It can feel like a bad break up. You build trust and rapport with a medical specialist who feels like family after overseeing your complex chronic health condition for years and then boom out of nowhere you find out they are moving away. Or maybe you’re relocating and trying to rebuild your dream team of health care providers. Whether this change is brought on by you or your care team it can feel a bit overwhelming to start anew.
My gastroenterologist of 8 years announced she was leaving on the Patient Portal in August. I was out running errands with my kids when a fellow IBD patient and friend texted me and shared the news. My heart sank and my stomach dropped, it never crossed my mind that she would ever leave. What do you mean SHE’S leaving? The doctor who finally got me into remission and has kept me there for nearly a decade. The doctor who oversaw all my family planning, pregnancies, and postpartum. The doctor whose rooted me on after each scope and always had an aggressive and thoughtful game plan no matter what twists and turns we face.
Unfortunately, this is the nature of the beast. I wrote a heartfelt “thank you” explaining my genuine gratitude for her efforts to always go above and beyond and all that she did to be extremely responsive and attentive to my needs. For the past 8 years when I send a Portal message, I always received a phone call from her—whether she was in clinic or on her cell. This time was different. This time there was radio silence and a one line canned thank you message from a nurse in the office. Just like that our worlds were not interconnected. I made a point to get my routine safety labs the Monday of her last week so that she could provide insight one last time. This time she didn’t comment on any of them and left September 15th without saying goodbye. It felt a bit like a slap in the face and stung.
As a chronic illness patient, we tend to feel a sense of comfort by care providers who help manage so much of our lives. This was a reminder to me that at the end of the day it’s a job for many and that even though we may feel that closeness, that bond may just be a façade. At the same time, I’ve also learned that some medical settings don’t allow doctors to communicate with patients, so who knows.
This week on Lights, Camera, Crohn’s I share tips for how I’m navigating finding a new GI that I think may help you along the way. I’m still feeling a bit lost and don’t know what the future is going to hold or what IBD Center I am going to land at, but I want to take you along for the ride.
The first steps to take
If a care provider is leaving the office or moving out of state, you will generally be placed with another doctor from the same team. This is not always a seamless transition though. Each doctor has a reputation. Some people want to be seen by a female care provider; others want a male. Years of experience and the college they graduated from and where they did residency may be of utmost importance to you. Just because the office says you can see “so and so” now, doesn’t mean you can’t speak up and advocate for what you’re looking for. In the realm of the healthcare world, you’re back to being “single” now and you can find who is the right match for you. Don’t feel pressured into anything. The long-term goal here is for a long-lasting relationship with a care provider who makes you feel like more than a number.
I have seen three different GIs in my 18+ years since my Crohn’s disease diagnosis. The first was incredible. I just so happened to meet him during my initial hospital stay, the day after I was diagnosed in the emergency room. He practices in my hometown (a Chicago suburb) and oversaw my care for a decade—even when I lived in Minnesota and Wisconsin while I was a news reporter and anchor.
When I moved to St. Louis in 2014 and my Crohn’s was flaring, I knew I needed to find a local provider. So once again, during a hospitalization for a bowel obstruction, I connected with the GI who was doing rounds at the hospital and loved his bedside manner. I felt safe and like I had found another great doctor. Unfortunately, while under his care I was very sick. We couldn’t figure out why my Crohn’s was so out of control. By the third hospitalization in 15 months, even while ramping up Humira injections to every week, and after several ER visits, his partner called me while I was in the hospital and said I needed an MRE to get to the bottom of what was happening. I did the MRE and was called back by that same doctor (not my GI) and he coldly told me over the phone that I needed a bowel resection—either the next day or in 10 days. He said I could go home and build up my strength. I chose to wait the 10 days. My actual GI never visited me in the hospital, never followed up…I knew it was time to drop him like a bad habit.
Enter in my most recent GI. Everyone raved about her. My colorectal surgeon and friends from the local Crohn’s and Colitis Foundation chapter all said she was the one to go to. So, I did…and now 8 years later I feel a bit stressed about starting the hunt for a great doctor all over again.
Amazing doctors can fall right into your lap, but sometimes you need to do some digging and research.
The behind-the-scenes work
At the end of the day, I find the most helpful advice comes from fellow IBD patients. There are several ways you can approach this.
Look up GIs in your area who specialize in IBD. This is key. You don’t want a run of the mill GI, if you have Crohn’s or ulcerative colitis you need a GI who specializes in IBD.
Check out online reviews and what people have to say about them.
Do a call out on your social media and see if anyone locally has any recommendations or personal experience. You want to hear the good, the bad, and the ugly. I have gained incredible insight this way. I had one fellow IBD friend message me about her experience with the provider I made an appointment with—and it made me a bit concerned. This week during my well woman visit, another IBD mom, who happens to work as a nurse practitioner in my OB’s office, told me about her awesome GI who is in the same group—so I plan to switch my appointment per her recommendation. This insight is GOLD.
Interview several GIs. Don’t feel pigeon-holed by only meeting with one possible new provider. Make a few appointments and see who jives the best with you. I have two appointments in January with two new GIs. My last clinic appointment was March 2023. I was supposed to be seen in October…that’s the soonest I can be seen.
Come up with a list of questions and see whose responses give you peace of mind and make you feel empowered to take on your IBD.
Be mindful of the office staff and how they treat you on the phone.
Make a pros and cons list of staying with your current GI team or starting fresh.
Decide if the doctor’s gender matters to you. I’ve had two male GIs and one female. I personally enjoyed having a female during my family planning and pregnancies, but now that my family complete it’s not *as* important to me, but still preferred.
To switch offices all your records and a referral will be needed by your current office, so make sure all your ducks are in a row and that the two offices have communicated. I made it clear with my current office that I am being seen by both IBD Centers, to see who is the best fit for me.
What questions to ask possible new providers
You may be wondering what to ask a new doctor or where to even start with your saga-long health history. We all know how rushed clinic appointments can feel. Here are some of the questions I plan to ask in January once we get the basic health questions out of the way.
How often will you be seeing me in clinic?
How often do you like patients to get labs? What kind of labs will you draw?
Will I keep my current medication regiment (ex. Biologic)? Will I stay with the originator/reference product biologic or are you planning to switch me to a biosimilar. Note: For you to be switched, your GI has to write a script for that to happen.
What days of the week are you in the clinic to see patients? If you have childcare or work conflicts, this can help so you know if their schedule/availability matches with your needs.
What hospital(s) do you treat at?
Are you apart of any research studies going on?
How often do you like patients to get a colonoscopy?
If I need pain medication to manage my symptoms, will you prescribe it? My last GI refused to—and I found that to be ridiculous.
Do you perform intestinal ultrasound here and if you don’t yet, when do you plan to?
If I run into insurance issues, will you go to bat for me and write an appeal letter or do what it takes to make sure I receive my medications on time?
Final thoughts
It’s jarring and takes a lot of time and energy to find a new provider but stay positive and know there are so many incredible gastroenterologists out there who genuinely care about patients and about helping our community out in any way they can. You are not civilly bound or married to your doctor—it’s not about hurting feelings or trying not to be a bother, be bold and do what’s best for you. I’m grateful to be in remission right now. My heart hurts knowing so many patients going through this same ordeal, while flaring, don’t have the luxury of taking their time or the privilege of living near an IBD Center with options. I always try and tell myself and I think this perspective will help bring you clarity, too—think of yourself at your sickest, lying in a hospital bed. Would you want that person leading your care? If there is any doubt or hesitation, keep looking for the right doctor for you.
It’s no surprise IBD impacts so much more than just our guts. Not only is there the gut and brain connection, but also the complex nature of our chronic illness(es) that can cause serious anxiety, depression, and mental health issues. The isolating nature of Crohn’s disease and ulcerative colitis, the unknowingness of what the next day holds, and the never-ending laundry list of procedures, labs, scans, and surgeries, year after year is a lot for any person to go through.
Even though I’ve lived with Crohn’s disease for more than 18 years, and have seen three different gastroenterologists in that time, not once has my mental health been brought up during a clinic appointment. When treating a person for IBD, the health of the whole person needs to be considered. I ran a poll on Instagram asking the IBD community if they’ve ever been to therapy. Out of 185 respondents, 70% seek therapy, 18% have not, and 12% are considering it.
I did an article in September 2020 about why a specific public bathroom at a grocery store I used to shop at triggers me and shared tactics for coping. You can read the article that featured Dr. Tiffany Taft here.
This week on Lights, Camera, Crohn’s we hear from those in our community about the advice that’s resonated with them the most since receiving their IBD diagnosis.
The words that have made a lasting impact
Olivia: “3% effort is still effort. You’re not going to be able to give 100% every day and that’s OK. Your best can look different from day to day.”
Julie: “It’s not your fault, you didn’t do anything wrong.”
Kristen: “You can’t drive forward if you’re always looking in the rearview mirror.”
Sarah: “Medical trauma is trauma and to give myself credit for all I have overcome.”
Cindy: “Remove all IBD related stressors from the bedroom to avoid impacting sleep. In our case, this meant no Humira injections for my daughter while sitting on the bed or nearby it.”
Tina: “Imitation is the best form of flattery.”
Lauren: “Don’t Google things you’re worried about, like symptoms.”
Jennifer: “Stay in the present.”
Heather: “Sometimes you just need to take a nap!”
Myisha: “If it’s not going to matter in five years, don’t give it five minutes of your energy.”
Kate: “It’s not your fault.”
Susan: “I’ve never seen a therapist, but I always tell myself it could always be worse.”
Stacey said: “You can’t control how seriously people take Covid. You can only control how you protect your physical and mental health. You have to put your health first. And, if people don’t agree with your choices, then that’s their problem. You can’t risk your health just to make it easy for others or to placate them. You come first in your life.”
Robin: “The “things” I do—my work advocating for others, supporting others, helping others face challenges with their diseases—I deserve that, too. Not from other people, but from myself. The beauty in therapy is that you’re receiving a non-biased/outsider opinion. This person that has no side and will sometimes say something you’ve heard 1,000 times in a way you’ve never heard before or even in a better way that allows you to really listen to what’s being said. To absorb it. Even to say it multiple times with no judgement if that’s what’s needed. Also, EMDR, which is a whole other thing and only part of the therapy experience.”
What is EMDR therapy?
Several people said EMDR therapy was their favorite and has been lifechanging. So, what exactly is it? Eye movement desensitization and reprocessing (EMDR) is a fairly new, non-traditional type of psychotherapy that’s popular for treating post-traumatic stress disorder. EMDR focuses on the natural tendencies our brains have for healing from traumatic memories. There are mental blocks (such as feelings of self-esteem issues and powerlessness) that can prevent us from healing. During EMDR, you are allowed to process the bad memories and experiences to start healing yourself. This helps our brains process challenging thoughts and feelings in a healthier way. Chances are through your patient journey you’ve endured several vivid and significantly painful moments that you haven’t been able to process and heal from.
Supportive Resources about managing mental health and IBD
There’s no doubt life with IBD brings on financial, social, and emotional pressure. These constant looming stressors can contribute to flares and unpleasant symptoms. This is where Project Crohn’s comes in. It’s a ministry that supports young adults with Crohn’s disease and ulcerative colitis. The main mission of this 501(c)3 non-profit, which launched in 2022, is to offer free access to mental health counseling, financial planning, and 1-1 mentoring. Anyone with IBD ages 18-30 is invited to apply for support programs that are possible thanks to generous donors.
This week on Light’s, Camera, Crohn’s we hear from the creator of Project Crohn’s and learn more about his mission to make a difference in the IBD community.
How Project Crohn’s came to be
Two weeks after John Christian Kuehnert’s 18th birthday, he started to experience intense gastrointestinal pains.
“It culminated in me passing out and being rushed to the hospital. A surgeon performed an emergency bowel resection, after finding a mass the size of a grapefruit on my intestines,” said John. “My surgeon saved my life, and I spent the next week in the hospital recovering. It took another eight months of slow recovery and meeting with gastroenterologists to discover I had Crohn’s disease.”
For the next 7-8 years, during college and after, John dealt with chronic pain that disrupted almost every aspect of his life. In recent years, he’s reached remission, but it took him a long time to get to where he is today.
“In college I started to see a clear connection between highly stressful situations and flare-ups of my disease. Sometimes, the internal pain would start less than a minute after being put in a stressful situation. Humira and 6MP have been crucial for me reaching remission. However, learning how to manage the primary stressors in my life has had a major impact on me reaching remission. I created Project Crohn’s to help others manage their stress and flare-ups more effectively,” said John.
The debilitating and unpredictable pain from IBD can lead to depression and anxiety and cause college students and young adults to have difficulty managing stressful coursework, while trying to juggle the debt from medical bills and college combined. John is determined to help ensure that no college students with IBD in the US face IBD alone. Project Crohn’s was created to provide the support his younger self could have benefited from.
Putting Mental Health and Financial Literacy in the Spotlight
Mental health is the primary focus of Project Crohn’s. The mind-to-gut connection is strong. This year, Project Crohn’s goal is to raise $100,000 to cover program costs for 25 young adults in the United States who are taking on IBD. Every penny from every dollar donated to Project Crohn’s is given to program recipients. By reducing stress and helping those with IBD learn to navigate life while managing their mental and emotional health, Project Crohn’s focuses on providing counseling and therapy services, while also building other helpful resources.
Here’s a look at the three main pillars of support that Project Crohn’s provides:
Personal mentoring: Ask helpful career-specific questions to help process challenging situations, while putting life’s crossroads in a positive perspective.
Financial advising: 1:1 virtual meetings to discuss your current and future financial situation, explore options, and suggest changes.
Counseling therapy: Promotes positive attitudes and develops effective coping strategies.
How to get involved and apply for assistance
You can apply for support directly on the Project Crohn’s website. It takes about 60 seconds. John wants people in our community to apply ASAP. Everyone who is accepted receives a scholarship, but currently, there are a limited number of scholarships available.
“We’re building a world where every young adult with IBD has full and free access to the secondary health resources they need to reach remission,” said John.
