When you hear the term “pay it forward” you may envision someone in a drive thru line surprising the person behind them by covering their order. Those words have held a different meaning for me as a person with IBD. When I had bowel resection surgery, I’ll always remember how my husband’s cousin and wife surprised us and showed up to the hospital with coolers of food and drink for my immediate family. It was an act of kindness and generosity that meant so much. That was six years ago, and we still talk about it.
Fast forward to present day and a friend of mine locally who has battled Crohn’s disease for decades had surgery. He’s a husband, a father of four, a successful businessperson, and leads our local Crohn’s and Colitis chapter as President of the Board. Through the years my husband and I have connected with him and his wife at Foundation events.
Staying connected through the pandemic
He recently posted on Facebook that he would be having his 8th Crohn’s-related surgery. He’s taken on Crohn’s with resilience and grit since being diagnosed more than 21 years ago. Thanks to the pandemic, the last time we had seen him, and his wife, was at the Crohn’s and Colitis Foundation Gala in November 2019. Despite two years passing without seeing one another in person, there’s something special about the IBD community and the family feel it creates.
When you’re knocked down by a disease over and over again and you’ve had surgery, you’re able to relate to the struggle, while also understanding how beautifully amazing recovery can be when you get a fresh start. While surgery is not a cure, it affords many of us with the opportunity to stay ahead of our disease and take out the portion of our intestine that is diseased and causing us problems.
A call to help
After I saw the social media post giving friends and family a heads up of the surgery happening in two weeks I grabbed my day planner and marked my calendar so I could be reminded of when to reach out to my friend in the days ahead, to pray, and to start thinking of how I could help his family of six during this uncertain and challenging time.
I immediately thought about his sweet wife trying to steer the proverbial ship for the family for months on end. Four young mouths to feed. I texted them both and said I would be bringing over a homemade meal. My text may have seemed out of left field, but I wanted them to feel supported and help in a way that doesn’t seem like a big deal, but has a lasting impact. Rather than asking how you can help, if you can help, or that “you are there if they need anything,” just come right out and say what you are going to do.
We picked a day for me to stop by with a homemade dinner and when we saw one another and were able to chat for a few minutes in person it warmed my heart. I could tell the gesture was so appreciated and that it brightened their day as much as it did mine. We all know how monotonous recovery can be, so having someone stop by—even for a few minutes—helps break up the boredom.
Hanging out at the Crohn’s and Colitis Foundation Gala in 2019. As my friend endures his recovery and now another surgery on the horizon, it’s friendships like this that deserve extra thought and care.
Passing along the appreciation
Fast forward to this week and while I was feeding my baby, an email popped up on my phone from a friend of mine in the patient advocacy space. She wrote:
“Dear Natalie,
Thank you for your tireless dedication to the patient community that you serve. I am deeply grateful for the opportunity to work with you, and always appreciate your willingness to jump in and help my clients transform healthcare. Patient Authentic wouldn’t run without you! Please accept this gift as a small token of my appreciation for your commitment to making the world a better place and your support throughout this past year. Wishing you a wonderful holiday season and a joyful new year!”
This was such a sweet surprise and brought me back to this notion of “paying it forward” in the patient community and going out of your way to brighten someone’s day. When you live with chronic illness, and never know what the day will bring, it’s wonderful to have moments of reprieve where you feel thought about, appreciated, and seen for all that you endure and all that you go through.
Paying it forward to someone with IBD this holiday season and beyond
It’s not about the monetary value, but rather the effort and thought.
Send a card expressing how you are thinking or praying for someone, rooting them on, supporting them through the ups and downs their disease creates.
Offer to help watch the kids so they can have an hour to take a walk, run an errand, or just relax.
Ask if you can join them for a doctor appointment, to get lab work, go to an infusion, be there at their home when they do an injection—anything to be there as a source of support. I recognize with COVID you may not always be allowed, but it’s worth an ask. By doing a “ride-a-long” with a friend or family member, you’ll get a small taste of what their reality is like. It’s often the drive to and from appointments and procedures that makes our minds race and can get emotional.
A simple “tell me about how your Crohn’s has been?” or “how has Crohn’s been impacting your day to day?”…or “what is it like to live with Crohn’s?” means a lot…don’t waste your breath only asking “how are you?”…because most people with chronic illness take this as an opportunity to downplay their struggles or sugarcoat the reality. Dig deeper and ask empathic questions that show you really care.
Share content of fellow advocates on social media—whether it’s a blog, a podcast, a reel, a post on Instagram—being a patient advocate takes a lot of time and effort, it’s rewarding when you see your words and your work reach more people and even better when you learn how a story you wrote or a post you shared touched another person’s life and impacted them in a positive way.
Over the weekend a fellow IBD mom friend of mine was hospitalized from a flare and faced with the need to start a biologic. When she got home with her family last night, she sent me an email with an update and ended it by saying “thank you” for being a mentor/friend/support in her corner. It’s moments like this that validate why I do, what I do.
Overwhelmed. Terrified. Unsure. When Heather Hausenblas’ son, Tommy, was diagnosed with Crohn’s disease December 6, 2018 at age 16, she didn’t even know what IBD stood for. She knew she had a lot to learn and was on a mission to get her son healthy. Fast forward three years and now she’s a published author on the topic.
“Invisible Illness” chronicles how it feels from a parent’s perspective when your teenage child is diagnosed with a chronic illness for which there is no cure. The book provides an inside look at a mother struggling to find her way forward and how she turned despair into hope not only for herself, but for her entire family.
Heather Hausenblas, PhD, is a mother of three boys, health psychology expert, and award-winning researcher. She says when her eldest son was diagnosed with Crohn’s, her personal and professional roles collided. Not only was she going to battle for her child, but she also began her mission to help those with chronic illness eliminate the overwhelm and (re)discover health.
Dealing with the words chronic and incurable
“I kept hearing there was no cure, no known cause, no one treatment, and no one symptom. No. No. No. No. He will always have it. It’s never going away,” writes Hausenblas in her book.
Chronic and incurable-these two words were exploding in Heather’s mind on repeat. Tommy went from being on the high school baseball team, with lots of friends, doing well in school, and being very active…to living with a complicated and often debilitating disease. Everything in their life came to an abrupt halt. She explains how the illusion of youthful invincibility began to fade. Something anyone in our community can relate to. Health is often taken for granted until it is robbed away from you.
Feeling helpless through the struggles
She writes, “I could hear the pain in Tommy’s voice. But I was helpless. To put his excruciating pain in perspective, one Crohn’s patient described it as, “I’ve given birth without an epidural twice in my life, and the pain of Crohn’s disease was far worse than that.” “Tommy’s physical agony was accompanied by the unending frustration involved in trying to diagnose this complex disease. His symptoms and complaints had been overlooked—even dismissed.”
When a child or parent is diagnosed with IBD it impacts not only the person with Crohn’s or ulcerative colitis, but each family member in a unique way. It’s often said that IBD is a “family” disease.
“Torture was seeing my child wasting away to a skeleton, dropping nearly twenty pounds on his already lean frame, constantly running to the bathroom, and having excruciating pain. Torture was watching him leave the house only to run back seconds later for the bathroom while his friends went to the party.”
As a mom with Crohn’s myself, reading Heather’s perspective as the parent watching her son endure pain and hardships struck a chord with me because when you’re a young patient and are diagnosed before becoming a parent yourself, you often don’t take the time to think about how your disease and struggles are impacting the people who love you most. Not out of disregard, but simply because you are dealing with so much internally and externally it can be difficult to think outside of yourself.
Healing with food
While Heather shares a great deal of insight about the importance of diet and nutrition as it relates to IBD throughout the book, she also talks about the challenges Crohn’s presents since each person tolerates food differently. She explains how it’s impossible to find a one-size-fits-all diet but advises patients to journal everything from what they eat to how often they go to the bathroom to try and tailor a personal diet that works for you. Discovering your own triggers and knowing which foods are risky or tend to cause pain is a huge step in managing your illness.
“After a few weeks of strictly following the SCD (Specific Carbohydrate) diet, Tommy said that gluten wasn’t his issue. He somehow knew. He knew his body. He now eats gluten when he wants…Tommy’s liberalization of the SCD highlights the practical concern of adhering to a very restrictive diet.”
“Invisible Illness” includes 30 pages of helpful inflammation-fighting recipes. Throughout the book Heather talks about how she “detoxed and decluttered” her home and the cathartic effect journaling had on her coping process then and now.
Now, as a sophomore at Clemson University studying engineering, Tommy is in remission and does not take medication. He manages his Crohn’s by eating a healthy diet made up of organic, whole food, has an active lifestyle, and says his Crohn’s disease does not define who he is.
Forming connections and offering hope
Heather hopes that by candidly sharing her family’s journey with IBD that she opens the door for connections between other parents and families living the same reality. She recommends fellow parents to get involved with local organizations, so you recognize from the get-go that you are not alone.
Her main goal with publishing “Invisible Illness” was to “to help others navigate through the storm of medical and health information to figure out the right wellness path.”
