New research published in Clinical Gastroenterology and Hepatology offers a glimpse into what Crohn’s disease may look like before it officially begins and the findings could have major implications for how we understand, monitor, and potentially prevent the disease in the future. As an IBD mom of three kids ages 8, 7, and 4, research like this always feels a bit bittersweet. While I’m grateful for the strides in research, I’m apprehensive about the burden and grief I would feel if I was able to know if my children would one day receive the same diagnosis.
As someone diagnosed with Crohn’s at age 21, I’m grateful for my two decades of blissful, perfect health. Had I known a complicated chronic illness would one day riddle my body, I’m not sure how I would have coped and dealt with that news.
This week on Lights, Camera, Crohn’s a look at what the latest research discovered, the complicated emotions IBD parents may feel, and what the future may hold for us all as a community.
Why This Matters: Crohn’s May Start Long Before Diagnosis
The study found that certain immune responses in the blood, specifically elevated IgG antibodies targeting a conserved region of bacterial flagellin (a protein found on gut bacteria) were present years before people were diagnosed with Crohn’s disease. In other words, the immune system appeared to be reacting to gut bacteria long before symptoms like abdominal pain, diarrhea, or weight loss ever showed up.
This study followed 381 first-degree relatives of Crohn’s patients, 77 of whom went on to develop the disease. Among them, 28 (more than a third) had elevated antibody responses.
One of the most important takeaways from this research is the timing. Most Crohn’s biomarkers are identified after the disease is active. This study, however, suggests that immune dysregulation may begin well in advance of clinical disease. This supports the idea that Crohn’s develops gradually rather than suddenly.
That distinction matters. If Crohn’s truly has a long preclinical phase, it opens the door to earlier monitoring and potentially earlier intervention, especially for people who are already at higher risk, such as first-degree relatives of those living with Crohn’s disease. A first degree relative is a parent, child, or sibling.
According to the Crohn’s and Colitis Foundation, 36% of children born to two parents with IBD will develop the condition at some point during their life. The risk is substantially less when only one parent has IBD, with The National Human Genome Research Institute sharing there’s a 7-9% chance.
A Potential Blood Test for Risk, Not Diagnosis (Yet)
It’s important to be clear: this is not a diagnostic test and it’s not something patients can request from their doctor today. But it does raise the possibility that, one day, blood-based immune markers could help identify those who are more likely to develop Crohn’s before symptoms begin.
For families affected by IBD, this kind of risk stratification could be meaningful. Instead of waiting years for symptoms to escalate, or for damage to occur, high-risk individuals might one day be monitored more closely or offered early preventive strategies. As an IBD mom, I feel as though I would struggle with knowing whether this was something I wanted to dig deep for, while also not wanting to get in the way of stopping disease progression. It’s not a black and white situation by any means. If these types of blood tests are available when my kids are teenagers, and I were to get results that broke my heart, I’d feel obligated to be transparent and share—would I really want my kids, who have witnessed me living with Crohn’s their whole lives, to know this would one day be part of their own story? It stresses me out just trying to imagine it.
What This Could Mean for Prevention Research
Another compelling aspect of the study is that the immune response was directed at a conserved portion of bacterial flagellin. This means it’s shared across many gut bacteria. That finding has sparked discussion about whether future therapies or vaccines could target these immune pathways in people who are high risk for Crohn’s.
While prevention remains a long-term goal rather than a current reality, this research reflects a broader shift in IBD science: moving upstream to understand why Crohn’s starts, not just how to treat it once it’s already established, and as an IBD mom I am certainly grateful for that.
What This Doesn’t Mean (Yet)
As exciting as this research could be, it’s not a crystal ball. Not everyone with these immune markers will develop Crohn’s, and many people with Crohn’s were never tested years before diagnosis. Larger studies are still needed to validate these findings across diverse populations and to determine how predictive these markers truly are.
For now, this study adds another piece to the puzzle, one that reinforces what many patients already know intuitively: Crohn’s disease doesn’t start the day you’re diagnosed.
The Bigger Picture
Our community often experiences years of delayed diagnosis, misattributed symptoms, and unanswered questions, so research like this matters. It shifts the narrative from “why didn’t we catch this sooner?” to “how early can we understand and intervene?”
While we’re not there yet, this study represents an important step toward a future where Crohn’s disease is identified earlier, monitored more thoughtfully, and one day possibly prevented altogether.
For parents living with IBD, research like this can carry an added emotional burden. The idea that Crohn’s disease may be detectable years before symptoms begin can stir complicated feelings, especially for those who worry about whether they’ve passed on a genetic risk to their children. Some parents may want every possible tool to protect their child’s future health, while others may find the thought of early testing anxiety-provoking or guilt-inducing. There’s no right or wrong response. I get it and struggle with how I’d handle this, too. Living with IBD already requires navigating uncertainty, and this research underscores how deeply personal decisions about risk, knowledge, and monitoring can be for families. As science moves forward, it will be just as important to support parents emotionally as it is to advance early detection tools.
At the inaugural Cedars-Sinai IBD and Women’s Health Conference, experts came together to spotlight the unique challenges women face at the intersection of inflammatory bowel disease (IBD) and women’s health. Co-directed by Dr. Puja Khanna, Clinical Director of the IBD Women’s Health Program, and Dr. Maria Abreu, Executive Director of the IBD Institute, the event featured a two-part format: clinical updates for providers and education for patients and caregivers. Topics ranged from fertility and pregnancy to nutrition and mental health.
One of the featured speakers was Neha D. Shah, MPH, RD, CNSC, CHES, Senior Dietitian at the Colitis and Crohn’s Disease Center at UCSF and founder of Neha Shah Nutrition LLC, a private practice specializing in nutrition care for patients with IBD. Her session focused on nutrition updates and strategies to support gut, muscle, and bone health in women with IBD. This week on Lights, Camera, Crohn’s I spoke with Neha, and she zeroed in on something every woman with IBD should care about: how to use nutrition to protect our gut, muscle, and bone health.
Why Nutrition Matters Beyond the Gut
Whether you live with IBD or care for patients, you know that IBD affects much more than the gut. Fatigue, abdominal pain, and debilitating flares that blindside us can make it feel like our whole body is affected. While we know this, it can be complicated to know how to address these specific challenges.
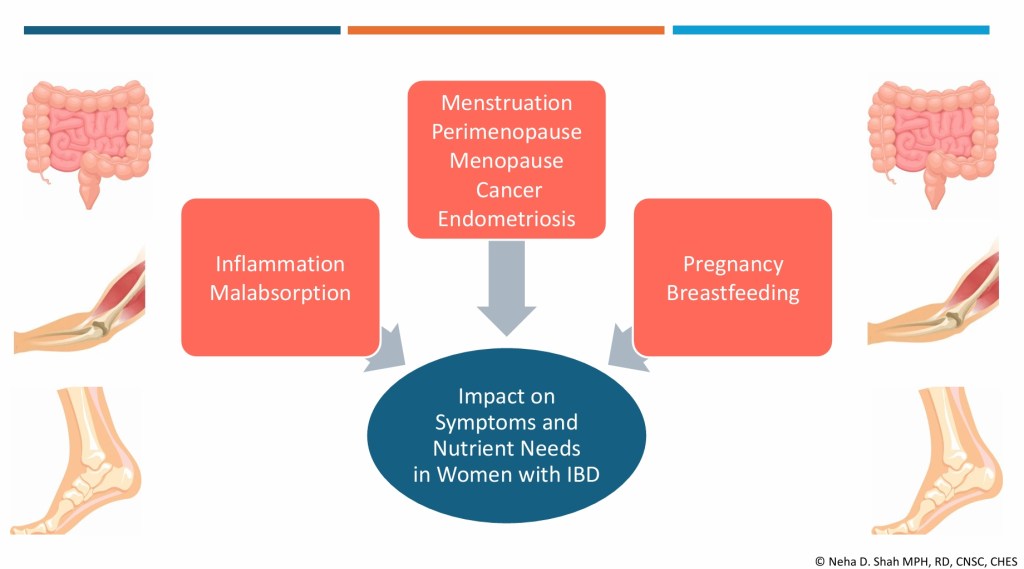
“Women with IBD face a unique set of challenges,” Neha explains. “Poor absorption can contribute to ongoing symptoms, muscle loss, and bone loss. Hormonal shifts, whether from PMS, pregnancy, or perimenopause add yet another layer, often making symptoms unpredictable.”
Her goal? To give women practical, evidence-based strategies they can use to better support their health, both now and as their bodies change through different life stages. As a woman who was diagnosed with Crohn’s disease at age 21, my questions and focus have shifted now that I’m 42 and my family is complete.
“Many women don’t just experience flare-ups; they live with changes in their body that evolve throughout life, impacting daily routines, work, and overall quality of life. In my presentation, I aimed to highlight both the latest updates and practical, whole-food strategies that women can use to better support their health.”
Key Takeaways from Neha’s Presentation
Gut Health
IBD symptoms often overlap with PMS and endometriosis: fatigue, abdominal pain, diarrhea, bloating, and constipation. If you’ve noticed an uptick in your IBD symptoms right around your period, you are not imagining it.
When combined, these conditions can intensify, highlighting the need for careful monitoring and proactive management.
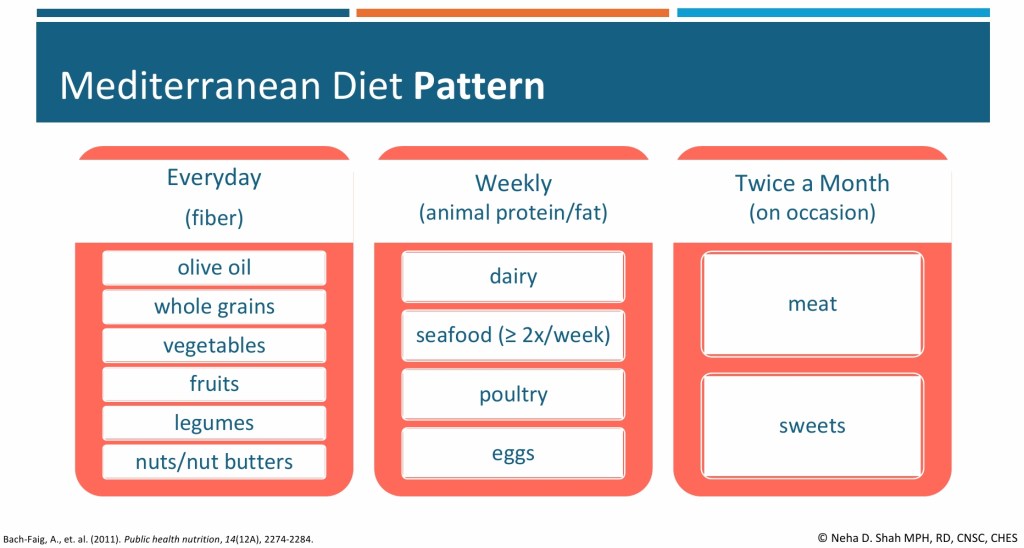
Dietary Patterns: A Mediterranean-style diet rich in fruits, vegetables, whole grains, legumes, nuts, and olive oil may reduce the risk of IBD flares and ease painful bowel symptoms in women with endometriosis.
Fiber Matters: Soluble fiber (oats, fruit) can slow diarrhea, insoluble fiber (leafy greens, brown rice) can help constipation, and less fermentable fibers may reduce gas and bloating. Adjusting textures, like blending or mashing can improve tolerance, especially for those with strictures.
Neha notes that further studies are needed here and she’s hopeful we’ll have even more intel in the future.
Muscle Health
Sarcopenia (loss of muscle mass and strength) is more common in IBD due to chronic inflammation and nutrient malabsorption. Hormonal changes and aging further increase the risk.
Nutrition + Activity: Adequate protein intake (1.2–1.5 g/kg per day for many with IBD) and resistance training are key. Individual requirements sometimes are even higher.
Gut-Muscle Axis: Emerging research suggests fiber may support muscle health by fueling beneficial gut bacteria. The National Health and Nutrition Examination Survey (NHANES) 2011–2018 survey data from 6,000 healthy adults (without IBD) showed each 5 g increase in fiber intake was associated with higher lean mass and grip strength, possibly through increased short-chain fatty acid production. Fiber’s role in IBD and sarcopenia remains understudied.
Practical Tip: Aim for 15–20 grams of protein per meal, combining both animal (e.g., fish) and plant-based sources (e.g., lentils, tofu, nut butter). People with IBD generally have higher protein needs, which can vary depending on weight, activity level, and disease state.
“Evidence in women with IBD is limited. One small case-control study of 23 women with UC versus age- and BMI-matched controls found reduced quadriceps strength, slower sit-to-stand and gait speed, and lower physical activity, though handgrip strength was preserved, says Neha. “Early assessment of nutrition, activity, and lower limb function is crucial. No IBD-specific sarcopenia guidelines exist, but recommendations from the International Clinical Practice Guidelines for Sarcopenia by the annual International Conference on Frailty and Sarcopenia Research by centers at John Hopkins University include increasing protein/calorie intake and resistance training.”
Bone Health
Women with IBD are at higher risk for osteoporosis and osteopenia, especially during perimenopause and menopause. The gut-bone axis reflecting the connection between gut microbes and bone health may play a role. Calcium and vitamin D requirements in individuals with IBD depend on factors such as disease activity, malabsorption risk, corticosteroid use, and deficiency status.
If you haven’t done so already, talk with your care team about getting a DXA scan (bone density scan) so you have a baseline. The earlier in your IBD journey, the better. Bone scans are non-invasive, and probably the easiest test we undergo. You wear your street clothes, lie down on a table, and it’s a quick and painless experience. I have a bone health doctor at Wash U (yes, that’s her title!), who focuses specifically on this after a bone scan in 2022 showed signs of osteopenia and osteoporosis in my 30s. Be mindful on the timing—do not get a bone scan while pregnant or breastfeeding as this can skew the results. If you’re nursing, it’s ideal to give your body at least 6 months after weaning before you get a bone scan, so your bone health is accurate.
Calcium & Vitamin D: People with IBD often under consume these nutrients, particularly when dairy is restricted. For most, calcium needs range from 1,000–1,500 mg/day, with vitamin D at 1,500–2,000 IU/day. In a cross-sectional study of 65 IBD outpatients, nearly two-thirds reported restricting dairy, leading to an average calcium intake of only 343 mg/day—well below the daily recommendation.
Practical Tip: For those who tolerate dairy, start small—a dollop of yogurt, a sprinkle of cheese, or lactose-free milk. Non-dairy sources and supplements can help fill the gaps. When you get labs, you can talk with your GI about looking at your vitamin D level to see if it is adequate or not. I was on 50,000 IU once a week for many years. Now, I take 2,000 IU a day. So, this figure does fluctuate and it can improve.
Nutrition Across Life Stages
Neha stresses the importance of tailoring nutrition guidance to a woman’s age and life stage:
Young women (around age 20): Focus on building peak bone mass, meeting calcium and vitamin D needs, and making realistic choices in dining halls or dorms. Portable, nutrient-dense snacks like yogurt, nut butter, or fortified bars can make a difference.
Premenopausal women: Greater emphasis on long-term bone and muscle health, distributing protein intake evenly throughout the day, and pairing nutrition with weight-bearing activity to maintain strength. Neha’s focus shifts more toward optimizing long-term bone health, since risk factors may be increasing.
“Across both age groups, I prioritize adequate protein and fiber in forms that are well tolerated to help manage symptoms and optimize muscle mass, while also monitoring common nutrient deficiencies such as iron, vitamin B12, and folate,” explains Neha.