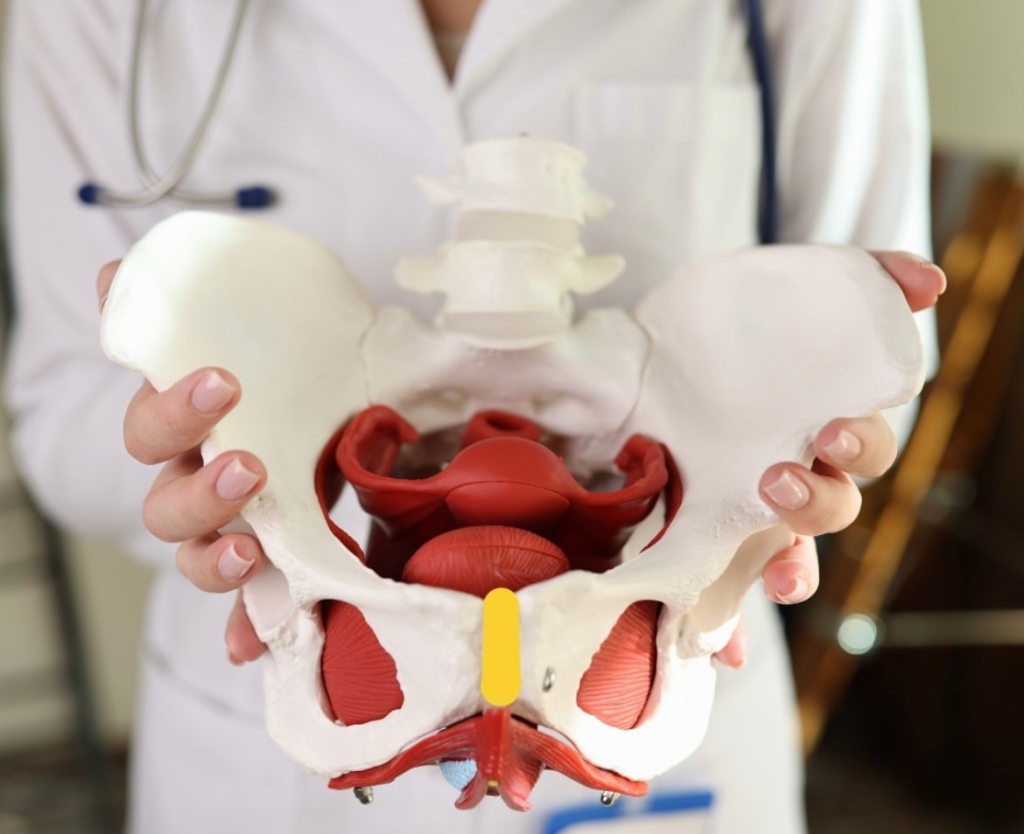
Chances are you’ve heard of Pelvic Floor Therapy but may not know what this entails or why so many people in the IBD community are talking about it. Individuals with IBD can have persistent symptoms of fecal incontinence, constipation, rectal discomfort, and diarrhea, despite having their IBD in remission with medical therapy. These persistent and often debilitating symptoms can have a major impact on your wellbeing and quality of life.
This week on Lights, Camera, Crohn’s we hear from two gastroenterologists from Mayo Clinic along with several IBD warriors who provide insight, helpful guidance, and information about pelvic floor therapy.
What exactly is Pelvic Floor Therapy?
Pelvic floor therapy is a treatment program performed by pelvic floor therapists to retrain the pelvic floor muscles to address underlying issues such as constipation, fecal incontinence, or urgency. Many patients with IBD in remission may develop pelvic floor dysfunction which is usually diagnosed from a digital rectal examination in combination with an anorectal manometry test.
“During an anorectal manometry, a small catheter with sensor probes and a balloon is placed into the rectum and is connected by a wire to the computer. During the test you are lying on your side and asked to perform maneuvers to determine how your pelvic floor muscles work. At the end of the test, they inflate a balloon in the rectum to help evaluate for sensation and then ask you to simulate having a bowel movement by pushing the balloon out,” explained Dr.Katie Dunleavy, MB BCh BAO, Gastroenterology Fellow, Mayo Clinic.
Based on normal values for your age and gender, you may be diagnosed with a pelvic floor dysfunction. Dr. Dunleavy went on to say that in IBD, there is less research on the benefits of pelvic floor therapy.
“But we have seen benefit in up to 80% for patients in remission who continue to have symptoms of constipation, urgency, or incontinence once active inflammation is fully ruled out. Similarly, some patients with IBD undergo total proctocolectomy with ileal pouch anal anastomosis (IPAA) may also benefit from pelvic floor therapy if they have issues emptying their pouch,” said Dr. Dunleavy.
Additionally, those with IBD who’ve had pelvic floor surgeries might experience sexual dysfunction and this type of therapy directed towards relaxation of the pelvic floor can lead to a better sexual experience.
Pelvic Floor Dysfunction does not discriminate across genders
Any person can develop pelvic floor dysfunction and may benefit from treatment with pelvic floor therapy in the right setting.
“While most studies describe pelvic floor in females, I believe individuals from all genders deserve evaluation of their pelvic floor the recommendation for pelvic floor therapy. Furthermore, individuals of a transgender experience, might undergo gender affirming surgery that impacts their pelvic floor muscles, and would benefit from pelvic floor therapy,” said Dr. Victor Chedid, M.D., M.S., Gastroenterologist at Mayo Clinic.
Dr. Dunleavy says, “As many as 50% of people with chronic constipation have pelvic floor dysfunction, which means there is impaired relaxation and coordination of the pelvic floor and abdominal muscles during evacuation. Some common symptoms include straining with hard bowel movements, a feeling of incomplete evacuation, pain with intercourse, or urinary symptoms.”
Certain risk factors make it more likely for men or women to develop pelvic floor dysfunction, this includes instrumented vaginal deliveries, chronic constipation with straining, prior surgery, prolapse, and age. It is important for men and women to discuss symptoms with their doctor to ensure they get the appropriate testing and treatment.
Apprehensive about getting looked at?
It is important for people diagnosed with pelvic floor dysfunction to seek out a qualified pelvic floor therapist who is specialized in GI and evacuation disorders. These are generally physical therapists or occupational therapists who complete extra training in pelvic floor therapy.
“You should find a therapist you trust and will feel comfortable with during your therapy sessions. The therapists who work in this area are fantastic and work diligently to explain what they will be doing. My patients tell me that the relief they feel from therapy well exceeds the apprehension they had prior to starting sessions,” said Dr. Dunleavy.
It’s important for patients to feel comfortable talking with health care providers and addressing concerns they may have on this topic. Dr. Chedid typically discusses the benefits of pelvic floor therapy with patients during clinic visits as a beneficial treatment option that does not require surgery. He provides patients with exercises and techniques to do at home that will have a major impact on general wellbeing and health.
“Individuals with IBD experience significant “negative” experience with the bathroom and with defecation that can be quite traumatizing, and therefore when they get in remission, they still have a negative association with the bathroom and might have “fear of defecation” despite being in remission. I equate that to “PTSD of the pelvic floor”, which is not a medical term, but an analogy I use. Therefore, pelvic floor therapy is essential to reverse this negative experience with the bathroom and make their bathroom experience a healthier and satisfying experience. Almost all patients who I describe this to get it right away and understand the importance of pelvic floor therapy,” said Dr. Chedid.
He adds that it’s imperative health care providers communicate with patients and ensure that the therapy session will be a safe space with at rained physical therapist who is trained in empathetic and trauma informed care. This is essential in putting a person’s mind at ease, as many patients might have experienced sexual trauma in their lifetime that makes pelvic floor therapy triggering for them.
The impact of Pelvic Floor Therapy post operatively and after IBD pregnancy
If you’ve had a total proctocolectomy and an ileal pouch anal anastomosis (IPAA), you might experience non-relaxing pelvic floor dysfunction or pouch evacuation disorder. This is similar to the rectal evacuation disorder in individuals with pouches.
“Typically, this is identified by history, physical exam, pouchoscopy, anorectal manometry and dynamic imaging of pouch evacuation. Additionally, someone who has had any form of trauma to the pelvic floor, including Perianal Crohn’s disease or surgeries for Perianal abscesses or fistulas or lacerations due to vaginal deliveries after pregnancy, these patient might experience rectal evacuation disorders after recovering and healing. In the proper patient, if identified by history, physical exam and the right testing, these patients will benefit from pelvic floor therapy,” said Dr. Chedid.
At the same time, there isn’t a lot of research on pelvic floor therapy in the post-operative state or following pregnancy in patients with IBD.
“There have been several attempts to find normal values for patients with IPAA who have undergone colectomy to help diagnose pouch related pelvic floor dysfunction. We generally recommend patients wait until the anastomosis following surgery is completely healed prior to having an evaluation with a balloon to ensure no complications. Similarly, patients who have recently undergone delivery from pregnancy will likely require time to heal. I would discuss this with your doctor to have more personalized information,” advised Dr. Dunleavy.
If your GI recommends pelvic floor therapy for your personal symptoms and struggles the overall response is tremendous.
“Recommending pelvic floor therapy to everybody, without identifying the right patient who would benefit from it is not typically beneficial. Therefore, in the right patient, pelvic floor therapy is extremely effective,” said Dr. Chedid.
What IBD patients have to say
Stacey has ulcerative colitis and went from having an ostomy to becoming a j-poucher. She’s a big proponent of Pelvic Floor Therapy. After her 3-step surgery to j-pouch in 2021, she knew she needed at least an evaluation from a pelvic floor physical therapist (PFPT) after urination became a challenge and inserting tampons became impossible during her takedown recovery.
“My surgeon wouldn’t write me a referral, citing that the anorectal manometry tests prior to surgery were all normal. My GI doctor didn’t want to go against the clinical judgement of my surgeon, so I couldn’t get one from her either, and finally I received a referral from my OB/GYN after explaining that penetrative sex was impossible (and felt unsafe to me) to even attempt,” Stacey explained.
These delays resulted in 5 months of significant pelvic pain that she felt ill-equipped and under-supported to handle, and this time could’ve been saved if she had gone into surgery with a referral to see PFPT from the get-go, even if she didn’t need to use the referral; it would’ve been nice to have.
“It’s so wild to me that orthopedic surgery has extensive PT rehabilitation protocols, and yet I was met with such resistance to gain access to the professionals who could help support my muscular recovery, even after such extensive GI surgeries,” she said.
During Stacey’s initial encounter with the PFPT, she spent the majority of the visit trying to gain a strong understanding of her entire pelvic and holistic health history, everything from sexual health to physicality to surgery, and all the in-between.
“She asked for consent prior to any invasive exams and explained them in thorough detail, reminding me that I was in control and could always choose to stop an exam if I felt unsafe. She continued to breathe with me during the exams and communicated her findings in real-time, which made me feel at ease. At the conclusion of our visit, I was told that I was experiencing hypertonic pelvic floor dysfunction from a decade of clenching for dear life trying to make it to the bathroom with mod-severe UC, even before my surgeries. The tightness of the muscles, coupled with three extensive pelvic surgeries, contributed to the pain and issues I was experiencing,” said Stacey.
During the visits with the PFPT, Stacey discovered she had no awareness of her pelvic floor muscles whatsoever. She could not distinguish the relaxation of the muscles from the contraction, and the entire area felt numb to her, like it was a holy, empty space. She says this made the exercises challenging to understand initially. She was prescribed specific exercises, not Kegels, including strategies to gain awareness of supportive muscle groups so she could begin to engage with this part of her body and start to heal.
“What I did not expect, however, was for this experience to be as enlightening and empowering as it was. Slowly but surely, the little life things showed me that they’re the big life things: being able to fully urinate in under 20 minutes, FINALLY being able to use tampons again- these were MASSIVELY important to my quality of life, and they became possible through the help and support of a PFPT and my adherence to their prescribed exercise regimen. I even realized one day while holding one of my exercise poses that I could feel the muscles DEEP in my abdomen! They felt heavy, full of pressure, as if they fired on to greet me, and then suddenly… I could feel them gently, slowly, RELEASE. I cried tears of relief realizing that I had been fearful of reconnecting with these muscle groups, and it really was safe and okay to be in my body.”
Stacey says she had NO idea these muscles existed, yet here they were. Had they been here all along?! She says she numbed them out from years of associating the deepest parts of her with pain from UC; and that her brain was protecting her. I truly wonder. All she knows is the day that she could FEEL her body experience relaxation and safety with FULL awareness of these pelvic muscles is the day that she knew that healing from these surgeries was going to be possible.
After one year of PFPT, Stacey “graduated,” not free of pain, but with the tools to know how to live within the ebbs and flows of pain. She tells me she still relies on the tools and bodily awareness that she gained through the experience.
Jessie was diagnosed with Crohn’s disease when she was 15 years old and after more than 22 surgeries later, at the age of 38, she says she completely underestimated how much her pelvic floor was affected over the years by the inflammation, surgeries, and her pregnancy.
“I was “guarding” badly (a response to pain) and so weak. I was having bladder issues, pelvic pain, rectal pain and so much more. After 2 years of being consistent going to pelvic floor therapy and doing the exercises I can say I’m about 85% better. I can’t say enough how much of a HUGE difference pelvic floor therapy made in my life and my IBD journey. My therapist explained it to me like this “you don’t have orthopedic surgery on your knee, wrist, ankle, spine, etc. and not get prescribed physical therapy. Same with an injury. It’s just standard procedure. But, for some reason, even though your pelvic floor consists of tons of muscles, ligaments, tendons, bone, etc. the same process is not considered – but IT SHOULD BE!” Your pelvic floor needs to be rehabbed after any injury, strain, surgery, etc. just like any other muscle/tendon/ligament/bone in your body,” explained Jessie.
Claire started PFPT because all imaging and tests showed that while her inflammation is under control, she still experiences extreme pain.
“I was tested, and they found I have dyssynergic defecation. This was caused by my chronic pain due to long-lasting fissures as well as chronic constipation. I’m grateful my GI thought to have me tested for this, as many don’t make that connection since the symptoms are so similar to Crohn’s. During PT, I have learned that my muscles do not relax and are constantly tense, so we work on trying to get them relaxed in order to successfully pass bowel movements. Like all other PT, one downside is that it is a lengthy process and takes up a lot of time. I have a one-hour appointment every week for 12 weeks and an hour or two of exercises and stretches on my own every day.”