How to purchase “Invisible Illness”
You can get your hands on a book by ordering a copy on Amazon.
Work life balance takes on a whole new meaning when you have chronic illness. Molly Dunham-Friel can attest to that. Diagnosed in 2012 with ulcerative colitis, one year after receiving her undergraduate degree, Molly was forced to begin her professional career with unexpected titles she was just getting accustomed to—IBD and IBS. Molly remains just as ambitious and aspirational as she was prior to her diagnosis, but undoubtedly has experienced common roadblocks that come along with living with chronic health conditions. While the career detours were not always welcome, the experiences Molly has had over the last nine years blossomed into finding what she is truly passionate about.
This week on Light’s Camera Crohn’s we take a close look at having IBD in the workplace, whether you work in an office or at home.
Quite the Go-Getter
While IBD is unpredictable, one constant in Molly’s life has always been her go-getter attitude. She tells me she’s been known to work multiple jobs since the age of 15.
“I am not very good at slowing down and I get frustrated when anything gets in my way, including being chronically ill. The one professional aspiration that I have always held is my drive to help people in need, the marginalized, the forgotten, the invisible, the ones who truly need my help.”
Since her ulcerative colitis and IBS diagnoses, Molly has worked full-time, while often holding additional part-time jobs. At one point she was working five jobs, simply to pay for her healthcare costs! Molly says life got more complicated and extremely overwhelming once she turned 26 and could no longer be on her parents’ medical insurance
“It was stressful and defeating because now I had added pressure to hold a job that provided me with affordable medical insurance to get the care I need as a chronic illness patient. IBD is extremely expensive to manage due to the medication, procedures, doctors’ visits, labs, you name it, it costs a lot. This felt heavy as a 26-year-old still learning how the world works and how I wanted to make the world a better place.”
Molly has had to leave jobs she enjoyed to go to companies with better benefits, which also came with less satisfaction.
“I have been stuck in jobs solely because I needed the cost controlling benefits the organization offered. I have had to say no or not apply to amazing jobs and organizations because the benefits would not cover my chronic illness needs enough where I could afford it. I feel like my health insurance needs as a chronic illness warrior trump my career aspirations, which feels suffocating and leaves me frustrated. I want to do what brings me joy and not just what brings me healthcare coverage.”
New purpose, new goals
After starting her blog, Better Bellies by Molly, beginning to volunteer with the Crohn’s & Colitis Foundation, and connecting with amazing warriors via social media. Molly realized her passion for helping to support the IBD community.
“My goal is to support, educate and empower chronic illness patients, particularly those living with IBD and IBS, so they don’t feel alone, like I did upon my diagnosis. I am also passionate about helping patients feel empowered to advocate for their health. I haven’t figured out how I will turn this into my career, but blogging and social media is a great start!”
Advice for those with chronic illness nervous about working
There is no sugar coating how hard and demanding it is to work full-time on top of the full-time job of managing chronic illness life. Here is Molly’s advice:
No job is worth your health. Put your health first whenever you can.
Know your rights. IBD and IBS are both conditions listed in the American Disability Act. If you are discriminated against due to your IBD or IBS, speak to someone you trust to fight for your rights. Depending on the organization, employees with disabilities can submit formal paperwork to receive reasonable accommodation, which is any modification or adjustment to a job. Like most things with chronic illness, there is a lot of paperwork involved, but reasonable accommodation is one mechanism to look into in addition to going to HR and asking what other accommodations your employer offers.
Who you work for matters. Having an empathetic and compassionate boss and supervisor makes working full-time while chronically ill more enjoyable.
Disclose what you wish to disclose when you wish to disclose it. I currently find disclosing my disability status/medical conditions helpful so that my leadership can support me, but it took me six years to get to this level of confidence speaking about my chronic illness life. Give yourself time and grace. I have not always been met with compassion and understanding so follow your intuition and share when you feel ready. I have only held two jobs in the last 10 years where my diagnosis was discussed prior to being hired and onboarded and one of those times it was because my diagnosis related directly to the work and the other was because my advocate work made its way onto my professional resume and after sharing my story online and growing comfortable talking about it.
The more flexibility the better! Ask about work life balance ahead of time. It is especially hard to work an 8:30-5 job which a chronic illness because work hours directly conflict with when doctors’ offices are open and operating. Most medical facilities outside of hospitals are not open for routine or diagnostic care on nights and weekends so the more flexibility your work will allow, the better.
Follow your passion, even if you must detour. I have had so many career detours due to my health insurance needs and flare-ups, but I have never stopped pursing my passion for helping others, even if that meant starting something of my own outside of my full-time work.
Working full time is hard, working fulltime while chronically ill is harder. Juggling work alongside appointments, sick leave, flexible scheduling, and economical health benefits can be overwhelming. These can be hard to find, but as chronic illness patients we are no stranger to doing hard things.
The new perception of working from home
The pandemic has helped companies, organizations, agencies, managers, supervisors, and senior leaders recognize that so much can be accomplished and in many instances that more can be accomplished, by working from home, teleworking more often, and commuting less. It’s not surprising that companies that have pivoted into a more flexible scheduling system will be more likely to retain top talent, including us chronic illness warriors!
“I wish it didn’t take a global pandemic to teach the world that we can work from anywhere, that we can be trusted as employees and that yes more flexibility might actually make us better employees. I think the perception of working from home has drastically shifted and is no longer viewed as an “easy way out” or something that will lead to employee’s “slacking off.” However, I have realized that while many companies and leaders have made this shift, not everyone has and that there is still much room for improvement.”
Working from home benefits patients with IBD and IBS by:
Being able to use our own bathrooms, with our preferred toilet paper and easy access. No longer fearing if the bathroom is occupied when the moment hits.
Not commuting lowers stress and gives us back the time it takes to travel back and forth each day.
Being able to work while feeling ill is easier when in the comfort of your own home, with your blankets, heating pad and supplies to help keep your body as comfortable as possible, while also getting work done. Many times, this would not be possible in an office setting.
Leaving the house can be anxiety producing for those with IBD and IBS due to the often very sudden need to use the restroom. Being able to work from home can diminish that fear.
Having access and privacy for administering medications throughout the workday is easier done at home.
Allowing flexibility to work around doctor appointments, infusions, lab work, procedures, you name it.
Breaching the subject with a boss or superior
Much like the stress surrounding when to tell a love interest about your health conditions, knowing when to the tell a boss you have IBD can be worrisome as well.
Here are Molly’s tips for approaching the subject:
Unless an emergency is forcing you to disclose your condition, I recommend sharing when you feel comfortable to do so.
Begin by asking if they know what your condition is “Have you ever heard of IBD? Do you know what IBD is?”
Based on their answer, follow-up with education and explaining how your condition impacts your life.
A good supervisor will ask you how they can support you. Be prepared to ask them for what you need which might be a flexible schedule or understanding that your illness is invisible, and you are in fact a motivated and loyal employee.
Sharing is not for everyone, but you might be surprised who else at work is dealing with a chronic illness, bosses included.
IBD Wins in the Working World
*Having bosses who support you personally and professionally lowers stress which supports optimizing mental and physical health.
*Finding ways to unwind—whether it’s exercising, taking Epsom salt baths, or going to therapy.
*Use each professional experience to help shed light on where your passions lie. You’re constantly learning what you like, what you don’t like, and each experience helps to inform the direction your career will take.
*Celebrate all the wins—large and small.
*Be mindful of how your employer handles a hospitalization, flare up, or surgery. It’s telling to see how your work family supports you or doesn’t in times of need. Your health should always be the top priority.
*While chronic illness may hijack where you thought you would be in your career, it may help dictate what you enjoy doing.
“As chronically ill workers we need to voice our needs and push for systems to change so that we can break down barriers, make working more accessible to the chronic illness community, and to obtain and retain talented chronic illness employees.”
Key Takeaways
It won’t be easy, but you can do it!
Feel empowered to stand up for yourself.
You deserve to be accommodated in the workplace and it is not a weakness to have a disability or need special needs.
Chronically ill people belong in the workforce.
You can still achieve your dreams after diagnosis, they might just look different.
Your career path might not go according to plan, and that is ok.
Follow your passion and heart whenever possible.
Working full time isn’t the answer for everyone.
Give yourself grace.
No job is worth your health.
If a job is making you sicker due to stress, toxic environment, or lack of flexibility, work towards changing that situation.
Your aspirations, dreams, goals, and plans will shift over time. Honor where you are and how far you have come!
Less than one percent of the world’s population has it. I’m talking about Infantile VEO-IBD, or “Very Early Onset” IBD. What’s that you may wonder? It’s a rare and often fatal subset of Crohn’s disease that impacts children ages two and under. This week we hear from a mom whose daughter Riley was diagnosed with Infantile VEO-IBD as a newborn, she’s now 18 months. During her first year of life, Riley spent 27 weeks in the hospital. Jana Gilkey opens up candidly about what it’s like to be this type of IBD mom, what she wants others to know about her daughter’s patient journey, and how you can best support families with medically complex children.