The Role of an IBD-Specialized Dietitian
A dietitian specializing in IBD plays a vital role in helping patients understand how inflammation and treatments can affect digestion, absorption, and food tolerance.
“We stay up to date with the latest evidence and tailor nutrition strategies to each stage of the disease—whether someone is newly diagnosed, recovering from surgery, or in remission. For example, we help patients identify which types and textures of fiber are best tolerated, since not all foods impact the gut the same way,” says Neha. “We also emphasize balanced protein intake from both animal and plant sources to protect muscle mass, and ensure nutrients for bone health, like calcium and vitamin D are optimized from both dairy and non-dairy options. Just as importantly, we integrate these strategies into each patient’s lifestyle, culture, and social settings so that recommendations are practical, sustainable, and supportive of long-term quality of life.”
By seeking out a registered dietitian who specializes in IBD you are truly targeting your treatment and receiving personalized care that helps you cut through the confusion, especially if you are newly diagnosed. Their strategies are not just good on paper; they work at your kitchen table and in your daily routine to help you get your health and well-being back under control.
Accessing a dietitian may depend on the healthcare system. Patients can ask their gastroenterologist for a referral, or they may be able to connect with an IBD-specialized dietitian through private practice. Many registered IBD dietitians also do virtual video calls, so it’s not necessary for in-person, local appointments. The Crohn’s & Colitis Foundation provides resources to help connect patients with dietitians who have expertise in IBD.
Final Thoughts
Nutrition in IBD isn’t one-size-fits-all. It requires careful personalization and an understanding of the unique challenges women face throughout their lives. By focusing on gut, muscle, and bone health, women with IBD can better protect their bodies today while laying the foundation for stronger health in the future. It’s not just about flares and managing our IBD, it’s about how our bodies uniquely absorb nutrients, how inflammation affects our strength, and how hormonal changes shift the way we fell over time. Muscle weakness, bone loss, and unpredictable symptoms tied to our menstrual cycles can be a lot, but small, realistic changes in how we eat and move our bodies can make a lasting difference.
Whether you’ve experienced one colonoscopy or 20, you know the process is far from enjoyable. This past week while scrolling through Instagram I came across a story an IBD caregiver posted as her young daughter prepped for her scope. During the video she explained how her husband rolls dice, and whatever number it lands on is how many sips their daughter has to take of prep. I was amazed at this brilliant trick to ease the struggle of getting the prep down, and it inspired me to dig a little deeper and ask the IBD community what their “tips and tricks” are.
This week on Lights, Camera, Crohn’s read firsthand advice from caregivers and patients of all ages. My hope is that you find comfort and maybe even a new idea or two to make your next prep a little less stressful.
Firsthand advice for pediatric IBD caregivers
Mara’s daughter has IBD and has already been through eight colonoscopies in just five years. She says the dice game was a huge success for their family the first time around:
“She was at the perfect age for a little competition as motivation with a reward at the end for the winner…of course she always won. It was honestly so easy to prep her I was shocked.”
However, being NPO (derived from the Latin saying ‘nil per os’ or nothing by mouth/no food or drink) after midnight was NOT easy.
“There were lots of tears and anger directed at us. We bought her a special blanket and stuffed animal, which helped diffuse some of that anger.”
As many caregivers know, every prep is different. Mara recalls their second scope being much more difficult, requiring hospitalization and an NG tube after her daughter couldn’t keep the prep down. Now, they focus on giving their daughter as much autonomy as possible, letting her choose flavors, snacks, and activities.
“On prep days or days, she must be NPO, dad and I also follow that diet. It gives her a sense of belonging and that we are struggling right alongside her. We’ve done it for all eight scopes, and we will continue to do it if she needs us to.”
Over time, Mara says they let their daughter lead as much as they can. They give her a “yes” day.
“Whatever she wants (within reason) to eat or drink. Gummy bears, sure. Popsicles, sure. Want to try to mix three different Gatorades? Why not? She wants to watch TV while she preps or play hockey, absolutely.”
Emily’s Family Emily has three daughters with IBD (now ages 9, 12, and 15) who’ve been doing preps for over a decade. Their youngest had to prep for a scope when she was only 21 months old. Their top tips include:
Only prepare 8oz of the drinking mixture at a time. With MiraLAX prep, we let them pick a new flavor to mix each 8oz.
Think outside the box with the liquids for MiraLAX! One preferred water once! (With other electrolyte drinks that day.) One daughter does her whole prep with tea and chicken broth. (Add MiraLAX after the liquid is warmed.)
Use distraction!! This is our biggest piece of advice. We surprise the girls with a new activity the day of prep. They know there will be something fun to do – just not what it is. We have gotten Lego sets, multi-step craft projects, etc. We pick something that we can partition up and give them one part at a time in celebration for ounces drunk!
Keep them active. We have found that the girls tolerate the large amounts of liquids better if they get up and get moving! In the warmer months, they go walk laps around the driveway between cups of the prep.
Pick the “fun” liquids together ahead of prep day. Since they normally cannot have juice or soda, they pick out a few drinks that they are excited to have. This helps them to drink more, once the MiraLAX prep is complete.
I set timers for myself for the day of prep for every 10 mins or so. Just to check in on their drinking. It’s easy to lose track of time and accidentally go 30 mins (or more!) without drinking.
Pack a bag of supplies for the scope day. We always take extra clothes and baby wipes for any accidents. Games/books/crafts are great to keep the girls distracted during the wait before their procedure time. We take some water/light snacks for afterwards. (Check with your providers to see what/when your child can eat afterwards.) Chapstick is always requested by mine now too.
Remember that you can speak up and (nicely!) ask for what your child needs to make them comfortable. For example, at our hospital, the kids usually get their IV’s after they are sedated with some gases through their breathing mask. This is great to avoid needle anxiety for many kids. However, mine have taken a dislike to the masks and the smell of the gas. Since they get regular med infusions, they prefer to get their IV’s back in the holding area and then use the IV for their sedation to sleep. While not the normal procedure, the anesthesiologists and nurses have kindly worked with us to do it the way my kids prefer.
Cindy’s Perspective Cindy, mom to a teenage daughter with Crohn’s disease, says scheduling scopes early in the day is key. Even if you have a teen who likes to sleep in, sleeping in is worth nothing if you already feel like crud due to the prep. She emphasizes advocating during IV placement and following your gut as a caregiver:
“A parent’s intuition of how much is too much comes into play, and you’ve got to listen to that voice. Tell the nurse you (parent and child) did your best to complete as much of the prep as possible. If you can’t finish it to a T, they can still make it work. They know they are working with a child. If they are having trouble placing an IV, advocate for your kid. Give them two tries and then request another person to try. We’re still traumatized from watching them work for 10 minutes to get an IV into my dehydrated and scared 9-year-old, and I think that trauma will live with us both forever.”
She also believes in being honest with your child without over-preparing. Start the conversations when it’s time, but don’t talk about it for days or even hours beforehand.
“This is not going to be fun, and it won’t feel good. But I know you can do it and we are going to do it together because I will be beside you every step of the way. Here are the steps we will take and outline them in age-appropriate detail. Let’s think about how amazing this is going to be once it’s done! This is our focus for the next 24 hours… that moment when it’s done… that will be the best! As soon as you are done at XYZ time tomorrow, we can celebrate and go back to normal life, and you can eat whatever you want.”
Additional feedback for pediatric patients
“For pediatric prep, popsicles are necessary. Blue popsicles allow kids to “poop blue,” which many like. The Gatorade with the MiraLAX is the easiest for them to get down. We tried magnesium citrate once and it was a disaster. Gatorade is where it’s at. Also, we make it a party. Popsicle party. Jokes and TV while pooping. Anything to keep the mood light.”
“Turn the ordeal into a scavenger hunt by completing parts of the prep with small stickers to earn up to something whether it be completing a picture or something to distract when prep is working.”
“My daughter’s first prep at home didn’t go well, but prep while in-patient thru NG tube really worked.”
“If the hospital or your GI team has a Child Life specialist, they can send prep books to families ahead of time so they can help prepare kids for what to expect the day of the procedure.”
“Bribes! Lots of bribes! New toys or games. Legos keep little ones busy. Family doesn’t eat in front of them. Lots of snuggles. Clear your schedule to spend time with them. For young kids, put all food out of reach or lock the pantry so a hungry little one doesn’t get into something they can’t have and make you have to cancel the procedure, which is always my fear!”
“I have a prep approved Starbucks order—Mango Dragonfruit refresher, Venti, no ice, no Dragonfruit fruit inclusions, peach juice blend, in my personal cup … I like to line up cups so I can visually see how much is left and removing one feels like an accomplishment. A seasonal suggestion is using an advent calendar and dividing prep by 24 and opening one door after each one…just make sure the prizes are not food!”
“Arts and craft activities and projects can be a good distraction. Recently gave a sensory art bin to a VEO-IBD patient through their first scope as a kid it helped me to have new things to do.”
“My mom fasted with me when I was doing the prep as a kid! My tips now as a mom myself are to make Jello without Red 40. Ramen seasoning dissolved in water tasted way better than broth to me as a kid…I know that’s not good for you. I would make it a fun and relaxing day, so your kiddo is distracted. I would recommend not watching TV or YouTube because there are so many advertisements for food everywhere and it didn’t help distract me much. I advise having a movie marathon instead!”
“We didn’t eat out much when I was a kid, so eating out with my parents only was a big treat for me to look forward to after starving the day before! Back in the day, GIs used to do a combination of drinkable prep and suppositories for pediatric patients, and I’m glad my mom did the suppositories for me because it was not something else you had to drink. Ask pediatric GIs about low consumption prep so your child doesn’t throw up.”
“When I was a pediatric patient, my mom took me to the store to pick out different drinks for the mix, Jello flavors, etc.… which would make it fun picking it out myself and this also gave me a sense of control in a very out my control situation. My mom always fasted with me, which I appreciated not feeling alone in it. I was also able to pick the restaurant to go to after for something to look forward to!”
“Have your child drink their prep in a fun container., a Disney theme with a silly straw. For adults, use a wine glass or fun mug. Cheers!”
“My 12-year-old just had their first colonoscopy. As a Crohn’s patient myself, I have done one every other year for 25 years and it was hard to watch him go through it. He was tougher than me. The hardest part was him not eating! He had to do a full two days of clears only—per our doctor’s recommendation. That’s my hack as an adult, too. I start taking a Dulcolax dose and not eating a day or two earlier than recommended. You only have to drink the drink until it’s clear in the toilet. The milder/longer prep is easier on me and saves me drinking half the magnesium citrate drink.”
“My daughter couldn’t get any of the prep down at age 16 and by this summer, at age 19, she felt ready. This time we tried over the counter prep of MiraLAX and Dulcolax. The doctor said if she did it this way, she would need to fast for 48 hours instead of 24. She was fine with that. She started taking a couple of Dulcolax tablets at 5 pm the night before. Then, we put half a bottle of MiraLAX into Sprite. She drank a cup every 10 minutes until it was gone. We did the same thing a few hours later. She was clear before going to bed at night. It was easy and stress-free for her.”
“My parents would set me up with my iPad for movies, a desk chair, and a blanket in the bathroom so I could go back and forth from the toilet easier.”
“Make MiraLAX with white grape juice instead of Gatorade! Drink with a fun straw so you can put it on the back of your tongue and taste less. Put on headphones with loud music to distract your sense from the taste so you can drink the prep faster.”
“I confirmed with my child’s GI that colorless cotton candy is a clear liquid! Obviously in moderation, but this could be super helpful for kids and adults who need a different texture than liquid or gelatin.”
Prep Hacks for Adult Patients
Our IBD family had plenty of creative hacks for adults, too:
“The MiraLAX + Dulcolax prep hands down!! I’ve tried them all, and it’s tasteless and easiest.”
“Lemonheads or lemon jolly ranchers RIGHT after you get done drinking a dose!”
“Gummy bears and lifesavers! I love having stuff to chew. I also had pickle juice shooters, which gave me some salty/sour taste to balance all the sweet stuff. I also keep my schedule open for the remainder of the day and allow myself to relax.”
“I put my Suprep in the fridge (even though it says not to) and it makes it SUBSTANTIALLY easier to drink (and doesn’t seem to make it less effective in any way). I also buy myself a new book to read or save a special TV show episode, so I have something to look forward to when I’m drinking prep at 2 in the morning. Colonoscopies are miserable and until they figure out how to make them a nicer experience, it’s great to team together to gather the best tips.”
“Clear Gummy Bears!! This keeps it fun for all ages! Here’s a recipe!
“Drinking chicken broth throughout the day. This gives energy and takes away the bad taste of the prep drink. As a kid, my sister used to make a colonoscopy prep kit. Every 8 oz. I drank; there would be a little gift or activity to do. For example, after the first 8 oz., I got a nice bottle to drink the rest from. The next thing was a Lego kit or a paint by number.”
“I begin my prep four hours ahead of their suggested time, so I can sleep through the entire night. Getting up in the middle of the night, especially for children to complete round two of the prep is just borderline inhumane. What a nightmare. The catch is waking up and hydrating with enough water before the anesthesia cut-off which requires not to drink anything 2 hours before the procedure.”
“Wet wipes and diaper cream are super helpful!”
“A lot more MiraLAX than the prescription prep. And gummy bears (except red ones) are a gamechanger. They let you feel like you’re eating, but they liquify in your gut.”
“Rotate flavors and get some protein through broths. Have broth, then 2 hours later do Jello or change the texture and taste, then 2 hours later do broth and rotate.”
“Strain chicken noodle soup to just have the clear broth, it has more sodium.”
“Avoid eating vegetables/fruits/seeds three days before. Taking preps that you can take with a glass of water and then drink two liters of tea or water.”
“My son, Andrew, has autism and Crohn’s disease. When he has to do colonoscopy prep, he likes to listen to Disney music and use a timer. Andrew is almost 30 years old and has been having to do colonoscopies since he was 17. This past year, for the first time, he did the pill prep and loved it. He used a timer to tell him when to take the next pill. Andrew told me he will never go back to liquid prep. Pill prep was so much easier for him, especially with his sensory issues.”
“Take notes on all preps you’ve been assigned and take notes and photos of what it felt like. I found one that was less painful for me, and I always request it. I also alternate sips out of a straw with apple juice. I drink the prep in my kitchen, near a bathroom, and watch TikTok’s while drinking to distract myself.”
“I only eat soft foods 2-3 days before, make sure to hydrate, and follow the instructions they give about not eating things like seeds or nuts a week before.”
“Have a bidet and diaper cream ready.”
“Desitin, Gatorade that is the Frost Glacier Cherry flavor (not red) frozen or really cold to help me stay hydrated.”
“Make freezer pops out of the Gatorade prep mix.”
“For me—finding fun drinks, whether a tea at Starbucks or stocking up at the grocery store, really makes it feel less horrible. I started this as a teenager. I make a list of movies or shows I want to binge. If you’re comfortable with it, have a friend there to distract you—at 15 years old, my boyfriend stayed with me all day for my surgery prep which was the same as a colonoscopy and we watched movies and he distracted me/made me laugh and at times I forgot what was going on!.”
“Savory liquids to balance out the sweet!”
“Mix the prep with Crystal Light Lemonade—instead of the lemon mix the pharmacy provides. Drink the prep through a straw and suck on hard candy (e.g., Werther’s Originals) in between doses to get rid of the taste and have something to look forward to.”
“Take SUTAB (pill prep) and Zofran and then fall asleep. Your bowels will wake you up and you’ll avoid the nausea but start the pooping process. I do the same for the morning dose! If you vomit, at this point it’s fine, just hopefully after the nap and pills are digested!”
