New research published in Clinical Gastroenterology and Hepatology offers a glimpse into what Crohn’s disease may look like before it officially begins and the findings could have major implications for how we understand, monitor, and potentially prevent the disease in the future. As an IBD mom of three kids ages 8, 7, and 4, research like this always feels a bit bittersweet. While I’m grateful for the strides in research, I’m apprehensive about the burden and grief I would feel if I was able to know if my children would one day receive the same diagnosis.
As someone diagnosed with Crohn’s at age 21, I’m grateful for my two decades of blissful, perfect health. Had I known a complicated chronic illness would one day riddle my body, I’m not sure how I would have coped and dealt with that news.
This week on Lights, Camera, Crohn’s a look at what the latest research discovered, the complicated emotions IBD parents may feel, and what the future may hold for us all as a community.
Why This Matters: Crohn’s May Start Long Before Diagnosis
The study found that certain immune responses in the blood, specifically elevated IgG antibodies targeting a conserved region of bacterial flagellin (a protein found on gut bacteria) were present years before people were diagnosed with Crohn’s disease. In other words, the immune system appeared to be reacting to gut bacteria long before symptoms like abdominal pain, diarrhea, or weight loss ever showed up.
This study followed 381 first-degree relatives of Crohn’s patients, 77 of whom went on to develop the disease. Among them, 28 (more than a third) had elevated antibody responses.
One of the most important takeaways from this research is the timing. Most Crohn’s biomarkers are identified after the disease is active. This study, however, suggests that immune dysregulation may begin well in advance of clinical disease. This supports the idea that Crohn’s develops gradually rather than suddenly.
That distinction matters. If Crohn’s truly has a long preclinical phase, it opens the door to earlier monitoring and potentially earlier intervention, especially for people who are already at higher risk, such as first-degree relatives of those living with Crohn’s disease. A first degree relative is a parent, child, or sibling.
According to the Crohn’s and Colitis Foundation, 36% of children born to two parents with IBD will develop the condition at some point during their life. The risk is substantially less when only one parent has IBD, with The National Human Genome Research Institute sharing there’s a 7-9% chance.
A Potential Blood Test for Risk, Not Diagnosis (Yet)
It’s important to be clear: this is not a diagnostic test and it’s not something patients can request from their doctor today. But it does raise the possibility that, one day, blood-based immune markers could help identify those who are more likely to develop Crohn’s before symptoms begin.
For families affected by IBD, this kind of risk stratification could be meaningful. Instead of waiting years for symptoms to escalate, or for damage to occur, high-risk individuals might one day be monitored more closely or offered early preventive strategies. As an IBD mom, I feel as though I would struggle with knowing whether this was something I wanted to dig deep for, while also not wanting to get in the way of stopping disease progression. It’s not a black and white situation by any means. If these types of blood tests are available when my kids are teenagers, and I were to get results that broke my heart, I’d feel obligated to be transparent and share—would I really want my kids, who have witnessed me living with Crohn’s their whole lives, to know this would one day be part of their own story? It stresses me out just trying to imagine it.
What This Could Mean for Prevention Research
Another compelling aspect of the study is that the immune response was directed at a conserved portion of bacterial flagellin. This means it’s shared across many gut bacteria. That finding has sparked discussion about whether future therapies or vaccines could target these immune pathways in people who are high risk for Crohn’s.
While prevention remains a long-term goal rather than a current reality, this research reflects a broader shift in IBD science: moving upstream to understand why Crohn’s starts, not just how to treat it once it’s already established, and as an IBD mom I am certainly grateful for that.
What This Doesn’t Mean (Yet)
As exciting as this research could be, it’s not a crystal ball. Not everyone with these immune markers will develop Crohn’s, and many people with Crohn’s were never tested years before diagnosis. Larger studies are still needed to validate these findings across diverse populations and to determine how predictive these markers truly are.
For now, this study adds another piece to the puzzle, one that reinforces what many patients already know intuitively: Crohn’s disease doesn’t start the day you’re diagnosed.
The Bigger Picture
Our community often experiences years of delayed diagnosis, misattributed symptoms, and unanswered questions, so research like this matters. It shifts the narrative from “why didn’t we catch this sooner?” to “how early can we understand and intervene?”
While we’re not there yet, this study represents an important step toward a future where Crohn’s disease is identified earlier, monitored more thoughtfully, and one day possibly prevented altogether.
For parents living with IBD, research like this can carry an added emotional burden. The idea that Crohn’s disease may be detectable years before symptoms begin can stir complicated feelings, especially for those who worry about whether they’ve passed on a genetic risk to their children. Some parents may want every possible tool to protect their child’s future health, while others may find the thought of early testing anxiety-provoking or guilt-inducing. There’s no right or wrong response. I get it and struggle with how I’d handle this, too. Living with IBD already requires navigating uncertainty, and this research underscores how deeply personal decisions about risk, knowledge, and monitoring can be for families. As science moves forward, it will be just as important to support parents emotionally as it is to advance early detection tools.
Community and chronic illness can be thought of as a beautiful tapestry. Our lives and experiences, while unique, become intertwined, and once we recognize we don’t have to embark on the isolating journey alone, we are forever changed. We are so much stronger together. Johnson & Johnson’s published White Paper developed through IBD Social Circle entitled, “The Power of Community in Inflammatory Bowel Disease: Coming Together to Reduce physical and psychosocial impacts” highlights key touchpoints of the patient and caregiver experience and shows the ripple effect of Inflammatory Bowel Disease and how complexity and intricacies of Crohn’s and ulcerative colitis reach far beyond the gut. IBD impacts our careers, our relationships, our identities, our mental and emotional health, and it often dictates how our life stories unfold.
This week on Lights, Camera, Crohn’s, I’ll walk you through the valuable insights from the white paper and show what the research uncovered when it comes to stigma, mental health, online communities, and more. You’ll hear heartfelt reactions from IBD patients and caregivers about the findings and hear what two leading gastroenterologists have to say about the research.
Leaning on the lifeline of community
Jessie Magaro was diagnosed with IBD when she was 15 years old. Her reaction to the white paper speaks volumes.
“I was almost in tears reading this research. When I was first diagnosed as a child, there was no readily accessible community to lean on. It was isolating, depressing, and incredibly lonely. But when my disease returned in adulthood after years of remission, I realized the world had changed,” she recalls. “Suddenly, there was visibility. People sharing their stories openly online, entire communities forming on social media. For the first time, I could connect with others who were like-minded and like-bodied, people who understood my fears, my choices, and my fight.”
That connection wasn’t just comforting; it was lifesaving. It became essential to Jessie’s mental health and gave her the strength to make the hard, necessary decisions about her body and her health that helped her survive.
The white paper digs deep into how and why patients and caregivers crave additional information and resources within the IBD community. According to the survey, “Nearly all people with IBD (95%) are looking for IBD information and resources beyond what their physician provides or discusses with them.” The survey found:
42% of people with IBD have participated in online IBD support groups
37% have engaged with social media forums or group chats on platforms like Facebook and Reddit
28% have followed influencers who share their IBD journey on social media platforms.
Dr. Jami A. Kinnucan, MD, is an IBD specialist at the Mayo Clinic Florida. She says, “This research is profoundly impactful for the IBD community, as it highlights many of the challenges that patients experience but often do not share with friends, family, or even their healthcare team. It opens the door for important conversations within the IBD community and reinforces the need for clinicians to explore the broader effects of disease beyond physical symptoms.”
The pediatric caregiver perspective
Cindy Hancock’s daughter was diagnosed with Crohn’s at age eight, she tells me if there can be a “best” part of being an IBD caregiver, it is “absolutely the online community she’s been so grateful to find and learn from.”
As a result of how heavily her and her daughter have leaned on and benefited from the support of others who “get” the reality of life with IBD, Cindy was not surprised by the findings of this white paper that highlight the power of community.
“The courage to seek out a second opinion, and bring info shared by the second-opinion gastroenterologist to our established gastroenterologist? CHECK. Information about how to interpret iron blood work that helped me advocate for transformational care for my daughter, CHECK. Learning what intestinal ultrasound is, and why it presents an amazing opportunity for IBD care and joining forces with other patients to informally advocate for its increased usage in the U.S., CHECK. Anecdotes about drug interactions via lived experiences of other people with IBD, CHECK. Recommendations about favorite heating pads, CHECK. Learning from another Crohnie that gummy bears who aren’t red or purple are part of a colonoscopy prep diet, CHECK!! I could go on and on all day!” says Cindy.
She feels fortunate that her daughter has a good team of physicians, and they always seek their opinions first of course. But Cindy feels the tidbits they’ve gleaned from the IBD community online are what have transformed her daughter’s quality of life with Crohn’s. “The impact is incalculable.”
Cindy credits patient advocates for helping guide healthcare decisions, saying “the IBD community is akin to a warm blanket. We very rarely interact with people in the “real” world who live with IBD, but every day we get to interact virtually with people just like us who understand this life… and that sense of community is priceless.”
Bridget Brown’s daughter was diagnosed with Crohn’s two years ago when she was eight. She says, “Humans are built for connection—but when you’re handed a diagnosis that isn’t widely understood, it can feel incredibly isolating. Most families reach an IBD diagnosis after some really dark, confusing months and years. The IBD community brings the light back in.”
She says as a parent, hearing other people’s stories and experiences is everything.
“I don’t know what it feels like to live inside my daughter’s body, but the insight gathered from the online IBD community helps me support her better. There’s real strength in shared stories, and there is nothing more valuable than being heard from someone who truly gets it.”
Dr. Hilary Michel, MD is a pediatric gastroenterologist at Nationwide Children’s Hospital in Ohio. She says in reading this white paper she could not help but think about how the concepts also apply to children and adolescents with IBD.
“In addition to physical symptoms, youth with IBD are also at increased risk for anxiety and depression and school absenteeism. In a period of life characterized by marked changes in development, independence, and relationships, the diagnosis of a chronic disease like IBD can be incredibly impactful,” says Dr. Michel. “Access to the IBD community for education and support is likely to be equally as important to young people with IBD and already exists in formats including in person and online groups, advocacy efforts, and camps, such as Camp Oasis. Just knowing they are not alone with IBD is so powerful. Additional attention should be paid to privacy and safety concerns when developing interventions for young people.”
Dr. Michel also feels support for parents and caregivers of youth with IBD is essential.
“Parents are at risk for missed work themselves and experience immense guilt and stress related to caring for their child. Connecting with other parents who have “been there,” sharing tips and tricks to navigate their journey, or simply having a listening ear can go so far in allowing parents to feel supported.”
The Power of the IBD Social Circle: A Veteran’s Perspective
Suzy Burnett is an IBD mom of three and blogger at Crohnie Mommy was diagnosed with Crohn’s in 2008. She says when the white paper was published, she read, and re-read, the IBD Social Circle’s latest report.
“The first reading left me stunned by the raw reality encapsulated in the statistics. The second reading became a series of nods: “Yes, that’s me,” I found myself thinking with every single finding. I found the white paper to be fascinating, maddening, raw, and often heartbreaking. Mostly, because I have personally walked down, or known someone in the IBD community who has walked down, every single path described. Simply put, this report is SPOT ON.”
Suzy says her own patient experience deeply resonated with the segment that focused on the critical role our community plays in every aspect of life with IBD: from the shock of diagnosis and the struggle with relationships to the relentless search for answers and navigating new medications.
The Birth of a Community
“When I was first diagnosed, Crohn’s disease was relatively unknown. The internet was not the wealth of knowledge it is today,” explains Suzy. “I was handed a packet of paper, told there was no cure, and left to grapple with denial, depression, and severe flares for years.”
As Suzy grappled with her disease and the years ticked on by, she felt as though the IBD community was born.
“Or we all simply started emerging from the woodwork, bloggers, patient advocates, and a growing number of patients sharing their stories. It felt as if we made an invisible pact: to stick together, stay strong, and fight for each other. It felt like a window of hope opened: I found others. Others like me.””
