This post is sponsored by Corra. All thoughts and opinions shared are my own.
For as long as Elya Lane can remember she had signs and symptoms of a health condition. It wasn’t until college that she received her official diagnosis of Ehlers Danlos Syndrome and POTS. She says her poor health started to spiral with other comorbidities popping up, the worst of which was chronic UTIs that left her whole body in crippling, burning pain and weak from the antibiotics. Elya’s personal journey with chronic illness inspired her to create the Corra App. This week on Lights, Camera, Crohn’s we learn about how she made her dream a reality and how she hopes to improve peoples’ lives.
The breaking point
“I was constantly plagued with fears of antibiotic resistance, infection complications, or complications from long term antibiotic use. I got to the point where I was so sick that I wrote letters to my kids and my family in case something happened to me. I started tracking all our passwords and making videos for my husband on where our important files were, how different things were stored, all the kids’ data, etc. While I tried to face this potential outcome bravely, I was devastated imagining my kids growing up without a mom,” said Elya.
As she navigated these dark and daunting days, the despair caused her to think about how she could fight back and regain control of her health.
“I started to religiously track my health in journals before transferring to Excel spreadsheets. I was so frustrated by how exhausting and impossible it felt to crunch that much data, so I turned to searching for a symptom track and correlative software to help me. I downloaded and tried every single one I could find – but none met my needs. Some even gave me back faulty data which made me angry. That’s when I decided to create a solution myself,” she explained.
In 2020, after losing access to all her healthcare management tools, and with her health declining rapidly, she decided to create Corra.
The meaning of Corra
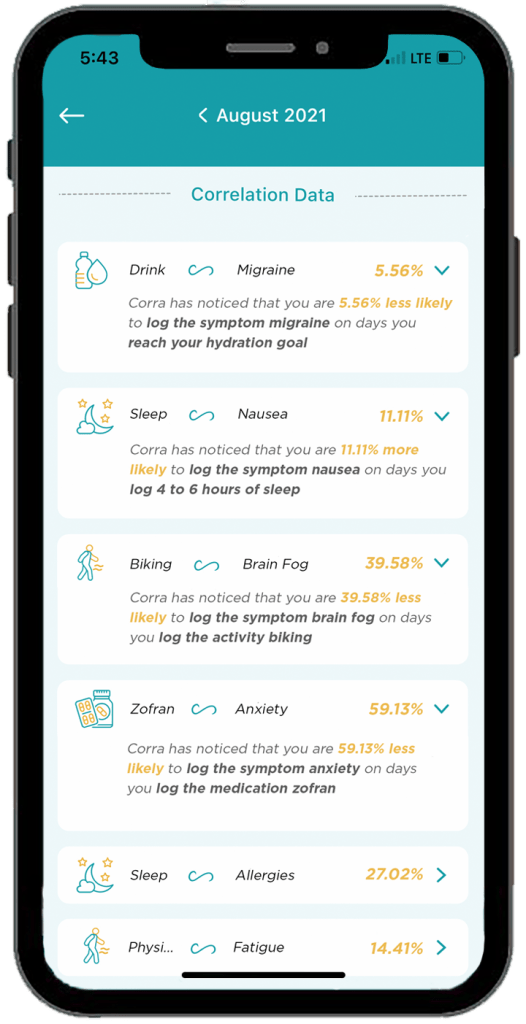
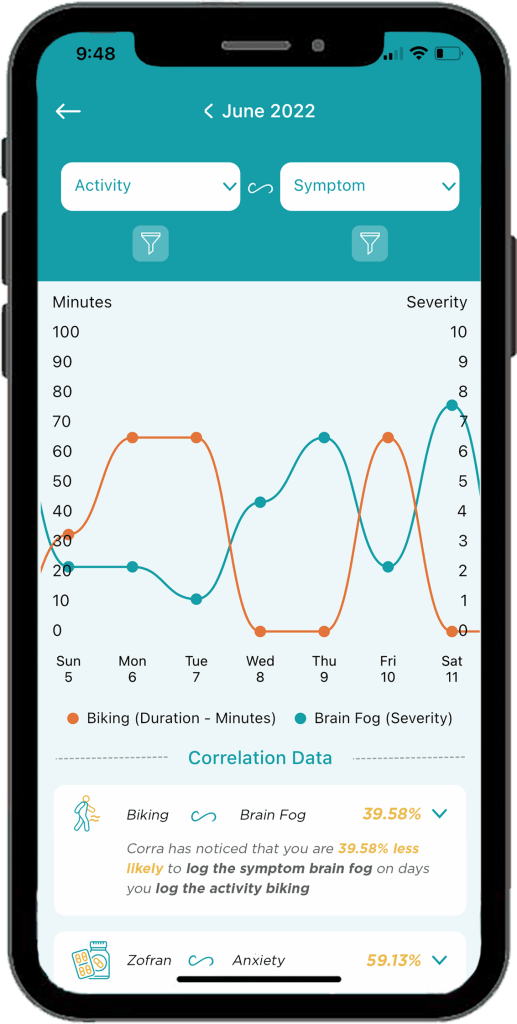
There are quite a few chronic illness apps on the market, some that even attempt to offer correlative insights. Corra is short for correlations. Elya wanted to identify correlations in her health so that she could find her triggers and optimize her lifestyle.
Here’s what sets Corra apart from other chronic illness apps on the market:
The algorithm was custom built by Corra’s chief data scientist, Simeon Wilson, who has a master’s in quantitative economics from UCLA. “We are not aware of any software that exists that compares to what Corra is currently offering with our correlative algorithm.”
Corra was designed by individuals with chronic illness. “Not just me! While the idea and original designs are all mine, we brought on more than 200 beta testers with various chronic illnesses to provide their feedback and help us tailor the app to the needs of the chronic illness community. Even now, we continue to rely on the insights and feedback from the community to enhance and adjust the app. I want Corra to always be designed by and created for our community.”
We correlate with nutrition in an accurate and helpful way. “I believe nutrition plays a massive role in our health so one of our key focuses with our algorithm was to be able to correlate seamlessly with nutrition inputs.”
Corra does not sell user’s data. “We don’t scrape your data from your device or browsing history, we don’t use your data to sell you anything, we don’t share your data with third parties. Your data is yours alone. As an individual with a chronic illness who often feels more like a commodity than a person, making sure people can receive personalized insights into their health without signing away their privacy is incredibly important to me.”
Corra’s bells and whistles to check out
The ability to track health data in one place without having to use five different apps to log information. “My favorite part of Corra is of course the correlations, because getting detailed insights like that about my health is equivalent to having a team of data scientists run extensive tests on my health and provide me reports. It’s life changing to be able to learn about my health overtime and create a custom-built lifestyle that caters to my future.”
Discovering positive and negative correlations. “You may receive insight that something has x% chance of increasing or decreasing a symptom. I think being able to get data on the things that are helping is just as important as being able to identify triggers.”
The ability to log appointments, download PDFs of your data to share with my doctor, track medications and supplements, track mood and stress levels, etc. “I’m also extremely excited about all the upcoming integrations we have in the works! Soon we will be connected to Fitbit and Apple Health with Garmin, Cronometer, Weather data, and hopefully Oura coming shortly after! Over time we will continue to integrate with as many devices and apps as possible so users can have all their data in one location!”
A promising future
Elya says being able to learn what foods, activities, supplements, and medications help or cause symptoms has enabled her to have a much better understanding of how best to manage her health conditions.
“I’ve been told to go vegan, cut out red meat, don’t eat dairy, sugar, gluten, eat paleo, try a carnivore diet, go vegetarian, and try cutting out leafy greens… what I found with Corra is that I didn’t need to make these drastic nutrition changes, I only needed to cut out some foods in each of those categories. For example, I discovered that I have a high trigger correlation with ground beef. I can eat steak and other red meat, but not ground beef. Similarly, chicken thighs are a trigger for me, but chicken breast is not. Same with gluten, there are some gluten products that are triggering for me, but not all gluten triggers me. Being able to identify exactly which foods to cut out, rather than willy nilly cutting out entire food groups or going on drastic diet changes, has been an absolute game changer.”
Elya has also discovered that cold and flu medications like Mucinex are major triggers for her. This helped her realize why she would get a horrible flare a few days after coming down with a cold or flu.
“Now, I try to manage my colds and flus with other medicine to try to prevent the flare on top of the cold. It’s also important to note that I’m not cured! I have to manage my diet and my activities and my supplements every day. The difference is, I’m no longer throwing shots in the dark, I now have the information I need to manage my condition to the best of my ability.”
Information really is power, and it has given Elya control over her life and reduced her anxiety. Because of Corra, she is now coming up on two years without the need for daily antibiotics. It’s been over 2 years since she visited the emergency room.
“I’ve found that medical providers are far more willing to accept unbiased data from an algorithm than trust my verbal expression of my experience, so in that way Corra becomes my advocate and backs up my statements,” said Elya.
She says her health conditions have caused her to go through depression, isolation, and hopelessness. But her hope for Corra is two-fold.
“First, I believe it can help others identify their triggers and optimize their life so that their conditions can become more manageable, but I also hope that Corra can be a beacon of light for those struggling to see they are not alone. There are so many steps between the start of symptoms and any kind of treatment let alone cure (depending on if your condition is even curable)… and I want to be the one that goes into the trenches and helps people who are suffering the most. So many people in the chronic illness community get forgotten or left with “your test results are normal” when they know there is something wrong with them. I want to create a company that comes alongside them and lifts them up and allows them to have their voices heard.”
Downloading Corra
You can download Corra directly from the App store or the Android playstore. There is a free version as well as premium access. The premium version is $7.99/month or $24.99 if you enroll for a 6-month subscription. Elya is looking for Corra Insiders who are interested in getting free access to the app. By joining the Insiders group, you get a first look at upcoming features. This provides you the opportunity to share feedback on what you do/don’t like or would like to see improved or added in the future. Sign up for the Corra Insiders program here.
It’s the first of its kind program dedicated to training dietitians about IBD-focused nutrition. Cedars Sinai Hospital in Los Angeles, California launched its IBD Dietitian Apprenticeship in July 2023.
Registered IBD dietitian Stacey Collins was the first registered dietitian to be selected, participate, and complete the program. I’ve been amazed at all she does for our community and been excited to dig deep and learn what her key takeaways have been from this experience. As someone whose lived with ulcerative colitis since 2012, when she was 21-year-old, Stacey has a unique perspective and approach.
This week on Lights, Camera, Crohn’s we’ll hear about her firsthand experience and why this Apprenticeship program is just what our community needs. The hope is that registered dietitians who participate in the program can take their knowledge from the experience and be able to plug themselves into an IBD Center to build and strengthen an IBD program.
Going up against lack of education and funding
Stacey tells me there is little to no education that they receive in dietitian training on how to do nutrition specific to gastroenterology, much-less IBD, and she says this Apprenticeship program fills the gaps and then some.
“So much of what I learned was through self-study before this program. But in the Apprenticeship, whether I was part of the team rounding on patients in the hospital, or seeing a newly diagnosed patient in clinic, or sitting on the floor with a 3-year-old patient asking about their Paw Patrol toys, I left every encounter feeling that special kind of discomfort and gratification that comes with growth and learning. This was truly a hands-on learning experience from many different sides of the IBD rubix cube, and I’m so grateful I wasn’t learning it all by reading slides from a PowerPoint and taking a test- who learns that way anyway?!”
Addressing the unmet needs
Once registered dietitians complete the Apprenticeship they can work in an academic center or a private practice that values IBD nutrition and has the financial backing to justify the need for a dietitian.
“There are institutions and people in places of power who are advocates for the profession of IBD RDs, and this work is simply impossible without them. IBD RDs have the potential to support patients throughout their journey as an accessible, consistent member of their multidisciplinary care team. Unfortunately, a lot of this potential is systemically handicapped by the lack of funds: RDs are investments rather than quick money-makers for a clinic without physician advocates and creativity, and we NEED people at institutions to see our value,” said Stacey.
The main programmatic goals are to provide a structured, supervised training program for dietitians to learn a model wherein dietitians work together with physicians and advanced practice providers for the care of adults and children with IBD.
Places do exist (and many are coming) that support this multidisciplinary model of healthcare delivery, but there’s such an unmet need, especially for people who don’t have access to these IBD centers. The hope is for this Apprenticeship program to fill the gaps of that unmet need by signaling to physician advocates at these institutions that a nutrition professional with intense training and experience DOES exist, ESPECIALLY for more complex patients who have IBD.
So much to be done for patients Registered IBD dietitians can assess people for malnutrition regardless of their stage of IBD, which is common even in remission and linked to poor health outcomes, along with so much more. Stacey says:
We can help catch micronutrient deficiencies or insufficiencies that many other care team members might miss, and we can correct and monitor them.
We can help patients experiencing food insecurity find ways to nourish themselves within their budget constraints with an eye toward prevention of other comorbidities.
We can help nutritionally prepare patients for surgery.
We can help patients in need of a medical or therapeutic diet intervention find a way to make it a sustainable intervention for themselves.
We can help patients nourish themselves using a whole-person approach, whether they are juggling multiple diagnoses, starting a new job, headed off to college, or too tired to eat: we have tools for helping patients feeling like they can handle it all
We can help prevent re-hospitalizations from small bowel obstructions or dehydration by giving patients IBD-specific tools for understanding their body.
We can save physicians time by inheriting questions about nutrition and/or supplementation regimens, and we can personalize these for each patient.
We can even show GI or IBD Fellows what it’s like to feel spoiled working with an IBD dietitian, and hopefully they’ll advocate to hire one of us wherever they make their final clinical stop
She’s confident IBD dietitians can make nutrition an accessible tool when it so often feels inaccessible with IBD!
Stacey’s top apprenticeship moments that left a lasting impression
Six months is a long time to pick up your life, move to another state temporarily, and fine tune your knowledge and expertise on nutrition and IBD. Here are the key takeaways Stacey says she took away from the experience:
1. Patience with patients is key; everyone is on their own timeline.
“I got to see a doctor celebrate with a patient who finally quit smoking cigarettes for good. After that encounter, he told me that he had been pleading with that patient for 20 years to stop, but he never blamed the patient for having a tough time stopping. He really was empathetic to the fact that they had a lot going on, and he knew they’d get around to it once life allowed. That was really enlightening to see: patients really are doing their best. How can I support them, especially if their timeline looks differently than the expectations that I have?”
