if I “don’t want to get better” and if I “just want to keep getting sick.” She said, “Let me do my job and grabbed my arm hard.” I tried to suppress the screams as it was extremely painful. She tried seven times. My GI was livid. He put in a warning to the hospital about her. It was extremely scary to have someone be so rough when I’m so vulnerable and to be at their mercy. In contrast, I just had an amazing experience during my iron infusion. Each nurse tapped my veins for ages and then said they were going to call someone better than they were. I ended up with the head doctor from the ICU!”
“In the early stages of diagnosis, anytime I would go to the ER in pain, I would give the nurses a heads up that my veins were hard to get a successful IV started in. I know they hear that comment a lot, but they should just smirk and brush it off. It took eight tries one time before the nurse decided to get a vein finding machine. As she walked in with it, she said, “You weren’t lying when you said your veins were a hard get.”
“I’m often made to feel guilty. I’ve been asked why I don’t have a port if I’m such a hard stick. One time I was sent home from a scheduled treatment because the infusion nurse was so flustered that she couldn’t get a vein and I had “messed up her patient schedule” for the day. I found myself apologizing on the way out and now realize how wrong that entire situation was. The blame is usually placed on me for not hydrating properly.”
“I always tell them there is typically the most success in my hands and on several occasions the nurses in the ER will say “Oh well, this vein looks better, and I’m more comfortable doing this location.” This usually results in getting poked three times and blowing my veins and then finally trying my hand and being successful. When I tell phlebotomists or any of my surgery prep team, they take me seriously and usually use an instant heating pack to help and get it first try. They take their time and make sure they only do one stick. It’s really only nurses in the ER or Urgent Care settings who give pushback which is WILD because every time I’m admitted I am severely dehydrated so it’s going to be even harder than normal, and that’s basic knowledge nurses should have.”
“When I had a colonoscopy, the anesthesiologist poked me three times after I told her where my good vein was and she said out loud to the doctor, “Doc, your patient is telling me how to do my job!” Luckily, the doctor ignored her after he saw two blown veins.”
To disclose about “tough veins” or not to
“I warn everyone who is going to try and stick me. They usually try everything to get my veins to pop, sometimes it takes one try, other times it takes five. I can’t remember any nurses or phlebotomists giving me attitude, they usually try and make me laugh so that they don’t feel much pressure.”
“I do give them a heads up that I have thin veins and require the thinnest needle. I have certain veins that are more successful. I’ve allowed them two chances, but if it requires a third try, I request the best person they have. This can be super painful. I think it’s extra important to bring it up for colonoscopies when you’re dehydrated.”
“I’ve never had any issues when telling nurses or phlebotomists that I have bad veins. They’re usually happy I have told them because it makes it easier on them. I have decent veins, but they can roll and if I don’t mention it, more often not, it won’t be done right.”
“I’m a hard stick and after a recent 17-day hospitalization, I came home with SO many bruises and scars from IV’s and blood draws. Every IV infiltrated. I’m always outspoken about my veins and while some nurses believe me, I’ve faced pushback. Despite me telling them I know my veins and which ones are easier. The best part is when I’m right, my veins roll, and they miss and then they’re amazed because I told them so. The most resistance I’ve encountered as a patient has been with anesthesiologists—ego is often an issue. For a surgery in 2020, one was trying to place an IV and it hurt me immediately once it was in. So much so that I was crying. I asked him to remove it and try elsewhere and he refused. I had to ask for an attending doctor to step in.”
“I went in for an MRI and told them I had terrible veins and I’m a hard stick. The gentleman was kind and when he started to look for a vein said, “Oh, you actually DO have bad veins.” He said they often have patients tell them they have hard veins when they don’t. They called in the IV team, and it took them two tries.”
“I usually start by saying that they usually have a hard time getting it and I need to use a butterfly needle. I have been told several times that they know what they are doing and refuse to use butterfly needles. One time a needle was causing me such discomfort that I vomited. The nurse never apologized even though I had been pleading with her to take it out and try elsewhere.”
“I tell everyone I have baby veins that move and have been traumatized. I get a lot of pushback because most people think they are the one with the magic touch. I have a 2-stick rule before they must get the next best person.”
IBD hospital visit and infusion center horror stories
“The most common pushback is that the first person that tries sees it as a challenge. But not in a good way, in a prideful way. I had one guy refuse to let someone else try after 3 or 4 failed sticks and then made the executive decision that I would just orally hydrate with Gatorade in the ER…for dehydration. I also have had a lot of trouble with people not believing me when I tell them the IV has infiltrated. I was crying in pain from an infiltrated potassium IV. They didn’t believe me because potassium is known to burn. They were running it at the same time as iron and after a little while there was a stain in my arm from the iron.”