Clinical characteristics of Infantile IBD are different from those of an adolescent or adult-onset case with features that are more aggressive & rapidly progressive. There is no known treatment plan and no known cure. Much of the treatment and therapies available are considered research and trial based and are not currently approved by the FDA due to the young age of those diagnosed.
Jana says she could tell something was off from the moment Riley was born. At first as an exclusively pumping mama, she thought her daughter had a dairy intolerance, so she cut every common allergen from her diet.
“We saw our first pediatric gastroenterologist when Riley was one month old. As a mom, my intuition was screaming at me that something was terribly wrong. We saw a few different pediatric gastroenterologists and by month two of life, her symptoms had only progressed. By the time she was 3 months old, she was not stable enough to stay home and had completely stopped eating by mouth. What little we could get her to eat, she was unable to keep down. She was diagnosed with failure to thrive and rapidly declining on all accounts.”
Riley was hospitalized for the next three months. Every day brought new symptoms and complications. She had been evaluated for every condition and received her first PICC Line in which she received continuous TPN & Lipids due to not tolerating any kind of substance in her stomach. Riley also received a series of blood, iron, and albumin transfusions.
Receiving the Infantile VEO-IBD diagnosis
An upper and lower endoscopy revealed lesions throughout Riley’s entire GI Tract. Bingo.
“I began to scour the internet on anything and everything I could find on Infantile VEO-IBD. There was a white board in our hospital room. I wrote down everything I could find on that board. I drew myself diagrams and made notes on doctors to try and connect with. I recorded nearly every second of my daughter’s day those 3 months of our first hospital stay. I ordered books and searched and listened to every podcast I could find on children diagnosed with autoimmune diseases in the first few months of life. I fell asleep most nights watching YouTube videos on nearly every kind topic you can imagine regarding genetics, the immune system, how the body processes monosaccharides, how the brain communicates to the GI tract, and everything else in between I could find to better understand, educate, and advocate for my daughter.”
Like anyone with IBD can relate to—the unpredictability and uniqueness of each person’s experience with IBD makes a diagnosis extremely challenging to cope with.
“While all of my research and studies have been vital to my education and understanding, the very best education (and support) we have received has been from those who also walked a similar journey battling Infantile VEO-IBD.”
How it feels to watch your baby fight a chronic illness
The way Jana describes what it’s like to be a mom watching your child fight an uphill battle against their health had me crying. She explains her experience and perspective so beautifully, yet it’s heart-wrenching to read.
“Most of the time it feels like frantically trying to catch little fireflies that show a glimmer of themselves and then seem to disappear just before jarring them all up. Impossible to fix and yet, aren’t good moms supposed to fix things for their babies? It feels like trying to catch water in the cup of your hands. It just keeps slipping through, no matter how tightly you squeeze. To me, watching my daughter endure such chronic pain and struggle, feels like a constant dance between surrender and war.”
You can feel the pain and the love in her words.
“When Riley was first diagnosed. I was ready to fight, on a mission to find a cure, fly her anywhere, climb the highest mountain, swim to the bottom of the ocean to find that one special pearl that could bring her healing. I believed (and still believe) that the healing remedy for her is out there. However, I have since come to terms that the journey we are on is not a sprint. It is a marathon. I surrender to the things which I cannot control or change. But I will never stop fighting for better. I am willing to run this marathon for the rest of my life so that, Lord willing, my daughter or maybe even those that come after her don’t have to.”
How IBD has “given” to Jana’s family more than it’s taken
Jana says Riley’s disease has changed everything about her outlook on health and her overall perspective on life in general.
“I believe it has given to our family more than it has taken. Riley’s battle with Crohn’s Disease may have robbed us of nearly all of her first year of life on what “could have been.’’ However, it has given us as a family the opportunity to choose what is and what can be. We have been given the opportunity to choose joy during uncertainty and at times chaos.”
Through the pain and tears Jana has realized that we do not own our health but steward it.
Photo cred: Alisha Gilkey
She says, “health is not ours to claim but to honor and look after. While it may at times feel as if I have somehow failed my daughter’s health, this is not true. I have honored it with all it has brought. It was never within my control to begin with. I believe the same is true for others within the chronic illness world. There is a lot of room for grace here.”
A life-threatening setback
Riley recently was unable to absorb any nutrients in her GI tract. She started refusing to take anything by mouth and was provided nutrients intravenously through a catheter in her chest the first 10 months after her initial Infantile VEO-IBD diagnosis. The hope—once the right combination of medications was found to wrangle Riley’s disease under control that a gastrostomy tube (g-tube) could be placed.
“One of the many risks of living life with a central line can be infection of the blood. Riley was at high risk for infections due to the medications she was receiving for treatment in addition to being immunocompromised. Unfortunately, Riley developed a blood infection on three different occasions and one put her body in a state of shock.”
Jana says thanks to the grace of God, Riley recovered and does not have any known organ damage at this time. The last four months she’s been home and started to tolerate food in her GI tract. She’s completely weaned from being fed through her veins!
Photo cred: Alisha Gilkey
“While we are still searching and longing to find remission for her, she is able to finally have a little more freedom to be the toddler she is. We still have some hard days, but we do feel hopeful we are on the path to remission and will soon see her body heal. Each day that she feels better, we see more of her personality. It is so fun to finally get to know her and see her able to explore more of her world!”
Treating and managing Infantile VEO-IBD
In her 18 months of life, Riley has been on a laundry list of medications and treatments and endured countless procedures and surgeries.
Medications/Treatments
Proton Pump Inhibitors
Liquid, Topical, & Inhaled Corticosteroids
Biologics
Chemotherapy Trails
Glycopeptide Antibiotics
Additional Daily Dietary Supplements
TPN & Lipids
Surgeries:
Multiple Invasive & Non-Invasive Diagnostic Tests and Scopes
Gastronomy Tube Placement
Catheter Placements & Removals
Riley becomes a big sis
This past August Riley became a big sister to Josephine. Since Riley’s health has not been stable enough to travel or be around people because of the pandemic, Jana is FINALLY able to travel back home for the holidays with her family of four. Many of their loved ones met both daughters for the first time this past week at Thanksgiving. Jana says while the lows of Crohn’s disease have been really low, it makes the highs feel that much higher. As she juggles life with a medically challenged child and a healthy child alongside her husband, she’s trying her best to enjoy being a “mom” instead of solely a caretaker.
Photo cred: Alisha Gilkey
“While it is very busy, I will say, that in a way my second born has helped us all to take a breather as a family. It’s helped to remind me that I am their mother still and more than a caretaker to both of them. Up until recently, our life has been about keeping Riley here with us. Thankfully, she is in a much better place, and I can also focus on raising her and her baby sister together! This would all be so much more tough without our wonderful support system we have. My husband is unbelievably helpful in addition to my own mother who has been with us every step of the way in this journey.”
Jana says having tangible support is a huge stress relief. By tangible she means, physical help with chores around the house like doing dishes, the laundry, and even having family members learn how to manage a g-tube so her and her husband can take a nap every now and then.
Photo cred: Alisha Gilkey
“None of it is how I envisioned our life going and it sure isn’t perfect, but I would not trade either of my girls for one second. I believe every child comes to the world at the time they are destined to come. I know they are meant to be here at the time they are and together.”
How IBD has impacted motherhood from a parent perspective
Jana says she no longer looks forward to the expectations she may have had for her children. Instead, she looks forward to watching whatever they choose to paint the canvas in front of them.
“It’s actually so much more exciting to not have expectations, just enjoying what I can from each day with them, and on the edge of my seat to cheer them on in whatever they do. They are God’s children, and it is a great honor and challenge for me to be able to steward them well. I trust He will fight for them and will always be with them even when I can’t.”
The journey over the past 18 months has helped Jana gain a better understanding of fellow moms as well.
“What may be best for one family may not be best for the next and that is something to celebrate really – not be judgmental or weary of. Moms have way too much on their backs to place any judgement. The children we have been given were given to each of us as individuals for a reason and no one else. There is no longer room for guilt or judgement here, just grace and support.”
Best ways to support families with medically complex children
When loved ones and friends go through health hardships, we often want to help in some way. But unbeknownst to us some of the ways we approach the conversations can be off-putting without even realizing it. Jana says knowing so many people (many whom they have never met) are praying for Riley, interested in her journey, and supporting them, has been incredibly overwhelming.
“I met so many truly inspiring families and individuals over the last year and a half since Riley’s diagnosis. Sometimes, it can be exhausting to share our story, as there is so much to explain. But, each time I share, I am reminded that we are not alone in this. That is really a huge encouragement when times have felt isolating.”
Photo cred: Alisha Gilkey
Jana has come to realize that when it comes to health and those walking through a medical journey, that what we may know or what they choose to share about their story is often just the tip of the iceberg to what they are going through.
“Offer grace, not judgement. Offer time, not advice. People genuinely mean it when they say, “Let me know how I can help.” These questions are well meaning but they put the ball in the court of the person who may be enduring rather than the one seeking to support. It’s often difficult to understand what your own needs may be when in seasons of crisis.”
