Lights, Camera, Crohn’s: An Unobstructed View is officially SEVEN years old! If you told me when I started blogging what a labor of love this website would become for me, I never would have been able to imagine what it would become for my life, for the IBD community, and for patient advocacy efforts. I went into blogging blindly. I had no clue how to format the site, but I knew the types of stories I wanted to share and the messages from patients that I wanted to get across.
As a seasoned journalist who spent nearly a decade as a TV news anchor, reporter, and producer, I’ve used my love for storytelling to try my best to be the voice I so desperately needed to hear upon diagnosis, through my professional life, finding love, family planning, pregnancy, motherhood and beyond. It’s been quite the ride these last seven years. My first article went live July 23, 2016, on the 11th anniversary of my Crohn’s disease diagnosis. I found out I was pregnant with my now six-year-old, two days later. The first six years of Lights, Camera, Crohn’s (and 3 kids later), I shared a new article every single Monday.
Through these seven years, Lights, Camera, Crohn’s has been viewed half a MILLION times, by more than 320,000 people around the world. On this site alone, I’ve shared 368 articles, which does not account for the countless other IBD articles I’ve created for other websites. As I reflect on this milestone, I’m proud of what I’ve accomplished thus far, but know there’s much more work to be done.
This week I want to give you a behind-the-scenes look at how my storytelling process comes to life—I often get asked “how do you become a patient advocate?” and “how do you start blogging?” I hope this advice inspires you to take the plunge, as there are endless seats at the proverbial advocacy table and your voice, your story, your valid experiences, deserve to be heard.
Choosing What’s Newsworthy
It can be overwhelming trying to come up with content that is new and fresh for your blog and social media. I’ve found it extremely beneficial to have an editorial calendar that helps guide the stories that I share. My editorial calendar is in my email in the draft folder. I simply list out the dates (articles have always been shared on Mondays on Lights, Camera, Crohn’s…so I list out all the Mondays for the next 3-4 months). This serves as a reminder of my game plan and when I need to do outreach for the stories.
As a journalist you’re taught and it’s almost innate in some ways to always be on the lookout for a story. I’m always keeping my eye out for tweets and posts on Instagram, conversations in real life, experiences that happen to me when I see my GI or get a scope, that I think will resonate with our community. I think about the pain points I’ve felt along the way and the advice I wish I had when I was struggling in certain moments. I think about the questions I’ve had along the way when Google was scaring the bejesus out of me, and I just wanted real life advice from someone who understood my reality. Think about what uncertainty, questions, concerns you’ve had and what you want to learn more about and then go after the story.
Writing for the Reader
Everyone has a unique writing style, but one of the most common “mistakes” I tend to see with blogging is when writers go on and on and on about their own experience. The articles sound more like a diary entry—and if that’s what you’re going for, great—but usually, you’re wanting to draw readers in. To do this, I use my own experience as a foundation—a sentence or two in the intro and then the rest of the article is written to and for the reader. Try to write your blog articles like a news story. Use sub heads, get reliable sources, attribute studies, share credible information. Give readers in the chronic illness community news they can use. Empower others on their patient journeys so they learn something by checking out your content. Let others see that they are not alone in what they are going through and that you get where they are coming from. By including the expertise of medical professionals, it helps your articles really come to life and allows you to build a rapport and a reputation with the GI community. It’s always incredible to hear when a GI shares Lights, Camera, Crohn’s with their patients.
If you’re unsure how to reach a GI who is not your doctor, I advise going on Twitter and sending doctors a DM asking if they’d be interested in providing input for an article you’re working on. 9 out of 10 times you’ll get a yes. As we all know, doctors are busy, so try and give them a longer lead time to respond to interview questions. I like to include a headshot when I quote a doctor, so I have them send you one.
My Patient Experience articles have become one of my favorite parts of Lights, Camera, Crohn’s—these articles are a major labor of love. I interview 10-20 patients, along with physicians, and spend upwards of 20+ hours out of the goodness of my heart to create a resource that a patient and caregiver can have at their fingertips when they’re trying to make major decisions about how they choose to manage their disease. Topics range from biologics to infertility or life with an ostomy. Rinvoq is coming up next, folks…I just need a breather since I finished writing Skyrizi earlier this month. By crowdsourcing and sharing the good, the bad, and the ugly I’ve been able to provide a complete look at the reality patients face and provide background that shows more than just my experience.
The Art of Interviewing
Whether you’re interviewing a fellow patient or a healthcare professional, the same process goes a long way. Try thinking about the main points of the article and the flow before you write the questions. You almost must think backwards. I do all my interviews over email—for multiple reasons. The number one reason, is that as a mom of a 6-year-old, 4-year-old, and 2-year-old, I don’t get many breaks and trying to conduct an interview over the phone or Zoom and capturing the true essence of what someone is saying is nearly impossible. I also prefer email because it gives people a chance to articulate their responses and enables me to accurately share their quote—word for word, without paraphrasing. I rarely give interviews over the phone, as I like fellow writers/editors/journalists to have what I’m saying verbatim.
When I send the interview email for Lights, Camera, Crohn’s, I provide a deadline in bold and then list the questions. I always ask for a high-level explanation of a person’s patient journey so I have an understanding of what they’ve been through and so I can paint a clear picture for the reader. Try to never ask “yes” or “no” questions—you want people to give good explanations and descriptions.
An example of email outreach to a pediatric gastroenterologist for an article I worked on.
Often the most important question you can ask if “Anything you’d like to add?”—in TV, podcasts, you name it, this is when people let loose a little bit and can provide you with key nuggets of information.
Once I receive the interview responses, I open up Word, and take all the content and start compiling what’s going to be a quote and what’s going to be a part of my wording/storytelling. Then, much like journalists do in TV news, I write the story around the quotes.
Have a Copy Editor (aka family member/friend review your content)
It’s always helpful to have an extra set of eyes on your articles before you share them. Since the day I launched Lights, Camera, Crohn’s, my mom has been my “copy editor.” I email her a draft of the article along with an explanation of what I’m hoping to get across and then she goes through each article with a fine-tooth comb and provides edits and feedback. If I get too fired up about something, she may politely advise I take a certain line of the story out or re-think how I word a sentence. She’s been my voice of reason through this entire process and as my mom, she’s my biggest cheerleader in not just life with Crohn’s, but everything. As a nurse of more than 40+ years, she’s also well versed in medical situations, as well as grammar.
Be Vulnerable and Transparent
Despite how many people advocate for IBD, Crohn’s and ulcerative colitis still have stigmas. It can be daunting to put your words down on paper and share them with the world. I spent the first decade of my disease just telling close family members and friends. What I’ve found since blogging and being a vocal patient advocate, is that by being open, you open yourself up to endless support and camaraderie. There is such strength that comes from saying you’re not ok or need help. Tell it like it is and don’t sugarcoat your story. At the time same, one of the main pillars of my advocacy has to always been to be transparent, while also positive.
Back in the day when I was diagnosed, and those first 10 years when I was living in silence, most of the content I read was pretty doomsday. While I understand and empathize with the pain and horror Crohn’s can cause in one’s life, I’ve tried to never sit in that sadness for long. If anything, IBD has given me perspective and clarity about the fact that IBD doesn’t have to destroy your life or who you are. Yes, it can create major complications, unpredictable setbacks, and hurdles, but those detours don’t have to rob you of what you hope to accomplish or become. While it’s important to be real, I find it just as important to provide hope and inspiration for those who wonder what their futures may hold.
Keep on Swimming
Due to social media algorithms and the lack of engagement many of us see online, it can feel disappointing at times when you put all this effort into an article or a blog and feel like you’re talking or reaching no one. I’ve been there countless times. Don’t let the “likes” or the follows deter you. Know that your words and your stories just need to get into the hands of one person who needs them, and that makes all the effort, time, and energy worth it. Your articles have legs—meaning that once you post them, continue to post, and share for months and years to come because these “evergreen” articles are always timely and necessary. Try to collaborate with others when you can. If news outlets reach out for a quote or if a health website asks for your input, give it—and then ask for your blog to be a part of how you’re attributed in the quote. If you see someone’s Instagram story referring to an article topic you’ve covered, grab the link and send it their way over DM.
If you feel like you’re in a rut or if you’re having a tough time creating content—don’t force it. Ask your followers what topics they’d like you to cover. Use the timing of the year to help come up with stories (for example, navigating diet around the holidays or back to school time and being an IBD teacher). Support the content of fellow advocates—comment and share articles that intrigue you and help others get their words out and the same will be done for you. Rather than seeing advocacy as a competition, view others as your ally—we’re all doing this to help others, spread awareness, drive research, and together we can truly amplify the patient voice—one article at a time.
There’s no telling what Lights, Camera, Crohn’s will look like seven years from now, but I don’t plan to stop storytelling anytime soon. Thanks for all your kind words, for telling me when my stories have touched your life or helped you make a tough decision, and for being there for me when I need support. If you’d ever like to collaborate with me to share your story or if you have a topic you’d like me to write about—please don’t hesitate to reach out.
Here’s to another seven years of breaking stigmas, spreading awareness, and making everyone in the IBD community feel seen.
When you hear the word “Skyrizi,” you may think people are referring to an up-and-coming rapper or something fun, but in case you didn’t know, Skyrizi (risankizumab-rzaa) is a biologic drug that was approved to treat Crohn’s disease in June 2022. With the medication only being around for IBD less than 13 months, finding patient experiences wasn’t as “easy” as previous articles I have covered on Lights, Camera, Crohn’s about biologics, but I learned a lot writing this and I think you will gain a better understanding of Skyrizi after reading this, too.
Some background on Skyrizi
Skyrizi was previously approved for moderate to severe plaque psoriasis and active psoriatic arthritis. It’s worth noting that Skyrizi is the first treatment for Crohn’s that targets the interleukin-23 (IL-23) protein, which is responsible for inflammation in our bodies. By going after IL-23, Skyrizi helps reduce inflammation that can contribute to Crohn’s symptoms.
When it comes to dosing, patients receive an intravenous (IV) infusion that lasts about an hour at week 0, week 4, and week 8, followed by a self-administered subcutaneous injection with an on-body injector (OBI) at week 12 and every 8 weeks after that. This whole OBI situation is incredibly intriguing to me. I’ve been doing Humira injections for 15 years (!) this week, so I’m used to self-injecting, but knowing technology like the OBI exists gives hope to people who are fearful of needles and having to give themselves a shot. We’ll get into more about the OBI and what fellow patients have to say later in the article.
As far as safety, prior to starting Skyrizi, it’s advised that your GI order lab work that looks at your liver function. If results come back abnormal, this may not be the right drug for you. If you are in the family planning stages, pregnant, or breastfeeding, speak to your doctor. You can also enroll in the ongoing PIANO study, which looks at the safety and efficacy of IBD medications during pregnancy and beyond. Since Skyrizi is so new to the game, research is needed to help pave the way for IBD moms and their children.
Let’s hear from the patient perspective
Prior to starting Skyrizi in February (2023), Stelara failed Stéphane. I’m always careful with how I word this—and I wish all patients and healthcare providers would be conscious of not saying “the patient failed” anything—at the end of the day, it’s the drug that fails us. Stéphane says he didn’t start feeling a response until this month (July)—just before his second OBI (on-body injection). Although his calprotectin started to respond positively in May.
“The good is that I’ve responded and feel better. The bad is that we don’t know how long my response will last or how much it’ll stop inflammation and the formation of strictures. I’ve responded to Remicade, Entyvio, Stelara, but I’ve also developed strictures and had surgeries on all of them. I can hope that Skyrizi won’t continue this dire and disappointing record.”
Megan says before she started Skyrizi she was on the path to an ostomy. Entyvio had failed her, and she was experiencing perianal Crohn’s symptoms that were keeping her from being the mom, wife, and employee she wanted to be.
“My medical team and I decided to start Skyrizi and plan for a temporary ostomy to help my symptoms while we waited for the medication to take effect. After my second Skyrizi infusion, I noticed significant improvement in my symptoms! My bowel movements were more regular, there was a decrease in drainage from my setons, and I had less pain overall. Given my positive response to the medication, we were able to table ostomy surgery. I was extremely relieved and grateful that I had such a quick response to Skyrizi.”