Suzy says the research done in this report should be shared with every newly diagnosed patient and every “old veteran”.
“We are IBD warriors, and this white paper embodies that truth to the core. It is an invaluable resource for all who suffer from IBD, as well as for the caregivers and family members who stand by their side.”
Recognizing the importance of treating the whole self
Katie Connelly has lived with Crohn’s disease for more than 20 years. She says hearing that patients are afraid to share their emotional burdens with their HCPs is defeating and eye-opening.
“As someone who is lucky enough to have one of those GI specialists who sees me as a whole person, it is imperative that I let her know how I am feeling about my quality of life. It helps her gauge where I am both physically and emotionally with the treatments I am on,” she shares. “With the mind/gut connection being such a real thing, it needs to be instilled in every HCP’s practice to inquire on how their patients feel in life. The responsibility cannot always fall to the patient to disclose everything.”
As a woman living with perianal fistulizing Crohn’s disease, Katie knows firsthand how isolating and complicated the patient journey can be. She credits the patient community for helping her cope and get educated about the questions she has had about intimacy and sexual dysfunction.
“I have had fistula for six years now and have both dated and ended up married while living with them. It has been far from easy, and there is a lack of understanding and communication around it. I hope to start bringing up my own sexual experiences and helpful tips through my own community, Badass with a Bad Ass in hopes to help lower those numbers. I just want us all to feel less isolated in this.”
Being wary of misinformation shared online and in person
Kelly Dwyer says she’s benefited from both in person and online IBD communities over the many, many years of living with her disease. While she’s grateful for community support, she believes misinformation is one of the greatest threats to IBD patients.
“When I attended my first support group after I was diagnosed, I found a community of people who were anti-biologic and unsupportive of many questions I had about treatments and medical care for IBDers. I was so dismayed to see that they were the only in-person support community in one of the US’s largest metropolitan areas, and promoting non-science backed theories of IBD care,” recalls Kelly. “Commitment to strict content moderation and upholding science-backed information is one of the reasons that support communities affiliated with national IBD organizations are an essential part of IBD care and connection.”
While she agrees the online community is beneficial, she also wants patients and caregivers to always have their guard up and be aware of the misinformation and opportunists who go after vulnerable IBDers by attempting to spread fake cures and push “snake-oil” treatment to a make a quick buck.
“As with many chronic illness communities, the newly diagnosed are uniquely susceptible to bad actors because of the desperation and grief that comes with being diagnosed with this incurable, devastating disease,” says Kelly.
While she believes many patient advocates seek to promote accurate and data-driven information, such as advocates like Tina Aswani-Omprakash and Brooke Abbott Abron who are cited in this study, Kelly wants to warn others that just as many others are publicly sharing their support for dangerous treatments, unregulated supplements, and potentially harmful lifestyle and diet choices.
“National organizations, physicians, patient advocates, and support communities like IBD Social Circle are doing their best to create easily accessible, data-driven, and science-backed resources for education for IBDers at all levels of managing their disease, and from diverse cultural and racial backgrounds. Making sure these resources speak loudly and spread far online will be a vital step to combatting the harms of misinformation. We all need to do as much as we can to educate and inoculate fellow IBDers against the dangers of anti-science rhetoric,” advises Kelly.
The financial trade-off and workplace woes with IBD
Ian Goldstein has lived with Crohn’s since 16 years old. The white paper’s discussion on disclosing diagnosis in the workplace and requesting accommodations hit home for him.
“I was fearful of mentioning my disease on job interviews and at work because I did not know if my co-workers would view me differently, if they would think I was less equipped for my role or more expendable. For a long time, I had to get weekly iron infusions, and I don’t know if my employer didn’t like that I worked remotely because of this, says Ian.
The white paper highlights a 2024 survey from the Crohn’s & Colitis Foundation that found more than 40% of people with IBD have made significant financial trade-offs to afford their healthcare, including giving up vacations or major household purchases, increasing credit card debt, and cutting back on essential items such as food, clothing, and basic household items.
“YES! 1000% YES. If I ever take a vacation, it is a weekend trip upstate because I need to make sure I have money set aside to afford my one thousand dollar a month health insurance premium in addition to the deductible and copay costs. If healthcare didn’t cost so much, my life would look quite different,” says Ian.
Everything from career impact to diet resonated with Ian. The focus in the research on foods and beverages that are staples for most but may be on the list of foods people with IBD should avoid (such as fried or greasy foods, spicy foods, sugar-sweetened drinks, and whole-fat dairy). Ian believes it’s important that people understand that it is not just the “unhealthy” or “junk” foods that can exacerbate symptoms.
“For 10 years I avoided vegetables and nuts completely because they put me at risk of having a bowel obstruction. The same foods that would make me healthy could also send me to hospital,” explains Ian.
Falling back on community for overall well-being and treatment decisions
The white paper highlights that, through IBD community engagement and support, patients have reported positive impacts on:
Physical well-being and treatment decisions
39% reported that it has helped them identify ways to make improvements in their physical health and well-being
39% learned how to improve their ability to communicate with their HCPs
39% became more informed about IBD treatment options, including different treatment options they did not know about before
32% learned how to better advocate for themselves with their HCPs
Ian couldn’t agree more, “Community has been a game changer for me. Because of two friends I met from social media, I learned about an amazing surgeon in New York who did an outstanding job with me in 2025, and I haven’t felt this good in years.”
He puts on comedy shows in New York centered around healthcare and because of one show called, “The Autoimmune Saloon,” Ian crossed paths with an audience member who mentioned Intestinal Ultrasound. “No doctor had ever mentioned it to me, but this random audience member did. Because of her, I’m able to get this test, which is much less invasive and informative when it comes to my Crohn’s. This is how community makes an impact: we teach others what we know, things that doctors may never think to tell us.”
Facing the music and fighting the stigma across all races and cultures
According to the white paper, up to 84% of adults with IBD feel that there is perceived disease-related stigma against them, which results in social stereotypes making them seem unreliable or antisocial.
IBD has historically affected White populations at a higher prevalence than other groups; however, the research shows the incidence of IBD is increasing in all races and ethnicities across the US, including in people who are Black, Hispanic, Latino, and East or Southeast Asian. Research also suggests that Black, Asian, and Hispanic individuals with IBD may have a higher incidence of more severe disease.
Kimberly Hooks says, as a Black woman living with IBD, she knows exactly what it feels like to be dismissed, overlooked, and told that her symptoms didn’t fit the picture.
“I was diagnosed late, and even after that, there were delays in getting the medication I truly needed for my severe Ulcerative Colitis. That delay cost me my colon. My story isn’t unique; it reflects what so many Black and Brown patients experience when our pain is minimized or our symptoms aren’t taken seriously,” Kimberly shares. “That’s why this research matters so much. It confirms what we’ve been living. IBD does not discriminate, and our communities are being affected at rapidly increasing rates. This is why I advocate, because visibility saves lives, and every person deserves to be heard, believed, and treated with quality care.”
Kimberly went on to say how incredibly grateful she is for the IBD Social Circle creating a safe space for patient voices and grounding this work in real lived experiences.
“Partnering with advocates to highlight our real stories and pairing those stories with research exploring the physical and psychosocial factors impacting patient care is powerful. It shows the benefits of community and how connection can support people with IBD in every part of their disease management. This kind of work gives me hope. When patients and community come together, we don’t just raise awareness, we help shape a better, more equitable future for everyone living with IBD,” she says.
Acknowledging the struggles IBD can present in motherhood and beyond
As a patient leader and an IBD mom of two small kids, Michelle Pickens appreciates the white paper for a multitude of reasons, especially the notion that we can appear “fine” even while we’re struggling. She also valued the discussion around the wide range of symptoms patients face and how this variability can delay diagnosis and access to support.
“That “in-between” period—when someone is sick but unsure where they fit or where to turn—is incredibly challenging. You experience symptoms consistent with IBD, yet you don’t quite feel part of that community without a formal diagnosis,” Michelle explains.
The section of the white paper on remission really resonated with Michelle. There is often an expectation that once you begin treatment, you will immediately feel better, but that is not always the case. She says it’s important to acknowledge the need for community support when clinical measures indicate remission, but physical symptoms persist.
“I was glad to see the impact on the family unit addressed, especially in areas such as domestic responsibilities and parenting. These are areas where I personally struggle at times. In the workplace, accommodations can be requested to help manage IBD symptoms, but parenting offers no such structure,” Michelle shares. “As a mother, it can be difficult to find someone who can step in and keep things running the way you would, so the responsibilities often fall back on you, even when you’re unwell. This contributes to significant “mom guilt,” and while mom communities exist, the parenting experiences of those without chronic illness differ greatly from my own.”
Addressing mental health struggles
The white paper reveals that more than half (52%) of people with IBD consider the impact of IBD on their mental well-being as negative. Other research studies have shown that individuals also experience depression and anxiety—with as many as 40% and 30%, respectively, experiencing these comorbidities, even while in remission.
The body image issues that stem from IBD such as weight loss, hair loss, steroid-related weight gain, ostomy bags, fistula, and other extraintestinal manifestations make life feel like a minefield. We are constantly up against the unpredictable nature of living with a disease that can rear its ugly head at any given moment. We are constantly forced to pivot and make decisions that often have a direct impact on our overall body image. I remember when I was in college (prior to my Crohn’s diagnosis) that I loved being on camera, working in TV news. Fast forward to five months post-graduation and three months post-diagnosis, and I was mortified anytime anyone tried to take a picture of me. Looking in a mirror was a stark reminder of what I was now and what I used to be.
These photos were taken 3 months apart. Pre-diagnosis and while on 22 pills a day.
Please know that if you struggle with this, you are not alone. As the white paper notes, “as many as 75% of women and 50% of men experience body image issues because of their IBD.”
Final thoughts
This white paper is a gift to the IBD community. As someone who was diagnosed with Crohn’s in 2005, I would have given anything to have a resource like this at my fingertips to validate my struggles and recognize my fears. We are at a pivotal point in patient advocacy and leadership where we can help shape the future of what it means to live with IBD and thrive despite the dark days.
Dr. Matthew Ciorba, MD, a gastroenterologist at Wash U in St. Louis says, “This work offers patient-identified, doctor-approved insight. It brings together perspectives that clinicians alone often cannot fully grasp. The document fills a unique niche in the IBD space. It bridges the lived experience of patients with the expertise of leading clinician advocates. There is truly nothing else quite like it.”
Our community, everyone from patients to caregivers, and medical providers, is so unique. For many of us, these connections and friendships (whether online or in person) have helped us to reclaim a sense of purpose within our disease journeys. My hope is that medical providers and GI psychologists use this research to empower and educate the community by providing this incredible research to patients and caregivers.
Check out the Executive Summary of the White Paper
At the inaugural Cedars-Sinai IBD and Women’s Health Conference, experts came together to spotlight the unique challenges women face at the intersection of inflammatory bowel disease (IBD) and women’s health. Co-directed by Dr. Puja Khanna, Clinical Director of the IBD Women’s Health Program, and Dr. Maria Abreu, Executive Director of the IBD Institute, the event featured a two-part format: clinical updates for providers and education for patients and caregivers. Topics ranged from fertility and pregnancy to nutrition and mental health.
One of the featured speakers was Neha D. Shah, MPH, RD, CNSC, CHES, Senior Dietitian at the Colitis and Crohn’s Disease Center at UCSF and founder of Neha Shah Nutrition LLC, a private practice specializing in nutrition care for patients with IBD. Her session focused on nutrition updates and strategies to support gut, muscle, and bone health in women with IBD. This week on Lights, Camera, Crohn’s I spoke with Neha, and she zeroed in on something every woman with IBD should care about: how to use nutrition to protect our gut, muscle, and bone health.
Why Nutrition Matters Beyond the Gut
Whether you live with IBD or care for patients, you know that IBD affects much more than the gut. Fatigue, abdominal pain, and debilitating flares that blindside us can make it feel like our whole body is affected. While we know this, it can be complicated to know how to address these specific challenges.