Instead seek to understand. While it feels natural to ask questions like, “Are you/they feeling better?, “How was your day?”, or “What can I do to help?” These types of questions can feel broad and difficult to answer in the world of chronic illness.
Jana recommends asking questions to seek understanding. She says asking the right questions can be helpful for those we want to support.
Here are some examples:
Can you tell me about your day today?
I spent some time researching the diagnosis you shared with me, and I have a few questions…would you mind if I asked you so I can better understand what it looks like for you?
I would like to know more about what the days look like for you. Would you like to share?
How does your daughter’s diagnosis and patient journey affect you?
Want to do something spontaneous, without asking? Go for it. Deliver a meal, write a letter, offer your time in a way that does not require a friend who may be in crisis to ask things of you. Pain can often feel like a burden and be very isolating. Having someone ask to better understand and invite themselves into our pain helps to lift that burden – just knowing someone else sees.
When she’s not on the runway during Fashion Week or gracing magazines, Keyla is doing all she can to be an advocate for IBD. She was diagnosed with ulcerative colitis eight years ago, but this year, she found out she has Crohn’s disease.
“As a child, I always had intense stomach aches, and difficulty going to the restroom. Sometimes I’d even pass out. Doctors always told me it was constipation. It wasn’t until I was at work one day and passed out that my boss convinced me that I needed additional medical attention.”
At that point, Keyla was having 8-10 bloody bowel movements a day. Prior to ulcerative colitis, she was diagnosed with celiac disease and went on a strict gluten free diet. But unfortunately, the symptoms persisted. She got a second opinion and that’s when she was diagnosed with IBD. Keyla recalls that in the beginning moments of her patient journey she struggled to grasp that chronic illness meant her disease was a “lifelong partner” and that IBD would change her life in unimaginable ways.
The journey to an ileostomy
Fast forward two years after her IBD diagnosis and Keyla rushed to the hospital after noticing unexplained bleeding. Turns out she was hemorrhaging from her uterus and was told she had uterine cancer.
“After having a partial hysterectomy and no longer being able to have children, I’m not sure if it was the stress from everything happening but my UC was never able to be controlled after that. From failed medications like Methotrexate and Remicade to looking like Quasimodo from eye swelling caused by Entyvio and having less hair than a toddler from being on Humira. My body and I had enough. My clinical team and I decided it was time to evict my colon.”
In September 2018, Keyla began her 2-phase j-pouch procedure. Unfortunately, the surgeon discovered her colon was much more diseased than he had thought. Keyla’s colon had become fused to her stomach, resulting in part of her stomach to be removed as well.
“For 2 months I felt amazing with my ostomy and was excited for my reversal in December 2018. But shortly after, I began developing chronic pouchitis, could not gain weight, required IV fluids regularly, with a failed midline and then needed a central line. We decided to disconnect my j-pouch and create my end ileostomy in September 2020.”
All was well until January 2021 when Keyla started bleeding from her ileostomy. It was at this point she was diagnosed with Crohn’s disease and started Stelara. After a few hospital stays and some improvement with her symptoms, she began to experience an increase in rectal pain, urgency, and discomfort, so Keyla needed yet another surgery.
October 27th (less than one month ago!) she had her j-pouch removed with a proctectomy and officially made her stoma permanent. She’s recovering from this surgery as we speak.
How Modeling Came into Play
After reading that challenging medical history, you may wonder how Keyla finds the time to focus on a profession. Modeling is something Keyla always wanted to do when she was younger, but she was too embarrassed to tell anyone. She sort of stumbled into it. Keyla had done a fun photoshoot with a friend and those photos were shown to another friend who works in the fashion industry. Before she knew it, Keyla was a published model!
“Sometimes I still can’t believe I’m living my dream despite having health issues. I had the honor to walk at London Fashion Week this year and have been published in magazines out of the US, UK, and Canada.”
SURREAL Lifestyle Magazine and 4 Seasons Magazine have been her favorite features thus far because the publications have allowed her to speak about her IBD advocacy work. Modeling serves as the perfect platform for spreading awareness to others about ostomies and life with Crohn’s.
“I always try to take the time for myself and make sure I am doing the things my mental health needs to stay focused and feel well. I also try to own those feelings. If I’m symptomatic, I try to accept it and openly communicate my struggles with others.”
Keyla says having an ileostomy can make modeling a bit more complicated, especially if she has to wear form fitting or tight clothing. If that’s the case, she ends up having to empty her bag more times than she really needs to. She’s grateful her modeling gigs have followed strict COVID guidelines, which helps her feel more at ease during these uncertain times.
When a project allows, she especially enjoys getting to show her ostomy in photos or on the runway. She chalks that up as her biggest career win of all!
A model mother
Keyla’s main focus whether she’s modeling or fighting a flare in the hospital is her family. She has an 11-year-old son who inspires and motivates her to push through the difficult days.
“IBD has made motherhood challenging. Without chronic illness motherhood can be difficult as it is, adding health issues on top of it makes it more complicated. I constantly question whether I’m making the right choices. But I also tell myself all I can do is try and hope that I’m being a good role model for him.”
It pains her to see how her son gets anxious about her IBD and healthcare. He’s been by her side every step of the way since she was diagnosed after he was born. Despite the highs and lows, Keyla feels her son is stronger because of her illness and has an innate sense of empathy and understanding for others.
If her IBD has taught her anything it’s that good days give us happiness and bad days give us experience. Modeling has enabled Keyla to be comfortable in her own skin and live the life she imagined long before Crohn’s was ever a part of who she was.
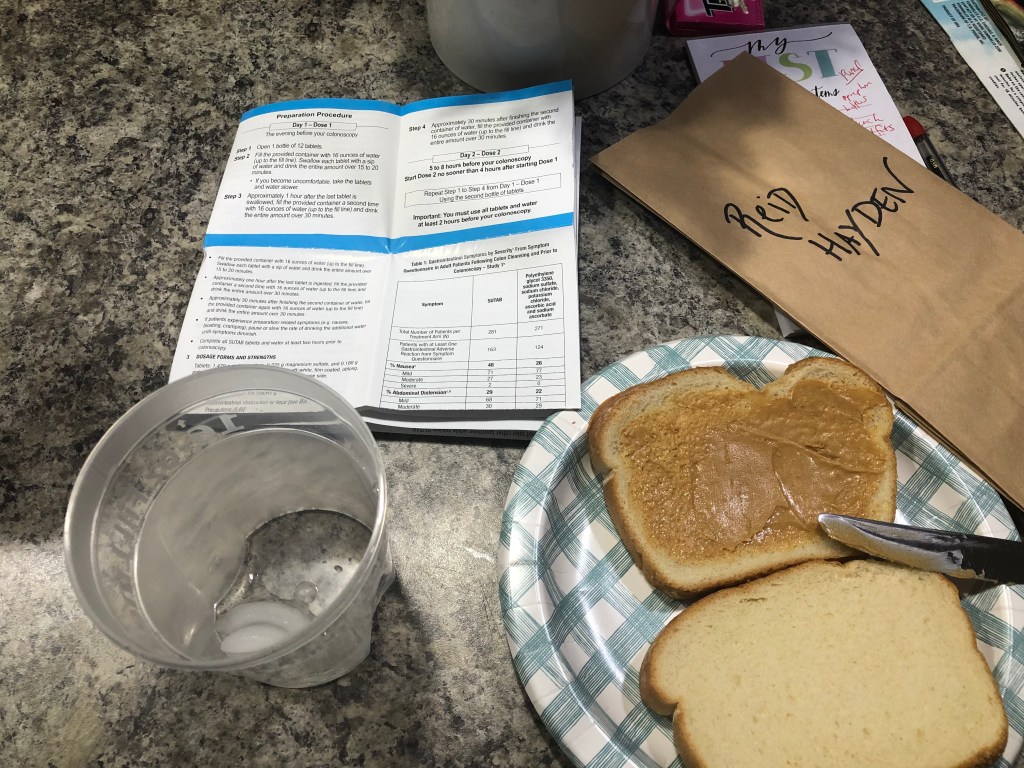
‘Hello darkness, my old friend. I’ve come to talk with you again’. Ahh, the dreaded annual, routine, colonoscopy. I got a little spoiled because my last scope was July 2019. I decided to hold off in the thick of the pandemic out of safety concerns and did a fecal calprotectin test instead. Then, I got pregnant…so I had quite the enjoyable hiatus.
This time around, I decided to try SUTAB, a 24-pill prep + Magnesium citrate, rather than my typical Miralax-Dulcolax-Magnesium citrate. Without insurance and utilizing the patient savings card that’s online, SUTAB can be costly. I went here and printed out a coupon, I was able to get it from the CVS Pharmacy in Target for $50. While it’s more expensive than most preps, to me, it was worth the try.