She says she’s started to notice improvements and found ways to make her pain more bearable, though it’s something she will have to continue working on for a long time.
Tiffany has accessed pelvic floor therapy for herself and having previously been a physio and a fellow Crohnie, she recommends people speak with their doctors because it can make a world of difference, especially after surgery, hospitalization, or a flare.
“The neural connection we have to our trunk and pelvic muscles can be re-trained and strengthened, allowing less pain, and for me an improved sense of control over urgent bowel movements.”
Preslie was diagnosed with Crohn’s in June 2016, and after two years of battling severe symptoms, she had a colonoscopy that showed she was in remission. It may sound like lovely news, except Preslie was still living with a ton of pain, so her and her care team started digging for answers.
“This led to an Endometriosis diagnosis in August 2018. That was great news, except I STILL was not getting relief, and started having severe burning anytime I urinated, but always tested negative for UTIs. I went to a male urologist who told me I was just constipated, which was not the case. After well over a year of extremely painful sex, constant pain, and burning when I peed, I went to a urogynecologist who talked with me for less than 10 minutes and had the diagnosis: Interstitial Cystitis and Levator Ani Syndrome. I finally felt heard. I started pelvic floor therapy shortly after and immediately felt relief.”
Rocio says pelvic floor therapy was recommended to her by a home health physical therapist who was treating her for neuromuscular issues after bowel resection surgery for her Crohn’s in 2020.
“During my resection recovery, I was struggling tremendously with constipation, which was unfortunately always my issue with my IBD. Although uncommon, it’s been my reality for the last 20-plus years. The reason I share this is because I wish someone would have recommended pelvic floor therapy to me over all those years.”
She began seeing a pelvic floor therapist in January 2021 and completed two years of treatment. During that time, Rocio says she learned a lot about the intricacies of all the muscles, the nerves, the internal blood flow, and so much more. Because of two fistulotomies and a stricturplastly, she has numerous anatomical issues which prevent her from having normal bowel movements.
“Pelvic PT changed that completely and I have normal/formed BM’s every single day, without any signs of constipation and without any straining. I’ve learned ways in which I can help relax and release the pelvic floor should I face issues in the future.”
Separately, Rocio has learned how beneficial pelvic floor therapy is for many IBD patients post-operatively, including the ileal resection she had. Her therapist worked on her abdomen significantly during appointments to prevent adhesions and scar tissue. She says there are so many benefits to pelvic floor therapy that it does make her wonder why more IBD health care providers aren’t encouraging patients to pursue care.
Annie started pelvic floor therapy two weeks ago. She was referred based on suspected interstitial cystitis, not her IBD. She was shocked to learn during her first appointment that treatment was for all conditions that involve urgency of any kind.
“The game changer was the pelvic exam itself, I never realized what my PT noticed right away, which is that my first layer of pelvic muscles are unnaturally sensitive. This is massively helpful for IBD and IC, but the most validating part was having a lifetime of excruciating intercourse and painful pap smears and knowing the reason. My PT told me this is not how my life has to be. After just two weeks of exercising my pelvic muscles with a vaginal wand and daily targeted yoga, my urgency, both with my Crohn’s and IC, has gotten so much more manageable. I started this journey running to the restroom every 30 minutes (even at night), now I feel like I’m starting to get my life back.”
Jasmine says pelvic floor therapy helped her a ton following j-pouch surgery.
“I truly believe it should be integrated into post-op care plans, I had to seek it out and ask for it.”
Amy says that while she doesn’t have experience yet with PFPT, she has a complicated Crohn’s history for the past 25-plus years. Now that she’s over 40 and has had three vaginal births, she recently asked her doctor about pelvic floor therapy.
“Because of all the IBD women sharing their journey with this on the Internet, it inspired me to look into therapy for myself. In my first request, the response was that it might be a fantastic idea, but to wait and see. My next visit is in a couple of weeks and I’m looking forward to utilizing this article to share and take with me to help me advocate for myself.”
A look at the insurance piece
Yes, pelvic floor therapy can be covered by insurance, but it can vary based on the type of insurance. It is also important to ask about coverage for biofeedback therapy which is an essential part of the therapy based on prior research studies. Many insurance companies will need proof of diagnosis using an anorectal manometry with balloon expulsion test or defecating proctogram.
“If the proper indication based on testing is identified with the referral to pelvic floor therapy with a script written by someone’s GI provider, then typically insurance should cover it,” said Dr. Chedid.
Closing thoughts on Pelvic Floor Therapy and IBD
It is important to discuss with your doctor if pelvic floor therapy is right for you. Once patients with pelvic floor dysfunction have these basic tools, they can begin retraining the pelvic floor muscles with biofeedback. Biofeedback provides auditory and visual feedback to help retrain the pelvic floor and relax the anal sphincter. Biofeedback training is the treatment of choice for medically refractory pelvic floor constipation, with some studies showing improvement in more than 70 percent of patients. Patients also learn to identify internal sensations associated with relaxation and long-term skills and exercises for use at home.
At Mayo Clinic patients have had more than 70% response at 3 months following initiation of pelvic floor therapy. The response usually takes weeks to months to see a clinical difference and requires patients to practice their exercises and biofeedback at home.
“Although many centers are familiar with retraining techniques to improve pelvic floor dysfunction, few have the multidisciplinary expertise to teach patients with constipation how to appropriately coordinate abdominal and pelvic floor muscles during defecation, and how to use bowel management techniques, along with behavior modification, to relieve symptoms. Because pelvic floor dysfunction can be associated with psychological, sexual, or physical abuse and other life stressors, psychological counseling is often included in the evaluation process,” said Dr. Dunleavy.
If you have chronic pain, you may also need to see a physician to have these issues addressed prior to starting pelvic floor therapy.
Key takeaways from fellow IBD patients
PTs are an excellent resource, but just like getting an IBD-ologist is superior to a general GI doctor, PFPTs are an even stronger resource, ESPECIALLY in the context of chronic GI disease where so many of our deepest muscles are constantly working on our behalf.
You can always say “no thanks!” You don’t need to agree to any sort of exams or exercises that you’re not ready for, and a compassionate PFPT will empower you to make decisions and communicate in alignment with your body’s needs.
ANYONE can benefit from PFPT: any age, any gender.
Normalizing pain and discomfort is a survival instinct, but it’s not necessarily serving you for the GOOD life- it’s okay to get evaluated if you’re concerned about sexual pain or dysfunction, pain with periods, or if you also have IBD and simply want to be sure that you’re supporting your pelvic and spinal muscles the best you can so that you can, especially in the bathroom!
YOU get to decide! Having an evaluation may be all you have the capacity for, and that’s okay! You can return for a plan of attack later, or you can wait until you have the capacity to dive in head-first! There’s no one right way.
If you decide while talking to a PFPT before they do ANY manual evaluations that something doesn’t feel right- YOU GET TO CHOOSE, and you can always, always say, “nevermind”. Advocating for your body is always progression in your healing journey, every single time.
SPEAK UP! It’s RIDICULOUS that patients have to ask and ask and ask for the bare minimum, but if it helps your quality of life and it’s within your capacity- it’s certainly worth it.
A big deterrent for patients can be cost, but the investment is worth it, if you can swing it. You would be surprised how much every system of your body is so connected and feeds off one another!
Helpful resources to check out
Find a Pelvic Floor Therapist Close to Home
Utilize the “Section on Women’s Health” or the “Herman & Wallace” websites. Both these groups train therapists who specialize in pelvic floor disorders.
The Section on Women’s Health (SOWH) website has a “PT Locator” tab. You can enter search criteria including your geographic location (e.g., zip code) and specialty (e.g., constipation) to identify a therapist closer to home.
The Herman & Wallace website has a “Resources” tab under which you will find a “Practitioner Directory.” Use the map features to locate a therapist near you.
Utilize the “find a provider” section of www.pelvicrehab.com for a local PT by zip code.
The therapists who work with pelvic floor disorders may be in Gastroenterology, Urology, Gynecology, Physical Medicine, and/or Women’s Health, etc. You may be able to find someone through your local physicians or contacts.
For those in Canada, check out the Canadian Physiotherapy Association. It has a “Find a Physiotherapist” tab which allows you to connect with the sites of participating provinces/territories. By specifying a “Women’s Health” therapist or equivalent, you may find someone who specializes in the field of incontinence, pelvic pain, constipation, etc.
The benefit of pelvic floor therapy also involved patient education, relaxation exercises, diaphragmatic breathing, and correction of maladaptive toileting behaviors. Some studies have shown improvement in quality of life relating to symptoms, and mental health.
One of the worst aspects of life with IBD (in my opinion) are the side effects of the devil’s tic tacs aka steroids and what they do to your outward appearance. It’s a shock to the system to go from looking malnourished and thin to having a moon face and an insatiable appetite coupled with irritability, the shakes, acne, and insomnia. The weight fluctuations patients endure throughout their journey is a rollercoaster of unexpected twists and turns. Our bodies transform from being thin and sickly to healthy and in remission with weight we’re not used to. While IBD is called an “invisible” illness, our outward appearances take a hit more often than most might think. Those around us often compliment us when we’re “skinny” and stay silent when we’re a normal weight—this is detrimental because there is SO much more than meets the eye.
These photos are three months apart. Pre-diagnosis and on 22 pills a day (60 mg of prednisone).
This week on Lights, Camera, Crohn’s we peel back the layers of complexity regarding body image and self-esteem with IBD. Hear the candid commentary and often heartbreaking reality from 27 patients and caregivers.
The steroid struggle
I always know that after 3 weeks of prednisone my face and looks change dramatically. I went from someone with aspirations to work in TV news, on camera every day, to not letting my mom take pictures of me. I started in the TV business as a producer and once I was off prednisone and well managed, I got promoted to an on-air role, talk about messing with your head. I used to dread being a morning show anchor and returning to the news desk after being out for weeks. Nobody knew I had IBD or what my health struggles were, but they could see something was up. The calls to the newsroom and the comments were mortifying. I used to chew gum all day long while on prednisone to try and curb my appetite. My former GI told me to be careful doing that because the ingredient Sorbitol can cause stomach upset and diarrhea.
Katie: “The moon face with prednisone really did a number on my body image. I was in seventh grade and the kids and teachers would ask me what happened and why my face was like that. My school nurse, after I was out for two weeks because of a flare, came up to me and said, “Glad to see you, but honey, you look like crap.” I was in middle school when this happened, so I always just associated having Crohn’s with being ugly and that has been a long and hard battle. When you’re relapsing and you lose a lot of weight, people tell you that you look great, but when you’re healthy and in remission and you’ve gained weight back, people stop commenting about how good you look.”
Katie’s awful experience as a middle schooler inspired her to go into education. She is now a high school teacher. She says half the reason she went into teaching was to make sure students who have chronic illnesses, or who were absent, had someone who could empathize with them and just try to make sure that the experience never happens to anyone.
Danielle: “Prednisone destroyed my body image. When you look in the mirror and don’t recognize yourself, it’s really an emotional experience. In so many ways, prednisone is amazing, it got me out of my flare, but it turns my face into a swollen balloon. I can’t look at pictures of myself during that time. I am always so self-conscious when I’m on prednisone and feel like everyone can see it. IBD does many things, one of which is controls how you look which is a difficult part of the disease. I just got married and am in a minor flare and I delayed starting budesonide because I didn’t want to risk any moon face.”
Ross: “For me, what’s had the biggest negative impact is the side effects of steroid use, specifically back acne. This developed the first time I took steroids for my Crohn’s six years ago and it still has never gone away. It has had such a negative impact on my body image even though it’s not something anyone would really see. It has stopped me from taking my shirt off during summer months in public, or I’m self-conscious of having my top off at the gym changing room or even around friends or anyone I was dating. It’s something that I would almost always be conscious of these last six years. Even now, when it’s not too active, the scars and pigmentation and redness would stop me from taking my shirt off or make me very self-conscious around other people. I don’t think it will ever go away. It used to get me so down when I was already struggling with flare ups, etc.”
Laura: “Long-term steroid use was the most damaging for me. I was unrecognizable to myself and to others. I never found much support for those body changes and the mental health impact from ‘roids.”
Chanel: “I have struggled much more with weight gain from steroids and other medications than I ever have with the weight loss that is oftentimes common in IBD. Many informational graphics and articles out there about IBD always mention weight loss, but never the issue with weight gain. I’ve always had an unhealthy relationship with my body image because of the constant weight fluctuations due to medication.”
The fluctuations from being thin to gaining weight
I’ll never forget back in 2012 noticing that I was getting thinner and thinner by not eating any differently or increasing my physical activity. I was a morning news anchor at the time in Springfield, IL and I remember weighing myself each morning and seeing 1-2 pounds drop off each day…for weeks. At the time I wasn’t very well informed about IBD and didn’t realize that was a sign I was flaring. I was in my late twenties and gearing up for a trip to the Dominican for a childhood friend’s wedding. To be honest, I was happy, and I liked how my sickly body looked.
Fast forward to 2015, I was engaged and had bowel resection surgery. I had never weighed more than 127 pounds in my life and had dropped to the teens when I was unwell. My first post-op appointment with a new GI I gained seven pounds, and I wasn’t happy about it. My GI said, “this is what happens when you’re healthy and finally absorbing nutrients.” When you’re planning a wedding, healthy weight gain hits a bit differently.
Ever since then, I’ve been in remission and I’m so grateful for that, but my weight has been something I think about now—not only because of my IBD being in check, but after having three kids. My self-confidence and how I feel about my reflection in the mirror has taken a blow as the years have gone on.
Madison: “ When I was in a severe flare in 2020 after being diagnosed, I dropped 20 pounds unintentionally. I was normally around 127 pounds and during my worst flare I was down to 107 pounds. It was absolutely horrifying. I was devastated. I remember going to American Eagle to buy shorts in a 00 size because none of my clothes fit me. I felt sick and looked sick, which made everything 10 times worse. Not being able to eat food and constantly running to the bathroom in pain led me to be malnourished. I remember being at my GI appointment when we were trying to figure out a treatment plan and my nurse said after taking my blood pressure, “Madison are you eating?” I started to cry to her and said “everything hurts me. I can’t eat.”