Maha went on Skyrizi after the biologic she was on failed her after six years. As she was reeling from the reality that the biologic that had put her into clinical remission could suddenly not work anymore, she was hesitant and nervous about how to decide the next treatment options.
“After reviewing all of my options with my doctor, I chose Skyrizi based on data and evidence, and also on a gut feeling that this might be the right next step. I’m happy to report that I was right, and in the time that I’ve been on Skyrizi, I’ve achieved a state of remission I could only dream of, with no side effects!”
Elizabeth was in the clinical trial for Skyrizi. She says the biologic “changed her life.” After fighting a Crohn’s flare for seven years, it’s been the only medication that’s wrangled her disease under control.
Kelly started to flare last Fall, because of a loss of response to Remicade (infliximab). Her gastroenterologist suggested Skyrizi as an option that aligned with her drug priorities: namely safety and efficacy.
“The drug has very good data behind it, and she had heard of excellent response in the clinical trials. But it was very new to GIs across the US. It was a gamble, but one that we both thought was worth trying.”
Unfortunately, Kelly dealt with significant problems and delays with her prior authorization and needed to use the AbbVie Bridge Program to get her first infusion dose covered.
“My insurance company used my participation in the Bridge Program as a reason to deny my coverage for the drug. But AbbVie anticipated this issue and has several support programs that cover longer use of the drug and help with deductibles until insurance companies change their policies about drug coverage. I strongly believe that the months of stress and anxiety and daily hours-long phone calls to try to get this drug covered and delivered seriously exacerbated my flare symptoms,” said Kelly.
This cat and mouse game is something far too many of us can relate to. It’s sickening and ridiculous what chronic illness patients have to go through month after month, just to receive medication on time. Kelly was constantly anxious and worried about whether her Skyrizi would be covered.
Kelly tells me her first two infusions were easy and that she had almost zero side effects aside from very mild fatigue, like her normal Crohn’s baseline.
Kelly’s final Skyrizi induction infusion
“My third infusion was a little heavier hitting, like how Remicade infusions felt: a pronounced bit of fatigue, headache and brain fog that lasted less than a day. It was very tolerable. I didn’t have to premedicate before the infusions either, although my doctor had started me on budesonide to try to control the inflammation and keep the flare from getting worse while we waited for the Skyrizi to kick in.”
Cassandra says this is her third biologic and the whole experience in and of itself has been a bit nerve wracking. She lives in Canada and was the first to receive Skyrizi in her city.
“I didn’t love being the first, having the nurses learn on me, not knowing what to expect was difficult as I typically try finding online forums where others share their experiences. So far, I feel ok with it. Skyrizi hasn’t gotten me into remission, but we will see how it goes!”
The OBI (On-Body Injector)
Like anything new, getting used to a new medication and the mode of delivery can have a bit of an adjustment period. You wear the device on your thigh or abdomen for 5 minutes while the medication gets into your skin.
Kelly – “The neat thing about Skyrizi is the Obi, or on-body injector. It’s a brand-new device that is halfway between an infusion and an injection. It’s a small rectangular device with adhesive on the whole back that sticks to your leg. The needle in the device is tiny and I had zero sensation or pain. The button to trigger the needle is large and doesn’t have the same kind of chunky CLICK that the Humira pens do, which was nice and felt less aggressive and intimidating. Because the device infuses the medication into your body over several minutes, it uses an electronic pump. This means you cannot wear your fitness device or Apple watch or have your phone anywhere near it while you’re doing the injection.”
Kelly says she expected to have difficulty with the adhesive since it covered such a large area of skin and was strong. Other than mild discomfort while peeling it off (like taking off a band-aid), her skin didn’t have any other reaction.
Stéphane-“The written instructions for Skyrizi make the self-administering with the on-body injection unnecessarily complicated. I counted 33 warnings of what not to do, something that just generates anxiety. In fact, it’s simple and easy and the Skyrizi video they provide on the website is far more confidence-inspiring and useful.”
Stéphane says it’s helpful to watch the video after reading the instructions. He says the video is good at stripping the process down to essentials and showing that the injection process is in fact easy.
“The front of the thigh is simpler than the stomach because it naturally offers the flat, smooth, easily accessible space you need to place the injector. You clean the small end of the vial, stick it into the injector so it clicks, close injector door, clean area of skin, take the two strips off the back (top first), place it on your thigh and press down the adhesive, then press forcefully on button of injector,” he said.
Jessica made the switch to Skyrizi after being on Stelara. So far, she hasn’t experienced side effects and the medication has kept her Crohn’s in remission.
“The new on-body injector technology is weird and takes some getting used, but overall, it’s painless. It’s just been a little complicated to learn. If there’s a lump on your skin after you take the injector off. She says it goes away. While the needle doesn’t hurt, Jessica feels as the medicine goes into your system you start to feel more pressure.”
So far, Megan has completed two OBIs at home. She says the OBI is extremely easy to use. She’s done Humira, Stelara, Cimzia, and methotrexate in the past and says the OBI for Skyrizi is the easiest and least painful.
“I like to head to a secluded area, so I don’t chance my son trying to wrestle or play and accidentally knock it out of place. (IBD mom hack!) While I still have hard days and I’m not symptom-free, my hard days are much less frequent than before starting Skyrizi!”
Cassandra-“The OBI is amazing. I have been getting IVs monthly/every other month for 9 years, so to not have to get an IV has been wonderful. I have grown to really hate them and have had some bad experiences getting IVs so to not have to face that has made a world of difference. The OBI is so simple, so quick, and relatively painless (though I have felt some slight pinching/stinging). All in all, it’s very simple and I find the mechanism very innovative and cool! I haven’t had any side effects yet, aside from injection site swelling and redness the day of.”
Maha-“The best part is the ease with which I can do my Skyrizi injections via the on-body injector: it’s painless, quick, and honestly I forget that I have to do them until my next injection rolls around.”
Benefits of utilizing the Nurse Ambassador Program Much like other biologics on the market, patients can tap into the free Nurse Ambassadors on hand to help ease the transition to Skyrizi. These nurses provide invaluable guidance and comfort every step of the way. Not only is utilizing these programs beneficial for patients, but also caregivers who may be helping to administer medication.
Kelly-“The device is so new, and the instructions can be long and a little complicated, but AbbVie has a nurse ambassador program that is free for all patients. I cannot recommend the program enough. My nurse ambassador came to my house before I even received the first infusion dose and answered all my hundreds of questions about the expected side effects, the rate of response, and showed me a demonstration with the OBI. It was helpful to get comfortable with the training device. My nurse ambassador also showed up to my house for my first injection and walked me through each step and was excellent at providing support.”
Natalie started Skyrizi infusions in May, 2 infusions down, 1 more to go before she starts with the OBI. She says while she hasn’t experienced huge benefits yet, she’s still hopeful. This is her first biologic and she’s appreciative of how helpful the AbbVie nurse has been through the process.
“I am still pretty new to this myself, but talking with the Skyrizi nurse has helped a great deal, especially getting their co-pay program and just having someone to check in on you.”
Jessica– “AbbVie has an amazing support system, and you can always have a nurse ambassador visit you in person or Facetime you. When I FaceTime the nurse, she guides me through it. Just talking to her while the injector is on for five minutes has made a difference.”
Cassandra-“I live in Canada, so things may be different elsewhere, but Skyrizi is the first biologic where I was sent a “Welcome package” which had a little health/wellness goal setter, appointment tracking sheets, a large needle disposable cartridge for my used injectors, and a mini cooler with reusable ice packs. I was super impressed, and it was fun and cute to receive. I have used the nurse ambassador a few times, especially at the beginning. It’s nice to ask questions or voice concerns with them. Having a nurse ambassador gives me peace of mind.”
Maha-“I really appreciate AbbVie’s commitment to patient education and support through their Skyrizi Hub which provides insurance specialists, nurse ambassadors, and an on-call line to help with any medical or financial concerns! My nurse ambassador walked me through my first injection and has followed up with me regularly to check on my progress both in terms of clinical symptoms and also quality of life!”
Struggling with the “newness” of being a biologic the first year it’s approved for IBD
Kelly ended up flaring badly between her third induction infusions and the fourth dose (her first at home injection). She met with her GI several times, discussing what to do. Since Skyrizi is such a new IBD drug, there really isn’t any extensive anecdotal evidence or patient stories about whether it be worth it to continue the drug, or if she would be considered a “primary non-responder.”
“We struggled with what criteria to use to determine if I just needed to wait longer or if I needed to switch drugs. My GI reached out to the Skyrizi sales rep for their practice and was told not to give up on the drug before 24-26 weeks because clinical trials did show that a non-trivial number of outliers did capture response to the drug later than the expected 8-12 weeks that was seen with most primary responders. At 14 weeks, I could tell that I wasn’t seeing any response to the drug because I was tracking my symptoms, daily bowel movements and pain. It was helpful to have that data to show us in black and white that I wasn’t doing well.”
Looking at the reality of the data and watching her symptoms escalate and her inflammation creep higher and higher despite the steroids and Skyrizi, Kelly and her care team made the decision to discontinue Skyrizi and move to another drug.
“It’s hard to hear from so many medical professionals that a drug with only about a 40% response rate is considered a raving success in the GI community. For me, that’s an enormous number of people who did not respond to this drug. I wish very much I had been one of them, because it’s scary and upsetting when you burn through a drug and cannot go back to it in the future because of possible antibody development.” says Kelly.
Ultimately, the decision to try a medication is a highly personal decision, one that should be made well-informed and jointly with your GI healthcare provider.
Maha says, “My experience with Skyrizi has affirmed that there is hope in all the new therapeutic modalities that are coming out, and that they can offer patients a strong quality of life while delivering treatment as minimally invasive as possible.”
Interested in reading previous Light’s Camera Crohn’s Patient Experience articles about other biologics?
Raise your hand if you’ve ever been blindsided by an IBD flare. My Crohn’s has landed me in the hospital with zero warning on several occasions. The unpredictability of IBD is a huge challenge we all face. But what if a wearable device could signal when our disease course is going off the tracks? What if we had warnings long before we were face to face with our next flare?
An ongoing “Stress in Crohn’s” study out of Mt. Sinai’s IBD Center in New York and The John Radcliffe Infirmary/Oxford University in the United Kingdom has been investigating this since February 2021, with the help of 200 participants. The study wrapped up in June 2022 and was conducted in partnership with 4YouandMe and funded by a grant from The Leona M. and Harry B. Helmsley Charitable Trust to 4YouandMe.
The goal? To empower those with Crohn’s to monitor stress responses and early signs of impending illness worsening in between clinic visits, while providing a means to navigate life and mitigate the consequences stress has on our disease journey. While stress has long been known to somehow affect our IBD, the details of the relationship are poorly understood.
This week on Lights, Camera, Crohn’s we hear from an IBD mom and educator who recently participated in the Stress in Crohn’s study in hopes of taking action to help advance our knowledge of diseases like Crohn’s and ulcerative colitis.
The mission of the Stress in Crohn’s study
Wearables such as smart rings, smart watches, and smart scales, along with our phones, can collect information emanating from us. They can record our physiology and our routines that we are learning to weave together into “clinical symptoms”- such as fatigue, sleep, and stress.
“The main mission of 4YouandMe (nonprofit) is to empower individuals to navigate their own health by using wearables and apps while sharing their own health related data and insights for the benefit of all. This desire was birthed after working at Apple on their Special Projects team and grew out of asking “why can’t the data that emanates from each of us come back and help each person improve their health on a daily basis”,” said Stephen Friend, President 4YouandMe(nonprofit) , Visiting Professor of Connected Medicine, Oxford University.
Tina Aswani-Omprakash, MPH, Wearables Research Coordinator at Mount Sinai’s Susan & Leonard Feinstein IBD Center & Patient Advocate/Founder of the blog ‘Own Your Crohn’s’ says the promise of wearable devices in the prediction of IBD flares and drug response is real and something she’s excited about.
“As we know, IBD can be a progressive disease and it is important to shut down inflammation quickly to prevent complications. The wearable studies at Mount Sinai’s Susan & Leonard Feinstein IBD Center are looking to develop algorithms using measures such as heart rate variability, sleep duration & quality, essentially autonomic/ parasympathetic nervous system fluctuations via data collected through wearable devices. The hope is to help predict IBD flares and showcase drug response utilizing wearable device signatures,” said Tina.