Thoughts on doing a pill prep
So, this entire experience was a bit complicated for me. The night before my scope, I was miserable from the Magnesium citrate and the initial 12 pills. First off, I’ve come to learn that most GI’s do not make you take magnesium citrate on top of the typical prep. I’m just one of the lucky ones. Magnesium Citrate has always made me vomit, even if I take Zofran before. Prior to this prep, I always did the lemon flavor. I switched to the cherry flavor this time, GAME CHANGER. I had no problem getting it down…but it only stayed down for about an hour or so.
I threw up an unbelievable amount multiple times and never had a bowel movement. After not eating a solid meal for three days I was anxious and worried that I wouldn’t be cleaned out enough and that I was going through this hell for nothing. Sadly, Reid and Sophia witnessed it all go down and it broke my heart that they had to see me so sick and weak on the bathroom floor.
I relied on many members of the IBD community and medical professionals on social media to help guide me through the unknown. I took a Zofran and went to bed. I never woke to use the bathroom. I set my alarm for 3 a.m., took another Zofran, did NOT take the second 10 ounces of Magnesium citrate, and timed the remaining 12 pills every 3 minutes (rather than taking them back-to-back). I found that tip on Twitter and it made a huge difference! I decided not to take the second bottle of Magnesium citrate because in the medical instructions from the SUTAB box it says *not* to take any additional laxatives.
My scope was scheduled for 8:30 in the morning. I finished the pill prep at 4 a.m. and between then and 6:45 a.m. when we got on the road to hospital, I got completely cleaned out. I didn’t get nauseas, and everything fell into place. Now, I credit this with the fact I barely had anything in my body, which makes the prep much easier in my opinion.
If you would have asked me my thoughts on SUTAB vs. my typical go-to, Miralax + Dulcolax + Magnesium citrate the eve of the scope, I would have told you I would never do a pill prep, again. But once I took the Zofran, didn’t take the Magnesium citrate, and timed out the pills, only having to chase with pure water was amazing and very simple. All you have to do is drink 16 ounces of water with the 12 pills, and then an additional 32 ounces of water spaced out after. You can have more water if you want it.
My mom was laughing because she was watching me do multiple loads of laundry, make my son’s school lunch, pump milk for my 4-month-old, shower and get dressed…all on 4 hours of sleep, while in the middle of colonoscopy prep. As an IBD mom, I felt empowered in that moment of all I was capable of doing in the midst of what previously had been a nightmare.
Unfortunately, what is generally the “easy” part of the process—the hospital portion and the actual scope was very emotional and painful for me. My GI had ordered my usual routine labs to be drawn through my IV (to try and save me a trip) but I was so dehydrated from the prep and breastfeeding that the nurses could not get any blood. It took sticking me 8 different times. I felt like a human pin cushion. The IV was placed in a very tiny vein in my hand and the Propofol burned SO badly going in that I almost couldn’t handle it.
I kept asking for my husband Bobby to be allowed in recovery and felt like no one was listening to me. The nurse was gruff and kept poking me, even after I told her I would just go to a lab this week once I was hydrated. The blood pressure cuff even bruised my arm. I cried a lot of tears and the experience brought me back to a traumatic 2008 hospitalization for an abscess in my small intestine that involved 8 tries to get an IV.
My recommendation—do NOT allow labs to be drawn after you are done prepping for a scope. Save yourself the pain and the prodding. I overhead the nurses talking (outside the curtain) of my “room” saying they refuse to ever do this again to a patient and that we should all just go to labs to get bloodwork, rather than trying to get it done when we’re all terribly dehydrated. I had so many band-aids and gauze all over both my hands and arms, the nurses even sent me home with more gauze and band-aids in case I bled in the car. Fun times.
The best news
Luckily, the heaviness of this entire ordeal lifted a bit when my GI walked into the recovery room and said, “your small bowel and colon could not be more gorgeous. It was so pretty in there!” Best compliment you can give a gal with IBD!
She said even my anastomosis site (where my large and small intestine were reattached in 2015) …looked perfect. She explained how ulcers develop and indicate lack of blood flow. No ulcers, mucosal healing, and no biopsies needed. I feel incredibly fortunate that I have been lucky enough to hold onto my remission that came about because of my bowel resection surgery in August 2015.
I understand that “remission” is a complicated term in the IBD world. It doesn’t mean symptom-free, it doesn’t mean a cure…to me, it means I have many more days that I feel well than when I don’t. It means my Crohn’s disease doesn’t have to dictate or rule my life and that I’m able to be present for my family and for myself. It’s knowing that remission can go away in the blink of an eye. It’s happened to me before, and I know it will happen again. But for now, I’ll take a deep breath and enjoy this reprieve from the havoc I know my disease is capable of causing and continue to do all I can to stay well by staying on my biologic, keeping tabs on my lab work, and checking in with my GI whenever I feel like something may be starting to go awry. Remission is not something to be taken for granted. I often get asked what I do to “stay” in remission, I honestly don’t feel like I deserve much of the credit other than being a compliant patient and being very in-tune to how my body speaks to me through symptoms.
Moments that helped me get through
When my kids kept bringing me play food to help me feel better when they realized I couldn’t eat “real food” all week.
How my mom flew in from Chicago to help with the kids and to be an added support (like she does for every scope, procedure, and hospitalization).
When my husband, Bobby, came home late from work and rather than sitting at the kitchen table to eat, I caught him standing at the sink with his dinner plate and back turned so he wouldn’t be eating in front of me.
Knowing I was going to have a breakfast date with Bobby at our favorite spot and keeping my eye on the prize after going so many days without eating solid food.
Using my frozen breastmilk stash the day before and day-of the procedure to ease the burden of having to use energy and my body to feed Connor.
Reading all the comments on Instagram and hearing from friends and family near and far over text message and through phone calls really helped lift my spirits and conquer this as an exclusively breastfeeding mama.
Long story short—Aside from checking with your GI and getting a prescription for SUTAB, I would recommend trying the pill prep and from a patient perspective remind you to do the following:
Have your GI provide you with a prescription of Zofran (if you don’t have one already).
Take Zofran 30 minutes prior to taking the pills.
Set a timer on your phone and take one pill every three minutes.
While the pills are large, they are no bigger than a Prenatal vitamin and are doable.
For my self-imposed liquid diet this is how I plan it out for a Friday morning scope:
Last solid meal Monday evening
Tuesday-Wednesday full liquids
Thursday-Friday am clear liquids…and don’t forget my favorite tip of all…GUMMY BEARS! They are considered clear liquids, just steer clear from the red and purple ones.
Over the weekend (Saturday, November 6) I received my third dose of the Pfizer vaccine. When I had my second vaccine on August 11, I never dreamed I would be getting another jab so soon. But here we are. In talking with several IBDologists and patients I felt the need to expound on this topic, as misinformation is driving quite a bit of confusion about what additional doses and boosters mean for the IBD community and how we can best sort through all the information being thrown our way.
What’s the difference between an additional dose (3-part vaccine series) vs. a booster?
Dr. Meenakshi Bewtra, MD, MPH, PhD, Penn Medicine,helped me better understand this by explaining, “a 3rd dose implies that you had a less-than ok response to two doses and need a “3-dose regimen” to get the same response that someone else would get with two doses.”
The 3-dose regimen caters to those who are severely immunocompromised—those on chemotherapy and organ transplant recipients.
“Most IBD patients do NOT have this problem. Some small studies have shown varying responses; the largest is PREVENT-COVID which was over 3,000 patients. The study found that those on monotherapy TNF had similar response to the COVID vaccines as the general population. It was only in the setting of combination therapy (anti-TNF plus azathioprine or methotrexate) that you had a blunted antibody response (again–this was a research study),” said Dr. Bewtra.
She went on to say she has not been recommending that all her patients get a 3rd dose—rather, reserving that for patients who are on combination therapies. At the same time, this is a very fluid discussion, and the decision needs to be made on a case-by-case basis between each patient and their physician.
A booster is if you had an adequate response to the first 2 doses and are now 6 months past your primary series and fall into the recommended categories (over 65 years old or age 50+ with high-risk medical conditions), if you are part of a younger age group with high-risk medical conditions, or for those who work in occupations that put them at high risk for COVID. Booster shots are most effective 6 months after your initial series for Pfizer and Moderna and 2+ months after J&J, although the data really supports waiting until at least 6 months for best response. Age is the biggest determinant of needing a booster, whether you have IBD or not.
Dr. Peter Higgins, MD, PhD, M.Sc., University of Michigan Health, explained this clearly on Twitter. He tweeted, “It is a catch-up dose for folks who for various reasons (anti-TNF’s, steroids, chemo) will not have a great response to two doses. To catch-up to everyone else. Then a booster dose later to keep pace.”
I’m *only* 38 years old. I’m *only* on Humira. Why am I getting a 3rd dose two months after my 2nd vaccine?
I saw my gastroenterologist for a check up last week and she ordered a SARS-Cov-Z Antibody (IgG) Spike Semi Quantitative test at Quest Labs. My results came back and from a range of 0-20, I was at 4.42. My GI was surprised my response had dwindled so quickly and recommended I receive a third dose to help mount a more robust response.