“I straight up told a nurse once she couldn’t poke me anymore because she blew all my veins and instead of getting someone else or getting an ultrasound machine, she just wrote, “Refusing Treatment” in my chart and I went over 12 hours without antibiotics until the resident intervened. “
“I have tiny veins and I’m a tough stick. Sometimes they have to move to a different spot and multiple times I have had someone else come in to try. My worst experience was during a scan with contrast dye. I told the woman repeatedly the needle was not in, and she wouldn’t listen. They put me in the machine, and I had to yell to the radiologist because I had a golf ball size lump on the back of my hand. She then started slapping it until it went down, which was incredibly painful, and I now have a small scar from it.”
“One time I warned a nurse when getting an infusion and she made a snarky comment that she’d been a nurse for 20 years. She injected Benadryl into my arm making it swollen and blue for days. I was crying and she told the doctor who was on call that she’s a “good nurse” and I was overreacting.”
“I once had to get stuck the week before my wedding 32 times. It took four nurses, anesthesia, and peds! I was so bruised the make up artist had to cover my bruises for my wedding and the photographer had to edit them out.”
“I usually have okay veins, but one time was sent for TB bloods before starting a new biologic. The abuse I got from the phlebotomist when they had difficulty getting a vein left me in tears.”
“I went to the same infusion center for 2 years and it was always the same two nurses. Every time I had to tell them about my fear of needles and tell them not to tell me what they were doing. I don’t even know how many times I cried there.”
“I’ve dealt with enough nurses at my infusion center and in the ER that I have ridiculous PTSD and anxiety when it comes to getting poked. I’m 42 and cry like I’m 4 when I get someone who doesn’t take my guidance about my best vein. What makes it extra frustrating is that I used to be a phlebotomist. I know firsthand patients know their bodies better than me and for both our sakes a one and done poke is worth everything.”
“After years and years of infertility and countless blood draws, I’ve seen too many nurses, medical assistants, and phlebotomists being rude and pushy. Everyone seems to “love a challenge” and sometimes their cockiness and attitude to never miss a vein make me their punching bag and experiment.”
“One nurse wouldn’t listen to me and keep rooting around. I told her she was going to blow my only good arm vein. We got into an argument, and she stormed out with the needle dangling out of my arm and my vein blown.”
Bringing out the IBD mama bears
“There is a nurse known for being good at inserting IVs at our Children’s Hospital’s Radiology department (i.e., for MRE’s). I learned this after a challenging IV my daughter experienced at her first MRE, when she was called in and I was told she was “the best at doing it.” With this knowledge, I immediately asked for her the second visit. I was dismissed and someone else spent 15 minutes trying to start an IV on my daughter, at which point the “good nurse” was called in to handle it. The experience was traumatizing for my daughter, and we now have to put off a necessary MRE because of this trauma. If/when we go back for the next MRE, I will not let anyone, but the “good nurse” touch her. We will up and leave if we have to, that’s how strong I feel about it.”
“As the mom of a VEO-IBD (Very Early Onset) IBD patient, we always ask for the PICC team and an anesthesiologist to start our daughter’s IVs. We always have to explain ourselves and get so much pushback each time. Everyone always thinks they can be the one to do it and it’s beyond frustrating. I don’t let any nurses see my daughter anymore unless it’s an extenuating circumstance.”
“The infusion nurse missed twice trying to start an IV for my daughter’s Remicade infusion. I was watching closely and not even sure she was going for a vein. My daughter is usually an easy stick! Easy to see veins and we focus on hydration prior to an infusion. Before the third stick, she asked ME where she should try next. I said how about getting another nurse or the IV team with ultrasound, if necessary. She became so offended, but I had a very nervous kiddo. The next nurse got it quickly without a problem. The first infusion nurse continued to give us attitude the rest of the appointment. I let the nurse manager know I did not want her caring for my daughter at any future appointments.”
“At my son’s second scope (He was 3 years old), I told the anesthesiologist that he’s a tough stick and does best in the right hand or arm. She half laughed and said, “It will be ok, Mom. We will get it.” When she returned the IV was in his foot and he had FOUR other band aids on him from failed attempts, none on his right arm or hand. She said, “You were right, he is a tough stick.” And walked away. We since have left that doctor because that was the only hospital with which he was associated. Now we go to an amazing Children’s hospital and have no complaints.”
