This post is sponsored by the American Gastroenterological Association (AGA). I am a paid program Brand Influencer; this post is sponsored and includes my own personal experiences.
Breastfeeding is a labor of love. Like many women, it doesn’t come easy for me. As an IBD mom who already fears passing my disease down to my kids, there’s added pressure and stress. In the United States, an estimated 1.6 million people have Crohn’s disease or ulcerative colitis. Of those, roughly half are women, and most will carry the diagnosis during childbearing years, throughout all phases of family planning: trying to conceive, pregnancy and postpartum. As an IBD mom of three going through postpartum right now, one of my biggest stresses and focuses revolves around breastfeeding.
-What if I take this pain medicine for my Crohn’s? Will I need to supplement?
-What if I have a postpartum flare, will my milk supply go away?
-What will happen if I’m hospitalized?
-Will I flare once I stop breastfeeding and my hormones regulate?
-If I stop too soon, will my child end up having an increased risk of IBD?
…the list goes on…
The journey to motherhood for women with IBD requires several complex decisions and coordination among specialty care teams from the stage of family planning until postpartum and beyond. The IBD Parenthood Project aims to address common misperceptions and fears women with IBD and their providers experience throughout all phases of family planning (conception, pregnancy and after delivery). By eliminating the gray area and serving as the gold-standard for navigating pregnancy and motherhood with IBD, our patient community can rely on this support that helps uncomplicate the journey.
This beneficial and much-needed initiative was created by gastroenterologists (GIs), maternal-fetal medicine (MFM) subspecialists, and patients and is led by the American Gastroenterological Association (AGA) with support from the Society for Maternal-Fetal Medicine, the Crohn’s & Colitis Foundation, and patient support network, Girls With Guts. The IBD Parenthood Project launched in January 2019, just as I delivered my second child. To this day, I feel so grateful to have this information and confidence in my choice to become a mom even though I’ve lived with Crohn’s disease for more than 16 years. It’s empowering to know despite the unpredictability of IBD, this initiative allowed me to feel like I’m in the driver’s seat when it came to creating my family and knowing the choices I’ve made were and are supported by science and medical facts.
To the random lady in the church elevator who asked me if I was breastfeeding my son Reid when he was a month old, and I was a first-time mom.
To the lactation consultant after I delivered my daughter Sophia, who told me since I have Crohn’s, it’s imperative her gut only be lined with breastmilk.
To the nurse coaching me nonchalantly about breastfeeding my son Connor and underestimating the challenges it can present…who I later found out “only” breastfed one of her children for 2 weeks…
To anyone who is struggling with the physical, emotional, and mental stress of something that sounds “easy” and “natural” — simply feeding your baby — I get how complex and taxing it is. I’m in the thick of it now with my son who was born July 14. So far, he’s only had breastmilk…both from nursing and by a bottle. But it’s not pretty for me. The engorgement, the round the clock pumping, the soaked t-shirts, the night sweats, the discomfort to even wear a bra or sleep on my side. It weighs on me. There’s the outside pressure and the pressure I put on myself to keep going, even though I don’t enjoy it. It’s super rewarding to see Connor thriving and making gains all because of me. But there’s also a lot of stress to be a child’s only source of food, especially as an IBD mom.
Different feeding approaches with all my babies
With my firstborn in 2017, I wasn’t well-versed on the benefits of breastfeeding and feared not only further exposure to my biologic, but also flaring, so I only breastfed my son for 3 days in the hospital so he could get colostrum. By 2019, I was well-versed on the positive impact and the safety profile associated with breastfeeding while on a biologic, so I breastfed my daughter until she was 6 months old. I had hopes of making it a full year, but unfortunately my milk supply disappeared once my menstrual cycle started back up. This time around, I felt the anxiety about having to breastfeed creep up when I was only a few months pregnant. Between research showing that breastfed babies have a lower risk of IBD, coupled with antibodies from the COVID-19 vaccine, I feel the need to do all I can to protect my son from the what if, even if it feels mentally, physically, and emotionally taxing each day.
The Fourth Trimester has several challenges for women that often go undiscussed. However you choose to feed your child is your business and should be based on what is best for you and your family. This is a judgement free zone. I’ve fed my three babies differently. But the pressure mounts when you yourself have an illness with no cure and feel as though breastfeeding can help improve your odds of not passing it on to your offspring. In my mind, down the road, I don’t want to ever think I coulda, shoulda, woulda done anything differently when it comes to protecting my offspring from IBD.
The IBD Parenthood Project tackles some of the common questions related to breastfeeding as an IBD mom. There’s a downloadable toolkit that features patient-friendly information and easy-to-digest lists of key questions to ask your doctor as you’re thinking of becoming pregnant and beyond.
What I Want Fellow IBD Moms to Know
Navigating motherhood while taking on IBD is overwhelming. With proper planning, care and coordination among treating healthcare providers, women with IBD can have healthy pregnancies and healthy babies—and breastfeed if they choose to do so. For me, breastfeeding provides a sense of normalcy and gives me a renewed sense of love for what my body is capable of, despite having Crohn’s disease. Give yourself credit for going through pregnancy with IBD, delivering a baby, and continuing to nourish your little one with your body when they are in the real world. The blood, sweat, and tears are inevitable.
Just this week I experienced awful abdominal pain. The kind of pain where you can barely breathe, your hands start to tingle, and you go back and forth about whether a trip to the emergency room is imminent. As I rocked myself on the toilet and heard my newborn crying in the bassinet my mind raced. My 4-year-old stood before me. I could see the fear in his eyes. My immediate thought was—what can I take to get this pain under control—will it affect my ability to breastfeed? In that moment, the pressure to think outside of myself and manage my disease felt suffocating.
There comes a point when the mental health and wellbeing of the mother must come first so she is able to be the best version of herself for her kids. If breastfeeding is taking away from the joy you could be experiencing or the connection you are longing for with your child, don’t feel guilty. Whether your child is exclusively breastfed, or formula fed, or receives a little of both, they will thrive. I’m personally all about flexible feeding. A little nursing, some pumping, and some formula has worked best for me. When the time comes, and I need a break or feel too consumed by being the sole provider of nourishment for Connor, I’ll feel confident in supplementing with formula. There’s no shame in my game and there shouldn’t be in yours, either. Take advantage of invaluable resources like the IBD Parenthood Project and be confident in each of your personal health decisions when it comes to whether or not you want a family and how you choose to feed your baby.
When IBD mom Jessie Magaro was pregnant with her first child, she knew early on she wouldn’t be able to carry another baby herself. Between the hormones from IVF and her Crohn’s disease raging, there was no way her or her doctors felt comfortable embarking on another pregnancy.
Before she got pregnant, Jessie had been in remission for more than 12 years. With pregnancy and IBD, there’s the ‘rule of thirds.’ One third of women will see their symptoms improve, one third will stay the same, and one third get worse. Unfortunately, Jessie fell into the last category. Since having her daughter, Mary Ligon on New Year’s Eve 2018, Jessie’s gotten an ileostomy and has grappled with her Crohn’s being out of control. When her and her husband started thinking about baby number two, she knew surrogacy was her safest and smartest option.
“My daughter Millie (born in April 2021) needed me more to be there as her momma once she got here than she needed me to carry her. Not only was my baby safer, but I was in a much better position health-wise to care for both my daughters.”
The Surrogacy Process
Surprisingly, the FDA controls surrogacy and has specific requirements for the IVF part of the process. Jessie recommends making sure your fertility clinic is well-versed on how everything goes down. Surrogates and biological parents go through medical testing and psychological evaluations prior to the transfer of the embryo.
“This was probably the hardest part for me mentally and emotionally. I was so frustrated and hurt that I had to pay someone a pretty penny to tell the government that I was mentally ok to have my own baby. It was just pouring salt into an already large and festering wound. Can you imagine having to have a stranger tell you if it was ok or not for you to bring your own child into this world?”
It’s important to note that surrogacy laws vary state to state, but in Georgia (where Jessie lives), you must adopt your baby back from the surrogate, even if the child is 100% genetically yours.
“You hire an attorney (one for yourself and one for your surrogate) and they actually file a lawsuit claiming your parental rights to the unborn baby on your behalf. I had to go before a judge and field questions on why I was pursuing surrogacy and whether or not I felt my husband and I were able to take care of the child once it was born. Again, insult to injury.”
There are several ways to go about surrogacy:
You can hire an agency to find you a surrogate and manage the process
You can use a friend or family member (they will still have to be medically and psychologically cleared by the clinic)
You can try to find one via word of mouth in your community.
There are tons of Facebook groups where you can “match” with one (local, regional, national, interest groups i.e., christian, altruistic, low comp, natural minded, etc).
“Normally, you would be able to attend all OB appointments with your surrogate, but Covid made things a little trickier for us. We were unable to attend the transfer, which was sad, but I was able to go to a fair amount of the appointments. My husband unfortunately wasn’t allowed to attend any. We both were allowed to be in the room for the birth though and that was the most important thing to us.”
The experience of having a surrogate
Jessie says had she not been able to carry her first child that she feels surrogacy would have been harder on her. She feels so fortunate that she was able to experience pregnancy once.
“I had already gotten to a place mentally and emotionally where I knew the only way to get my daughter here safely was by having someone else carry her. I wasn’t ever triggered per se by seeing a pregnant belly because I knew she was safer inside our surrogate. I had so much PTSD and trauma from my first pregnancy as well that looking at another pregnant person never made me think “oh man I wish that was me again” if that makes sense. I did/do still deal with mourning though over how pregnancy played out for me and that I was unable to carry safely again. I also find myself spiraling occasionally thinking about how much it cost us to get our children here versus someone who could just have them themselves naturally. It’s been a massive financial burden/sacrifice for my husband and I (but oh so very worth it).”
The Financial Cost of Surrogacy
When looking into surrogacy, Jessie tells me you can ballpark around everything costing $100,000. There are many factors involved that play into whether that number is more or less depending on if you’ve already gone through IVF and have embryos. Much like IVF, there are some grants available for surrogacy, though much less common.
“The ways to bring the cost down for surrogacy would be to do an “independent journey” like we did where you don’t use an agency. You can also use a surrogate (whether it’s a friend, family member or even a stranger) who does not want to be compensated or wants very little. Medical bills will bring the cost up or down significantly depending on insurance plans and same with your legal fees as those will vary based on the surrogacy laws in your state.”
Defending her Decision
While Jessie says it was empowering to make the decision to utilize a surrogate to do what was best for her health and for her family, it’s been frustrating to constantly feel like she still needs to defend her decision to other people and even some doctors.
Whether it was …
“Aren’t you worried about having another child when you’re so sick?”
“Why don’t you guys just adopt??”
“Aren’t you worried the surrogate will want to keep the baby?”
“Aren’t you worried she won’t know you/you won’t be bonded to her??”
“Just one kid is great you should just be ok with having just the one”
etc …
“I know most of the time these comments don’t come from a place of mal-intent, and I try to use them as an opportunity to educate if it feels productive, but everyone is different what they’re open to accepting in their heart and their mind. In my mind, the girls are going to know the stories of how they came to be eventually, and hopefully they’ll see how wanted and loved they were. How unbelievably hard they were fought for. And how many people played a part in bringing them into this world.”
Managing IBD and Motherhood
Prior to looking into surrogacy, Jessie and her husband had to discuss at length if they would be able to handle a second child with her IBD. They also had to loop in their families knowing they would need their help when they couldn’t manage everything on our own.