Dr. David Rubin, MD, Professor of Medicine, University of Chicago, and Chairof the National Scientific Advisory Committee of the Crohn’s & Colitis Foundation told me that multiple studies on antibody response in patients with IBD have shown that after two doses the titers are similar to that of the general population. So, my result, is an aberrancy compared to the data. He said getting a 3rd dose seems right for me, given my personal results.
“We have suggested the booster for everyone and think of the COVID vaccines as part of a 3-dose series. When it comes to true protection from the infection, memory B cells (cellular immunity) are more important than antibodies. There is not a commercial test for that yet, but we are studying it.”
In a recent talk Dr. Rubin gave about COVID, vaccines, and the updated recommendations for additional doses and boosters, he discussed how IBD is a condition of an abnormal immune response. Therapies to manage IBD are predominately immune-based and immune-modifying. The information shared by the CDC and FDA is not specific to IBD and is confusing (for everyone).
“CDC recommends individuals should get a third vaccine if:
Previously received two doses of an mRNA vaccine
Currently taking select therapies, including anti-TNF and anti-metabolites
“Other biologic agents that are immunosuppressive or immunomodulatory”
High dose steroids (prednisone ≥20 mg/d or equivalent for ≥2 weeks)
All other individuals are recommended to get a booster 6-8 months after second mRNA vaccination.”
But wait, what’s the recommendation on antibody tests? Are they valid?!
This is where I get confused too, folks. Prior to receiving my antibody test and following my doctor’s orders I was not aware that the FDA and CDC both strongly recommend NOT checking or acting on antibody levels, as the tests outside of research studies are unreliable and unvalidated. Antibody tests do not paint a full picture of our immune system.
“There are strong recommendations from the CDC, FDA and ACIP (Advisory Committee on Immunization Practices) that patients NOT check antibodies nor use them in decision making. The only time they should be used is in the setting of research studies,” said Dr. Bewtra.
The reason for this is multifold:
-Antibody tests are not validated.
-Since they are not validated, there is no comparison for values. For example, my 4.42 on one test may be completely different in a different test.
-We know that antibodies are testing only one aspect of the immune system—there is a LOT more to immunity than an antibody level.
Dr. Jami Kinnucan, MD, University of Michigan Health advises all her IBD patients to receive a third dose, or a booster vaccination based on their risk factors and immunosuppression medications.
Dr. Kinnucan says, “Overall the current recommendations are to get a dose #3 on certain immunosuppressive therapy, which is different than a true booster dose. In addition, it is hard right now to understand what the true threshold of immunity is with antibody testing so I would not put too much into antibody test results. I do not recommend that patient’s routinely have their antibody status checked (unless they are involved in current studies). I would recommend getting dose #3 or booster dose for IBD patients.”
Vaccinated diverse people presenting shoulder
During the holidays we should all continue to follow CDC recommendations when it comes to social gatherings, social distancing, wearing masks, and properly washing our hands. Everyone that you spend time with should be fully vaccinated so the only thing being spread is holiday cheer. If you plan to spend time with anyone who is not from your immediate bubble, it’s recommended they take a rapid test before coming over.
Key Reminders as We Head into the Holidays
Vaccines are not 100% protective and Dr. Bewtra says “no one is fully vaccinated.”
“No one should think that just because they’ve had two vaccines, or 3 or 4, that they are safe. Protection is a function of the community: when community levels are high, even if you just got your vaccine, you need to wear a mask and practice all the recommendations from the CDC.”
What are the studies saying about the IBD Community
The data from science is highly variable. Studies looking at Rheumatoid Arthritis are not translatable to IBD, even when patients are on the same drugs. We have the real-world data from IBD, and it shows that the vast majority of IBD patients respond to vaccines appropriately. So not everyone needs to rush out to get a 3rd dose.
“We are doing a lot of vaccinating “the worried well” in this country. That may be fine because we are in a rich enough place to do that over and over, but it should not infer a feeling of false protection and it may be unnecessary,” said Dr. Bewtra.
Closing Thoughts
On the fence about receiving a 3rd dose and/or a booster dose? Have a discussion with your physician who specializes in caring for your IBD and prescribes your medications. Much like how IBD and COVID manifest differently in each person, it’s not fair to make blanket decisions about the entire patient population.
Dr. Rubin wants to reassure those with IBD that they are not at increased risk of bad COVID outcomes (but not at decreased risk either). He says most patients with IBD on therapy beyond 5-ASA or budesonide are eligible to get a third dose now. For patients on combination therapy with anti-TNF and thiopurine, methotrexate or high dose steroids, it’s reasonable to get the third dose/booster early.
Stay tuned for the evolving research. As the months go by and more research studies are completed, we’ll have a clearer picture of how to tackle this as well as additional guidance.
Save the Date: Facebook Live Event on Global Perspectives on COVID + IBD
The South Asian IBD Alliance (SAIA) is hosting a Facebook Live event Saturday, November 20 at 10 am EST. Patients and physicians will share their perspectives on COVID from the United States, United Kingdom, and India. Doctors will explain study data on serocoversion (development of specific antibodies in blood serum as a result of infection or immunization) in IBD patients and what their thoughts are on boosters and a 3-dose regimen, along with their viewpoints on mixing and matching vaccines. Patients will share their experiences from each respective country and discuss the challenges the pandemic has caused in terms of care.
Whether it’s a holiday like Halloween or a wedding weekend (both of which I experienced the past few days), it’s important to stay ahead of IBD symptoms and be proactive in how you approach the big moments and the big days in your life so you can enjoy them. The unpredictability of Crohn’s disease and ulcerative colitis can feel suffocating when you are hoping and praying your body doesn’t betray you on the big days.
Here’s how I mentally and physically prepare so I can stay ahead of my Crohn’s and be in the moment with family and friends.
Be extra cautious with what you drink and your diet. Caffeine and alcohol are triggers for me…and for many people with IBD. The day of my brother’s wedding I refrained from drinking coffee and alcohol so I didn’t have to worry about needing to run to the bathroom in my bridesmaid dress or have to think about how bloated I could get from the abdominal pain a few drinks can cause. My Crohn’s felt non-existent the entire day, thank you Jesus!
When I am traveling and away from home, I am extra mindful of what I eat and keep it on the safe side, especially if I’m going on a road trip with my family or flying the friendly skies. You know your triggers, try to steer clear from them as much as you can. If I am celebrating a holiday at home or at my parent’s house, I tend to be a little “riskier” because of the comfort level I have using the bathroom there, resting, etc.
Be choosy about your shapewear. I don’t know about you, but ever since my Crohn’s diagnosis I’ve never liked Spanx, belts, or anything restrictive around my waist. I rarely ever wear jeans with a button. For my brother’s wedding I wore Spanx that were biker shorts that went up to the bottom of my bra and it was a game changer, especially being 3 months postpartum! I didn’t have any stomach or bloating issues. Highly recommend the Spanx High-Waisted Power Short.
Pack pain medication and maintenance meds. Just because you’re away from home celebrating a holiday or a wedding, doesn’t mean it’s time to be flippant about managing your disease. When I’m packing, I always take more than I need when it comes to pain medication, even if I haven’t needed it or used it for months. Bring extra strength Tylenol and any prescription pain medication you may need along with your “typical” medication (if you take it). Be mindful of how long you are traveling and if you could face delays, etc. If you are flying, always keep medication on you, so it’s right where you need it and so you don’t chance anyone taking it out of your luggage.
With my Humira I look ahead when I have a big event and plan accordingly. For my wedding for instance, my injection was due two days after I tied the knot. My GI had me move up my dose to the day of the rehearsal dinner so I could have some extra coverage.
Try and get as much rest as possible. With IBD we all know fatigue is one of our most difficult symptoms to handle. Throw in travel and being out of your normal surroundings and life can really feel like an uphill battle. Allow for downtime and breaks throughout the day if you’re able so you can give your body time to adjust to the hustle and bustle.
Practice deep breathing and mindfulness. If you feel symptoms creeping in try and take deep breaths and ground yourself. Lay down and gently put one hand on your chest and your other hand on your belly. Feel your stomach slowly rise and be present in the moment. Close your eyes—remind yourself that pain is fleeting and go to your happy place. Diaphragmatic Breathing, also known as deep breathing or belly breathing, helps to manage stress.
Don’t suffer in silence. This is the hardest part of all. I always struggle articulating when I’m not feeling well on the “big” days. I never want to damper the mood or make people worry so I internalize my pain and put on a smile. As a mom of three little ones, especially on holidays like Halloween and Christmas I never want to allow my disease to take away from the special, memorable moments. But this can make the struggle even worse. I find quietly telling my husband or my mom that my “Crohn’s is acting up” that it takes some of the weight off my shoulders so they at least know why I may need help, may not be as talkative, or may not seem to be acting myself.
Use these times as a “teachable” moment. Before I started sharing my story publicly, you’d never hear me tell someone I barely knew I had Crohn’s disease. But now, I find it extremely helpful to drop that line whenever I can. You’ll find making others aware can bring about much needed support, understanding, and even intrigue. Telling others I have Crohn’s disease feels like a normal, casual part of conversation now for me. At my brother’s wedding my IBD came up several times in conversation—with the hair and make up people, to my cousins coming up to me and saying, “I have co-workers with Crohn’s, and I tell them all about your blog.”