“Gummy bears/worms!”
“Pill prep has been a gamechanger for me!”
“Extending the clear liquid diet an extra half day or full day helps a ton with prep.”
“You have to have a movie downloaded on a device that you can have in the bathroom and a pillow for the toilet seat for your back. I’m a fan of disposable diapers because after the first several poopy poops, you get to the drizzle stage and then it’s annoying to have to get up every two seconds towards the end. They also come in handy when you’re sleeping and when you’re traveling to the procedure.
“Before I have a colonoscopy I write down positive affirmations and thoughts and there is like a Table of Contents that’s like “When you’re sad” or “When you need a good laugh” and it really helps me though the ups and downs, although it may sound silly. I choose what to drink and I always have my good luck drink which is blue Gatorade.”
“Use nuun electrolyte drink instead of Gatorade!”
“My personal hacks are to follow what you know works for you. I followed the timings of when to take what from the last instructions and it wasn’t the cleanest prep. I should have listened to my gut and started doing that earlier. I resort to drinking Ensure Plus instead of just relying on broth and soft foods to keep me feeling full. It’s helped me SO much. I know not everyone can tolerate it or like it, but when I was on a liquid diet about a year ago for two months, I only had Ensure Plus. I got used to it. It’s now a lifesaver, especially if I’m traveling or on the road and not sure what food I will have access to. It helps to start the diet a bit earlier, so mash and fish instead of just toast and pasta.”
“I mix apple juice with my Suprep! I also always buy bone broth or stock because the protein per cup is higher. I like the Zoup brand because there’s 3 or 4 gram of protein per cup. I also get the College Inn brand bone broth which has up to 10 grams of protein per cup.”
“Gummy bears!! Just not the red or purple ones. Just being able to chew something helps! Progresso Chicken Soup. Use a metal strainer to strain out all the solids and then sip the broth. It’s thicker and has more flavor than regular stock and it’s just more satisfying.”
“Remind yourself “this is only temporary.” Having loved ones supporting also helps to distract a little, which makes it easier to get through. Focusing solely on drinking cup after cup can seem very overwhelming.”
“Start a low residue diet a few days early even before your doc says to. Mix prep with Sprite. Have hard candies or gum to chew on while doing prep. Use a measuring cup or something to lines to indicate how much to drink.”
“I really love the Trader Joes less sugar lemonade mix with water for my prep. I chugged and it was so delicious! Also, ice pops like the good pop brand were yummy.”
“Gummy bears! Making ice cubes out of juice and chewing on the ice.”
“Make sure it’s cold! Drink with a straw, chew Juicy Fruit gym in between drinks, this helps cut the saltiness. Do two-step prep if your practitioner allows it (half the night before and the other half in the morning). Ask if you can use one of the lower volume prep or the MiraLAX and Gatorade prep.”
“For the MiraLAX prep I use two different flavors so I can alternate when I get sick of one.”
“Mix the prep early and put it in the fridge. Have music and TV on to help distract yourself.”
“While most people say to drink it cold, I prefer my prep at room temperature so I can chug it faster.”
“Always lots of ice and drinking thru a straw. Big gulps. Have a station in the bathroom with a laptop streaming Netflix. I also got a Bidet before my last one!”
“Gummy bears! I buy the Haribo ones and don’t eat the red ones. My favorite prep hack thus far. It’s great getting to chew something when everything else is liquid.”
“Lots of mint tea when the cold chills kick in a few hours before you have to go in for the procedure.”
“Use a Pedialyte jug and ensure it is very cold and drink the prep with a straw. The slower you drink, the worse it is. I always chug it super-fast through a straw and it gives me 10-15 minutes between each cup. Have lots of other drinks that you don’t normally consume to make it fun and have lots of juice, Jello, soda, and popsicles on hand!”
“I’ve turned prep days into self-care days. I binge shows, nap, relax, and try to take care of myself.”
“I like to alternate between sweet/cold beverages and salty/warm soups when I am trying to stay hydrated before starting prep. Sprite/popsicles/lemon ice and then chicken broth.”
“I chase my prep by sucking on approved colored Lifesavers. They truly are a lifesaver for me. I could never do it without them.”
“I recommend the pill prep instead of liquid prep if you’re neurodivergent or have issues with taste and textures. Maybe keep a backup on MiraLAX and Gatorade or juice in case you can’t tolerate the liquid prep. If you know you get nauseated, take prescription anti-nausea medication like Zofran before you begin the prep. I like Squatty Potty and having wipes to dab and pat my skin. A Peri Bottle can be useful. If you’re prone to hemorrhoids or know you have vascular issues like pelvic congestion syndrome, apply hemorrhoid cream in advance. Keep Zinc Oxide handy if it starts to burn or feel raw. Get into comfortable clothes that’s easy to get in and out of in the bathroom. I personally use a heating pad and Bentyl for intestine cramping. I usually make sure I’m scheduled first thing in the morning, and I ask for extra IV fluids.”
The Takeaway
Colonoscopy prep is a universal challenge in the IBD community, whether you’re a child facing your first scope or an adult whose been through dozens. But as the stories above reveal, there are countless ways to make it less daunting through creativity, distraction, teamwork, and sometimes sheer humor.
I personally start a full liquid diet 4-5 days before my scope to ease the actual prep. I make sure I have Zofran on hand to manage my nausea (I always vomit, regardless), and I prefer the SUTAB pill prep. I’ve done multiple preps since being diagnosed with Crohn’s disease in 2005, and my last three preps, SUTAB pills have been the “most tolerable.” While MiraLAX/Dulcolax is popular, I never enjoyed having to drink such a large volume of liquid. Having gummy bears on hand is also a necessity for me! My husband always takes the day off work, and we go out to breakfast and spend the day together afterwards as a reward for all I went through.
If you’re gearing up for a prep, remember you’re not alone. Thousands of IBD patients and caregivers are walking this same path and learning tricks along the way. Find what works for you (or your child), advocate for needs, and give yourself grace. And once it’s done? Celebrate that victory meal and the relief of getting through another milestone in your IBD journey.
When you’re living with a chronic illness like Crohn’s disease or ulcerative colitis, it’s easy to become hyper-aware of every medication, every symptom, and every nutrient—or lack thereof. One essential mineral that often flies under the radar is magnesium.
Magnesium supports nerve function, hormone balance and how we respond to stress, so when levels drop, the nervous system can become overly reactive. For those with Inflammatory Bowel Disease (IBD), these symptoms can be even more noticeable because our bodies often struggles to absorb and retain magnesium properly.
According to Hollie King, Founder of Sweet Bee Organics, this humble mineral could be one of the most powerful tools in the IBD toolkit. This week on Lights, Camera, Crohn’s Hollie explains why magnesium matters so much for people in our community.
While I was working on this article, I did an Instagram poll asking the IBD community if they take a magnesium supplement. Of the 245 people who responded, 34% said “yes”, 29% said “no”, and 37% replied “should I be?”
The power of Magnesium
“Magnesium is one of those quiet powerhouses in the body,” Hollie explains. “It’s often overlooked, but absolutely essential. It plays a role in over 300 biochemical reactions, helping muscles relax, supporting proper nerve function, balancing hormones, and aiding energy production.”
When magnesium levels drop, your body knows it—but it doesn’t always scream it out loud. Instead, it whispers. Symptoms like anxiety, poor sleep, muscle cramps, low energy, and even restless legs may emerge. But there are subtler signs too: eye twitching, heart palpitations, tingling sensations, and a hypersensitivity to noise or stress.
For those with IBD, particularly Crohn’s disease, magnesium deficiency can be even more pronounced. “When the gut is inflamed or damaged, it struggles to absorb nutrients properly,” Hollie shares. “And magnesium is one of the first to drop.”
The Magnesium–IBD Connection
Recent research, like the article “Magnesium—A Potential Key Player in Inflammatory Bowel Diseases?” published in the Journal of Inflammation Research, highlights the strong link between magnesium deficiency and IBD. But knowing you’re deficient and being able to do something about it are two very different things, especially if your gut can’t absorb it well.
That’s where Sweet Bee Organics comes in. Rather than relying on supplements taken by mouth, Hollie and her team focus on transdermal support—a method that completely bypasses the digestive system.
“Our Sweet Sleep Magnesium Butter delivers highly absorbable magnesium chloride directly through the skin,” Hollie says. “You simply massage it into your chest, feet, lower back, or even your tummy before bed. It’s not just about topping up magnesium—it’s about calming the nervous system, supporting sleep, and helping the body reset.”
The Sweet Sleep Magnesium Butter isn’t just effective—it’s a best-seller across the U.S. and U.K. for a reason. “We’re obsessed with packing as much magnesium as possible into our balm,” says Hollie. “It’s not easy, but we’re committed to delivering a product that works—and works quickly.”
For people with Crohn’s or ulcerative colitis, the benefits of restoring magnesium levels can be profound. Balanced magnesium supports better digestion, improves sleep, reduces muscle tension, steadies mood swings, and even eases PMS symptoms. You sleep better. You feel calmer. Your energy becomes more stable, and your muscles feel less tight or twitchy.For IBD patients in particular, it can help calm inflammation and improve nutrient absorption—essential steps in managing the day-to-day symptoms of the disease.
“It’s not a magic fix, but it’s one of those foundational nutrients that helps everything else work better. The biggest thing people notice? They just feel more like themselves again,” Hollie explains.
Hollie’s Health Journey
This mission is deeply personal for Hollie, who was diagnosed with aggressive cervical cancer and had to completely reimagine how she cared for her body. “Magnesium became an important part of my healing journey. It wasn’t just about sleep or stress—it was about helping my body heal, rebuild, and feel safe again.”
Screenshot
Hollie happens to be my husband’s first cousin—and witnessing her health transformation and all she’s accomplished since her cancer diagnosis has been awe-inspiring. We’re not only family, but friends and I admire her and the genuine work she’s doing. We’ve wanted to collaborate for awhile and when Hollie saw the recent published medical study regarding magnesium and IBD we knew this was the perfect opportunity.
Hollie and I took our kids trick or treating this past Halloween when she was back in the States
Her empathy extends to the IBD community. “For anyone living with IBD, I truly see you. I know how exhausting it can be to manage symptoms, juggle treatments, and wonder if your body is even absorbing what it needs. That’s why I created Sweet Bee. Magnesium might seem like a small thing, but sometimes the smallest shifts are the ones that change everything.”
How is Magnesium Measured—and Why the Standard Test Might Miss the Mark
Many of us assume a blood test will tell the full story, but Hollie points out that traditional serum magnesium tests only measure about 1% of the magnesium in your body.
At my clinic visit with my GI last week, my doctor included magnesium in my lab work and the results were within range, but he also told me there would be no harm in using the transdermal magnesium discussed in this article.
For people with IBD, especially those experiencing persistent symptoms, your GI may suggest testing beyond the standard serum magnesium draw or even recommend supplementation based on symptoms alone. This may be something you want to bring up during your next clinic visit or over the Patient Portal.
How to Naturally Raise Your Magnesium
While supplements are helpful, diet is still key. Magnesium-rich foods include:
Pumpkin and chia seeds
Almonds, cashews, and peanuts
Beans and legumes
Spinach, broccoli, and potatoes with skin
Whole grains like oats and brown rice
Avocados, bananas, raisins
Milk, yogurt, and soy milk
Salmon, halibut, chicken, beef
Fortified cereals
That said, people with IBD often can’t rely solely on food due to absorption challenges. This is where topical support like Sweet Bee’s magnesium products truly shine.
Can You Take Magnesium with Crohn’s or Colitis?
Yes, but with care. Magnesium—especially in forms like citrate—can cause loose stools, which is problematic for IBD patients. That’s why topical magnesium is often a safer, more effective choice.
Always consult with your gastroenterologist before starting new supplements, especially if you’re in an active IBD flare, dealing with kidney disease or if you’re concerned about the medication(s) you are on.
Final Thoughts
In the landscape of IBD care, it’s easy to feel overwhelmed. But as Hollie reminds us, simple, natural tools—when thoughtfully applied—can offer real relief. Whether you’re struggling to sleep, feel calm, or just want to feel like yourself again, magnesium might be what your body’s been craving.
“You deserve to feel strong, rested, and well in your body. Replenishing magnesium levels in a gentle, non-irritating way can make a real difference in how you feel, both physically and emotionally,” Hollie says. “And we’re here to support that every step of the way.”
Learn More About Sweet Bee Organics
To explore Sweet Sleep Magnesium Butter and other clean wellness products created with love and integrity, click here. Use code NATALIE15 for 15% off sitewide.
Sweet Sleep was recently spotlighted on The View Co-Host’s Favorite Things for Mother’s Day. Check out the segment here.
Disclaimer: This article was not sponsored, but the content is for informational purposes only and does not replace professional medical advice. Always consult your healthcare provider before starting any new supplement.
Inflammatory bowel disease is increasingly recognized as a condition associated with systemic complications beyond the gastrointestinal tract. Among these, cardiovascular (CV) complications stand out due to their potential impact on morbidity and mortality. One of the presentations I attended at the Advances in IBD conference that took place in Orlando this month explored the relationship between IBD and cardiovascular disease, focusing on the effects of disease activity and commonly used therapies. This week on Lights, Camera, Crohn’s a look at what we need to watch out for as a patient community and how we can be proactive with our providers.
Cardiovascular Risks in IBD
Meta-analyses indicate that IBD is associated with a 24% increased risk of ischemic heart disease. Moreover, there are higher rates of premature (under age 55) and extremely premature (under age 40) atherosclerotic cardiovascular diseases in our population. The underlying mechanisms are multifactorial, but persistent inflammation and disease activity are key drivers of arterial events.
Heart failure (HF) risk is also elevated among individuals with IBD. Notably:
The risk appears greater in patients with ulcerative colitis compared to Crohn’s disease.
Female patients with IBD demonstrate a higher predisposition to HF than their male counterparts.
Corticosteroid use further exacerbates the risk of HF in this population.
Cardiovascular Considerations for IBD Therapies
Anti-TNF Therapy
Anti-TNF agents (infliximab, adalimumab, certolizumab pegol, and golimumab) have been linked to worsening congestive heart failure (CHF). In patients with pre-existing heart conditions or known cardiomyopathy, baseline cardiac assessment is critical. Recommendations include performing a transthoracic echocardiogram (TTE) before initiating anti-TNF therapy and monitoring for new or worsening cardiac symptoms during treatment.
JAK Inhibitors
The use of Janus kinase (JAK) inhibitors ( Tofacitinib, filgotinib and Upadacitinib) raises concerns regarding cardiovascular risks, including:
Increases in low-density lipoprotein (LDL) and triglycerides.
Development or exacerbation of hypertension.
Major adverse cardiovascular events (MACE).
For patients starting on JAK inhibitors, clinicians should:
Discuss the patient’s cardiovascular history and risk factors.
Perform a baseline lipid profile, with a repeat evaluation at 8-12 weeks after initiating therapy.
S1P Receptor Modulators
Sphingosine-1-phosphate (S1P) receptor modulators, a newer class of therapies for IBD (ozanimod, etrasimod, fingolimod and laquinimod), can impact cardiac conduction. To mitigate risks:
Screen for symptoms suggestive of conduction abnormalities.
Review the patient’s drug history for concurrent use of anti-arrhythmic agents or drugs that prolong the QT interval.
Perform an electrocardiogram (ECG) prior to initiating therapy.