2. It doesn’t have to be all-or-nothing; don’t let perfection be the enemy of good nutrition.
“One day I was with Erin Feldman, RD (Cedar’s Pediatric GI and IBD RD). She was listening to a worried mom talk about how she didn’t want her kid to eat sugary cereal, but that’s ALL they would eat for breakfast: it was the sugary cereal, or it was nothing at all. The child was exercising their choice autonomy and exploring what that looked like around mealtimes, and it was a challenge for the parents. Erin had a rapport established with the family, and I could see that they really trusted her. Plus, Erin is a mom, too, so she speaks the same first language as parents, and she really empathizes with the fact that many IBD parents are blamed for their child’s symptoms or disease. She truly met the parents right where they were at that moment.”
“Instead of focusing on the PERFECT breakfast with beautifully-balanced macronutrients and color that the child certainly would refuse, she said, “What if you just added PLAIN Cheerios and a couple of raspberries to their sugary cereal, that way they’re getting some antioxidants from the berries and a more diverse source of grains into their breakfast?” It was TOO easy, and the parents were like, “YES. We can do that.” and just like that: not a perfect solution, but a practical intervention that would work for where the child is right now.”
And that’s the power in having multiple touchpoints to a dietitian: next time they see the doctor again, they’ll see Erin, too, and they can make more adjustments for how life is being lived around food at that stage, too. So often people have the ambitious idea of going from zero to specific carbohydrate diet (SCD) all in one encounter, and the reality is that often multiple conversations and coordination of resources are needed, and meeting patients where they are looks different for everyone.
3. Nutrition interventions can be hard, and multidisciplinary support really is key.
“So often as dietitians, it’s easy to get stuck in the weeds of research and to get excited over interventions that have promising outcomes. This happened with a patient needing Exclusive Enteral Nutrition, but ~5-7 days into it, they were uncomfortable, and they really missed food. I was able to have a conversation with the patient alongside their doctor in the same room, who patiently reiterated our rationale behind the intervention and said, “not if it compromises your mental health. Let’s stop it if your brain is telling you we need to stop- we need to respect that. You should be proud that you tried this, and now you know!” And I could tell the patient was so relieved to have reassurance from their doctor that no matter what THEY chose for THEIR body they’d be supported by their doctor and by their dietitian. It really does take a team.”
4. GI Doctors REALLY do not get exposure to solid nutrition in their training
Kelly Issokson, MS, RD (Clinical Nutrition Coordinator, Course Director: DIET Executive program, Apprenticeship Director) arranged for Stacey to lead a learning session with the GI Fellows at Cedars, and in a room full of some of the smartest and most compassionate clinicians.
“They wanted to know all about the different nutrition interventions that we can recommend for patients. It felt like they had been rewarded for being the best of the best all by themselves their whole lives, and now they had an opportunity to learn more about how to collaborate effectively. They were all so enthusiastic.”
Stacey noticed after that session that the GI Fellows felt comfortable texting her while on rounds if she wasn’t there to ask if she’d stop by a patient’s room, or they’d text to ask about B12 supplementation after remembering to screen for a deficiency.
“They really understood the value that IBD RDs bring, and it’s not because I’m a great public speaker (I’m really not); it’s that they had this additional exposure to working with a dietitian with specialized training. This really made everything click for me: doctors don’t always know the right questions to ask patients about our nutrition needs, because most of them haven’t had the education OR the exposure to team members with the expertise to be truly helpful for patients. Working in silos keeps patients isolated, and I’m hopeful that the GI Fellows, when/if they leave Cedars become physician advocates to ensure that their patients have access to an IBD experienced RD.”
Plans for the future
When Stacey completed her Apprenticeship this winter, she did not envision returning full-time to her online private practice. She thought she’d start working at an academic institution, because the purpose of the program is for the dietitian to seamlessly integrate into a multidisciplinary GI care team.
“I am still holding out on hope that one day I could have both (but I’ll never give up my private practice- I love it so much). Truthfully, I’m thrilled to be back with such a passion for teaching patients how to implement some of the skills that I’ve learned into their own life, plugging it into their existing care teams, even if I’m on my own in private practice. I already helped patients through perioperative nutrition before this program, but now I’ve got some RICH resources to help make IBD surgery and nutrition really make sense for patients now in a much clearer way,” Stacey explained.
She’s able to take the research that they did from the perioperative IBD Nutrition program that exists at Cedars and put it into practice with her patients, and it’s a bit of a full-circle moment for her, having lived through IBD surgery with limited support.
“I’m a much better listener than I was before this program, a skill I learned from Kelly Issokson, MS, RD (Clinical Nutrition Coordinator, Course Director: DIET Executive program, Apprenticeship Director). Additionally, I’m more practical in my approaches and meeting patients where they really are, too, a skill I learned from Erin. I’m working on some ways to expand IBD RD accessibility, too. I’m a much more confident advocate on behalf of my patients now, too.”
Advice for the newly diagnosed
If you’re reading this and you or a loved one was recently diagnosed with IBD, ask your GI doctor to hire an IBD Dietitian. Stacey knows this doesn’t exist in most places, and as a patient, she understands how silly it is to constantly be burdening patients with requests. But the field of IBD Nutrition exists because enough patients asked, “What can I eat?” and enough doctors paid attention to it to be documented research. This is the next piece of the puzzle.
If your care team provides a registered dietitian who doesn’t specialize in IBD, that’s not going to cut it. Be assertive in asking your GI office to hire an IBD Dietitian, or invest in training their Dietitian, if they really want to help their patients.
Stacey advises patients and caregivers to stay off online forums. There’s so much food fear there, and life is bigger than that. Lastly, she advises reaching out for help. Even if Stacey may not be a good fit for you, she’s happy to provide patients with other RDs that she’d enthusiastically see, because an informed decision is a good one.
During her Apprenticeship, Stacey chose to do a research project to examine the effects of malnutrition and perioperative nutrition supplementation on surgical outcomes in people getting IBD surgery, whether that be for j-pouch, permanent ostomy, lysis of adhesions, or a resection.
“We had a small sample size (n=25). Regardless, we found that perioperative nutrition supplementation had a statistically significant impact on decreasing the length of stay, meaning that greater adherence to the nutrition supplementation protocol was associated with a shorter time spent in the hospital. Regardless of nutrition status (malnourished or not), everyone seemed to benefit from the nutrition supplementation protocol that we recommended for before and after surgery.”
Stacey is hopeful that more research with an even larger sample size will help inform these results so that this can be a resource more widely available for patients!
The future is bright
“If I dared to dream about what this could look like in the future, the closest possible model in existence is at UCLA under Dr. Niru Bonthala who is the Director for Women’s Health in IBD. Basically, I see the RD’s role evolving to cover every nutritional aspect of IBD with specialized knowledge to support patients in each life circumstance: from surgical prehabilitation to home nutrition support (TPN or EEN) and transitioning back to eating; to the overlap of eating disorders; to fertility and perimenopause; from anywhere along the spectrum of LGBTQIA+ care and/or transgender care; from peds transitioning to adult care, and even adults to aging adults; even athletics and/or eating disorders.”
There’s a rich opportunity within all these Venn-diagrams for a specialist interest and training to exist in IBD Nutrition, and this learning opportunity exists at Cedars.
“I’d also love to see the RD in an outpatient clinic even able to do community outreach: teaching basic cooking skills, procuring menu items for their medical diet (and beyond), and even showing patients and their families what this could look like by partnering with local food banks. Again, this is just me dreaming here in a world that I think should exist for people who have IBD and for RDs who are trained in IBD Nutrition,” said Stacey.
The current IBD Apprentice Yi Min Teo (@herbsandfood) came from both clinical and private practice backgrounds like Stacey. Yi Min will finish her training in July 2024. The program is supported by a grant from Leona M. and Harry B. Helmsley Charitable Trust.
In addition to dietitians wanting more IBD nutrition education, there’s also an Executive Program for MDs/DOs, APPS, and includes both virtual and in-person learning opportunities. You can apply here.
Did you know within the next decade, one in three IBD patients will be over age 60 and that right now, adults over 60 make up the greatest portion of the IBD population? As someone who was diagnosed with Crohn’s disease at age 21, who is now 40, I’ve started to think more about what managing and living with IBD will look like as I continue to age. Managing IBD in older adults is complex and requires considering each person’s individual risk of complications and co-morbidities.
This week on Lights, Camera, Crohn’s a look at the research that’s available and what we can expect as an aging patient population. Before we get started, it’s important to note there are two groups—adult-and-pediatric onset IBD who are getting older and then a group of people who are diagnosed later in life (after age 60) referred to as “elderly-onset IBD”. Every review I saw online uses age 60 as the benchmark to differentiate these two groups. Elderly onset makes up about 10-20% of patients who are newly diagnosed with IBD.
Unfortunately, there’s limited data and studies that have followed patients for 20-plus years, so we don’t know a ton about how aging impacts patients who were diagnosed as pediatrics or as younger adults compared to those who are in their later years. While there’s a well-known belief that IBD can “burn out” as we age, meaning that symptoms for some quiet down, that is of course not the case for all.
Considerations when treating IBD in older age
Have you ever talked to your GI about how your IBD will be managed as you age? I know I haven’t. I feel that there’s so much to focus on in the “now” it can be overwhelming to think about how we’ll take care of ourselves 20-40 years from now! As we surpass age 50, there are important discussions to be had.
What patients and providers need to consider:
Risk of disease and treatment related complications
Tolerability of IBD therapies, which is unique to each person’s personal experience
Drug metabolism and how it alters with aging
Body composition changes which include a reduction in total body water and an increase in total body fat.
The delicate balance of disease-related risks vs. treat-related complications.
Risk of adverse events from medications vs. benefit shift (higher rates of infections, malignancy, and drug intolerance).
Given these factors alone, the way in which IBD is managed in older age isn’t as clear cut as when we’re younger. With both thiopurines and biologics, older patients are more likely to discontinue treatment. Older adults may value symptomatic remission (and quality of life) more than mucosal healing.
This study entitled, “The elderly IBD patient in the modern era: changing paradigms in risk stratification and therapeutic management” states, “Despite elderly onset IBD presenting with a less extensive or aggressive phenotype than adult-onset IBD, its disease course is not necessarily more benign. In Everhov et al.’s work, 22% of elderly onset Crohn’s patients underwent surgery by 5 years, although the rate was lower in UC patients (6%). Similarly, the cumulative probability of surgery at 10 years was 32% in Crohn’s patients compared with 8% in UC in another population-based study.”
According to an article in Time called “The Connection Between IBD and Aging”, whereas IBD was once thought as a disease with two spikes in onset—20s to 30s and 40s to 50s—doctors are learning there is a third spike that begins later in life. For those of us who are diagnosed when we are younger, our bodies have lived with decades of damage the disease has caused, often we’ve had surgery, been on medications with serious side effects, and ongoing flare-ups for much of our lives. For those who get IBD after 60, rather than seeing damage in various parts of the intestinal tract, more activity is seen in the colon.
The article goes on to say, “It’s no surprise IBD causes chronic inflammation, and so does aging. So, as we age with IBD, we’re at greater risk for inflammation linked-health issues, including cardiovascular disease, cancer, hypertension, chronic obstructive pulmonary diseases, chronic kidney diseases, obesity, skin issues, blood clots, arthritis, dementia, and skeletal muscle loss.”
Comorbidities and IBD
According to the Crohn’s and Colitis Foundation, people who have Crohn’s may also have a better quality of life as they age, partly thanks to modern medications and less use of steroids long term, which can trigger bone loss and cataracts over time, among other symptoms. Steroids are the most dangerous medication we have to treat IBD, sometimes of course they are necessary, but long-term use should be avoided at all costs.
People over 60 are more prone to infections and have a greater likelihood of being on medications for additional health conditions. They also often have visual, cognitive impairments, risks for falls, and surgery complications.
Underrepresentation in clinical trials
One of the main reasons we lack data about IBD in older age is because this population of patients is often excluded from clinical trials. This study from The Lancet Gastroenterology & Hepatology says, “A deeper understanding of biological and functional age, dynamic risk stratification strategies (including frailty-based risk assessment tools), comparative effectiveness and safety of current therapies and treatment strategies, and shared decision making to inform treatment goals and targets is needed to improve outcomes in older adults with IBD.”
A Crohn’s and Colitis Foundation study found that clinical trials for biologics only included 1% of people over age 65. How can patients feel safe about being put on biologics when there isn’t research to back up the safety and efficacy of these heavy-duty medications when they reach that age bracket?
As far as menopause goes, we still don’t know much yet about how this impacts women and the role it plays in disease course. Some small studies have found a modest protective role for estrogen-replacement therapies for IBD activity. But there’s more research needed in this area. According to the Crohn’s and Colitis Foundation menopause may begin earlier in IBD patients, but this does not appear to have any negative effect on disease activity or progression. Women with IBD are at greater risk for osteoporosis in menopause, this is why it’s so important we’re proactive in younger age by getting bone density tests and taking calcium and vitamin D supplementation (if labs show you’re deficient). I have taken 50,000 IU of Vitamin D once a week for years to help combat bone loss and this past year I started seeing a Bone Health Doctor to keep a close eye on my osteopenia. My GI told me during my clinic visit this month he wants me to take 2 Tums a day for added calcium.
As far as men, aside from methotrexate, IBD medications do not usually cause erectile dysfunction. Ileal pouch anal anastomosis (IPAA or J-Pouch) surgery, while sometimes associated with loss of sexual function, is not associated with erectile dysfunction. There’s also no known connection between IBD and prostate cancer.
Patient inputfrom those who are 60-plus
Patti says her age has changed how she manages her IBD.
“I’m 60 years old. Mostly, I compartmentalize social outing to 2 hours at a time. If I extend it, I’m exhausted and feel crummy for the entire next day or two. If there’s a situation where I know it will have to be more than three hours, I make sure to rest and eat less the day before, and then eat minimally until the last hour or so of the outing. This way, I don’t have to feel like I’m running on empty during the entire outing, and I can prepare to be home for whatever the food decides to do, in addition to the exhaustion and pain that I know are coming.”
Patti went on to say that she feels her Crohn’s brought on menopause sooner, but also that her Crohn’s may have masked menopause symptoms because she was used to low-grade fevers and sleep interruptions.
“I found out I was post-menopausal at 50 and I basically missed the transition (the symptoms). I took that as a win (ha), but I do feel like my body is older than my age. I can’t really explain why, but the constant inflammation, plus my body trying to resolve it—I believe it’s taken a toll on my aging. But recently turning 60 feels AMAZING. TO be sick since I was 8 years old and have fought my way to my sixth decade feels like I climbed a mountain! I’m proud of how hard I’ve fought all these years, while still thoroughly enjoying life, my marriage, my daughters, and my career!”