“My husband and I say all the time, in all seriousness, that my illness has become a third child in a sense. There’s not a day, hardly an hour, that I don’t have to think about my Crohn’s or manage something with it in some way. It’s a difficult balancing act every day when I wake up trying to prioritize who needs the most at what moment (my kids, myself, or even my husband). I deal with a lot of guilt and grief with that. That I’m not the mom or wife I want to be … that I’m not able to give everyone what they need and deserve.”
Jessie often thinks of the oxygen mask analogy and says as an IBD mom it’s imperative to make sure her proverbial mask is on and secured first before she can help anyone else, which is very hard to do as a mother.
Meeting Millie the Day She Was Born
It makes Jessie emotional to think about what it was like to walk into the hospital with her husband and know they were about to meet their daughter. They were able to be in the delivery room when Millie came into the world.
“I had an overwhelming sense of gratitude looking at our surrogate knowing what SHE went through and had sacrificed to get her here. All the anxiety I had been suppressing for months and months from having someone else carry her, to giving up all control, to doing it in the middle of the pandemic, to being so scared something would go wrong like it so often had for us in the past. It just all came pouring out of me uncontrollably as she was pushing. The moment she was placed in my arms it just felt like a lightning bolt connecting us. I felt bonded to her instantaneously. She was mine and I was hers and there was nothing on this earth I wouldn’t do to protect her.”
Jessie knew from the start of this journey that her surrogate would be a lifelong friend. Their families grew close through the process, and they live nearby one another. She says she’ll always hold a deep place in her heart for her and is incredibly grateful to be a family of four.
This post is sponsored by Naturally Free from IBD—all thoughts and opinions are my own.
She’s a doctor with IBD who says her call to medicine began from her own hospital bed. Dr. Christina Campbell, DO, Certified Functional Medicine Physician, Board Certified Emergency Medicine was diagnosed with Crohn’s disease 40 years ago when she was only 12 years old. She’s utilized her own personal struggles and setbacks to guide the way she treats patients and helps others in our community. Through her own journey, she says many doctors left her feeling frightened, unmotivated, even angry. Christina learned early on about the importance of bed-side manner, compassionate care, and the gift of not only listening, but hearing what a patient is expressing. Her overarching goal—to be a physician who inspires faith, confidence, and a will to fight within her patients.
She’s dedicated her life’s work to facilitating and growing the value of a patient-physician partnership rather than what she calls a “DOCtatorship.” Christina believes that a personalized approach to health works better than recipe medicine, meaning she’s passionate about finding the root cause of disease and improving underlying health and the body’s biochemistry by intervening at the level of the root cause, through a functional medicine approach. Before we dig into the amazing work she’s doing, let’s take a walk down memory lane to see how Christina got to the point where she is today.
Christina’s Journey with Crohn’s
A diagnosis of IBD in 1983 looked a lot different than present day—and not for the better. When she was 14 years old, Christina faced a near death experience from extensive bleeding and lesions from her mouth to her anus. Her gastroenterologist said she had one of the worst cases of IBD he had ever seen and shared her case at global medical conferences and in case studies. Christina was averse to undergoing a complete colectomy and colostomy, so she underwent six months of bowel rest (nothing by mouth). She received all hydration and nutrition through an IV in her veins around her heart called a Hickman catheter. At the time, the only medications available for Crohn’s were Sulfasalazine and Prednisone. Can you imagine?!
Since her diagnosis, Christina has been on many different medications through the years (Asacol, Delzicol, Sulfasalazine, any number of antibiotics, steroids, Toradol, Tylenol, Tylenol #3, Vicodin, Percocet, Compazine, Phenergan, Tigan, Tagamet, Pepcid, Bentyl.) When the first biologic was approved for treatment of Crohn’s (Remicade in 1998), she was in remission and graduating from medical school.
“My personal story is fraught with difficulties and each of my struggles has blessed me with a deep understanding of others and the ability to empathize and connect with patients. I have learned how to listen and really hear what they are saying. I have learned the power of creating a therapeutic partnership. My goal for each of my health participants is to match their lifespan to their health span. Quality of life alongside quantity of life is key. My personal journey has taught me that it only takes one step in a new direction to change the entire path of one’s life. It has also shown me the power of understanding your personal timeline. Looking back at our past journey helps us to understand the path that has led us to where we are,” Christina explains.
The Power of Responding to the Root Cause
Before Christina knew how to treat root cause issues and was solely utilizing conventional medicine, she says her immune system remained dysregulated. She was treating her symptoms with medications that acted like band-aides without addressing the cause.
“My functional medicine training has taught me the value of information and the concept that many with the same diagnosis may have completely different root causes. Utilizing detailed functional labs to discover altered biochemistry is an incredible tool to getting things back on track. These labs are not used in conventional medicine where the focus is on illness, not on wellness. It is a completely different perspective, which makes all the difference in helping someone find not just improved health, but optimal wellness.”
When it comes to discovering optimal wellness, Christina says this includes investigating genetics, epigenetics, metabolomics, oxidative stress, cellular energy and mitochondrial health, detoxification pathways, gut health and microbiome imbalances, inflammatory factors, and so much more.
“Once we uncover this information, we can begin to make changes personalized to your life, your body, your biochemistry, your genetics, your mind, and your spirit. Patience and grace with oneself are paramount to health as are understanding and forgiveness.”
The Transcend 3-step signature program
Christina works with IBD patients through her 3-step signature process to discover the root cause of symptoms, intervene at that level, revitalize health, and teach people how to maintain and excel for the rest of their lives. She uses natural and lifestyle interventions to create a personalized program which improves the health participant’s innate healing abilities to reverse symptoms, decrease pain, and improve all aspects of their lives.
“My Transcend program is my signature 3-step process which guides you through your precision blueprint for regenerating a healthy, joyful, vital you! This program is the culmination of 23 + years of medical expertise and 40 years’ experience as a Crohn’s disease patient. It is my passion project to help as many IBD patients as I can! I am on a mission to change the medical approach to Crohn’s and UC leading to fewer surgeries, stopping the path to health decline and disability by finding and fixing the root cause. We will Transcend IBD together living healthy vibrant lives.”
The process begins with uncovering your health history and detailing your timeline. Next, Christina works with patients to order specialized cutting-edge functional lab studies to help pinpoint where the most critical areas of intervention are needed. The third step is the Excel phase where you learn how to maintain these changes and continue to progress over time.
Christina is hosting an online Zoom webinarSeptember 1 at 7pm EST. By attending this webinar, you will learn three secrets for managing IBD and have an opportunity to ask questions. Tickets are $9.95 and limited in number. Get your ticket today!
Ready to Make a Change?
Set up an initial consultation here for men and here for women. Use coupon code Natalie20 for 20% off any time in 2021. HSA/FSA are applicable. This consultation is the first step to discovery. During this consultation you will discuss your body’s problematic areas as well as the areas where you are succeeding based on extensive intake paperwork and a 60-minute consultation. Potential interventions will be discussed, labs will be ordered, and a personalized care plan will be created.
Christina says, “I provide options for anyone who meets with me. However, I do not invite everyone into my signature 3-step Transcend program. It is important that we both feel we are a fit to work together to make this program successful. You must be ready to make the necessary changes and be open to new information. You must focus on progress and commit to never letting your self-doubt stop you from having what you want. There is hope! You can change your health and life for the better.”
Six years ago, I was shaking like a leaf getting rolled into the operating room for bowel resection surgery. Six years ago, I felt overwhelmed by the thought of my body getting cut into, by the realization of my body having scars, by the fear of the unknown, and feeling as though I had failed myself and those close to me. The first decade I had Crohn’s disease, I always thought of surgery as the last resort. With each flare up and hospitalization, my biggest worry was needing a surgery of some sort. I constantly wondered about becoming one of the 50% of people with Crohn’s who ultimately end up with surgery. August 1, 2015, I became part of that statistic, when I had 18 inches of my small intestine, appendix, ileocecal valve, and Meckel’s Diverticulum removed. Surgery went from being an option to a necessity.
Looking back now—I want you to know if you need surgery, it’s not a reflection of failure on your part as a patient. While it may feel like the world is crashing down around you, you’ll see the pain, the fear, the recovery—it’s all fleeting. Time waits for no one. Before you know it, you’ll be like me. I blinked and it’s been six years. The scars and memories remain, but as more and more time passes, they become less of a big deal.
I’ve had several fellow IBD’ers reach out with questions recently about bowel resection surgery—everything from bleeding to bloating, asking me about my experience, and surprisingly it’s hard for me to remember those details!
I credit bowel resection surgery for removing a decade of disease from my body (not curing me) but giving me a fresh start and ultimately putting me into surgical remission. Remission that has been maintained for six years now. Prior to surgery, the first ten years I had Crohn’s, I was never in remission. Since surgery I was able to get to a place in my disease journey where family planning and pregnancy were possible without any complications or waiting. I’ve been able to bring three babies into the world and haven’t needed to be hospitalized for my Crohn’s since becoming a mom. I went for a walk with my husband and three kids yesterday (August 1, 2021) and found myself reflecting and feeling a great deal of gratitude as I thought about the stark contrast of where I was six years ago in comparison to now.
August 1, 2021. 6 years post-surgery.
Tips for Surgery: Before and After
Take a before photo. The day before my surgery, I took a photo of myself standing in front of the bathroom mirror in my bra and underwear so that I could remember what my body looked like before it had scars. I took the picture for myself and have never shared it. When I look at the picture now, I see a girl with sadness in her eyes and a longing for days without pain. I see a girl who is petrified of what could be and praying for relief. I see a thin, untarnished body on the outside, but one that is very sick on the inside. I highly recommend you take a photo of yourself prior to surgery so you can capture that moment. One day you’ll look back on that time and be able to see how far you’ve come. You won’t think of your scars in a negative way, but rather a reminder of all you’ve overcome. I don’t even notice my scars when I look in the mirror now.
Communicate with your surgeon. If your surgery isn’t an emergency and you have some time to talk with your surgeon, make sure you do. Talk with your care team about what the surgery will entail—how many inches of intestine will be removed, if an ostomy is a possibility, where they will do incisions, etc. This will help you mentally prepare for what’s to come. My surgeon came into my hospital room prior to my bowel resection and asked me where I would want the incisions. We knew I would have the laparoscopic incisions, but we discussed a horizontal vs. vertical incision as well. I said I wanted the incision to be as low as possible—he told me he would do a “c-section incision” …which worked out wonderfully for me. I know of many people who have had a couple inches of intestine removed and have a large vertical scar (I had 18 inches taken) and that type of incision was not necessary.
Once you’ve had surgery push yourself to get up and get moving. Don’t overdo it, but every step, every movement will help you heal. Before you know it, you’ll be able to bend down and tie your shoes, walk a little further, and stand a little taller. After my surgery it was a struggle to walk around my family room, then before I knew it, I was walking outside…each day making it to one house further around the block. Before I knew it, I was able to take long walks. When you’re laughing, coughing, sneezing, or driving, have a small pillow nearby to hold against your incision, this will alleviate a lot of the pain. The first two weeks is the hardest. Once you hit the 2-week mark, you’ll feel a ton better. You’ll be able to drive and get around with minimal pain. Just hold on to that thought those initial days when it’s emotionally and physically pretty brutal. I remember crying my first night at home because I was so overwhelmed by the pain and my inability to get out of my own bed. At the time a family member was battling ALS. Her fight and knowing that her health was deteriorating daily, while mine was improving with each hour that passed, gave me perspective and brought me back to earth.