Tips for getting through from the IBD family
“They’re always cocky and think they’ll get it. But I honestly find that warning them makes them look harder and they’re usually more successful if I give them a heads up. If I fail to give them a warning, it usually takes a few tries. I have had a specialist use the vein finder ultrasound once. It was super cool! He took one look and said, “Yup! Those are the veins of a Crohn’s patient.”
“I’ve been on Remicade since 2003 so needless to say my veins are shot. My best ones left are in my hands and I always say, “Sorry, my veins are tiny and collapse easily, but don’t worry I’m an easy patient so it’s ok if it takes a few tries. My hands are your best bet, but sometimes they have luck with xyz veins.” I can’t tell you how many times they say that the hand hurts more. As both a nurse and a patient, I know how important it is to advocate for yourself as the patient and listen to what your patient has to say.”
“One thing I’ve learned from several hospital stays is that when you get into the ER and they do the initial IV, make sure it is in a place that will work for a long stay. Not in the crux of your arm, but maybe the hand even though it hurts. That way you can maneuver it better in bed and when walking around the hospital corridors. “
“I have a routine that helps. I’ve been poked 5-7 times to start an IV or get blood. I’ve realized the more often I would say something, the more often they would miss (for a blood draw). For an IV, I started to communicate which vein to hit. Sometimes nurses resist and it sucks because you want the infusion so badly and you’re already nervous or have taken time off, gotten a sitter, and you start wondering if you won’t get your medication and if you’ll need to come back another time to do it all again. I usually take anxiety medication prior to infusions.”
“I truly believe if you go in saying “Oh my veins are easy, no problems here” it gives the nurse confidence! The only times I’ve had trouble are when I tell them I have tough veins. It psyches them out.”
“I always say to the person starting my IV, “I’m not doubting your skills, but the best place to access my veins are this vein and this vein, even though they don’t look promising.”
Perspective from and IBD patient + Healthcare Professional
Michelle Ladonne, 34, was diagnosed with Crohn’s disease in 2010. She’s also an Operations Manager of a large GI practice in Boston, so she sees both sides of the issue not only as a patient, but from the healthcare perspective.
“I am a tough stick and have had some horrible experiences (10+ sticks to get an IV, then having it infiltrate because it wasn’t fully in—so painful). But working in healthcare and managing nurses, medical assistants and phlebotomists who do this work every day, I also see the other side of things.”
Michelle says patients often come in and make comments like “you get one try” and “I can only be stuck in this particular vein,” which can be challenging for the nurse and phlebotomist.
“They’re trying hard for a safe and comfortable draw. My staff tries to listen to the patients’ experience and respect that they know their body better than we ever could. But also, the staff member is responsible for patient safety and if they can’t feel a particular vein or aren’t comfortable with a certain stick, they need to share that perspective politely and respectfully with the patient.”
She says patients can advocate for themselves, while also helping nurses and phlebotomists use their own judgement. For example, Michelle advises saying, “The vein in my antecubital (inside my elbow) looks like a good one, but there is a lot of scarred tissue there, so people usually have a hard time getting the IV all the way in. I tend to have better luck with a wrist or hand IV, but you know best!”-Luckily in the GI practice Michelle manages, several staff members and physicians have IBD.
“Our medical director of the IBD Center has had Crohn’s since he was a teenager, and it gives so much perspective in being able to see both sides of the issues. If it’s an elective blood draw or an infusion, hydrate, hydrate, hydrate! I chug my iced coffee before my Entyvio infusions to get my veins nice and plump. Not always possible clearly for patients coming in through the ER who are dehydrated and have been vomiting, but for elective draws, it’s a huge thing.”
In closing, it’s often a difficult balance when you’re in dire circumstances and the last thing you’re worried about is being polite or feeling the need to forgo your needs to appease a healthcare worker’s feelings. Speak up. As someone with a chronic illness, you are a professional patient. I always state from the beginning that I’ve had Crohn’s for 17 years, IBD gives you street cred for having strength. Make it clear you aren’t doubting their skills, but that you know your body best. Hydrate if you’re able, ask for heat packs to get your veins to perk up, inquire about the vein finder ultrasound, and put limitations on the number of sticks you’re willing to allow before it’s time for someone else to tap into the ring. This isn’t about not hurting feelings or being the “bad guy,” it’s about putting your wellbeing first and doing what you need to do to limit the possibility of another traumatic experience in your patient journey. Your trepidation is valid and justified, don’t let anyone tell you otherwise.