Clinical Implications
Cardiovascular complications are common in patients with IBD, often presenting at a younger age than in the general population. The association between active disease and increased CV risk highlights the importance of maintaining disease control. Non-steroidal options for long-term management should be prioritized, as corticosteroids exacerbate both IBD and CV risks.
Therapeutic decisions should also account for the cardiovascular safety profile of IBD medications. High clinical suspicion and proactive monitoring are essential for detecting underlying or developing cardiovascular disease in IBD patients. Understanding the risks associated with specific therapies, such as anti-TNF agents, JAK inhibitors, and S1P receptor modulators, can guide personalized treatment plans and improve long-term outcomes. When meeting with your gastroenterologist communicate any concerns you may have about chest pain or your blood pressure.
Closing Summary
Cardiovascular complications in IBD patients necessitate a high level of vigilance from healthcare providers. Early detection and management of cardiovascular risks are paramount, particularly in young IBD patients who may already be vulnerable to inflammation-driven atherosclerotic changes. A tailored approach—balancing effective disease control with an awareness of therapy-specific cardiovascular risks—is critical to optimizing care in this complex patient population.
If you’re a young girl or woman diagnosed with a chronic illness, prior or during your “childbearing” years, chances are you or your parents may wonder what this means for your future family. When I was diagnosed with Crohn’s disease at age 21 in 2005, the thought of settling down and having kids was not on the radar but ever since I was a little girl I always aspired to be a mom. Fast forward to 2008, I was hospitalized for an abscess and taken off Mesalamine and put on a biologic injection (Humira). I can still picture the discussion with my GI. My mom sitting on the couch alongside the hospital window, looking at me wide-eyed, and us wondering if I’d ever be able to have children on my new medication. A medication I was told I’d be on for the rest of my life. I was 24. Back then there was nowhere near the research or guidance available like we have today.
August 2008-One month after starting Humira and on heavy duty steroids.
It was the first time I really began to question and worry about whether I’d physically be able to be a mom. As the flare ups, ER visits, hospitalizations, and tests persisted for years, I honestly didn’t have the energy to think about what my life would look like down the road, I only had the energy to focus on what was going on in that moment. I was not a patient advocate and looking back I was a bit naïve and uneducated about what it meant to have not reached remission.
When I met my husband in 2013, little did we know that for the next two years I would be at my sickest. What we did know—is that we both wanted kids one day. After my third bowel obstruction hospitalization in 15 months, I needed bowel resection surgery in August 2015, which FINALLY put me into surgical remission. Ironically, I was engaged to be married. Babies were on the brain. Since I lived a decade without remission, we knew we were going to have to try for a baby as soon as we got married, as remission can be fleeting. At 32 years old, I didn’t want to take any chances.
A lot has happened since we got married. We got pregnant a month after getting married. Lost our second baby around 7 weeks. And then had our rainbow baby in 2019 and our caboose of the family in 2021. If you’ve followed my advocacy and blog, you know I’m passionate about showing all that’s possible despite your IBD. I know each of our journeys is incredibly intricate and unique, each of us deals with our own set of challenges. But I also know that my younger self would have benefited immensely from seeing and hearing fellow women who’ve been there and done it and have families to show for it despite their chronic illness.
This week on Lights, Camera, Crohn’s we hear from several IBD moms—with kids ranging from newborn age to now adults—who offer amazing perspective that I hope will make you feel comfort in what the future could hold for you.
What IBD moms want you to know
Jennifer: “It’s 100000000 percent worth it! And be honest with your kids and spouse about how you are feeling and what you are going through. Of course, make it age appropriate, but they need to know the struggle.”
Liz: “Your kids will learn their limits and love on you when you need rest. It’s ok to go slow. Even if you flare after birth, you will come out of it.”
Amber: “I would tell a younger me that my body WAS capable of carrying and delivering healthy BIG (lol) babies. After struggling with fertility and then conceiving twins and carrying them full-term, I realized my body hadn’t failed me (how I think so many of us with IBD feel. Motherhood is possible for us and thank you Natalie for reminding us of that.”
“Find your people and be honest with them about how you are doing. Don’t ever feel bad asking for help. It truly takes a village to help.”
Brooke: “One day, you will be better. One day, you will coach little league and make the playoffs. One day, you will work on Capitol Hill. One day, you will live in another country. One day, you will be the best mom and you will thrive through IBD. You’re almost there!”
Jaime: “I would tell my younger self that fertility is not something you take for granted especially with a chronic inflammatory disease that can leave you prone to developing scar tissue. I’d also tell her that IBD may make life hard for awhile but with the right doctors, life will improve and the family you dreamed of having will happen.”
Jessica: “Motherhood is hard. It’s ever harder when you have an illness. It’s ok to rest when needed without feeling guilty.”
Kaitlyn: “Your kiddos are more resilient and adaptable than you think they are. I had a major flare about 7 months after my son was born. I put off being admitted to the hospital for weeks because I was so scared and felt guilty for leaving my baby and thinking he would feel abandoned without any way to explain to him that I was gone. He ended up having a blast with my husband for a week and I finally was able to achieve some sense of relief (slowly coming out of that flare, but there is a light at the end of the tunnel). Also, you’re not a bad mom for not being able to do the things you think you should be able to do (Spoiler Alert: Your baby doesn’t know other moms take their babies on long walks around the park and don’t have to drag you into every public bathroom you pass while running errands).”
Patti: “You only get one chance to raise your babies, so don’t sweat the small stuff. And frequently remind yourself (on the roughest days) that you really ARE doing the absolute best you can…and that is OKAY.”
Alyssa: “Sometimes you’ll be holding your baby on the toilet, but you’ll be okay, and your baby will be okay. The road will be tough, but so worth it. Some days the kids will watch more TV than you want, but you must take care of yourself too so you can be present for them. They’re resilient and will love you no matter what.”
Ally: “Rest when you can! Your body will most likely go into remission once pregnant so not need to get scared or nervous about it.”
Liv: “Make yourself and your health a priority. I went into a huge flare after having my first baby because I was SO focused on her and not eating properly or showering or taking care of me. Meal prep to make the mental load of eating easier! And ask for help!”
Patra: “Don’t be so hard on yourself when you feel the need to rest.”
Phoebe: “I would tell her to follow Natalie Hayden’s blog and IG account (haha)…seriously though, when I see you and other people share about their pregnancies and family life, it gave me hope to have my child. I would also tell my younger self it’s ok if you’re a mom with chronic illness! My younger self assumed I had to have a perfectly healthy body to have babies and raise babies.”
“Take care of yourself, even if it means asking your loved ones to look for signs of your anxiety and exhaustion that you may just be trying to push through or ignore.”
Jenni: “I would tell myself not to be so hard on myself. I would say don’t take on all the sick mom guilt. To let them watch movies and eat cereal without stressing about it when I wasn’t feeling well. I would also say…you don’t have to pretend to be brave all the time. It’s ok for them to see you cry or feel frustrated or be sick. They can handle it, and it is creating such strong, caring, empathetic humans!”
Courtney: “I would tell my younger self that I am enough for my kids and that they will be better people because of what they learn and see.”
Mallory: “Your children are strong, and they understand that it’s not your fault.”
Meg: “You did the right thing by staying on your meds through pregnancy and your baby is perfect.”
Kelly: “You are enough. Don’t feel like you’re not able to be as great of a mom as a healthy mom is.”
Ryann: “All you need is love. While I’m sure my son loves the active days when we’re doing lots of activities, he’ll be fine on the days that I’m laying down on the couch as long as I show him love.”
Rachel: “You’re stronger than you know, and everything will work out no matter what happens.”
Amanda: “Not to let fear of the “whatifs” cripple you.”
Brenda: “You will do great and be sure to find a selfless hands-on partner.”
Kristin: “Give yourself some grace. I didn’t get diagnosed or have any Crohn’s issues until my son was 15 months old. The symptoms came on like wildfire and it took a village to help until I figured it all out.”
Anna: “I want to jump in this convo as a 50 year old who wanted to be a mom, but due to the severity of my disease (diagnosed at 18), was told at 29 to have children by 35 due to being high risk and at 34, I was told not to carry due to complications and unfortunately adoption was not in my future as a single woman with severe illness no another option (freezing eggs, etc.) at that point in time. I feel like that is the MAIN thing Crohn’s stole from me! After many years of therapy, I cope with it very well now; however, I still from time to time mourn not being able to have children that aren’t four-legged…#dogmama!”
Courtney: “I would tell my younger self not to worry about having to use the bathroom urgently so much and that you’ll be carrying around diapers, wipes, and a little potty in your car for years. Your kids will also be able to relate to having accidents. I would all tell her that fertility declines a lot faster for people with chronic inflammation and to get your AMH levels checked early. Or think about freezing embryos if you want a big family in your mid to late thirties. Lastly, that breastfeeding won’t stop your kid from having IBD, so don’t worry about giving them formula.”
Ashley: “So, one time I posted on Reddit about how I have ulcerative colitis and didn’t know if I should have kids…I got a lot of responses. I got 56 that told me not to do it. How they were miserable. Or how their mom had it and they suffered as a kid. It was honestly traumatizing. And int that moment, I made the decision not to have kids.”
Tricia: “There will be some really tough days with your illness, and trying to take care of your kids, but you’ll get through this, and better days are ahead.”
Shannon: “Nap when the baby naps is legit. But also, when the baby is 12, you’re still going to need to take a nap. And that’s okay. It doesn’t make you less than because your body requires rest and reset. It is productive to take a nap if it’s necessary.”
Chanel: “That this chronic illness has a direct effect on pregnancy. Having this disease since 7 years old, no doctors ever thought it would be helpful to mention how important being in remission was before getting pregnant or trying for a baby until I was 26 years old and happened to nonchalantly mention to my doctor at the time that we were going to start trying.”
Jennifer: “Don’t worry! You will be blessed with two beautiful children and IBD will not define who you are and will not hold you back from anything!”
Stephanie: “Be easy on yourself and don’t put high expectations on yourself. It will all be worth it. Take it a day at a time and do what you need to do to feel better. Your kids will learn and be more empathetic and compassionate people for it.”
Bhavna: “It’s going to be hard. More emotionally than physically. You will even doubt whether you should have kids for fear of passing it on. I know eventually I did. My daughter now has an autoimmune condition. But despite all of this, you will make it through. Stronger. Resilient. Sometimes a tad sadder.”
Rosanne: “Kids are more resilient than you think. Motherhood is worth having to potentially miss a few things because of a flare or a difficult day. Your kids will understand and be stronger because of it.”
Pie: “Mum guilt will chew you up on the days that you can’t get out of bed. It’s okay, your little one will grow up to be empathetic and understanding of others.”
Amy: “I was completely well for the 8 years I was pregnant and breastfeeding my three boys. Almost a year after finishing feeding my youngest, I immediately went into a massive flare and have not managed to recover yet (10 months now). I felt betrayed all over again by my body, just at the time when I needed it to be strong. I would tell her that the most important thing is that you’re well, so that you can be the best version of yourself. Children are beautiful, they will take you exactly as you. Try to follow their lead. You are enough. They will forget at times you were absent due to resting, appointments, etc. But they will remember how hard you fought for your health. My middle school boy now seems to be suffering with gastro issues and it’s essential to me that I show him that I have the disease, it does not have me (enough though some days that doesn’t quite work out).”
Megan: “Some days are hard, but you can do it! You will be shocked at how much compassion it gives your children. They understand “mommy doesn’t feel well” at such an early age and really want to help take care of us. Vivi asks me daily, “Mommy, does your belly hurt today?” and says, “I’ll take care of you, Mommy.”
Kara: “Don’t forget to take care of you before it’s too late! You are doing your best and your children will only remember that later. My kids are 8 & 10 now, but when I was pregnant with my youngest, I went into a flare and refused to tell anyone or acknowledge it, thinking it would make me a bad/weak mom…so dumb right? By the time my youngest was 1, I was making an appointment for a temporary ileostomy bag. But my kids only remember the sweet stuff.”
Stephanie: “Simply, it’s possible! It was worried for so long that it wasn’t possible, especially once on a biologic and your Instagram page, Natalie, gave me so much hope! Now, less than 2 weeks from delivering my second baby (but my first pregnancy on a biologic).”
Marnie: “I would tell my kids your disease becomes part of your everyday routine, but it doesn’t define you.”
Crystal: “Make sure your baby learns to take a bottle in case you end up in the hospital with a flare.”
Leslie: “Don’t be scared to be on all the medication you need. You’ll get pregnant one day like you always dreamed.”
Keyla: “This journey will be hard but no matter what your little one becomes stronger through it with you.”
Christine: “Here I am celebrating my 47th birthday with my teenagers! One of the first questions I asked my doctor, according to my mom, was will I be able to have kids? That was when I was 23 years old. Here I am at 47, and they have seen me at my best, and unfortunately, my worst. They are truly the reason why I keep going and want to keep fighting at the worst of times.”
Amy: “Your journey might look different than others, but you can still have a family. Also, accept help when you need it.”
Robin: “My kiddos are 27 and 25 now and I was diagnosed when the 27-year-old was 2.5 and the 25-year-old was a baby. She turned one and took her first steps in the family visiting room at the hospital. So, I have the benefit of living with the fruits of my parenting labor. My IBD has taught me that life is precious. Each moment is precious. Because of this, I really tried to take advantage of life when I was feeling well. AND ALSO, I tended to push through when I wasn’t feeling well if something was important to my family, specifically my children. Your first instinct as a parent will be to protect your children from what you are going through – but it’s ok to be open about what you are experiencing in age-appropriate ways. There is no one perfect way to be a parent, much less be a parent with a chronic illness. Give yourself some GRACE.
If dads, or aunts, or family friends, or grandparents are jumping in to chauffeur your kiddos and/or take them to do fun things that you can’t do – IT STILL COUNTS! Your kids are still getting to do the thing. Your kiddos will benefit from having other adults they know and trust in their lives.
Parenting isn’t for the faint of heart. Connect with people that can share the burden. It’s ok to ask for help. I write this while remembering my mantra was “suck it up and figure it out” when they were little. Granted – I was a single parent for a lot of their young life, and I was fortunate to have a strong support system. Even with the support it was difficult to ask for help. SO, ASK FOR AND ACCEPT HELP.
I don’t know what kind of mom I would have been without IBD, but based on who my girls are now, I’m ok with the mom I was and am with IBD.”
Final Thoughts
Hearing this firsthand perspective from all these incredible IBD moms is so inspiring and comforting. It’s a reminder we are not alone in our struggles or our fears—and let’s face it, motherhood isn’t all sunshine and rainbows. But the beauty motherhood brings to our lives and the unbelievable love you feel for your children is the sunshine and the rainbows that makes it all worth it. When you’re an IBD mom, yes there’s a lot of internalized pain and worry. But there’s also so much motivation and joy found in looking into the eyes of your children and knowing that you are enough and will always be enough for them because you’re you.
There are times when their diapers and bathroom habits may set off alarm signals in your head. Don’t think I haven’t brought one of my kids to the ER because I was fearful, they had IBD…wasn’t that. There have been moments where I’ve been bent over making school lunches. There are times I’m on the couch with a heating pad during bedtime stories or in the bathroom mapping out my game plan of how life will go on if I’m hospitalized, and all the moving places I have to orchestrate if I’m out of commission. But SO much overshadows those moments.
As an IBD mom of three, my kids give me such purpose to celebrate each day and soak in each experience I’m blessed to share with them. They provide me with renewed faith in my body and all that I’m capable of. They remind me to laugh and not take life so seriously. When I’m in pain or going through prep for a scope or an uncomfortable procedure my thoughts float to their sweet faces and the incredible memories we’ve shared and it’s the best reprieve from my painful current reality.