Trust in your care team. Once you have surgery, then the priority is to determine how managing your IBD will look moving forward. I, like many, had this false sense of security after surgery that I felt so great, I wouldn’t need to go back on my biologic…or any medicine for that matter. After a lot of tears and discussion, I followed my GI’s recommendation to re-start Humira and add a bunch of vitamins and supplements to the mix (Vitamin D, Calcium, Folic Acid, and a prescription prenatal). I give my GI a lot of credit for being proactive and having a “come to Jesus” talk with me, if you will. She warned me my Crohn’s disease is aggressive and by going med-free, my risk of being back on the operating table 3-5 years down the road would go up exponentially. Six years later, I’m so glad I listened.
Be patient with your healing. I’ve had three C-sections and bowel resection surgery, and the recovery is very different. I try to explain this to women who come to me with questions wondering about the two. With a C-section you have incisional pain/burning, but with an IBD-related surgery you also have to heal from the inside, too. Organs are cut, removed, and reattached. Your digestion needs to recalibrate. It’s a lot more intense of a recovery than a C-section (which I’m going through right now). Be patient with your body. Ease back into normal activities. After my bowel resection surgery, it took me nearly 8 weeks to return to work full-time at my desk job. Prior to returning to the office, I worked half days for two weeks from home because it took time to heal enough to sit upright in a chair. As your digestion re-works itself, it’s not unusual to have an accident or not be able to ‘hold it’ the same as you could prior. For me, this was temporary. But in those initial weeks and months, it’s a good idea to have a change of clothes in your car or packed with you and to be mindful of where the nearest bathroom is. I had one accident during my recovery—luckily, I was home alone (working a half day), it was mortifying, and I was by myself. Don’t try and rush back to normalcy, give yourself time to heal mentally, physically, and emotionally.
3 weeks post-op, laughing through the pain during engagement photos.
If you find out you need surgery—it’s understandable to be upset. But also give yourself a chance to think of all that could be possible. Try and focus on the promise of how surgery could help you get into remission or at least help you in having more “feel good” days. It’s normal to grieve and to be tearful and fearful, but I hope you find comfort in knowing once you wake up from surgery, you will be on the road to a recovery that paves the way for feeling empowered against your illness. And from that point forward you won’t be as scared of future surgeries because you’ll have a better idea of what to expect and a better understanding of how it feels to be well after being in pain for so long.
After a lot of thought and consideration, I decided to hold off on getting my COVID-19 vaccines until after I delivered my son. Before we dig deeper into this topic, I want to clarify that this was solely my choice, everyone needs to do what they are most comfortable with. Since the pandemic began, unprecedented pressure and stress has been placed on pregnant and lactating women to make one decision or another. For me, as a stay-at-home mom, who continued to keep a low profile while pregnant, I felt more at ease waiting to get my vaccines until after my son was out of my body. My care team made up of a maternal fetal medicine doctor, OB, and gastroenterologist all supported my choice to wait.
My main reasoning was limiting the variables of exposure. All my kids were exposed to Humira while in utero. While there are long term studies that show the safety and efficacy of biologics in pregnancy, you never know. If down the road my son had any health complications or issues, I didn’t want to have to grapple with whether my biologic or a vaccine contributed or were to blame. As an IBD mom, we deal with enough guilt as it is.
So, I chose to wait. Anxiously. Patiently. Luckily, I delivered my third child, Connor Christopher, July 14th, and did not encounter any COVID-19 scares while pregnant. Once I was home from the hospital following my C-section, I talked with my gastroenterologist and OB about getting my first COVID vaccine and scheduled an appointment at Walgreens ASAP.
Getting the first jab
Wednesday, July 21, I finally got my first dose! A little late to the party, but I’m currently exclusively breastfeeding (and pumping), and I’m hopeful that once I’m fully vaccinated (two weeks after my second dose in August), my son will receive antibodies from the vaccine that way. It felt a bit surreal to finally be at a point where I felt comfortable with my personal choice to get the vaccine.
According to the CDC, since January 2020, there have been 34 million cases and 607,000 deaths. As of July 21st, 161.9 million people are fully vaccinated—that’s 48.8% of the total population, or 57.1% of the population older than age 12. Virus variants threaten new outbreaks among the unvaccinated.
Much like making decisions to manage IBD, it’s imperative our community looks at the benefits vs. the risks of getting the vaccine.
Words from leading medical experts in the IBD community
This past week Dr. David Rubin, MD, Professor of Medicine, University of Chicago presented, “Updates on COVID-19 for Patients with Inflammatory Bowel Disease”.
“Everyone needs to be vaccinated, this includes pregnant women and new moms. The Delta Variant is VERY contagious. The data in IBD is reassuring when it comes to immune responsiveness compared to the general population, especially with the two dose mRNA vaccines. Antibodies against many things are transmitted in colostrum, and that may be the anti-SARS-CoV-2 spike antibodies too, which may provide protection to the baby. It’s definitely NOT dangerous to breastfeed after vaccination.”
Speaking of the Delta Variant, according to Dr. Rubin’s presentation as well as guidance from the CDC, “Delta was 1% of COVID-19 cases during the week of April 10th. By the week of July 3rd, Delta is estimated to account for 57% of new COVID-19 cases. Within a matter of 12 weeks of being introduced to the US population, it became the dominant variant here.
Dr. Uma Mahadevan, MD, University of California San Francisco agrees, saying given the ongoing crisis with COVID-19, all eligible people should get vaccinated.
“Breastfeeding mothers can get vaccinated per CDC guidelines and there is data that the antibody from the vaccine crosses to the infant via breastmilk, possibly providing them with protection as well! For many infants of moms with IBD, they have detectable levels of biologic agents in their blood for the first 6 months of life. Having antibody against SARS-Co-V-2 may provide them some protection against getting ill if exposed to the virus.”
Dr. Meenakshi Bewtra, MD, MPH, PhD, Penn Medicine, has IBD herself and has been a vocal advocate for our patient community since the start of the pandemic. She implores everyone to get the vaccine, immediately.
“Don’t wait. In fact, I, every doctor I know, American College of Gastroenterology, and Maternal Fetal Medicine recommend getting the COVID-19 vaccine while you are pregnant. Why? Because we’ve seen what happens to pregnant women who get COVID. There are women who got the vaccine in trials; there were women who got vaccinated while pregnant (>10,000 at this point)—we have a lot of data. The evidence is crystal clear. The same holds for getting it while breastfeeding. COVID is real, it’s out there; you can get sick and die; you can transit it to your infant or others in your house. There is absolutely no reason why anyone should not be getting vaccinated unless you know you have an allergy to something in the vaccines themselves. Your protective antibodies can pass to the infant.”
COVID-19 in the IBD Community and Vaccine Response
Thanks to the SECURE-IBD database, we have more guidance about how those of us with Crohn’s and ulcerative colitis have responded and continue to respond to not only COVID, but the vaccine. People with IBD do not have an increased risk of getting it. Aminosalicylates, biologics, and immunomodulators show no increased risk of severe COVID- 19. Steroids are associated with worse outcomes. And biologic therapy is associated with decreased risk of severe COVID-19 outcomes.
One of the main concerns many of us in the chronic illness community on immunosuppressive drugs have wondered about is the efficacy of the vaccines in our body. Good news—a recent study of 246 patients with IBD who received both doses of the vaccine showed similar adverse events as in the general population. Sore arm, headache, and fatigue are the most common adverse effects of the vaccine. All I had after my first Pfizer vaccine was a sore arm. More importantly, the study showed no increase in IBD flares.
The Prevent-COVID study shows even more promising data with more than 1,700 participants with IBD. Click here to see results of the study—everything from rates of vaccine side effects to lab titers three months out.
As of now, there’s no recommendation or approval regarding a booster vaccine. Pfizer announced that their clinical trial data showed that a third shot may increase antibody levels, but nothing has been published yet. Without more research, it’s unclear if an increase in antibody levels will provide greater protection from the virus than two doses.
Get Involved in COVID-19 Vaccine studies
University of Chicago Inflammatory Bowel Disease Center COVID-19 Vaccine in IBD Study
This study is analyzing the durability, safety, and efficacy of COVID-19 vaccines in patients with IBD, If you are interested in participating in the study (whether you have already been vaccinated or not) please email: covidvaccine.ibd@lists.uchicago.edu.
Prevent COVID Research Study
If you are 12 to 17 and have received your first COVID-19 vaccine in the last 90 days, you may be able to take part in PREVENT COVID, a research study to learn about the vaccine experiences of people with IBD. Click here to learn more.
CORALE-Vaccine IBD
The purpose of this research being conducted at Cedars-Sinai is to understand the effects of vaccination against COVID-19 in people with IBD. To achieve this goal, a national and local group of adults with IBD who are eligible to receive any available vaccine against COVID-19 are being recruited. Within this group we will evaluate the antibody levels of the body’s response to the vaccine. Questions about the study? Contact the CORALE-V IBD Research Team at Cedars-Sinai at ibdresearch@cshs.org or call 310-423-5643.
Washington University in St. Louis: COVID-19 Vaccine Response in Patients with Autoimmune Disease
School of Medicine researchers are leading a clinical trial to evaluate the safety and effectiveness of COVID-19 vaccines in people taking immunosuppressive drugs. Such drugs are prescribed to treat autoimmune diseases, including arthritis, Crohn’s disease, and psoriasis. Researchers will enroll up to 500 adults ages 18 and older in the St. Louis region. They are recruiting health-care workers at the School of Medicine and patients seen in Washington University outpatient clinics. Eligible patients who have preregistered for the COVID-19 vaccine will be contacted to assess their interest in being recruited into the study. For information about participating in the trial, email covaripad@wustl.edu, or contact either Alia El-Qunni at 314-249-1151 or Lily McMorrow at 314-280-3894.
V-Safe
Use your smartphone to tell the CDC about any side effects after getting the COVID-19 vaccine. The tool uses text messaging and web surveys to provide personalized health check-ins after you receive a COVID-19 vaccine. Depending on your responses, someone from the CDC may call to check on you. Participation is voluntary and you can opt out at any time. Sign up at: www.vsafe.cdc.gov.