Heidi was diagnosed with Crohn’s at age 50 after years of being told she had IBS. She found out in July 2023 that she had a” severe Crohn’s reoccurance after 5 years on Stelara. Her options were Skyrizi or Rinvoq since she has a history of TNF inhibitors failing her. Even though Rinvoq had a slightly better chance of putting her in remission, her and her care team thought Skyrizi would be a safer option due to her age. Rinvoq has a warning regarding increased cardiovascular events, such as heart attack, stroke, or death in people 50 years or older, along with risk of blood clots.
“If I don’t respond well enough to Skyrizi, we will then try Rinvoq, but the safety profile seemed better especially for me being over 60, and that’s important to me. I also worry about what is going to happen when I retire and my medical insurance goes from commercial to Medicare! I think they often have a deductible that is much higher than commercial insurance.”
Heidi was also diagnosed with osteoporosis in her 50’s and took treatment for it for 5 years.
“My risk for fracture still increases as I age, so my GI ensures I have DEXA scans every 2 years.”
Brenda had diverticulitis for a few years, and beginning in December 2011 she started having other bowel problems. She went straight to her general practitioner, and he ordered a colonoscopy, which confirmed her Crohn’s disease diagnosis at age 63.
“After many failed medications, I had part of my colon removed and I had a temporary ileostomy. Unfortunately, I got an abscess which made me really sick and in 2015 I had more colon removed and the stoma was made permanent. Since that surgery, I’ve been quite well and basically get on with my life without any IBD medication.”
Brenda is now 75 and worries about getting sick again and needing additional surgeries. She also worries that as she ages that one day she may not be able to deal with her ostomy bag herself and that concerns her.
Keith has ulcerative colitis and his wife was diagnosed in her 20s with ulcerative colitis. Her IBD was under control for years until she was hospitalized 20 years ago. She underwent her first operation then and it was successful. Fast forward two decades and she flared and required additional surgery.
“She’s doing ok now, but both surgeries were a result of her bowel narrowing.”
Jody is on Remicade and is currently in remission. She started with colitis in her 20s and then her diagnosis shifted to Crohn’s in her 60s. She’s in her early 70s now. She’s tried several biologics and medications.
“Not sure when I started Remicade. I have tried a few before and they were either too expensive or I had issues with them. I am in the United States so our insurance is not easy. I also have taken Mesalamine for years for colitis, which has worked great but it’s another expensive drug, so the prescription was cut in half due to cost a few years ago.
Sherry hasn’t changed much in her 44 years of living with Crohn’s, but has more of a focus on an overall healthy lifestyle.
“I’ve gotten better at avoiding trigger foods and being more diligent taking necessary vitamins. I’ve always been active (weight training, golf, and skiing) and remain so if not more these days. The introduction of biologics has obviously been a game changer a huge benefit.
Jeff says gastroenterologists seem to believe you more as you age.
“As you get older, more things in your body are broken. It’s a balancing act as to what is most critical. You also start running into unknown territory for GI docs, as many treatments do not have much data, if any, for seniors. GI docs do seem to believe you more when you need help.
Kanchan is currently 74. She has had a J-Pouch since 1989.
“For the last 4-5 months I am making probiotic yogurts at home and the last month I started making Kefir. I’m hoping for good results.”
Sherri– “I was diagnosed with IBD in 2015 when I was 56. I’m tired of the whole thing. What’s going to happen when I can’t look after myself?”
Closing Thoughts
It’s important for us to work closely with our healthcare teams, not only gastroenterologists, but all specialists, to manage IBD effectively as we age. It is beneficial to check in with a registered IBD dietitian, as aging may affect the body’s ability to absorb nutrients. I often wonder if when my kids are in high school or college (my youngest is 2.5!), if I’ll play a little Russian Roulette and try going off my biologic. I’ve been in surgery-induced remission since August 2015 and if this continues (God willing), I think I will try. Right now, as an IBD mom of 3 kids (ages 6, 5, and 2.5), I don’t feel confident enough that I won’t flare and need to pull out all the stops I can, so I can be present and well for my young family.
There’s a delicate balance with each decision we make along the way and the best we can do is advocate for ourselves, be proactive and take measures now to be healthy, do our research, and stay as educated as we can about what’s coming down the pipeline for the IBD community as we age. By controlling inflammation in our younger years, we can help improve our future quality of life and prevent age-related symptoms.
It’s not surprising there’s stigma that surrounds gut health. Even though “everybody poops” it’s still a bit of a taboo topic, and don’t even get the general population to think about getting the dreaded colonoscopy. This is where the GH Foundation comes into play. Co-Founders, Dacia Heck and Kristin Lynn Grubehave both been personally impacted by gastro health in unique ways and their journeys inspired them to create a non-profit to help break down barriers and start critical, life-saving conversations.
According to the Crohn’s and Colitis Foundation, “patients with IBD appear to be at notably increased risk of colorectal cancer compared to the general population, with one recent study demonstrating a 7% colorectal cancer risk after 30 years of the disease. I had my first colonoscopy at age 21, which confirmed my Crohn’s disease diagnosis. Since 2005, I’ve had more scopes than I can count. I typically get a colonoscopy every year. While it’s not an enjoyable experience, it gives me peace of mind that I’m being proactive about my health. I’ll be getting my next scope in the coming months.
This week on Lights, Camera, Crohn’s we hear from Dacia and Kristin to learn more about their mission, the difference they hope to make, and how you can get involved and feel supported.
The personal connection
Until your gut starts causing health problems, chances are you don’t often think about it. Kristin was diagnosed at age 27 with Serrated Polyposis Syndrome (SPS), which is characterized by the occurrence of multiple polyps throughout the colon and/or rectum that can develop into colorectal cancer (CRC). She discovered this through a colonoscopy.
Kristin Lynn Grube, co-Founder of the GH Foundation
“My diagnosis has taught me to be my own relentless health advocate and speak up for myself. I continue to learn how to cope with SPS’s ongoing effects – emotionally, physically, and spiritually. Some days are easier than other days.”
Dacia lost her healthy, active sister from Stage IV colon cancer. Her sister was diagnosed at age 43 and passed away less than 4 months later.
Dacia Heck, co-founder of the GH Foundation.
“My sister’s diagnosis was a complete shock, as we didn’t have a family history of colorectal cancer and she was well below the screening age of 50 at the time of her diagnosis.”
The inspiration behind the GH Foundation
While Dacia and Kristin have different stories and experiences, they are both passionate about bringing important resources to the general public and are adamant about making gastrointestinal (GI) conversations not only more accessible, but also more mainstream, in order make the path to GI wellness and cancer prevention easier for others.
“We truly believe we can make a difference – one conversation at a time. As Kristin and I discussed where we wanted to focus our time and energy, we kept circling back to the “stigma” associated with GI diseases. That stigma often delays people talking to their family or medical provider about GI-related conditions. We decided the way we could make the biggest impact was to create GH Foundation and focus our mission on breaking that stigma,” said Dacia.
The GH Foundation’s main mission is to destigmatize conversations around GI, or gastro, health issues. 1 in 16 people in America will get CRC and 0 in 16 like talking about it. The GH Foundation encourages everyone to start the conversation. True prevention starts with educating the public on what is normal GI health and when to speak with a medical provider.
Discovering the loopholes in gastro health
As Dacia and Kristin did their research and spoke with different folks from all walks of life, they kept noticing that the conversations around gastro health have to start with a younger audience. Young adults in their late twenties to early forties are not discussing the importance of gastro health with their medical providers.
“We believe this is mostly due to the deeply rooted societal stigma surrounding gastro health. Given the uptick in early age onset (EAO) CRC, it may be too late to prevent a late-stage diagnosis once they qualify for screening. We want to focus on the very beginning and origin of it all – the conversation, whether it is with your family, friends, or network. Take that first step and reach out to someone, ask questions, make that list of symptoms you are experiencing, find out if you have a family history of GI diseases,” said Kristin.
While it’s intimidating, Dacia and Kristin guarantee that the first step will go a long way and may improve your quality of life, or even save your or someone else’s life.
“Our goal is to bridge the gap between the medical terminology and the general public’s knowledge about GI health. We are finding ways to make medical terminology and information accessible to the public. We encourage everyone to listen to their body, and to get the tools to empower them to speak up if they have issues,” said Dacia.
Taking their mission into action
The GH Foundation works to meet people where they are and find different ways to overcome the stigma. For some people, it’s learning about the basics of gastro health through an educational webinar, for others, it is hearing a survivor’s story and becoming inspired to take that first step.
“It’s connecting at a social gathering and finding a space where you can share your day-to-day challenges that you thought you were experiencing alone. Other times, we just want to have fun – we play GI trivia games and entertain each other with the Poo Squad mascots (more on that later in this interview). With all our events, we create an environment where it is safe to ask any questions. There is never TMI; we can talk about poop all day if you like,” said Kristin.
The Three Main Pillars of the GH Foundation’s Advocacy
Gastro Health
Inform and educate the public about the importance of GI health. So far, the GH Foundation has focused on the human GI anatomy, common myths and facts about GI health, ostomy facts, and CRC-related information. You can find out more about resources and past events on the GH Foundation website.
Proactive Advocacy
Proactively provide information and strategies to create positive shifts in how we communicate and influence others. Using what they’ve learn from other organizations, medical providers, patients, and cancer survivors, the GH Foundation has created educational content to then share with the public. Be on the lookout, you may just see their Mascots or Bristol Stool Charts popping up more and more near you!
Impact/Prevention
Educate and inspire people to take action to live a healthier life by fostering an open environment where no topic or question is off limits. Kristin and Dacia lead by example by first sharing something about themselves or asking someone at an event if they would like to share their experiences. They want to help people become as comfortable as possible about talking with their medical providers so they can get the most accurate information about their symptoms and find the best treatment for them.
Making a Difference
Since launching the GH Foundation, Kristin and Dacia have heard from many people that they scheduled their colonoscopy after attending one of their events or receiving one of their resources.
“People have also spoken with family members about their family history to get genetic testing and have said they felt more prepared about what to ask their medical provider at their next visit. People have approached us and expressed a sense of relief that we are creating an environment where they can ask any question, as uncomfortable or personal as it may be. Our mascots have received positive feedback as well. Seeing Sir Colon has taught them what the “colon” looks like,” said Dacia.
Through their initiative “GHF on Campus” they bring gastro health conversations to the forefront of young adult minds through a series of captivating events exclusively tailored to undergraduate students.
“One of our main approaches at the GH Foundation is targeting who we call the “pre-screening community”. Young adults under the age of 45 need to be made aware of common myths and facts on GI health, CRC signs and symptoms to keep watch, and what to ask if CRC symptoms emerge. GHF on Campus has a dual impact: Not only are they learning for themselves, but they can go back home and share what they have learned with family and friends. They can ask about their family history and encourage their family members to act, like scheduling a colonoscopy,” said Kristin.
So far, the GH Foundation has collaborated with the vibrant student communities at the University of Iowa and Northwestern University. Kristin and Dacia are looking to expand campus programming—if you’re reading this and would like to learn more, click here.
Finding humor through the message
You must meet people where they are. One of the ways they are doing that is with a sense of humor.
“We have designed our GHF mascots that bring some fun and lightness to topics that can be very overwhelming and serious,” said Kristin.
The GH Foundation’s mascot crew features: The Poo Squad (from left to right)—Ms. TP, Plungy, Mr. Poo and Sir Colon.
They will show up in different ways. One of the ways is our “Check your Colon” t-shirt with our very own Sir Colon. You can purchase a shirt here.
You can register now for a virtual webinar panel discussion entitled, “Destigmatizing Ostomy 101” taking place Tuesday, February 20th, 2023 at 6:30 pm CT. The discussion will feature Wound Ostomy RNs Jennifer Bart, MSN, RN, CWOCN, and Aimee Sheddan, BSN, RN, CWOCN.
Getting Involved with the GH Foundation
Talk – Initiate the conversation with your family, friends, and colleagues. Educate your loved ones about the risk of neglecting their gastro health. It may seem like a small step but can change the trajectory of life.
Volunteer – Help connect your community to life-saving resources about GI health.
Donate – Your donation directly funds our efforts to distribute educational materials and health guidance to the public.
Engage – Reach out to us! We welcome new ideas on how we can break the stigma.
Follow us on our socials so we continue to reach more and more people.
Connect with the GH Foundation on social media and follow the amazing work they’re doing:
During my annual skin check at the dermatologist in September my doctor biopsied two small marks on my back. In the moment, my doctor expressed that she wasn’t concerned, and neither was I. Fast forward two weeks, and I was about to speak at a health conference for patient advocates in New Jersey when I received a phone call from an unknown number. I answered and was caught off guard when the voice on the other end was a nurse from my dermatologist’s office telling me both spots came back with pre-cancerous spots and that I needed to get excision surgery on both as soon as possible.
Hearing that news was unexpected. I felt unsure and scared. That anxiety built up until I finally was able to schedule the procedure for November 30th. Life as an IBD mom makes these types of health hiccups tricky. I had to keep pushing off the surgery because of different family activities and obligations during this extra busy time of year.
This week on Lights, Camera, Crohn’s I take you on a behind-the-scenes look at my patient experience and discuss skin cancer and IBD and what you need to be aware of.
How I felt going in
Going into the surgery I felt uneasy. I wasn’t sure what the recovery would entail. I’ve only had abdominal surgeries, a bowel resection and three c-sections. One of the spots was on my upper back and the other was right above my bra strap. I was worried about how it was going to feel to lay down, sit back, move my arms, pick up and hug my kids…the list goes on.
As always, I turned to our IBD community for input, intel, and perspective. The experiences and advice shared not only educated me but left me feeling comforted before I went under the knife. Here is some of the feedback I received:
“You only live once and it’s on your back. In my opinion, the only way to wear a scar bad is to wear it with insecurity. Cover it up with confidence, or reveal it with confidence, but if you do either with insecurity, that makes it much more obvious.”
“After surgery when you’re up and about, focus on excellent posture almost to the point of bending backwards. You’ve had a resection and with any abdominal surgery, you hunch over a little bit to keep the incision from pulling. Do the same with the back ones, but you have to kind of have a bend to your back. Move slowly and if it pulls, you’ve pushed too far. With abdominal surgeries, I stay very on top of pain meds, with this, I would make sure you’re in a little bit of discomfort, just so you know when you’ve pushed too far. Not enough to be in actual pain, but enough to be uncomfortable and feel it when it pulls.”
“Be extra careful with what activities you do with it being on your back. I popped stitches on my back once because it’s such a high-tension area. The worst part is having a scar left behind.”
“My doctor gave me an option: stitches vs no stitches. Choose closure with stitches, otherwise healing is long.”