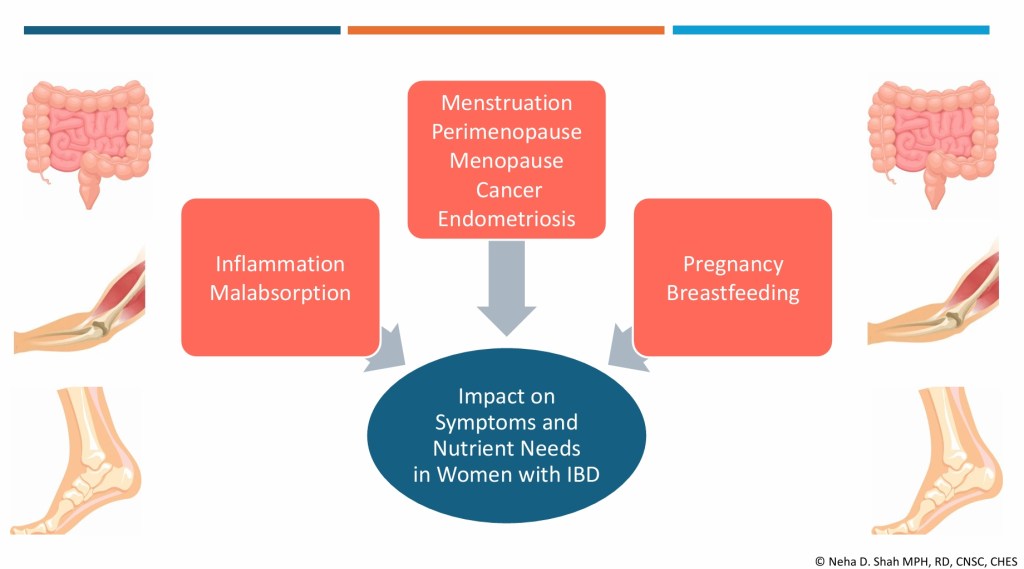
“Women with IBD face a unique set of challenges,” Neha explains. “Poor absorption can contribute to ongoing symptoms, muscle loss, and bone loss. Hormonal shifts, whether from PMS, pregnancy, or perimenopause add yet another layer, often making symptoms unpredictable.”
Her goal? To give women practical, evidence-based strategies they can use to better support their health, both now and as their bodies change through different life stages. As a woman who was diagnosed with Crohn’s disease at age 21, my questions and focus have shifted now that I’m 42 and my family is complete.
“Many women don’t just experience flare-ups; they live with changes in their body that evolve throughout life, impacting daily routines, work, and overall quality of life. In my presentation, I aimed to highlight both the latest updates and practical, whole-food strategies that women can use to better support their health.”
Key Takeaways from Neha’s Presentation
Gut Health
IBD symptoms often overlap with PMS and endometriosis: fatigue, abdominal pain, diarrhea, bloating, and constipation. If you’ve noticed an uptick in your IBD symptoms right around your period, you are not imagining it.
When combined, these conditions can intensify, highlighting the need for careful monitoring and proactive management.
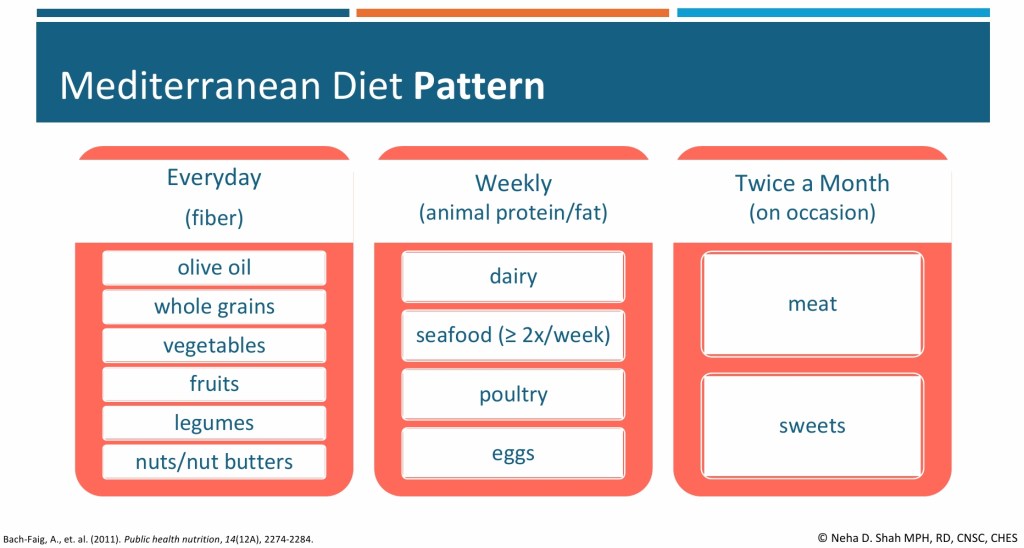
Dietary Patterns: A Mediterranean-style diet rich in fruits, vegetables, whole grains, legumes, nuts, and olive oil may reduce the risk of IBD flares and ease painful bowel symptoms in women with endometriosis.
Fiber Matters: Soluble fiber (oats, fruit) can slow diarrhea, insoluble fiber (leafy greens, brown rice) can help constipation, and less fermentable fibers may reduce gas and bloating. Adjusting textures, like blending or mashing can improve tolerance, especially for those with strictures.
Neha notes that further studies are needed here and she’s hopeful we’ll have even more intel in the future.
Muscle Health
Sarcopenia (loss of muscle mass and strength) is more common in IBD due to chronic inflammation and nutrient malabsorption. Hormonal changes and aging further increase the risk.
Nutrition + Activity: Adequate protein intake (1.2–1.5 g/kg per day for many with IBD) and resistance training are key. Individual requirements sometimes are even higher.
Gut-Muscle Axis: Emerging research suggests fiber may support muscle health by fueling beneficial gut bacteria. The National Health and Nutrition Examination Survey (NHANES) 2011–2018 survey data from 6,000 healthy adults (without IBD) showed each 5 g increase in fiber intake was associated with higher lean mass and grip strength, possibly through increased short-chain fatty acid production. Fiber’s role in IBD and sarcopenia remains understudied.
Practical Tip: Aim for 15–20 grams of protein per meal, combining both animal (e.g., fish) and plant-based sources (e.g., lentils, tofu, nut butter). People with IBD generally have higher protein needs, which can vary depending on weight, activity level, and disease state.
“Evidence in women with IBD is limited. One small case-control study of 23 women with UC versus age- and BMI-matched controls found reduced quadriceps strength, slower sit-to-stand and gait speed, and lower physical activity, though handgrip strength was preserved, says Neha. “Early assessment of nutrition, activity, and lower limb function is crucial. No IBD-specific sarcopenia guidelines exist, but recommendations from the International Clinical Practice Guidelines for Sarcopenia by the annual International Conference on Frailty and Sarcopenia Research by centers at John Hopkins University include increasing protein/calorie intake and resistance training.”
Bone Health
Women with IBD are at higher risk for osteoporosis and osteopenia, especially during perimenopause and menopause. The gut-bone axis reflecting the connection between gut microbes and bone health may play a role. Calcium and vitamin D requirements in individuals with IBD depend on factors such as disease activity, malabsorption risk, corticosteroid use, and deficiency status.
If you haven’t done so already, talk with your care team about getting a DXA scan (bone density scan) so you have a baseline. The earlier in your IBD journey, the better. Bone scans are non-invasive, and probably the easiest test we undergo. You wear your street clothes, lie down on a table, and it’s a quick and painless experience. I have a bone health doctor at Wash U (yes, that’s her title!), who focuses specifically on this after a bone scan in 2022 showed signs of osteopenia and osteoporosis in my 30s. Be mindful on the timing—do not get a bone scan while pregnant or breastfeeding as this can skew the results. If you’re nursing, it’s ideal to give your body at least 6 months after weaning before you get a bone scan, so your bone health is accurate.
Calcium & Vitamin D: People with IBD often under consume these nutrients, particularly when dairy is restricted. For most, calcium needs range from 1,000–1,500 mg/day, with vitamin D at 1,500–2,000 IU/day. In a cross-sectional study of 65 IBD outpatients, nearly two-thirds reported restricting dairy, leading to an average calcium intake of only 343 mg/day—well below the daily recommendation.
Practical Tip: For those who tolerate dairy, start small—a dollop of yogurt, a sprinkle of cheese, or lactose-free milk. Non-dairy sources and supplements can help fill the gaps. When you get labs, you can talk with your GI about looking at your vitamin D level to see if it is adequate or not. I was on 50,000 IU once a week for many years. Now, I take 2,000 IU a day. So, this figure does fluctuate and it can improve.
Nutrition Across Life Stages
Neha stresses the importance of tailoring nutrition guidance to a woman’s age and life stage:
Young women (around age 20): Focus on building peak bone mass, meeting calcium and vitamin D needs, and making realistic choices in dining halls or dorms. Portable, nutrient-dense snacks like yogurt, nut butter, or fortified bars can make a difference.
Premenopausal women: Greater emphasis on long-term bone and muscle health, distributing protein intake evenly throughout the day, and pairing nutrition with weight-bearing activity to maintain strength. Neha’s focus shifts more toward optimizing long-term bone health, since risk factors may be increasing.
“Across both age groups, I prioritize adequate protein and fiber in forms that are well tolerated to help manage symptoms and optimize muscle mass, while also monitoring common nutrient deficiencies such as iron, vitamin B12, and folate,” explains Neha.
The Role of an IBD-Specialized Dietitian
A dietitian specializing in IBD plays a vital role in helping patients understand how inflammation and treatments can affect digestion, absorption, and food tolerance.
“We stay up to date with the latest evidence and tailor nutrition strategies to each stage of the disease—whether someone is newly diagnosed, recovering from surgery, or in remission. For example, we help patients identify which types and textures of fiber are best tolerated, since not all foods impact the gut the same way,” says Neha. “We also emphasize balanced protein intake from both animal and plant sources to protect muscle mass, and ensure nutrients for bone health, like calcium and vitamin D are optimized from both dairy and non-dairy options. Just as importantly, we integrate these strategies into each patient’s lifestyle, culture, and social settings so that recommendations are practical, sustainable, and supportive of long-term quality of life.”
By seeking out a registered dietitian who specializes in IBD you are truly targeting your treatment and receiving personalized care that helps you cut through the confusion, especially if you are newly diagnosed. Their strategies are not just good on paper; they work at your kitchen table and in your daily routine to help you get your health and well-being back under control.
Accessing a dietitian may depend on the healthcare system. Patients can ask their gastroenterologist for a referral, or they may be able to connect with an IBD-specialized dietitian through private practice. Many registered IBD dietitians also do virtual video calls, so it’s not necessary for in-person, local appointments. The Crohn’s & Colitis Foundation provides resources to help connect patients with dietitians who have expertise in IBD.
Final Thoughts
Nutrition in IBD isn’t one-size-fits-all. It requires careful personalization and an understanding of the unique challenges women face throughout their lives. By focusing on gut, muscle, and bone health, women with IBD can better protect their bodies today while laying the foundation for stronger health in the future. It’s not just about flares and managing our IBD, it’s about how our bodies uniquely absorb nutrients, how inflammation affects our strength, and how hormonal changes shift the way we fell over time. Muscle weakness, bone loss, and unpredictable symptoms tied to our menstrual cycles can be a lot, but small, realistic changes in how we eat and move our bodies can make a lasting difference.
It is an exciting and transformative time for the IBD community when it comes to family planning and pregnancy. For years, patients and providers faced uncertainty and conflicting guidance about everything from fertility to medication safety. Now, with the publication of the Global Consensus on IBD and Pregnancy, we finally have a unified, evidence-based roadmap created by leading experts worldwide.