It’s been 6,207 days since my life changed forever. On July 23rd, 2005, I was diagnosed with Crohn’s disease at age 21. Since that time, I’ve evolved and changed in ways I may not have if it weren’t for my IBD. After living in silence with my condition while working in television news for a decade, I decided to use my love for storytelling and speaking to be the voice I needed to hear upon diagnosis as I navigated the many crossroads of young adulthood (finding love, a fulfilling career, and having a family).
July 23rd also marks the day I launched my blog, Lights, Camera, Crohn’s. Since 2016, I have shared fresh content, every single Monday (sometimes even twice a week!). 336 articles on my site alone. More than a quarter-million visitors and more than 387,000 views.
It’s been a labor of love and a mission project that continues to fill my cup and implore me to constantly want to learn more and shed light on topics that are often not talked about. Every day of every week since my blog began, I’m constantly thinking about story ideas, topics of interest, people to interview, ways to word content, images that are needed…the list goes on.
This photo was taken at a wedding July 23, 2016, right after I pressed “Publish” on the first Lights, Camera, Crohn’s article. I found out I was pregnant two days later.
The weekend I started my blog in 2016, I was one month into married life and found out days later I was pregnant with my first child. Since then, I am now a stay-at-home mom of three children (ages 5, 3, and 1). Life has gotten way more hectic and busier with each year that passes, but I’ve held tightly onto fulfilling my promise to the patient community, and to myself, to deliver new content each and every week. I’ve been organized through the years—often having an article written days before my Monday deadline, but this past year, with another baby added to the mix, it’s been more of a stress on me. I’ve spent many Sunday nights finishing my articles. At times it’s felt like a lot to juggle. I haven’t wanted to let anybody down, including myself. And I haven’t wanted my content to start lacking in any way.
Don’t worry, Lights, Camera, Crohn’s is not going anywhere
My blog has grown into more than I ever thought possible. It’s so rewarding to know my words have helped comfort and guide so many in the IBD community. I need to cut myself some slack and give you a heads up that moving forward there may not always be an article on Mondays. It pains me to say that, but at this point in my life, in this season of IBD motherhood, I need to start taking time to rest and relax. Since having my third baby last summer, I get my kids down for the night and START to work around 830 pm. It’s just constant. I truly rarely get a break. I’ve been in remission since August 2015, and I don’t want the stress to get the best of me.
You may not be aware—but my blog is only one aspect of my advocacy work. I also spend a great deal of time working with digital healthcare companies, patient-centered non-profit organizations, sitting on advisory boards and patient engagement teams, communicating with patients in need online and over the phone, and do freelancing work on the side, all without childcare.
I laugh as I write this because I already have three articles lined up for August…so there will be months where there IS an article every Monday. Just not always. My commitment and desire to serve as a patient leader is not waning in any way—I just want to be honest with you, my loyal readers, that this mama needs to lighten the load and take a little self-imposed stress off my shoulders.
I started contemplating this a few months ago, and almost changed my mind this week about sharing, but it’s time. We had an AMAZING 6-year streak of constant new content. I’m excited to see what this coming year brings in the way of patient stories, research, and perspectives. Having extra time to work on articles will really allow me to do more special reports and expand my “IBD Motherhood Unplugged” and “Patient Experience” series.
Thank you for giving me so much to talk and write about, always. There are endless topics that need to be brought to the forefront and I love providing a platform for others to share their journeys and experiences with the community. As always, please reach out if you have a story idea you want me to cover. Lights, Camera, Crohn’s has truly evolved from being a blog about my IBD experience to an award-winning and well-respected site that has highlighted hundreds of different patient stories and physician perspectives—and I love that. There’s no greater compliment then when I hear a gastroenterologist uses my blog to educate their patients.
Excited to see what 2022-2023 brings! Thanks for the love, support, and understanding and for making the first six years of Lights, Camera, Crohn’s what it was.
Love can be extra complicated to find, trust, and open yourself up to when you have IBD. This week on Lights, Camera, Crohn’s we hear from five different IBD couples (dating and married), but they aren’t your typical couples. In these cases, both partners have IBD.
Emily + Jason
Emily Geist and her husband, Jason, of Pennsylvania had an unusual diagnosis journey. Their children were surprisingly diagnosed before they were! Their oldest daughter was diagnosed with IBD in 2014 when she was four years old. Then a few months later, their middle daughter was diagnosed with IBD at just 21 months old. Through the process, Emily and her husband were asked if they had any family history of IBD and the answer was “no” at the time.