While Madison was growing up, she always thought being thin was attractive. After being so severely sick, she now personally affiliates being thin with being sick.
“Being on prednisone to help was both a blessing and a curse as it helped get my flare under control, but also led to unwanted weight gain in my face, which makes me super self-conscious, especially in pictures. I know that side effects are temporary, but it can really hurt someone’s self-esteem.”
Fast forward to now—three years later, Madison is on a treatment plan that works for her and she’s proud of her body. She says she looks forward to being weighed at the doctor and at infusions appointments just to see a healthy weight.
“Weight and IBD is very fluid, and I constantly remind myself to give my body grace. When you’re losing weight on top of being sick, it can be detrimental to your mental health. You look in the mirror and see someone you don’t recognize.”
Ashley: “I’ve kept three different sized sets of clothes with my ulcerative colitis. My normal size, a smaller size for when I’m extremely sick, and a larger size for when I’m on prednisone. I’ve always been super self-conscious about my body size because a lot of time it’s out of my control. I also feel self-conscious when I’m so sick and lose weight and people comment about how good I look. I’ve felt guilty because I didn’t work out to “earn” that body. Then, I’ve felt frustrated because it made me mad that to look a certain way that got me compliments, I had to be extremely sick and unhealthy. Now, I have a permanent ileostomy. I am more confident in my body than I have ever been. I think that’s mainly because I’m so healthy now and I have more control over my body and life.”
Danielle: “So many things come to mind. I was 14 when I was diagnosed, and while I was sick prior to being diagnosed, I was judged for being too thin and accused of being anorexic or bulimic. Then upon diagnosis, I gained 30 pounds in 2 weeks from prednisone. At 14 years old, I was swollen and chubby and self-conscious. Since being diagnosed, I haven’t struggled with being “too thin” again, but with weight gain from prednisone and other medications. I’ve been told far too many times that “anyone can lose weight by eating right and exercising” but it’s not that easy with a chronic condition. Some mornings, I’m so fatigued and achy, I can’t get out of bed, and it takes my energy to get ready for work. My diet is extremely limited as I had a bowel resection and I’m allergic to dairy products. So, I live off protein and carbs which are not ideal for weight loss or even maintenance.”
Amber: “I have been on Stelara and have reached remission, but the thing people don’t talk about is after being in constant flares, you have no idea how much weight you might gain because of not flaring. It is a great thing and I’m so happy to be in remission, but now I must learn how to work on the nutrition aspect of it all. To be honest, all these years of being sick, I never had to worry about weight gain. I had to worry how much weight loss affected me and most people do more posting about that. Not the up sides of remission, but also what we do now to get onto a new lifestyle change. We have to learn a whole new way of nourishing our bodies.”
Stephanie: “I have found that when I’m flaring at my worst, I lose weight from not being able to eat and my body not retaining anything that I eat. I get so many compliments about the weight loss, but it breaks my heart because I might look good to others, but I’m at my sickest.”
Jennifer: “It’s crazy to know how jarring it can be to see your weight fluctuate so much so fast. Diagnosed with UC about a year ago and went through a huge flare, lost like 35 pounds. I hated looking at my body because I was under 100 pounds as an adult woman. Fast forward to now and I’m back to my “normal” weight, but still have issues with how my body looks as weight came back. It’s softer and less toned than before. I’m sure it’ll get back to the place where I was, but what if it doesn’t? Our bodies can go through so much and I’m thankful for its resilience, but the mental toll the fluctuations can be a lot to try and manage and reflect on as we navigate this journey.”
Louise: “I’m newly diagnosed and dealing with my second flare. I worry about the impact it has on me mentally because I am happier with my body when I’m very ill, and unhappy with it when I’m on steroids and feeling better. It can’t be good for us. Negative comments (from my mother!) when my face gets chubby on steroids and compliments from people when I’m not eating and very unwell are difficult to process. I get angry when they compliment me on how well I look just because I’m skinny, because I feel like it minimizes how bad things are and how unwell I am. I also like it because I like being slimmer. It is so messed up! When I get my appetite back, I try to fight the cravings and then binge and then feel awful for it. I have never been this way pre-IBD. I was always fit and healthy and in control of my relationship with food. There’s also a weird part of me that wants to look thinner because it’s an invisible illness, I want people to see how unwell I’ve been, so they don’t think I’m lying.”
Louise said it felt good to let it all out and that she’s never said any of this. Coping with big health issues comes first, but this annoys her during quiet moments. Her sentiments ring true for so many of us.
Myisha: “I struggle with body image a lot. I’m naturally 127 pounds, but with prednisone I got to 210 pounds and no longer recognized the person I was staring at in the mirror. I cried for weeks unable to recognize myself. I still cry now and I’m down to 139. My clothes still don’t fit, and I still have clothes that are a size 12-14 because I know that prednisone is an ongoing possibility and that I might get back to that size if I have a bad flare.”
Jessie: “The constant weight fluctuations have always made me self-conscious. It messes with your head too because when you lose weight from a flare, people say “oh my gosh you’re so skinny you look great, what did you do?”…but then when you gain weight (from medications not from becoming healthier) no one comments and you’re just self-conscious about it.”
Celia: “Before I was diagnosed, I was happy with losing weight. I was 13 and hated my body. I remember I had my diagnostic colonoscopy and the day after I took a picture of my stomach, it was as flat as it’s ever been. I felt good about how I looked, but keep in mind I was barely 100 pounds and 5’5’. I felt awful and I was tired all the time. As I started Humira and was gaining weight, I missed my old (very unhealthy) body. I constantly am reminded by loved ones that this weight gain is good. I just returned to the weight I was pre-symptoms almost 4 years later and I feel good overall! I still struggle with how I look and have developed a connection between food, weight gain and loss, and pain from Crohn’s that I still need to work on, but I’m doing my best. As a 17-year-old, we all tend to struggle with how we look, and I need to remember all my body has been through and done for me.”
Kindra: “Along with IBD, I also have Primary sclerosing cholangitis (PSC), so when I flare or I’m unwell, I lose weight and I can’t do anything to keep it on. I will eat all day long and you can count my ribs and see all my chest bones sticking out. I get compliments from people who don’t know me well about how thin I am/how they wished they could eat like me, and I never quite know what to say. When I am healthy and can gain weight and I have to shop for bigger clothes, I get a complex thanks to years of the American media diet culture.”
Leah: “I feel like weight gain after a flare has been challenging. All the body yo-yo and knowing the weight coming back on is so healthy and just what your body needs, but I believe it can be tough at times.”
Kelly: “I’m scared to go below a certain weight in fears of having a flare, but on the backside, I feel unattractive for my partner and fight with self-image.”
Bloating is a bitch
Even in remission, bloating is one of my main IBD symptoms. I often tell my husband, friends, and family, “you can physically see my pain right now. Feel how hard my stomach is. I look like I’m 5 months pregnant.” The reaction is always one of shock, raised eyebrows, and a bit of sympathy. Because of this I usually wear elastic waistbands or dresses. You’ll rarely ever see me wearing pants or shorts with a button. When I used to work in corporate America, my Crohn’s was out of control, and I would repeatedly have to unbutton my pants in the board room and lean back in my chair during meetings with co-workers. It was humiliating, but I always tried to make light of it. It’s amazing how we can wake up with a flat stomach and have a distended belly that truly looks like there’s a pregnancy going on by dinner.
Courtney: “Being emaciated from poor nutrient absorption, but bloated from gas and inflammation at the same time can lead to a confusing relationship with food. I don’t think it’s quite the same psychology as an eating disorder, but when eating causes you pain, or makes you literally change your pant size pre and post meal, it can be easy to want to postpone meals if you have plans, eat little in social situations, and can create an unhealthy relationship with food. Food is not the enemy, it’s a necessity—it’s all about finding the proper treatment and lifestyle to manage your IBD.”
Courtney adds that living with an ostomy is a huge adjustment with major impacts on how you perceive your body and appearance.
“My first ostomy was such a shock to the system. It feels almost surreal to see a piece of your intestine outside your body. If you have no control over output timing, which can leave you feeling broken and helpless during bag changes. It wasn’t until my second ostomy that I was able to recognize and be grateful for the benefits it affords me. I now live a healthy, active, pain-free life and couldn’t be more grateful.”
Patti: “My everyday bloated belly is like a giant dark cloud that blankets my self-image. I really try to embrace the rest of my healthy body and be grateful that I’m able to leave the house and do some functional activities and can sometimes hide my ugly belly if I’m completely emptied out, but my typical mantra is that I look disgusting because of my belly. I know this is negative thinking and messes with my mental health, but after dealing with Crohn’s for the past 51 years, I’m not sure I can ever stop that thinking.”
Alyson: “Bloat makes a girl feel AWFUL. Add in intestinal dysmotility with Crohn’s and I literally start the week at a size 8 and end in a size 10. Then we just switch to those wide leg pants with the elastic. Prior to my diagnosis, I never had to unbutton pants before or after eating. Now, it’s the first move the second we get in the car to leave because, ouch. It really makes you feel cute.”
Alannah: “For me weight fluctuation is my biggest struggle. One week I’m slim with minimal bloating then the next I’m bigger and bloating more. My partner has always struggled with confidence with his stoma due to weight gain even though he’s perfect as he is. He will never go without a top off ever.”
Naima: “Bloating is the worst. I am getting married in three weeks and I’m so worried about being bloated or gassy or having a minor flare. It’s hard to feel pretty when you can’t control how your body is feeling. Some days I feel strong and look lean—other times I hate how I look.”
Post surgery swelling, scars, and ostomies
Sabrina: “I’ve struggled with my body image after being diagnosed and going through three surgeries in a matter of two years. Seeing myself with a bag was hard and the changes that came with post-surgery swelling, scars, and fluid buildup. Body image and my new body will always be something I struggle being comfortable with.”
Mark: “I’ve had Crohn’s for more than 37 years and in that time multiple operations. I have many scars, but they are a part of my life and badges of honor in my constant battle with this disease. My IBD has thrown everything at me including short bowel syndrome, liver failure, osteoporosis, broken vertebrae, septicemia, lymphoma, coma, hepatic encephalopathy, and the list keeps growing. When I see my scars, it reminds me to keep fighting. Crohn’s will not win or stop me from living a full life. If someone asks me about them, I don’t hide. I tell them it’s battle scars. Body image is important to me, and it reflects how strong I am, and no one can take that away. I’ve worked all my life and traveled the world. This year (one year after coming out of a coma) I’ve been on a Pole-to-Pole journey.”
Martin says body image is both how you feel and how you look to others, as well as yourself in the mirror. In his early days post-diagnosis, as a young adult starting a career, he felt anxious and angry, but looked normal.
“Post surgery and with time came the additional stress of looking and behaving differently and additional comorbidities that accompany IBD. This included dental and bone issues. I was hugely lucky to have found my lifetime soul mate before my Crohn’s became active, illness and surgery haven’t changed anything for us. I have been various shades of ill with Crohn’s all my adult life and it hasn’t helped self-love, including self-image on any level. I survived and thrived because of my family’s support and very little real-world commentary on my body from others, although I sometimes preempt this by joking about looking like Homer Simpson these days. I now face further life changing surgery and I worry about the impact of my quality of life on my family. I no longer care about how others see me.”
From a caregiver perspective
Cindy: “My daughter is so deeply at war with her body, and I know thanks to chronic illness it’s so much more complex than simple teenage-girl-in-the-age-of-Insta feelings of “I don’t like my shoulders” or “I should watch my calories” (both of which are things she thinks). It is rooted in a real fear of and discomfort with her body and what it puts her through. She has so many years to live in her body and I wish more than anything I could give her peace with it…the same relative peace and confidence I have always had with my body. I just can’t relate.”
Keyla and her teenage son have IBD: “The struggle is real. Not only do we have a condition that there is stigma about, then we have constant weight issues, scars, bruising, and so much more that leaves us with body image issues. Our bodies have been through enough and done so much for us. Let’s care for it, nourish it, nurture it, and be kind to it.”
Taking on body image one day at a time
Focus on strength and resilience. Recognize your ability to navigate through challenges and adapt to changing circumstances. Once you’ve been through the flare and recovery process once, you know what to expect. Find comfort in knowing you’ve done this before and know most of the unpleasant side effects are temporary.
Seek support. Surround yourself with a strong support system of family, friends, or support groups who understand and empathize with your experiences. Sharing your thoughts, concerns, and emotions with others who have similar experiences (hello online IBD fam!) can help you feel heard and supported. Surround yourself with people and media that promote positive body image and self-acceptance. Be selective in the content you consume, ensuring it supports a healthy perspective and challenges unrealistic beauty standards.
Educate yourself. Learn more about IBD and its impact on the body. Understanding the reasons behind changes in your body and recognizing that they are a result of the disease, not a reflection of your worth, can assist in developing a more positive body image.
Practice self-care. Engage in activities that promote self-care and boost your self-confidence. This can include hobbies, exercise, meditation, or anything that brings you joy and helps you connect with your body in a positive way. Oftentimes our fatigue can hinder what type of daily activity we feel capable of, take everything in stride and don’t overdo. Start with a 10-minute walk and build up from there. The fresh air and simple movement will do wonders.
Focus on what your body can do. Shift the focus from how your body looks to what it can do. Appreciate the functionality of your body, such as its ability to heal, fight illness, and carry you through daily activities.
Reece was diagnosed with Crohn’s disease in 2014. Since then, he’s endured countless surgeries, flares, and setbacks, but chooses to focus on the beauty his life still bestows despite the challenges.
“I’m a shell of my former self, but I am okay with it. I’m grateful for my life. I have people who love me and care for me. When I look in the mirror, I see a fighter. All of the marks and scars are just evidence of my battles. It was not easy to get here, but here I am. I will never be the person I was before Crohn’s, but my disease has taught me so much about myself and life.”
Communicate with your healthcare team. Discuss any concerns or insecurities related to body image with your healthcare team. They can provide guidance and offer resources to support you in addressing these concerns. Therapy may help you cope with these struggles and provide helpful tools for living with the uncertainties and challenges.