This groundbreaking research, jointly published across multiple top journals, is more than just a collection of data—it’s a lifeline for patients, caregivers, and clinicians seeking clarity and confidence. And for the first time, that guidance comes to life through a series of 12 videos now available online. As the sole U.S. Patient Ambassador and Group Lead for patient advocates worldwide, I was honored to contribute not only to this historic project, but also to share my own journey in the video series—bringing the patient perspective directly into the global conversation.
Grateful for Dr. Uma Mahadevan and the entire team for their incredible work on the Global Consensus.
Check out the video series
Following the release of the research from the 2025 Global Consensus Conference on IBD, a series of 12 videos were also published on the PIANO (Pregnancy in IBD and Neonatal Outcomes website), featuring experts speaking on best practices, emerging data, and consensus statements.
Among those 12, my Patient Perspective video is unique. It’s the only video in the lineup where you hear firsthand experience from an IBD mom. During my unscripted 18-minute video, I share openly about the tough decisions I faced personally, the hopes and worries I encountered while bringing babies into this world, and what I want fellow patients and doctors to know. As an IBD mom of three kids (now ages 8, 6, and 4) who were all exposed in utero to Humira, I have a unique perspective to share.
I know what it’s like when you’re 32 weeks pregnant and have to do a biologic injection while you see your baby’s foot kicking at your belly. I know how stressful it is when you don’t know if you’re going to flare while pregnant or shortly thereafter. I know how complicated and overwhelming it can feel when you’re juggling a chronic illness along with pregnancy and motherhood.
Having a patient video placed alongside expert commentaries is a statement: our lived experience is essential to understanding how guidelines work in the real world. I hope my words leave you feeling seen and empowered.
Preconception Counseling and Contraception for Patients with IBD
The Patient Perspective
Why These Videos Matter
Each video is a piece of a bigger puzzle. Together they tell a story about where we are now, where we need to go, and how patients can be—and must be—central to that journey.
Bridging gaps between patient, clinician, and researcher. These videos are designed not just for patients, but for caregivers, physicians, policy makers, and anyone interested in improving IBD care. Seeing things through the patient lens can spark better communication, more empathic care, and guidelines that address what matters most.
Empowerment through shared experience. Whether it’s coping with symptoms, navigating treatment decisions, or facing uncertainty, this research will make you feel more confident in every decision you make along the way. Rather than feeling like there’s an overwhelming amount of gray area, you can see the roadmap of decision-making created from the Consensus that will help you each step of the way.
How to Watch & What To Do Next
Watch the videos: Listen firsthand and educate yourself. An educated patient is an empowered patient. It’s one thing to read a published medical study, it’s especially helpful to see these videos and watch the research come to life.
Join the conversation: Use these videos as conversation starters, take what you learned into clinic visits, have conversations with your partner/family/friends, or on social media. When you’re talking about family planning, make sure your GI and Maternal Fetal Medicine doctors are aware of the Global Consensus on IBD and Pregnancy to ensure they are up-to-date on the very latest research.
Join the PIANO study. This is a great way to become a citizen scientist and use your journey to motherhood as a way to pave the way for others. I participated in PIANO with my youngest child, and he will continue to be “followed” until age 18. It does my heart good to know we’re helping bridge the gaps in understanding so women with IBD now and in the future can feel more comfortable about staying on medication in pregnancy and during breastfeeding.
Too often, patient voices are an afterthought or an add-on. Being featured as an integral voice, not a sidebar, is a powerful shift. The fact the Global Consensus Conference team made such a point to incorporate patients like myself who are IBD moms, from around the world, goes to show just how inclusive and comprehensive this research is.
Final Thoughts
Living with IBD means navigating uncertainty, physical challenges, and emotional strength, but it also means being part of a community that continues to push boundaries in care. These videos highlight not only the science and data, but the lived realities that bring those numbers to life. Patient voices don’t just complement medical expertise, they help shape the future of care. By placing my perspective alongside global experts, the Consensus reminds us that guidelines are most powerful when they reflect both evidence and experience.
As an IBD mom, I think about what this progress means for my three children and for the next generation of families impacted by this disease. I volunteer my time and energy for these projects because they are at the heart of my patient advocacy and genuinely matter so much to me. The inclusion of patient voices today paves the way for a future where no one feels alone in their decisions about pregnancy and IBD. Together—patients, clinicians, and researchers are building a roadmap that will make the journey clearer, safer, and more hopeful for those who come after us.
When you live with Inflammatory Bowel Disease (IBD), you become an expert in knowing life can throw you curveballs at any given moment. Those curveballs are especially worrisome and scary during pregnancy and after you become a mom.
For one IBD mom who wishes to remain anonymous, that curveball came in the form of a rare and dangerous vitamin K deficiency that caused life-threatening complications for both her and her newborn son after delivery. Now, two years later, a published medical case study based on their experience is helping raise awareness of this rare issue, offering hope that future pregnancies in the IBD community might benefit from earlier detection and intervention.
Diagnosed Young, Navigating the Unknown
This mom was diagnosed with Crohn’s disease at age 13, and now at 34, she’s lived with IBD for more than 20 years. Her journey has included numerous medications, including a long stretch on Humira, which she remained on during her pregnancy, and four partial small bowel resections. She’s also undergone several exams under anesthesia due to complications like abscesses and fistulas.
Thankfully, during her pregnancy, her Crohn’s was well-controlled with no active disease, making the post-delivery complications much more shocking.
A Sudden Turn After Delivery
After giving birth to her son (we’ll call him “B”), what should have been a joyful moment quickly turned traumatic.
She spent 16 days in the hospital, including three in the ICU, while her newborn faced a 23-day NICU stay. The cause? A severe, undiagnosed vitamin K deficiency, which led to hemorrhaging in both mom and baby. The medical team was blindsided—none of them expected this.
Understanding Vitamin K Deficiency & IBD
Let’s get one important thing straight first. This situation is not about skipping the vitamin K shot that newborns typically receive. The mom explains:
“It’s imperative that newborns receive a vitamin K shot after they are born to prevent vitamin K deficiency bleeding. The American Academy of Pediatrics recommends that all newborns receive a single dose of vitamin K, because babies are naturally born with very little in their bodies. In our case, my son did get the shot—but because I was unknowingly severely deficient in vitamin K during pregnancy, his vitamin K levels in utero were dangerously low, leading to a brain hemorrhage before he was even born. The bleeding he experienced was similar to what some babies experience when they don’t receive the shot, but in our case, it happened earlier—and was not caused by withholding care. In fact, he needed far more vitamin K after birth to restore safe blood clotting levels.”
This vital distinction can prevent confusion and reinforce just how important that standard vitamin K shot is for all newborns.
What She Wants Other IBD Moms to Know
“Knowing what I know now,” she says, “I want fellow IBD women to understand a few key things about vitamin K deficiency during pregnancy:”
This is rare. Most pregnant people with IBD will never encounter this issue. “I hope that offers peace of mind. But as we all know, knowledge is power—especially when you live with IBD.”
If you’ve had bowel resections or are deficient in other fat-soluble vitamins (like A, D, or E), consider bringing this case study to your GI and OB/Maternal Fetal Medicine (MFM) doctors. Ask about checking vitamin K levels, as well as PT/INR and PTT, which monitor blood clotting.
You can develop a deficiency during pregnancy even if you’ve never had one before. “Outside of pregnancy, I had no clotting issues. But between my history of resections and my baby’s increasing demand for nutrients, my levels dropped—and no one knew.”
Looking Back: What She Wishes Had Been Done
“If we had been monitoring my vitamin K levels, PT/INR, and PTT throughout my pregnancy, we likely would have seen early warning signs,” she says. “These aren’t standard tests, but I hope someday they will be for IBD moms with similar risk factors.”
A Silver Lining in the Study
Despite the trauma, having their experience turned into a published medical case study brought a sense of closure.
“When they told us they wanted to publish it, I felt incredibly validated. This wasn’t just something we lived through—it’s now out in the world to potentially save lives. That’s the best-case scenario for us.”
The comprehensive care team—consisting of her OB, MFM, GI, hematologist, and PCP—remained closely connected throughout the experience. After both mother and baby were stabilized, Ohio State’s hematology team and Nationwide Children’s Hospital worked together to identify the deficiency as the root cause for both patients.
“They didn’t miss anything—they acted on the knowledge they had at the time, and when things went south, they sprang into action. I’ll always be grateful for that.”
“B” Today: A Story of Resilience
Despite a traumatic start, B is now a thriving, happy, and a miraculously healthy two-year-old.
“We were so worried about long-term impacts due to the hemorrhage in his brain, but he is now meeting and exceeding all his developmental milestones. He doesn’t need any additional support. It’s truly a miracle.”
His early care included close monitoring from neurology and the Early Development Clinic at Nationwide Children’s Hospital, along with early intervention specialists. Today, all those appointments are in the rearview mirror.
What About Future Pregnancies?
The reality is that this situation may recur if she decides to grow her family.
“My doctors believe I’d face similar risks, so we would monitor everything very closely: vitamin K levels, PT/INR, PTT and I’d likely receive IV vitamin K infusions throughout pregnancy to stay ahead of any deficiencies.”
Lifting the Tide for Others
After two decades of managing Crohn’s, she knows how isolating chronic illness can be.
“It’s hard. It’s lonely. It’s easy to feel invisible. But finding others who share their stories and who get it has been a game-changer for me. That’s why I’m sharing this now. Even if this specific challenge never affects you (and I truly hope it doesn’t), I hope you feel a sense of solidarity. A rising tide lifts all ships and if sharing our story lifts someone else’s experience just a little, it’s worth every word.”
If you’d like to contact this IBD Mom don’t hesitate to reach out to me, and I will connect you. It’s stories like this that help to pave the way for future families.
When you’re living with a chronic illness like Crohn’s disease or ulcerative colitis, it’s easy to become hyper-aware of every medication, every symptom, and every nutrient—or lack thereof. One essential mineral that often flies under the radar is magnesium.
Magnesium supports nerve function, hormone balance and how we respond to stress, so when levels drop, the nervous system can become overly reactive. For those with Inflammatory Bowel Disease (IBD), these symptoms can be even more noticeable because our bodies often struggles to absorb and retain magnesium properly.
According to Hollie King, Founder of Sweet Bee Organics, this humble mineral could be one of the most powerful tools in the IBD toolkit. This week on Lights, Camera, Crohn’s Hollie explains why magnesium matters so much for people in our community.
While I was working on this article, I did an Instagram poll asking the IBD community if they take a magnesium supplement. Of the 245 people who responded, 34% said “yes”, 29% said “no”, and 37% replied “should I be?”
The power of Magnesium
“Magnesium is one of those quiet powerhouses in the body,” Hollie explains. “It’s often overlooked, but absolutely essential. It plays a role in over 300 biochemical reactions, helping muscles relax, supporting proper nerve function, balancing hormones, and aiding energy production.”
When magnesium levels drop, your body knows it—but it doesn’t always scream it out loud. Instead, it whispers. Symptoms like anxiety, poor sleep, muscle cramps, low energy, and even restless legs may emerge. But there are subtler signs too: eye twitching, heart palpitations, tingling sensations, and a hypersensitivity to noise or stress.
For those with IBD, particularly Crohn’s disease, magnesium deficiency can be even more pronounced. “When the gut is inflamed or damaged, it struggles to absorb nutrients properly,” Hollie shares. “And magnesium is one of the first to drop.”
The Magnesium–IBD Connection
Recent research, like the article “Magnesium—A Potential Key Player in Inflammatory Bowel Diseases?” published in the Journal of Inflammation Research, highlights the strong link between magnesium deficiency and IBD. But knowing you’re deficient and being able to do something about it are two very different things, especially if your gut can’t absorb it well.
That’s where Sweet Bee Organics comes in. Rather than relying on supplements taken by mouth, Hollie and her team focus on transdermal support—a method that completely bypasses the digestive system.