Meet Nicole, Stress in Crohn’s study participant
Nicole Pavlin became a patient at the Mount Sinai IBD Center in New York and received an official diagnosis of Crohn’s disease of the ileum and jejunum in 2021, but her symptoms began more than 16 years prior. At the time Nicole was just beginning her teaching career and she was focused on raising her family. Once Nicole received her IBD diagnosis, she would often search GI research publications to better understand Crohn’s, along with the treatments and procedures available to patients.
“By educating myself about the disease, I’ve been able to communicate more efficiently with my healthcare team and advocate for my needs. The opportunity to participate in IBD research is always exciting to me, especially since the results could potentially help patients in the future,” said Nicole.
Nicole chose to participate in the “Stress in Crohn’s Study” from July 2021 to May 2022, which captured a period of time when her IBD symptoms took a turn for the worse. Nicole had bowel resection surgery that involved the removal of 6 inches of her ileum, including her Meckel’s diverticulum.
Getting recruited for the Stress in Crohn’s study
You may be wondering how Nicole got involved with this study. A Clinical Research Coordinator from the Mt. Sinai IBD Center reached out to Nicole to see if she’d be interested in participating. The researcher told her digital devices were being used to learn the relationship between Crohn’s disease symptoms and stress to try and predict the onset of flares.
“I was given detailed information about the study and instructions on downloading the app. The researchers provided me with an Oura ring, an Empatica EMBRACE wristband, and a Bodyport scale. I completed various surveys and tasks within the Stress Study app each day. Whenever I had a bowel movement, I would note the characteristics of the stool on the Pooply app based on the Bristol stool scale. The Rescue Time app was optional, and I chose not to use that one,” Nicole explained.
Daily points were awarded for wearing the Oura ring and Empatica wristband, using the Bodyport scale, answering survey questions, and completing tasks on the study app. Nicole received extra “boost points” for using the devices multiple days in a row.
“Every two weeks I gained points for completing a video diary and a cognition task. About five times during the study, I completed a Calprotectin stool sample at home through the IBDoc app. I had a support team and check-in calls each month to answer questions about my mental health and medications. There was also a study visit every three months to complete additional surveys about my health and Crohn’s disease.”
By the end of the study, Nicole earned more than 20,000 points for completing these tasks and eventually received 5 stars for being a “Groundbreaking Contributor” to science. She says the point system was a big motivator and a fun challenge. The study lasted 9 months. Nicole was compensated $400, and she got to keep the Oura ring.
Wearables provide a “new voice of objective data”
Up till now, those with chronic diseases have had to use their memory and feelings to convey their diseases. The wearables offer a new voice of objective data for themselves and for their physicians about what precisely occurred.
“In this study of Crohn’s disease, we were more interested in unlocking the link between stress and flares in Crohn’s. This is part of a larger set of feasibility studies to build for individuals a “Stress Load Navigator” for we note a tight connection between not just inflammatory bowel disease, but also diseases as diverse as diabetes, heart attacks, arthritis and even Alzheimer’s,” said Dr. Friend.
Marco Altini, Founder of HRV4Training, advisor at Oura, and Guest Lecturer at VU Amsterdam, says recent advancements in wearable technology are making it possible to move away from the lab and monitor our physiology continuously, in real life, when and where it really matters.
“In the context of many chronic conditions, the ability to monitor our own, individual changes in resting physiology over long periods of time, and in relation to symptoms or other makers, could finally help us better manage our health,” said Marco.Devices such as the Oura ring can monitor accurately resting heart rate and heart rate variability over time. These signals are tightly coupled to our stress response, which is often an important part of the picture when managing our health.
Participating in research as an IBD mom
Since there is a genetic component to IBD, Nicole says she worries that her children could show signs of the disease in the future. She’s been very open with her children about the challenges she’s faced with the disease.
“I want to model resilience for them so they can see how to navigate difficult situations. By participating in research, I want to show them that we have a chance to use these challenges to help others and make a difference in the future.”
Nicole says it’s encouraging that wearable devices could potentially predict the onset of flares, which might offer faster treatment to prevent the escalation of inflammation and disease progression.
The importance of contributing to IBD research
Nicole’s hope is that by sharing her experience, it will inspire others to participate in IBD research and encourage more funding for these types of initiatives.
“Our research contributions as chronic illness patients have so much potential to benefit others in the future. This study was fascinating, and it was truly a pleasure to participate in the research.”
She says by taking the daily surveys and performing the tasks, it made her feel like someone was paying attention to her struggles.
“It gave me an incentive to be strong, thinking that my challenges could be helpful to IBD research!”
Nicole’s final thoughts on wearable devices
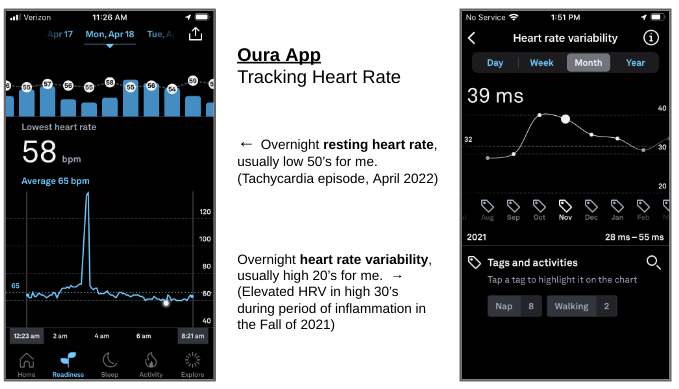
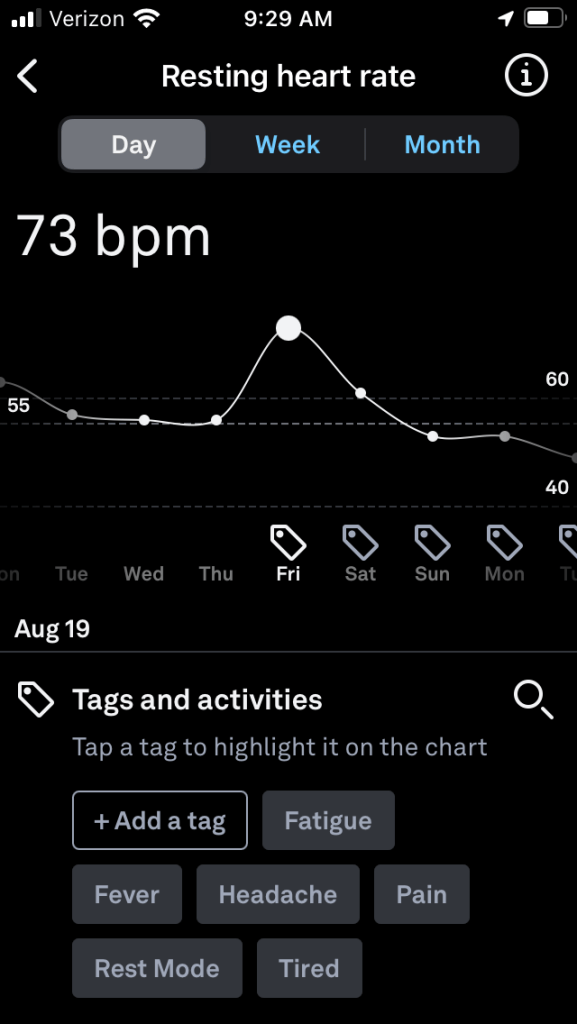
Wearable devices present a great opportunity for patients to monitor their health and provide feedback to healthcare professionals. “Since the study, I’ve continued to wear the Oura ring, and it’s been especially helpful to follow my progress as I rebuild and strengthen my body. Each morning I can check my readiness level to see how my heart has recovered from various activity levels. My sleep analysis has also been helpful for establishing a healthy sleep routine.”
The Oura ring has captured periods of strain on my body, and I can often tell when I’m getting sick with slight elevations in body temperature and resting heart rate. “During my Covid infection, the ring app even showed a fever spike along with elevated heart rate. I’ve also been able to monitor episodes of tachycardia with the help of the Oura ring and a KardiaMobile device, which is a single-lead portable EKG connected to a phone app. In addition, we have a pulse oximeter at home to monitor heart rate and oxygen saturation.”
With so much information to collect on our health, these devices can be overwhelming and anxiety provoking. “During the study, I was constantly monitoring my symptoms which led to a hyperfocus on my disease. Weighing myself each day also contributed to anxiety. Each time my weight dropped a little bit, I got worried and discouraged. The constant focus on weight can also contribute to issues with body image, and I’ve since decided to just weigh myself at medical appointments. For anyone considering wearable devices, it’s very important to keep moderation in mind.”
When we step out into the world, we need navigation tools. The same goes with wearable technologies. Soon, we’ll be able to use the data taken directly from our own bodies, during our day-to-day lives, to follow what is happening and help us to better navigate our own health paths. According to Dr. Friend, last year almost half of American adults were wearing some form of smart watch, and as of Spring 2022 more than 90% of smart watch users state they use health related apps to follow their health.
Interested in becoming a citizen scientist like Nicole? Learn about additional research opportunities:
In the future, Nicole plans to contribute to the Mount Sinai Million Health Discoveries Program which aims to understand how to treat different diseases in patients of all races, ages, and genders. She has also been invited to collaborate with Nutritional Therapy for IBD whose mission is to improve the lives and outcomes of patients with Crohn’s disease and ulcerative colitis through evidence-based nutrition.
Closing thoughts
The information collected from wearables can be a gamechanger for us as patients. Many of us call our doctors or go to the ER based on symptoms, but if we have remote monitoring via such devices, we could perhaps prevent this disease from spiraling. Kudos to Nicole and the many other research participants who are helping to push the needle and change the future of what it means to live with IBD.
“To me, that’s not just hope. That’s the future of managing this disease better and truly owning our Crohn’s or ulcerative colitis,” said Tina.
Healthcare for those with IBD in the LGBTQIA+ community looks a bit different. IBD often affects young adults, many of whom are just beginning to become comfortable in their sexuality and gender identity. This can be especially hard for LGBTQIA+ folks, who have already had to work through stigma and discrimination, and then have the additional burden of a new diagnosis of IBD. The LGBTQIA+ community is a big, diverse group of people and each person is unique.
This Pride Month on Lights, Camera, Crohn’s a close look at the most common concerns and patient experiences, helpful guidance to support the LGBTQIA+ community, tips for finding and communicating with your care team about your sexual orientation, and exciting news about how the University of California-San Francisco Medical Center is working to provide a safe space for patients.
You may not be aware that IBD symptoms can affect sexual function, colectomy and J-pouch surgeries can impact receptive anal sex, transgender people with active pelvic inflammation may have issues undergoing bottom surgery as part of gender affirming, and much more. The mere act of communicating with your care team can be an overwhelming and daunting experience.
Coming soon: An IBD Clinic specifically serving the LGBTQIA+community
Dr. Justin Field, MD, University of California, San Francisco, is passionate about supporting IBD patients who are part of the LGBTQIA+ community, as a gay man himself, he’s on the forefront of making the UCSF Medical Center one of the first in the country to have an IBD clinic geared towards treating IBD in the LGBTQIA+ community.
Currently there are two other clinics in the U.S. that specialize in treating LGBTQIA+ IBD patients, the Mayo Clinic in Rochester, Minnesota, run by Dr. Victor Chedid and Capital Digestive Care in Washington D.C. Dr. Jessica Korman, MD, specializes in LGBTQIA+ patients with all GI issues, including IBD. She also does anal cancer screenings.
“The clinic at UCSF is set to open this Fall and will offer comprehensive IBD care to anyone who is interested and will be a safe and inclusive environment where everyone involved in patient care will have special training in the unique needs and concerns of LGBTQIA+ patients. The clinic will offer screening for anal cancer, which is increased in patients with IBD, in men who have sex with men (MSM), patients living with HIV, those who have receptive anal sex, patients with prior cervical or vaginal cancers, and in those on long term immunosuppression,” said Dr. Field.