When you’re a mom with chronic illness, sure the days can feel long and the years short…but you have a different level of gratitude for what may seem mundane to others. You will second guess yourself more than your children ever will. They are sponges, watching and soaking up their lived experience with you and without even doing anything you’re raising a children with innate empathy and compassion that you’ll see play out as they grow up—I’ve seen it for YEARS with my kids—and while I wish they weren’t the way they are because of my health, I also wouldn’t have it any other way. IBD is a family disease, it impacts way more than just the patient and know that if you choose to carry children, adopt children, or have babies through surrogacy, you are never a burden to your family. You are enough and always will be to your beautiful babies.
My family planning advice for you
My advice family planning
Have the discussion about your future 3-5 years out (if possible) so you can get a game plan in place. Something as simple as letting your provider know…”someday I hope to be a mom”…is sufficient. This sets the stage for what makes the most sense medication wise, targeting and tracking remission, planning scopes so you can get the ‘green light’ before conception, etc.
Do not try and conceive if you haven’t been in remission for at least 3-6 months. Sure, pregnancies are not always planned and can be a surprise but try not to get pregnant while you’re flaring or have active disease as that increases the likelihood of flaring during pregnancy and after delivery.
Once you find out you’re pregnant, alert your GI the same day as your OBGYN and get the ball rolling on finding a maternal fetal medicine (high risk OB) to be part of your care team.
Do not try and go rogue and go off all medications for pregnancy. Talk with your care team. Do the research so you can see firsthand about the safety and efficacy of most IBD meds in pregnancy and breastfeeding and be confident that by keeping yourself well and your disease controlled in pregnancy, you are helping you and your baby.
Check out the PIANO study and MotherToBaby research opportunities so you can help pave the way for future IBD moms and contribute to research. It’s so rewarding, and your voice and input makes a world of difference. My older two were part of MotherToBaby studies and my youngest is part of PIANO, he’s being “followed” until age 18!
Never hesitate to reach out to fellow women with IBD on social media who are moms and receive firsthand advice about their journey so you can feel a bit more at ease about yours.
Ever have a feeling in your gut that says you can trust someone or to make a certain decision? Get diarrhea or constipation when you’re under a lot of stress or anxiety? Your gut is so sensitive and smart scientists call it your “second brain! The human body is a complex ecosystem, with various systems interconnecting in intricate ways. One of the most fascinating of these connections is between the gut and the brain, often referred to as the “gut-brain axis.” This communication network plays a crucial role in maintaining our overall health, influencing everything from mood and cognition to immune function and digestive health. Emerging research indicates that the gut-brain axis may significantly influence the development and progression of IBD. The big question being—how?
This week on Lights, Camera, Crohn’s a look into how the Gut-Brain Axis works and what this means for the future of IBD treatment and care. Whether it’s stress, people pleasing, avoiding emotions, or anxiety—there are many triggers aside from food.
The Gut-Brain Axis: A Two-Way Street
Before we get started, it’s helpful to understand what the gut-brain axis involves and the multiple pathways it impacts, including the nervous system, the endocrine system, and the immune system. The primary components of this axis are:
The Enteric Nervous System (ENS): Think of this as how it feels when you get “butterflies in your stomach”. The ENS is a vast network of neurons (nerve cells that send messages all over your body to allow you to do everything from breathing to talking, eating, walking, and thinking) embedded in the walls of the gastrointestinal tract. It operates independently of the central nervous system but communicates with it via the vagus nerve, which runs from the brainstem to the abdomen.
Neurotransmitters and Hormones: The gut produces and responds to various neurotransmitters and hormones, including serotonin, dopamine, and cortisol. These chemicals are crucial for regulating mood, stress responses, and digestive functions.
The Microbiome: Trillions of microorganisms reside in the gut, forming a complex and dynamic community known as the microbiome. These microbes play a critical role in digestion, immune modulation, and even the production of neurotransmitters.
The Gut-Brain Connection and IBD
Chronic inflammation in IBD can affect the enteric nervous system, leading to alterations in gut motility and sensitivity. Those of us with IBD often experience abdominal pain, cramping, and changes in bowel habits, which are partly mediated by the nervous system. Conversely, stress and psychological factors can exacerbate IBD symptoms. Stress activates the hypothalamic-pituitary-adrenal (HPA) axis, leading to the release of cortisol and other stress hormones, which can, in turn, promote inflammation in the gut.
The Role of the Microbiome
The gut microbiome is crucial in maintaining intestinal health and regulating immune responses. For those with IBD, the composition and diversity of our gut microbiomes are often disrupted, a condition known as dysbiosis. Dysbiosis can contribute to the chronic inflammation seen in IBD by impairing the gut barrier function and promoting an overactive immune response. Interestingly, the microbiome also communicates with the brain through the production of metabolites and neurotransmitters, which influences mood and cognitive function.
You can optimize your gut microbiome with diet by eating:
Low sugar fruits (avocado, bell peppers, cucumber, tomato, zucchini, limes, and lemons)
*Before altering your diet or incorporating foods that could trigger disease activity, please talk with your care team and discuss this further with a registered dietitian who specializes in IBD.
Psychological Factors and IBD
IBD is often associated with psychological conditions such as anxiety and depression. According to the Crohn’s and Colitis Foundation, we’re two to three times more likely to deal with anxiety and depression than the general population. These mental health issues can both contribute to and result from the physical symptoms of IBD. For instance, chronic pain and discomfort can lead to increased stress and anxiety, while anxiety and depression can exacerbate gut inflammation and symptom severity. It’s a vicious cycle that can often feel out of our control.
Therapeutic Implications
Understanding the gut-brain connection opens new avenues for the way we treat IBD. Traditional treatments focus on reducing inflammation and managing symptoms through medications and lifestyle changes. However, addressing the gut-brain axis could provide additional therapeutic benefits. Some potential approaches include:
Probiotics and Prebiotics: These can help restore a healthy balance in the gut microbiome, potentially reducing inflammation and improving gut health. Talk with GI about their thoughts on this, as each provider has their own opinion.
Psychological Interventions: Cognitive-behavioral therapy (CBT), mindfulness-based stress reduction (MBSR), and other stress-management techniques can help manage the psychological aspects of IBD, potentially reducing symptom severity. Tools such as breath work and gut-directed hypnotherapy can help to improve GI systems, while improving your mood and decreasing stress. This works by softening the body’s stress response, inhibiting the secretion of cortisol, decreasing inflammation, and supporting the immune system.
Dietary Modifications: Certain diets, such as the low-FODMAP diet, can help manage symptoms by reducing gut irritation and inflammation. Personalized nutrition plans based on an individual’s microbiome composition are also being explored. Connecting with a registered IBD dietitian can provide you with a personalized plan geared to where you’re at on your patient journey—this will differ if you’re recovering from surgery, pregnant, flaring, the list goes on. Diet is not a one size fits approach, it’s unique to you. Before you start eliminating entire food groups and putting difficult limitations on yourself, talk with a professional.
Pharmacological Treatments: Medications that target the gut-brain axis, such as those that modulate neurotransmitter levels, are being investigated for their potential to treat both the psychological and physiological aspects of IBD.
Final thoughts
Our gut and brain are in constant contact through nerves and chemical signals, and taking care of our mental health and our gut health goes hand in hand. The relationship between our gut and brain is a fascinating and complex one that significantly influences our overall health, playing a pivotal role in everything from mood and cognition to immune response and digestive health. For those of us living with IBD, understanding and addressing this connection can provide new insights into the management and treatment of our disease.
As research continues to uncover the complexities of the gut-brain axis, we move closer to a holistic approach to IBD care that considers the intricate interplay between mind and body. Know that there are psychologists who specialize in gastrointestinal illnesses as well as dietitians who do as well. By adding specialists like this to your care team, you’ll be better equipped to manage the unpredictability of life with Crohn’s and ulcerative colitis.
Imagine a medication that not only helps shed unwanted pounds but also holds the promise of alleviating the painful and debilitating symptoms of inflammatory bowel disease (IBD). For millions battling the dual challenges of IBD and weight management, this could be a game-changer. Some reported data suggest approximately 15 to 40% of IBD patients experience obesity. As obesity has been linked to more severe disease activity, anti-obesity medications, such as GLP-1 (glucagon-like peptide-1) receptor agonists (RA), could be a novel treatment strategy for IBD.
Recent research into GLP-1RA medications, primarily known for their role in weight loss and diabetes management, suggests they might have unexpected benefits for those with Crohn’s disease and ulcerative colitis. Could these medications pave the way for a new era in IBD treatment? This week on Lights, Camera, Crohn’s let’s dive into the intriguing possibilities that lie at the intersection of weight loss and inflammatory bowel disease management. You’ll hear from gastroenterologist and researcher Dr. Aakash Desai, along with 25 people who have IBD and have tried or are currently taking GLP-1RA medications.
What is a GLP-1RA medication?
GLP-1 (glucagon-like peptide-1) medications are primarily known for their role in managing type 2 diabetes and obesity. GLP-1 agonists, such as liraglutide (Victoza), semaglutide (Ozempic), and dulaglutide (Trulicity), mimic the action of the endogenous hormone GLP-1. These drugs enhance insulin secretion, inhibit glucagon release, slow gastric emptying, and promote satiety, thereby aiding in blood glucose control and weight loss.
The majority of these drugs are subcutaneous injections, with only one currently available orally. The frequency of taking the medication varies with each GLP-1RA and can be weekly, daily, or twice daily. But, the typical dose is a weekly self-injection, which can be done in your stomach, upper arm, buttocks, or thigh.
The Mechanistic Link to IBD
Anti-inflammatory Properties: GLP-1 receptors are present in the gastrointestinal tract and on immune cells. Activation of these receptors has shown anti-inflammatory effects in preclinical studies. This suggests that GLP-1 medications could theoretically modulate immune responses and reduce inflammation in the gut.
Mucosal Healing: Animal models have demonstrated that GLP-1 agonists can promote mucosal healing in the intestines, a critical aspect of managing IBD. This potential for enhancing intestinal barrier function and reducing inflammation holds promise for IBD therapy. Scroll to the bottom of the article to check out the latest research.
Considerations between providers and patients
Dr. Aakash Desai, MD, Allegheny Health Network in Pittsburgh, Pennsylvania says that before discussing if GLP-1RA is appropriate for his patients, he tries to understand their weight loss journey on a case-by-case basis.
“This is unique for every patient, so it’s important for the physician to understand where they’re at and the efforts that have been made. I like to ask what type of dietary and lifestyle modifications they have attempted, exercise (finding out actual numbers, number of days/minutes per week of exercise, moderate/strenuous intensity), prior consultations with nutrition and/or weight loss specialist, and prior exposure to weight loss medications. It’s also important to consider comorbidities, especially history of pancreatitis, gallbladder disease, type 2 diabetes mellitus, and psychiatric diseases including eating disorders.”
He tells me a “good” candidate is a patient who is obese or overweight with weight-related complications who is willing to undergo lifestyle interventions in close collaboration with nutrition and a weight loss specialist. From an IBD standpoint, before starting on this type of medication, Dr. Desai likes to see his patients in remission.
“GLP-1RA medications have several GI side effects, so it can be challenging to differentiate if a patient’s symptoms are related to GLP-1RA, active IBD or both. Patients should have their IBD in remission, clinical and endoscopic, and radiographic, if applicable,” explained Dr. Desai.
There is preclinical data suggesting that GLP-1RA can modulate inflammatory responses.
Dr. Desai explained, “Mechanisms include its impact on oxidative stress, immune cell recruitment, cytokine production, and gut microbiota modulation. There is also some clinical data from retrospective studies showing improved IBD outcomes, however we need data from prospective studies to see if these medications can be used as adjuncts with existing IBD therapies.”
He would not recommend starting GLP-1RA for obesity management during a flare/active disease given the risk of drug related GI side effects. This could worsen symptoms which could inadvertently lead to increased dose of steroids, prolonged steroid use or a change in IBD therapy. Additionally, providers prescribing GLP-1RA have a low threshold to discontinue the medication if patients with IBD develop even mild GI symptoms out of potential concern for worsening IBD.
Ongoing research underway
Dr. Desai is working on a study that involves 150 people with IBD who are obese and taking semaglutide.
“We found similar weight loss compared to patients without IBD. We also found higher weight loss with semaglutide compared to other anti-obesity medications except tirzepatide. We did not observe worsened IBD specific outcomes in patients on semaglutide. In another study from a large database, we found that GLP-1RA use for type 2 diabetes in patients with IBD was associated with a lower risk of surgery for ulcerative colitis and Crohn’s disease, but we did not observe a lower risk of steroid use.”
He tells me it’s important to note that this is retrospective observational data. However, Dr. Desai hopes this sets the stage for prospective studies and future randomized controlled trials.
From a safety standpoint, there is limited data, however it appears to be reassuring for serious side effects. Dr. Desai believes until we have more robust data, the key will be disease remission at the time of initiation of GLP1-RA. Keep this in mind if you are dealing with active disease and hope to start this type of medication.
There is no data to suggest that patients on biologics or small molecules cannot be on a GLP-1RA if their disease is in remission. The approach needs to be individualized factoring in clinical characteristics and disease profile.
Scope and Scans and GLP-1s
There seems to be confusion in the patient community about how these weight loss mediations can impact how we prep and undergo scopes and scans. Dr. Desai says there is currently no data supporting stopping GLP-1RA before elective endoscopy – which is a multi-society statement.
“I follow the clinical practice update published by American Gastroenterological Association (AGA) which suggests an individualized approach to each patient. If patients are on GLP-1RA only for weight loss, I think there is little harm in holding the medicine a week before elective endoscopy. An alternative would be to continue the GLP-1RA and place patients on a liquid diet the day before the procedure.”
Dr. Desai says he likes to discuss extended bowel prep (2 days) with his IBD patients.
“Alternatively, I recommend a low fiber low residue diet for 5 days plus 2 days of a clear liquid diet with 1 day of prep. I would encourage patients to discuss management of GLP-1RA and bowel prep with their IBD providers prior to elective endoscopy as institutional protocols especially for anesthesia may vary.”
Hear what an IBD mom has to say about her experience
Emily says she’s been overweight most of her life. She tried everything to lose weight, and nothing seemed to work—or she’d lose weight and gain it right back. She talked with her primary doctor about the weight loss medications and her provider is a big fan of them for the right person and thought they’d be a great fit for her. As an IBD mom of two boys, Emily was worried about what her gastroenterologist would have to say.
“At first, I was nervous about it because I didn’t want him to tell me I couldn’t do it. But he was okay with it. He said if I didn’t have any IBD complications, that I would be fine to be on it. He didn’t have any hesitation since I have been in remission and my colonoscopy and upper endoscopy looked good. I explained that I was followed closely with my primary and that I would let him know if I had any issues that came up. Thankfully, my Crohn’s has stayed in remission!”
Emily started semaglutide in November 2022 and was on that for 7 months and then switched to tirzepatide. She’s now been on that for one year.
“I am starting the process of going into maintenance and will decrease my dose until I find what works for me and plan to stay on this long term.”
Emily’s remarkable transformation from 2022 to now.
She’s currently taking Stelara to manage her Crohn’s. Emily is down 93 pounds, and she feels amazing. She says she has dealt with minimal side effects—some nausea and constipation, but nothing that lasts long. As most of us are, she’s very conscious of her bathroom habits and says if she starts to feel constipated, she takes stool softeners.
Firsthand experience from an ostomate
Elizabeth has perianal Crohn’s and has participated in two clinical trials (stem cells). She has had two gracilis flap surgeries, among others. She says while many IBD patients struggle with keeping weight on, this has not been the case for her.