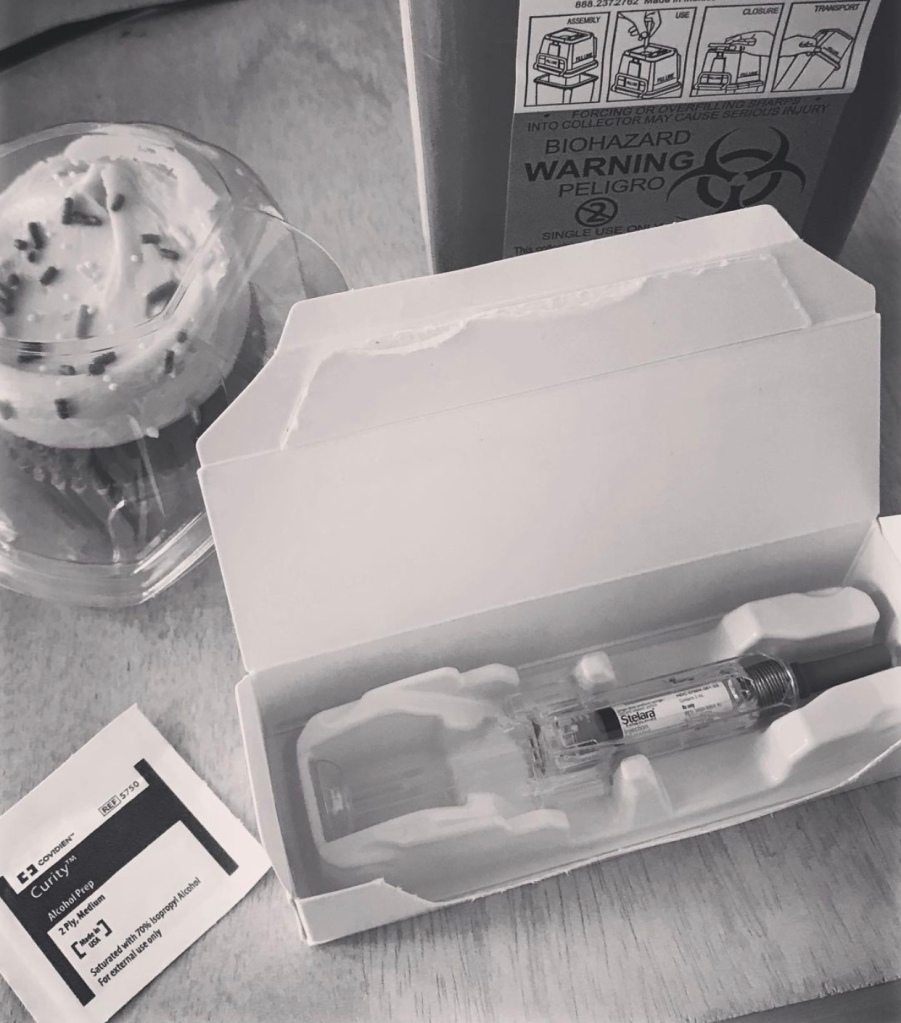
Starting on a biologic and finding one that helps manage your IBD can be challenging physically, mentally, and emotionally. Nearly 13 years ago (July 14, 2008) I sat in my GI’s office like a fish out of water petrified of injecting myself with four Humira shots. I remember how daunting and overwhelming taking the plunge into life on a biologic was and know I would have given anything to hear firsthand experiences from fellow IBD patients. This inspired me to launch a special series on Lights, Camera, Crohn’s hearing firsthand accounts from people like you and me, living life on biologics. So far, I’ve covered Remicade and Entyvio.
This week—we tackle Stelara (ustekinumab). Stelara is categorized as a human interleukin-12 and -23 antagonist. Patients receive a one-hour loading dose infusion and follow up with an injection every 8 weeks. As you’ll read, some patients receive their injection every 6 weeks, others every 4. Stelara is indicated for Crohn’s disease, ulcerative colitis, severe plaque psoriasis, and active psoriatic arthritis. As a biologic, it joined the IBD game in September 2016 for Crohn’s disease and October 2019 for Ulcerative Colitis.
“I’ve been on Stelara for almost 5 years. I started taking it right when the FDA approved it for Crohn’s disease. I have only good things to say, because it’s keeping me in remission. It’s easy to administer and doesn’t burn like Humira used to (prior to the Citrate-free formula). I stayed on Stelara throughout both my pregnancies. My GI had me skip my last dose both times I was pregnant, and I re-started my injections once the babies were here,” said Ashley Miller.
Patient Advocate and Co-Founder of IBD Desis, Tina Aswani Omprakash, joined a clinical trial for Stelara to treat her Crohn’s disease. She says it took months to work, but it was the first time in a decade of having IBD and enduring more than 20 surgeries that she was able to achieve remission.
“At that juncture, I thought my life would always be in shambles and that I would never be able to rise from the ashes of this disease. But here I am today pursuing advocacy work and going to graduate school part-time. Modern medicine is nothing short of a miracle and I can’t help but count my blessings every single day to have been given another chance at life again. Thank you, Stelara, for making me whole again.”
Click here to learn more about Tina’s clinical trial experience with Stelara.
Making the Switch
Lauren Gregory is an IBD mom and a pediatric hospitalist. Even as a physician herself, she was nervous about switching biologics. Prior to starting on Stelara, she took Humira injections for 8 years. Unfortunately, the Humira induced numerous medication related side effects that really affected her quality of life.
“I was worried that Stelara wouldn’t work and that I would feel even worse. Switching medications ended up being the best decision. I have been in remission since starting Stelara four years ago and feel better than I have since diagnosis. Stelara also allowed me to have a healthy pregnancy and baby!”
Jenna Ferrara recently made the switch from Remicade to Stelara. Last week, she did her first self-injection and says Janssen was beyond helpful throughout the process. Click here to learn about the Nurse Navigator Program. The program provides a registered nurse (in-person) to help support you as you learn to give yourself injections.
“Between the nurse navigator and sending a training nurse to my house, they made it so easy. I was nervous before my first shot, but thanks to the nurse, it was great!! I’m still waiting to see results, but things have been slowly getting better after only two doses.”
“I tried Stelara after Humira failed me and it never helped or worked from the start, but regardless it was sold to me as the best option. My attending at the time even said it was his top choice for patients and would have put me on it from the start if he had been my GI who diagnosed me. I was super disappointed it failed, but now I’m on Remicade and feeling better than ever,” said Julie Mueller.
Erin O’Keefe was diagnosed with ulcerative colitis in 2017 and initially was able to control her IBD with mesalamine. She started Humira in January 2020 and had what was believed to be a drug-related reaction that landed her in the hospital for 2 weeks and the ICU for 3 days.
“After I was discharged, I was started on Stelara, and I couldn’t be happier with the results. My symptoms are minimal, and I have even been able to re-introduce foods that I tended to stay away from. The injection is easy and I’m so happy not to be taking pills daily. Fingers crossed I can stay on Stelara for many years to come!”
“My 15-year-old son started Stelara last fall after a Humira fail (he was on Humira for 4 months when he developed psoriasis). It seems to be working as his markers and symptoms have slowly subsided. He has also put on some much-needed weight. Therefore, his doctors have recommended that he step up to the adult dose. Their aim to fully eradicate the inflammation—his calprotectin is still elevated. While Stelara is approved for pediatric use for psoriasis, it’s not yet approved for Crohn’s…so there have not been any studies.”-Michelle Boas
Hayley Weiss had to switch to Stelara after Humira caused her to get Psoriasis on the bottom on her feet and the palms of her hands. She just celebrated two years of being on Stelara. The 8-week dosing wasn’t doing enough to keep her IBD under control, so she was switched to every 6 weeks.
“I was doing well for awhile on the 6-week injections, but then at about 5 weeks I was getting symptomatic, so my doctor decided to actually give me another loading dose and I kept on with the 6 weeks for a little while until September of last year. At that time, my doctor approved me for every 4 weeks and that is what I have been doing.”
“I switched to Stelara from Humira in February 2019. I feel the best I’ve ever felt in a long time. A lot less breakthrough flares, energy levels are back, and inflammation numbers are lower than when I was on Humira. I haven’t had any negative reactions and have zero complaints!”- Erin Forman Carmiel
Martin R. was on Humira for about a decade. During that time, he calls the drug a “game changer” for bringing stability to his life when it came to managing his Crohn’s disease and reducing the need for steroids and antibiotics.
“After the regular blood tests for the azathioprine which I’ve been taking since 1992, I showed I had developed antibodies to Humira. I chose Stelara two years ago and it seems to have taken over where Humira left off. I don’t have additional side effects and a longer interval between injections, so that’s a bonus.”
After two years of remission, special education teacher, Jasmine Edwards, started flaring, despite being on Entyvio. Previously, Humira and Remicade gave her drug-induced lupus. Now, after just receiving her first dose of Stelara, she’s hoping the fourth biologic is a charm.
“I’m looking forward to the freedom of not having to get monthly infusions at the doctor’s office. I really hope Stelara puts me in LASTING remission so I can get back to a better quality of life. I’ve been feeling well since my loading dose infusion, but I’m also on prednisone. The only side effect I had after the infusion was feeling tired. In four weeks, I will administer my first at-home injection. I’m nervous about giving myself a shot because with Humira I used the pen, but I’m READY for remission, so I’ll try anything!”
Amanda Hart has had two doses of Stelara so far. Unfortunately, her MRI still shows new inflammation.
“I’ve been increased to once every 4 weeks. If there is no improvement in three months with the higher dosage, I’ll be looking for a new approach. I was originally on Humira, but switched due to my symptoms. Sadly, the symptoms on Stelara have been worse and my diet is more restricted then when Humira was not considered effective anymore.”
Alli Butler was previously on Humira, she finds Stelara makes her feel similarly.
“I’m currently taking Stelara, it has worked great for me and got me through my third pregnancy. Hoping it continues to work well through my postpartum experience.”
Tips for Self-Injecting Stelara
Lori Plung has battled Crohn’s disease for more than 40 years. Since that time, she’s been on four different biologics. She credits Stelara as her easiest patient experience.
“Remicade and Entyvio are obviously infusions—they took time and planning to organize appointments at infusion centers and waiting there while being infused. I was on Humira which was nice to have the freedom to inject at home, but I didn’t like the pen model of injecting. I haven’t had any problems with Stelara. I started my loading dose infusion in April 2019 and give myself the injection every 8 weeks. I love that it’s a pre-filled syringe and that I can do the injection in my home.”
Claire Paschall recommends taking the injection out of the fridge so it can warmup to minimize the burn.
“The automatic needle pullback jolts if you take your thumb off once done and it can hurt (so slowly take your thumb off). I feel like it took longer to build up in my system than Remicade and Humira, however I haven’t had any side effects to report. I have been flaring with my rectal disease, but my small intestine disease is in remission.”
Plea for a Pen-Style Injection
Courtney Meyer started Stelara in March and immediately saw improvement with her symptoms. Previously, she had tried Remicade, Humira, and Entyvio.
“It’s so nice not to have to get an IV after the loading dose. The only downside is that it doesn’t come in a pen option like Humira, and I have difficulty with needles, so I get it administered by a nurse in my GI office every 8 weeks. They inject it in the back of my arm, so I don’t have to deal with the usual stomach or thigh injection sites. It’s the most convenient and easiest treatment of Crohn’s that I’ve been on in 15 years! I was able to stop other medications and I’m just on Stelara. No side effects so far.”
Julianne Bossert was diagnosed with Crohn’s more than 25 years ago. She was on Humira for almost 5 years and says it worked great, until it didn’t. She started Stelara in February and is gearing up for her fourth dose next week.
“I feel like I’m on the cusp of getting better, but not quite there yet. I’m about two weeks out of being off steroids that I have been on for a year. So, my crutch is now gone, and we will really begin to see if Stelara is working. My two biggest complaints are the shot itself. It’s not a pen like Humira, which was way easier to administer. The syringe is way scarier, and they show you how to inject it once and then off you go! Awful anxiety. The other complaint is how different the relief is. When I was due for my Humira about two to three days leading up to I was in bad shape…very sick. But I’d get the injection and feel better within an hour. Leading up to Stelara, I feel awful, get the shot, and still feel awful for days. The turnaround time isn’t as quick for me.”
Emily Beaman is an IBD mom of two who initially started on Humira and was switched to Stelara two years ago.