“Our Sweet Sleep Magnesium Butter delivers highly absorbable magnesium chloride directly through the skin,” Hollie says. “You simply massage it into your chest, feet, lower back, or even your tummy before bed. It’s not just about topping up magnesium—it’s about calming the nervous system, supporting sleep, and helping the body reset.”
The Sweet Sleep Magnesium Butter isn’t just effective—it’s a best-seller across the U.S. and U.K. for a reason. “We’re obsessed with packing as much magnesium as possible into our balm,” says Hollie. “It’s not easy, but we’re committed to delivering a product that works—and works quickly.”
For people with Crohn’s or ulcerative colitis, the benefits of restoring magnesium levels can be profound. Balanced magnesium supports better digestion, improves sleep, reduces muscle tension, steadies mood swings, and even eases PMS symptoms. You sleep better. You feel calmer. Your energy becomes more stable, and your muscles feel less tight or twitchy.For IBD patients in particular, it can help calm inflammation and improve nutrient absorption—essential steps in managing the day-to-day symptoms of the disease.
“It’s not a magic fix, but it’s one of those foundational nutrients that helps everything else work better. The biggest thing people notice? They just feel more like themselves again,” Hollie explains.
Hollie’s Health Journey
This mission is deeply personal for Hollie, who was diagnosed with aggressive cervical cancer and had to completely reimagine how she cared for her body. “Magnesium became an important part of my healing journey. It wasn’t just about sleep or stress—it was about helping my body heal, rebuild, and feel safe again.”
Screenshot
Hollie happens to be my husband’s first cousin—and witnessing her health transformation and all she’s accomplished since her cancer diagnosis has been awe-inspiring. We’re not only family, but friends and I admire her and the genuine work she’s doing. We’ve wanted to collaborate for awhile and when Hollie saw the recent published medical study regarding magnesium and IBD we knew this was the perfect opportunity.
Hollie and I took our kids trick or treating this past Halloween when she was back in the States
Her empathy extends to the IBD community. “For anyone living with IBD, I truly see you. I know how exhausting it can be to manage symptoms, juggle treatments, and wonder if your body is even absorbing what it needs. That’s why I created Sweet Bee. Magnesium might seem like a small thing, but sometimes the smallest shifts are the ones that change everything.”
How is Magnesium Measured—and Why the Standard Test Might Miss the Mark
Many of us assume a blood test will tell the full story, but Hollie points out that traditional serum magnesium tests only measure about 1% of the magnesium in your body.
At my clinic visit with my GI last week, my doctor included magnesium in my lab work and the results were within range, but he also told me there would be no harm in using the transdermal magnesium discussed in this article.
For people with IBD, especially those experiencing persistent symptoms, your GI may suggest testing beyond the standard serum magnesium draw or even recommend supplementation based on symptoms alone. This may be something you want to bring up during your next clinic visit or over the Patient Portal.
How to Naturally Raise Your Magnesium
While supplements are helpful, diet is still key. Magnesium-rich foods include:
Pumpkin and chia seeds
Almonds, cashews, and peanuts
Beans and legumes
Spinach, broccoli, and potatoes with skin
Whole grains like oats and brown rice
Avocados, bananas, raisins
Milk, yogurt, and soy milk
Salmon, halibut, chicken, beef
Fortified cereals
That said, people with IBD often can’t rely solely on food due to absorption challenges. This is where topical support like Sweet Bee’s magnesium products truly shine.
Can You Take Magnesium with Crohn’s or Colitis?
Yes, but with care. Magnesium—especially in forms like citrate—can cause loose stools, which is problematic for IBD patients. That’s why topical magnesium is often a safer, more effective choice.
Always consult with your gastroenterologist before starting new supplements, especially if you’re in an active IBD flare, dealing with kidney disease or if you’re concerned about the medication(s) you are on.
Final Thoughts
In the landscape of IBD care, it’s easy to feel overwhelmed. But as Hollie reminds us, simple, natural tools—when thoughtfully applied—can offer real relief. Whether you’re struggling to sleep, feel calm, or just want to feel like yourself again, magnesium might be what your body’s been craving.
“You deserve to feel strong, rested, and well in your body. Replenishing magnesium levels in a gentle, non-irritating way can make a real difference in how you feel, both physically and emotionally,” Hollie says. “And we’re here to support that every step of the way.”
Learn More About Sweet Bee Organics
To explore Sweet Sleep Magnesium Butter and other clean wellness products created with love and integrity, click here. Use code NATALIE15 for 15% off sitewide.
Sweet Sleep was recently spotlighted on The View Co-Host’s Favorite Things for Mother’s Day. Check out the segment here.
Disclaimer: This article was not sponsored, but the content is for informational purposes only and does not replace professional medical advice. Always consult your healthcare provider before starting any new supplement.
It feels like a punch to the gut. Even though you’re anticipating it, the experience is not easy for anyone. For patients with inflammatory bowel disease (IBD), stability is everything. Whether living with Crohn’s disease or ulcerative colitis, finding a medication that keeps symptoms under control is often the result of years of trial and error. So, when insurance companies or healthcare systems mandate a switch from a familiar biologic like Humira to a biosimilar such as Hyrimoz or Amjevita, the decision can feel sudden, confusing, and unsettling. As of right now (May 2025) there are 22 FDA-approved biosimilars on the market for infliximab (Remicade), adalimumab (Humira), and Ustekinumab (Stelara) with many more coming down the pipeline.
It’s easy for providers to rely solely on the science that says it should be a “seamless,” effortless transition for patients and caregivers—but that’s not always the case, nor is it ever a guarantee. This week on Lights, Camera, Crohn’s we hear from more than 30 patients who have lived this reality. While many people seem to do well clinically, it’s imperative that we also discuss the mental and emotional toll this forced non-medical switch takes on people with chronic, debilitating illnesses and their caregivers. This blog aims to demystify biosimilars, highlight the emotional and clinical complexity of switching therapies, and provide guidance for healthcare providers and patients navigating this challenging transition.
As someone who was forced off my Humira after being on it for 16 years and put on Hyrimoz, I empathize with how complicated this is for patients. Not only was I petrified to switch—but I had a God-awful experience that resulted in going from deep remission to dealing with an adverse response for two months of my life, while trying to be a mom to three young kids.
I don’t take this subject lightly and frankly; I don’t care who I piss off by sharing this patient experience transparently. I angered some donors from a Pharmacy Benefit Manager (PBM) when I spoke on stage in front of a large crowd last fall genuinely thanking my IBD nurse who went to bat for me countless times to help me win my appeal to get back on Humira—this isn’t about profit, it’s about patients. We don’t owe anyone an apology for being uncertain about being told we need to switch our heavy-duty drug therapy not by a doctor, but by someone working in corporate America.
Biosimilars are not generics
First things first, I must clear the air on this. Almost every direct message I receive from patients refers to biosimilars as “generics” …and that’s a common misconception that needs to be done away with.
Unlike generic drugs, which have identical active components, biosimilars are comparable but not identical to their originator drugs. According to the US-FDA, a biosimilar is a biological product that is potent, pure, and safe and that is “highly similar to and has no clinically meaningful differences from an existing US-FDA-approved reference product”. In other words, biosimilars are equivalent to the reference biologics regarding safety and efficacy.
When you hear the terms “originator” or “reference” biologics—that means Infliximab (Remicade), adalimumab (Humira), and Ustekinumab (Stelara). There are many other biologics of course, but so far, these three biologics have biosimilars approved by the FDA. You can familiarize with their names that I’ve listed below so if you see one listed in a letter it’s not foreign to you.
Infliximab Biosimilars:
Inflectra (infliximab-dyyb)
Renflexis (infliximab-abda)
Avsola (infliximab-axxq)
Ixifi (infliximab-qbtx)
Zymfentra (infliximab-dyyb)
Adalimumab Biosimilars:
Amjevita (adalimumab-atto)
Cyltezo (adalimumab-adbm)
Abrilada (adalimumab-afzb)
Hadlima (adalimumab-bwwd)
Hulio (adalimumab-fkjp)
Hyrimoz (adalimumab-adaz)
Idacio (adalimumab-aacf)
Yuflyma (adalimumab-aaty)
Yusimry (adalimumab-aqvh)
Simlandi (adalimumab-ryvk)
Ustekinumab Biosimilars:
Wezlana (ustekinumab-auub)
Selarsdi (ustekinumab-aekn)
Otulfi (ustekinumab-aauz)
Imuldosa (ustekinumab-srlf)
Yesintek (ustekinumab-kfce)
Pyzchiva (ustekinumab-ttwe)
Steqeyma (ustekinumab-stba)
Important note: While these biosimilars have received FDA approval, the availability of some may be subject to patent litigation settlements or market launch agreements, potentially delaying their commercial availability.
Let’s look at the real-life numbers
While working on this article, I ran several polls on Instagram asking the IBD community about their personal experiences. Some of the findings surprised me:
Have you received a letter saying you have to switch? Of the 265 respondents, 64% of patients said “yes”, and 36% said “no”.
Did you appeal before switching to a biosimilar? Out of 200 responses, 33% responded “yes” and 67% responded “no”.
For those who switched was the transition seamless—or did you notice an uptick in symptoms? Of the 140 responses, 51% had a seamless transition and 49% noticed an uptick in symptoms. This right here speaks volumes.
If you responded poorly to your biosimilar and your GI appealed insurance, what was the outcome of the appeal? Out of 75 responses—38% of patients were denied, 32% were put back on the originator drug (biologic), and for 30% after multiple appeals they finally won and returned on their biologic.
Let’s hear directly from patients
Bre: “I was taken off Humira after the New Year and placed on Simlandi for my ulcerative colitis. I was nervous as I had just come out of a two-year flare and had finally found a drug that worked and even though I was reassured that this was as good as Humira, I still had my doubts. Thankfully, I have had a positive experience and have remained in remission since starting Simlandi in January. I hope this story helps others feel less afraid of the potential outcomes when they get the dreaded non-coverage letters.”
Kyrsten: “Back in April I was forced off Stelara to the biosimilar, Yesintek. I went into it with an open mind because my Crohn’s has been in remission for about a year and a half. Unfortunately, I am now experiencing more symptoms that I’m documenting and oral manifestations of Crohn’s and need to see an oral medicine doctor now.”
Stefanie: “I’ve had to switch biosimilars twice at this point, this second time, while I was pregnant. I’m doing just fine!”
Alexandra: “I was first afraid of Humira, then I grew into being afraid of not having it; so, when my insurance mandated the switch to Hyrimoz late last summer, I was so worried (as all are/were)! In September, I was starting to feel some symptoms pop in, so we did all the tests, which indicated that I was still in clinical remission. Thankfully, I am doing ok now with no issues.”
Christina: “It was first recommended to me by my GI a couple of months after diagnosis in 2021 to start on biologics, since the oral medications had stopped working for me. We collectively decided the best option for me would be Remicade, however when it was brought to my insurance company, they immediately denied it. Insurance said it wasn’t their “preferred method” and wanted me to try and fail Humira first. When my GI tried to get the Humira approved, my insurance company ended up denying that, too, and this time, their excuse was it “wasn’t medically necessary.” It took my GI a couple of months to get a biologic approved and I almost ended up back in the hospital as a result.”
After receiving her first injection, Christina ended up developing an allergic reaction and had to be switched to something else. After another month of fighting insurance, Christina’s GI was able to get Remicade approved.
Christina goes on to say, “I did very well on that for about a year, until my body developed antibodies, and I had to switch once again. I then started Entyvio infusions which I have been on ever since, and so far, I’ve been doing well on it.”
Audrey: “I was forced to switch from Remicade to Inflectra a few years ago due to insurance coverage. My job at the time was horribly stressful and very time-consuming and getting the news then about my medication no longer being covered and that my next infusion was delayed because of this change over the phone from my infusion clinic was terrible. I remember sitting in the workplace cafeteria when my phone rang, and I burst into tears and was pleading with the pharmacist that gave me the news prior to receiving the letter.”
At this point, Audrey was receiving Remicade every seven weeks. With the delay and having to wait for Inflectra to be shipped, she was pushed out an extra week.