“I have always been in a larger body (even before my Crohn’s diagnosis 20+ years ago). I workout daily and eat a balanced diet but have, like many, found a natural weight plateau. Since my bloodwork always looks great, I really hadn’t thought about it as it would be seemingly for vanity’s sake.”
With more than a dozen IBD surgeries so far and at least one or two more in the future, she was discussing with her GI wanting to optimize future success post-operatively, when her doctor brought it up.
“Since I carry more weight in my mid-section and currently have a loop ileostomy, which also is poorly placed and with a hernia that causes further projection, addressing those issues was certainly on my mind. I was open to learning more and she was bullish, referring me to a fellow GI doctor who specialized in the area.”
As an ostomate, Elizabeth was concerned about blockages, in addition to insurance not covering the cost.
“My consulting doctor felt confident I was a good candidate, and we both thought it may actually improve my fast GI tract and high-output ostomy (which had been causing daily leaks recently). While insurance denied two different options based on plan carve outs, even after appeals, I decided to try paying out of pocket.”
She started on Zepbound four months ago, in conjunction with her biologic and small molecule medication to manage her IBD. Elizabeth says she was less concerned about adding a medicine but, like many of us, would like to be on fewer longer term.
So far, she has lost 30 pounds or about 12% of her starting weight!
“I wasn’t at my highest all-time weight, but I had gained. The effect was almost immediate for me — with the biggest short-term (and continued) win being the delayed gastric emptying, meaning less liquid output, less rapid output, and less visits to the bathroom to empty. I also stopped having leak issues almost completely and, in conjunction with my IBD meds, my symptoms and inflammation are the best they’ve been in years.”
In terms of the non-IBD effects, the impact on what they call “food noise” was huge and, because food stayed in her stomach for more than an hour or two, her hunger changed dramatically.
“I can’t explain how odd it feels to have to remind yourself to eat and to simply feel full. Fortunately, I have had few side effects as, thanks to my ileostomy, I was already focused on staying hydrated.”
Elizabeth encourages those with IBD to research and consult with a doctor who specializes in obesity medicine (and versed in IBD and/or willing to work with your IBD team). Unlike many of the medications we use to control our disease, antibodies aren’t a concern, and it could be worth a try. Also, she says not to be discouraged if it doesn’t work for you as, just like IBD meds, what works for one person may not work for someone else.
“While the weight loss is great, the impact on my IBD-related quality of life has been just as important. I hope there is more research in this area and potential a path for these medications to be considered as part of a covered treatment plan for patients with IBD and other chronic conditions.”
What other IBD patients have to say
Thank you to those who submitted input for this article—there’s nothing like hearing firsthand perspectives from those living our reality. I have purposefully left all the quotes anonymous.
“I have been on Wegovy for over a year, and I have ulcerative colitis. I’ve had a positive experience and from what my GI told me, there are clinical trials going on for its effect on IBD patients specifically.”
“I started Ozempic last week. My GI approved it. There is lots of research about reducing inflammation, along with other benefits. I am way overweight, and I needed help.”
“I’m on semaglutide, which is the generic compound of Wegovy. My GI approved it and it’s been great. It’s the only way I’ve been able to lose weight in years! It has helped me with cravings, with blood sugar stability, and with my emotional connection to food. The first six weeks, I lost my interest in food and had a weird metal taste in my mouth. But slowly that went away and now I am back to myself but feeling more in control and with a healthier view of food. I have not lost weight as fast as some, more like 1-2 pounds a week with a plateau where we found the dosage needed to be increased. Slow and steady has been fine for me.”
“I have ulcerative colitis and got a jpouch back in 2010. I was on Ozempic last year but got off to get pregnant. Once I’m six months postpartum I was told I could go back on it.”
“My CRP is back to normal, even though my SED rate is still elevated, my IBD is non-existent. My constipation did get worse though. But it’s nothing that daily Miralax can’t help. I had to come off it because it made my anxiety worse. Being on that medicine made me as close to feeling like a normal human being as ever.”
“I have been on Ozempic for the past month. No lie, best I’ve felt in years! It’s taken my 20 bowel movements a day down to 3-4. I have nausea, but it’s tolerable. I don’t have diabetes, so I’m paying out of pocket for it. Those with diabetes get a greater benefit from it. You have to be serious about eating protein and about eating better. Since the food you eat sits in your stomach longer, you’ll feel sicker if you’re just eating junk.”
“I would love to hear more about this as IBD is one of the contra indications for this medication and is not usually prescribed in the UK for people with Crohn’s/ulcerative colitis, as it can cause GI upset. So, I would love to hear more about people’s experiences with this as this is something I have looked into for my weight, and I have Crohn’s.”
“My PCP said in her experience they have helped GI outcomes, but I haven’t talked with my GI to see his response. I will say, as an OR nurse, we have been seeing a lot of exploratory laparoscopic surgeries with patients on these medications.”
“I have UC and they put me on Ozempic last year! One shot and I couldn’t stop vomiting. I lost 35 pounds, but I had to take Zofran daily and used a Scopalamine patch so I would not vomit. I started in April, and I didn’t get better until July or August. I went into the ER and urgent care several times for dehydration. It was mild pancreatis, but my labs were not bad enough for them to admit me.”
“I was on Victoza! My GI symptoms were exacerbated by the medicine, but my A1C went down significantly. Unfortunately, I was throwing up for the first month I was on it and because of that my appetite was not suppressed.”
“I was on Ozempic. It made me nauseous and sick. I had terrible stomach pains and TMI, but super gross mucus-y stools. As soon as I stopped, everything went back to normal. I lost 20 pounds and then gained it all back immediately.”
“I have Crohn’s and I’ve been on Saxenda for 8 months and I’m down 20 pounds. Other than a little nausea in the beginning, it’s been great for me!”
“Started semiglutide injections 2 weeks ago and I’ve been able to stop taking my Loperamide completely (I have ulcerative colitis and a jpouch). Semiglutide wasn’t covered by insurance even with appeals for weight loss and motility, but I got it pretty affordable online through Henry Meds. I’m still on the loading doses but haven’t had side effects so far. It takes about 2-3 months of weekly injections to build up to a full dose.”
“I experience nausea day two after taking the shot. Other than that, I haven’t dealt with anything negative. I lost weight that wasn’t coming off due to hormones being completely screwed from pregnancy and 60 mg of prednisone for almost 9 months. GLP-1s also constipate you, due to your gut not emptying as quickly as it normally would. This is one of the reasons it’s being explored as an IBD option. Taking magnesium, bulking up on fiber or taking fiber helps with this.”
“I am on semeglutide week 6 tomorrow—this is my second time—I did it last summer for about 3 weeks. I went up on my dose last week, I haven’t noticed a difference with anything yet, but I haven’t changed my diet much and that’s on me. There’s no difference in my ulcerative colitis symptoms, I’ve had mild active uc for awhile now. I’m trying to get it under control, but also need to lose a bit of weight.”
“Back in 2022, I was on Mounjaro for about 8 months. I was finally able to lose weight. I am a Crohnie who gains weight because my body has a hard time digesting nutrients. Because of this, my body is in starvation mode a lot. When I was on Mounjaro, I lost about 80 pounds, and my inflammation was well managed. It was the first time I was able to feel energetic and wasn’t tired all the time. It helped with my diarrhea because it made me constipated for the first time in 5 years. It then became regulated. I still had stomach pains and indigestion issues, but overall, the medication improved my quality of life quite a bit. I am pre-diabetic and now my insurance will not cover it. My doctor tried appealing it many times, explaining that Mounjaro was helping to manage my inflammation caused by Crohn’s disease, and they still denied it. I have gained 30 pounds back and have a hard time with energy and my diarrhea has returned on and off.”
“I’m on Mounjaro and taking it specifically to help with my high output ostomy. I have Type 2 diabetes, so I’m able to get it through insurance luckily, since we’re using it “off label”. A friend of mine who has a jpouch was on Saxenda, then Ozempic, for the same reasons. She recently had to go off it because of new insurance and she developed pouchitis within weeks of having to stop it. I have two other friends with ostomies taking it, both with a history of Crohn’s. One is a CEO of a biotech company and has been chatting with the different GLP-1 manufacturers trying to convince them to do trials in patients with short gut or high output ostomies.”
“The first thing I asked my GI doctor is HOW can someone have IBD and be overweight or obese? And he said it’s quite common! When I started to flare, he wanted to blame the diarrhea on GLP-1 (Wegovy). But I asked him for a colonoscopy which showed active ulcerative colitis, unrelated to the medication. I am now on Zepbound. For some reason, these medications don’t help me lose weight. I can’t help but wonder if the inflammation from IBD is preventing successful weight loss. I can have many bowel movements a day and not lose a single pound!”
“I have had a good experience with it. I have a really tough time eating vegetables and some fruits, nuts, etc. because of my Crohn’s. The fact that the medication decreases that hunger helps me maintain a healthy weight. I tell people that all the “food noises” I used to experience are gone.”
“I am researching this for Crohn’s myself. I am interested to see your article and opinion. I’m in the UK and recently heard about the benefits of microdosing and I wanted to see if IBD people had experienced positives.”
“I was originally on Ozempic, and it wrecked my stomach. I had to take a break from it, but I lost weight. I switched to Mounjaro due to insurance and have had way better luck with no GI issues. Altogether, I have lost almost 50 pounds. I should mention that I am pre-diabetic. I have a really hard time losing weight. When I was pregnant, I lost 35 pounds after I gave birth and didn’t gain a pound during. I felt amazing, not sure why I wasn’t hungry when I was pregnant. Mounjaro has allowed me to not think about food 24/7. It’s been a game changer.”
“I’ve Googled it before (because who that’s overweight hasn’t been at least curious) and I remember reading that because it slows digestion it can help IBD patients. I’m still worried about the unknown long-term effects to try to it.”
Final thoughts
It’s important to understand that these are chronic medications for obesity management. GLP-1RAs are not a substitute but should be used in conjunction with lifestyle interventions including diet and exercise. This is necessary for sustained long-term weight loss. This requires a multi-disciplinary team-based approach with nutrition, weight loss specialist, primary care and your IBD provider.
As you heard from the patient community, access and cost for these medications remains a key issue for many. The high cost and complex insurance landscape pose significant barriers for many patients seeking these treatments. The monthly cost of these drugs in the United States can range from several hundred dollars to over one thousand dollars, presenting a substantial financial burden for patients. Many insurance companies require prior authorization for GLP-1RA medications, necessitating extensive documentation and justification from healthcare providers. This process can be time-consuming, and as we’re all too familiar with, may delay treatment.
I’ll leave you with an impactful quote from Emily, “I think for the right person these meds are life changing. I know for me they have been. There is a lot of chatter on both sides, and I have learned to block it out. I work closely with my primary doctor and know that she would never steer me wrong. I also know that my GI is on board and that has helped, too. Don’t let the opinions of others deter you. If this is something you want to do and you have the support from your doctors that is all that matters!”
The moniker “IBD Mom” is commonly used in the patient community. As a mom with Crohn’s disease who has three children, I focus a great deal of my advocacy efforts on family planning, pregnancy, and motherhood. But I recognize the decision and choice to have children isn’t for everyone. Studies on voluntary childlessness among people with IBD suggest a higher prevalence compared to the general population. Research has indicated that concerns about health, the impact of the disease on parenting ability, and the potential genetic transmission of IBD are significant factors influencing this decision.
So, what about the women who make the personal and often emotional decision not to have children or who didn’t have the option to choose, due to health complications? This week on Lights, Camera, Crohn’s a look at being childfree and the many factors that may deter people from becoming parents. You’ll hear from several women in the IBD community about their decision.
Key factors that influence being childfree
Disease Activity: Active IBD puts a halt on family planning, as women are told to be in remission 3-6 months prior to conception. The unpredictability of the disease can make finding the right timing to have a baby tricky. If a woman conceives while flaring, there is a much greater likelihood of flaring during pregnancy.
Medications: Some of the medications used to manage IBD can pose risks to a developing fetus. If a woman finally finds a treatment protocol that gets her IBD under control it can feel daunting to stop and risk losing remission.
Surgical History: Surgeries for IBD, especially those involving the intestines and rectum, can affect fertility and pregnancy outcomes.
Genetic Considerations: IBD has a genetic component, meaning there is a risk of passing the disease on to offspring. While this is a major deterrent for many, it’s important to understand what that risk is. For Crohn’s, there’s a 7% of passing on your disease and even less for ulcerative colitis. When both parents have IBD that number goes up astronomically.
Physical and Emotional Well-Being: Managing IBD is physically and emotionally demanding, trying to imagine what it is like to care for yourself and take care of a child can be overwhelming for many.
Firsthand accounts from the patient community
Kat: “This doesn’t mean I won’t change my mind in the future, but my health has had a huge impact on why I have decided not to have kids. I think a big part of not wanting to carry a baby anymore is because of the trauma my body went through when I was sick in my 20s.”
Rachel: “I was diagnosed with Crohn’s disease almost three years ago, and I’m on my second biologic. I’m 25 and have decided that I don’t want to carry my own children. Due to the currently unknown effects of biologic drugs on development, but also the risks for myself coming off a biologic and flaring. I have also considered the complications of having a c-section before or after other potential abdominal surgeries and the complications from that. The main one for me though is also the genetic chance of passing IBD on to my kids. I have always been open to adoption anyway and have decided this is the route I would pursue if I do decide to have children.”
Kate: “We are going through fertility treatments after five years of secondary infertility and I chose to stop to start Rinvoq and save my rectum. I am not having my eggs retrieved and frozen in the hopes that we find a gestational carrier for our embryos.”
Kendall: “I am 30 and single and haven’t made the firm decision to be childfree, but as I get older and my Crohn’s disease gets more challenging, it’s definitely something that I’ve been questioning. Wondering if I will have the health and energy to be able to take care of myself and my kids. I worry about the impact of pregnancy on my body and of course finances are also a consideration.”
Alesha: “I’ve questioned being a mother. I’m 33 and I was diagnosed with Crohn’s in 2022. After having a perforated small intestine in 2015, an ostomy for 6 months, and the reversal in 2016…only to suffer with so much pain from the scar tissue being so narrow. I’d visit the hospital a few times a year and try to work through the pain. Now, I’ve been on Stelara for a little over a year. It’s been helping, it’s just hard to be told that the medication will be lifelong. While I desire to be a mom, I just don’t know how my body will respond.”
Liz: “I have chosen not to have kids for many Crohn’s reasons: Having to come off meds to protect pregnancy, the risk of flares and them causing infertility anyway (my periods always stop in a flare), the massive risk from common childhood illnesses, adhesions due to surgery and just the added stress and time needed to devote to a kid to raise them is something I just can’t do on top of a career as a doctor.”
Meredith: “I’m currently in this situation now. My husband and I held off having kids until we were ready (different components here—moving, reaching career milestones, enjoying our lives as they were, but in the past few years we felt we were ready except my body wasn’t. I had a terrible flare that knocked me on my ass for about a year and then I was put on my methotrexate and was told I could not become pregnant, or I would need a medical abortion. I’ve since gotten off that medicine but was told to hold off trying until after my colonoscopy. I had another small flare, and my GI wants me to wait until I’m healthier. He says, “healthy mom, healthy baby” and I don’t think he’s wrong, but it isn’t what I want to hear. So now, I’m just waiting to see what happens.”