“I will say the only thing I don’t like is the injection. I prefer the Humira pen-style. I have yet to be able to give myself the injection which means I have to rely on my husband to do it. I find it hurts more than the original Humira did for me (the Citrate-free version wasn’t available while I was on it) I really wish they would come out with a pen-style injection. I worry about if I ever had to give it to myself…that I wouldn’t be able to.”
Stelara Tips for the IBDMom (or Dad!)
Brooke Abbott is a patient advocate, single mom, and co-founder of IBD Moms. She shares helpful tips for administering the injection whether at home or at your doctor’s office.
If injecting at home:
Keep an injecting kit. Have a small kit prepped with alcohol wipes, band-aids, and cotton balls or pads.
Prep the night before. Hydrate as much as possible and make sure you have your kit ready and prepped.
Injection day. Make it a relaxing event. Have your injection before a family movie night so you can get some cuddles in after injecting yourself or being injected.
Normalize your treatment. “Practice” with your little ones with a play doctor’s kit. I used to always play doctor and do fake injections, to normalize living like a patient for my little one.
If injecting at the doctor’s office:
Book Appointments to include self-care time. I try to book appointments for my injections early in the day so I can have time after to do something for me. Whether it’s going to grab a coffee and read, meet with a friend, or have a nice lunch.
Take the LO (little one) with you. I am all about including my LO in my patient life. I want him to be able to ask questions and voice concerns. So sometimes when he is out of school, I will take him with me. It’s good for him to hear the progression of the treatment and to see mommy being brave and getting an injection.
Multitask. Try and take all your blood tests and everything at one time. That way you don’t have to make any unnecessary trips to the doctor’s office.
Let’s Talk Side Effects
Overall, the consensus from patients was little to no side effects—which is a HUGE win. Of course, each person’s experience with IBD and with biologics is unique.
Stelara is the first biologic for Shanna Quinn. She started on it in July 2020 following bowel resection surgery. She found starting off with an infusion was a bit “scary” and much preferred giving herself a shot which she says is “so easy.” In her opinion, making the decision to start a biologic was the biggest hurdle, rather than choosing one.
“It doesn’t hurt, although you do have to go slow or else the medication will sting a bit. One drawback is that I get tired afterwards. I’ve learned to take the day and relax and sleep, if needed. I do my shots on the weekend to allow for that. My GI and I discussed a few options before choosing Stelara. I took a test that asked questions about priorities, risks, concerns, etc. The results gave me details about how each biologic stacked up against your concerns and priorities. Take the “IBD&Me” test for yourself here. Knowing you may need to be on a medication for life or knowing it may fail you is hard to wrap your brain around. I hope IBD will get way more targeted and specific regarding treatment options.”
A patient who wishes to remain anonymous has found the side effects of Stelara to be more draining than Remicade, but not as bad as Entyvio. He says the first three days after the injection he needs considerable rest.
“I have also noticed systemic night sweats as far out as five weeks after the injection. For me, this is unique to Stelara in terms of my individual experience. The silver lining is that Stelara seems to have generated more stability and normalcy from an IBD symptom perspective. My level of disease is quite severe and to date, Stelara has had the best outcome. One drawback however is that insurance companies are less willing to grant physicians discretion to prescribe more frequent injections. My GI has said he faces greater pushback on Stelara specifically.”
Paula Hepburn has been on Stelara for 1.5 years, it’s the only biologic she’s been on thus far. She feels like it’s working well to control her Crohn’s disease.
“The first infusion gave me crazy fatigue for four days and I often get tired after each injection. Sometimes it only lasts a few hours, sometimes into the next day. I feel fortunate to have access to this medication because it helps control my IBD so well.”
Madison Morgan has been on Stelara for 2 years. She started it following an ileocecal resection that involved the removal of 8 inches of intestine. Madison finds the injections to be easy. She does experience some side effects though.
“I get a headache immediately after the injection that lasts about 15 minutes, the worst side effect I’ve had is yeast infections and UTI’s, I’ve never had them until Stelara and have had 6-7 yeast infections in the last two years and 2 UTI’s. A couple weeks before my Stelara injection (once every 8 weeks, 95 mg), my arthritis from my Crohn’s gets pretty bad, but seems to get better after my injection.”
“Stelara has been amazing! Aside from the infusion loading dose, it’s quick and easy and fairly pain free. I have minimal side effects other than sometimes feeling sleepy after my injection, but other times I have crazy energy. Overall, this is the only biologic that has worked for me for more than a couple of years.”-Bethany Lowe
“I’ve found the injections to be almost painless and I’m a huge wimp with shots. It took a few tries to find the right timing and frequency for my shots, but I do them every 4 weeks and approximately 1-3 days before each shot, I start to get some IBD symptoms…so I know it’s working!”-Danielle Fries
Olivia L. was diagnosed with ulcerative colitis 20 years ago. She’s an IBD mom of 3. Lucky for her, she was able to get through the first 18 years of living with IBD without being on a biologic. Unfortunately, she experienced a postpartum flare two years ago that is still wreaking havoc on her life.
“I started Stelara about a year ago. It’s super easy to use. The only side effects I’ve felt are being tired for a day or two after the injection. I feel quite lucky that I was able to start Stelara, rather than other options. It’s easy to take because you do it at home, and the side effects are non-existent for me. Unfortunately, it hasn’t been as effective as we had hoped. I do my injection every 4 weeks instead of 8. From a tolerance and side effect standpoint, Stelara has been a good medication for me, but it still frightens me to be on a biologic. I know everybody manages this dance in their own way.”
Krista Cherrix has been on Stelara for one year. She prefers the syringe injection over the Humira pen but has unfortunately dealt with weight issues since starting it.
“I have gained a TON of weight on it and can’t seem to get it to budge even with diet and exercise. I also have not been able to get pregnant so far, which isn’t necessarily the drug, but I got pregnant with my first (pre-diagnosis) without trying.”
“I took Stelara monthly for nearly 2 years and had no side effects. My diarrhea was still frequent and after having an MRI and a colonoscopy, the results showed that I still have significant inflammation in my small bowel. I am going to be starting Humira in hopes of healing the inflammation.”-Marsha Gagnon
Dealing with Insurance and Cost
Shawn Bethea is an IBD patient advocate and author of “My Tummy Really Hurts”. Overall, she considers her experience on Stelara to be good, but wants others to know there have been some hurdles to cross along the way.
“At first, I truly didn’t think the medication would work for me. I was placed on the standard dosing and scheduled to receive my injection every 8 weeks. During the initial weeks I’d feel great! I had more energy and didn’t feel the sharp pains as I usually did (in my stomach area). I wasn’t going to the bathroom as often and even my Eczema seemed to be clearing up.”
However, after those first initial weeks, she noticed a decline. Her energy decreased, her Eczema became bothersome, and her joints would ache. She communicated her concerns with her GI who prescribed injections every four weeks.
“With any high dollar medication comes unique challenges to those of us who don’t live on a Beyonce budget. Between my insurance, the patient assistance program, and copay, the drug was running about $20,000 monthly. When you have insurance and nothing changes like a lapse of coverage or a job change, this is something you can possibly juggle (depending on the level of coverage/assistance, but mine was pretty good). The problem came in when I changed jobs, lost insurance, and had to wait for new insurance to take effect – which was delayed, of course.”
Shawn stopped taking Stelara, due to lack of insurance coverage, everything was impacted. She began to experience joint pain, became extremely tired, and was using the bathroom more—even experiencing extreme constipation.
“Overall, I love Stelara, but I hate the way our healthcare system operates. No drug should run half of someone’s salary monthly. But I subscribe to the system because I simply want to live and be healthy like everyone else.”
Jacquie Persson has been on Stelara since 2019. She started off with the recommended dosage of injecting every 8 weeks, but after 6 months, she was moved to every 4 weeks.
“Since starting Stelara, my Crohn’s disease has been well-managed I haven’t had to take prednisone since 2018, after depending on steroids on and off from 2016-2018. Financially, being on this drug is a little anxiety inducing. The list price is over $20,000 per injection and I’m constantly on edge wondering when or if my insurance will decide to stop covering it. My copay is over $200. I currently have copay assist which brings my out of pocket down to $5, but what if that program were to go away?”
“I started Stelara in December 2016 after Remicade failed me. I had success with small flares here and there. In March of 2021 I had a big flare—my first in about 5 years and was out of work for 2 months. My GI wanted to increase my Stelara from every 6 weeks to every 4, but my insurance repeatedly denied it and just finally approved it about a month ago, thankfully in time for me to be feeling better.” – Mary Fordham
“The dosing is wild! I started at 8 weeks and now I’m moving to six…and I know some people on every 4 weeks. Insurance has a really hard time approving more frequent injections.”-Catalina Berenblum
Click here to learn more about Janssen’s CarePath Savings Program for Stelara.
Success Stories on Stelara
“Stelara has been a Godsend for me. I had an ileocolic resection nearly five years ago and have maintained remission with Stelara and azathioprine since my surgery. The side effects have been minimal. For me, it’s been one of the easier injections I’ve used. It doesn’t sting or burn like Humira did prior to the release of the Citrate-free version. I take Stelara every four weeks instead of the typical eight.”-Jennifer Ryan Carmichael
Amanda Pennwell was diagnosed with Crohn’s when she was 8 years old. She’s now a mom of 3 and due with her fourth baby this October. She’s been on almost every drug approved for Crohn’s disease. She says she can honestly say Stelara has changed the severity of her Crohn’s the most significantly, with the least amount of side effects and the biggest improvement to her day-to-day life. She started Stelara in April 2019 after flaring with her twins. She was able to get pregnant, have a smooth postpartum experience and breastfeed her third baby while on it.
“Stelara helped me get my life back. This is something I never dreamed my broken body would ever be capable of doing. I’m so thankful that Stelara is continuing to work for me. I have been healthier than ever. I work out all the time and my body feels strong. I haven’t experienced abdominal pain more than a dozen times in the past two years. It’s truly remarkable. Stelara has enabled my husband and I to chase our dreams while raising our babies! I work part-time while staying home with the kids. We our building our dream home and I know I couldn’t keep up with it all if I felt the way I did two years ago. I’m thankful for research and better IBD drugs like Stelara.”
Patient Advocate, Founder & President of Patient Authentic, Lilly Stairs, credits Stelara for saving her life.
“I have been in medically controlled remission for nearly 8 years from all three of my autoimmune diseases – Crohn’s Disease, Psoriatic Arthritis, & Psoriasis. I went from bleeding ulcers in my small intestine and total body arthritis that left me paralyzed in pain to living symptom free and thriving as a solopreneur. I am so grateful for this brilliant medical innovation and only hope that someday all autoimmune patients can have this type of experience on a medication.”
Check out previous biologics that have been featured on Lights, Camera, Crohn’s. These articles have NO affiliation or guidance from pharma. All content was created thanks to countless IBD patients sharing their personal patient journeys with the hope of helping others.
Imagine having a dad who’s a gastroenterologist and a husband who is a GI fellow… and having Crohn’s disease. For 32-year-old, Lauren Gregory, that’s her reality. She was diagnosed with Crohn’s in 2008. Lauren is also a doctor herself and an IBD mom! When she’s not taking care of pediatric patients in the hospital, she’s enjoying time at home with her husband, Martin, and 6-month-old son, Connor. In light of Father’s Day, this week on Lights, Camera, Crohn’s, we share about how the most important men in Lauren’s life have helped her cope and overcome challenges IBD has presented along the way.