“The local anesthetic stings a little, but nothing worse than a biologic that you’re used to. They’ll tell you to keep the sutures moist with ointment (NOT Neosporin) and covered during the day. Wash gently with your regular soap and water. The sutures on the back are usually in for about two weeks. Make sure the pathology checks margins (so you know all atypical cells were excised). Compared to everything IBD moms endure, this is a piece of cake!”
“Surgery is an easy recovery. I had stitches for two weeks. Make sure you keep the area moist with Aquaphor or Bacitracin. Be careful not to lift anything with the stitches so you don’t pop a stitch or cause further scarring by stretching the open area. It might hurt the first couple of days, but Tylenol will do the trick.”
“My best friend had a pretty good size excision surgery on her back, and everything went smoothly, and it was painless for her. She healed up nicely and the scar is minimal.”
“Recovery was straightforward! Just keep up on any pain meds prescribed and try to take it easy. I had a wide excision on my toe that sucked because walking was hard for a few days. Little movement until your incisions are healed a bit is helpful.”
“Sitting back and laying down might hurt for a couple of days, but you should be fine after that. You don’t want to pop the stitches. You can’t take a bath or submerge the incisions for at least two weeks. Showering is fine after 24 hours, but just be gentle with them. I did derm nursing for many years.”
“I’ve had this (Crohn’s med complication), and it was far less bad than I thought. Briefly painful, but recovery is quick. I found vitamin E cream super useful while it was healing or (La Roche- Posay Cicaplast) also once healed. Make sure you rub the scar, so it doesn’t ‘tether’.”
“Find out your surgeon’s preferred ointment. Mine okayed Aquaphor. Set pillows so you can sleep comfortably once you find a position that works. The pain is worst at night. Sending you big hugs and wishing you speedy healing with clean margins!”
What excision surgery entailed
Leading up to the excision surgery—especially the week of—my mind started to race a bit when I went to bed at night and started thinking of the procedure and recovery. It was my first time needing something more than a biopsy at the dermatologist, so I wasn’t sure what to expect. The excision surgery process involved so many lidocaine and epinephrine shots that I was in tears by the end. The areas of my back were so sensitive and by the time I had 10-15 shots I could feel, I hit a bit of a breaking point.
One of the nurses brought me an ice pack to grip onto and it really helped stop my anxiety and shaking on the table. The actual surgery on the two spots took an hour. It’s always an odd feeling while you lie awake and know your body is being cut into. I have dissolvable stitches underneath my skin and on top on the incisions.
Here’s a photo of the two incisions. They are larger than I had anticipated, and I’m not thrilled about them, but I know once they’re healed, they won’t look so angry.
Recovery is not linear
The first night of recovery I was able to keep the pain under control for the first 10 hours or so, but I woke up at 4 in the morning in excruciating pain. I felt like my back was on fire and I couldn’t move. It was a horrible feeling. My husband helped me out of bed, and we went downstairs. He propped me up on a ton of pillows and set an alarm for my next pain pill. The first two days were a rougher recovery than I had anticipated, but I’m so grateful my dermatologist caught this when she did.
By day 3 I was doing laundry, cleaning, organizing my son’s room, packing up toys to donate, and making dinner. As I write this, I’m 4 days post-op and I just have slight twinges of pain here and there and itching sensations. The hardest part for me has been not being able to lift or hold my 2-year-old or being able to help my 4-year-old daughter who’s had a club cast on her dominant hand and arm and has needed my help to do everything from getting on the toilet to climbing into her car seat. That being said, my kids have all been incredibly patient and empathetic and my husband has been a rockstar at making sure I don’t overdo and feel supported every step of the way.
My toddler walked up to me when I was in pain and said, “your tummy hurt, mama?” Not this time, buddy. It amazed me that his mind went there when he saw me hurting. With that, he snuggled me on the couch and gently grabbed both my hands and kissed them.
Is there a link to IBD meds and skin cancer?
There is some evidence to suggest a potential association between IBD and an increased risk of skin cancer, particularly non-melanoma skin cancers such as squamous cell carcinoma and basal cell carcinoma. When I asked my surgeon prior to my procedure if being on Humira put me at greater risk for this, she told me there’s not enough conclusive evidence and she did not relate my situation to my medication, but I’m still not convinced. I was told that the pre-cancerous cells would have turned to melanoma if this was not caught.
The relationship between IBD and skin cancer risk is complex and may involve various factors:
Immunosuppressive Medications: Prolonged use of medications, such as corticosteroids or certain biologics, can weaken the immune system, increasing susceptibility to infections and possibly contributing to a higher risk of skin cancer.
Chronic Inflammation: IBD itself is characterized by chronic inflammation in the gastrointestinal tract. Chronic inflammation has been linked to an increased risk of certain cancers, including skin cancer. The inflammatory process may contribute to the development of cancerous cells.
Sun Exposure: Some studies suggest that those with IBD may be at an increased risk of skin cancer due to excessive sun exposure. It’s important to note that certain medications used to treat IBD, like thiopurines (Imuran and Purinethol), make the skin more sensitive to sunlight.
Genetic Factors: There may be genetic factors that contribute to both IBD and an increased risk of skin cancer. Some people have a genetic predisposition that makes them more susceptible to both conditions.
Final thoughts—Get those annual skin checks!
When it comes to skin cancer, we can control our sun exposure and how we protect our skin when outdoors and that should not supersede the importance of taking medication to treat and manage IBD.
Talk with your care team about the frequency you should be screened. Once you have skin cancer or a biopsy, it’s not unusual for bi-annual visits or even every three months. If I can share anything—it’s to get your annual skin check. Skin cancer is nothing to mess around with. Ignorance is not bliss. Give yourself peace of mind and schedule a dermatologist appointment, whether you have IBD or not. My husband and I have both had scares now when it comes to our skin. Be proactive and in the new year I hope you take the appropriate steps to make sure you’re in the clear.
It’s that time of year when sickness lurks around every corner. For those of us who are immunocompromised, run of the mill “regular people” sickness can hit us extra hard. Since the end of September, I’ve dealt with bronchitis for 5 weeks, followed by pink eye in both eyes, and I currently am dealing with a bacterial infection in my right eye. Being an IBD mom with young kids in preschool and elementary school brings extra germs into our house. While I’ve been under the weather, I keep second guessing what supplements are deemed “safe” and beneficial for me to take since I’m on a biologic. Even 18-plus years into the game, I still get confused about the gray area around supplements to help us improve or boost our immune systems and which we need to be careful of.
This week on Lights, Camera, Crohn’s we hear from three gastroenterologists who take a deep dive into this topic, along with a registered pediatric GI dietitian, and several people from the patient community. Before we get started, I want to preface this by saying this is a complex issue that is not black and white. Even after digging deep researching this topic—I’m still not completely clear on what’s best for myself.
There’s been conflicting beliefs on whether Elderberry is “smart” to take when you’re immunocompromised. I ran a poll on Instagram asking our community what they’ve been told. Of the 260 people who responded 72% said “This is a thing?!”, 21% of those polled said they were told to “Steer clear when on immunosuppressants”, and 7% of people were told by their provider that it’s “Safe and advised” to take Elderberry.
Let’s hear what patients have to say
Samantha: “I was advised not to boost my immune system. So, I focus on nourishing my body well when sick. I drink a lot of smoothies and fresh juice. I’d avoid Elderberry for sure. I take daily vitamins and get my levels checked regularly to make sure I’m getting enough of what I need. However, I have a kid in school who brings all those lovely germs home. I had a GI once explain it to me like this…my immune system is overactive; I have to take medication to weaken it, which brings it down to a “normal” range. If I try to “boost” it, I’m working against my medication.”
Cindy: “My mother-in-law purchased some Elderberry for my daughter with Crohn’s shortly after her diagnosis. “A woman at Whole Foods told me this could be good for her.” She meant well. Anyway, I understood that my daughter shouldn’t take Elderberry, after consulting with Dr. Google. I believe it was a reputable website that contraindicated Elderberry for patients on immune suppressing medications.”
Emily: “I have been told both—that Elderberry is safe and that it is not. My family doctor told me to avoid it and my GI nurse says that it’s ok sometimes when sick?! So confusing!”
Alyssa: “My husband has Crohn’s and is on Entyvio. He takes Elderberry if he has flu or cold symptoms, whereas I take it daily during the winter. Funny enough, I’m sick A LOT more than him!”
Jessie: “I’ve been told by some doctors not to take immune boosting supplements with biologics and others that it doesn’t matter, but I can’t find the concrete research/facts I need to be sure.”
Lindsey: “I find my symptoms flare when I have Elderberry!”
Rachel: “I’m always confused if I should be taking anything to “boost” my immune system when I’m on suppressive meds. I asked my provider years ago, but I didn’t really get a real answer. I’ve always thought it was good to take supplements to help my immune system, but then I get concerned about them counteracting my medication.”
Hermione: “I have been told it is a placebo effect by my immunologist.”
Kristen: “I read that you don’t want to boost your immune system since that’s the system you want suppressed and caused your disease in the first place.”
Bee: “I was told not to take things that will “boost” the immune system. In South Africa, it’s Echinacea. I was told not to take it. So, my approach has been to “indirectly boost” my immune system by taking vitamins and fresh fruit and vegetables as much as I can tolerate.”
Rocio: “I’ve had this conversation with providers, particularly when I had COVID. I was told NOT to take Elderberry because it has been shown to increase cytokine storm which is present in both COVID and IBD. From an IBD specific point of view, the anti-TNFs seem to calm that storm which is why some were used as COVID therapeutics. So, I wouldn’t say it’s because of being on immunosuppressants, but rather the disease itself.”
Julie: “I live on Elderberry but never asked my doctor, so I’m hoping it’s ok!”
Laura: “I’ve taken Elderberry for years on Remicade (also working as a nurse practitioner in pediatric primary care) and it has helped keep me well and my GI docs have never been opposed to me taking it. I do usually skip it the night before and after an infusion though.”
Jana: “I was told it could cause increased risk of cytokine storm for those with IBD in general, whether on immunosuppression or not.”
Heather: “My son’s GI said NO to Elderberry. We used to take it every winter, but once he was diagnosed with Crohn’s they said to stop using it. I always worry about this time of year and all the yucky stuff going around. My son takes the Liquid IV Vitamin C packets and puts those in his water. I don’t know if they help, but I feel better knowing he is taking something to maybe help give him a boost!”
Beth: “I’m so glad you’re covering this because there is so much confusion—should we try to boost our immunity or not? My personal experience is that I was taking it trying to boost my immunity before a busy event season when I needed to stay healthy. About three weeks later, I was wracking my brain trying to figure out what was flaring my Crohn’s because I’d been eating right, sleeping more, hydrating…and I think it was the Elderberry. In general, I have tried to shift my logic to “these are things that help keep me healthy” versus “how do I boost my immunity?”
Madison: “My first GI told me “No” if you’re on biologics. Not sure if that’s true, but I just trusted that guidance and still avoid it!”
Jess: “I was told to steer clear of Elderberry because of having IBD.”
Jaclyn: “I have asked so many times what I can take, and I’m always told there is basically nothing extra I can do. I have a 4-year-old and 5-month-old in daycare, so they are always bringing home sicknesses.”
Elderberry: To take or not to take?
After reading those firsthand experiences it’s clear—the patient population is unclear and hesitant about what is best when it comes to boosting immunity. While Elderberry has gained popularity for its potential immune-boosting properties, its safety for those of us with IBD is not well-established. Elderberry supplements are often promoted for their antiviral and immune-enhancing effects, primarily attributed to compounds like flavonoids and anthocyanins.
Before I became a patient advocate, I would take elderberry anytime I felt a sniffle or had a sore throat. I really felt like it made a positive difference. Fast forward a few years and I started hearing that Elderberry could interact with Humira and cause my immune system to become over-active, so I stopped taking it all together. To this day, I wonder about taking it—and I know many of you do, too!
There are a few considerations for those with IBD when it comes to Elderberry:
Sorbitol Content: Elderberry products, particularly some syrups and extracts, may contain sorbitol, a sugar alcohol. Sorbitol can have a laxative effect and may exacerbate symptoms for those with IBD, especially if you are sensitive to sugar alcohols.
Potential Interaction with Medications: Elderberry may interact with certain medications or treatments for IBD. Elderberry is believed to have immune-modulating properties. When taken with immunosuppressive medications like Humira or Remicade, there is a potential risk of enhancing the immunosuppressive effects, which might increase the susceptibility to infections. It’s important to discuss this with your healthcare provider to understand the potential implications.
Limited Research: There is limited research specifically addressing the safety and efficacy of Elderberry in individuals with IBD. The specific interactions can vary, and it’s essential you ensure there are no adverse effects or diminished efficacy of your prescribed medications.
The GI’s weigh in on the debate
Dr. Miguel Regueiro, M.D., Chief, Digestive Disease Institute, Cleveland Clinic, says that while he does not want to sound dismissive of supplements, that we lack good data to make claims for or against. Personally, he does not feel Elderberry is harmful, and does not have a problem with his patients taking it.
“I am not aware of good, randomized data to indicate true harm from Elderberry in immunosuppressive or immunomodulatory medications, even though there are warnings listed,” he said. “Theoretically, Elderberry will “stimulate” or “activate” the immune system and has been a popular supplement that some recommend for “cold/flu” or to prevent cold and flu. If that theory is true, then potentially elderberry as an immune stimulant would offset or counteract an immunosuppressive.”
Without good, randomized safety data, it is difficult to make this strong claim one way or another. Given that Elderberry may or may not help with cold/flu, in an abundance of caution it would be reasonable to avoid in patients on immunosuppression.
“My sense is that the dose of Elderberry is low enough that even with immunosuppression, there should not be a problem, but, again, without confirmatory evidence to say that Elderberry effectively “fights off” or “prevents” cold/flu, one could simply avoid it in patients who are immunosuppressed.”
Dr. Regueiro says the ideal health-related approach is to ensure that IBD patients are eating a whole food diet, avoiding processed/ultra processed foods, drinking plenty of water each day (1-2 liters), exercising regularly, and having good sleep hygiene.
“Regarding additional supplements, based on a patient’s history and certain IBD meds, we recommend different supplements. For example, for patients who have been on steroids in the past, we recommend a bone densitometer for osteopenia (and osteoporosis). If bone mineralization is low, we recommend supplemental calcium and Vitamin D. If a patient has had ileal (small bowel) surgery, we will check a vitamin B12 level and if it’s low, we recommend parenteral (subcutaneous) shots, as they will not be able to absorb oral B12.”
He went on to say that iron levels should be checked, as iron deficiency is common. If iron levels are low and a patient is anemic, parenteral (IV) form of iron is recommended, as oral iron can upset the stomach and even lead to more IBD symptoms.