Sarah: “Not sure what I’m looking for because I have two kids, but I had them prior to my Crohn’s diagnosis at age 30. The diagnosis prevented us from having more children. We always planned on four kids, but because of my diagnosis, we didn’t continue to try and only have our two that I had before developing Crohn’s.”
Belinda: “We’ve decided not to have any kids. I know my history with my Crohn’s hasn’t been as bad as some other ladies who would struggle to conceive and carry a child. I might have been fine to. I had two resection surgeries, at age 24 and 39. The first one was very traumatic, and I was very sick for many, many years. I just didn’t ever feel I wanted to take a risk to “rock the boat” as I’m always trying to keep my health stable. I didn’t feel I had it in me to manage a potentially difficult or risky pregnancy or bad flare after the baby. I do think there might be other reasons why we’ve decided not to have kids, so it might not be fair to blame it all on my Crohn’s. I’ve never had the urge or yearning to be a mom. It’s very prevalent in my family, too. Three out of four cousins on my dad’s side have Crohn’s and my mom’s cousin does, too. The nature of the world, healthcare issues, and so many other issues make me wonder if it influences would-be mothers. Our health is already such a scary unpredictable element of our being…who has the capacity to navigate it all?”
Kelsey: “I’m childfree by choice! I’m a professional auntie. I was diagnosed with ulcerative colitis after I had already made that decision, but it has 100% solidified it. I’ve watched my other childfree friends waiver with their decisions and some choose to have children later in life.”
Deanna: “I got married in October and my husband and I talk about this a lot. I never expected I’d be childless, but I don’t have a strong drive to have children either. The fact that the decision was made for me is something I am trying to navigate emotionally.”
Jessica: “I was always on the fence about children, even when meeting my partner six years ago when we were 25. I decided a few years ago that I did not want to have children. While there were a few factors in my decision, my ulcerative colitis was a big decision to choose not to. Stress and lack of sleep (I need at least 8 hour a night) are a prime duo for flare ups for me. I knew that if I was going to be lacking sleep in the many stages of childhood, and stressed many times, I wouldn’t be able to care for myself, and therefore wouldn’t be able to truly take care of children. I know there are so many moms out there with IBD or another autoimmune disease that are rocking it, but this was the right choice for me.”
Courtney: “To be honest, having children was just never something that was on my mind in my twenties and thirties. I was diagnosed with ulcerative colitis in college and had a colectomy in graduate school. During most of that time, I was in a 10-year relationship. Towards the end, it became clear we had different ideas about where our futures were headed. He wanted a traditional family life in a small town, and I wanted to focus on my career and stay close to my medical team in an urban area.”
Ashley: “I’ve been really scared due to medical trauma and not feeling ready to trust my body. It’s hard because I have a strong desire to have a child, but it would also mean putting myself back into situations that genuinely scare me.”
Kaycie: “My IBD is one of the several reasons I decided to be childfree. I was so sick throughout my early to mid-20s when I finally went into remission in my late 20s, the last thing I wanted was to risk falling out of it to have a child. I’m in my mid-30s now, living abroad for work, traveling all the time, and able to have the freedom I craved in my 20s when I was chained to a toilet with my ulcerative colitis. A child just doesn’t fit the life I’ve built, and my husband and I are happy with that choice.”
Lauren: “I miscarried many years ago and was told I was high risk at the time and that it would be a battle to get pregnant and carry full term. After being diagnosed with Crohn’s, I didn’t think it would be healthy to try further with my body. With so many flares and surgeries, we decided if we had children we’d adopt. It was like grieving a major loss of something I’d always wanted. I love my life and my marriage. I had a few great years of remission and have been flaring for about one year now. I’m not comfortable adopting when my health is so on and off. I don’t think it’s fair to a child or my husband to not always be present.”
J: “For me, every time we were going to try for a second child, something my with health would come up. I’ve had a collapsed lung, broken rib, inflamed pleural pace, and IBD flares. Between all those health setbacks, coupled with chronic fatigue, it felt like I couldn’t get to a place healthy enough to support a second pregnancy and even if I could, I wouldn’t have the energy to survive the first three months postpartum with such little sleep going on. So, we opted to no go for more and be as present as we could for our existing child.”
Casey: “My husband and I have had a to delay trying to conceive due to a flare and were going to delay trying even further as I just had to switch from Humira to the biosimilar, Hyrimoz. I don’t want to be pregnant while navigating a chance in medication in case it doesn’t work the same.”
Hannah: “There is still quite a lot of taboo around being childfree and it isn’t something I feel I can share with everyone. I don’t have a strong desire to be a mother. It’s difficult to know how much of that is due to my challenging childhood and adolescence due to my Crohn’s. I have a vivid memory from when I was 11 years old watching my siblings playing outside from the bedroom window and of being very upset that I didn’t have the energy to join them. That memory is very poignant and painful for me. It’s one that has been at the forefront of my mind as a 34-year-old woman as I decide whether to remain childfree. I fear repeating that feeling of being at the periphery but this time as a mother, rather than as an 11-year-old girl. Another fear is that I might pass on Crohn’s to my child. While the risk is small, I would find that difficult to bear.”
Lizzy: “I’ve had IBD for almost two years. I am on Remicade and methotrexate. Since methotrexate can’t be taken during pregnancy, it would be concerning number one of having to switch to a pregnancy-safe alternative and hope it works as well as my current regimen. Additionally, periods make my Crohn’s symptoms worse, so I haven’t had a period in over a year due to birth control. Having to get off birth control and deal with horrible symptoms sounds miserable. I get sick when I don’t sleep, and it wouldn’t be fair to always make my partner get up in the middle of the night. I am also gay so going through the stress of IVF or artificial insemination when trying to maintain Crohn’s remission would be stressful.”
Sexual and reproductive considerations
Amy Bugwadia is an MD student with scholarly concentration in medical education/health equity and social justice at Stanford. She collaborated with some IBD patients and clinicians and authored a paper about sexual and reproductive health considerations. She says, “while we were writing and listening to patient feedback there were a few salient themes:”
Mis and dis-information
Stigma: patients being too shy or not knowing if this is a topic that they can or should talk to their GI about
Confusion about language: Doctors saying “you can’t get pregnant while on this med”—do they mean “difficulty getting pregnant” due to potential infertility or “should not get pregnant” due to potential medication impacts on the fetus.
Outdated information: Many patients (especially when young) have been on the certain medication for a long time, but as time has gone on, we have new/updated data on safety profiles that not all patients are up to date on, especially relevant for pediatric patients as they transition to young adulthood.
Voluntary childlessness or being childfree among individuals with IBD is a multifaceted issue influenced by health concerns, genetic considerations, quality of life, and psychosocial factors. As you heard from several IBD women, the decision to remain childfree is often a carefully considered and personal choice determined after talking with healthcare providers, significant others, family, and support networks. I hope after reading this you feel less alone if this is your reality—whether it’s something you’ve always wanted or if it’s a decision you struggle with.
Crohn’s disease and ulcerative colitis can cause symptoms both in and out of the gut. When our disease wreaks havoc on other parts of our body, outside of our intestines, it’s known as an extraintestinal manifestation (EIM) or complication. Did you know, according to the Crohn’s and Colitis Foundation, anywhere between 25-40% of people with IBD experience some type of EIM? EIMs arise in the joints, skin, eyes, bones, kidneys, and liver or as anemia. This week on Lights, Camera, Crohn’s a deep dive into the heavy toll of living with not only IBD but the EIMs that come along with them and how more than 30 patients manage these issues that can significantly impact the quality of life and overall health of IBD patients.
One of the most interesting quotes from a patient was that while one man doesn’t like EIMs, he’s grateful for them because that’s often the only time family, friends, and medical providers can see with their own eyes what a serious illness IBD is. It’s heavy, but it makes sense. IBD is so much more than a bathroom disease and EIMs go to show how severe Crohn’s and ulcerative colitis can be and how this is a full body disease.
The most common EIMs associated with IBD
Joint problems: This is the most common EIM and affects around 25% of IBD patients. The pain normally occurs in the knees, ankles, and wrists, but can also happen in the spine in the form of ankylosing spondylitis. For many of us, our biologics or biosimilars are approved to treat both IBD and rheumatoid arthritis and this can help alleviate joint pain.
Skin Conditions: The two main conditions are Erythema nodosum and Pyoderma gangrenosum. EN is characterized by tender red nodules that usually occur on the shins. PG is a more severe skin condition that causes painful ulcers. Those with IBD also have a greater chance of developing skin tags, anal fissures, and fistulas, both Enterocutaneous (from the intestine to the skin) and Perianal (around the anus that can drain blood, pus, and/or stool.
Eye Disorders: When those with IBD deal with red eyes, pain, and vision problems, uveitis and episcleritis tend to be the culprit.
Kidney complications: Medications tend to cause this, and serious kidney complications associated with IBD are rare, but still can happen in the way of kidney stones, hydronephrosis (an obstruction of the ureters, which connect the kidney to the bladder), and fistulas (abnormal connections between the intestines, bladder, or ureter). Amyloidosis (an abnormal deposit of protein in the kidneys) and Glomerulonephritis (inflammation in the kidney that limits its ability to filter properly) can also occur.
Liver and Biliary Tract Diseases: Primary sclerosing cholangitis (PSC) is a serious liver disease is most commonly seen in conjunction with ulcerative colitis. This is often discovered when lab works show liver markers are out of whack and it’s diagnosed with a liver biopsy to determine the stage and level of severity. Fatty Liver Disease, Hepatitis, and Gallstones are also considered EIMs.
Bone Health Issues: Osteoporosis and osteopenia can result from years of chronic inflammation, steroid use, and malnutrition. It’s a good idea to get a baseline DEXA bone scan and to get scans periodically to make sure you’re not experiencing this.
Lung Issues: While this is less common, lung involvement can include airway inflammation and interstitial lung disease.
Managing EIMs along with your IBD
Managing and treating EIMs is no easy feat and often necessitates a multidisciplinary approach, including your gastroenterologist, rheumatologist, dermatologist, and other specialists, depending on what organs are affected. Treatment strategies might include non-steroidal anti-inflammatory drugs (NSAIDs), immunosuppressive medications, and biological therapies which are tailored to reduce inflammation and manage symptoms.
You may wonder if there’s any way to prevent EIMs from happening in the first place. There are several strategies that can help reduce your risk, but much like anything with IBD, don’t blame yourself if EIMs keep happening to you and feel out of your control.
Effective IBD Management: Controlling your IBD through appropriate medical therapy is crucial, whether that’s in the way of aminosalicylates, steroids, immunomodulators, and biologics/biosimilars. The goal is to reach and sustain remission of your IBD, which can help reduce the risk of EIMs popping up.
Communicating when you see a change: Once you notice a possible EIM, it’s imperative you share this with your healthcare provider. Early detection and treatment of EIMs can prevent them from getting more severe. A simple message on the Portal to your GI addressing your concern or worry helps alert your doctor so they can take the appropriate measures before symptoms spiral out of control.
Lifestyle Modifications: Smoking is known to worsen the course of IBD and increase the risk of EIMs, especially in Crohn’s disease. Consulting with a dietitian who specializes in IBD can help ensure you are receiving adequate nutrition and getting regular exercise can help reduce inflammation, improve bone health, and enhance your overall wellbeing. Speaking of bone health, calcium and vitamin D supplements can help counteract the lasting effects of steroid use and malnutrition.
Collaborative Care: By branching out from your GI and seeking care from specialists, you have the best bet of ensuring EIMs are treated promptly and effectively. Talk with your GI about the potential signs and symptoms of EIMs so you know what to watch out for and have a game plan in place if one were to arise to feel more in control.
Medical gaslighting and EIMs
Unfortunately, far too many patients and caregivers feel symptoms are dismissed or not taken seriously by healthcare providers, which can be particularly discouraging and frustrating.
“I had a tough time getting my consultant to take me seriously. The eye problems were “probably just bad eye strain,” the mouth ulcers were “maybe the cups in the office not properly being cleaned, and the rashes were “probably a reaction to laundry detergent or maybe insects getting on my clothes while they are on the clothesline outside.”
Here are some helpful strategies to help you speak up in these situations and feel empowered to advocate for your health effectively:
Document Your Symptoms: You may think you’ll remember what’s going on, but life with chronic illness gets hazy and when we think back, we can lose sight of the actual frequency and intensity of what we’re going through. A detailed diary will help provide concrete evidence to discuss with your healthcare provider and may even help assist in identifying patterns that are relevant to your diagnosis and treatment.
Seek Second Opinions: If you don’t feel listened to or heard, don’t hesitate to get a second opinion, and find a provider you jive well with. Each doctor has varying levels of experience with IBD and EIMs, find the person who best understands your personal situation and is willing to get you to where you need to be, rather than dumbing down or belittling your experience.
Be Prepared for All Appointments: Write down a list of questions and concerns before your appointments. Bring your symptom diary and any other relevant medical records. By being prepared, you can better focus and ensure that you’re capitalizing on the one-on-one time you have with your doctor while you’re face to face.
Bring an Advocate: Having a trusted friend or family member at your appointment can provide support and help ensure that your voice is heard. That person can also help remember details on the appointment that you may not.
Be Clear and Assertive: There is a delicate balance between being assertive about your concerns without being confrontational. Be descriptive and transparent about the impact your symptoms have on your daily life, paint as clear a picture as you can and explain why it’s important for these symptoms to be addressed.
Educate Yourself: By understanding what EIMs are ahead of your appointment you can feel more confident about asserting your concerns and how best to improve your health. If you’re able to “talk the talk” with medical language about your condition, your healthcare professional will be more apt to listen.
Formal Complaints: If you repeatedly feel as though you’re dealing with an unprofessional doctor who has a dismissive attitude, or if you feel your care is compromised, it may be necessary to share a formal complaint with the medical facility.
Let’s hear from IBD patients and caregivers
Leah daughter was diagnosed with Crohn’s when she was five.
“Little did we know our most difficult days would come a few years later and be due to an extraintestinal manifestation of her IBD. It started off as bruises on my daughter’s shins. I thought it was related to her sledding on her knees with the recent snowfall. Unfortunately, I had never learned about Erythema nodosum being related to IBD and would later learn this is what she had. The spots on her legs grew and grew. They eventually got raised and painful. I emailed our GI nurse and thankfully she instantly knew and sent us for stat labs. My daughter was on Humira and wasn’t in remission, so the drug was increased. Week by week things got worse and more painful. The redness and swelling covered her entire shins. The bumps spread to the bottom of her feet and were extremely painful. Her feet swelled and she was crying in pain and no longer able to walk on them.”
Leah ended up taking her daughter to the ER where she got steroids and started on antibiotics as it looked like the spots had turned into cellulitis on her feet.
“I was not prepared that EN could be associated with IBD. I wish I had known earlier, so her condition could have been treated more aggressively from the beginning. It was many months before she healed, and her maintenance medication was switched.”
Emilie– “This is such an important topic and I wish it were discussed more! Most of my UC complications have revolved around extraintestinal manifestations (as opposed to typical UC symptoms). I have had arthritis and uveitis and for me, extraintestinal manifestations always come first, before a typical flare and always stay long after the typical UC symptoms have resolved. At times, I’ve just had extraintestinal manifestations without any typical UC flare symptoms. The most frustrating part about EIM symptoms is that most GI doctors aren’t super familiar with them and only think they happen after a UC flare. Thankfully, I’ve been followed by a rheumatologist since I was diagnosed (because I had EM symptoms long before I had typical UC symptoms and saw a rheumatologist first). My rheumatologist is always like, “we follow people with these symptoms to see if they develop IBD” and many of my GI doctors have said, “this can’t be because of your UC.”