The clinic will also offer coordination between Gastroenterology and other specialties such as Colorectal Surgery and Transgender Care. For people who are interested, UCSF will offer the ability to participate in research that adds to the knowledge base about the unique needs of LGBTQIA+ people who have IBD.
“This clinic came from the realization that LGBTQIA+ folks often have unique needs that aren’t always addressed in other traditional settings. Also, patients often feel hesitant to fully discuss their sexual orientation and gender identity with healthcare providers due to fear of stigmatization or being treated differently. I wanted to create a safe space where patients can feel comfortable and empowered to be open with their healthcare team, and where they can receive the relevant expertise to meet their needs,” says Dr. Field.
Because LGBTQIA+ people have so often been left out of research (by not including sexual and gender diverse identities in research studies), having a dedicated LGBTQIA+ IBD clinic helps improve medical knowledge about how IBD affects LGBTQIA+ individuals, by allowing more patients to choose to participate in research.
“I have received incredible support from the University of California – San Francisco to start the clinic. The clinic continues to be a work in progress, and I’m continuing to seek out a wide variety of patient and provider input to ensure the clinic effectively serves the community,” explained Dr. Field.
Living with the stigma of IBD and being LGBTQIA+
CC Springhetti was diagnosed with ulcerative colitis when she was 12. She’s has an ileostomy and says sometimes she jokes that the universe keeps punishing her with stigmatized labels.
“I’m a woman, gay, AND I have a disability now?! In all seriousness, I try to view all my labels as gifts. They each make me who I am, and though it’s taken me some time to get to this point, I’ve learned to be proud of who I am and what I have. I know that sharing my life helps normalize and de-stigmatize IBD and queerness. Representation is so important, and being able to show up exactly as I am to show that you can be queer with IBD and still live a full life is a precious gift I have been given.”
CC and her wife share their life online and have been the target of extreme hate and prejudice. They’re received hundreds of threats.
“It can be draining to keep up with the amount of comment/message removal needed to keep our internet pages safe for young viewers and it’s incredibly disheartening on a regular basis. I sometimes give myself several days away from social media just to clear my mind – the hate and threats cause so much stress, and it can be difficult to separate internet life from real life. Those of us with IBD know how stress can affect our bodies, so this is a constant issue I am still working through every day.”
CC says when she’s admitted to the hospital, she’s dealt with the stress of her partner not being taken seriously of being allowed to make big decisions during emergency situations.
“We live in the south in the United States – it sometimes can be difficult for us to know who is able to separate their work life from their personal beliefs. When you’re in a hospital setting there really is no knowing, and this is something we always try to stay vigilant about and are very communicative with our care teams about what our needs and wishes are.”
The impact of IBD on sexual function
Brad Levy started to experience IBD symptoms in January 2022. He was diagnosed with Crohn’s the following month. His dad has ulcerative colitis, which sped up the diagnosis process significantly. Along with having Crohn’s Brad is a married gay man and a dad. Shortly after his diagnosis, Brad started to worry about how his disease would impact not only his life in general, but his intimacy with his husband.
Dr. Field explains why IBD can have such a big impact on the sex lives of LGBTQIA+ people.
“Receptive anal sex is an important part of sexuality for both LGBTQIA+ and non-LGBTQIA+ people but is especially important in this community. IBD often involves inflammation around the anus or in the rectum and this can make sex difficult or painful. For transgender folks, active inflammation in the pelvic area can affect their ability to undergo gender affirming surgery, so it’s especially important to address any pelvic inflammation.”
Brad says, “There is some shared stigma around IBD and being a gay receptive partner. Specifically, within the gay community there can often be some unrealistic expectations about how “cleaned” out you should be before engaging in receptive sex. The reality is though that shit happens, quite literally. The shame and judgment around a critical and natural bodily function such as elimination needs to end.”
Overcoming the fear of judgement and finding a care team you can openly communicate with
Talking about sex, sexual orientation, and gender identity can be scary as a patient, because often those in the LGBTQIA+ community have prior experiences telling people about their sexual orientation or gender identity which may have been met with rejection or judgement.
“Historically, the medical community has treated the LGBTQIA+ community poorly and considered LGBTQIA+ identities as pathologic. This historical context is important because there are very logical reasons patients aren’t comfortable talking about this with their doctors. In some areas, it truly isn’t safe for LGBTQIA+ individuals, especially the trans and non-binary community,” said Dr. Field.
Now more than ever, there are lots of affirming healthcare providers. Individual providers and practices can take measures to ensure a LGBTQIA+-friendly healthcare setting (For example, by following these recommendations put forward by the American Medical Association.
Demonstrating to patients that they are in a safe space to talk about their sexuality or gender identity can go a long way in facilitating sensitive conversations. Providers can seek additional education on sexual health in gender and sexual minority patients, so that they feel more capable of addressing the needs of the IBD community.
Dr. Fields says, “Providers should know it’s ok to make mistakes when it comes to addressing diverse sexual orientations and gender identities. What’s most important is that we acknowledge the mistake, apologize, and move on.”
CC is a firm believer that your doctor should be someone you never lie to. Honesty will help you navigate problems and solutions in a sensitive manner.
“I remember I was nervous to share with my gastroenterologist that I was gay. Whenever I referred to my partner and he responded back to me with questions or comments, he would always say “boyfriend” or refer to my partner as “he”. It felt scary to correct him (especially after all of these years) so I just didn’t. I was nervous it would embarrass him or make him feel silly, and I always want to protect people from that when I don’t feel they deserve it,” she said.
Then one day, CC was at a different doctor and she made sure to share to share that she was married to a woman and had been in a same-sex relationship exclusively for a number of years.
“I had this doctor add this information to the top of my medical chart. Now when I go to any doctor and they pull up my chart, they can see that I’m gay and can provide sensitivity to me in that way when speaking to me.”
Seeking out LGBTQIA+ affirming healthcare providers
Patients can feel empowered to seek out LGBTQIA+ affirming healthcare providers like Dr. Field.
Find providers with a special interest in LGBTQIA+ health. Patients can also look at lists such as the LGBTQIA+ Healthcare Directory.
Patients should feel empowered to be their own advocate. It’s a patient’s right to have their sexual health needs met and to receive care that is affirming of all genders.
Patients can bring a list of items that they want to discuss to a visit, and it’s best to mention those at the beginning of a visit to help set the agenda. It’s also always ok to seek a second opinion if you feel like your provider hasn’t gotten a satisfactory answer to your questions or if you feel another provider perspective would be helpful.
“Having a GI doctor you trust and feel comfortable enough to discuss your sexuality with is so important. When having receptive anal sex, things happen sometimes, such as tears, and you want to be able to talk with your GI doc openly so you can triage whether something is related to your IBD or not,” said Brad.
Additional IBD screenings for the LGBTQIA+ community
According to Dr. Field, men who have sex with men that are living with HIV should be screened for anal cancer.
“Other at-risk groups for anal cancer are men who have sex with men over age 40, people with prior cervical or vulvovaginal squamous cell cancer, patients that have receptive anal intercourse, and those with multiple sexual partners,” he said.
The risk of anal cancer is increased in patients with IBD, and doctors are continuing to learn more about this risk through ongoing research studies. Screening for anal cancer is with a rectal exam and a swab of the anal canal, called an anal pap smear. If these are abnormal, they must be followed by a procedure called a High Resolution Anoscopy, which is the best test for detecting anal cancer and its precursor.
“Anal cancer is caused by HPV, and there is a vaccine against HPV. Anybody who has not received the HPV vaccine, regardless of age or gender, can talk to their doctor about HPV vaccination. Currently, the CDC recommends HPV vaccination regardless of gender up to age 26 to prevent HPV related cancers, and the vaccine can be given up to age 45 on a case-by-case basis, if it’s felt it would benefit,” said Dr. Field.
Brad lives in the Chicago suburbs. As a result, he says the attitudes towards the LGBTQIA+ community are generally that of acceptance and love.
“I have always had a gay primary care physician because I want to make sure I am comfortable discussing any health issues with them. My GI is also aware of my sexuality, and we’ve had candid conversations about what intimacy looks like during a flare and what vaccines I should consider. For example, my GI recommended I receive the Gardasil HPV vaccine based on my sexuality and increased risk.”
Other cancer screenings to keep in mind are Colon cancer screening for all patients, Cervical cancer screening for patients who have a cervix, and skin cancer screening for all patients who have received immunomodulators, small molecules, and biologics.
“Much of the existing research on things like sexual health and surgery in IBD didn’t ask participants about their gender identity, sexual orientation, or typical sexual practices. This can leave both patients and providers at a loss for answers to sexual concerns,” said Dr. Field.
More and more, sexuality and gender identity are being included in research studies, and this will paint a clearer picture about how many LGBTQIA+ people are impacted by IBD, and how the course or experience of IBD is similar or different between LGBTQIA+ and non-LGBTQIA+ individuals.
Juggling a love life and fatherhood with IBD
Brad and his husband have been together for 13 years, so luckily communicating about his IBD has come easy.
“But I can recognize for others, in shorter relationships or dating, this isn’t always the case. All I can recommend is transparency and having a partner you feel you can be honest with. There will be times (such as a flare) where intimacy will look different. You want your partner to know that it’s because of your IBD activity and not because of them or some issue with your relationship,” said Brad.
As the years go by, Brad says the more authentically he lives, the happier he is. For him, that means living as an out gay man who has an amazing family. It also means living with Crohn’s disease, Anxiety, and Depression. Brad is open about his health struggles with family, friends, and close colleagues/bosses. He says transparency has served him and his relationships well.
As an IBD Dad to a five-year-old girl who is on the spectrum, Brad says focusing on self-care to help manage stress makes all the difference.
“Focusing on self-care enables me to show up as an active and healthy dad. My self-care includes hopping on my Peloton (#ThatDadBrad for the Peloton readers), bi-weekly therapy, monthly massages, and getting my nails professionally done. While not all these activities are for everyone, I strongly encourage folks to pour into their own cup or put on their own mask first. You can’t fully show up for you me kids and your family if you’re not grounded and the healthiest version of yourself, whatever that looks like for you.”
Brad wants to reiterate that his experience as a cis gay white man is “only one voice (and a privileged one at that) out of the vast and vibrant LGBTQIA+ community.” You can connect with Brad on Instagram at: @bssl.
CC says there are a number of ways our IBD community can show support. You can follow CC on Instagram at: @ccspringhetti.
“We’re all human, and I would encourage the IBD community just like I would encourage any community to show your support during Pride month and all year long through any means appropriate for your situation. Support LGBTQIA+ owned businesses, hang a Pride/Progress flag, post your support on social media, or even attend your local Pride events! If you’re ever looking to support a good LGBTQIA+ charity, I always suggest The Trevor Project.”
Certain roadblocks and issues that are a concern to one person, may not bother another. Just like every IBD patient, regardless of sexuality, the experience is unique. We all need to feel seen, understood, and respected, as one united IBD family.
Dr. Field’s views are his own and do not represent the University of California San Francisco.
One in three people with inflammatory bowel disease (IBD) has iron deficient anemia. This common, but often underrecognized and undertreated extra-intestinal manifestation impacts so many of us. You may wonder why. The reason is three-fold.
First being that long-term irritation and inflammation in our intestines can interfere with our body’s ability to use and absorb vitamins and minerals properly. When our intestines don’t absorb enough iron, folate, B12 and other nutrients, our bodies are unable to create more red blood cells. Those with IBD are also at risk for blood loss—both visible and microscopic and we often don’t eat as much iron-rich foods. So, what can we do to boost our reserves and increase our energy? How as patients can we better advocate for ourselves to stay on top of screenings? This week on Lights, Camera, Crohn’s an in-depth look at anemia in both adult and pediatric patients and input from Dr. Alka Goyal, who recently co-authored a major study on pediatric anemia.
Symptoms to watch out for
As someone who was diagnosed with Crohn’s disease in July 2005, I experienced anemia long before my diagnosis. I often wonder if my anemia was a warning sign of the larger issue, my IBD. In fourth grade, I fainted on the teacher’s desk while waiting for her to look at an assignment. Throughout my life I’ve experienced light-headedness, weakness, black outs, and extreme fatigue. My symptoms were never addressed prior to finding out I had Crohn’s. A simple lab test would have shown all along. When I was diagnosed with IBD and hospitalized my hemoglobin was a 7. To give you an idea, people are given blood transfusions once they drop to 7 (or below). Throughout my 18 years with IBD, my hemoglobin was rarely ever in “double digits”—and I took over the counter iron supplements for years.