Remember, your worth is not defined by the physical changes caused by IBD. Surround yourself with positivity, celebrate your strengths, and prioritize self-care to foster a positive body image and improve overall well-being. Most importantly, after reading this I hope you feel seen and realize that your struggles and insecurities are not unique to you.
There’s not a magic bullet for helping us cope with these insecurities, I know it can be a daily challenge. I truly believe we are our own toughest critics. If family members or friends compliment you when you’re unintentionally thin, respond by saying it’s because your IBD is out of whack. Speak up and inform those who have no idea what’s going on in your mind, with your body, when you look in the mirror, get on a scale, or have to think about how your outfit choice could impact your physical symptoms every day…it’s a lot. You are beautiful. You are strong. You are capable. There’s no one like you in the world. Your body, no matter the size, is working overtime with IBD, please take a moment to show yourself and it, some love.
To receive biologic infusions at home or within a medical setting? That is the question. As an IBD mom of three who has done self-injections for 15-plus years, it’s intrigued me to see how many people in the IBD community now receive at-home infusions. This inspired me to dig deeper and hear firsthand what fellow patients have to say about their experience. When polled on Instagram—out of 260 votes, 55% of IBD patients prefer at home infusions compared to 45% who would like to receive their medication in a medical setting. This week on Lights, Camera, Crohn’s hear advice, guidance, the role insurance plays in all of this, and perspective on treating your IBD at home versus at an infusion clinic or hospital. I learned a lot and I think you will, too!
Discussing Home Infusions with your Care Team
If receiving your infusion at home interests you, here’s what you can do to get the ball rolling on making it happen.
Talk with your GI about whether home infusions are an option in your area and if they feel comfortable with you doing so. Discuss the risks and benefits. Your GI will need to write a prescription.
Call your insurance and make sure home infusions are covered in your health plan.
Amanda has been doing Remicade infusions at home since the pandemic started and she says it’s been much better for her. Being able to receive her medication at home and cuddle with her 4-year-old daughter and dog are big wins for her. Recently, she also receives daily IV fluids, and thanks to her Port and home health, she’s been able to do it herself.
Amanda: “Home infusions have changed the game for me. They make me feel safer as someone whose immune compromised. I almost always have the same nurse, and I don’t have to commute before or after. How grateful am I!”
She says how you coordinate setting up home infusions is dependent on your insurance. Personally, after talking with her insurance she found a list of home health agencies within 30 miles of her house and called and spoke with a few.
“Some did not administer my medication, some charged separately for nursing fee, and some were not taking new patients. Once I found a good option for my family, the home health company reaches out to your GI doctor, who then sends the script to the Specialty Pharmacy, rather than to an infusion center.”
When Bad Veins and IV issues Set You Back
One of the main reasons I chose to do a self-injection rather than an infusion was because of how horrible my veins are. When I was told I needed to start a biologic during a hospitalization in July 2008, it was the same hospitalization where it took three people and eight tries to start an IV on me. To this day, I’m still a bit fearful of getting IVs because of that traumatic situation. Several people wrote to me with the same concerns—this is something to consider if you typically need a Vein Finder for hospital visits and procedures.
Olivia: “I initially loved the idea of doing infusions at home. My first one went smoothly, the nurse had a bit of trouble finding a vein and drawing blood, but no problems after that. The ability to do my infusion in my bed or on my couch was so much more comfortable than the hospital! But then, the next two infusions, the nurse had trouble getting a vein and one had to be rescheduled because of hospital policy. That infusion took over an hour to find a vein. After that, we spent a month trying to convince insurance to let me go back to the hospital so I could use the ultrasound to get IVs placed. Ever since, I’ve been doing infusions at the hospital. The idea of doing infusions at home was nice, but it didn’t work for my situation.”
Meredith: “I get my Entyvio infusion at home. I don’t love it. It is more convenient than having to go to the hospital/office, but nurses often have trouble starting IVs on me and at home they are the only option. There is no backup and I’ve had a few bad experiences. Things have gotten better because I now have in my profile that I need pediatric needles, but they aren’t the standard, so those types of needles are not always supplied. The insurance decided for me that I would receive my infusions at home because it’s cheaper and since I’ve never had allergic reaction. The service by me is different, but there is no future scheduling. You know around the date that your next infusion is and then you’re contacted one day beforehand with a time. I’m too high strung to be comfortable with that, but it is what it is.”
Much like Amanda, Meredith loves having her dog there for support. When she initially started getting home infusions her dog needed to stay outside the room because she was too interested in what was going on, but now she’s used to the process and equipment and can snuggle.
Heidi: “My insurance made me switch to home infusions. At first, I was nervous because I’m a hard stick and always require a vein finder. I also just felt safer in a hospital setting. But, I’ve been doing home infusions for three years and I love it. I have my “old faithful” vein and I like being in my own home with my own bathroom and other comforts. I also have wonderful nurses whom I look forward to seeing each time. Everything is so much more personal this way.”
Melissa: “Sadly my veins are awful, and I wouldn’t want to chance the one person who comes not being able to get an IV started.”
Concerns from the Community Regarding Home Infusions
Ashley: “With my ulcerative colitis, comes other chronic illnesses. Which is true for a lot of people in our community. I have POTS, so having my infusions done in a healthcare setting is more reassuring for me because there’s more safety nets in place.”
Emilie: “I don’t get my infusions at home anymore (I used to!) because I hated it. The nurse was always texting me to reschedule, I was always having to deal with CVS trying to get my medication delivered on time, and I had to store all the stuff. It also made me feel like a “patient” in my own home. Mentally it was incredibly stressful organizing and coordinating everything and feeling like I was constantly sick because the medical equipment was always around. I much prefer going to an infusion center, where I just show up and they have everything ready to go. Just another perspective—I know a lot of people love getting infusions at home and I’m in the minority, but there are cons to consider.”
Mary: “I don’t currently do an infusion medication, but I have in the past with Remicade. My GI office set home infusions up for me after I did the first few in the office. It was more convenient for me due to the office being about 1.5 hours away from where I live. I was provided with an IV pole to keep at home among other supplies and a nurse came to my house to do the infusion. It was awkward at first, but after a few times it got better. Unfortunately, during one infusion, I had an allergic reaction unexpectedly, during which the nurse had to give me Benadryl and another medication. After that happened, I couldn’t do them at home anymore and had to go to the office. After two more infusions, my GI discovered I wasn’t responding to Remicade anymore and I had to switch to Stelara. The cons are the risk of something happening and not being in a medical setting. Luckily, I had a great nurse who knew what to do.”
Adam: “I prefer the clinic and the reason is, when I was on Humira and had to self-inject, I always worried I didn’t get it in the right spot or the full injection and miss some of my medication. For me, it’s a piece of mind that my infusion is done properly.”
IBD Moms Experience
Miranda was diagnosed with Crohn’s during the height of the pandemic. When she started Entyvio it was in an infusion center, and she felt like she was putting herself and her family at risk each time she went in. By receiving infusions at home, you can potentially be exposed to fewer hospital-acquired infections. This is especially important for individuals with compromised immune systems, as it helps minimize the risk of additional health complications.
“I saw a few ladies (connections on Instagram) who were receiving home infusions, so I asked my doctor about it. He said it would be no problem to connect me with a company in Dallas that handles nursing and medications for in-home infusions. My only obstacle was seeing if my insurance company would approve home nursing. After calling them to go over benefits, my insurance informed me I could receive in-home nursing. I did have to escalate the call to get it pushed through. At the end of the day home infusions were approved. The same company that ships my meds provides nursing. I do have to make a phone call every January to make sure coverage is good, but other than that it’s a flawless process. The nurse and I are close friends.”
Christina: “I specifically told my GI I don’t want to get infusions at home because I like my “me” time in the infusion clinic. Two hours to read my Kindle in peace! I also decline the accelerated rate…perspective changes when you have kids. My nurse jokes they’re my spa days!”
Krista: “I moved to home infusions once I had my daughter. It was more convenient because I didn’t have to find someone to watch my daughter (I had nobody to help or to ask) so that I could attend my infusions. I had a pleasant experience, and the nurse was fantastic. Being able to do infusions in the comfort of my home was fantastic, especially needing an infusion only 2 weeks postpartum, while recovering from a c-section.”
Getting adjusted to receiving medication without support from fellow patients in the room
Kristi has been receiving Remicade at home monthly since January. Her GI office stopped doing infusions at their office due to staffing issues. After a time or two at the hospital-run infusion center, her insurance company called her to see if she’d be interested in home infusions. Since she had been driving an hour each way for years, she jumped at the chance!
“The idea of not having to worry about getting my infusion during a winter storm was enough for me. My doctor’s office was hesitant at first. I was always on board with the idea, and I was shocked to see the cost was similar to my doctor’s office but significantly less than an infusion center. Home infusions have allowed me more flexibility in scheduling. I also feel like my resting period post-infusion is much easier since I’m already home. While I love home infusions, there are some downsides. I don’t think I would have wanted this back years ago when I started infusions. There’s a lot to be said about the community and the support I received just by being in an infusion room with similar patients. It was also nice to be in my doctor’s office monthly, where I could easily report any symptoms, I was having health wise. I am the person that needs to have my house looking perfect before company comes over, so that adds an extra level of stress during an infusion week. It’s also a bit odd to have the nurse here for so many hours. However, I’ve had two nurses so far and they’ve always been very good and very respectful in my home and if I wanted quiet time. Overall, I don’t think I could go back to going somewhere.”
Kristi says now that she doesn’t have the infusion room support, she relies even more on the social media community and the IBD family online. She also loves getting to snuggle with her dog and use him as a heating blanket while she receives her infusion.
Final Thoughts
Balancing the risks vs. benefits. As you’ve read, home infusions are not a one-size-fits-all approach. What works for one person, doesn’t for another. While the benefit of being at home is a big one, having to worry about the sole nurse at your house finding a vein and not knowing if you’re going to have a bad reaction are just some of the cons that can make the experience worrisome for people.
The convenience of home. Home infusions offer the convenience of receiving treatment in the comfort of your own home. This eliminates the need to travel to a medical facility and allows you to maintain your daily routine more easily. For IBD parents and caregivers it alleviates the need of finding childcare. By fitting infusions into your daily life, it helps to reduce the disruption that may come with hospital or infusion center visits. So many of us deal with medical PTSD and having the comfort and familiarity of home can help to ease that burden a bit.
Kat: “I received home infusions for years for UC. My doctor’s office got them set up because I live in a rural area. The pros were the convenience and being in the comfort of my home. The cons were having a stranger in my home for over an hour. Dealing with the company’s billing department was also horrendous.”
A more personalized treatment experience. You can have a dedicated healthcare professional who gets to know you and your specific needs, creating a customized care plan to address your individual symptoms and concerns. Many IBD people I speak with have a close bond with the nurse who visits their home and feel supported during the process.
Jill started on Humira and was later switched to Remicade infusions. She started receiving infusions at the hospital and then her GI recommended she try home infusions to limit exposure to germs.
“My GI’s office took care of the paperwork and I had the choice between two home health companies. This has been a game changer for any guilt I felt around missing work, because the nurse comes to my home and I can continue working on my laptop, if needed. Or I schedule infusions to begin at the end of my work day. I have a great relationship with my home health nurse and she knows me and my veins so well now. I value the relationship and level of care as well as the flexibility I have found with this option. It’s a win for my mental health as well.
Matt received home infusions for seven years. If he could pass along any advice, he says to be even more proactive about your health.
“I had to always coordinate shipments, supplies, and the infusion schedule. The pros are the flexibility and comfort, but the cons are not being at an infusion center where you can unplug and be in your own thoughts.
It’s important to discuss the option of home infusions with your healthcare team to determine if it’s a suitable choice for you. Your care team can address any concerns or questions you may have, educate you on the process, and help you make an informed decision. Remember, you have options and support to manage your IBD effectively, even when it comes to receiving necessary infusions.
Lights, Camera, Crohn’s: An Unobstructed View is officially SEVEN years old! If you told me when I started blogging what a labor of love this website would become for me, I never would have been able to imagine what it would become for my life, for the IBD community, and for patient advocacy efforts. I went into blogging blindly. I had no clue how to format the site, but I knew the types of stories I wanted to share and the messages from patients that I wanted to get across.
As a seasoned journalist who spent nearly a decade as a TV news anchor, reporter, and producer, I’ve used my love for storytelling to try my best to be the voice I so desperately needed to hear upon diagnosis, through my professional life, finding love, family planning, pregnancy, motherhood and beyond. It’s been quite the ride these last seven years. My first article went live July 23, 2016, on the 11th anniversary of my Crohn’s disease diagnosis. I found out I was pregnant with my now six-year-old, two days later. The first six years of Lights, Camera, Crohn’s (and 3 kids later), I shared a new article every single Monday.
Through these seven years, Lights, Camera, Crohn’s has been viewed half a MILLION times, by more than 320,000 people around the world. On this site alone, I’ve shared 368 articles, which does not account for the countless other IBD articles I’ve created for other websites. As I reflect on this milestone, I’m proud of what I’ve accomplished thus far, but know there’s much more work to be done.
This week I want to give you a behind-the-scenes look at how my storytelling process comes to life—I often get asked “how do you become a patient advocate?” and “how do you start blogging?” I hope this advice inspires you to take the plunge, as there are endless seats at the proverbial advocacy table and your voice, your story, your valid experiences, deserve to be heard.
Choosing What’s Newsworthy
It can be overwhelming trying to come up with content that is new and fresh for your blog and social media. I’ve found it extremely beneficial to have an editorial calendar that helps guide the stories that I share. My editorial calendar is in my email in the draft folder. I simply list out the dates (articles have always been shared on Mondays on Lights, Camera, Crohn’s…so I list out all the Mondays for the next 3-4 months). This serves as a reminder of my game plan and when I need to do outreach for the stories.