“The thing that made me so angry, was that I had already received my Remicade shipment, the nurses just weren’t allowed to mix and dispense it because of the insurance change. I refused to toss that Remicade dose until the vials expired, since I knew how costly it was. I called so many charity pharmacies for low-income folks to see if they could take the vials and since its temperature controlled, they couldn’t. Such a waste,” said Audrey.
Thankfully, Audrey tells me she hasn’t had any issues with the switch, and she’s stayed in remission—even during and after her first pregnancy. But she says the stress and frustration that occurred impacted her mental health at the time.
Kelly: “I just got the letter. Been on Stelara since 2017. I also take it every four weeks, even though the recommended dose is every eight weeks. I get my insurance through my husband and our insurance turns over on 6/31/25. The new policy begins July 1st. I’m really concerned and honestly don’t want to deal with this.”
Sandi: “I was forced to change from Remicade that had me in remission for several years to Inflectra and the outcome was not good. I had multiple Crohn’s flares a month, which was not happening when I was in remission. My GI appealed and after a year, insurance started to cover my Remicade again. Since getting back on Remicade, I’m in deep remission, again.”
Britt: “I was diagnosed with Crohn’s in 2011 at the same time I was diagnosed with Primary Sclerosing Cholangitis (PSC), a rare liver disease. I was on Remicade and was switched to Avsola. For a while, I was quite skeptical, but we stayed the course. I had some ups and downs with my health, but I was just told I am in histological remission by my GI! After five years of struggles to find the right medication, my health finally seems to have aligned. I also take 6mp to reduce antibody development to the Avsola.
Danielle: “I went into my pregnancy in remission and my first and second trimesters were lovely. About halfway through my pregnancy, insurance decided it was the right time to swap my medications. Two weeks following that change, I was already struggling. I ended up finishing my pregnancy on two different rounds of methotrexate and iron infusions. I had a scheduled C-section at 39 weeks, and I think my care team hoped that my body was just struggling balancing pregnancy and Crohn’s…that was not the case at all.”
Danielle says she tried two more Inflectra infusions after her daughter was born and saw no improvement. She required a round of prednisone and that didn’t help either. She was then switched to Humira injections every two weeks and they seemed to work wonderfully and she started to feel better.
“Then my insurance threatened to switch me to a Humira biosimilar, but Humira failed me right when that was supposed to happen, so I was transitioned to Entyvio. For six months I saw no improvement on Entyvio…more prednisone and still NO improvement. Finally when my daughter was 14 months old (so over a year and a half of feeling like absolute garbage and having no energy) I got bowel resection surgery and switched to Stelara.”
Danielle went on to say she’s been in remission since December 2021, and she still wonders if switching to the Remicade biosimilar caused all this to happen.
“I truly feel like that change took part of the joy of pregnancy away from me and also took a lot of special time away from my daughter the first 14 months of her life. I spent her second Christmas in the hospital unable to see her for two weeks. I was on so many pain medications for so long before the surgery that I don’t remember her first birthday. I lost a lot simply because someone was trying to cut costs and making decisions they are not educated about.”
Brooke: “I was on Remicade for 15 years, then I was forced to switch to Inflectra. I was incredibly stressed and tried to appeal but lost that battle. I’ve now been on Inflectra for 3 years and I am doing well! I still hate that we are forced to change when something is going well. The amount of stress, anxiety, and time I spent fighting the insurance company took a toll on me.”
Brooke went on to say that she got pregnant and had a daughter while on Inflectra. Her GI and OB had no concerns with the biosimilar during pregnancy.
Maya: “At the beginning of March, I was told by my insurance that Stelara will no longer be covered and that I would be put on Yesintek. I’ve only gotten one dose of it so far, but I very much empathize with all the emotions that come with getting the letter. So far, I haven’t noticed any additional symptoms or changes in how I feel. I’m hoping Yesintek works for me and that I continue to feel ok!”
Maria: “I live in Sweden where Humira is covered by the State since no private insurance is needed, the last year though I was recommended from doctors to switch to a biosimilar. So, in autumn of last year, I decided to try Hyrimoz. I noticed no difference in the first three months, but after that, I saw an increase in symptoms, especially for my rheumatoid arthritis. My doctor recommended that I take the injection weekly instead of biweekly, but that didn’t help at all. Since I haven’t developed any antibodies, my doctor switched me back to Humira and I felt the difference right away.”
Sadly, Maria recently got the news that Humira will no longer be covered in Sweden starting in August, so she will either have to pay out of pocket or find another medication.
“You can imagine how that feels. Humira has been my trusted friend since 2008, managing my Crohn’s and RA so well. Hard to think of life without it,” Maria said with a tearful emoji.
Kenzie: “I’ve been on two different biosimilars of Remicade. Inflectra was seamless—no issues. Then, a few years later, I got new insurance, and they made me switch to Avsola, which I had an allergic reaction to. No allergic reactions to Remicade or Inflectra, after being on them for more than six years. Now I’m on Cimzia injections (not a biosimilar) because it’s safe for nursing and that just seemed like the better option for me right now. I’ve only been on Cimzia for 10 weeks, but so far, my Crohn’s and RA seem slightly better.”
Audrey: “I switched to a biosimilar (Inflectra) in January 2022. I got pregnant in June 2024 and delivered a healthy baby boy this March. No disease issues thus far.”
Tara: “I was on a biosimilar when I conceived and throughout my entire pregnancy. I’m on Hulio and everything went well. I stayed in remission throughout the pregnancy and postpartum.”
Amanda: “I was able to conceive and am currently pregnant on a biosimilar. Everything is going great, thankfully I was on Humira for about six years and then got the dreaded letter to switch. I went on Hyrimoz at the end of last summer and was on it for five months prior to getting pregnant.”
Lauren: “I conceived and was pregnant with my now 3-week-old all while on Inflectra. I stayed in remission the whole time.”
Katie: “I was able to conceive while on Avsola, a biosimilar to Remicade. I haven’t experienced any issues related to pregnancy. I did develop some antibodies though and had to escalate my dose while pregnant. I also take premeds of Solumedrol and Benadryl before every infusion now. I got hives during the Avsola infusion while I was pregnant.”
Erica: “My doctor wouldn’t appeal it. I was put on Amjevita. Thank goodness and knock on alllll the wood…it’s been going well. I haven’t noticed any difference in symptoms. It’s been a little over a month, so I pray it stays that way.”
Jessica: “Conceived and pregnant on Inflectra infusions. I just had a healthy baby girl one month ago, and I’m now breastfeeding. No problems at all.”
Marla: “I switched to Hyrimoz while pregnant and I did not notice a change. However, I will say I’ve been in remission since getting pregnant with my first child and I don’t always take my medicine on time, so I don’t know if the transition was seamless because the medicine is truly fine or if it’s because my body just does well while I’m pregnant and breastfeeding (which I basically have been the past four years having three babies). I will say it’s an ABSOLUTE nightmare trying to get my medication each month. Constant bills I’m having to fight and constant new prescriptions and prior auths from my doctor for the SAME medication. It’s literally unreal. I blame that on CVS Specialty pharmacy.”
Amanda: “While I was pregnant, my OB appealed because insurance would no longer cover my Delzicol for ulcerative colitis. I won but was only allowed to stay on it until I delivered, then I had to switch to a generic mesalamine.”
Christine: “Pregnancy is what got me a temporary appeal. Once the baby was born, I had to switch, but it was peace of mind not having to make the transition during pregnancy. I was anxious that it was just a regular infusion, there wasn’t a loading dose or a slow rate or anything. They just infused the Inflectra the same way they infused the Infliximab. About two years after making the switch, I had to go from every 7 weeks to every 6, but I will never know if it was due to the biosimilar or if after 10 years on a biologic/biosimilar, my body just needed the drug at more regular intervals.”
Danielle: “I was pregnant (in remission), and my GI decided that was the correct time to switch me to Inflectra from Remicade…it did NOT go well.”
Jordyn: “I found out I was pregnant around the same time I had my first biosimilar infusion. I went through my whole pregnancy on the biosimilar and only noticed an uptick in symptoms around 10ish weeks, which a course of steroid foam resolved. Postpartum is when I noticed the return of symptoms the most. After 2 or 3 infusions (I get them every 4 weeks) with no improvement, I asked for an appeal, and it was granted for me to go back on Remicade.”
Natalie: “I got pregnant the month after switching to Avsola. I made the switch November 2022 to the biosimilar and found out I was pregnant December 29th. Pregnancy went fine, delivered in August 2023, all my problems started in February 2024. I went back on Remicade at that point because my GI suspected I had serum sickness for months on end, and to this day, they still aren’t sure if the serum sickness initiated my problem of Crohn’s attacking my joints.”
Angie: “We were told we would have to switch, but the doctor office contacted them, and they will be covering me at least until September for Humira…then we will renew the prescription and hope that it will be covered, again.”
Jasmine: “I’m on Avsola (biosimilar for Remicade) and I wasn’t trying to get pregnant, but did, and had a perfectly healthy pregnancy.”
Allie: “My specialists appealed saying I was going through fertility treatments and then insurance approved my Remicade for another year.”
Malea: “I got my insurance letter recently and have been meaning to reach out as I remember your Humira nightmare. I have not appealed yet, partly because my GI office is incredibly dysfunctional and hard to get ahold of. I am on Stelara, which is the first thing to have kept my Crohn’s in remission and they want me to switch to Selarsdi, which I can not find any patient experiences/anecdotal evidence about.”
Georgia: “I was on Humira last summer when Accredo tried to switch me to a biosimilar without notification. I had a letter saying that my Humira was still covered. I worked with my GI who told me they are seeing this a lot and if the person doesn’t push back, they just switch them to a biosimilar. But, if the person pushes back, the GI calls Accredo with a code (DW1 Brand Medically Necessary) to block it. That’s what I did, and they therefore had to send me my Humira since my insurance was still covering it. I want to let others know in case they have a prior authorization from their insurance saying they will cover Humira, despite the pharmacy trying to switch them!”
Jessica: “I so appreciate you talking about this. For my daughter, I went to refill her Humira, and insurance said the doctor allowed the switch. I asked the doctor, and they said no…it’s insurance. I had to use one of my daughter’s biosimilar pens while mine was being shipped, and I noticed more pain and burning. I advocated for my daughter to be on brand name only and they approved the request. When it came to my biologic, my letter had the same wording and once again it was insurance, not my doctor.”
Jessica’s GI said despite her being in remission for so long, she would need to try the biosimilar, then if any symptoms occurred then they could fight for return to the originator drug.
The Emotional Toll of a Forced Switch
For many patients, switching medications, especially after long-term remission, can trigger anxiety, mistrust, and a profound sense of vulnerability. Here are a few of the emotional and psychological responses patients may face:
Fear of Flare-ups: Patients often fear that a new medication might not work as well, risking disease recurrence and potentially hospitalization. So many of us have been relying on our biologic as a crutch for several years if not decades, it’s worrisome when you find a medication that works and have to change simply because insurance decides it’s necessary.
Loss of Control: Being told to switch due to non-medical reasons (like insurance mandates) can feel disempowering.
Medical Trauma: Those who’ve experienced years of instability before finding an effective treatment may associate medication changes with setbacks and suffering.
Distrust in the System: Patients may feel like financial decisions are being prioritized over their health and well-being.
How to Comfort and Support Patients Through the Transition
Healthcare providers and care teams play a critical role in guiding patients through these difficult changes. Here are some key strategies to help:
Educate With Compassion: Clearly explain what biosimilars are, how they’re tested, and what the current evidence says about their safety and effectiveness in IBD. Emphasize that switching is based on clinical research and real-world data, not just cost. Have discussions about biosimilars with patients in clinic even if they haven’t received a letter in the mail yet so they are prepared.
Validate Their Concerns: Avoid minimizing fears. Instead, acknowledge them openly. Saying, “I understand why you’re anxious about this” creates space for honest discussion and trust-building.