Once I had my bowel resection surgery in 2015, my iron panel slowly started to improve. It takes time. Last month, I had my “highest” hemoglobin since diagnosis, ever—12.9 (which really isn’t that high, but I’ll take it!). It’s difficult to put the fatigue caused by anemia into words, but you can physically tell such a difference when your iron panel is where it needs to be.
When you have anemia, you have less blood carrying oxygen throughout your body. The most common symptom is feeling tired or lethargic. Other symptoms include dizziness, headaches, feeling cold, pale skin, being irritable, and shortness of breath. Not everyone experiences symptoms, so it’s important as a patient to speak with your GI about making sure that when you get labs, an iron panel is part of the workup.
Screening for Anemia
Anemia screening is driven by patient symptoms and/or a care provider’s recognition of lab abnormalities. It’s important to note that anemia is not *just* a low hemoglobin, all the lab figures matter. With iron deficiency anemia (IDA), red blood cells are smaller and paler in color. Your hematocrit, hemoglobin, and ferritin go hand in hand. Ferritin helps store iron in your body. Iron deficiency anemia is the most common type of anemia and is caused by a lack of iron-rich foods, malabsorption, and blood loss.
Other types of anemia include vitamin deficiency anemia and anemia of chronic disease. Vitamin deficiency anemia is a result of poor absorption of folic acid and vitamin B12. My GI has me on daily folic acid. Luckily my B12 has never been an issue, but it’s worth a discussion with your care team. If you’re deficient, you can receive B12 injections. Diseases such as IBD and other inflammatory diseases can interfere with the production of red blood cells. When this happens anemia can often only be resolved once remission is reached or inflammation calms down.
In order to address the need for improved patient management, the Crohn’s and Colitis Foundation created the Anemia Care Pathway (ACP) to standardize clinical management of anemia in IBD. This pathway helps to identify high-risk patients so that timely intervention and care can be provided. The hope is that this pathway will improve patient outcomes and our quality of life. Patients are assessed based on the severity of their anemia and iron stores to determine the type of iron therapy (intra-venous or oral) that is best suited.
The importance of accurately diagnosing the type of anemia you have
According to the PubMed study, Management of Anemia in Patient with Inflammatory Bowel Disease, despite iron deficiency anemia impacting one third of IBD patients, “more than a third of anemic ulcerative colitis patients are not tested for IDA, and a quarter are not treated with iron replacement therapy.” While oral iron tablets are effective for treating mild IDA, it’s not for everybody. The study also notes, “it is important to recognize that ferritin is elevated in chronic inflammatory states and among patients with active IBD, ferritin levels less than 100 are considered to be diagnostic of iron deficiency.” Iron infusions have a solid safety profile and can be used to help boost your iron stores and prevent future iron deficiency.
While treatment goals are well-defined, selecting a treatment is often not as straightforward. The PubMed study previously mentioned recommends that all IBD patients with IDA should be considered for oral supplement therapy, whereas someone with clinically active IBD, or someone who is not tolerant of oral iron, with hemoglobin levels below 10 g/dl be given IV infusions therapy. While oral iron is safe and affordable, some people experience GI issues from oral iron, it can also increase inflammation and contribute to flares in patients who are not in remission.
“Though intravenous (IV) iron is substantially underused, it’s considered first-line treatment for patients with active disease, severe anemia, oral iron intolerance, and erythropoietin (a hormone secreted by the kidneys that increases the rate of production of red blood cells in response to falling levels of oxygen in the tissues.)
Anemia in pediatric IBD patients
The most common cause of anemia in children with IBD is iron deficiency. It results from chronic blood loss, poor absorption, and less intake of foods that are rich in iron due to poor appetite, food selection or intolerance. According to the World Health Organization’s definition of anemia, prevalence in the pediatric IBD population ranges from 44% to 74% at diagnosis and 25% to 58% at 1 year follow-up.
Anemia can be both a biomarker of disease activity and a subtle or debilitating extraintestinal manifestation. According to, Anemia in Children With Inflammatory Bowel Disease: A Positi… : Journal of Pediatric Gastroenterology and Nutrition (lww.com), “newly diagnosed children with IBD are more likely to have IDA in contrast to anemia of chronic disease. No significant improvement in the hemoglobin was observed when patients were assessed after 13 weeks of induction therapy with conventional drugs that included nutritional therapy, azathioprine, steroids, and 5-ASAs. Despite the recognition of anemia, fewer than half of anemic patients received indicated iron therapy.”
Dr. Alka Goyal, MD, Clinical Professor of Pediatrics, and Interim Associate Chief of Clinical Affairs at Stanford University of Medicine, co-authored this study on pediatrics and tells me the key message is that anemia is the most common extraintestinal manifestation in patients with IBD.
“More than 2/3rd of children with IBD are anemic at the time of diagnosis. The treatment of IBD alone does not resolve anemia, which can be associated with a variety of symptoms. Persistent anemia indicates a more aggressive disease course,” said Dr. Goyal.
Hemoglobin levels across genders and race
According to the study, hemoglobin levels are similar in preteen boys and girls; however, after menstruation, the cutoff hemoglobin in girls is lower than in boys and is even lower in pregnant versus nonpregnant women. The African American population tends to have lower hemoglobin concentration compared with Caucasians.
“Although the normal range of hemoglobin varies with age, gender, and race, a hemoglobin level below 10 g/dL is considered to be consistent with moderate anemia and below 8 g/dL as severe anemia, whereas in young children below the age of 5 years and pregnant women, a hemoglobin level below 7 g/dL is deemed as severe anemia.”
Dr. Goyal says it’s important to monitor anemia regularly in all patients with IBD.
“Anemia can be an early indicator of active disease or an impending flare of IBD. When the body has inflammation, the iron stored in the body cannot be metabolized to help manufacture more hemoglobin and additionally there is suppression of normal blood production, resulting in anemia of chronic disease.”
Other causes include vitamin deficiency, medication side effects, or breakdown of red blood cells due to other inherited or disease-related complications.
“Patients should be monitored not just by symptoms, but also by blood tests like complete blood count, Ferritin, and markers of inflammation like CRP every 3 months when they have active inflammation and every 6 months when patients are in remission,” Dr. Goyal explains.
Bringing a dietitian on board to help
Registered dieticians who specialize in IBD can advise patients and families about foods that contain iron naturally. The iron in meats is more readily absorbed than that present in a plant-based diet.
Dr. Goyal says another important concept is food pairing.
“With food pairing, iron-rich foods like spinach, kale, and Swiss chard are ingested with citrus fruits, melons, or vegetables like bell pepper, broccoli, beans, carrots, tomato, etc. Avoid simultaneous ingestion of foods rich in dietary fiber, soy, cereals, coffee, tea, and animal protein like milk, and eggs. Children should consume at least three servings of iron-rich foods like fortified cereals, red meat, tofu, etc. The recommended daily intake of iron in healthy children is 7-11 mg daily,” says Dr. Goyal.
Treating anemia in the younger IBD population
When it comes to treating anemia, Dr. Goyal has helpful tips. She says it’s important to recognize and treat anemia along with the treatment of IBD and vice versa.
Oral iron can be tried in mild anemia when the hemoglobin is above 10 gm/dl, preferably given with juice or citrus fruits.
Avoid taking oral iron multiple times a day or in high doses.
Brush your child’s teeth after taking liquid iron.
If your child experiences side effects including abdominal pain, nausea, or constipation, and/or has no significant improvement with oral iron, it is safe to give intravenous iron.
Timely treatment may save a blood transfusion. excessive unabsorbed iron is not healthy for our digestive system, so avoid overdosing on oral iron.
Patients with persistent anemia lasting for three or more years were noted to have a higher prevalence of more severe and complicated disease (stricturing and penetrating phenotype) with a greater need for surgical intervention.
Whether you’re an adult patient or a caregiver to a child or young adult with IBD, be mindful of the importance of keeping tabs on whether anemia is creeping in and hindering you or someone you loves quality of life. Have the conversation with your GI and make sure you are being vigilant and proactive about doing all you can to prevent, manage, and treat anemia.
When you have IBD and you start to notice GI symptoms going awry, it’s easy to allow your mind to start racing and your worries to become all-consuming. This past week I did an in-person patient advocacy speaking engagement, came home, and started feeling extremely fatigued. Within an hour, I vomited, and the diarrhea began. Not to be TMI (is that even a thing when you have IBD?), but this wasn’t just “normal” diarrhea. It felt like I was prepping for a colonoscopy. Straight water-like diarrhea that hit me like a ton of bricks. I couldn’t stop. In that moment, I thought about how I was on an antibiotic for a sinus infection and bronchitis and knew that alone, with Crohn’s disease, put me at greater risk for C.diff.
For those who don’t know, “C.diff” or Clostridioides difficile is a bacterium that causes an infection of the large intestine (colon). Symptoms can range from diarrhea to life-threatening damage to the colon. According to the Mayo Clinic, C.diff typically occurs after or during the use of antibiotic medications. In the United States, about 500,000 people are infected each year.
The risk of C.diff and IBD
When I couldn’t stop going to the bathroom, I immediately contacted my GI. Being that it was 4 pm on a Friday, the timing of it all was challenging. She called me from home and said she normally wouldn’t be too concerned, but the fact I had just finished a course of prednisone while being on doxycycline put me at greater risk. She warned that if I had diarrhea the following day or if I had a fever at any time, that I would need to get tested for C. diff and go to the hospital. She put in orders so I would be able to do so and told me to contact the Fellow on staff if I had concerns over the weekend.
Saturday came and with the bathroom trips came unbelievable abdominal pain, reminiscent of what a bowel obstruction feels like. I could barely walk and was grasping my abdomen in pain hunched over. I had already called and spoken to the Fellow on call three different times. In that moment, my husband called his mom so she could watch our three kids and we rushed to the emergency room.
A study by the University of Michigan recently looked into the relationship between IBD and C.Diff. The study found that people with IBD are at an increased risk for C.diff, even if we haven’t taken antibiotics. It’s believed something about the IBD gut supports C.diff colonization and growth, but the actual relationship is still a bit mysterious. This study looked at a mouse model and found, “inflammation and changes in the gut microbiota associated with IBD promote C.diff intestinal colonization.”
For those of us with IBD, our immune system mistakes normal intestinal microbes as harmful invaders and attacks them, leading to inflammation in our guts. The cause of C.diff is similar, with the immune system, microbiota, and C.diff itself playing a role in infection.
The burden of C.diff on the IBD population
According to an interview in Pharmacy Times, we’re at greater risk for C.diff when our IBD is active. This is because active inflammation changes the flora in our microbiome and puts us at greater risk for developing infection. In this piece Bincy Abraham, MD, MS says we see C.diff in both ulcerative colitis and Crohn’s disease patients but tend to see it more in those with UC since the colon is directly impacted.
Get this—A database of patients with IBD showed 10% will have at least one C. diffinfection over the course of their lifetime. Half will have more than one. WebMD shares that C.diff infection begins with frequent, watery, foul-smelling bowel movements and cramps in your abdomen. When I was unsure if I had C.diff that was the number one question I kept getting asked. People told me the smell was very unique—like a barnyard, sour smell. Thanks to my sinus infection congestion, I had no idea what it smelled like. But—it’s important to look out for that if symptoms present. Medical professionals told me they can tell right away by the smell, if it’s C.diff.
Symptoms of C.diff
While watery diarrhea with a strong odor is the main indicator—there are other symptoms to watch out for:
-Abdominal pain and cramps
-Fever (I had the chills, but my GI assured me that was due to dehydration from the diarrhea)
-Nausea and/or vomiting
-Dehydration
-Loss of appetite
-Weight Loss
-In severe cases, blood or pus in stools
For anyone with IBD, these symptoms are reflective of what we experience with an IBD flare. So, it can feel especially concerning in the moment as you try and figure out what’s going on.