As a journalist you’re taught and it’s almost innate in some ways to always be on the lookout for a story. I’m always keeping my eye out for tweets and posts on Instagram, conversations in real life, experiences that happen to me when I see my GI or get a scope, that I think will resonate with our community. I think about the pain points I’ve felt along the way and the advice I wish I had when I was struggling in certain moments. I think about the questions I’ve had along the way when Google was scaring the bejesus out of me, and I just wanted real life advice from someone who understood my reality. Think about what uncertainty, questions, concerns you’ve had and what you want to learn more about and then go after the story.
Writing for the Reader
Everyone has a unique writing style, but one of the most common “mistakes” I tend to see with blogging is when writers go on and on and on about their own experience. The articles sound more like a diary entry—and if that’s what you’re going for, great—but usually, you’re wanting to draw readers in. To do this, I use my own experience as a foundation—a sentence or two in the intro and then the rest of the article is written to and for the reader. Try to write your blog articles like a news story. Use sub heads, get reliable sources, attribute studies, share credible information. Give readers in the chronic illness community news they can use. Empower others on their patient journeys so they learn something by checking out your content. Let others see that they are not alone in what they are going through and that you get where they are coming from. By including the expertise of medical professionals, it helps your articles really come to life and allows you to build a rapport and a reputation with the GI community. It’s always incredible to hear when a GI shares Lights, Camera, Crohn’s with their patients.
If you’re unsure how to reach a GI who is not your doctor, I advise going on Twitter and sending doctors a DM asking if they’d be interested in providing input for an article you’re working on. 9 out of 10 times you’ll get a yes. As we all know, doctors are busy, so try and give them a longer lead time to respond to interview questions. I like to include a headshot when I quote a doctor, so I have them send you one.
My Patient Experience articles have become one of my favorite parts of Lights, Camera, Crohn’s—these articles are a major labor of love. I interview 10-20 patients, along with physicians, and spend upwards of 20+ hours out of the goodness of my heart to create a resource that a patient and caregiver can have at their fingertips when they’re trying to make major decisions about how they choose to manage their disease. Topics range from biologics to infertility or life with an ostomy. Rinvoq is coming up next, folks…I just need a breather since I finished writing Skyrizi earlier this month. By crowdsourcing and sharing the good, the bad, and the ugly I’ve been able to provide a complete look at the reality patients face and provide background that shows more than just my experience.
The Art of Interviewing
Whether you’re interviewing a fellow patient or a healthcare professional, the same process goes a long way. Try thinking about the main points of the article and the flow before you write the questions. You almost must think backwards. I do all my interviews over email—for multiple reasons. The number one reason, is that as a mom of a 6-year-old, 4-year-old, and 2-year-old, I don’t get many breaks and trying to conduct an interview over the phone or Zoom and capturing the true essence of what someone is saying is nearly impossible. I also prefer email because it gives people a chance to articulate their responses and enables me to accurately share their quote—word for word, without paraphrasing. I rarely give interviews over the phone, as I like fellow writers/editors/journalists to have what I’m saying verbatim.
When I send the interview email for Lights, Camera, Crohn’s, I provide a deadline in bold and then list the questions. I always ask for a high-level explanation of a person’s patient journey so I have an understanding of what they’ve been through and so I can paint a clear picture for the reader. Try to never ask “yes” or “no” questions—you want people to give good explanations and descriptions.
An example of email outreach to a pediatric gastroenterologist for an article I worked on.
Often the most important question you can ask if “Anything you’d like to add?”—in TV, podcasts, you name it, this is when people let loose a little bit and can provide you with key nuggets of information.
Once I receive the interview responses, I open up Word, and take all the content and start compiling what’s going to be a quote and what’s going to be a part of my wording/storytelling. Then, much like journalists do in TV news, I write the story around the quotes.
Have a Copy Editor (aka family member/friend review your content)
It’s always helpful to have an extra set of eyes on your articles before you share them. Since the day I launched Lights, Camera, Crohn’s, my mom has been my “copy editor.” I email her a draft of the article along with an explanation of what I’m hoping to get across and then she goes through each article with a fine-tooth comb and provides edits and feedback. If I get too fired up about something, she may politely advise I take a certain line of the story out or re-think how I word a sentence. She’s been my voice of reason through this entire process and as my mom, she’s my biggest cheerleader in not just life with Crohn’s, but everything. As a nurse of more than 40+ years, she’s also well versed in medical situations, as well as grammar.
Be Vulnerable and Transparent
Despite how many people advocate for IBD, Crohn’s and ulcerative colitis still have stigmas. It can be daunting to put your words down on paper and share them with the world. I spent the first decade of my disease just telling close family members and friends. What I’ve found since blogging and being a vocal patient advocate, is that by being open, you open yourself up to endless support and camaraderie. There is such strength that comes from saying you’re not ok or need help. Tell it like it is and don’t sugarcoat your story. At the time same, one of the main pillars of my advocacy has to always been to be transparent, while also positive.
Back in the day when I was diagnosed, and those first 10 years when I was living in silence, most of the content I read was pretty doomsday. While I understand and empathize with the pain and horror Crohn’s can cause in one’s life, I’ve tried to never sit in that sadness for long. If anything, IBD has given me perspective and clarity about the fact that IBD doesn’t have to destroy your life or who you are. Yes, it can create major complications, unpredictable setbacks, and hurdles, but those detours don’t have to rob you of what you hope to accomplish or become. While it’s important to be real, I find it just as important to provide hope and inspiration for those who wonder what their futures may hold.
Keep on Swimming
Due to social media algorithms and the lack of engagement many of us see online, it can feel disappointing at times when you put all this effort into an article or a blog and feel like you’re talking or reaching no one. I’ve been there countless times. Don’t let the “likes” or the follows deter you. Know that your words and your stories just need to get into the hands of one person who needs them, and that makes all the effort, time, and energy worth it. Your articles have legs—meaning that once you post them, continue to post, and share for months and years to come because these “evergreen” articles are always timely and necessary. Try to collaborate with others when you can. If news outlets reach out for a quote or if a health website asks for your input, give it—and then ask for your blog to be a part of how you’re attributed in the quote. If you see someone’s Instagram story referring to an article topic you’ve covered, grab the link and send it their way over DM.
If you feel like you’re in a rut or if you’re having a tough time creating content—don’t force it. Ask your followers what topics they’d like you to cover. Use the timing of the year to help come up with stories (for example, navigating diet around the holidays or back to school time and being an IBD teacher). Support the content of fellow advocates—comment and share articles that intrigue you and help others get their words out and the same will be done for you. Rather than seeing advocacy as a competition, view others as your ally—we’re all doing this to help others, spread awareness, drive research, and together we can truly amplify the patient voice—one article at a time.
There’s no telling what Lights, Camera, Crohn’s will look like seven years from now, but I don’t plan to stop storytelling anytime soon. Thanks for all your kind words, for telling me when my stories have touched your life or helped you make a tough decision, and for being there for me when I need support. If you’d ever like to collaborate with me to share your story or if you have a topic you’d like me to write about—please don’t hesitate to reach out.
Here’s to another seven years of breaking stigmas, spreading awareness, and making everyone in the IBD community feel seen.
When you hear the word “Skyrizi,” you may think people are referring to an up-and-coming rapper or something fun, but in case you didn’t know, Skyrizi (risankizumab-rzaa) is a biologic drug that was approved to treat Crohn’s disease in June 2022. With the medication only being around for IBD less than 13 months, finding patient experiences wasn’t as “easy” as previous articles I have covered on Lights, Camera, Crohn’s about biologics, but I learned a lot writing this and I think you will gain a better understanding of Skyrizi after reading this, too.
Some background on Skyrizi
Skyrizi was previously approved for moderate to severe plaque psoriasis and active psoriatic arthritis. It’s worth noting that Skyrizi is the first treatment for Crohn’s that targets the interleukin-23 (IL-23) protein, which is responsible for inflammation in our bodies. By going after IL-23, Skyrizi helps reduce inflammation that can contribute to Crohn’s symptoms.
When it comes to dosing, patients receive an intravenous (IV) infusion that lasts about an hour at week 0, week 4, and week 8, followed by a self-administered subcutaneous injection with an on-body injector (OBI) at week 12 and every 8 weeks after that. This whole OBI situation is incredibly intriguing to me. I’ve been doing Humira injections for 15 years (!) this week, so I’m used to self-injecting, but knowing technology like the OBI exists gives hope to people who are fearful of needles and having to give themselves a shot. We’ll get into more about the OBI and what fellow patients have to say later in the article.
As far as safety, prior to starting Skyrizi, it’s advised that your GI order lab work that looks at your liver function. If results come back abnormal, this may not be the right drug for you. If you are in the family planning stages, pregnant, or breastfeeding, speak to your doctor. You can also enroll in the ongoing PIANO study, which looks at the safety and efficacy of IBD medications during pregnancy and beyond. Since Skyrizi is so new to the game, research is needed to help pave the way for IBD moms and their children.
Let’s hear from the patient perspective
Prior to starting Skyrizi in February (2023), Stelara failed Stéphane. I’m always careful with how I word this—and I wish all patients and healthcare providers would be conscious of not saying “the patient failed” anything—at the end of the day, it’s the drug that fails us. Stéphane says he didn’t start feeling a response until this month (July)—just before his second OBI (on-body injection). Although his calprotectin started to respond positively in May.
“The good is that I’ve responded and feel better. The bad is that we don’t know how long my response will last or how much it’ll stop inflammation and the formation of strictures. I’ve responded to Remicade, Entyvio, Stelara, but I’ve also developed strictures and had surgeries on all of them. I can hope that Skyrizi won’t continue this dire and disappointing record.”
Megan says before she started Skyrizi she was on the path to an ostomy. Entyvio had failed her, and she was experiencing perianal Crohn’s symptoms that were keeping her from being the mom, wife, and employee she wanted to be.
“My medical team and I decided to start Skyrizi and plan for a temporary ostomy to help my symptoms while we waited for the medication to take effect. After my second Skyrizi infusion, I noticed significant improvement in my symptoms! My bowel movements were more regular, there was a decrease in drainage from my setons, and I had less pain overall. Given my positive response to the medication, we were able to table ostomy surgery. I was extremely relieved and grateful that I had such a quick response to Skyrizi.”
Maha went on Skyrizi after the biologic she was on failed her after six years. As she was reeling from the reality that the biologic that had put her into clinical remission could suddenly not work anymore, she was hesitant and nervous about how to decide the next treatment options.
“After reviewing all of my options with my doctor, I chose Skyrizi based on data and evidence, and also on a gut feeling that this might be the right next step. I’m happy to report that I was right, and in the time that I’ve been on Skyrizi, I’ve achieved a state of remission I could only dream of, with no side effects!”
Elizabeth was in the clinical trial for Skyrizi. She says the biologic “changed her life.” After fighting a Crohn’s flare for seven years, it’s been the only medication that’s wrangled her disease under control.
Kelly started to flare last Fall, because of a loss of response to Remicade (infliximab). Her gastroenterologist suggested Skyrizi as an option that aligned with her drug priorities: namely safety and efficacy.
“The drug has very good data behind it, and she had heard of excellent response in the clinical trials. But it was very new to GIs across the US. It was a gamble, but one that we both thought was worth trying.”
Unfortunately, Kelly dealt with significant problems and delays with her prior authorization and needed to use the AbbVie Bridge Program to get her first infusion dose covered.
“My insurance company used my participation in the Bridge Program as a reason to deny my coverage for the drug. But AbbVie anticipated this issue and has several support programs that cover longer use of the drug and help with deductibles until insurance companies change their policies about drug coverage. I strongly believe that the months of stress and anxiety and daily hours-long phone calls to try to get this drug covered and delivered seriously exacerbated my flare symptoms,” said Kelly.
This cat and mouse game is something far too many of us can relate to. It’s sickening and ridiculous what chronic illness patients have to go through month after month, just to receive medication on time. Kelly was constantly anxious and worried about whether her Skyrizi would be covered.
Kelly tells me her first two infusions were easy and that she had almost zero side effects aside from very mild fatigue, like her normal Crohn’s baseline.
Kelly’s final Skyrizi induction infusion
“My third infusion was a little heavier hitting, like how Remicade infusions felt: a pronounced bit of fatigue, headache and brain fog that lasted less than a day. It was very tolerable. I didn’t have to premedicate before the infusions either, although my doctor had started me on budesonide to try to control the inflammation and keep the flare from getting worse while we waited for the Skyrizi to kick in.”
Cassandra says this is her third biologic and the whole experience in and of itself has been a bit nerve wracking. She lives in Canada and was the first to receive Skyrizi in her city.
“I didn’t love being the first, having the nurses learn on me, not knowing what to expect was difficult as I typically try finding online forums where others share their experiences. So far, I feel ok with it. Skyrizi hasn’t gotten me into remission, but we will see how it goes!”
The OBI (On-Body Injector)
Like anything new, getting used to a new medication and the mode of delivery can have a bit of an adjustment period. You wear the device on your thigh or abdomen for 5 minutes while the medication gets into your skin.
Kelly – “The neat thing about Skyrizi is the Obi, or on-body injector. It’s a brand-new device that is halfway between an infusion and an injection. It’s a small rectangular device with adhesive on the whole back that sticks to your leg. The needle in the device is tiny and I had zero sensation or pain. The button to trigger the needle is large and doesn’t have the same kind of chunky CLICK that the Humira pens do, which was nice and felt less aggressive and intimidating. Because the device infuses the medication into your body over several minutes, it uses an electronic pump. This means you cannot wear your fitness device or Apple watch or have your phone anywhere near it while you’re doing the injection.”
Kelly says she expected to have difficulty with the adhesive since it covered such a large area of skin and was strong. Other than mild discomfort while peeling it off (like taking off a band-aid), her skin didn’t have any other reaction.
Stéphane-“The written instructions for Skyrizi make the self-administering with the on-body injection unnecessarily complicated. I counted 33 warnings of what not to do, something that just generates anxiety. In fact, it’s simple and easy and the Skyrizi video they provide on the website is far more confidence-inspiring and useful.”
Stéphane says it’s helpful to watch the video after reading the instructions. He says the video is good at stripping the process down to essentials and showing that the injection process is in fact easy.