“For patients with short bowel syndrome from extensive bowel surgery, they should be managed by a nutrition team who specializes in short gut as the evaluation of nutrients and vitamins is more comprehensive and detailed. Finally, for most of our IBD pts who do not have any of the above vitamin deficiencies, as long as they’re eating a well-rounded, healthy diet, they need no other vitamins. However, I tell my patients that taking a once per day over the counter vitamin is generally safe and ensures all nutrients are covered.”
Dr. Yezaz Ghouri, M.D., Director of Inflammatory Bowel Disease Services, University of Missouri School of Medicine at Columbia, says elderberries seem to have high amounts of antioxidants.
“The main antioxidant seems to be a bioflavonoid called Anthocyanin. These give purple pigment in the berries and have powerful antioxidant properties. Antioxidants have an anti-inflammatory and anti-carcinogenic effect in the body. Patients with IBD have chronic ongoing inflammation and are at increased risk of developing colon cancer. Carcinogenesis refers to the conversion of normal tissues to cancer. In general, we recommend the use of berries in IBD patients, and these are a good source of minerals, vitamins, and healthy carbs. The Crohn’s and Colitis Foundation cautions the use of Elderberry in IBD patients due to concerns that this fruit increases production of certain types of chemicals in the body that can cause IBD type inflammation. One of these chemicals is called tumor necrosis factor (TNF), the same which is blocked by medications used to treat IBD.”
Immunosuppressive medications and antioxidants work hand in hand in preventing inflammation.
“But there have been some studies that showed the effect of Anthocyanins on a group of immunosuppressive medications used in IBD called anti-TNF alpha inhibitors (examples: infliximab, adalimumab, certolizumab, golimumab). There is inconclusive evidence in this matter and there are no large clinical human studies showing that use of Elderberry is linked with an effect on TNF alpha inhibitors ,” explained Dr. Ghouri. “Please consult with your GI specialist prior to their use. Taking Elderberry in moderation should be ok, but if one develops any signs of disease flare, then stop the use,” he said.
Dr. Ghouri agrees that it is “ok” for IBD patients to take Elderberry.
“Elderberry has very strong anti-inflammatory properties that may contribute towards preventing damage from chronic ongoing inflammation and free radical based tissue injury.”
Dr. Ghouri recommends the following protocol for labs to indicate whether you need specific supplements/vitamins added to your regiment:
Checking Vitamin D levels at least once a year
Checking Vitamin B12, Folic acid and Iron (Ferritin) levels, if anemic
Specifically checking Vitamin B12 level once every 6 to 12 months in patients with Crohn’s disease involving the small bowel
Checking other mineral or vitamin levels may be patient dependent, please check with your GI specialist or PCP. There is a need for checking vitamin and mineral levels more frequently in patients who have lost most of their small bowel, due to Crohn’s disease. These individuals have a diagnosis of short-gut syndrome and sometimes require IV nutrition. These patients are at higher risk for developing all sorts of vitamin and rare mineral deficiencies. They need to be seen by a specialist with a background in managing such patients and require frequent blood testing for several minerals and vitamins.
The Pediatric Perspective
With young people often being the carriers of so many germs and being susceptible as school age kids—I wanted to hear from Dr. Michael Dolinger, M.D., MBA, Assistant Professor of Pediatrics, Associate Pediatric Gastroenterology Fellowship Program Director, Icahn School of Medicine at Mount Sinai.
“For any patient on immunosuppressive medications, it is important to have an open discussion with your treating gastroenterologist about Elderberry, specifically Sambucus nigra, which is used in most herbal supplements. This could stimulate the production of components of the immune system that cause inflammation, mainly cytokines and tumor necrosis factor,” explained Dr. Dolinger. “Many effective therapies target these cytokines or tumor necrosis factor to treat inflammatory bowel disease, as they are often elevated. There is no clear evidence to support this either way, but if you are on a therapy that targets tumor necrosis factor or cytokines for your inflammatory bowel disease, I would certainly have a discussion with your gastroenterologists to review the potential risks and benefits first.”
He went on to say that one of the largest issues with using supplements, particularly in children, is that they are not regulated by the Federal Drug Administration, and you have no way of knowing if what is on the label is in the supplement you would be giving your child.
“I always encourage parents who are thinking about giving supplements to children to assess if there have been any studies of this particular supplement in children or ongoing studies and if not, I urge them to use the same caution they have surrounding any therapy and that is to place safety at the forefront and not give unregulated supplements to children,” said Dr. Dolinger.
For children with IBD, a well-balanced diet with adequate calories for growth and development is the most important recommendation. Supporting supplementation with iron, vitamin D, vitamin B12, and calcium is needed when these levels are low.
“Routine monitoring of vitamins and micronutrients is essential in the care of inflammatory bowel disease patients. For example, vitamin C deficiency often goes unrecognized. We see zinc or selenium deficiencies not uncommonly too. It is most important to have routine monitoring for vitamins and micronutrients at diagnosis and when doing well, at least yearly,” he said.
Erin Feldman, R.D., CSP is a pediatric dietitian. She looked up Elderberry on a database called NatMed. Here’s what she found:
“On the natural medicine database, under “interactions with drugs” immunosuppressants are listed and it states—theoretically, Elderberry might interfere with immunosuppressant therapy, due to its immunostimulant activity. Elderberry has immunostimulant activity, increasing the production of cytokines, including interleukin and tumor necrosis factor. On the patient handout it states that Elderberry might cause the immune system to become more active. This could increase symptoms of autoimmune diseases. If you have one of these conditions, it is best to avoid Elderberry.”
Supplements and Lifestyle Choices that may offer general immune support
If you plan to incorporate any supplements into your routine, please consult with your care team, preferably a gastroenterologist or a registered dietitian, who is familiar with IBD and how it manifests in our bodies. Here are some different supplements you may want to check out:
Probiotics: Probiotics are beneficial bacteria that can help maintain a healthy balance in the gut microbiome. Some studies suggest that certain probiotics may be helpful for individuals with IBD, but their effectiveness can vary. Different strains may have different effects, so it’s crucial to consult with a healthcare professional before using probiotics.
Vitamin D: Adequate levels of vitamin D are important for overall health and immune function. Many people with IBD may have lower levels of vitamin D. This can be determined by a simple blood test. I personally have been vitamin D deficient for years, so I’m prescribed 50,000 IU a week right now.
Omega-3 Fatty Acids: Omega-3 fatty acids, found in fish oil, flaxseed oil, and certain nuts and seeds, have anti-inflammatory properties. They may help support the immune system and reduce inflammation. Again, consult with your healthcare provider for appropriate dosages.
Zinc: Zinc is essential for immune function. Some people with IBD may have lower levels of zinc, so supplementation may be considered under the guidance of a healthcare professional.
Turmeric/Curcumin: Turmeric, and its active compound curcumin, have anti-inflammatory properties. Some studies suggest that curcumin may have potential benefits for those with IBD, but more research is needed. It’s essential to consult with a healthcare provider before using curcumin supplements.
Quercetin: Quercetin is a flavonoid with antioxidant and anti-inflammatory properties. It is found in various fruits and vegetables. Some studies suggest it may have potential benefits for individuals with IBD, but more research is needed.
Lifestyle Factors: Adequate sleep, stress management, and regular exercise are crucial for overall health and immune function. Ensure you are getting enough rest and engaging in stress-reducing activities.
Final Thoughts
Given the potential for interactions and the need to manage the delicate balance of the immune system in individuals with IBD, it is highly advisable to consult with your healthcare provider before adding Elderberry or any new supplement to your routine. A lot more research is needed in this field to better understand supplements and their effects on medications.
There is no clear evidence that immune boosting supplements such as elderberry produce cytokines and tumor necrosis factor to counteract medications, but there is also no strong evidence that they do not either. We don’t know the way in which supplements support or do not support individual immune systems in patients with inflammatory bowel disease on therapies that target the immune system.
Your healthcare provider may guide you on whether elderberry or other immune-supportive supplements are appropriate for you, and if so, what dosage is safe. Always follow their recommendations to ensure the best possible outcomes and to minimize the risk of complications.
When you have IBD and need a biologic, it used to be all infusions or self-injections. But starting in March 2022 (for ulcerative colitis) and May 2023 (for Crohn’s) a daily pill known as Rinvoq (Upadacitinib), entered the game. Rinvoq is the first approved oral product to treat Crohn’s. This once-daily pill is prescribed for those with moderately to severely active IBD who have had a lackluster response or an intolerance to one more TNF blockers (such as Humira and/or Remicade). Rinvoq is also prescribed for rheumatology and dermatology conditions, such as rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, non-radiographic axial spondylarthritis.
Doses range from 15 mg, 30 mg, or 45 mg. According to AbbVie’s website, “Rinvoq is a selective JAK inhibitor based on enzymatic and cellular assays. Rinvoq works with your body to fight the inflammation that can lead to IBD symptoms. Rinvoq stops the activity of some inflammatory proteins known as Janus kinase (JAK) to help reduce inflammation.
This week on Lights, Camera, Crohn’s we talk with 29 IBD patients about their personal experience on Rinvoq, along with Dr. Uma Mahadevan about key information for those in the family planning stages of their lives.
What patients have to say about the induction dose and the quick improvement in symptoms
Rinvoq is the first JAK inhibitor medication that Brooke tried and she didn’t know what to expect. She started Rinvoq in July and says her body has done a complete 180.
“All of my immediate issues have healed, and my long-standing symptoms have begun to fade. In the beginning during the loading dose, I felt a bit more tired. But after two weeks, I had more energy and have experienced less symptoms. Most of my extraintestinal manifestations have cleared up.”
Brooke says she has caught two colds since being on it, so she’s still masking and being diligent around crowded spaces, especially during flu season. She advises fellow patients to talk to their physicians about the dosage they need.
“Because of how much I’ve been flaring, I’m on a higher dose longer than I may have been if I started in a healthier place. Make sure you and your care team agree on a dosage that is not only good for you, but also that you agree with.”
Brooke sets alarms to take her meds because she is used to an infusion or subcutaneous injection, and it’s important not to miss a dose of Rinvoq.
Tonya: I’m only two weeks in, so still on the induction dose, but this is the first time my symptoms have been somewhat controlled in four years.”
Sarah: “I just started Rinvoq and it’s helping me come out of a flare up.”
Melissa: “My 17-year-old son has been on Rinvoq for about six months after Xeljanz failed him. He’s doing great on it and it’s super easy since it’s a pill once a day. He has also been on Humira and Entyvio in the past. Rinvoq has been the easiest transition so far.
Jennifer L.: “I went on Rinvoq after Remicade failed me and then went on Cyclosporine to bridge the gap before I could switch to Rinvoq. I started it in December of last year and this has been the one drug that has subsided a lot of the symptoms. No nocturnal bowel movements, the only major side effects I’ve had is some acne, but I would say it’s hardly noticeable. I did have to come off hormonal birth control as a side effect can also be blood clots, so you can’t have two drugs that increase your risk of that together. I’m single and wasn’t really thinking about dating coming out of a huge flare, so it was a no brainer for me there. If you’re looking to get pregnant, I’ve heard you can’t be on it because studies have shown birth defects, so that’s a concern potentially for some women or for contraceptive options given that you’re only limited to non-hormonal options while on this.”
Krista: “My fiancé just started Rinvoq and after one day he was feeling better. His energy is up, he has an appetite again, and is showing significantly less signs of inflammation. We still have a journey, but it’s been a miracle drug for him.”
Lizzie: “I have been on this now for 3 months after Humira and Stelara stopped working. So far, my Crohn’s symptoms have subsided. I’m no longer flaring. I would say since taking Rinvoq, I feel more fatigued, but apart from that, I feel really good.”
Marla: “I started Rinvoq 24 days ago, so I don’t have a lot to tell you. I don’t think it’s anything bad. It’s hard to tell if the medication is working yet. I do blood work in November.”
Lauren: “I’ve been on Rinvoq for about one year now. Didn’t work at first, but found out I simultaneously had C-diff. I was on vancomycin and Rinvoq for about 4 months and was scoped for the first time in 4 years because I was in remission. I ended vancomycin and flared again. I will be transitioning to Skyrizi soon, but even though I’m not in remission, Rinvoq has been the only thing that has gotten me in the best place I’ve been in 4 years. I love the ease of one pill a day, no infusions, no shots, etc.”
The main reason Lauren can’t stay on Rinvoq is that it’s not safe for pregnancy and she hopes to have another child. She’s bummed this medication is the only thing that’s shown her improvements and that she needs to switch.
Amber: “I just started Rinvoq last week, so perhaps it’s too early. I am adding Rinvoq to Entyvio for fistulizing Crohn’s. The one thing we are trying to figure out is how it works with an ileostomy. I tend to have a fast track and has passed pills in the past and Rinvoq is an extended release.”
Dana: “I’m currently on Rinvoq! Although I’ve only been on it for 3 weeks, I don’t have any real side effects so far.”
Lindsay: “I’ve only been on Rinvoq for about 3 weeks. I was hoping for a more dramatic change based on things I have read. My fevers have gone away, and I feel like I have more energy, but I still go to the bathroom just as much and the urgency has not changed. I also had to give up breastfeeding to start Rinvoq, so that was hard!”
Sarah: “I started Rinvoq after Humira was not putting me in remission after 1.5 years on it (even with methotrexate added to help). I saw an immediate improvement in my stools. I might have a few pimples as a side effect. It’s only been 3 weeks, but so far, so good!”
Erica: “I’ve been on Rinvoq since May. I haven’t had any improvement. I was hoping when I started that it would work for me. I heard so many people call it their miracle drug. I was scared to try it at first because of all the warnings, but once I started it, I was hopeful. Unfortunately, it was not my miracle drug and I had to add Skyrizi to it…I’m still not better.”
Denise: “I’ve been on Rinvoq for about 7 years. I’ve been part of a clinical trial. I don’t think I have anything bad to say about it. I was so sick with few options, so I took a risk, and it fixed me. I don’t think I’ve had any side effects. I still get scoped annually as part of the study and my intestines have looked great. Sure, I still have tummy troubles, but not the main Crohn’s ones! I get blood work done every 3 months and everything has been normal there as well.”
Abigail was prescribed Rinvoq in late August 2022. At the time, she was hospitalized with the worst flare she’s ever had and was admitted 3 separate times for a 37 day stay. She was facing steroid and Remicade failure and running out of time before requiring emergency surgery. Abigail was given the option of trying Rinvoq for 2 weeks. If it didn’t work, surgery would be required to remove her colon. Her care team got insurance to approve it and she started it right away. Abigail took a double loading dose. Usually, you do 45 mg for 8 weeks, but she did it for 16 weeks instead.