My rough ER experience and finally getting tested
I always him and haw and dread the thought of seeking medical care at the ER. It brings about so many emotions and past trauma. But in this case, I knew I needed to wave the white flag and get to the bottom of what was happening. After waiting four excruciating hours in the ER, I wasn’t sure how much more I could take. I was moaning in pain and hobbling back and forth repeatedly to the bathroom. Bobby was using a wheelchair to push me around. The nurses in triage were incredibly unprofessional and lacked any empathy. It was like nothing I’ve ever experienced. I was basically reprimanded for showing emotion about my pain and told others had it worse. It was despicable. She waved her “RN” badge in my face and said she had a woman die from a pulmonary embolism while in the waiting room and she didn’t make a peep. As I was crying, I yelled back, “I’M NOT A WIMP! I have Crohn’s disease!”
Once I was finally brought back to a room, the same nurse acted sweet as sugar. Gag me. The ER doctor had no clue what was going on. I was taken for a CT scan with contrast while in the waiting room and the young doctor walked up to me all cocky and said, “ So, you have an ileostomy.”…I said, no I don’t have an ostomy. He then proceeded to say, “Oh, so you had a reversal.” NO. I had bowel resection surgery. The fact the doctor was clueless to IBD and thought that because I had an anastomosis indicated a reversal (even though I have Crohn’s) was scary. I was given Zofran, fluids, and Dilaudid and was told it was most likely a stomach bug, but that they would like to do a stool sample to rule out C.diff.
Unfortunately, since I had literally shit my brains out in the ER for hours, I had nothing left. I hadn’t eaten in almost 30 hours. By the grace of God, around midnight, I was able to go. I was so grateful to have a stool sample and get some answers. The shift changed and a new doctor walked in. She was empathetic, kind, and knew her shit about IBD. I felt an immediate sense of relief. She told me they were going to do one more round of Zofran, fluids, dilaudid and add in Benadryl and Droperidol for anxiety and to calm things down and if that didn’t help, I would be admitted. Luckily, that heavy hitting dose of IV fluids and meds did the trick and I was finally comfortable and able to go home around 1:30 a.m., knowing that I’d get the C.diff result the next day.
Despite testing negative for C.diff, my diarrhea and excruciating abdominal pain lasted from Friday at 2 pm until Tuesday evening. This stomach bug was no joke and I always feel when you have IBD with a stomach bug, it’s next level.
The Patient Experience: What you had to say about C.diff
I ran a poll on Instagram, 307 people with IBD responded. Of that group, 37% have had C.diff. On Twitter, 147 people responded and 28% shared they had C.diff at some point during their patient journey. I was blown away by the hundreds of DM’s I received on Instagram when I asked for advice and was freaking out about the possibility of having it. I learned a great deal from all the insights shared. Here are some of the messages I received that I feel can benefit our community moving forward:
“I went through a case of C.diff this summer after two rounds of antibiotics and a round of steroids at the same time. I was miserable, only eating boiled potatoes with a little salt and bananas. Once I got meds (dificid), I saw improvement quickly. I also take Visbiome probiotic (prescription strength) and taking that regularly helped me in a period of waiting for results.”
“I had C.diff back in 2015…awful. It was so brutal. I was sick for over a month with it, just couldn’t shake it even with the crazy dosing of antibiotics.”
“Keep an eye on your temperature and if you’re running a fever with the diarrhea—that’s a big indicator.”
“I had C.diff on and off for four years and just got a fecal transplant in November and have been “cured” since. I’ve never thought C.diff was like the stomach flu/norovirus. C.diff to me is more like a bad IBD flare with some fever/chills and diarrhea that’s very distinct from whatever your “normal” IBD diarrhea may be.”
“I battled C.diff for a year. Ask for Vancomycin right away. It’s the best medication for it. Having Crohn’s and C.diff is a horrible combination. It caused me a lot of issues.”
“I had C.diff earlier this year. My symptoms included a very smelly gas, low-grade fever, abdominal cramps, and mushy stool. Pedialyte, broth, and tea helped a lot.”
“Every time I take antibiotics, I take saccharomyces boulardii (probiotic). The specific strain helps prevent C.diff.”
“C.diff is MISERABLE. I can normally smell if it’s C.diff. I’ve had it five times. Go to the ER and do not wait. It’s so horrible. It’s exhausting and being that sick is the worst. The pain is awful, too. No one ever discusses how much pain it puts people in.”
“I’ve had C.diff so many times. Output is like colored water, and I go 20-plus times a day. Mine way always a weird yellowish color. Going to the ER means a quicker diagnosis and for me I end up inpatient, too. With C.diff I’ve found liquid Vancomycin works best as it’s absorbed faster, the pills just went straight through me.”
“C.diff is super hard to get rid of, so fast treatment is key. I had a recurrent infection for nearly a year. I took Vancomycin 4x/day for a few weeks and eventually tapered down. I think it was just a nasty strain, but I eventually kicked it out.”
“C.diff is a doozy to have. The hardest part for me was keeping family and friends away as it’s super contagious, too. I remember a lot of Zofran. IV fluids and sleeping as much as humanly possible. Use wipes instead of toilet paper so your bum doesn’t get raw.”
“My brother had C.diff and the only thing to get rid of it was very strong antibiotics. Every time I’m on an antibiotic, it makes me very sick and puts me in a flare and I have choice but to start probiotics.”
“C.diff is rough and highly contagious. I had it right before I went on Humira. Make sure to bleach your bathroom and not to prepare food. My GI was super concerned about me giving it to my husband. My treatment was Vancomycin 125 mg orally 4x a day for 10 days.”
“I have been battling reoccurring C.diff for almost 2 years. Coming up on my second Fecal Transplant as the first failed. I was in a flare and absolutely nothing was working. Finally discovered underlying C.diff. Vancomycin changed my life. Within 48 hours I went from 15-20 bowel movements a day to 1-2.My doctors are baffled by how well I respond to it.”
“I’ve had C.diff more than once, the first time I waited almost too late to seek testing and ended up with dangerously low potassium, EKG changes, and was hospitalized. The second time I didn’t even know I had it until I was being worked up to join a clinical trial for my UC and had to do treatment, again. Liquid IV packets help ward off dehydration.”
“My son who has Crohn’s has had C.diff two times. Vancomycin with a long, slow taper was key to get rid of it both times. Wipe the bathroom down with bleach constantly.”
“C.diff is the actual worst. If you have it, skip Flagyl and go straight to Dificid. Flagyl made me SO sick. Like so much worse and it didn’t get rid of it…and that’s the case for multiple other people I know who’ve had it.”
“I had C.diff. I played the waiting game, and it was miserable. If your stool is completely watery and very foul smelling, then it’s C.diff.”
“I take Culturelle Probiotics Digestive Health Extra Strength whenever I’m on an antibiotic to prevent it.”
“I had reoccurring C.diff during the pandemic, a few months after my bowel resection, and for recurring months after. They would usually do a fecal transplant, but they were on hold because of COVID. It took months to get better.”
Kick C.diff to the curb
Ironically, while C.diff can be brought on by antibiotics, the only way to get rid of it…is to take more antibiotics. The three most prescribed are Vancomycin, Flagyl and Dificid. In severe cases, especially when toxic megacolon becomes an issue, you might need surgery to remove the damaged portions of your bowel. Other options for reoccurring infection include Fecal Microbiota Transplant (FMT), where donor stool is introduced in your colon. Probiotics and antibody therapy are often used as well. Certain antibodies are known to provide immunity against the toxins produced by C.diff. A combination of the medications actoxumab and bezlotoxumab can lower your changes of the infection coming back.
When I received the negative C.diff test result I felt such relief. So many of my symptoms aligned with the tall-tale signs, I wasn’t sure what to expect. The entire process has been such a learning experience and I hope that you’ve taken away some helpful nuggets of knowledge should you ever question you have C.diff yourself.
Parenthood when you live with a chronic illness like IBD can make you feel anxious, worried, and uneasy. As an IBD mom of three, I often connect with and share the stories of fellow women with Crohn’s disease or ulcerative colitis who have brought life into this world, despite their disease.
This week on Lights, Camera, Crohn’s we hear from a soon-to-be IBD Dad, Brad Watson-Davelaar. He was diagnosed with Crohn’s in 2001 at age 17. His name and face may look familiar, as I featured him in an article entitled: IBD Dads: What these patient heroes have to say about fatherhood. In that article, Brad was recently married and discussed his hopes for the future. Those hopes came to fruition, as he and his wife are awaiting the arrival of a baby girl in late June!
Leading up to the pregnancy, Brad was a bit scared of what fatherhood would look like while living with an unpredictable disease. Like many of us, Brad fears when his IBD will rear its ugly head again and cause him not to be as present as he wants to be, hindering his ability to be a “proper teammate” for his wife.
“Prior to my wife being pregnant, I think I was scared. I’ve wanted to be a dad for some time, but with the way my health has been over the last several years, the prospect of having kids while I was in that physical state freaked me out. Not because I didn’t want kids, but because I was worried I wasn’t going to be enough for them.”
Finding out he was going to be a dad
When Brad found out his wife was expecting he was elated. They had been trying for a few months and he was only a couple months post-op from his ileostomy and barbie butt surgery. While Brad knows life as an IBD Dad will have its ups and downs, he knows the highs will far outweigh any of the difficult days.
“I’m so thankful for Shawn, my stoma, for coming in and giving me a new lease on life. I feel ready to tackle this new chapter of our life and all that comes with it. The good, the bad, the ugly, and the beautiful.”
Since he’s lived with IBD for nearly 22 years and has been an ostomate for 6 months, Brad feels his patient journey has conditioned him to deal with the unexpected. He hopes to connect with fellow IBD dads who have paved the way before him and shown all that’s possible.
Discussing IBD with his daughter in the future
As his daughter grows up, Brad plans to be an open book about his battle with Crohn’s.
“I want to help her understand what IBD and ostomies are. Especially ostomies. It will take time, but I believe in being open and not hiding things. I want her to see that my IBD does not define me and show her how important it is to advocate for yourself.”
As Brad and his wife gear up to become a family of three, they are overjoyed and excited about the new chapter in their lives that is about to begin.
“I’ll be there to look after this wee little one, which will fill my heart with warmth. Being able to focus on her achievements will be a brilliant way to get through the rough days. In the past, it was the little things that got me through. Now, I’ll have all the little moments to continually push me.”
His wife, Sydney, feels so lucky to have Brad by her side as they experience this adventure.
“He had struggled so much over the last couple decades, especially these last couple of years and his perseverance and strength through it all makes me know that nothing is too big for him to overcome. I know he is going to be an amazing dad with so much love, nerdiness and laughter. His Crohn’s is a part of him, but his IBD does not define him. I know no matter what we can get through it together. Brad’s last surgery has definitely given him a new lease on life. With a baby on the way, his ostomy will help him be more present, active, playful, adventurous and helpful. I cannot wait to see him hold our little girl for the first time,” she said.
Raise your hand if you were told ‘diet doesn’t matter’ when you were diagnosed with IBD? Personally, the dietitian who visited me while I was hospitalized after my initial Crohn’s disease diagnosis in 2005, scared the bejesus out of me. I’ll never forget her sitting by my bedside with a clip board rattling off all the foods I would never be able to eat. Fruits, vegetables, anything raw, fried foods, wheat…the list goes on. I felt incredibly overwhelmed and defeated in that moment. Even though it was nearly 18 years ago, it’s a moment in my patient journey that is still upsetting to think about.
When Brittany Rogers, MS, RDN, CPT was diagnosed with ulcerative colitis in high school after suffering in silence for five years, she was 20 pounds underweight, exhausted, in pain, and experiencing frequent and urgent trips to the bathroom. She was put on medication and given little to no direction in the way of diet. Inspired by a nutrition class she took in high school and coupled with her own experience with trigger foods, Brittany pursued a degree in nutrition and became a registered dietitian. She strongly believes that learning about nutrition in college and applying that information to how she managed her IBD drastically changed the trajectory of her disease and quality of life.
Brittany as a teenager after her ulcerative colitis diagnosis.