“Their diagnoses made my husband and I rethink the “sensitive stomachs” that we thought we had. We had previously talked with our health care providers, and no one thought of IBD, given our mild symptoms. Since I was pregnant with our third daughter when our second daughter was diagnosed, it took some time for me to see a GI and be diagnosed in 2016 with ulcerative colitis. My husband’s symptoms were more significant, and he ended up getting diagnosed with ulcerative colitis the same year as me.”
Emily says they were in shock after all four of them were diagnosed with IBD within a two-year period, not to mention having a newborn thrown into the mix!
“I joked that my husband and I were perfect for each other – so perfect we both had the same chronic disease and didn’t know it for the first 8 years of our marriage.”
She is grateful in a way for their delayed diagnoses as a couple, since passing along IBD when both partners have Crohn’s disease or ulcerative greatly increases.
“It was a blessing, in a way, that we had our family of three beautiful girls before we even knew we both had IBD. If my husband and I, and the two older girls had been diagnosed before I became pregnant with our third daughter, I am not sure what we would have done. And this thought hurts my heart, knowing the uniquely amazing kid we have in our third. We have watched our youngest so carefully for signs of IBD. Last fall, based on some very minor issues that might have been ignored in any other family, she had scopes and we found out she also has IBD at the age of six.”
Emily says Jason and her approach medical issues differently. He is calm, she’s a bit anxiety ridden. It’s always like that, right?!
“This works in my favor often as he can help calm me down. I lean hard on him during tough times. While we both have IBD, I think much of Jason’s empathy and support come from other health challenges he has faced. Jason was hospitalized as a teen for a (benign) sinus tumor and associated surgery. He also had cancer and underwent surgery and chemo for it. (We were married during his first round of chemo – but that is a whole other story!) He remembers what helped him in both of those situations and uses it to help our daughters and myself.”
Emily and Jason are on two different 5-ASA medications. Jason and two of the girls are on sulfasalazine, one daughter is on Remicade, another on Humira.
“There are two things I tell my girls: (1) Everyone has something…everyone has a challenge they work to overcome…and ours is IBD. (2) It takes intense pressure to create a diamond, we can deal with our ‘pressure’ and use it to become something rare and amazing.”
Amanda + David
Amanda Vogel moved to Colorado Springs in late August 2021. Two weeks after moving there, she started talking to a guy named David through a dating app. It just so happens they lived across the street from one another, so they planned to meet at a restaurant the following day.
“The day we were supposed to meet, he texted me and said he had to cancel our date due to “stomach issues.” I immediately thought to myself, “Hmm, I wonder if he has Crohn’s disease”? I brushed it off, we continued to text back and forth and made plans for that weekend. While we were texting, I made a joke about him canceling on me again and that’s when he told me he had Crohn’s disease. I was mind blown and told him how I have Crohn’s myself. I shared with him my blog post from March 2020 and felt an instant connection. We were both diagnosed with Crohn’s disease at age 13 and both have the same incision on our stomachs.”
Amanda couldn’t believe these incredible coincidences or the odds of their paths crossing.
“It’s mostly an understanding of each other’s dietary preferences, with some gentle encouragement to try things in moderation here and there. Also, a no-explanation-needed approach to random stomach stuff that can pop up anytime.”
While she says there is a “baseline” of empathy and understanding, which is amazing, it’s surprised her how differently IBD presents in each of them.
“The most surprising thing has been being so close to someone else with the same diagnosis but with very different day-to-day and long-term symptoms, medications, and little personal details of the whole patient experience. It’s helped me understand that one of the frustrations of IBD is how differently it can affect people, which can make it difficult for others to really understand. For me, that translates to empathy in the form of knowing Crohn’s can interject itself into our day whether we expect it or not and making sure to accept that without blame or guilt.”
These lovebirds joke about one day doing a “couples colonoscopy.” David is on Humira, and Amanda has an appointment in upcoming weeks with her new GI to discuss treatment plans moving forward.
“Anyone that would treat you like a burden due to a health problem that you’re doing your best to manage is not someone who deserves to be in a relationship with you. There are plenty of loving, understanding people out there, IBD-savvy or otherwise. Love yourself and the rest takes care of itself.”
Anika + Louis
Anika and her boyfriend, Louis, of Virginia, were friends for years before they officially started dating. They were out with friends one night and she mentioned she had ulcerative colitis. He replied that he did, too.
“When we started dating, I was less than a year into my diagnosis and I felt less alone when I found out he had it, too. Before I began my clinical journey to a diagnosis, I had never heard of UC let alone knew anyone under the age of 70 who had it. There are so many things that I assume I would have had to explain to a partner, that I didn’t have to explain to him because he had a similar experience.”