“This medication not only saved my colon, but arguably my life, as I had faced death twice during that hospitalization. I was able to get off steroids. I now take 30 mg of Rinvoq daily and I’m in clinical remission. My next colonoscopy is at the end of this month, so it may show even further remission. I was nervous to start Rinvoq, since it is so new, but given the circumstances, I agreed to it. I am honestly so glad I did. The only side effect I have experienced is high cholesterol. My care team will be addressing this after my colonoscopy. I am forever grateful to Rinvoq for giving me my life back. I choose to do medication and therapeutic diet (SCD). For me, this combination has really helped.”
The visible side effects
Jessie started on Rinvoq to treat her Crohn’s before it was FDA approved because of a flare she couldn’t get under control. She was put on the 45 mg dose for 2 months and saw quick improvements in how she was feeling. After years and years of being poked and prodded for infusions and labs she says she’s so grateful to give her body a rest and just take a daily pill.
“Rinvoq has been like a miracle drug for me. Despite the side effects of weight gain, constipation, and acne on my face and body, I don’t even care because it’s the best I’ve felt in more than 5 years. I’ll take the acne and backne any day.”
Jessie spent hundreds of dollars on skin products and through patient support groups she was recommended CeraVe Moisturizing Cream with Salicylic Acid and CeraVe Body Wash with Salicylic Acid and has noticed a huge improvement. Both products are available over the counter.
Madison: “I am on Rinvoq and I hate it. Let’s say first, it works fast. Within 48 hours, my symptoms were gone, and it’s done a great job at keeping my UC in check. However, the side effects are awful. Acne is the most common side effect and I have it everywhere. My face used to be dry, but now it’s VERY oily. My cholesterol has gone up, which is a known side effect and doctors are keeping close tabs on it. Lastly, weight gain. Weight gain was recently acknowledged as a side effect and I’ve had that, too. The first-generation JAK inhibitors were notorious for weight gain, so I’m not sure why it wasn’t acknowledged in this second generation.”
Madison adds that it’s hard to acknowledge that Rinvoq is working well, but it comes with its fair share of side effects. While the side effects are annoying, she says they are not as bad as a flare.
Alexandra: “I took Rinvoq for 5 months. It did absolutely nothing for my UC, but it gave me horrible acne.”
Lisa: “I was on 45 mg for 3 months. I hated it. I had some sort of infection the entire time and had bruises everywhere. I started Skyrizi three days ago.”
Elizabeth: “I’ve had great results on Rinvoq, I take 30 mg along with Entyvio. My only complaint with Rinvoq is the acne.”
Jenna: “I just stopped Rinvoq. I had a horrible face rash as a side effect. It seemed like an acne flare when it started back in early August and no matter what I tried, it got worse and worse. My dermatologist and doctors both believed it was some sort of rash caused by being on immunosuppressant drugs and stopped my Rinvoq. I took an anti-parasitic and the acne is mostly cleared up.”
Kelly: “I started Rinvoq and only completed 6 weeks (the loading dose and start of the treatment). Insurance issues were part of the reason why I stopped taking it. I also knew that I wanted another child. If I was able to…and there were minimal to no studies for a safe pregnancy. The only symptoms I had were small rashes on my hands and feet, kind of pimple like, not painful or concerning…just something I noticed.”
Jennifer V.: “On Rinvoq and love it!! It’s a pill so it’s easy and it has put me mostly into a therapeutic remission. The cons: weight gain, fatigue, elevated liver enzymes, and anemia. All in all, if you are not having any more children, I would highly recommend this medication. I would need to see more time and research if I were to recommend it prior to pregnancy.”
Jennifer V. had to go off Rinvoq last week while she was taking Paxlovid to clear up Covid and she lost weight for the first time in ages. Now she says she’s back on Rinvoq and the weight is coming right back.
Emily: “I have had Crohn’s and lupus since 2020 and I took the highest dosage of Rinvoq, and it didn’t do much to help me. While I was on it, I thought I saw some improvements, but as soon as I went off it, I realized it wasn’t doing much good. It made my skin break out really bad. I often would pass the pill whole when going to the bathroom. It’s a big pill, easy to see. I’m on Skyrizi now and hoping to reach remission.”
Kendall: “I’ve been on Rinvoq about 3 months. My symptoms have improved, but I’m surprised at how many of the side effects I have experienced: styes, mouth sores, cold sores, and acne. I’m planning to stay on it. My IBD is not stable yet, but I’m hopeful Rinvoq will get me there. Afterwards, I’ll see if diet and lifestyle can maintain remission. It’s nice that you can start and stop Rinvoq!”
Implications for pregnancy and breastfeeding to consider
Sarah: “I just started Rinvoq and it’s helping me come out of a flare up. I am wrapping up my third month. I started to feel improvement after two weeks. It’s such a relief to take a pill after self-injecting for the past 15 years. So far, I don’t have any bad side effects. The only thing that stresses me out is that you can’t be pregnant while taking it, so as a 34-year-old, ready to have a second child, it’s in the back of my mind—how am I going to get off (and back on this), how will I keep my Crohn’s under control when I’m pregnant next? But, in the meantime, I’m grateful that it’s helped me get control over a bad flare that caused me to take a medical leave from my job.”
Allie: “I feel like I had a good experience on Rinvoq. I would say the good is that it works very fast. I was starting to feel better from my flare within 3 days. I was able to get off prednisone because it worked so quickly. The bad is that Rinvoq made me gain weight that I haven’t been able to lose, but my doctors won’t confirm it’s related to the medication. I also felt very bloated all the time. I did not like having to take a pill every day (going from being on Entyvio), so I would sometimes forget to take it. The last thing for me is that I’m still hoping to have another child and it’s not safe for pregnancy, so it was not a long-term option for me, even though it helped me achieve healing from a flare.”
Carmen started taking Rinvoq in February after multiple biologics and non-biologics failed to treat and manage her ulcerative colitis. So far, she says her experience has been very positive. She went into clinical remission within the first month of being prescribed 45 mg.
“I’ve since been tapered down to 15 mg and it’s still looking very positive. Bloods, calprotectin, and how I generally feel has massively improved, along with my quality of life. The negatives I’ve experienced so far have been some mild skin issues, mainly rashes on my face, chest, and upper back, this is currently controlled by over-the-counter salicylic acid face and body wash. I’ve also picked up a few fungal infections and have lost my big toenail because of one of the infections that required antibiotics. For me, these are minor issues and outweigh the overall treatment plan. My GI believes as we’ve decreased the dose to 15 mg, that these minor side effects will disperse over time.”
Carmen says taking a once daily pill is much simpler than some of the other biologic drugs that require visiting an infusion center and taking multiple other medications either intravenously or orally. The cost for me is relatively high for Rinvoq at $150 a month, but this will depend on what medical insurance and copay you have. All in all, Carmen says Rinvoq has been a positive experience and has done what other medications have failed to do.
Important Considerations Regarding Family Planning While on Rinvoq
Dr. Uma Mahadevan, MD, Director of Colitis and Crohn’s Disease Center at University of California San Francisco and lead investigator of the Pregnancy in IBD and Neonatal Outcomes study (PIANO) says when it comes to Rinvoq, the medication has been associated with birth defects in animals at the same dose as given to humans (30 mg), so she avoids prescribing this in pregnancy.
“I do not prescribe Rinvoq to someone who is about to get pregnant. However, Rinvoq is generally given to people who have not responded to anti-TNF, so if Rinvoq is the best medicine for them, I do not hold the fact that they are a woman of child-bearing age against them and give them the therapy to best put them in remission.”
Dr. Mahadevan says if a woman is on Rinvoq and becomes pregnant she has successfully transitioned patients to Skyrizi. This can be more challenging with UC as there are fewer options. The PIANO study is currently researching the safety and efficacy of these drugs. There are several Skyrizi patients being monitored right now and 2 Rinvoq patients so far. You can learn more about being a part of PIANO here. I participated in PIANO with my youngest child as an IBD mom who is on Humira. Being a part of this research is invaluable for our community and helps current and future families.
It’s believed that Rinvoq crosses into breastmilk, so you should avoid feeding your baby that way if you are taking this medication.
Rinvoq Complete Patient Support
Much like other biologics, there are patient support services in place that you want to be aware of. RINVOQ Complete provides personalized patient support when you need it. With RINVOQ Complete, you get 1-to-1 assistance with finding potential ways to save on the cost of your prescription and more. I use Humira Complete for my prescription needs.
You can also get help making sense of your insurance and finding ways to fit Rinvoq into your everyday routine.
If you have commercial insurance, you may be eligible to pay as little as $5 a month for your prescription with the RINVOQ Complete Savings Card. Click here to sign up for your RINVOQ Complete savings card.
Final thoughts
It’s important to remember that just because someone has a miraculous experience or a terrible one with a specific drug, does not mean that you will. I will say, with all the biologics that I’ve covered on Lights, Camera, Crohn’s the visible side effects (weight gain and acne specifically) were the most widespread and common among the patient population. So many of you said you felt guilty feeling “vain” about not wanting to be on a drug because of that, and I want you to know those feelings are valid and matter. At the end of the day, we all must measure risk vs. benefit and what matters most when it comes to keeping our IBD in check.
You can check out other Patient Experience articles that I’ve covered here:
It’s no surprise IBD impacts so much more than just our guts. Not only is there the gut and brain connection, but also the complex nature of our chronic illness(es) that can cause serious anxiety, depression, and mental health issues. The isolating nature of Crohn’s disease and ulcerative colitis, the unknowingness of what the next day holds, and the never-ending laundry list of procedures, labs, scans, and surgeries, year after year is a lot for any person to go through.
Even though I’ve lived with Crohn’s disease for more than 18 years, and have seen three different gastroenterologists in that time, not once has my mental health been brought up during a clinic appointment. When treating a person for IBD, the health of the whole person needs to be considered. I ran a poll on Instagram asking the IBD community if they’ve ever been to therapy. Out of 185 respondents, 70% seek therapy, 18% have not, and 12% are considering it.
I did an article in September 2020 about why a specific public bathroom at a grocery store I used to shop at triggers me and shared tactics for coping. You can read the article that featured Dr. Tiffany Taft here.
This week on Lights, Camera, Crohn’s we hear from those in our community about the advice that’s resonated with them the most since receiving their IBD diagnosis.
The words that have made a lasting impact
Olivia: “3% effort is still effort. You’re not going to be able to give 100% every day and that’s OK. Your best can look different from day to day.”
Julie: “It’s not your fault, you didn’t do anything wrong.”
Kristen: “You can’t drive forward if you’re always looking in the rearview mirror.”
Sarah: “Medical trauma is trauma and to give myself credit for all I have overcome.”
Cindy: “Remove all IBD related stressors from the bedroom to avoid impacting sleep. In our case, this meant no Humira injections for my daughter while sitting on the bed or nearby it.”
Tina: “Imitation is the best form of flattery.”
Lauren: “Don’t Google things you’re worried about, like symptoms.”
Jennifer: “Stay in the present.”
Heather: “Sometimes you just need to take a nap!”
Myisha: “If it’s not going to matter in five years, don’t give it five minutes of your energy.”
Kate: “It’s not your fault.”
Susan: “I’ve never seen a therapist, but I always tell myself it could always be worse.”
Stacey said: “You can’t control how seriously people take Covid. You can only control how you protect your physical and mental health. You have to put your health first. And, if people don’t agree with your choices, then that’s their problem. You can’t risk your health just to make it easy for others or to placate them. You come first in your life.”
Robin: “The “things” I do—my work advocating for others, supporting others, helping others face challenges with their diseases—I deserve that, too. Not from other people, but from myself. The beauty in therapy is that you’re receiving a non-biased/outsider opinion. This person that has no side and will sometimes say something you’ve heard 1,000 times in a way you’ve never heard before or even in a better way that allows you to really listen to what’s being said. To absorb it. Even to say it multiple times with no judgement if that’s what’s needed. Also, EMDR, which is a whole other thing and only part of the therapy experience.”
What is EMDR therapy?
Several people said EMDR therapy was their favorite and has been lifechanging. So, what exactly is it? Eye movement desensitization and reprocessing (EMDR) is a fairly new, non-traditional type of psychotherapy that’s popular for treating post-traumatic stress disorder. EMDR focuses on the natural tendencies our brains have for healing from traumatic memories. There are mental blocks (such as feelings of self-esteem issues and powerlessness) that can prevent us from healing. During EMDR, you are allowed to process the bad memories and experiences to start healing yourself. This helps our brains process challenging thoughts and feelings in a healthier way. Chances are through your patient journey you’ve endured several vivid and significantly painful moments that you haven’t been able to process and heal from.
Supportive Resources about managing mental health and IBD
Chances are you’ve heard of Pelvic Floor Therapy but may not know what this entails or why so many people in the IBD community are talking about it. Individuals with IBD can have persistent symptoms of fecal incontinence, constipation, rectal discomfort, and diarrhea, despite having their IBD in remission with medical therapy. These persistent and often debilitating symptoms can have a major impact on your wellbeing and quality of life.
This week on Lights, Camera, Crohn’s we hear from two gastroenterologists from Mayo Clinic along with several IBD warriors who provide insight, helpful guidance, and information about pelvic floor therapy.
What exactly is Pelvic Floor Therapy?
Pelvic floor therapy is a treatment program performed by pelvic floor therapists to retrain the pelvic floor muscles to address underlying issues such as constipation, fecal incontinence, or urgency. Many patients with IBD in remission may develop pelvic floor dysfunction which is usually diagnosed from a digital rectal examination in combination with an anorectal manometry test.
“During an anorectal manometry, a small catheter with sensor probes and a balloon is placed into the rectum and is connected by a wire to the computer. During the test you are lying on your side and asked to perform maneuvers to determine how your pelvic floor muscles work. At the end of the test, they inflate a balloon in the rectum to help evaluate for sensation and then ask you to simulate having a bowel movement by pushing the balloon out,” explained Dr.Katie Dunleavy, MB BCh BAO, Gastroenterology Fellow, Mayo Clinic.
Based on normal values for your age and gender, you may be diagnosed with a pelvic floor dysfunction. Dr. Dunleavy went on to say that in IBD, there is less research on the benefits of pelvic floor therapy.
“But we have seen benefit in up to 80% for patients in remission who continue to have symptoms of constipation, urgency, or incontinence once active inflammation is fully ruled out. Similarly, some patients with IBD undergo total proctocolectomy with ileal pouch anal anastomosis (IPAA) may also benefit from pelvic floor therapy if they have issues emptying their pouch,” said Dr. Dunleavy.