“The front of the thigh is simpler than the stomach because it naturally offers the flat, smooth, easily accessible space you need to place the injector. You clean the small end of the vial, stick it into the injector so it clicks, close injector door, clean area of skin, take the two strips off the back (top first), place it on your thigh and press down the adhesive, then press forcefully on button of injector,” he said.
Jessica made the switch to Skyrizi after being on Stelara. So far, she hasn’t experienced side effects and the medication has kept her Crohn’s in remission.
“The new on-body injector technology is weird and takes some getting used, but overall, it’s painless. It’s just been a little complicated to learn. If there’s a lump on your skin after you take the injector off. She says it goes away. While the needle doesn’t hurt, Jessica feels as the medicine goes into your system you start to feel more pressure.”
So far, Megan has completed two OBIs at home. She says the OBI is extremely easy to use. She’s done Humira, Stelara, Cimzia, and methotrexate in the past and says the OBI for Skyrizi is the easiest and least painful.
“I like to head to a secluded area, so I don’t chance my son trying to wrestle or play and accidentally knock it out of place. (IBD mom hack!) While I still have hard days and I’m not symptom-free, my hard days are much less frequent than before starting Skyrizi!”
Cassandra-“The OBI is amazing. I have been getting IVs monthly/every other month for 9 years, so to not have to get an IV has been wonderful. I have grown to really hate them and have had some bad experiences getting IVs so to not have to face that has made a world of difference. The OBI is so simple, so quick, and relatively painless (though I have felt some slight pinching/stinging). All in all, it’s very simple and I find the mechanism very innovative and cool! I haven’t had any side effects yet, aside from injection site swelling and redness the day of.”
Maha-“The best part is the ease with which I can do my Skyrizi injections via the on-body injector: it’s painless, quick, and honestly I forget that I have to do them until my next injection rolls around.”
Benefits of utilizing the Nurse Ambassador Program Much like other biologics on the market, patients can tap into the free Nurse Ambassadors on hand to help ease the transition to Skyrizi. These nurses provide invaluable guidance and comfort every step of the way. Not only is utilizing these programs beneficial for patients, but also caregivers who may be helping to administer medication.
Kelly-“The device is so new, and the instructions can be long and a little complicated, but AbbVie has a nurse ambassador program that is free for all patients. I cannot recommend the program enough. My nurse ambassador came to my house before I even received the first infusion dose and answered all my hundreds of questions about the expected side effects, the rate of response, and showed me a demonstration with the OBI. It was helpful to get comfortable with the training device. My nurse ambassador also showed up to my house for my first injection and walked me through each step and was excellent at providing support.”
Natalie started Skyrizi infusions in May, 2 infusions down, 1 more to go before she starts with the OBI. She says while she hasn’t experienced huge benefits yet, she’s still hopeful. This is her first biologic and she’s appreciative of how helpful the AbbVie nurse has been through the process.
“I am still pretty new to this myself, but talking with the Skyrizi nurse has helped a great deal, especially getting their co-pay program and just having someone to check in on you.”
Jessica– “AbbVie has an amazing support system, and you can always have a nurse ambassador visit you in person or Facetime you. When I FaceTime the nurse, she guides me through it. Just talking to her while the injector is on for five minutes has made a difference.”
Cassandra-“I live in Canada, so things may be different elsewhere, but Skyrizi is the first biologic where I was sent a “Welcome package” which had a little health/wellness goal setter, appointment tracking sheets, a large needle disposable cartridge for my used injectors, and a mini cooler with reusable ice packs. I was super impressed, and it was fun and cute to receive. I have used the nurse ambassador a few times, especially at the beginning. It’s nice to ask questions or voice concerns with them. Having a nurse ambassador gives me peace of mind.”
Maha-“I really appreciate AbbVie’s commitment to patient education and support through their Skyrizi Hub which provides insurance specialists, nurse ambassadors, and an on-call line to help with any medical or financial concerns! My nurse ambassador walked me through my first injection and has followed up with me regularly to check on my progress both in terms of clinical symptoms and also quality of life!”
Struggling with the “newness” of being a biologic the first year it’s approved for IBD
Kelly ended up flaring badly between her third induction infusions and the fourth dose (her first at home injection). She met with her GI several times, discussing what to do. Since Skyrizi is such a new IBD drug, there really isn’t any extensive anecdotal evidence or patient stories about whether it be worth it to continue the drug, or if she would be considered a “primary non-responder.”
“We struggled with what criteria to use to determine if I just needed to wait longer or if I needed to switch drugs. My GI reached out to the Skyrizi sales rep for their practice and was told not to give up on the drug before 24-26 weeks because clinical trials did show that a non-trivial number of outliers did capture response to the drug later than the expected 8-12 weeks that was seen with most primary responders. At 14 weeks, I could tell that I wasn’t seeing any response to the drug because I was tracking my symptoms, daily bowel movements and pain. It was helpful to have that data to show us in black and white that I wasn’t doing well.”
Looking at the reality of the data and watching her symptoms escalate and her inflammation creep higher and higher despite the steroids and Skyrizi, Kelly and her care team made the decision to discontinue Skyrizi and move to another drug.
“It’s hard to hear from so many medical professionals that a drug with only about a 40% response rate is considered a raving success in the GI community. For me, that’s an enormous number of people who did not respond to this drug. I wish very much I had been one of them, because it’s scary and upsetting when you burn through a drug and cannot go back to it in the future because of possible antibody development.” says Kelly.
Ultimately, the decision to try a medication is a highly personal decision, one that should be made well-informed and jointly with your GI healthcare provider.
Maha says, “My experience with Skyrizi has affirmed that there is hope in all the new therapeutic modalities that are coming out, and that they can offer patients a strong quality of life while delivering treatment as minimally invasive as possible.”
Interested in reading previous Light’s Camera Crohn’s Patient Experience articles about other biologics?
Raise your hand if you’ve ever been blindsided by an IBD flare. My Crohn’s has landed me in the hospital with zero warning on several occasions. The unpredictability of IBD is a huge challenge we all face. But what if a wearable device could signal when our disease course is going off the tracks? What if we had warnings long before we were face to face with our next flare?
An ongoing “Stress in Crohn’s” study out of Mt. Sinai’s IBD Center in New York and The John Radcliffe Infirmary/Oxford University in the United Kingdom has been investigating this since February 2021, with the help of 200 participants. The study wrapped up in June 2022 and was conducted in partnership with 4YouandMe and funded by a grant from The Leona M. and Harry B. Helmsley Charitable Trust to 4YouandMe.
The goal? To empower those with Crohn’s to monitor stress responses and early signs of impending illness worsening in between clinic visits, while providing a means to navigate life and mitigate the consequences stress has on our disease journey. While stress has long been known to somehow affect our IBD, the details of the relationship are poorly understood.
This week on Lights, Camera, Crohn’s we hear from an IBD mom and educator who recently participated in the Stress in Crohn’s study in hopes of taking action to help advance our knowledge of diseases like Crohn’s and ulcerative colitis.
The mission of the Stress in Crohn’s study
Wearables such as smart rings, smart watches, and smart scales, along with our phones, can collect information emanating from us. They can record our physiology and our routines that we are learning to weave together into “clinical symptoms”- such as fatigue, sleep, and stress.
“The main mission of 4YouandMe (nonprofit) is to empower individuals to navigate their own health by using wearables and apps while sharing their own health related data and insights for the benefit of all. This desire was birthed after working at Apple on their Special Projects team and grew out of asking “why can’t the data that emanates from each of us come back and help each person improve their health on a daily basis”,” said Stephen Friend, President 4YouandMe(nonprofit) , Visiting Professor of Connected Medicine, Oxford University.
Tina Aswani-Omprakash, MPH, Wearables Research Coordinator at Mount Sinai’s Susan & Leonard Feinstein IBD Center & Patient Advocate/Founder of the blog ‘Own Your Crohn’s’ says the promise of wearable devices in the prediction of IBD flares and drug response is real and something she’s excited about.
“As we know, IBD can be a progressive disease and it is important to shut down inflammation quickly to prevent complications. The wearable studies at Mount Sinai’s Susan & Leonard Feinstein IBD Center are looking to develop algorithms using measures such as heart rate variability, sleep duration & quality, essentially autonomic/ parasympathetic nervous system fluctuations via data collected through wearable devices. The hope is to help predict IBD flares and showcase drug response utilizing wearable device signatures,” said Tina.
Meet Nicole, Stress in Crohn’s study participant
Nicole Pavlin became a patient at the Mount Sinai IBD Center in New York and received an official diagnosis of Crohn’s disease of the ileum and jejunum in 2021, but her symptoms began more than 16 years prior. At the time Nicole was just beginning her teaching career and she was focused on raising her family. Once Nicole received her IBD diagnosis, she would often search GI research publications to better understand Crohn’s, along with the treatments and procedures available to patients.
“By educating myself about the disease, I’ve been able to communicate more efficiently with my healthcare team and advocate for my needs. The opportunity to participate in IBD research is always exciting to me, especially since the results could potentially help patients in the future,” said Nicole.
Nicole chose to participate in the “Stress in Crohn’s Study” from July 2021 to May 2022, which captured a period of time when her IBD symptoms took a turn for the worse. Nicole had bowel resection surgery that involved the removal of 6 inches of her ileum, including her Meckel’s diverticulum.
Getting recruited for the Stress in Crohn’s study
You may be wondering how Nicole got involved with this study. A Clinical Research Coordinator from the Mt. Sinai IBD Center reached out to Nicole to see if she’d be interested in participating. The researcher told her digital devices were being used to learn the relationship between Crohn’s disease symptoms and stress to try and predict the onset of flares.
“I was given detailed information about the study and instructions on downloading the app. The researchers provided me with an Oura ring, an Empatica EMBRACE wristband, and a Bodyport scale. I completed various surveys and tasks within the Stress Study app each day. Whenever I had a bowel movement, I would note the characteristics of the stool on the Pooply app based on the Bristol stool scale. The Rescue Time app was optional, and I chose not to use that one,” Nicole explained.
Daily points were awarded for wearing the Oura ring and Empatica wristband, using the Bodyport scale, answering survey questions, and completing tasks on the study app. Nicole received extra “boost points” for using the devices multiple days in a row.
“Every two weeks I gained points for completing a video diary and a cognition task. About five times during the study, I completed a Calprotectin stool sample at home through the IBDoc app. I had a support team and check-in calls each month to answer questions about my mental health and medications. There was also a study visit every three months to complete additional surveys about my health and Crohn’s disease.”
By the end of the study, Nicole earned more than 20,000 points for completing these tasks and eventually received 5 stars for being a “Groundbreaking Contributor” to science. She says the point system was a big motivator and a fun challenge. The study lasted 9 months. Nicole was compensated $400, and she got to keep the Oura ring.
Wearables provide a “new voice of objective data”
Up till now, those with chronic diseases have had to use their memory and feelings to convey their diseases. The wearables offer a new voice of objective data for themselves and for their physicians about what precisely occurred.
“In this study of Crohn’s disease, we were more interested in unlocking the link between stress and flares in Crohn’s. This is part of a larger set of feasibility studies to build for individuals a “Stress Load Navigator” for we note a tight connection between not just inflammatory bowel disease, but also diseases as diverse as diabetes, heart attacks, arthritis and even Alzheimer’s,” said Dr. Friend.
Marco Altini, Founder of HRV4Training, advisor at Oura, and Guest Lecturer at VU Amsterdam, says recent advancements in wearable technology are making it possible to move away from the lab and monitor our physiology continuously, in real life, when and where it really matters.
“In the context of many chronic conditions, the ability to monitor our own, individual changes in resting physiology over long periods of time, and in relation to symptoms or other makers, could finally help us better manage our health,” said Marco.Devices such as the Oura ring can monitor accurately resting heart rate and heart rate variability over time. These signals are tightly coupled to our stress response, which is often an important part of the picture when managing our health.
Participating in research as an IBD mom
Since there is a genetic component to IBD, Nicole says she worries that her children could show signs of the disease in the future. She’s been very open with her children about the challenges she’s faced with the disease.
“I want to model resilience for them so they can see how to navigate difficult situations. By participating in research, I want to show them that we have a chance to use these challenges to help others and make a difference in the future.”
Nicole says it’s encouraging that wearable devices could potentially predict the onset of flares, which might offer faster treatment to prevent the escalation of inflammation and disease progression.
The importance of contributing to IBD research
Nicole’s hope is that by sharing her experience, it will inspire others to participate in IBD research and encourage more funding for these types of initiatives.
“Our research contributions as chronic illness patients have so much potential to benefit others in the future. This study was fascinating, and it was truly a pleasure to participate in the research.”
She says by taking the daily surveys and performing the tasks, it made her feel like someone was paying attention to her struggles.
“It gave me an incentive to be strong, thinking that my challenges could be helpful to IBD research!”
Nicole’s final thoughts on wearable devices
Wearable devices present a great opportunity for patients to monitor their health and provide feedback to healthcare professionals. “Since the study, I’ve continued to wear the Oura ring, and it’s been especially helpful to follow my progress as I rebuild and strengthen my body. Each morning I can check my readiness level to see how my heart has recovered from various activity levels. My sleep analysis has also been helpful for establishing a healthy sleep routine.”
The Oura ring has captured periods of strain on my body, and I can often tell when I’m getting sick with slight elevations in body temperature and resting heart rate. “During my Covid infection, the ring app even showed a fever spike along with elevated heart rate. I’ve also been able to monitor episodes of tachycardia with the help of the Oura ring and a KardiaMobile device, which is a single-lead portable EKG connected to a phone app. In addition, we have a pulse oximeter at home to monitor heart rate and oxygen saturation.”
With so much information to collect on our health, these devices can be overwhelming and anxiety provoking. “During the study, I was constantly monitoring my symptoms which led to a hyperfocus on my disease. Weighing myself each day also contributed to anxiety. Each time my weight dropped a little bit, I got worried and discouraged. The constant focus on weight can also contribute to issues with body image, and I’ve since decided to just weigh myself at medical appointments. For anyone considering wearable devices, it’s very important to keep moderation in mind.”