She says as long as they’ve been together neither of them has felt ill on the same day.
“It’s usually clear if one person is sicker than the other, so the less-sick individual takes more of the heavy lifting. I recently had to undergo a colonoscopy and without me asking he took off work so he could drive me to and from my appointment. He religiously read the prep materials the doctor had given me to make sure I took the right medication at the right time and even did all my prep shopping (buying me Jellos and Gatorades so I had prep friendly snacks). I think in general he’s an extremely empathetic person, but the fact that he can also relate is unbelievably nice.”
Both of these lovebirds take four mesalamine pills a day. They tease each other that if they forget their medication they can just borrow from the other person since they’re on the same prescription. She wants everyone with IBD to remember they are not a burden and deserve to be loved like everyone else.
“I don’t think you should ever think of yourself as a burden, and I know that’s a lot easier said than done. I believe that if someone loves you, like fully loves you, they will love you no matter what and be there to support you in anything you have to deal with. If someone shows early on that they are not compassionate or caring or can’t show up for you, then that’s a blessing that you found out early on and not when it’s too late. You deserve someone who loves you for all that you are.”
Brittany + Morgan
Brittany Wheaton and her boyfriend, Morgan, of British Columbia, both didn’t have IBD when their paths first crossed in 2018. Morgan was diagnosed with ulcerative colitis in 2013, but Brittany didn’t have answers for the symptoms she’d been experiencing since 2016. She says her boyfriend tends to be private about sharing about his ulcerative colitis, so he didn’t share his health situation with her until a few months after she had been diagnosed and he was sure they had a future.
“Since I was diagnosed while we were together, Morgan walked through the process with me and figured out the connection when he learned my new GI was his long-term GI! He didn’t grasp the connection between Crohn’s and UC right away as his awareness of his disease comes from his GI and doctor only – I’m more literate and curious about it!”
When it comes to having kids one day, Morgan has zero concerns. He’s confident that the medical supports are increasing every day and is excited about the prospects of new drugs and treatments if they are in the position of becoming parents to a child with IBD.
“He also reminds me regularly that we would be the greatest advocates and supporters to that child. We live in Canada, so we have the reassurance of universal healthcare which is such a privilege. I am more apprehensive about kids, particularly as I spent the past two years in a severe flare that I was worried might end my life. I struggle with the guilt of knowing I could pass these difficult experiences on by no ill-intention of my own. I also worry what pregnancy would be like on my body and have concerns around not being able to sustain a pregnancy due to my difficulties with nutrition. I also acknowledge that choosing to not have a child due to the risk of IBD can fringe on eugenics and is quite ableist.”
Brittany and Morgan often talk about how despite their IBD they have been fortunate to live beautiful, fulfilled lives and have gotten unique lessons and learnings about themselves and each other through their personal limitations.
“We choose to live in an apartment because we’d rather spend our healthy time having fun and relaxing rather than maintaining a stand-alone home; we’ve planned and started saving for retirement and periods off work at 29 and 34 because we know it’s likely inevitable; we have stringent boundaries around stress and taking on too much because the busyness isn’t worth the cost of our health; we have decided to do everything we can do to maximize our rest and fun, and minimize the stress of a too-full life because we know how fragile life really is, and have seen what is really important to us as IBD has taken it away before for periods of time.”
Brittany and Morgan place importance on being independent as patients but are grateful to have each other to understand the language of IBD and take advantage of having a partner who intuitively gets it.
“The day that we decided that we would be together for the long-haul, we committed to always putting our health first. Having a partner who understands that my physical and mental well-being and his physical and mental well-being need be our priority has provided such a rich and earnest connection without shame or guilt. It’s so beautiful to have a partner who encourages me to take care of myself rather than forcing his way in and trying to micromanage it for me. I feel empowered and trusted, and when I’m in a place where I need the external help, he’s always ready and waiting to step in.”
Brittany and Morgan are both on a 4-week cycle of Entyvio and the nurses at the clinic think it’s a hoot! Morgan is also on azathioprine. Since she was diagnosed while knowing Morgan, they both see the same GI.
“It was funny telling our doc because he (and pretty much everyone) suspects we must have met because of our conditions, but we just ignorantly both swiped right and found out the details later! Our general practitioners find it so interesting that we found each other and ask a lot of interpersonal questions about how we pull it off!!”
IBD is a part of who they are, and though Brittany is not thankful for the disease, she’s thankful for the lessons the IBD experience has brought them both. She says the emotional infrastructure of having IBD has made them better matches for each other!