Additionally, those with IBD who’ve had pelvic floor surgeries might experience sexual dysfunction and this type of therapy directed towards relaxation of the pelvic floor can lead to a better sexual experience.
Pelvic Floor Dysfunction does not discriminate across genders
Any person can develop pelvic floor dysfunction and may benefit from treatment with pelvic floor therapy in the right setting.
“While most studies describe pelvic floor in females, I believe individuals from all genders deserve evaluation of their pelvic floor the recommendation for pelvic floor therapy. Furthermore, individuals of a transgender experience, might undergo gender affirming surgery that impacts their pelvic floor muscles, and would benefit from pelvic floor therapy,” said Dr. Victor Chedid, M.D., M.S., Gastroenterologist at Mayo Clinic.
Dr. Dunleavy says, “As many as 50% of people with chronic constipation have pelvic floor dysfunction, which means there is impaired relaxation and coordination of the pelvic floor and abdominal muscles during evacuation. Some common symptoms include straining with hard bowel movements, a feeling of incomplete evacuation, pain with intercourse, or urinary symptoms.”
Certain risk factors make it more likely for men or women to develop pelvic floor dysfunction, this includes instrumented vaginal deliveries, chronic constipation with straining, prior surgery, prolapse, and age. It is important for men and women to discuss symptoms with their doctor to ensure they get the appropriate testing and treatment.
Apprehensive about getting looked at?
It is important for people diagnosed with pelvic floor dysfunction to seek out a qualified pelvic floor therapist who is specialized in GI and evacuation disorders. These are generally physical therapists or occupational therapists who complete extra training in pelvic floor therapy.
“You should find a therapist you trust and will feel comfortable with during your therapy sessions. The therapists who work in this area are fantastic and work diligently to explain what they will be doing. My patients tell me that the relief they feel from therapy well exceeds the apprehension they had prior to starting sessions,” said Dr. Dunleavy.
It’s important for patients to feel comfortable talking with health care providers and addressing concerns they may have on this topic. Dr. Chedid typically discusses the benefits of pelvic floor therapy with patients during clinic visits as a beneficial treatment option that does not require surgery. He provides patients with exercises and techniques to do at home that will have a major impact on general wellbeing and health.
“Individuals with IBD experience significant “negative” experience with the bathroom and with defecation that can be quite traumatizing, and therefore when they get in remission, they still have a negative association with the bathroom and might have “fear of defecation” despite being in remission. I equate that to “PTSD of the pelvic floor”, which is not a medical term, but an analogy I use. Therefore, pelvic floor therapy is essential to reverse this negative experience with the bathroom and make their bathroom experience a healthier and satisfying experience. Almost all patients who I describe this to get it right away and understand the importance of pelvic floor therapy,” said Dr. Chedid.
He adds that it’s imperative health care providers communicate with patients and ensure that the therapy session will be a safe space with at rained physical therapist who is trained in empathetic and trauma informed care. This is essential in putting a person’s mind at ease, as many patients might have experienced sexual trauma in their lifetime that makes pelvic floor therapy triggering for them.
The impact of Pelvic Floor Therapy post operatively and after IBD pregnancy
If you’ve had a total proctocolectomy and an ileal pouch anal anastomosis (IPAA), you might experience non-relaxing pelvic floor dysfunction or pouch evacuation disorder. This is similar to the rectal evacuation disorder in individuals with pouches.
“Typically, this is identified by history, physical exam, pouchoscopy, anorectal manometry and dynamic imaging of pouch evacuation. Additionally, someone who has had any form of trauma to the pelvic floor, including Perianal Crohn’s disease or surgeries for Perianal abscesses or fistulas or lacerations due to vaginal deliveries after pregnancy, these patient might experience rectal evacuation disorders after recovering and healing. In the proper patient, if identified by history, physical exam and the right testing, these patients will benefit from pelvic floor therapy,” said Dr. Chedid.
At the same time, there isn’t a lot of research on pelvic floor therapy in the post-operative state or following pregnancy in patients with IBD.
“There have been several attempts to find normal values for patients with IPAA who have undergone colectomy to help diagnose pouch related pelvic floor dysfunction. We generally recommend patients wait until the anastomosis following surgery is completely healed prior to having an evaluation with a balloon to ensure no complications. Similarly, patients who have recently undergone delivery from pregnancy will likely require time to heal. I would discuss this with your doctor to have more personalized information,” advised Dr. Dunleavy.
If your GI recommends pelvic floor therapy for your personal symptoms and struggles the overall response is tremendous.
“Recommending pelvic floor therapy to everybody, without identifying the right patient who would benefit from it is not typically beneficial. Therefore, in the right patient, pelvic floor therapy is extremely effective,” said Dr. Chedid.
What IBD patients have to say
Stacey has ulcerative colitis and went from having an ostomy to becoming a j-poucher. She’s a big proponent of Pelvic Floor Therapy. After her 3-step surgery to j-pouch in 2021, she knew she needed at least an evaluation from a pelvic floor physical therapist (PFPT) after urination became a challenge and inserting tampons became impossible during her takedown recovery.
“My surgeon wouldn’t write me a referral, citing that the anorectal manometry tests prior to surgery were all normal. My GI doctor didn’t want to go against the clinical judgement of my surgeon, so I couldn’t get one from her either, and finally I received a referral from my OB/GYN after explaining that penetrative sex was impossible (and felt unsafe to me) to even attempt,” Stacey explained.
These delays resulted in 5 months of significant pelvic pain that she felt ill-equipped and under-supported to handle, and this time could’ve been saved if she had gone into surgery with a referral to see PFPT from the get-go, even if she didn’t need to use the referral; it would’ve been nice to have.
“It’s so wild to me that orthopedic surgery has extensive PT rehabilitation protocols, and yet I was met with such resistance to gain access to the professionals who could help support my muscular recovery, even after such extensive GI surgeries,” she said.
During Stacey’s initial encounter with the PFPT, she spent the majority of the visit trying to gain a strong understanding of her entire pelvic and holistic health history, everything from sexual health to physicality to surgery, and all the in-between.
“She asked for consent prior to any invasive exams and explained them in thorough detail, reminding me that I was in control and could always choose to stop an exam if I felt unsafe. She continued to breathe with me during the exams and communicated her findings in real-time, which made me feel at ease. At the conclusion of our visit, I was told that I was experiencing hypertonic pelvic floor dysfunction from a decade of clenching for dear life trying to make it to the bathroom with mod-severe UC, even before my surgeries. The tightness of the muscles, coupled with three extensive pelvic surgeries, contributed to the pain and issues I was experiencing,” said Stacey.
During the visits with the PFPT, Stacey discovered she had no awareness of her pelvic floor muscles whatsoever. She could not distinguish the relaxation of the muscles from the contraction, and the entire area felt numb to her, like it was a holy, empty space. She says this made the exercises challenging to understand initially. She was prescribed specific exercises, not Kegels, including strategies to gain awareness of supportive muscle groups so she could begin to engage with this part of her body and start to heal.
“What I did not expect, however, was for this experience to be as enlightening and empowering as it was. Slowly but surely, the little life things showed me that they’re the big life things: being able to fully urinate in under 20 minutes, FINALLY being able to use tampons again- these were MASSIVELY important to my quality of life, and they became possible through the help and support of a PFPT and my adherence to their prescribed exercise regimen. I even realized one day while holding one of my exercise poses that I could feel the muscles DEEP in my abdomen! They felt heavy, full of pressure, as if they fired on to greet me, and then suddenly… I could feel them gently, slowly, RELEASE. I cried tears of relief realizing that I had been fearful of reconnecting with these muscle groups, and it really was safe and okay to be in my body.”
Stacey says she had NO idea these muscles existed, yet here they were. Had they been here all along?! She says she numbed them out from years of associating the deepest parts of her with pain from UC; and that her brain was protecting her. I truly wonder. All she knows is the day that she could FEEL her body experience relaxation and safety with FULL awareness of these pelvic muscles is the day that she knew that healing from these surgeries was going to be possible.
After one year of PFPT, Stacey “graduated,” not free of pain, but with the tools to know how to live within the ebbs and flows of pain. She tells me she still relies on the tools and bodily awareness that she gained through the experience.
Jessie was diagnosed with Crohn’s disease when she was 15 years old and after more than 22 surgeries later, at the age of 38, she says she completely underestimated how much her pelvic floor was affected over the years by the inflammation, surgeries, and her pregnancy.
“I was “guarding” badly (a response to pain) and so weak. I was having bladder issues, pelvic pain, rectal pain and so much more. After 2 years of being consistent going to pelvic floor therapy and doing the exercises I can say I’m about 85% better. I can’t say enough how much of a HUGE difference pelvic floor therapy made in my life and my IBD journey. My therapist explained it to me like this “you don’t have orthopedic surgery on your knee, wrist, ankle, spine, etc. and not get prescribed physical therapy. Same with an injury. It’s just standard procedure. But, for some reason, even though your pelvic floor consists of tons of muscles, ligaments, tendons, bone, etc. the same process is not considered – but IT SHOULD BE!” Your pelvic floor needs to be rehabbed after any injury, strain, surgery, etc. just like any other muscle/tendon/ligament/bone in your body,” explained Jessie.
Claire started PFPT because all imaging and tests showed that while her inflammation is under control, she still experiences extreme pain.
“I was tested, and they found I have dyssynergic defecation. This was caused by my chronic pain due to long-lasting fissures as well as chronic constipation. I’m grateful my GI thought to have me tested for this, as many don’t make that connection since the symptoms are so similar to Crohn’s. During PT, I have learned that my muscles do not relax and are constantly tense, so we work on trying to get them relaxed in order to successfully pass bowel movements. Like all other PT, one downside is that it is a lengthy process and takes up a lot of time. I have a one-hour appointment every week for 12 weeks and an hour or two of exercises and stretches on my own every day.”
She says she’s started to notice improvements and found ways to make her pain more bearable, though it’s something she will have to continue working on for a long time.
Tiffany has accessed pelvic floor therapy for herself and having previously been a physio and a fellow Crohnie, she recommends people speak with their doctors because it can make a world of difference, especially after surgery, hospitalization, or a flare.
“The neural connection we have to our trunk and pelvic muscles can be re-trained and strengthened, allowing less pain, and for me an improved sense of control over urgent bowel movements.”
Preslie was diagnosed with Crohn’s in June 2016, and after two years of battling severe symptoms, she had a colonoscopy that showed she was in remission. It may sound like lovely news, except Preslie was still living with a ton of pain, so her and her care team started digging for answers.
“This led to an Endometriosis diagnosis in August 2018. That was great news, except I STILL was not getting relief, and started having severe burning anytime I urinated, but always tested negative for UTIs. I went to a male urologist who told me I was just constipated, which was not the case. After well over a year of extremely painful sex, constant pain, and burning when I peed, I went to a urogynecologist who talked with me for less than 10 minutes and had the diagnosis: Interstitial Cystitis and Levator Ani Syndrome. I finally felt heard. I started pelvic floor therapy shortly after and immediately felt relief.”
Rocio says pelvic floor therapy was recommended to her by a home health physical therapist who was treating her for neuromuscular issues after bowel resection surgery for her Crohn’s in 2020.
“During my resection recovery, I was struggling tremendously with constipation, which was unfortunately always my issue with my IBD. Although uncommon, it’s been my reality for the last 20-plus years. The reason I share this is because I wish someone would have recommended pelvic floor therapy to me over all those years.”
She began seeing a pelvic floor therapist in January 2021 and completed two years of treatment. During that time, Rocio says she learned a lot about the intricacies of all the muscles, the nerves, the internal blood flow, and so much more. Because of two fistulotomies and a stricturplastly, she has numerous anatomical issues which prevent her from having normal bowel movements.
“Pelvic PT changed that completely and I have normal/formed BM’s every single day, without any signs of constipation and without any straining. I’ve learned ways in which I can help relax and release the pelvic floor should I face issues in the future.”
Separately, Rocio has learned how beneficial pelvic floor therapy is for many IBD patients post-operatively, including the ileal resection she had. Her therapist worked on her abdomen significantly during appointments to prevent adhesions and scar tissue. She says there are so many benefits to pelvic floor therapy that it does make her wonder why more IBD health care providers aren’t encouraging patients to pursue care.
Annie started pelvic floor therapy two weeks ago. She was referred based on suspected interstitial cystitis, not her IBD. She was shocked to learn during her first appointment that treatment was for all conditions that involve urgency of any kind.
“The game changer was the pelvic exam itself, I never realized what my PT noticed right away, which is that my first layer of pelvic muscles are unnaturally sensitive. This is massively helpful for IBD and IC, but the most validating part was having a lifetime of excruciating intercourse and painful pap smears and knowing the reason. My PT told me this is not how my life has to be. After just two weeks of exercising my pelvic muscles with a vaginal wand and daily targeted yoga, my urgency, both with my Crohn’s and IC, has gotten so much more manageable. I started this journey running to the restroom every 30 minutes (even at night), now I feel like I’m starting to get my life back.”
Jasmine says pelvic floor therapy helped her a ton following j-pouch surgery.
“I truly believe it should be integrated into post-op care plans, I had to seek it out and ask for it.”
Amy says that while she doesn’t have experience yet with PFPT, she has a complicated Crohn’s history for the past 25-plus years. Now that she’s over 40 and has had three vaginal births, she recently asked her doctor about pelvic floor therapy.
“Because of all the IBD women sharing their journey with this on the Internet, it inspired me to look into therapy for myself. In my first request, the response was that it might be a fantastic idea, but to wait and see. My next visit is in a couple of weeks and I’m looking forward to utilizing this article to share and take with me to help me advocate for myself.”
A look at the insurance piece
Yes, pelvic floor therapy can be covered by insurance, but it can vary based on the type of insurance. It is also important to ask about coverage for biofeedback therapy which is an essential part of the therapy based on prior research studies. Many insurance companies will need proof of diagnosis using an anorectal manometry with balloon expulsion test or defecating proctogram.
“If the proper indication based on testing is identified with the referral to pelvic floor therapy with a script written by someone’s GI provider, then typically insurance should cover it,” said Dr. Chedid.
Closing thoughts on Pelvic Floor Therapy and IBD
It is important to discuss with your doctor if pelvic floor therapy is right for you. Once patients with pelvic floor dysfunction have these basic tools, they can begin retraining the pelvic floor muscles with biofeedback. Biofeedback provides auditory and visual feedback to help retrain the pelvic floor and relax the anal sphincter. Biofeedback training is the treatment of choice for medically refractory pelvic floor constipation, with some studies showing improvement in more than 70 percent of patients. Patients also learn to identify internal sensations associated with relaxation and long-term skills and exercises for use at home.