Through the eyes of Lauren’s dad
Late one night during Lauren’s college sophomore Christmas vacation from college, her mom called her dad with words he will never forget. She said, “Lauren is having terrible abdominal pain and is on the floor.” After a quick exam and seeing how tender and distended her abdomen were, he knew it was time to head to the closest emergency room. A CT scan showed massive gastric dilation and small bowel thickening. The surgeon was called, and he agreed it was likely Crohn’s.
Lauren was discharged home on a liquid diet with outpatient GI follow up after New Year’s. Unfortunately, her concerning symptoms persisted and her dad called a friend who was a gastroenterologist. He directly admitted her.
“When Lauren was admitted to Barnes Jewish Hospital in St. Louis while in college at Wash U, her then boyfriend (now husband) sat by her bedside for days as she underwent scopes and a small bowel series. We knew he was a keeper then. As parents we always worry about our children. As a gastroenterologist, we may worry more when our children have GI issues. We are fortunate to have connections in GI which allowed Lauren to have prompt evaluation and ultimately a great outcome,” said Dr. Bruce Waldholtz.
Navigating love and IBD
Lauren met Martin in college. At the time, he knew he wanted to be a doctor, but he did not know what he wanted to specialize in. During internal medicine residency, Martin was torn between cardiology and gastroenterology. He ended up choosing GI and is about to start a one-year fellowship to get extra training in IBD and nutrition. (Small World Fun Fact: He is part of the same GI practice I go to in St. Louis!)
Martin says Lauren inspired him to choose gastroenterology and specifically focus on inflammatory bowel disease.
“Watching her go through what she did at such an important time in her life was inspiring. I was so grateful to her doctors taking such good care of her. I wanted to be like them. I wanted to help people like her succeed in living a rich, enjoyable, and rewarding life. “
Lauren feels incredibly lucky to have found someone as supportive as her husband. A month after they started dating, she was hospitalized with a partial small bowel obstruction. The fact he didn’t leave her side throughout that vulnerable and scary experience meant a lot to her.
When Lauren was hospitalized for one week during her fourth year of medical school, Martin was going through his second year of internal medicine residency. They were married, but in a long-distance relationship at the time.
“During residency you can’t just take days off, and it is challenging to find coverage. Because of this I did not expect him to be able to visit, but he somehow did. This flare occurred as I was transitioning from Humira to Stelara. I have been extremely fortunate to have stayed in remission since then (2017).
How personal life impacts professional life
“Without question Lauren makes me a better doctor, especially with taking care of IBD patients. I can understand the anxiety behind the questions they have about medications and what to expect because we went through the same thing as a family,” said Martin.
Lauren says her IBD has given her a unique outlook in how she cares for patients as well.
“My experiences with Crohn’s have made me more empathetic towards my patients, and now that I am a mom, I have much for empathy for my patients’ parents. Spending extra time with patients is not always easy given that I work mostly in the emergency room, but I make a point to take the time to listen to my patients and their parents’ concerns and provide reassurance when appropriate. In my marriage, my husband answers my medical questions and has a realistic perspective of what patients go through.”
Gratitude for her dad and husband
“I realize how fortunate I am to have a father (and now a husband too) who is a gastroenterologist who can answer my questions and to help me navigate our healthcare system, especially insurance! When my gastroenterologist decided I needed to start a biologic, and recommended Remicade, my dad pushed for Humira so that I wouldn’t have to worry about scheduling infusions around my college class schedule or worrying about transportation when I didn’t have a car. At the time I had no understanding of how having a chronic disease would affect my life.”
It was the first biologic created to treat Crohn’s disease (and later ulcerative colitis). Remicade (Infliximab) was approved by the FDA in 1998 for Crohn’s and 2005 for UC. The medication set the stage for a new way of treating and targeting IBD. A lot has changed in the last 23 years when it comes to treating IBD with biologics (Crohn’s and Colitis Foundation Biologic Fact Sheet). As patients we’re “lucky” that more options are available, and several medications are on the horizon. But Remicade remains a tried-and-true treatment option for IBD patients.
A few weeks back, I shared an article on my blog entitled, “The Patient Experience: What The IBD Community Says About Entyvio.” The article featured viewpoints, experiences, and tips/tricks from several people with IBD who are currently taking Entyvio or have in the past. That article and this one have NO affiliation or guidance from pharma. This is strictly created from the IBD patient experience.
The discussion on Entyvio was well-received and from there, I decided to do an exposé if you will, about other biologics, too. When I was told I needed to start a biologic while lying in a hospital bed in 2008, my mind was racing. I felt like I had nowhere to turn. There were only two options at the time. I didn’t know what resource to trust or where to go for information. My hope is that these articles help comfort you as you make these important, lifechanging health decisions, and alleviate a bit of the fear associated with being on a biologic drug long-term. Use these candid quotes to serve as your roadmap to navigate the unknown.
Before we dig deep into Remicade from the patient and caregiver perspective—a reminder that much like the way IBD presents and manifests in each of us, each person’s experience with biologics is unique to them. Remember that your experience could be better and could be worse.
What does anti-TNF mean?
Each biologic is associated as a class of drug. Remicade is an anti-TNF, meaning that the medication blocks a protein in your immune system called TNF-alpha. That protein can cause inflammation in your body. People with IBD produce too much TNF-alpha, which can cause our immune systems to mistakenly attack cells in the GI tract. Anti-TNF biologics work to regulate this protein in our bodies.
The Patient Voice
In this article you’ll hear from those who just started Remicade in the last week to someone who has been receiving infusions for 21 years! Thanks to each and every person who offered input, I wasn’t able to feature everyone’s perspective, but your narrative helped guide this piece.
Amanda Rowe started Remicade nine months ago. She was hesitant to start a biologic, but ever since taking the plunge, she hasn’t looked back.
“I haven’t had any issues. I get pre-meds of Benadryl and Solumedrol because I got slightly itchy during one infusion. It’s a nice quiet time to sleep or I bring my phone and earbuds and watch a show. It’s 2 hours where I get a break from hearing, “Mom, I need…” I currently have no active disease after being in a bad flare for two years. I flared that long because I was afraid of starting a biologic. My GI explained everything to me and calmed my fears about possible side effects and I finally agreed. I just wish I would have started Remicade sooner, so I could have felt the way I do now.”
Phylicia Petit has Crohn’s and has been receiving Remicade infusions since she was a teenager 11 years ago, she’s grateful the biologic has worked well for her.
“I’ve had a dosage increase and have added mesalamine for better inflammation control. Other than those changes, I’ve been relatively symptom-free, which is a major blessing! I would highly recommend having home health do your infusions. I haven’t had to take off work for my infusions and it’s so nice to be in the comfort of my home…especially with COVID! It’s also cheaper for insurance. I use Janssen Care Path for financial help. It helps to cover your infusion costs. I fortunately have never had any side effects.”
IBD is a family affair for Kara Cady. She has ulcerative colitis; her dad was diagnosed with Crohn’s as a teen and her little sister was recently diagnosed with UC. She just started Remicade last week.
“I’m still on the loading doses. The infusion process is long! It’s about 3 hours for me. I am able to get mine at my GI’s office. I can bring my laptop and work from there. I was super nervous for my initial dose, but my main “issues” are feeling tired, and having a headache and sore throat after. I’m looking forward to getting on my regular Remicade schedule, as I’ve been in flare for about 6 months.”
Laura Steiner is a nurse practitioner with ulcerative colitis who has depended on Remicade for over seven years.
“I have had to increase my dosage and shorten the interval but continue to stay in remission while on it. I’m usually wiped out the day of and the day after. I get my infusions on Fridays, so I have the weekend to recover. The only downside is many major insurance companies are forcing patients to switch to biosimilars, so after 62 doses of Remicade, my next infusion in June will be Inflectra. I’m hoping it will work equally as well.”
Laura is not alone in this fear and dealing with barriers to care and insurance coverage is a reality for many. While working on this article, a social worker from an insurance company reached out to me and said in the last week alone she’s dealt with several cases of people who have had their Remicade denied. She’s helping them through appeals. Until you’re a person who is dependent on a medication for improved quality of life, where timing is of the essence for receiving it, it’s difficult to grasp the magnitude and the pressure of not being able to receive your medication when you need it and risking a flare spiraling out of control or losing your remission.
Meg Bender-Stephanski was on Remicade to treat her Crohn’s for about a year and half. It worked well for her, but she says the infusions were not only inconvenient but costly, so she ended up switching biologics.
“I was going to college in Oregon while my main insurance was based in California, and the out of pocket costs the first few infusions in Oregon were around $18,000. It ended up being cheaper for me to fly home every 8 weeks for an infusion than it was to receive it in Oregon! I also really wanted to study abroad, and it was incredibly difficult to figure out the logistics. Remicade did work well for me and sometimes I have regrets for switching off it for personal reasons.”
Advice for Infusion Days
Kelly Dwyer was diagnosed with Crohn’s in 2018, but experienced symptoms for several years prior. She has great advice for gearing up for infusion day and beyond.
Take along a caregiver for your first infusion, if you can, just in case you have a reaction.
Make sure you make a plan for pre-meds or no pre-meds with your GI before you go to the infusion center, so you don’t get surprised by their policies. Kelly takes Zyrtec the night before, so she doesn’t get drowsy and Tylenol right before the infusion to alleviate the headaches she gets towards the end of an infusion.
The first few infusions should be slow infusions, to make sure you don’t have a reaction. Kelly has continued to receive hers at a slow rate (2-2.5 hours) because her blood pressure tends to bottom out when the Remicade is pushed to a higher rate. But for many, a higher rate works and helps the infusion go quicker.
Switch arms and spots for your IV. Kelly says she saves her “big veins” for times when the nurses need to do a blood draw before the infusion and have to use a larger gauge needle.
Hydrate well the morning of the infusion and bring along a heating pad, as it may help to wrap it around your arm if you’re dehydrated before the IV is started.
Openly communicate with your infusion nurses. Let them know if you feel weird or off in any way. Nurses have seen it all and can be very reassuring and helpful, but you need to give them feedback so they can help you and act right away if you’re starting to feel poorly.
Your reaction one day may be different the next. Kelly says she doesn’t have consistent reactions each time, so it’s important to be vigilant and always be prepared to expect the unexpected.
For Kelly, she doesn’t start to feel the effects of Remicade for a few hours after the infusion. She gradually starts to feel more and more grumpy and tired. She gets a very particular kind of fatigue the day of her infusion. She says it’s a very numbing, all-encompassing, tiring feeling.
Be aware of what dosage you’ve been prescribed. Understand there are several variables that your GI can change if the Remicade isn’t working immediately or enough. The interval time between infusions can be shortened, and/or the concentration of the medication can be increased.
Remicade is often given with other immunomodulators, like Methotrexate. Talk with your GI about scheduling and timing for the infusions with your other medications.
If you’re just getting started on a biologic, your GI will likely tell you to get vaccinated for Shingles and Pneumonia before starting. You’ll also need to do an annual TB test.
Kelly also advises patients to be aware of insurance companies in the United States. Like we touched on at the start of this article, she says many are requiring people to switch from the brand name Remicade to a biosimilar of Infliximab.
“I’m making the switch over at my next infusion in July and my GI and I agreed that we felt confident on the data out of Europe about the efficacy of biosimilars. I recommend everyone with IBD to do their own research and have this conversation with your GI. Be proactive and prepared to discuss options when the time comes with your insurance company.”