The driving force behind Romanwell
Managing diet when you have IBD is complex and dietitians treating people with IBD need to be well versed in the latest research to provide safe and effective care. If you’re lucky enough to live near an IBD center, you may be able to see an IBD dietitian for a few visits through your doctor’s office. However, most people don’t have access to these centers of excellence and need more than one or two appointments per year to come up with a personalized nutrition plan to reduce their symptoms, improve their quality of life, and restore their relationship with food. Brittany’s practice, Romanwell, is tackling this issue head on by making expert IBD dietitians accessible to anyone, no matter where they live or work.
“I started Romanwell to be able to provide an exceptional level of care to people all over the country. I don’t want anyone else to suffer with symptoms the way I did for so long. Nutrition and lifestyle factors, such as stress, play a huge role in the symptoms we experience as patients. Unfortunately, people often don’t get the guidance they need to help them feel better,” said Brittany.
Diet research is quickly evolving and more and more providers are acknowledging the role of diet in managing IBD. However, there’s still a long way to go before GI’s everywhere start to refer patients to IBD dietitians routinely.
“If someone’s provider doesn’t have a referral for them, the Crohn’s and Colitis Foundation has a directory of IBD providers including a number of dietitians that they can search for and reach out to. The American Gastroenterological Association (AGA) is also putting together a directory of dietitians that will make finding a GI-specific dietitian much easier. Patients can also always reach out to me and I am happy to point them in the right direction if our practice can’t meet their needs,” she explained.
The unique support of an IBD dietitian
In an ideal world, patients would get support from an IBD-focused registered dietitian starting the day they’re diagnosed. Examples of where it would be helpful to work with an IBD focused RD include:
At diagnosis, IBD dietitians can help answer questions around what they can eat, talk about the definitions of trigger foods, pro-inflammatory foods, & anti-inflammatory foods, and examples of each. They can talk about foods associated with an increased risk for active disease, foods associated with increasing the risk for colorectal cancer, and what to eat during active disease & in remission.
If someone needs IBD-related surgery, dietitians can help them optimize their nutrition before & after surgery to reduce the risk for postoperative complications.
If they’ve lost weight without trying or have a decreased appetite, they’re at risk for malnutrition and would benefit from working with an IBD focused registered dietitian.
Anytime they’re having symptoms- dietitians can help manipulate their diet to reduce symptoms & improve overall quality of life
If someone want to improve their relationship with food, or have a history or active eating disorder, Romanwell can help them expand their diet, include more cultural foods in their diet, and use non-diet evidence-based approaches to reduce symptoms. Dietitians can also help people work on improving their relationship with food, their body, and their food-related quality of life
And, anytime someone has questions about their diet, or are worried about their nutrient intake, they should have access to an IBD-focused dietitian.
“We offer programs rather than individual sessions in our practice which gives us the time to help our clients make sustainable changes to their diet and lifestyle that will last them a lifetime. We build relationships with our clients, take the time to understand their needs, cultural influences on food, food preferences, and implement 100% personalized programs that work for them in their life. 95% of our clients work with us for 12 sessions, which we typically run over 3-6 months. In the beginning of a client’s program, we deep dive into their medical history, labs, supplements, labs, diet and their relationship with food and their body, and then set goals for the end of the program. We meet weekly or bi-weekly to make progress towards the clients goals, and are available via messaging throughout the client’s program to answer any and every question that comes up in the moments when they arise.”
Those of us in the IBD community know how isolating and upsetting it is when you’re in the middle of a flare. Brittany’s goal is to ensure that every client seen at Romanwell feels seen and understood and realizes that they’re not alone in this.
“I want patients to feel as though they’re our only patient and that they’re not alone in this. We believe all patients deserve that level of responsiveness and empathetic care. We want them to feel and know that we care about them and want the best for them,” she said.
Creating evidence-based research that’s digestible for patients
When Brittany started Romanwell, she noticed that no one was talking about the research around diet and IBD on social media and translating that research and know-how into approachable and actionable content that people could easily learn from and implement in their daily lives. You may hear the term “medical nutrition therapy”—this is evidence-based diet and nutrition treatment for a specific medical condition(s) provided by a registered dietitian.
“I started publishing research summaries and tips on my Instagram pages (@weareromanwell; @brittanyb_therd) and people seem to really resonate with the content. Reading research articles is intimidating! It’s hard enough for someone with a scientific or medical background to stay on top of all the findings, let alone someone from a non-healthcare background. I try to create content that summarizes what we know (and acknowledges what we don’t) from the research and always try to find a way that someone could get immediate actionable value out of the content – be that by tips or recipes or swaps for trigger foods, etc.”
When working with clients, Brittany finds it helpful to know that oftentimes education on diet is insufficient in encouraging behavior change- instead, she’s found is that people also need help applying that information to their life.
“For instance, research suggests Crohn’s disease patients who consume the most fruit and vegetables were actually 40% less likely to flare than those who consume the least. Patients we work with often have already seen a dietitian or have received a handout on what to eat that may include this recommendation of eating lots of fruits and vegetables. And although this is great information to share with Crohn’s disease patients, sometimes it’s not very helpful because they often want to consume more fruits & vegetables, but don’t feel safe doing so because it triggers symptoms, or they’re afraid of causing a blockage,” Brittany said.
When implementing this recommendation with her clients, she shares the study, but then looks at a person’s individual diet, asks them which fruits and vegetables they enjoy, and makes a plan together with the client to slowly add in more servings week by week in a methodical manner, sometimes adjusting the texture or amount of what they are eating.
“By the end of the program, most patients are consuming at or above the recommended fruit and vegetable intake and have a huge list of meal/snack ideas they enjoy and that are tolerated so they feel confident the diet is sustainable.”
Working to improve access for patients
The key to helping as many patients as possible get access to the care they deserve is getting their GI providers to refer patients to IBD dietitians and getting health insurers to cover the cost of those services so that patients can make meaningful and sustainable changes that will benefit them for a lifetime.
“I think there’s enormous potential for providers to help their patients have better outcomes by working closely with IBD dietitians and for health insurers to lower their costs by equipping patients with the tools and resources they need to stay out of the hospital. We’re trying to make this a reality by showing that our clients do in fact have better health outcomes after completing our program. We collaborate with every client’s existing GI care team to make sure the patient is getting the support and guidance they need.”
Romanwell is also measuring their clients’ outcomes and recently presented a poster at the Crohn’s and Colitis Congress showing some preliminary results. They’re hoping to submit the results to a peer-reviewed journal later this year.
“Our goal long term is for every patient with IBD to have access to an IBD registered dietitian and for programs like ours to be covered by insurance so everyone can access them,” said Brittany.
Counseling on the complimentary role of diet and lifestyle alongside medication
There’s a tremendous amount of information out there about the pros/cons of certain medications and/or alternative approaches to treatment that can be really confusing, misleading, and scary when you’ve just been diagnosed with a lifelong chronic condition. Some people worry about the side effects of medication and want to “heal their gut” using diet alone.
“We would never judge people based on the information they’ve read or the opinions they’ve formed about what’s best for their care, but we want them to know the evidence-based information so that they can make the best decision for themselves. We want patients to feel as good as they possibly can for as long as possible, so we love it when patients use nutrition along with medication and lifestyle factors to help them feel their best. We don’t believe it has to be either diet or medication, they work beautifully together!”
Looking to the future
Romanwell recently hired a second dietitian and has plans to hire more this year and next year.
“Our goal is to be able to thoroughly train dietitians in how to deliver exceptional care in a way that really helps patients achieve their goals. Unlike the training one might receive to practice inpatient or outpatient dietetics, our training program includes aspects of health coaching, counseling, motivational interviewing, intuitive eating and a weight-neutral approach to health. Since we’re a telehealth practice, we’re able to see clients on their terms and schedule, but that also means we can hire dietitians anywhere around the country which gives us access to much more talent than we’d be able to find locally.”
Romanwell pays for dietitians to pursue licensure in a number of states, so they can see as many patients as possible.
“I can’t even describe in words how incredibly fulfilling it is to get to help others with IBD. It’s been such an honor to help IBD patients get the care they deserve. I’m so grateful I get to do this for my job!”
Managing a chronic health condition often means receiving medication through an infusion or a self-injection. If the thought of getting or even giving a shot brings on tears and fears, you are not alone. It’s no surprise, two-thirds of children and one-fourth of adults have apprehension and anxiety around needles. So, what do you do when your child needs to take self-injections to manage their IBD? It’s a complicated and emotional process for everyone involved.
This week on Lights, Camera, Crohn’s we hear from a certified Child Life Specialist, a former pediatric patient who experienced self-injections, and two mothers whose children were diagnosed with IBD at a young age.
Phylicia Petit is a Certified Child Life Specialist at a Children’s Hospital in Minneapolis, Minnesota. She says being truthful with your child about the self-injection helps to build trust.
“Prepare your child for what they may experience in an age-appropriate manner. Use soft language. For instance, instead of saying “don’t move,” say “hold still.” Avoid phrases like “you’re almost done” and “it’ll just take 3 seconds”. Instead, praise your child for what was done well. Say, “you did a great job holding your arm still” or “thank you for telling me how you felt during that.”
Phylicia also says if you are calm and relaxed, your child will be calmer and more relaxed.
“Children often feed off their parent’s emotions. Use gentle and helpful words such as, “do the best work that you can do,” “you did it!” and “your job was to hold still like a statue, and you did that so well.”
Setting a routine
By giving the injections at the same time of day and in the same place, children cope best when they know what to expect. Children’s bedrooms are a place of comfort, so use a different space.
Phylicia says that by offering choices, it gives your child a sense of control. You can achieve this by saying “do you want the injection in your right leg or left leg?” and “do you want me to count to three?”
Reduce the pain
No matter your age, most people don’t enjoy needles. You can help reduce the pain for your child by using numbing cream. Contact your local pharmacist or GI to discuss topical anesthetics.
Buzzy uses vibration and ice to distract the brain from feeling pain.
Shot Blocker uses several blunt contact points to saturate the sensory signals around an injectionsite to distract from pain signals
“Don’t forget, you are a comfort to your child. Comfort positioning can be used by parents and caregivers during injections to reduce stress and anxiety in your child and help safely immobilize an arm or leg,” said Phylicia.
Comfort and distraction items:
Pacifier
Blanket/stuffed animal
Favorite TV show
Blowing bubbles
Squeezing a squish ball
Have your child sit up. Children are often more scared when they are lying flat. If you need help holding your child still, try holding them in your lap in a firm, but comforting position.
Practice deep breathing. Take a big breath through your nose, then blow out through your mouth. Have your child do this 3 to 5 times. To make this more visual for a little one, you can use a paper flower, pinwheel, or bubbles, and practice this before, during, and after the shot.
“As a former pediatric patient there were a couple of things that helped. Finding ways to numb the spot prior, whether it was ice or a numbing cream. Using a room, I could distract myself in (typically with a TV). If I was able to do it myself, I would set up the space, so I was comfortable. If my mom helped this still applied, but we talked through the entire injection to occupy my mind. It came down to comfort and finding ways to manage my anxiety around the shot. Over the years, it got easier, especially when we switched from the auto-injector to the manual shot,” said Natasha.
Stacy Dylan’s son was diagnosed with Crohn’s when he was only 2 years old. She co-founded the nonprofit Connecting to Cure Crohn’s and Colitis to help families cope and conquer IBD.
Here are Stacy’s tips for caregivers when it comes to injections:
Acknowledge that as a mama this is going to be hard. “You are going to feel sad and wonder why you and your child have to go through this. It’s going to be hard to watch them have anxiety about the shot and to feel pain. Get support for yourself for this.”
Try not to let your child see your pain. “Even though you are feeling this way, you know that giving them their meds is going to (hopefully, although it might take a few different meds to find the one that works) make them feel better and happy and more like themselves so approach your child with compassion and assurance about the potential of the meds to make them feel better.”
Try to have a calendar that shows when the shot is due but don’t talk about it too much if they are not bringing it up. “Remind them the day before or the morning of the shot and set a time to do it.”
There are practical things that may work to ease the pain of the shot. “Ice before and after. Rubbing the site after it goes in. Emla cream is a great numbing cream. My son is 22 and has been getting infusions, injections, and blood tests since he was 2 and numbing cream is our friend. We also used the Buzzy. It’s held on the skin before and after the shot and it stimulates the skin to reduce pain.”