At Mayo Clinic patients have had more than 70% response at 3 months following initiation of pelvic floor therapy. The response usually takes weeks to months to see a clinical difference and requires patients to practice their exercises and biofeedback at home.
“Although many centers are familiar with retraining techniques to improve pelvic floor dysfunction, few have the multidisciplinary expertise to teach patients with constipation how to appropriately coordinate abdominal and pelvic floor muscles during defecation, and how to use bowel management techniques, along with behavior modification, to relieve symptoms. Because pelvic floor dysfunction can be associated with psychological, sexual, or physical abuse and other life stressors, psychological counseling is often included in the evaluation process,” said Dr. Dunleavy.
If you have chronic pain, you may also need to see a physician to have these issues addressed prior to starting pelvic floor therapy.
Key takeaways from fellow IBD patients
PTs are an excellent resource, but just like getting an IBD-ologist is superior to a general GI doctor, PFPTs are an even stronger resource, ESPECIALLY in the context of chronic GI disease where so many of our deepest muscles are constantly working on our behalf.
You can always say “no thanks!” You don’t need to agree to any sort of exams or exercises that you’re not ready for, and a compassionate PFPT will empower you to make decisions and communicate in alignment with your body’s needs.
ANYONE can benefit from PFPT: any age, any gender.
Normalizing pain and discomfort is a survival instinct, but it’s not necessarily serving you for the GOOD life- it’s okay to get evaluated if you’re concerned about sexual pain or dysfunction, pain with periods, or if you also have IBD and simply want to be sure that you’re supporting your pelvic and spinal muscles the best you can so that you can, especially in the bathroom!
YOU get to decide! Having an evaluation may be all you have the capacity for, and that’s okay! You can return for a plan of attack later, or you can wait until you have the capacity to dive in head-first! There’s no one right way.
If you decide while talking to a PFPT before they do ANY manual evaluations that something doesn’t feel right- YOU GET TO CHOOSE, and you can always, always say, “nevermind”. Advocating for your body is always progression in your healing journey, every single time.
SPEAK UP! It’s RIDICULOUS that patients have to ask and ask and ask for the bare minimum, but if it helps your quality of life and it’s within your capacity- it’s certainly worth it.
A big deterrent for patients can be cost, but the investment is worth it, if you can swing it. You would be surprised how much every system of your body is so connected and feeds off one another!
Helpful resources to check out
Find a Pelvic Floor Therapist Close to Home
Utilize the “Section on Women’s Health” or the “Herman & Wallace” websites. Both these groups train therapists who specialize in pelvic floor disorders.
The Section on Women’s Health (SOWH) website has a “PT Locator” tab. You can enter search criteria including your geographic location (e.g., zip code) and specialty (e.g., constipation) to identify a therapist closer to home.
The Herman & Wallace website has a “Resources” tab under which you will find a “Practitioner Directory.” Use the map features to locate a therapist near you.
Utilize the “find a provider” section of www.pelvicrehab.com for a local PT by zip code.
The therapists who work with pelvic floor disorders may be in Gastroenterology, Urology, Gynecology, Physical Medicine, and/or Women’s Health, etc. You may be able to find someone through your local physicians or contacts.
For those in Canada, check out the Canadian Physiotherapy Association. It has a “Find a Physiotherapist” tab which allows you to connect with the sites of participating provinces/territories. By specifying a “Women’s Health” therapist or equivalent, you may find someone who specializes in the field of incontinence, pelvic pain, constipation, etc.
The benefit of pelvic floor therapy also involved patient education, relaxation exercises, diaphragmatic breathing, and correction of maladaptive toileting behaviors. Some studies have shown improvement in quality of life relating to symptoms, and mental health.
To receive biologic infusions at home or within a medical setting? That is the question. As an IBD mom of three who has done self-injections for 15-plus years, it’s intrigued me to see how many people in the IBD community now receive at-home infusions. This inspired me to dig deeper and hear firsthand what fellow patients have to say about their experience. When polled on Instagram—out of 260 votes, 55% of IBD patients prefer at home infusions compared to 45% who would like to receive their medication in a medical setting. This week on Lights, Camera, Crohn’s hear advice, guidance, the role insurance plays in all of this, and perspective on treating your IBD at home versus at an infusion clinic or hospital. I learned a lot and I think you will, too!
Discussing Home Infusions with your Care Team
If receiving your infusion at home interests you, here’s what you can do to get the ball rolling on making it happen.
Talk with your GI about whether home infusions are an option in your area and if they feel comfortable with you doing so. Discuss the risks and benefits. Your GI will need to write a prescription.
Call your insurance and make sure home infusions are covered in your health plan.
Amanda has been doing Remicade infusions at home since the pandemic started and she says it’s been much better for her. Being able to receive her medication at home and cuddle with her 4-year-old daughter and dog are big wins for her. Recently, she also receives daily IV fluids, and thanks to her Port and home health, she’s been able to do it herself.
Amanda: “Home infusions have changed the game for me. They make me feel safer as someone whose immune compromised. I almost always have the same nurse, and I don’t have to commute before or after. How grateful am I!”
She says how you coordinate setting up home infusions is dependent on your insurance. Personally, after talking with her insurance she found a list of home health agencies within 30 miles of her house and called and spoke with a few.
“Some did not administer my medication, some charged separately for nursing fee, and some were not taking new patients. Once I found a good option for my family, the home health company reaches out to your GI doctor, who then sends the script to the Specialty Pharmacy, rather than to an infusion center.”
When Bad Veins and IV issues Set You Back
One of the main reasons I chose to do a self-injection rather than an infusion was because of how horrible my veins are. When I was told I needed to start a biologic during a hospitalization in July 2008, it was the same hospitalization where it took three people and eight tries to start an IV on me. To this day, I’m still a bit fearful of getting IVs because of that traumatic situation. Several people wrote to me with the same concerns—this is something to consider if you typically need a Vein Finder for hospital visits and procedures.
Olivia: “I initially loved the idea of doing infusions at home. My first one went smoothly, the nurse had a bit of trouble finding a vein and drawing blood, but no problems after that. The ability to do my infusion in my bed or on my couch was so much more comfortable than the hospital! But then, the next two infusions, the nurse had trouble getting a vein and one had to be rescheduled because of hospital policy. That infusion took over an hour to find a vein. After that, we spent a month trying to convince insurance to let me go back to the hospital so I could use the ultrasound to get IVs placed. Ever since, I’ve been doing infusions at the hospital. The idea of doing infusions at home was nice, but it didn’t work for my situation.”
Meredith: “I get my Entyvio infusion at home. I don’t love it. It is more convenient than having to go to the hospital/office, but nurses often have trouble starting IVs on me and at home they are the only option. There is no backup and I’ve had a few bad experiences. Things have gotten better because I now have in my profile that I need pediatric needles, but they aren’t the standard, so those types of needles are not always supplied. The insurance decided for me that I would receive my infusions at home because it’s cheaper and since I’ve never had allergic reaction. The service by me is different, but there is no future scheduling. You know around the date that your next infusion is and then you’re contacted one day beforehand with a time. I’m too high strung to be comfortable with that, but it is what it is.”
Much like Amanda, Meredith loves having her dog there for support. When she initially started getting home infusions her dog needed to stay outside the room because she was too interested in what was going on, but now she’s used to the process and equipment and can snuggle.
Heidi: “My insurance made me switch to home infusions. At first, I was nervous because I’m a hard stick and always require a vein finder. I also just felt safer in a hospital setting. But, I’ve been doing home infusions for three years and I love it. I have my “old faithful” vein and I like being in my own home with my own bathroom and other comforts. I also have wonderful nurses whom I look forward to seeing each time. Everything is so much more personal this way.”
Melissa: “Sadly my veins are awful, and I wouldn’t want to chance the one person who comes not being able to get an IV started.”
Concerns from the Community Regarding Home Infusions
Ashley: “With my ulcerative colitis, comes other chronic illnesses. Which is true for a lot of people in our community. I have POTS, so having my infusions done in a healthcare setting is more reassuring for me because there’s more safety nets in place.”
Emilie: “I don’t get my infusions at home anymore (I used to!) because I hated it. The nurse was always texting me to reschedule, I was always having to deal with CVS trying to get my medication delivered on time, and I had to store all the stuff. It also made me feel like a “patient” in my own home. Mentally it was incredibly stressful organizing and coordinating everything and feeling like I was constantly sick because the medical equipment was always around. I much prefer going to an infusion center, where I just show up and they have everything ready to go. Just another perspective—I know a lot of people love getting infusions at home and I’m in the minority, but there are cons to consider.”
Mary: “I don’t currently do an infusion medication, but I have in the past with Remicade. My GI office set home infusions up for me after I did the first few in the office. It was more convenient for me due to the office being about 1.5 hours away from where I live. I was provided with an IV pole to keep at home among other supplies and a nurse came to my house to do the infusion. It was awkward at first, but after a few times it got better. Unfortunately, during one infusion, I had an allergic reaction unexpectedly, during which the nurse had to give me Benadryl and another medication. After that happened, I couldn’t do them at home anymore and had to go to the office. After two more infusions, my GI discovered I wasn’t responding to Remicade anymore and I had to switch to Stelara. The cons are the risk of something happening and not being in a medical setting. Luckily, I had a great nurse who knew what to do.”
Adam: “I prefer the clinic and the reason is, when I was on Humira and had to self-inject, I always worried I didn’t get it in the right spot or the full injection and miss some of my medication. For me, it’s a piece of mind that my infusion is done properly.”
IBD Moms Experience
Miranda was diagnosed with Crohn’s during the height of the pandemic. When she started Entyvio it was in an infusion center, and she felt like she was putting herself and her family at risk each time she went in. By receiving infusions at home, you can potentially be exposed to fewer hospital-acquired infections. This is especially important for individuals with compromised immune systems, as it helps minimize the risk of additional health complications.
“I saw a few ladies (connections on Instagram) who were receiving home infusions, so I asked my doctor about it. He said it would be no problem to connect me with a company in Dallas that handles nursing and medications for in-home infusions. My only obstacle was seeing if my insurance company would approve home nursing. After calling them to go over benefits, my insurance informed me I could receive in-home nursing. I did have to escalate the call to get it pushed through. At the end of the day home infusions were approved. The same company that ships my meds provides nursing. I do have to make a phone call every January to make sure coverage is good, but other than that it’s a flawless process. The nurse and I are close friends.”
Christina: “I specifically told my GI I don’t want to get infusions at home because I like my “me” time in the infusion clinic. Two hours to read my Kindle in peace! I also decline the accelerated rate…perspective changes when you have kids. My nurse jokes they’re my spa days!”
Krista: “I moved to home infusions once I had my daughter. It was more convenient because I didn’t have to find someone to watch my daughter (I had nobody to help or to ask) so that I could attend my infusions. I had a pleasant experience, and the nurse was fantastic. Being able to do infusions in the comfort of my home was fantastic, especially needing an infusion only 2 weeks postpartum, while recovering from a c-section.”
Getting adjusted to receiving medication without support from fellow patients in the room
Kristi has been receiving Remicade at home monthly since January. Her GI office stopped doing infusions at their office due to staffing issues. After a time or two at the hospital-run infusion center, her insurance company called her to see if she’d be interested in home infusions. Since she had been driving an hour each way for years, she jumped at the chance!
“The idea of not having to worry about getting my infusion during a winter storm was enough for me. My doctor’s office was hesitant at first. I was always on board with the idea, and I was shocked to see the cost was similar to my doctor’s office but significantly less than an infusion center. Home infusions have allowed me more flexibility in scheduling. I also feel like my resting period post-infusion is much easier since I’m already home. While I love home infusions, there are some downsides. I don’t think I would have wanted this back years ago when I started infusions. There’s a lot to be said about the community and the support I received just by being in an infusion room with similar patients. It was also nice to be in my doctor’s office monthly, where I could easily report any symptoms, I was having health wise. I am the person that needs to have my house looking perfect before company comes over, so that adds an extra level of stress during an infusion week. It’s also a bit odd to have the nurse here for so many hours. However, I’ve had two nurses so far and they’ve always been very good and very respectful in my home and if I wanted quiet time. Overall, I don’t think I could go back to going somewhere.”
Kristi says now that she doesn’t have the infusion room support, she relies even more on the social media community and the IBD family online. She also loves getting to snuggle with her dog and use him as a heating blanket while she receives her infusion.
Final Thoughts
Balancing the risks vs. benefits. As you’ve read, home infusions are not a one-size-fits-all approach. What works for one person, doesn’t for another. While the benefit of being at home is a big one, having to worry about the sole nurse at your house finding a vein and not knowing if you’re going to have a bad reaction are just some of the cons that can make the experience worrisome for people.
The convenience of home. Home infusions offer the convenience of receiving treatment in the comfort of your own home. This eliminates the need to travel to a medical facility and allows you to maintain your daily routine more easily. For IBD parents and caregivers it alleviates the need of finding childcare. By fitting infusions into your daily life, it helps to reduce the disruption that may come with hospital or infusion center visits. So many of us deal with medical PTSD and having the comfort and familiarity of home can help to ease that burden a bit.
Kat: “I received home infusions for years for UC. My doctor’s office got them set up because I live in a rural area. The pros were the convenience and being in the comfort of my home. The cons were having a stranger in my home for over an hour. Dealing with the company’s billing department was also horrendous.”
A more personalized treatment experience. You can have a dedicated healthcare professional who gets to know you and your specific needs, creating a customized care plan to address your individual symptoms and concerns. Many IBD people I speak with have a close bond with the nurse who visits their home and feel supported during the process.
Jill started on Humira and was later switched to Remicade infusions. She started receiving infusions at the hospital and then her GI recommended she try home infusions to limit exposure to germs.
“My GI’s office took care of the paperwork and I had the choice between two home health companies. This has been a game changer for any guilt I felt around missing work, because the nurse comes to my home and I can continue working on my laptop, if needed. Or I schedule infusions to begin at the end of my work day. I have a great relationship with my home health nurse and she knows me and my veins so well now. I value the relationship and level of care as well as the flexibility I have found with this option. It’s a win for my mental health as well.
Matt received home infusions for seven years. If he could pass along any advice, he says to be even more proactive about your health.
“I had to always coordinate shipments, supplies, and the infusion schedule. The pros are the flexibility and comfort, but the cons are not being at an infusion center where you can unplug and be in your own thoughts.
It’s important to discuss the option of home infusions with your healthcare team to determine if it’s a suitable choice for you. Your care team can address any concerns or questions you may have, educate you on the process, and help you make an informed decision. Remember, you have options and support to manage your IBD effectively, even when it comes to receiving necessary infusions.