Balancing the Logistics of Infusions and Work/Life
Megan Alloway has counted on Remicade to keep her Crohn’s under control for 21 years. She prefers to get her infusions on Friday so she can use the weekends to recoup because it makes her so exhausted.
“While Remicade has been a blessing to me for over two decades, it feels like every time I turn around, it’s time for another infusion.”
An OBGYN with Crohn’s who wished to remain anonymous, has been on Remicade since she was 18. She’s now 35 and still receives her infusions every six weeks. She credits Remicade for giving her a full quality of life and enabling her to stay out of the hospital.
“Since starting Remicade, I have been able to finish college, med school, and residency with my symptoms under control. I’ve stayed out the hospital ever since I started Remicade. My main complaint is how long the infusions take. Different infusion centers have different protocols and requirements, but usually mine take over two hours. It’s annoying to find that kind of time on a weekday and be able to take care of my own patients, but I have to do it for my health.”
Heather Richter agrees the time an infusion takes can be inconvenient, but she’s learned to make the most of the “me” time as an IBD mom with Crohn’s disease.
“I’ve learned to embrace the “alone” time. Be persistent at your infusions and if something seems off to you, speak up and make sure you feel like you’re being listened to. My infusion nurse gives me Benadryl and Tylenol beforehand, so if I have the kids taken care of, I find it helpful to nap and rest afterwards.”
Kristi Reppel has been taking on Crohn’s for 18 years. She received Remicade from December 2005 until August 2011. She switched biologics for a lifestyle change and started Cimzia in September 2016. She ended up back on Remicade in December 2016. She currently received 7.5 mg/k every 4 weeks instead of the typical 6-8 weeks.
“This biologic works for me. It gets me in remission and keeps me there. I am a lot less symptomatic, thanks to my medicine. The bad part of all this is my veins are scarring over because I only have a few good ones and those are almost gone. The post infusion exhaustion and headache can also be a lot. As an attorney, finding the time to sit through an infusion and schedule it around court room hearings can be rough. I cannot recommend enough about the importance of hydrating with water that has electrolytes like Smart Water around infusion day. It’s made a big difference for me!”
Linde Joy Parcels says Remicade allowed her to reach remission in high school. She had swollen and painful joints, and after starting the biologic, she experienced a complete transformation.
“Unfortunately, I metabolized Remicade too quickly and had to transition to Humira after one year. I loved getting to take a day off school while on Remicade and spent my infusions relaxing with my mom watching soap operas. That was the silver lining for me!”
The Caregiver Perspective—from a wife to moms of pediatric patients
Remicade has been a lifesaver for Rebecca Kaplan’s husband. Before starting a biologic, she says his Crohn’s was not well-controlled. He was on one medication, going to the bathroom 25-30 times a day. By the time her husband started Remicade, the damage had already been done and was irreversible, so they didn’t see the true impact of the biologic until after he had bowel resection surgery.
He’s been on Remicade for 11 years this summer and in that time, he’s been able to graduate with a master’s degree, work full time, work out, play softball, and attend family functions. He’s also put on close to 45 pounds and gone from malnourished and underweight to thriving.
“Remicade isn’t picture perfect – the few days after his infusion I like to say he becomes a toddler who can’t control their emotions. He’s extremely irritable and says it feels like his brain is on fire. He gets sinus infections more often than before (and apparently that’s not uncommon when you are on a biologic), and he still has some symptoms from time to time. But his last colonoscopy showed that he is in deep remission, and I know that he wouldn’t have achieved that without being on Remicade.”
Rebecca waiting in the car (thanks to COVID) while her husband receives his Remicade infusion.
Alexia Anastasia’s 11-year-old daughter started Remicade in February. The list of side effects and hearing a horror story from a friend who “had a friend who had a stroke” made her a nervous wreck. Ultimately, she looked at the research and the long history of pediatric use of Remicade and felt she was making the right decision alongside her daughter’s GI.
“It’s been a game changer. We learned quickly my daughter needs it every 4 weeks after trying to go for 6 weeks. I’m so grateful it seems to be working. Her fecal calprotectin is almost normal from originally being 3,460. Her inflammatory markers are back to normal. I just hope it keeps working and the side effects remain minimal. It’s been a challenging 5 months with this new diagnosis. Now that I can reflect, I’m grateful my daughter’s GI pushed for us to start a biologic immediately. My daughter was withering away before my eyes and now she is back on track.”
Beth Otto-Stapleton’s daughter Penny started on Remicade when she was diagnosed with Crohn’s disease in January 2017 at age four. She was given two infusions a few days apart while hospitalized during her first flare. Unfortunately, that is when Penny suffered heart damage and was diagnosed with heart failure because of the Remicade.
“She now does Vedolizumab infusions instead because it is a different class of biologic. We are thankful as a pediatric patient, Penny can go to a Children’s Hospital for treatments…it keeps the hard parts of the disease there and keeps our home a safe/comfy space. The great part about the infusions is that we also get blood work done and get instant feedback. I always ask the infusion nurse to give her an extra bag of fluids so she’s well hydrated.”
Dermatological Side Effects
While talking with patients about their Remicade experience, skin issues came up in a few conversations.
Remicade was the first biologic Dana Drengler tried. She says it worked the best and the longest for her. She was in full remission and lived a normal life while on it. Unfortunately, after about 3 years in, she started to develop red spots on her lower legs. They looked like broken blood vessels at first, but then started to spread and get larger, eventually turning into deep and painful ulcers.
“The ulcers covered my lower legs and became super painful, to the point where I couldn’t walk some days. It stumped my doctors, and they only thing they could think of was that it was a reaction to Remicade. They had me stop taking it and within a few months, my legs started to heal. I still have scars 5 years later!”
Mia Frakes has been using Remicade to control her Crohn’s inflammation since 2017, overall, she feels the medication does the trick, but she has what she calls the “oddest side effect”.
“I’ve been dealing with extremely red, dry, and flaky skin in strange areas like behind my ears and my belly button. My GI says she has seen this dry skin in other patients, too. I have to go to the dermatologist, and they give me topical medication to put on the dry areas, which seems to help.”
Madelynn Jessberger was diagnosed with Crohn’s in 2008, she’s been on Remicade the last three years. She was receiving infusions prior to getting her colon removed and was put back on the biologic after. Aside from some aches and tiredness after infusions, she also developed a rash.
“I developed psoriasis all over my body and my GI is unsure if it’s a side effect, a separate autoimmune disease, or an extra intestinal manifestation of Crohn’s. I manage the rash with thick creams and topical medicine from my dermatologist. Everyone is different, this is just my experience.”
Pregnancy + Motherhood and Remicade
Alyssa Leggett started Remicade in August 2018. At first, she was getting infusions every 8 weeks. Then, in 2019, two weeks before an infusion she started feeling fatigued and was dealing with urgency, pain, and diarrhea. Because of those symptoms, her infusions were moved to every 6 weeks.
“After I gave birth, my doctor wanted to switch me to the rapid rate infusion. I’ve been doing those since November 2020. They’re about an hour shorter and I don’t have any side effects from them. I feel like I can have a more stable life. I still get symptoms from time to time, but I attribute that to the food I eat. Thanks to Remicade, I reached remission and had a healthy, full-term pregnancy.”
Allie Heiman is grateful for how Remicade has helped prepare her body for motherhood.
“I haven’t had any side effects from Remicade and have found the infusion to be easiest in my hand with only minor bruising the next day or two. I started in March 2020 and was cleared to start trying for pregnancy in December 2020. After 13 years of negative scope results and being told I was not healthy enough for pregnancy, I could not be more thrilled with the outcome. I am hopeful to be a mom in the future, and grateful that Remicade made that a possibility with Crohn’s.”
Tayler Jansen is an IBD mom of two. “Remicade has been amazing! Remicade and Imuran have kept me in remission for the past 9 years and enabled me to have two healthy pregnancies.”
Shakila Almirantearena has identical 5-year-old twin girls. She was diagnosed with Crohn’s shortly after they were born and is currently in remission. Along with Remicade, she takes Methotrexate.
“I take Tylenol and Claritin at the infusion center to prevent any rash, etc. I usually take the whole day off work and really allow my body to rest. I haven’t had any major side effects. I’m usually tired the next few days and sometimes get a headache the day after my infusion, but Tylenol helps alleviate any pain.”
Christine Renee has had Crohn’s for 20 years, she’s a mom of two teens and a teacher.
“Remicade was a game changer for me compared to the previous meds I was on. I eventually developed antibodies to it, and it wasn’t as effective. My tips for those getting started are to not be afraid. I was so nervous about starting a biologic, but after the way I was feeling and the tests that my doctor performed, I knew it was the right thing to do. I started Stelara a few days ago and I’m hoping for similar results.”
Hydrate well the day before, day of, and day after.
Remember your headphones or AirPods so you can drown out the noise and watch a movie or show. Noise canceling headphones for the win!
Pack games and books to pass the time or your laptop so you can work.
Have someone else drive you when possible, in case you are drowsy from the Benadryl.
Pack snacks and drinks. Many infusion centers will also have this available for you.
Have a sweater or blanket!
Lauren Hopkins has been on Remicade well over a decade and receives what’s considered a “double dose” every 5 weeks. She’s found her sweet spot and has been able to maintain remission. She says, “Refrigerated Remicade mixed with room temperature saline feels COLD pumping into your veins. It shouldn’t hurt, so if it does, say something to your nurse so they can fix your IV.”
Have the Infusion Nurse run saline before and after your infusion to help with headaches.
Be your own best advocate. Speak up to your care team if something feels off, if your symptoms are persisting, or if you’re dealing with side effects that make your life challenging.
Remember if a biologic fails—it’s not on you, you didn’t fail anything, the drug failed you.
In the spirit of Mother’s Day—today’s article celebrates mother and daughter duos with IBD. Rather than focusing on the hereditary factor of Crohn’s and ulcerative colitis, this story celebrates the camaraderie, bond, and connection created when a parent and child both share the same disease. While the chance of passing on IBD when one parent has Crohn’s and ulcerative is relatively low according to the Crohn’s and Colitis Foundation (between 5% and 20% of people with IBD have a first-degree relative, such as a parent, child, or sibling who has one of the disease), it happens. My hope is that if you dream of being a mom or a dad, you don’t rob yourself of going after that dream because of the fear of passing on your disease to offspring.
As a mom of two (soon to be three!), I am the only one with IBD in my entire extended family. But, I often worry and wonder if my Crohn’s will be passed on to my children. I know this is a common fear many in the community grapple with. Check out these thought-provoking and comforting firsthand accounts from 8 mother-daughter duos that show how families unite in their diagnosis and lift one another up.
Corri Gardner and her mom both have ulcerative colitis. Her mother’s father also had UC. Corri’s mom was diagnosed with IBD while she was pregnant with her. All she knows since being diagnosed herself is having her mom and grandpa to confide in through the ups and downs of the disease.
“My mom has always been there to validate my fears and feelings on such a deep level since she knows exactly what I’m going through. When I was diagnosed, she expressed how guilty she felt over and over again. I always assure her that I would much rather be on this earth, living with UC, than to not be here at all. If someone is hesitant about having children due to their IBD, I would urge them to not make life decisions based on fear.”
Camryn Asham and her mom both have Crohn’s. She says having a parent with IBD helped her feel less lonely and more understood when she was diagnosed. Like anyone with a chronic illness she’s gone through a range of emotions on her patient journey—everything from anger to grief.