While IBD is not our identity, it’s a large part of who we are and impacts many of the decisions we make each day that can influence everything from what we eat or drink at a party or social gathering to how we participate in milestones and festivities. Taking the guesswork out for others takes a bit of the pressure off and can make you feel less overwhelmed and more comfortable and at ease.
Biosimilars. When you hear the word how does it make you feel? Maybe a little skeptical. Maybe a little uncertain. Maybe a little leery. If so, you’re not alone. I’ve been on my current biologic more than 13 years and when I think about having to possibly make a switch in the future it makes me nervous, too. That’s why I called on IBD specialists and gurus Dr. Miguel Regueiro, Professor and Chair of the Digestive Disease and Surgery Institute at the Cleveland Clinic and Dr. Christina Ha, MD, FACG, AGAF, Cedars-Sinai to help educate the patient community and put falsehoods and myths to rest. Biosimilars are here to stay so it’s imperative we get comfortable with the uncomfortable.
What is a biosimilar?
First things first, let’s get the definition out of the way so you know what we’re working with here. Biosimilars are not the generic version of the biologics many of us are accustomed to. A biosimilar is a product, usually a medication, that is formulated in a fashion that is similar to the “reference” product, also known as the “originator” medication. Think Infliximab (Remicade) and Adalimumab (Humira).
I love the way Dr. Ha explained this, “It’s like identical twins sharing the same DNA but having different fingerprints. With biosimilars, dosing, administration, optimization, monitoring, and plan of care is the same, nothing changes except the Infliximab is now Inflixilmab-dyyb, for example.”
How You’re Told You Need to Switch
You may be wondering how this conversation and discussion even starts and how it translates over to the patient experience.
“The physician and patient are contacted by the insurance company indicating that the patient must switch to a biosimilar. This allows for some discussion between the physician and the patient. Although this should be the fashion in which it occurs, I know that this is not always the case and sometimes the notification is last minute or done in a way that leaves little time for education and discussion between the administration of the next dose of biologic and notification by the insurance,” said Dr. Regueiro.
Cost Savings and Access to Patients
I want to preface this by saying the cost savings varies from patient to patient and is largely dependent on a patient’s insurance company or health plan that covers the payment of their medication.
Dr. Regueiro says, “To provide a simple overview, each insurance company/health plan will contract with a pharmaceutical company for a certain medication. Much of this is dependent on getting the best price for the insurance company. A biosimilar is typically cheaper than the original (originator/reference) medication and the insurance company will then list the biosimilar as its preferred biologic for that condition, e.g., Inflectra or Renflexis for Crohn’s disease or ulcerative colitis. This makes the approval of that biosimilar “easier” for the patient and therefore access better. The question of where the savings are realized is another matter. Even cheaper drugs do not translate to savings directly to the patient.”
If you’ve been on a biologic “originator” successfully and are told you suddenly must make the switch, it’s not uncommon. Dr. Regueiro says he has many patients who have found themselves in this position. His advice? Speak to your healthcare team, but also go to trusted resources for education, e.g., the Crohn’s and Colitis Foundation website has some useful information for patients about biosimilars.
Addressing patient hesitancy
It’s no surprise this can be an emotional discussion. I try and envision myself being told that I had to switch after more than 13 years, and I know I would be crying because of the comfort and confidence I have had with my current therapy.
“The idea of switching to a biosimilar is fraught with concern. I typically acknowledge their concern, but then explain the data. There have been many studies that have shown that switching from a biologic to a biosimilar is well tolerated, is equally efficacious, and does not incur any different safety risk. I tell the patient that we technically cannot say that the biosimilar is the “same” as the biologic, but in essence it is. I also explain that I have had hundreds of my own patients switch and I have not seen a problem. In fact, in some patients I may get a drug level of the biologic before switching and then the same drug level of the biosimilar after switching and see no difference,” explained Dr. Regueiro.
For example, there is a blood assay for Remicade (Infliximab) that measures the Infliximab level and antibodies to Infliximab. When Dr. Regueiro has had patients switch from Remicade to a biosimilar, e.g., Renflexis or Inflectra, and then measure the same exact drug assay, the results of the Infliximab level and antibodies to Infliximab are the same. The biosimilar works in an identical fashion to the original biologic, and the blood assays show the same results. The body “cannot tell” the original biologic from the biosimilar.
Let’s read that sentence again. The body “cannot tell” the original biologic from the biosimilar.
Dr. Hasays, “The key here is to understand that you are being switched to an equivalent not inferior agent. Biosimilars are rigorously studied for safety, effectiveness, antibody formation with a lengthier, more involved FDA approval process than generics.”
Why Biosimilars are NOT generics
A generic medication has the same active ingredient as the brand name medication. An example would be the generic medication mesalamine for the brand name medication Asacol. Asacol’s “active ingredient” is mesalamine and the generic is simply formulated as mesalamine. The “packaging” of Asacol makes it Asacol, but its active ingredient is mesalamine and is identical to the generic formulation of mesalamine.
Dr. Ha explains why biosimilars are not generics.
“Generics are chemical compounds where exact replicas of the active ingredient are possible. However, biosimilars are biologic agents, complex protein structures constructed from living cells. Exact replicas aren’t possible but nearly identical structures can be manufactured – remember, these are very sensitive compounds. That’s why these medications need to be refrigerated and handled differently than a generic.”
I asked Dr. Reguiero if there’s ever a situation where he advises against a patient being switched to a biosimilar. He said generally, no.
“The only main question will be if a patient has already been on a biosimilar after the originator biologic and then needs to switch to another biosimilar. This would be a “multiple switch” rather than a single switch from the original biologic to biosimilar. Based on the limited data to date, and similarity between all of the biosimilars and original biologic, I do not even see this as a problem, but we need more research to make a final conclusion onto multiple switches.”
“Delaying treatment to stay on a version of a medication that really is not meaningfully different than the biosimilar may lead to far worse consequences than staying on schedule by switching to a biosimilar. Remember, delaying anti-TNF schedules may increase risks of antibody formation, infusion/injection reactions, and flares. I am far more concerned about staying on schedule and not missing doses than I am the biosimilar vs reference,” said Dr. Ha.
What if a biosimilar fails?
If a biosimilar fails, Dr. Regueiro looks at it the exact same way as if an original biologic fails. For example, let’s take the case of biosimilar Inflectra for Remicade.
“If a patient is started on Inflectra as their first biologic ever and it stops working, I generally check blood levels to determine if the patient has developed antibodies to Inflectra and that this is the reason for failure. If they have developed antibodies, and the Inflectra has worked well for a long time, then I would switch to another anti-TNF, but not another biosimilar to Remicade. The reason for this is that if a patient develops antibodies to the biosimilar, they will form antibodies to the original biologic or another biosimilar of that same biologic. However, I would switch this patient from Inflectra to Adalimumab (Humira) or one of the other anti-TNFs if needed. I would do the exact same thing if the first biologic I used was Remicade and it failed due to antibody formation.”
I went on to ask Dr. Regueiro when he would switch a patient to a biologic medication from a “different class.”
“Let’s take the example of Inflectra or Remicade. If a patient is started on Infectra or Remicade and they have no response from the beginning, and their drug levels of Inflectra or Remicade are good (and they have not had antibodies again) this means it should be working and it is not – this is a primary failure of that medication. In that case, not only would I not switch to another biosimilar or back to the original biologic, but I would also completely switch away from the class of anti-TNF, e.g., Humira, Cimzia, Simponi, as the patient is likely a non-responder to all anti-TNFs. In this case, I’d move onto something like Entyvio, Stelara, Xeljanz, or Zeposia (depending on whether it’s ulcerative colitis or Crohn’s disease).”
What’s coming down the pipeline for patients?
With all the biosimilars on the market and many more on the way—Dr. Regueiro and Dr. Ha say it’s quite likely all patients can expect to be switched off their current biologic at some point as insurance companies are able to get the biosimilar as a cheaper cost.
As far as savings programs, many of us are accustomed to with our biologics (I pay $5 a month for two injections), this would be dependent on what the company that makes the biosimilars offers and may look quite different to the originator biologic’s savings programs. However, I would anticipate the patient would not pay more for the biosimilar. There would either be a cost savings program with the pharmaceutical company that makes the biosimilar, or, more likely, the insurance company would keep the out of pocket cost the same for the patient.
Biosimilars are administered in an identical fashion to the originator biologic. So, you won’t be forced to go from doing a self-injection to getting an infusion. I asked Dr. Reguiero about Humira’s biosimilar in the future, and he anticipates that it will be citrate-free, just as the originator is now in the States.
Pediatrics and Biosimilars
As biosimilars come to market, the indications should be the same for the originator biologic. That is, if there is an approved indication in pediatrics for the originator biologic, the same should be true for the biosimilar. However, the FDA will make final guidance on the indications for a biosimilar and they could vary slightly on which diseases are approved and which age of patient approved.