Rebecca + Joey
When Rebecca Goodrich of California first met her husband, Joey, he opened up about having Crohn’s disease early on. At the time, she did not know she also had IBD. He candidly shared about his experiences with medication, flare ups, and traveling with Crohn’s. Rebecca was curious and eager to learn more about his patient journey, and at the time started to think she may be in denial about her own health.
“I knew what IBD was and was honored that he felt comfortable sharing his experiences with me. I was also so impressed with how determined Joey was to care for his body through healthy habits (sleep, hydration, meditation, etc.). When I was diagnosed, he was incredibly supportive—always reminding me through the tough moments that ‘this too shall pass’.”
She went on to say Joey has a way of keeping her grounded when she gets worked up about procedures or an uptick in symptoms. He takes Humira, she takes Lialda and Mesalamine enemas. Her current GI is Joey’s previous doctor.
“My advice for finding love with IBD is to be with someone who loves you for you. There’s no such thing as perfect, we all struggle with something. I am incredibly grateful to be married to someone who truly “gets it,” for my loyal Labrador Sherman-Shell, and for my family who has been there since the beginning.”
I can remember the moment vividly. Leaving a gastroenterologist appointment three months post-surgery and crying walking to get sushi with my husband on a chilly November day in the middle of the workday. When I walked into that clinic appointment, I was hopeful I would never need a biologic medicine again. We were planning to start trying for a family after our June wedding, but my doctor knocked me back to earth and told me my Crohn’s was too aggressive and I’d be setting myself up for disaster if I attempted going med-free.
The tears flowed. I felt like a failure. I worried about bringing babies into this world while on a heavy-duty drug and if my surgery would provide me with the remission I had never achieved the first ten years of having IBD. I was so upset my husband-to-be and I both called into work and took the rest of the day off. Over sushi we talked about our future family and my health. Everything seemed at our fingertips but out of reach at the same time. That was November 2015. Sometimes we don’t realize how far we’ve come unless we look in the rearview mirror.
Now July 2022, we’re gearing up to celebrate our third child’s first birthday (July 14). We had his first birthday party over the weekend. It’s been a surreal and incredible ride since that November day. I often find myself looking at my three children and still feeling surprised my body was able to create them and bring them safely into this world.
Knowing this is our last baby and the last “first” of everything is bittersweet and amazing all at once. I feel an immense sense of relief and comfort being at this stage and knowing I don’t need to count on my body to sustain life through pregnancy or breastfeeding anymore. I’ve made it an entire year exclusively breastfeeding and if you would have asked me if that would ever be possible a year ago, I would have said no way.
One of my fears is when my next flare will be and leaving my children for days on end while I’m in the hospital. While I know it’s a not a matter of if, but when, it puts me at ease that my children are almost out of the baby stage, and I can begin to explain my health struggles and why I may not always be like other moms. When my oldest was born I hoped to stay out of the hospital until he started walking. He starts kindergarten next month. I can only hope I stay flare-free until my other two are that old.
Learning as I went as a woman with IBD
When I think back to that November day and the tough love my GI professed, I’m so grateful I followed her lead and trusted her approach in managing my Crohn’s. Back then, I wasn’t a patient advocate. The only IBD mom I knew was my cousin’s wife. I navigated the waters of family planning and my first pregnancy all alone without much guidance. Each pregnancy I became more well versed on how to juggle IBD and family planning and everything that comes along with it, but I think back to how isolating and overwhelming it can feel when you dream of having a family, but don’t know how to make it happen when chronic illness is in the mix.
No one knows how their family will play out or if fertility or loss will be a part of their story. It’s sad how many women with IBD choose to be voluntary childless, not because they don’t want to be a mom, but because of the limitations of their IBD and overall well-being getting in the way. A day doesn’t go by that I don’t recognize how lucky I am that I “get” to be a mom. Not every day is wonderful, but even in the trenches as a stay-at-home IBD mom of three littles with almost no breaks, I do my best to remind myself of that day my husband and I got sushi and dreamed of living the life we are living today.
Take yourself back to the very first time you needed medical attention for your IBD (but didn’t know it yet). Close your eyes for a moment. Who was that person? Do you know them anymore? How have you changed and transformed since that life changing day?
I was diagnosed with Crohn’s disease July 23, 2005, at age 21. I was blindsided by a chronic illness after growing up as a literal picture of health. A three-sport, in shape athlete, who had never even had an ear infection or been to an emergency room. As a recent college graduate, my world flipped upside down as I struggled to find my way in the real world.