“I’ve had the “why me” feeling, but deep down I know it’s not my mom’s fault and there is no one to blame. I know my mom has felt guilty watching me go through traumatic moments and all the ups and downs. I’ve been able to witness my mom get through the highs and lows of IBD, and that reassures me I can get through any flare up or procedure, too. I know I can always count on my mom for help and support when I don’t feel heard or understood.”
Rachel Martin and her mom both have Crohn’s disease. Her mom was diagnosed at age 14, she found out she had the same disease when she was 22. While the diagnosis was devastating for both, Rachel says she finds comfort in knowing that she has someone close to her who can relate.
“I do feel as though my mom feels guilty for passing Crohn’s. I have a twin sister who does not have Crohn’s and it has been hard seeing her live her life without going through everything that I have gone through. Never in my life would I wish this upon anyone, especially my sister, however I wish that I never had to go through this. I never exactly blamed my mom, but I have spent a lot of time wishing I “lucked out” like my sister did. I know that my mom feels bad that I have had a really hard time coping and accepting that I also have a chronic disease.”
Diagnosed prior to a parent
Mary Catherine Kirchgraber was diagnosed with Crohn’s when she was 10 in 2000. Her mom was diagnosed during a routine colonoscopy when she was 50-year-old in 2013. Since her mom served as her caregiver and advocate since she was a pediatric patient, it’s made for a unique journey and perspective. They both seek medical care through the same GI practice and have been on the same medications. Mary says it’s nice to have someone to commiserate with about frustrations with insurance, feeling poorly, side effects, and more.
“My mom is the toughest person I know and never complains, so she inspires me in a million different ways. I wish she didn’t have to struggle the way I have, but it’s nice to have someone to lean on and ask questions to. My mom has always been my advocate and greatest support. She fought for accommodations at school, taken me to Mayo Clinic, dealt with insurance, and taken me to every doctor appointment and specialist I’ve ever needed. She created binders of medical records for me and often reminds me of my own health history when I don’t remember things from when I was a kid. I am so lucky to have her on my team.”
Sharan Kaur was diagnosed with Crohn’s in 2002, her mom found out she had ulcerative colitis in 2017. She says prior to her mom’s diagnosis she felt alone dealing with the day to day struggles of IBD. Sharan says because of her knowledge and experience living with IBD, when her mom began to experience symptoms, she was able to push for their general practitioner to take action immediately and reach a diagnosis. She is grateful to have another family member who can grasp the severity of the disease and who understands how easy it is to go from feeling perfectly fine one day, to barely managing to get out of bed the next.
“I think we find strength in one another. For years, my mom supported me through my worst days and although she didn’t completely understand how things were before her diagnosis, the support was always there. Finding out she had UC broke my heart because she’s always been so active, truly a supermom. I realized then that this would have to change for her as she would probably go onto face the same daily struggles that I do with fatigue. As an adult I’m sure this change in lifestyle is much harder to accept than it was for me.”
Mary McCarthy was also diagnosed with Crohn’s at age 12 in 1995, her mom didn’t discover she had Crohn’s until 2015 when she was 62 (and her dad has UC!). IBD was foreign to the McCarthy family when Mary was diagnosed though. She says her mom had a difficult time coping with having a child with a chronic illness. Even though her mom was well-versed on IBD by the time of her own diagnosis, hearing the news was still difficult for her.
“We deal with it mostly through empathy and humor. Being able to talk openly about the emotional and physical aspects of the disease helps. My parents and I joke about how we are colonoscopy experts and have seen every gastroenterologist in the city of Chicago. My mom knows exactly what I need before colonoscopies, which is often to get some alone time and get in the zone. We laugh about it now. “Mom, I love you, but I gotta get in zone. You can wait in the waiting room now.” My mom has been there for ALL important moments in my IBD journey. We sometimes reminisce about the complete chaos we went through when I was 12. We may have IBD, but we know life must go on.”
Michelle Schienle and her mom were both diagnosed with Crohn’s in 2015, she was 23 her mom was 52. Michelle’s diagnosis was the catalyst for her mom to seek additional treatment from a new gastroenterologist. As we all know it can be challenging to articulate IBD symptoms to those who haven’t experienced them. Michelle knows she can always count on her mom no matter what she’s going through. Even though she doesn’t blame her mom for passing on IBD to her, she did get frustrated that she didn’t recognize the suffering earlier as a child because that was her mom’s “normal”, too.
“Since she was living her life that way, she thought my problems were “normal”, so I had to wait until I was old enough to advocate for myself to get the answers I needed. I wish she wouldn’t feel guilty for passing it on to me, because it’s not her fault. Seeing my mom push through gives me strength. I’ve seen firsthand how she’s successfully raised a family, had a great career, and traveled the world (all things I aspire to do!) and done it with IBD. It’s a relief not to have to explain the pain and worry in detail because we just know what the other is going through. As unfortunate as it is that we both are going through this, having my mom understand what I am feeling both physically and emotionally helps to validate it. If my children are to ever get IBD, I am now confident that I am in the best position to take care of them because I know what to watch out for and how to be proactive about treatment.”
History repeating itself
Both Ellen Jenkins and her mom were diagnosed with Crohn’s when they were 18 and freshman in college at the same school! Ellen says her mom still feels responsible for her being sick, even though she has never blamed her for IBD.
“Growing up and watching my mom live a normal life despite her IBD comforted me when I was diagnosed. I am so thankful to have someone who understands firsthand what I go through. Although no parent would choose to pass Crohn’s on to their child, IBD has made us closer. I have never been upset that I got it from my mom. Instead, I’m thankful to always have her as an advocate in my corner who truly understands the struggles.”
A heartfelt thank you
As an IBD mom, hearing these experiences and perspectives really puts my mind and heart at ease. As you can see, there’s a common thread throughout. Rather than blame their parent for passing on IBD, these young adults look to their parents as a pillar of strength, a source of understanding, and as partners in taking on their illness. Through the pain and suffering there is also gratitude, clarity, and unbelievable resilience. Just how you have grown and evolved as a person after your diagnosis and throughout your patient journey, your child will do the same.
Special thanks to everyone who made this story possible. Your words, your raw emotions, and your candidness are sure to help many and shed light on the incredible dynamic that is created when a parent and a child both battle IBD…no matter what age their diagnosis comes about.
Being diagnosed with IBD as a pediatric patient looked different in the 1970’s. For 54-year-old Brett L., the start of his patient journey began when he was only nine. The year was 1976. He started experiencing fevers, bloody diarrhea, vomiting, and abdominal pain. As he puts it—the symptoms started a year-long quest to find an answer. A quest that involved frustratingly long waits at doctor offices, endless tests, and medical trials. He was ultimately diagnosed with acute ulcerative colitis at the age of 10. Now, in 2021, Brett has unique insight and perspective to share with our community.
Patient “Number 1”
As you can imagine, Brett spent many years on high dose steroid and sulfur pills. The side effects of the steroids (moon face, weight gain, bloating, mood swings, and ravenous hunger, etc.) added insult to injury. From 7th through 9th grade, Brett missed nearly 60 days of school each year due to severe flare ups and hospitalizations. By the time he was 13, Brett’s parents were desperate for a cure as his condition worsened. With no relief from traditional medicine, they sought out additional care from holistic doctors, nutritionists, even an angel healer at one point! Nothing helped to manage Brett’s IBD.
“In 1981, I was 14. I’d been battling debilitating and severe flare ups that made me so weak I had to crawl to the bathroom or walk doubled over in pain. Each hospitalization was taking its toll. Over the years, though I was growing, I had lost 30 pounds. It was at this point that my doctor proposed something that had never been performed on a pediatric IBD patient—a total colectomy and “pull through” operation that would leave me fully reconnected and waiting for the ileostomy closure…allowing me to eventually go the bathroom normally again after a recovery period of a year or so. It was risky surgery back then. But not having it was a risk too. I agreed, and we went ahead with the surgery.” said Brett.
Brett was deemed “patient number 1” for this pediatric procedure and his case study was published in medical journals. To this day he remembers waking up from surgery in the pediatric ICU at Westchester County Medical Center in Valhalla, NY. He recalls counting 18 tubes and lines connected to his body and thinking that he couldn’t believe he chose to do this to himself. The surgery lasted 14.5 hours and the incision ran from his pubic bone to his sternum—the entire length of his abdomen.
Living with an ileostomy as a teen
“I learned to manage the ileostomy with some upsetting and messy mishaps at the very beginning. And in class sometimes the stoma would make embarrassing sounds. I learned to feel it coming and cover it with my hand to quiet it. But without a colon, I was now a healthy 14-year-old. The doctors said that upon examining what was left of my colon, they estimated I had about two weeks left before a fatal perforation,” said Brett.
A year later his ileostomy was reversed, and he was able to go to the bathroom “normally”, again. While he’s grateful for this—it hasn’t been all sunshine and rainbows. Brett says he initially had an abscess at the closure of the stoma. Ever since, he has gone to the bathroom more than normal people. In recent years Brett developed a challenging case of chronic pouchitis that at its worst caused pain and had him going 20-30 times a night.
The good news is that “after about 4 years of this, I finally seem to have treated and solved it myself, with psyllium husk powder at breakfast and lunch times, and 3 Lomotil pills with dinner. I’ve also reduced fluid intake during meals and become more careful about not overeating. I learned some of this in my online research about immediate post-op colectomy patients. The doctors had a hard time helping me with this, but I seem to have resolved it myself.”
From past to present
Today, Brett is a healthy 54-year-old man and his pouchitis has never been more under control. Through all the ups and downs with IBD, he’s lived a fulfilling life as a professional singer, and as an executive of multiple companies.
“In my career I’ve been an investigator, a head of marketing and sales, I’ve grown startup companies, and have traveled the world for business and pleasure. I’ve earned an advanced degree from an ivy league school, and I have an amazing 16-year-old daughter who is a gifted, performing singer-songwriter in her own right.”
Brett believes his ulcerative colitis has made him more appreciative of life and the little things.
“I have always been that person who lingers over sunsets, gazes at the moon, and stops and notices the teeny flowers poking through the cracks in the sidewalk, or street art, and the coincidental things one comes across as noteworthy or remarkable. I notice and really drink in the happy, good moments because I know what it’s like to not be able to be out and experience these things. I know I am fortunate to be here to tell my story.”
Here are some helpful nuggets of knowledge Brett would like both those with IBD and their caregivers to know:
Don’t let fear of IBD stop you from living your life and having fun, or asking that person out, or going out with friends, when you are feeling well. As soon as I was feeling well enough to get back out there after a flare up, I lived life to the fullest and played like every other kid. You deserve to be there just as much as every other kid, teen, or adult does. When you are feeling well, try to make the most of that wellness, and not let the fear of what might happen stop you from living.
You are not “less than”, because you have an illness. In fact, you may even have an added level of maturity because of your illness that others do not, because of your need to contend with it, and interact more with adults and medical professionals and present your situation to them in a coherent and meaningful way. Look for the silver linings in everything. Notice the small pleasures, they help you get through the down times.
To parents—your child is a survivor. It takes a lot to keep them down. They will have ups and downs with their IBD. But 2021 is the best time ever to have to live with this diagnosis. Current treatments and even surgeries have changed the game and the patient experience, for the better and the future is even more promising. IBD can be traumatic. Children and adults can benefit from seeing a therapist to help cope with the lifelong nature and complications of the disease.