Advocate When Necessary: If a patient is stable and deeply concerned about switching, advocate on their behalf. Some payers allow exemptions if a provider makes a strong clinical case for staying on the original biologic. It may take extra paperwork, but the effort can mean everything to the patient, especially for pediatric patients and women who have family planning considerations.
Encourage Peer Support: Connecting patients with others who have made similar transitions can provide reassurance and reduce feelings of isolation. Patient communities, both online and in-person, can be powerful.
Navigating the Complexity of Informed Consent
True informed consent means patients understand not just the science, but the context of their decision. It’s more than ticking a box—it’s about creating space for dialogue, questions, and partnership. When I received the letter saying Humira would no longer be covered, I alerted my GI team not to sign the new script, as that gives the pharmacy/insurance the ability to switch you. A biosimilar is not able to be prescribed until your doctor signs off on it, remember that.
A thoughtful approach might involve:
Discuss what will happen if symptoms worsen after switching. My GI called me multiple times to comfort me and even prescribed a couple of Xanax pills to ease my anxiety leading up to the switch.
Review the process for switching back (if possible). Have a game plan in place so you’re not scrambling if you notice a change in your health.
Ensure patients know they won’t be left to manage complications alone. Support every step of the way makes all the difference.
Research articles to help you feel informed about biosimilars
An informed patient is an empowered patient. I did some research to help do the homework for you. By reading the articles below you should feel better educated on biosimilars so you feel more comfortable with the switch (if it’s a necessity) and about discussing this further with your care team:
Switching from a biologic to a biosimilar can feel like stepping into the unknown—but it doesn’t have to be done in fear or isolation. With transparency, empathy, and collaboration, patients can be empowered to make informed decisions, feel supported during the process, and maintain confidence in their care.
While some people feel more confident switching from a biologic to a different drug class (for example, Humira to Skyrizi or Stelara to Entyvio) to dodge the biosimilar, others are fearful of building up antibodies to a drug class that is otherwise working. You must weigh the pros and cons and do what you feel most comfortable doing. It’s important to remember it’s only a matter of time until all biologics for IBD have biosimilars, so by switching drug classes you are most likely just delaying the inevitable.
If you are planning to become pregnant or you are currently pregnant and on a biologic or a biosimilar please check out the PIANO registry so you can help pave the way for future IBD families and contribute to research so we have more information about the safety of these medications in pregnancy.
The science behind biosimilars is promising. But the human side of medicine—the fear, uncertainty, and trust involved in change, must be just as carefully managed. I hope after reading this article you feel less alone and supported in your personal health decisions.
There’s breaking news in the IBD community—and I can’t wait to share it with you! I’m thrilled to announce the launch of a groundbreaking new website dedicated to empowering women with Inflammatory Bowel Disease (IBD) by providing them with the critical information they need about family planning, pregnancy, and postpartum. This resource is a direct follow-up from the recent Global Consensus Conference on IBD and Pregnancy, which brought together a world-renowned group of scholars, physicians, and patient advocates from around the globe to review all available science, share information, experiences, and insights in the hopes of offering helpful recommendations designed specifically for women with IBD.
This week on Lights, Camera, Crohn’s a look at the website which launched today (March 4, 2025) and what this means for the patient community, along with sentiments from the one and only Dr. Uma Mahadevan.
Empowering Women with Accurate, Consistent Information
Women with IBD often struggle with overwhelming misinformation and confusion when it comes to family planning and pregnancy. I can speak from firsthand experience as an IBD mom of three kids ages 7 and under. Up until recently, there have been a great deal of gray areas that make family planning extra stressful for those with Crohn’s disease or ulcerative colitis.
From varying recommendations by different healthcare providers to conflicting advice from different countries, the lack of a consistent message leaves many women uncertain and fearful about the health of both themselves and their pregnancies.
Dr. Uma Mahadevan, the Chair of the Global Consensus Conference and the primary investigator of the Pregnancy in IBD and Neonatal Outcomes (PIANO) study, highlights this issue, “Women with IBD suffer from so much misinformation and fear. Recommendations vary from provider to provider and country to country. That is why the Global Consensus brought together GI’s, teratologists, pharmacists, surgeons, etc., from around the world to come up with one guidance document for all patients to have a consistent message.”
The new website, which is translated in six different languages, aims to deliver just that—a unified, trusted source of guidance for women with IBD. With contributions from a multidisciplinary team of experts, the website consolidates the latest, evidence-based advice to help women navigate their pregnancy journey with confidence.
As the Patient Ambassador for the United States, I had a chance to see the work that went into this remarkable resource, and I must admit seeing the site brought tears to my eyes. I can’t tell you how fortunate we are to have this information and scientific research available. Our community has needed this for so many years—and now, the patient experience of navigating pregnancy with IBD will be transformed in the best way.
Visited the FDA with Dr. Mahadevan in July 2024 to share the latest guidance from the Global Consensus Conference.
Addressing the Fear of Stopping Medications
One of the most significant concerns among women with IBD during pregnancy is the fear of medication use. Dr. Mahadevan points out that the absence of consistent advice can lead to a dangerous default, “When there is no consistent message, often the fear default is to stop the meds, which can be harmful to the pregnancy – both mother and child.”
The website’s primary goal is to ensure that women understand the importance of continuing essential medications where necessary and how to work with their healthcare providers to safely manage their IBD during pregnancy. The risks of stopping treatment without proper guidance can negatively impact both the mother’s health and the health of the baby, so providing accurate, clear information is crucial.
As a woman on Humira since 2008, I remember how scared I felt about continuing my medication throughout my pregnancies, but I trusted my medical providers (gastroenterologist, maternal fetal medicine, and OB) and had flawless, symptom-free pregnancies because my disease was so well managed. Yes, it’s emotional when you’re 35 weeks pregnant and feel the baby kick as you’re about to inject medication into your body, but I always told myself that by keeping myself healthy, I was protecting my babies. I also found great comfort in participating in the PIANO study with my youngest and MotherToBaby pregnancy studies with my other two children.
Providing Confidence and Joy for Women
Dr. Mahadevan hopes this website and these materials will give women the confidence to move forward with their pregnancy with joy, not fear, and the strength to resist the misinformation.
The resources on the website are designed to reassure women that pregnancy with IBD is possible, and they can be proactive in ensuring their health and the health of their baby. With expert advice, personalized care options, and up-to-date research, the website offers a beacon of support for women navigating this journey.
What Inspires Dr. Mahadevan’s Work in IBD and Family Planning?
Dr. Mahadevan’s dedication to research in IBD and family planning is rooted in both her professional expertise and personal experience. As a leader in this field, she is driven by the desire to make a tangible difference in the lives of women facing IBD-related challenges. “The science around pregnancy is fascinating, and there are always so many new questions to study. However, the most important thing is that I personally know how hard it is to have a family, and I want to do what I can to help other women complete their families, as there is no greater joy!”
Her compassion and commitment to helping women with IBD fulfill their family dreams are at the heart of this new platform, which seeks to bring scientific clarity and emotional support to those who need it most.
A Call to Action for Women with IBD
The launch of this website marks a major step forward in supporting women with IBD who are considering family planning or navigating pregnancy. It is a space where women can find reliable information, connect with healthcare professionals, and feel empowered to make informed decisions that prioritize both their well-being and the well-being of their future children.
If you or someone you know is living with IBD and considering pregnancy, this website is a must-visit. Please help me in spreading the word so patients across the world are aware of the information available right at our fingertips. Together, we can break down the barriers of fear and misinformation, helping women move forward with confidence, joy, and support.
Visit pianostudy.org/GCC_video/ today to access the resources, expert advice, and community support you need to make informed decisions about your pregnancy with IBD.
Be a Part of PIANO
The PIANO Study is a powerful opportunity for women to get involved in this groundbreaking research that could help shape the future of healthcare for women living with IBD. By participating in this study, you can make a direct impact on understanding the unique experiences and challenges that women with IBD face.
Being part of this research gives you a voice in advancing medical science and contributing to discoveries that could improve the lives of countless women in the future. This is your chance to be a part of something bigger than yourself, to make a difference for others who share your experiences, and to support the next generation of women living with IBD. Together, we can pave the way for a healthier, more informed future. I’m so grateful that my youngest child is a part of PIANO and that we’re contributing to the amazing research that is going on.
Crohn’s disease and ulcerative colitis often require medication to keep inflammation under control, but in some rare circumstances, just one medication isn’t enough. Research shows only 40 percent of people with IBD achieve remission within one year of taking a single drug. Dual Targeted Therapy (DTT) involves using two different types of treatments at the same time to achieve better disease control. This disease management plan comes to play when single-drug therapy does not adequately control symptoms or when a more aggressive treatment is needed.
This week on Lights, Camera, Crohn’s we hear from esteemed gastroenterologist Dr. Laura Targownik along with several IBD warriors who have utilized DTT to help manage their IBD.
IBD Dual-Targeted Therapy Options
There are several ways healthcare professionals can help manage IBD with dual therapy.
Biologics and Immunomodulators
More commonly, combining a biologic therapy such as infliximab (Remicade), adalimumab (Humira), or vedolizumab (Entyvio) along with an immunomodulator like azathioprine, 6-mercaptopurine, methotrexate. The purpose of this is to enhance the effectiveness and potentially lower the risk of developing antibodies against biologic drugs.
Biologics and Small Molecule Inhibitors
A newer approach involves combining a biologic with a small molecule inhibitor like tofacitinib (Xeljanz) or upadacitinib (Rinvoq). This can target different pathways of the immune response, potentially offering a more comprehensive approach to suppressing inflammation. This can be used in refractory cases and should only be prescribed by an expert IBD physician.
In patients who do not respond to single biologic therapy, there is growing interest in using two biologic agents targeting different inflammatory pathways. However, this approach is not yet widely supported as healthcare providers weigh side effects risks and this is considered experimental.
Dr. Laura Targownik, MD, MSHS, FRCPC, Mount Sinai Hospital (Toronto), Departmental Division Director (Gastroenterology and Hepatology), University of Toronto gives a case study for when she would consider using two biologics for example: in a person with fistulizing Crohn’s disease, whose fistulas have responded well to biologic therapy, she would consider adding another biologic if they’re still experiencing inflammation in the intestinal lining. Dr. Targownik says medications such as vedolizumab (Entyvio) or an IL-23 such as risankizumab (Skyrizi), mirikizumab (Omvoh), and guselkumab (Tremfya) could help to bring IBD under control.
“As a gastroenterologist, I don’t want to discontinue the anti-TNF because I fear their fistulas will worsen, so it makes more sense for me to add in a well-tolerated biologic like vedolizumab or an IL-23 to try to bring the luminal disease under control,” said Dr. Targownik.
She went on to say that patients support the idea of combining therapy with different mechanisms of action if the safety profile makes sense. Most patients who are in a position where dual therapy would be considered are open to do what it takes to get their disease under control.
Corticosteroids and Other Immunosuppressants
This is not strictly speaking dual therapy because corticosteroids are always used short-term. But prednisone in conjunction with other immunosuppressants can quickly reduce inflammation while waiting for the slower effects of immunomodulators or biologics to set in.
A Look at DTT and IBD Research
Dr. Targownik says the VEGA and EXPLORER clinical trials shed light on the potential benefits of combining biologics.
The VEGA trials looked at the benefit of combining an anti-TNF (golimumab) and an IL=23 inhibitor (guselkumab) to induce remission in people with moderate-to-severe UC.
“The combination of golimumab and guselkumab outperformed monotherapy, with a 15 percent increase in the likelihood of clinical remission and a 20 percent gain in endoscopic response. Patients then received an additional six months of either golimumab or guselkumab monotherapy,” says Dr. Targownik and the group on the dual treatment had higher rates of improvement and remission.
This suggests that the deep remission obtained early through DTT might have a sustained effect, even if you step down to monotherapy.