Now, 17 years later, I can tell you firsthand what I, you, and so many others have endured on our patient journeys and how each experience (even the mundane) serves as monumental touchpoints for gaining independence and confidence in making you a more empowered and direct patient.
Let me paint the picture clearly for you
The first time you bravely laid in an emergency room bed and every time there after—not knowing the tests, pokes and probs, and physical scrutiny you were about to go through.
How it feels to be wheeled by a stranger through stark hallways to CT scans, MREs, and scopes, wondering what the results will be on the other side and the repercussions for more medications, a longer hospital stay, or surgery.
The difference a couple months makes–pre-diagnosis in May 2005 and 2 months after 60 mg of prednisone a dayand 22 pills a day.
What it’s like when you say goodbye to loved ones and they roll you into the OR and you’re shaking like a leaf, all alone and feeling frail and broken, alone with your thoughts and prayers.
The number of moments you’ve watched nurses and even rapid response nurses fumble with IV’s try after IV try and when it’s been more than five, you find your voice from that point forward and start only giving medical professionals two tries before it’s on to the next.
How it feels at the butt crack of dawn when the world is sleeping and the hospital is bustling, waking you abruptly to get more vitals and more labs and you lay alone, haggard, frustrated, and delirious.
The moment when your GI has a heart to heart with you about starting a biologic and having to determine for yourself what route is your preference—infusion or self-injection. Would you rather sit for hours hooked up to an IV drip or sit on your couch with your kids looking on as you inflict pain on yourself.
The times you’ve sat up in the middle of the night wide awake thanks to the prednisone kicking in while the rest of your world is asleep wondering if you’ll ever regain some semblance of control of life.
What it’s like trying to eat meals inconspicuously with your family while they not so subtly watch each bite and every trip to the bathroom with sadness and worry in their eyes.
How it felt driving to a first date or a job interview and feeling like your IBD is a dark secret looming over the conversation and not knowing when to take down your walls and share.
Listening to your friends make comments about health and energy without considering what your experience with a chronic, debilitating illness may be like since you look well on the outside.
What it feels like to look at your reflection in the hospital bathroom. Battered arms, sunken in eyes, a shell of who you used to be. But as soon as you walk out of the door, putting a soft smile on to protect your visitors from worry.
What it’s like to sit on an airplane or be on a road trip with others and silently worrying about whether you’ll be able to make it and what your game plan will be.
When you’re up in the middle of the night doing the second half of colonoscopy prep and wondering ‘why me’ in your 20s and 30s, feeling isolated in the physical, mental, and emotional anguish the process puts you through year after year.
What you’ve internalized each time someone dumbs down your IBD, offers up ridiculous remedies or goes into a discourse about their aunt’s brother’s cousin who “healed” their Crohn’s this way.
When you’ve waved the white flag and alerted family and friends that you needed help or to be seen in the hospital after doing as much fighting as you could against your own body.
The first time you bravely looked down at your incision and saw your body forever changed and came to see your scars as battle wounds.
Waking up each day not knowing what the next 10 minutes will feel like for you and getting after it anyway.
Not knowing if you’ll find your person, but meeting people and having the courage to share about your health issues, even if there are heartbreaks and disappointments along the way.
Deciding to have a baby and discussing family planning, despite all the what ifs and becoming a parent because that’s what you hoped for prior to your IBD.
Landing that dream job with your IBD in your back pocket, not letting the detours stop you from finding the path you were meant to go on.
Celebrate the independence you’ve discovered
The list goes on and on! No matter how old you are when diagnosed with IBD, in that moment we are robbed of our naivety and thoughts of invincibility, and we’re forced to go on a lifelong war and conquest. Our bodies no longer feel like ours. Our dreams feel in disarray. Our people may change and not be who you thought they were. Our hearts may break, but like a phoenix this disease can build you up just as much as it breaks you down.
The reprieve of remission, while not perfect or without symptoms has enabled me to breathe and regain my grounding. In 2015, after three back-to-back bowel obstructions and 18 inches of my small intestine, Meckel’s diverticulum, and appendix removed, there was only one way to go and that was up.
Give yourself grace. Celebrate the independence you’ve discovered that you may not be able to have realized until you’re years out like it took me. And when you’re in the hospital, in for a routine clinic visit or for labs, taking your meds and balancing every daily decision against how it will make your IBD feel, you’ll come to realize what you take on and all you accomplish every day just to survive and thrive, makes you something special. While you may feel dependent on others—and the support of caretakers and a support system can’t be understated, neither can the endless strength that lies within you.