What Patients Have to Say
Christina received a letter from her insurance company in June letting her know that Remicade was no longer approved and that she would be switching over to Inflectra in July. The insurance company reached out to her directly and had not informed her GI. She was five months pregnant and was stressed and anxious about switching medications in the middle of pregnancy.
“I have been on Remicade since September 2013 and it’s working really well for me. My GI was super supportive with my desire to stay on Remicade through pregnancy and agreed that I should not switch medications. In part of the letter for my insurance company there was an appeal process, which my GI did on my behalf. A few weeks later I got a letter in the mail from my insurance company that my appeal was denied. I contacted my G.I.’s office and she had someone in her office do a follow up appeal. The insurance company finally agreed to approve me for Remicade through my due date, October 23rd.”
Christina’s baby was born October 11th, so she’ll be making the switch this week while she’s postpartum.
Vern lives in Canada and the government there forced him to make the switch.
“The cost is partially covered by the government. I was pissed to say the least. They kept telling me it was safe, but I wanted to see evidence it was safe to switch to a biosimilar after someone had been on a biologic long term. I never got an answer. Luckily, I’m doing fine, and I have not noticed a difference.”
Lizzy highlights the emotional struggle biosimilars burden patients with.
“Even though I don’t see an uptick in symptoms and my remissions has been maintained, emotionally the switch was really difficult. My insurance forced me to switch. I was extremely sick for a long time before starting Remicade while I was hospitalized. So, I was really afraid of the switch making me sick and of course it was horrible not to have a choice in my healthcare.”
Kelly attests to the emotional struggle and disappointment. She says she spoke extensively with her GI prior to making the switch and did her on own research.
“When I received the letter from my health insurance company telling me I would be forced to switch to a biosimilar I was disappointed. I had been on Remicade for more than two years and it had only recently put me into remission. But I knew the switch was coming, having heard from many people in the IBD community that they were being forced as well. I had already done research on the data from Europe and Canada showing that biosimilars of Infliximab had the same efficacy and safety profiles as Infliximab.
She’s now had two Inflectra infusions and hasn’t noticed any difference in the way her body handles the medication. Kelly is crossing her fingers for a continued great experience and hopefully no more frustrating insurance shenanigans.
Madelynn was on Remicade prior to being switched to Inflectra. Unfortunately, her care team and her insurance failed to communicate the change to her. She shockingly discovered the switch was made after proactively reading medicine notes on the patient portal.
“I was nervous about it, and a bit upset. Who wouldn’t be after being in remission with a medicine then having it randomly changed? I ended up researching quite a bit about it, which helped calm my nerves. I also asked more questions of my medical team. I was worried about the biosimilar not working and causing a flare and of possible side effects. Keep in mind, I have Remicade induced side effects already. Could Inflectra make them worse? When a medicine keeps you in remission, that is something you want to hold onto for as long as you can. If you are taking any medicine, never be afraid to ask questions, research, and advocate for yourself. If something does not work, speak up!”
Madelynn has only received one infusion of Inflectra, but so far, she feels well and notices no changes with her IBD.
A Word from the Crohn’s and Colitis Foundation
Laura Wingate, Executive Vice President of Education, Support, & Advocacy for the Crohn’s & Colitis Foundation encourages patients to learn as much as thy can about not just biosimilars but all treatment options available so we can be active and informed partners in making decisions with our healthcare teams.
“If you are informed you need to switch from a biologic to a biosimilar, you might be worried and that’s normal. But remember that biosimilars are just as safe and effective as your original therapy. Don’t be afraid to ask questions of your healthcare providers about the switch and why it’s happening and share any concerns you have with them. You can also contact the Crohn’s & Colitis Foundation for additional information, education on biosimilars, and support.”
Helpful Resources on Biosimilars
If you have questions about biosimilars– talk to your health care team. The more education, resources, and support they can provide you with to bolster your confidence that the biosimilars are an important part of IBD treatment, the better. I know personally as someone who depends on a biologic to maintain my remission, that doing the research for this article has made me feel a lot more confident and comfortable about biosimilars and what they mean for the patient community.
There are a several great resources about biosimilars to check out:
This post is sponsored by the Autoimmune Association. All thoughts and opinions shared are my own.
An educated patient is an empowered patient. Over the weekend the Autoimmune Association presented its Inaugural Autoimmune Summit that aimed to do just that. The virtual two-day event featured 23 educational sessions and more than 50 autoimmune experts including physicians, nurses, policy experts, and of course, patient advocates.
The Summit covered a wide variety of important topics that impact patients and caregivers who live with autoimmune conditions. I had the opportunity to moderate a panel discussion about fertility, family planning, and pregnancy alongside Dr. Marla Dubinsky, Chief of Pediatric Gastroenterology at Mount Sinai and Co-Director of the Susan and Leonard Feinstein Inflammatory Bowel Disease Clinical Center and Mariah Leach, a mom of three who lives with Rheumatoid Arthritis and Founder of Mamas Facing Forward. As an IBD mom of three chidren myself, I’m extremely passionate about sharing guidance and support for fellow women on this subject.
During the discussion, Dr. Dubinsky touched on many aspects of the journey to motherhood and beyond with IBD, but one comment she made resonated with me. She said the greatest gift a woman can give their child, is to stay on their medication, and allow their baby to thrive in an uninflamed environment. As someone who needed and depended on my biologic with all three of my pregnancies that comforted me greatly and really struck a chord.
Other topics of discussion during the Summit included tips and tricks for managing multiple specialists to clinical trials, health equity, advocating on Capitol Hill, and complementary medicine.
A dream come true
Lilly Stairs, Vice Chair of the Board of the Autoimmune Association and Summit Lead, lives with Crohn’s disease and arthritis. As a patient advocate, she understands the vital importance of providing those who live with chronic health conditions to share their voice and articulate their needs and struggles.
“It has been a dream of mine and the Autoimmune Association’s to plan an event that unites community members from across autoimmune conditions. Our patient odysseys share deeply rooted similarities. By coming together, we can accelerate autoimmune education, awareness, advocacy, treatment, and someday, cures.”
Goals of the Summit
The goals for the Summit were three-fold. Organizers and presenters like myself hope you walked away feeling connected to people across the patient community, while learning tangible tips for managing your autoimmune conditions. Lastly, the hope is that attendees and Summit participants feel energized and excited about what the bright future holds for those living with autoimmune diseases.
Lilly went on to say, “Events like the Autoimmune Summit are essential engagements for patients and caregivers to participate in. These events provide tools to navigate life with chronic illness and empower patients with the knowledge they need to be “CEO, secretary, and treasurer of your care” as Hetlena Johnson, Lupus Patient Advocate so eloquently stated in the Managing Multiple Autoimmune Conditions panel.”
Events like this are a reminder that we are not alone in our journeys. Even though chronic illness can be extremely isolating, events like the Autoimmune Summit offer the opportunity for connection that often feels like much needed chicken soup for the soul. The camaraderie that is possible even though Zoom has a lasting impact on helping to lift the burden and self-doubt many patients face.
From the Speakers
Tina Aswani Omprakesh participated in a panel on complementary medicine and autoimmunity. As an ostomate who juggles Crohn’s disease, Gastroparesis, and IBS, she knows firsthand how imperative it is to take on illness with multiple approaches.
“This is an important subject that’s often not discussed in the autoimmune space. The reality is that many patients are thinking about exploring it but don’t know how to navigate it in a way that can help complement their existing therapies. These conversations are essential to proliferate both credible information and sources of complementary therapies so patients can truly live their best lives possible.”
Molly Schreiber lives with Type 1 Diabetes, Rheumatoid Arthritis, and POTS. During the Summit, she spoke about what it’s like to manage multiple autoimmune conditions.
“Anytime I can share my story, my hope is that attendees feel less alone in their battle with chronic illness. We may have different health conditions, but our fight is often the same—pain management, medical providers who listen, and affordable medications we can easily obtain.”
Alisha Bridges is a patient advocate who lives with Psoriasis. She participated in a breakout session geared towards dermatology. She says having the chance to speak at the Autoimmune Summit was an honor.
“I hope my story helped viewers to better understand the unique challenges of living with psoriasis as a woman of color especially in the clinical trials sphere. These conversations are imperative to elicit change for better care of patients of all backgrounds.”
Curtain Call
It’s our hope attendees discovered tips for managing autoimmune disease from patient advocates like myself who understand your reality, while also learning about the latest research and future treatments on the horizon.
Did you miss tuning into the first-ever Autoimmune Summit? No worries! All the presentations were recorded and will be shared in the weeks ahead. I’ll be sure to share the Fertility, Family Planning, and Pregnancy discussion I was a part of on my social media channels as soon as the video becomes available.
Thank you to all who tuned in, to all who participated, to the organizers, like Lilly, and the generous sponsors who made this happen. It’s amazing to see what’s possible when patients have a proverbial seat at the table alongside medical professionals and digital health companies. Our voices matter and time and time again we’re being heard loud and clear.