When we step out into the world, we need navigation tools. The same goes with wearable technologies. Soon, we’ll be able to use the data taken directly from our own bodies, during our day-to-day lives, to follow what is happening and help us to better navigate our own health paths. According to Dr. Friend, last year almost half of American adults were wearing some form of smart watch, and as of Spring 2022 more than 90% of smart watch users state they use health related apps to follow their health.
Interested in becoming a citizen scientist like Nicole? Learn about additional research opportunities:
In the future, Nicole plans to contribute to the Mount Sinai Million Health Discoveries Program which aims to understand how to treat different diseases in patients of all races, ages, and genders. She has also been invited to collaborate with Nutritional Therapy for IBD whose mission is to improve the lives and outcomes of patients with Crohn’s disease and ulcerative colitis through evidence-based nutrition.
Closing thoughts
The information collected from wearables can be a gamechanger for us as patients. Many of us call our doctors or go to the ER based on symptoms, but if we have remote monitoring via such devices, we could perhaps prevent this disease from spiraling. Kudos to Nicole and the many other research participants who are helping to push the needle and change the future of what it means to live with IBD.
“To me, that’s not just hope. That’s the future of managing this disease better and truly owning our Crohn’s or ulcerative colitis,” said Tina.
Healthcare for those with IBD in the LGBTQIA+ community looks a bit different. IBD often affects young adults, many of whom are just beginning to become comfortable in their sexuality and gender identity. This can be especially hard for LGBTQIA+ folks, who have already had to work through stigma and discrimination, and then have the additional burden of a new diagnosis of IBD. The LGBTQIA+ community is a big, diverse group of people and each person is unique.
This Pride Month on Lights, Camera, Crohn’s a close look at the most common concerns and patient experiences, helpful guidance to support the LGBTQIA+ community, tips for finding and communicating with your care team about your sexual orientation, and exciting news about how the University of California-San Francisco Medical Center is working to provide a safe space for patients.
You may not be aware that IBD symptoms can affect sexual function, colectomy and J-pouch surgeries can impact receptive anal sex, transgender people with active pelvic inflammation may have issues undergoing bottom surgery as part of gender affirming, and much more. The mere act of communicating with your care team can be an overwhelming and daunting experience.
Coming soon: An IBD Clinic specifically serving the LGBTQIA+community
Dr. Justin Field, MD, University of California, San Francisco, is passionate about supporting IBD patients who are part of the LGBTQIA+ community, as a gay man himself, he’s on the forefront of making the UCSF Medical Center one of the first in the country to have an IBD clinic geared towards treating IBD in the LGBTQIA+ community.
Currently there are two other clinics in the U.S. that specialize in treating LGBTQIA+ IBD patients, the Mayo Clinic in Rochester, Minnesota, run by Dr. Victor Chedid and Capital Digestive Care in Washington D.C. Dr. Jessica Korman, MD, specializes in LGBTQIA+ patients with all GI issues, including IBD. She also does anal cancer screenings.
“The clinic at UCSF is set to open this Fall and will offer comprehensive IBD care to anyone who is interested and will be a safe and inclusive environment where everyone involved in patient care will have special training in the unique needs and concerns of LGBTQIA+ patients. The clinic will offer screening for anal cancer, which is increased in patients with IBD, in men who have sex with men (MSM), patients living with HIV, those who have receptive anal sex, patients with prior cervical or vaginal cancers, and in those on long term immunosuppression,” said Dr. Field.
The clinic will also offer coordination between Gastroenterology and other specialties such as Colorectal Surgery and Transgender Care. For people who are interested, UCSF will offer the ability to participate in research that adds to the knowledge base about the unique needs of LGBTQIA+ people who have IBD.
“This clinic came from the realization that LGBTQIA+ folks often have unique needs that aren’t always addressed in other traditional settings. Also, patients often feel hesitant to fully discuss their sexual orientation and gender identity with healthcare providers due to fear of stigmatization or being treated differently. I wanted to create a safe space where patients can feel comfortable and empowered to be open with their healthcare team, and where they can receive the relevant expertise to meet their needs,” says Dr. Field.
Because LGBTQIA+ people have so often been left out of research (by not including sexual and gender diverse identities in research studies), having a dedicated LGBTQIA+ IBD clinic helps improve medical knowledge about how IBD affects LGBTQIA+ individuals, by allowing more patients to choose to participate in research.
“I have received incredible support from the University of California – San Francisco to start the clinic. The clinic continues to be a work in progress, and I’m continuing to seek out a wide variety of patient and provider input to ensure the clinic effectively serves the community,” explained Dr. Field.
Living with the stigma of IBD and being LGBTQIA+
CC Springhetti was diagnosed with ulcerative colitis when she was 12. She’s has an ileostomy and says sometimes she jokes that the universe keeps punishing her with stigmatized labels.
“I’m a woman, gay, AND I have a disability now?! In all seriousness, I try to view all my labels as gifts. They each make me who I am, and though it’s taken me some time to get to this point, I’ve learned to be proud of who I am and what I have. I know that sharing my life helps normalize and de-stigmatize IBD and queerness. Representation is so important, and being able to show up exactly as I am to show that you can be queer with IBD and still live a full life is a precious gift I have been given.”
CC and her wife share their life online and have been the target of extreme hate and prejudice. They’re received hundreds of threats.
“It can be draining to keep up with the amount of comment/message removal needed to keep our internet pages safe for young viewers and it’s incredibly disheartening on a regular basis. I sometimes give myself several days away from social media just to clear my mind – the hate and threats cause so much stress, and it can be difficult to separate internet life from real life. Those of us with IBD know how stress can affect our bodies, so this is a constant issue I am still working through every day.”
CC says when she’s admitted to the hospital, she’s dealt with the stress of her partner not being taken seriously of being allowed to make big decisions during emergency situations.
“We live in the south in the United States – it sometimes can be difficult for us to know who is able to separate their work life from their personal beliefs. When you’re in a hospital setting there really is no knowing, and this is something we always try to stay vigilant about and are very communicative with our care teams about what our needs and wishes are.”
The impact of IBD on sexual function
Brad Levy started to experience IBD symptoms in January 2022. He was diagnosed with Crohn’s the following month. His dad has ulcerative colitis, which sped up the diagnosis process significantly. Along with having Crohn’s Brad is a married gay man and a dad. Shortly after his diagnosis, Brad started to worry about how his disease would impact not only his life in general, but his intimacy with his husband.
Dr. Field explains why IBD can have such a big impact on the sex lives of LGBTQIA+ people.
“Receptive anal sex is an important part of sexuality for both LGBTQIA+ and non-LGBTQIA+ people but is especially important in this community. IBD often involves inflammation around the anus or in the rectum and this can make sex difficult or painful. For transgender folks, active inflammation in the pelvic area can affect their ability to undergo gender affirming surgery, so it’s especially important to address any pelvic inflammation.”
Brad says, “There is some shared stigma around IBD and being a gay receptive partner. Specifically, within the gay community there can often be some unrealistic expectations about how “cleaned” out you should be before engaging in receptive sex. The reality is though that shit happens, quite literally. The shame and judgment around a critical and natural bodily function such as elimination needs to end.”
Overcoming the fear of judgement and finding a care team you can openly communicate with
Talking about sex, sexual orientation, and gender identity can be scary as a patient, because often those in the LGBTQIA+ community have prior experiences telling people about their sexual orientation or gender identity which may have been met with rejection or judgement.
“Historically, the medical community has treated the LGBTQIA+ community poorly and considered LGBTQIA+ identities as pathologic. This historical context is important because there are very logical reasons patients aren’t comfortable talking about this with their doctors. In some areas, it truly isn’t safe for LGBTQIA+ individuals, especially the trans and non-binary community,” said Dr. Field.
Now more than ever, there are lots of affirming healthcare providers. Individual providers and practices can take measures to ensure a LGBTQIA+-friendly healthcare setting (For example, by following these recommendations put forward by the American Medical Association.
Demonstrating to patients that they are in a safe space to talk about their sexuality or gender identity can go a long way in facilitating sensitive conversations. Providers can seek additional education on sexual health in gender and sexual minority patients, so that they feel more capable of addressing the needs of the IBD community.
Dr. Fields says, “Providers should know it’s ok to make mistakes when it comes to addressing diverse sexual orientations and gender identities. What’s most important is that we acknowledge the mistake, apologize, and move on.”
CC is a firm believer that your doctor should be someone you never lie to. Honesty will help you navigate problems and solutions in a sensitive manner.
“I remember I was nervous to share with my gastroenterologist that I was gay. Whenever I referred to my partner and he responded back to me with questions or comments, he would always say “boyfriend” or refer to my partner as “he”. It felt scary to correct him (especially after all of these years) so I just didn’t. I was nervous it would embarrass him or make him feel silly, and I always want to protect people from that when I don’t feel they deserve it,” she said.
Then one day, CC was at a different doctor and she made sure to share to share that she was married to a woman and had been in a same-sex relationship exclusively for a number of years.
“I had this doctor add this information to the top of my medical chart. Now when I go to any doctor and they pull up my chart, they can see that I’m gay and can provide sensitivity to me in that way when speaking to me.”
Seeking out LGBTQIA+ affirming healthcare providers
Patients can feel empowered to seek out LGBTQIA+ affirming healthcare providers like Dr. Field.
Find providers with a special interest in LGBTQIA+ health. Patients can also look at lists such as the LGBTQIA+ Healthcare Directory.
Patients should feel empowered to be their own advocate. It’s a patient’s right to have their sexual health needs met and to receive care that is affirming of all genders.
Patients can bring a list of items that they want to discuss to a visit, and it’s best to mention those at the beginning of a visit to help set the agenda. It’s also always ok to seek a second opinion if you feel like your provider hasn’t gotten a satisfactory answer to your questions or if you feel another provider perspective would be helpful.
“Having a GI doctor you trust and feel comfortable enough to discuss your sexuality with is so important. When having receptive anal sex, things happen sometimes, such as tears, and you want to be able to talk with your GI doc openly so you can triage whether something is related to your IBD or not,” said Brad.
Additional IBD screenings for the LGBTQIA+ community
According to Dr. Field, men who have sex with men that are living with HIV should be screened for anal cancer.
“Other at-risk groups for anal cancer are men who have sex with men over age 40, people with prior cervical or vulvovaginal squamous cell cancer, patients that have receptive anal intercourse, and those with multiple sexual partners,” he said.
The risk of anal cancer is increased in patients with IBD, and doctors are continuing to learn more about this risk through ongoing research studies. Screening for anal cancer is with a rectal exam and a swab of the anal canal, called an anal pap smear. If these are abnormal, they must be followed by a procedure called a High Resolution Anoscopy, which is the best test for detecting anal cancer and its precursor.
“Anal cancer is caused by HPV, and there is a vaccine against HPV. Anybody who has not received the HPV vaccine, regardless of age or gender, can talk to their doctor about HPV vaccination. Currently, the CDC recommends HPV vaccination regardless of gender up to age 26 to prevent HPV related cancers, and the vaccine can be given up to age 45 on a case-by-case basis, if it’s felt it would benefit,” said Dr. Field.
Brad lives in the Chicago suburbs. As a result, he says the attitudes towards the LGBTQIA+ community are generally that of acceptance and love.
“I have always had a gay primary care physician because I want to make sure I am comfortable discussing any health issues with them. My GI is also aware of my sexuality, and we’ve had candid conversations about what intimacy looks like during a flare and what vaccines I should consider. For example, my GI recommended I receive the Gardasil HPV vaccine based on my sexuality and increased risk.”
Other cancer screenings to keep in mind are Colon cancer screening for all patients, Cervical cancer screening for patients who have a cervix, and skin cancer screening for all patients who have received immunomodulators, small molecules, and biologics.
“Much of the existing research on things like sexual health and surgery in IBD didn’t ask participants about their gender identity, sexual orientation, or typical sexual practices. This can leave both patients and providers at a loss for answers to sexual concerns,” said Dr. Field.
More and more, sexuality and gender identity are being included in research studies, and this will paint a clearer picture about how many LGBTQIA+ people are impacted by IBD, and how the course or experience of IBD is similar or different between LGBTQIA+ and non-LGBTQIA+ individuals.
Juggling a love life and fatherhood with IBD
Brad and his husband have been together for 13 years, so luckily communicating about his IBD has come easy.
“But I can recognize for others, in shorter relationships or dating, this isn’t always the case. All I can recommend is transparency and having a partner you feel you can be honest with. There will be times (such as a flare) where intimacy will look different. You want your partner to know that it’s because of your IBD activity and not because of them or some issue with your relationship,” said Brad.
As the years go by, Brad says the more authentically he lives, the happier he is. For him, that means living as an out gay man who has an amazing family. It also means living with Crohn’s disease, Anxiety, and Depression. Brad is open about his health struggles with family, friends, and close colleagues/bosses. He says transparency has served him and his relationships well.
As an IBD Dad to a five-year-old girl who is on the spectrum, Brad says focusing on self-care to help manage stress makes all the difference.
“Focusing on self-care enables me to show up as an active and healthy dad. My self-care includes hopping on my Peloton (#ThatDadBrad for the Peloton readers), bi-weekly therapy, monthly massages, and getting my nails professionally done. While not all these activities are for everyone, I strongly encourage folks to pour into their own cup or put on their own mask first. You can’t fully show up for you me kids and your family if you’re not grounded and the healthiest version of yourself, whatever that looks like for you.”
Brad wants to reiterate that his experience as a cis gay white man is “only one voice (and a privileged one at that) out of the vast and vibrant LGBTQIA+ community.” You can connect with Brad on Instagram at: @bssl.
CC says there are a number of ways our IBD community can show support. You can follow CC on Instagram at: @ccspringhetti.
“We’re all human, and I would encourage the IBD community just like I would encourage any community to show your support during Pride month and all year long through any means appropriate for your situation. Support LGBTQIA+ owned businesses, hang a Pride/Progress flag, post your support on social media, or even attend your local Pride events! If you’re ever looking to support a good LGBTQIA+ charity, I always suggest The Trevor Project.”
Certain roadblocks and issues that are a concern to one person, may not bother another. Just like every IBD patient, regardless of sexuality, the experience is unique. We all need to feel seen, understood, and respected, as one united IBD family.
Dr. Field’s views are his own and do not represent the University of California San Francisco.