“The EXPLORER-CD study was an open label trial looking at high-risk patients early in the course of disease,” says Dr. Targownik. They received a triple combination with adalimumab, vedolizumab, and methotrexate for six weeks. By the end of the study, 55 percent were in clinical remission, and 35 percent were in endoscopic remission. As there was no comparison arm, it is not clear whether these rates are higher than what would be expected.”
Consequently, the use of tumor necrosis factor (infliximab , adalimumab, etanercept, and golimumab) in combination with newer agents which target interleukin (IL)-12 and IL-23 (ustekinumab, UST), a4b7-integrin (vedolizumab, VDZ) or a4-integrin (natalizumab), has become an increasing area of interest in patients with disease that is not responding to treatment.
According to a systematic review looking at the efficacy and safety of DTT, “There is an urgent need to optimize treatments for patients” so that they have a better chance of remission, which unfortunately remains unachievable for a large number of people living with aggressive IBD. More research is needed to evaluate what the optimal drug combinations are, as well as dose and frequency to limit the burden of side effects.
The DUET trials are looking at people with Crohn’s disease and ulcerative colitis, much like the VEGA study, to compare the effectiveness of golimumab + guselkumab versus either drug alone. Interestingly, in this study, golimumab and guselkumab are combined in a single medication, so even though there are two active ingredients, it is delivered like a single drug.
“If we limit our discussion to combinations of modern advanced therapies, the combination of an anti-TNF and either vedolizumab or an IL-23 holds the most promise,” Dr. Targownik says. ”The other combination that we are seeing more is combining a JAK-inhibitor with an anti-TNF for people with acute severe UC, where the JAK-inhibitor is used in addition or in place of a corticosteroid trial.”
Personal Experiences on DTT
I’ve lived with Crohn’s since 2005 and luckily have been on the same biologic since 2008. I ran an Instagram poll that asked, “Have you been on dual-targeted therapy for your IBD?” Of the 320 people who responded, 40 percent said “Yes”, and 60 percent said no. Here are some scenarios they share:
Candyce has managed her Crohn’s with infliximab (Inflectra) and azathioprine since 2020. A 10-day hospital stay led her to dual treatment therapy after she received the recommendation from both her rheumatologist and her gastroenterologist. “My GI wanted to try to wean me off the azathioprine in 2022 after a clear colonoscopy, and I flared to the point of her wanting to hospitalize me,” she says. “But I managed to gain remission with prednisone and getting back on azathioprine, along with increasing my Inflectra dose to every six weeks instead of every eight.”
Risankizumab wasn’t doing the trick on its own to control Brad’s IBD, so his GI added 28 days of Rinvoq as an alternative to prednisone. He says, “This really worked wonders. Being on both risankizumab and Rinvoq put me into biochemical remission in less than 60 days.”
Samantha’s daughter, Eloise, was on tofacitinib and vedolizumab prior to her colectomy.She shares that more families are talking about dual therapy options. “The major issue is getting these medications approved from insurance, especially for pediatric patients. Our doctor was able to get us samples of Xeljanz from a local adult gastroenterologist because insurance would not approve it.”
Kate currently takes vedolizumab and upadacitinib to manage her IBD. Previously, many biologics failed her and vedolizumab was the only one that worked, but it did not address her perianal disease. “The Rinvoq is beginning to work,” she says. “However, I will say it caused awful acne (which I’m now on medication for). I’m not out of the woods yet, but I am functioning again, and I can tell that two medications are working on what needs to be healed.”
Courtney has been on Remicade and Azathioprine since 2020, prior to that she was on Humira and Azathioprine. She says, “I had no reservations because I was sick and willing to accept any option that might bring relief. My doctor explained to me that Azathioprine helps prevent antibodies to biologics. Regular blood tests monitor for more serious concerns.”
Along with her Remicade infusions, Lauren takes methotrexate orally each week.I don’t love it to be honest. I feel much more fatigued and nauseous with methotrexate added into the regimen.”
Initially, Danielle was put on azathioprine when she was on Remicade to prevent antibody formation and to help keep trough levels high. She explains, “When Remicade wasn’t working and I switched to Stelara, we decided to keep the azathioprine on since it didn’t give me any noticeable side effects. I have had some liver abnormalities with the azathioprine. So, I’ve had to have blood work and even an MRI of my liver to make sure everything is ok (it is). Now that I’m in remission with Stelara, my doctor gave me the choice of coming off the azathioprine, but I wanted to keep it on because I haven’t been in remission so long.”
Cait receives infliximab infusions, and she takes azathioprine simultaneously. “So far, I’ve noticed a massive difference in the healing of my perianal Crohn’s.”
Katie manages her IBD with Skyrizi and methotrexate. She says the combination makes her fearful at times. “I feel like it is a lot for my body to handle, and I have never been able to tell if that is a true feeling or something that stems from the thought of it. I also want to get off methotrexate within the next year or two to prepare my body for pregnancy. But this combo has provided me with full remission and the best I have felt in years.”
Final Thoughts to Consider Before Trying DTT
It’s important to discuss whether DTT could be for you with your specialized IBD care team as DTT comes with its fair share of risks and considerations. Combining medications can increase the risk of adverse effects, including serious infections due to greater immune suppression. Also, getting dual therapies approved through insurance can be complicated, making the cost and accessibility an issue for patients.
“It is challenging to get coverage for patients to use more than one advanced therapy at a time,” Dr. Targownik says, but not impossible. “Often if a patient has another autoimmune disease, I can get one medication approved for the IBD, and then the other for the other autoimmune disease like rheumatoid arthritis.”
The Takeaway
The effectiveness of combination strategies in IBD has been demonstrated in various studies, but these decisions need to be made on a case-by-case basis, considering your personal disease severity, response to previous treatments, and overall health status. If you are struggling with getting your IBD under better control with one therapy alone, speak to your IBD physician about other options.
There’s a BIG advancement that was just unveiled this week regarding nutrition and IBD. Nutritional Therapy for IBD, a non-profit dedicated to improving the lives and health outcomes of patients with Crohn’s disease and ulcerative colitis through evidence-based adjunctive nutritional therapy, launched their The IBD Nutrition Navigator™ to the public yesterday.
It’s a project that’s been in the works for two years and it’s the first nutritional tool of its kind! This FREE resource allows patients, caregivers, and healthcare professionals to work together to find the best nutritional approach on a personal level. This week on Lights, Camera, Crohn’s we hear from Kim S. Beall, Pharm. D., co-founder of Nutritional Therapy for IBD and Dr. Ashwin N. Ananthakrishnan MD, MPH, FACG, AGAF. These two, in collaboration with dozens of healthcare providers, designers, patients and volunteers, made this resource a reality for the IBD community.
What is the Nutrition Navigator™?
The design was led by Dr. Ananthakrishnan, Harvard graduate, Director of the Crohn’s and Colitis Center at Massachusetts General Hospital and one of the top GI clinicians.
“The IBD Nutrition Navigator™ is a groundbreaking algorithm-based tool designed to assist healthcare providers and patients in determining a personalized approach to using nutritional therapy alongside medication to optimize care,” he says.
“The tool is based on discussions that Dr. Ananthakrishnan has with his patients about nutrition and how it can be used in conjunction with medications and surgery to improve health outcomes. The IBD Nutrition Navigator™ is interactive and walks providers and patients step by step through six questions to assess not only the patient’s individual disease state and goalsbut also their interest in resources for nutritional therapy,” explains Kim.
The tool is designed for healthcare providers and patients to use together in shared decision making. Once completed, the tool recommends the best fit for an evidence based nutritional therapy. These recommendations are geared 100% to the individual based on how they answer the questions. As we all know, there is not a one-size-fits-all answer when it comes to IBD nutrition, and the recommendation is never nutrition vs medication. It’s using nutrition as another tool alongside medication and other therapies.
The inspiration behind the IBD Nutrition Navigator™
Dr. Ananthakrishnan, an esteemed member of Nutritional Therapy for IBD’s medical advisor board, is the inspiration behind the IBD Nutrition Navigator™.
“He discusses nutrition with his patients and uses nutritional therapy alongside medication as part of his regular practice. “What should I eat?” is the most common question for patients after an IBD diagnosis. But because every patient is different, there is not a “one size fits all” answer to that question,” says Kim. “Weeding through the abundance of nutrition information available can be confusing and time-consuming. Dr. Ananthakrishnan felt that we should provide more guidance to healthcare professionals in a simple, evidence-based, clinical manner. And thus, the idea for the IBD Nutrition Navigator™ was born.”
A closer look at nutrition and IBD
Nutritionaltherapies used alongside medication and/or surgery can help manage symptoms, aid healing, and reduce inflammation in IBD patients.
“For a long time, it was thought that diet didn’t even matter when it comes to managing IBD. We now have growing evidence that suggests that food does indeed matter as both a risk factor and a therapeutic option,” says Kim. “Patients struggle, however, with the abundance of nutritional information AND misinformation available. They may want to incorporate nutrition into their IBD management but don’t know where to start.”
Another very prevalent struggle is malnutrition. Patients are often afraid to eat new or certain foods for fear that those foods may cause pain or other symptoms. I know in my nearly 20 years living with Crohn’s disease I was considered malnourished during my initial diagnosis and hospitalization and was watched closely when I was losing weight unintentionally prior to acute flares in the past.
At a baseball game with my brother days before my Crohn’s disease diagnosis in 2005. Little did I know I was malnourished here.
Cool features of the IBD Nutrition Navigator™ to highlight
Years of planning went into the development of the IBD Nutrition Navigator’s clinical algorithm, so the information you will find on the tool is all evidence-based and thoroughly reviewed by medical advisors.
“There are so many thoughtful features of this practical tool. First, while the development of the IBD Nutrition Navigator™ was quite complex, the result is a very straightforward, simple-to-use, interactive questionnaire. Because the tool is so concise, it can be easily used during a regular appointment with a healthcare provider. Two of the six questions gauge the patient’s interest and resources in using nutritional therapy. These questions evaluating the feasibility of and readiness for change are what makes the tool particularly unique and comprehensive. As patients and healthcare providers progress through the IBD Nutrition Navigator™, the suggested nutritional approaches appear on the screen and will adjust in real time. You can see how your answers to the questions may modify the dietary options.” says Kim.
Finally, once the recommended nutritional approach is selected, there are links to extensive resources from Nutritional Therapy with IBD to help you learn about incorporating that approach and even a recipe database with diet-specific dishes.
Tips for taking the information learned and discussing it with a registered dietitian/GI
The IBD Nutrition Navigator™ is designed to facilitate nutrition conversations between patients and healthcare providers, including registered dietitians who play a significant role in this process.
“Before using the tool, patients and healthcare providers must acknowledge that a full clinical assessment—including screening for malnutrition and eating disorders—is the necessary first step. The addition of or changes to nutritional therapy should always be made through shared decision-making between the patient and healthcare provider,” adds Kim.
Patients or caregivers interested in nutritional therapy can print this flyer to take to their provider. The QR code provides a link to Nutritional Therapy for IBD’s website where you will find the IBD Nutrition Navigator™ and many other evidence-based nutritional resources.
Final Thoughts
The IBD Nutrition Navigator™ aims to provide healthcare professionals and patients with a tool that helps us choose the right, individualized nutritional therapy to use alongside medication and/or surgery and optimize care. Once you discover the best nutritional fit, patients can gain confidence in their food choices and ultimately improve their overall health and healing.
I wish when I was diagnosed with Crohn’s in 2005 that I had a tool like this at my fingertips. A dietitian (who was not well-versed on IBD) told me I would never eat raw fruit or vegetables again and it felt like doomsday. I was overwhelmed, and at age 21, days after being given a chronic illness diagnosis, that advice devastated me. Our community is incredibly fortunate to have a tool like this so we can feel more in control and more empowered to make appropriate dietary changes that are personalized to our care and tailored to fit our ever-changing treatment plan. In addition to the IBD Nutrition Navigator™, this volunteer-led organization provides a wealth of information and resources about nutrition and IBD on its website. Click here to learn more.