Dina was diagnosed with UC in January 2022 after experiencing IBD-related symptoms six months prior. Since then, she’s had pneumonia, mono, CMV, RSV, and other illnesses. She went from weighing 150 pounds to 120 and was so weak she could barely walk. She was switched to Entyvio/Rinvoq as a combo therapy along with an anti-viral drug used to treat HIV to try and keep the CMV virus at bay. The CMV made her liver markers skyrocket, and it was discovered she has Stage 1 PSC, in addition to everything else.
“I consider this a blessing because once I went back on the full dose of anti-viral my liver counts normalized. We never would have known about the PSC until it got severe or at a later stage. My GI said he’s never seen PSC in this early stage, so I’m grateful we can start earlier than most to monitor it.
Lynette-“I’ve dealt with many EIMs. To manage my anemia, I take iron and having a hysterectomy helped. For my kidney stones, I stay hydrated with electrolytes daily. I had surgery for hemorrhoids and fistulas. I’m on medication to manage my joint pain and use my heating pad. I use a special toothpaste to prevent cavities and I floss daily. I do everything I can to reduce stress and anxiety—from breathwork, to meditation, and openly communicating with my family.
Madison-“My personal experience is severe joint pain and swelling, as well as erythema nodosum. My IBD flares typically begin with joint pain. At times, it can be so severe I can’t walk up and down stairs because my ankles are so swollen. When I was first diagnosed with Crohn’s, in addition to my joint pain, I started to develop red tender bumps all over my legs up to my knees. They were so painful to touch, and they were diagnosed as Erythema nodosum which only occurs in about 10-15% of Crohn’s patients. Once we got my IBD under control and found the underlying cause of my joint pain and erythema nodosum they thankfully got better.”
Myisha- “I experience inflammation in my eyes three to four times a year. I also deal with osteoarthritis. Mentally, I’ve checked out on my Crohn’s awhile ago. I just take it day by day. I have eye drops that I have to use daily to help with inflammation, but osteoarthritis is painful and some days I want to cut my limbs off. I always try to remind myself that someone out there has it worse and today might be a high pain day, but the darkness doesn’t stay around forever, eventually the sun will shine again, and I’ll have a low pain day.”
Christopher- “I’m 46. I was diagnosed with Crohn’s about two years ago. Three years before that I began having panic attacks and anxiety out of nowhere. I went from never having anxiety or panic to multiple incidents per week. At the same time, I had new joint pain in my knees, and developed arthritis in my shoulder joint as well as mild lower right quadrant pain. Now, looking back, these were all related to systemic inflammation from the undiagnosed Crohn’s. Now that I’m in remission, it’s all gone away.”
Vern– “OMG EIMs!?! I have so many. Along with Crohn’s, I have developed Gilbert’s Syndrome, short gut, Reynaud’s, rigors, kidney stones, skin problems, anemia, B12 and vitamin D deficiency, joint pain, fissures, fistulas, and hair loss. There’s not much to do when it comes to Gilbert’s, Reynaud’s, rigors, or skin…but with kidney stones I drink a lot of water everyday plus cranberry juice or tea every once in awhile. To manage my anemia, B12 and D, I take easily soluble supplements and B12 shots every month. I take Tylenol to manage my joint pain and rest. The fissures and fistulas have a mind of their own, so not much I can do until it’s taken care of surgically if it gets bad enough. The hair loss is from medication and even when I tried different treatments (home remedies) nothing worked until I was off the medication.”
Pao-“I have been experiencing skin issues for the last year and a half. I have a lesion under my armpit, behind my ear, and a gangrenous epidermis, which is healed. I had a biopsy on the lesion and then a corticosteroid cream healed it. The lesion on my ear won’t go away after months of putting cream on it.”
Kerry-“I deal with intense joint and muscle pain all over my body. My left hand got so swollen at one point that I tried to learn to write with my right hand. This was during my initial diagnosis. Once I started on Remicade it helped and now my joint pain is an indicator of disease activity for me. I log symptoms using the Wave app, I increase my rest, and use diclofenac gel as a topical analgesic. I also see a rheumatologist who has experience treating other IBD patients.”
Rocio: “One of my most debilitating and constant EIMs I’ve had over the last 20+ years is iron-deficiency anemia (IDA). The fatigue levels I live with are beyond frustrating. I know the disease itself can add to my fatigue, but even when at my healthiest, I’m constantly tired. And it’s the kind of tired no on understands. I’ve received countless IV iron infusions for my IDA as I can’t tolerate oral iron due to my previous history of chronic constipation. Fortunately, infusions and I’m able to go months without iron, but there have been times where I’ve received 5 infusions in 1 month – yikes!”
One of Rocio’s other debilitating EIMs is uveitis. She says it is truly one of the most excruciatingly painful manifestations.
“Despite having a high pain tolerance due to chronic illness, uveitis has been one experience I don’t wish upon anyone. And uveitis can progress to glaucoma or vision loss. I did have glaucoma along with my uveitis, but we treated it immediately. Due to recurrent uveitis flares and limited treatments that worked for me, I dealt with uveitis for nearly 3 years. The ophthalmological EIMs that can occur with IBD are not one to take lightly…we need our vision!”
The earliest EIM Rocio experienced were perianal fistulas – a common type of enterocutaneous fistulas. Unfortunately, she did not receive proper care initially, or her actual IBD diagnosis, for five years. She could have suffered far less had her fistulas been identified as an EIM of Crohn’s disease.
Jennifer-“So many doctors are just unaware or unwilling to see extraintestinal manifestations for what they are. When I was in my late teens and struggling with depression and a ton of stress in my first year of college, I was shamed by a doctor and told (without any testing) that I had herpes. Mind you, I had never been sexually active and never had symptoms before this point. I was in extreme pain and had painful ulcers from my mouth to my anus and genitalia. I left the appointment in tears and wanted to die. It was only years later that I learned of external manifestations of Crohn’s and had a doctor confirm that is what happening all those years earlier.”
Jennifer says she had far too many unpleasant encounters with doctors over the years. From doctors telling her that she was just a bored homemaker (because he felt my complaints were made up) to dentists shaming her in front of her kids (because her mouth health was in his opinion from lack of hygiene vs. effects of Crohn’s disease).
“I was also told by a GI doctor once that if my Crohn’s disease flared while pregnant that I should just have an abortion (for a pregnancy that I very much wanted). This is not a commentary on my stance on abortion, but rather the lack of empathy and respect that this male doctor had towards me, my health, and my choice in that moment.”
Becky- “Erythema nodosum is so scary and I had no idea what was happening to my legs. It was so painful to even walk. I’ve lived with Crohn’s for 30 years. I was admitted to the hospital and given steroids and the doctors drew black Sharpie circles around the red swollen lumps on my legs to see if they grew larger. I was there several days, and the doctor finally figured out what was going on based off my medical history. I was on steroids for awhile and then it finally cleared up.”
Liz- “Extraintestinal manifestations are one of the toughest parts of Crohn’s for me. I have joint aches, eye inflammation that is so painful and disruptive when it flares and chronic severe anemia. Each result in another doctor, another expensive treatment, and time not feeling well. Getting doctors to recognize that they are all connected is difficult as well.”
Anthony has lived with Crohn’s for almost 18 years and EIMs have been a big part of his journey. To him, they’re often a key indicator that a flare up is on the way and unfortunately EIMs have become a regular part of his life for the past decade.
“I get a lot of eye problems (swelling, overly sensitive to light, foggy vision). Once I woke up with my left eye swollen shut. I get a lot of ulcers on my gums, tongue, and in my throat along with rashes that break out on my arms, back, and hands. When I get ulcers, I have difficulty swallowing and need to consciously put effort into swallowing my tablets and often I’m forced to stay away from solid food and meals.”
Anthony goes on to say EIMs bring on depressive episodes for him, along with brain fog, and having issues concentrating and remembering.
“Some days I wake up at 4 or 5 in the morning with a cement block of sadness in my chest, preparing to go about a “normal” day and hoping not to feel the urge to burst out crying. Before I learned how to live with it and got mental therapy, I had to write almost everything down to the point of keeping a note on my phone with bus and train times that would get me to and from work or to various parts of the city because I’d draw a complete blank at times or couldn’t figure out the timetables. I am an engineer and almost had to give up my career because I couldn’t get through a workday.”
Deb– “I’ve had reoccurring Pyoderma Gangrenosum under the flange or baseplate of my ostomy to the point that the skin and tissue diminished and has now caused a very significantly sized peri stomall hernia. We haven’t landed on a treatment of late that has any amount of effect on the inflammation in my colon, so no hernia repair until we get the CRP way down.”
Courtney-“I’ve experienced blepharitis, which is an inflammation of the eyelid that may commonly be confused with pink eye. I’m not fully clear if it is an extraintestinal manifestation or side effect of immune suppression, but after 5 years “in the clear” it’s back. One of the few occasions when I actually “look sick” but feel fine. It’s treated with antibiotic eye drops. I saw a specialist who recommends a special cleanser with tea tree oil.”
Amanda-“During a particularly bad Crohn’s flare, I developed Erythema nodosum. They were painful welts that went up and down both legs. My legs got so swollen and covered with welts that I couldn’t bend them to walk. It was incredibly painful and difficult to need help just getting out of bed. They took awhile to go down and left bruises all over my legs. No one ever mentioned this to me as a possibility, so I didn’t even think to contact my GI, but my local emergency room doctor pointed me in the right direction.”
Krista– “Oof. Alopecia. I lost probably 50-75% of my hair. Now it’s thicker than it’s ever been. Very strange. I also have experienced bursitis and inflammation in my knees, but that’s only flared up once since my IBD diagnosis.”
Melanie-“I was diagnosed with IBD when I was 12 and by 15, I could no longer walk upstairs due to Crohn’s-related arthritis. I went on Remicade which got me walking again but have since been looking for options. Sometimes my Crohn’s and Arthralgia flare together, but in my experience, when I get one under control, I start having issues with the other one which can make disease management a challenge.”
Tish- “I got Uveitis and must always be on the watch for signs of it now. It was misdiagnosed as an eye infection, and I was sent to the eye and ear emergency, but they also misdiagnosed it. Thankfully, I was able to see my ophthalmologist who correctly identified and treated it properly. I also have very dry eyes, so I always use drops to avoid it leading to another Uveitis flare up.”
Eliza– “I’ve dealt with bone density issues related to my ulcerative colitis. I now take a prescribed high dose of D3 and incorporate calcium and other minerals as often as I can into my diet. I have been getting DEXA scans since I was 19!”
Allison-“Skin!! Why are there no IBD-expert dermatologists anywhere?! Why can’t my doctors give me more information about extraintestinal Crohn’s related skin issues? Are we really suggesting bleach baths as the only path for resolution because that feels insane. I’m struggling to find the right resources to help.”
Stacey-“I developed Type 2 diabetes as a result of the inflammation in my pancreas. In addition to diabetes, I also have Rosacea caused by my Crohn’s. We first thought it was an allergic reaction to my Stelara. However, the Rosacea persisted after I stopped Stelara. I saw a Dermatologist who made the diagnosis, and I was then able to get back on it. Like many IBD patients, I also deal with dry eyes, dry mouth, fatigue, and achy joints.
Dana– “I’ve struggled with cutaneous Crohn’s (perianal and elsewhere) and oral Crohn’s, including mouth sores, gum inflammation, and recession. I’ve been prescribed a lot of various topical medications (tacrolimus, taclonex, steroids…just to name a few). It causes a huge gluteal cleft fissure and a lot of damage to my skin in the perianal area in general, which was resolved when I had my proctocolectomy surgery. They had to cut my rectus abdominis muscle to create a flap and place it in the area where they had to cut out all the tissue and skin. Regarding oral Crohn’s, I have steroid ointment that I use as needed for inflammation/sores and I’ve had three gum graft surgeries so far.”
Gabriella-“I have chronic urticaria and dermatographia that was triggered by a rare reaction to the carrier protein used in Humira and Remicade. The reaction hasn’t gone away despite stopping those medications, and despite taking Xyzal and Benadryl daily. I still have extremely high IgE levels. I had had all the major inflammatory skin conditions associated with Crohn’s as well: Erythema nodosum, Pyoderma gangrenosum, and just general infections from “normal skin flora.” I’ve had multiple bad IBD flares where I’ve experienced inflammatory arthritis in all joints from my hips down.”
Ben-“I was diagnosed with gastroduodenal Crohn’s and UC over 30 years ago when I was six. Back then, it started with Erythema nodosum, which led to a colonoscopy, when then ended in my first polyps removed and a diagnosis. I still have issues with it today. I also picked up an obscure kidney cancer about five years back. My oncology and GI teams feel it is related to my Crohn’s/UC somehow, as they don’t see this type of cancer in patients under age 80. Crohn’s also gives me severe anemia.”
Stephane– “After 15 years of partial obstructions, during which I amazingly enough, managed to avoid diagnosis or treatment, it was the obviousness of an extra-intestinal manifestation, my left ankle swelling for no reason, which marked the beginning of the end of my epic denial. Over the summer, my knees swelled too, and walking became painful and slow. By September, I couldn’t walk at night because of the pain in my joints and had to crawl to the bathroom. Finally appearing in the ER, sent by my GP, ankles, and knees puffy and swollen, anemic, malnourished and down 30 pounds, the doc only needed to glance at my chart and test results to give me a diagnosis of Crohn’s.”
Amanda-“Extraintestinal manifestations I’ve dealt with include mouth ulcers, inflammation of my eyes (so red!), joint pain (specifically knees and hands), TMD (no classic clicking or popping, just mass inflammation of the joint and muscles), eczema, anxiety, slow wound healing, fatty liver (non-alcohol, I don’t drink, I am a fitness and nutrition professional so I know my lifestyle is on point), and kidney stones.
Amanda manages this by having exceptional oral hygiene. She brushes and flosses twice a day and uses Orajel mouth wash. She sees an Ophthalmologist to ensure she doesn’t have damage to her eyes and uses Lumify drops to combat the redness. Amanda takes a curcumin supplement (primary bioactive substance in turmeric) for its anti-inflammatory properties, which may also help with joint pain. She uses a bite splint and warm compresses for her TMD and eczema patches on her face, around her ears, eyes, and neck. Amanda has two different prescriptions from her dermatologist to address this: hydrocortisone cream and fluocinolone oil. She also uses Skin Smart antibacterial eczema spray every night. To deal with the remainder—she practices stress reduction when and where she can, continues to focus on her diet and weightlifting and keeps her sugar intake low. She doesn’t drink alcohol and only takes moderate caffeine each day. She’s also hyper focused on micronutrients, specifically fiber, vitamin D, iron, zinc, folate, and B vitamins for overall health and wound healing. Her Avsola infusion for her IBD also is approved to treat Rheumatoid Arthritis so she feels that helps her joints feel significantly better.
Dealing with the mental health challenges of EIMs
Much like IBD, EIMs take a toll on our mental and emotional wellbeing. By seeking mental health support from a psychologist or counselor trained in chronic illness management, you can receive valuable support. Cognitive behavioral therapy (CBT) is particularly effective for managing depression and anxiety associated with IBD. If this article has done anything, I hope it’s shown you that you are not alone and sadly how common these complications are in our community. By simply going on social media and looking up hashtags for your EIM, you will see so many others who are living your reality and can learn a thing or two and feel understood, seen, and heard. There’s so much power that comes from us joining forces as a shoulder to cry on and an ear to listen, even if we’re thousands of miles apart.
By educating yourself and being proactive about what could happen to your body now or in the future, it can help reduce fear and anxiety that is associated with these unexpected and often unruly symptoms.