Offer a reward. “At times I offered something post shot that motivated him when he was younger. Perhaps being able to watch a little more TV that day. Or a small new toy. Or a food treat that they can have, and it could be special for the shot day.”
Look into having a home nurse, if needed. “My son has been on so many of these meds since he was 7. When he was on Humira from age 9-10, it was before the citrate free (pain free) version and the Humira shot was very painful. It became too hard for me to do it and was too difficult for our relationship. It is rare that you can get insurance to cover a home nurse to do this, or to bring the child to get the GI office nurse to do it. We were able to pay a nurse to do his Humira shot for a brief period of time until he adjusted to it. It helped a lot.”
Cindy’s 12-year-old daughter was diagnosed with Crohn’s disease four years ago. She helps her daughter with weekly Humira injections and also offers helpful advice from a caregiver’s perspective about what it’s like to give your child an injection and cope with the difficult experience.
Don’t let your nerves show. “When I became responsible for giving the injections at home, I was nervous about doing it and it was important to me that I not transfer my own personal anxiety to my daughter. To this end, I really wanted to practice giving shots on anything other than her, so that when I had to inject her, I felt comfortable with what I was doing. Unfortunately, I only came upon the advice later, so it didn’t help me at the time…but I heard to use an already used syringe on a naval orange for practice.”
Do the injection in a neutral space. “A psychiatrist advised us to do injections in a neutral place. I had been giving my daughter her injections in bed because to me, this was the place where she was most comfortable. Unfortunately, she developed sleep problems, and our psychiatrist helped me understand that a negative association with the injection is not something that you want to combine with a happy place. In the summer, we inject it on our back porch and in the colder months we usually do it in our guest bedroom.”
Syringe instead of auto-injector. “We also find the syringe to be so much better than the pen. The pen made us feel tense and the lock was Pavlovian. The syringe allows for more control. No sounds. Go fast or go slow. My daughter takes a lot of comfort in her Buzzy.”
It gets easier. “Not better…but easier. For the first couple months, we had to physically restrain my daughter when injection day rolled around. It was soul shattering. However, we all did become used to what needed to happen and now (while not fun at all, it is a non-event). We do the injection now and move on with our day. We are thankful for the ease and convenience of injecting at home, and always thankful this medication is preserving my kid’s quality of life.”
It’s considered the most common surgical procedure for ulcerative colitis patients when medication fails to keep IBD under control. The ileal pouch anal-anastomosis (IPAA) or j-pouch, is created after a surgeon removes your colon and rectum and uses the end of your small intestine to form an internal pouch, which looks like the shape of J.
This week on Lights, Camera, Crohn’s we hear from a colorectal surgeon and IBD patient himself, along with several women with j-pouches about their experience, what they’ve learned along the way, and what they hope others know who are living similar realities.
What does the j-pouch procedure entail?
Before we dig deeper, a short “lesson” on what the j-pouch procedure involves. It’s typically a one, two, or three stage process.
According to the Crohn’s and Colitis Foundation:
The first surgery removes your colon and rectum and preserves your anus and anal sphincter muscles. The ileum is made into a j-shaped pouch and connected to the top of your anal canal.
A temporary ileostomy is typically created to give your newly formed pouch a chance to heal. A loop of your small intestine will be pulled through an opening in your abdomen, called a stoma, to allow waste to exit your body into an ostomy bag.
During this time, you will need to always wear an ostomy bag, and it will need to be emptied several times a day.
You will have your second surgery eight to 12 weeks later, once the pouch has healed.
The second surgery will reverse the temporary ileostomy and reconnect your small intestine. Your internal pouch will then collect waste and allow stool to pass through your anus in a bowel movement.
Some surgeons choose to perform this surgery in just one stage, in which the pouch is created and joined to the anus without a temporary ileostomy. This is done less often than the two-stage procedure because of an increased risk of infection.
This topic resonates with Dr. Stefan D. Holubar, MD, MS, FASCRS, FACS, IBD Surgery Section Chief & Director of Research for the Department of Colorectal Surgery at Cleveland Clinic, for many reasons. He was diagnosed with Crohn’s colitis when he was 7 years old and was on and off steroids (the only treatment at the time) for many years.
“I had learned to live with chronic embarrassing urgent incontinence, as well as being small and skinny, and with a swollen face from the steroids. I was offered an end ileostomy as a teenager (not a J-pouch as it was Crohn’s) and was lucky to get a second opinion with the famous Dr. Daniel Present (RIP) at Mount Sinai. I went on NPO and TPN for one year which helped get me into remission and grow about a foot in one year. Somehow, I made it through college and got into medical school, but it turned out I hadn’t had a colonoscopy in about a decade.”
Over Christmas 1999, Dr. Holubar had a colonoscopy and received a call a few days later while he was skiing that he had colon cancer.
“That same day, the tumor swelled from the biopsies, and I developed a large bowel obstruction. I had emergency subtotal colectomy w ileosigmoid anastomosis without an ileostomy. After chemotherapy and completing medical school, I needed the rectum removed (due to risk of rectal cancer) and underwent a modified 2-stage J-pouch without ileostomy one month before surgical residency. I’ve been great ever since, not perfect as I have had some complications over the years, but great, with three kids, the best job and wife in the world.”
During the second half of medical school, Dr. Holubar was considering going into GI or Medical Oncology and learned that colorectal surgery was a specialty.
“Once I learned Colorectal was a specialty and they are the IBD experts, my future path was set in stone. It’s rare to know that you want to be a colorectal surgeon that early in training. I’m blessed to share my successful story and give patients with complicated IBD like me hope every single day of my life. My experiences have also influenced me to do clinical research to try to change care more broadly and ideally, globally. My IBD history is a source of endless inspiration for our innovative work.”
I asked Dr. Holubar what advice he has for patients who are on the fence about getting a J-pouch. His most important advice—is to seek expertise.
“I would recommend looking for surgeons who specialize in IBD. J-pouch surgery is a niche these days (hence “IBD Surgeons”), and your care team should be expert in taking care of the complications that may develop. A majority (>90%) of patients with a pouch would do it again and/or recommend it to a friend or family member.” (Fazio et al., Annals of Surgery, 2013, PMID: 23299522).
Dr. Holubar wants to highlight a couple important points in terms of this article:
Only about 10% of people who are deemed candidates for a pouch choose not to have it, for personal reasons such as work, or lifestyle-related reasons such as lack of access to a toilet for many hours at a time, or those who prefer a one-and-done approach (Holubar, Inflamm Bowel Dis, 2009, PMID: 19266572). We have a new article on this, but it has only been published as an abstract so far (Total Proctocolectomy with End-Ileostomy Versus Ileoanal Pouch for Ulcerative Colitis: Who Doesn’t Pouch, And How Do They Do? Dis Colon Rectum 64;5; Meeting AbstractPOD169)
On the other hand, the overall long-term pouch survival is about 90-95% which is very high (in other words, it works out most of the time, but not always) (Fazio et al., Annals of Surgery, 2013, PMID: 23299522).
In the current digital era, we are blessed to have support groups on social media and active discussions on #SoMe4IBD. That said, it’s important to know that not everyone who has a pouch – whether the experience is great, or they have complications – is vocal on social media. It’s important to check with your care team to discuss the best treatment options for you.
When it comes to the risk and benefits of having a J-pouch, Dr. Holubar says each patient needs to chart out the pros and cons of end ileostomy (or rarely a continence ileostomy aka Kock pouch) vs. IPAA as the risk-benefit profiles are quite different.
“The main benefit is that a patient can maintain transanal defecation and avoid a permanent ileostomy and care of the ileostomy. An added “benefit” of having a pouch is that you can almost always go back to an ileostomy if it doesn’t work, or you are not satisfied with the function. Going back into the belly is of course with some risk of further surgical complications,” he explained.
The j-pouch patient perspective
Jackie was diagnosed with ulcerative colitis in March 2009. She was 24 years old and had been given a multiple sclerosis diagnosis before that. At the time, her care team was concerned a biologic could set off her MS.
“Less than a year after my diagnosis, I was told that I’d run out of medication options and I’d need to have my colon removed and opted to schedule surgery at that time to work towards a j-pouch,” said Jackie.
Getting acclimated to having an ostomy didn’t come easily. She says her biggest obstacle was getting over her own biases.
“I didn’t know anything about ostomies except from what I read online from other patients at the time and the consensus in the online forums was not good. I was nervous, but I learned almost immediately that I felt better, was healthier, and could do more. After my first surgery, I traveled across the country and hiked through some parks in Oregon. None of that would have been possible before my ostomy. It only took a few experiences like that to realize how much the ostomy had really given me.”
Of course, there’s a learning curve. There’s new terminology to learn, you must find what works on your body, and that can be frustrating.
“I was curious from day one. I knew that I was sent home in the appliance the hospital had set me up with, but I wasn’t convinced that was the best one for me, so I took it upon myself to test lots of brands and products to get the one that worked best for me.”
Jasmine was diagnosed with ulcerative colitis in 2017 when she was 19. She was a freshman in college. Two years later she dealt with a flare she started Entyvio, but the drug failed her shortly thereafter. She switched to Remicade in January 2020 and had the same problem, even after receiving the highest possible dosage every 4 weeks. Her health continued to rapidly decline, and she was hospitalized in March 2020.
“This was the first-time surgical intervention, an ostomy, and a j-pouch were mentioned to me in a real way, however, the doctors continued to say they felt cautiously optimistic Remicade would pull me out of my flare. Throughout these months, I tried a variety of diets including SCD and AIP, visited multiple dieticians and nutritionists, met with natural health doctors, sought out second opinions, and followed a robust supplement regime that was continuously updated by my functional health doctor.”
Despite every effort, by April of 2020, her health was the worst it had been her my entire life. Weighing 105 pounds, she lived in constant, excruciating pain, unable to sleep or eat, too weak to stand in the shower for longer than five short minutes.
“IBD completely ruled my life. When I spoke with my doctors in early May, they told me I had two options: I could try Stelara, the last drug available to me, which my team was 99% sure would not work and would result in emergency surgery since the drug takes months to kick in and provide relief. Otherwise, I could have surgery immediately. My options hardly felt like options when both resulted in the same outcome, just at different times. I opted to have surgery sooner rather than later. If it was inevitable, I wanted to begin the process and start feeling better as soon as possible, rather than continuing to needlessly suffer.”
A few days later, Jasmine met with a surgeon, and less than a week after that appointment (and the morning after her college graduation), she was rolled into the operating room to have my colon removed.
“No life experience prepares you to look down and see an internal organ on the outside of your body. A stoma is far outside the lines of normal human experience, and despite all the preparation in the world, your brain can’t fully process what it will be like until it’s happened. I found the transition to be difficult; while the nurses in the hospital were helpful, the nurses sent to my home barely seemed to know what to do. I had to teach myself how to empty the bag, and at first, it often took me an hour to change the ostomy. However, with time and as my body healed from surgery, I became more confident and able to quickly take care of the ostomy in under five minutes,” said Jasmine.
Even though the physical acclimation was challenging, Jasmine says the mental acclimation was even harder.
“At the time, I was 22 years old and had never in a million years imagined my life to involve a bag of waste attached to my stomach. I felt like I was constantly grieving the life I’d imagined and the life I’d never get to live. The ostomy felt like a reminder of all that had been taken from me that I couldn’t ignore, concrete proof of how different I was from all other 22-year-olds and how far my life had diverged from the normal college experience. I spent many days looking in the mirror and crying at what I saw, struggling to accept the ostomy as the life saver it was. Over time, as I began to regain more freedom and control over my life, eating the food I wanted, sleeping through the night, exercising, and traveling, I slowly began to make peace with the ostomy through the lens of all it enabled me to do.”
Aimee was diagnosed with ulcerative colitis in 2011 when she was 22 years old. She struggled responding to medical intervention and dealt with severe abdominal cramping and high levels of blood in her stool which destroyed her quality of life.
“I had to give up my job, my life, my apartment, my social life and moved back to my hometown to be taken care of by my parents. In one hospital admission 9 months after first symptoms, the surgical team advised I do the ostomy to avoid a tear or rupture to the colon which could lead to emergency surgery or worse, sepsis.”
The ostomy relieved Aimee’s constant cramping and she felt instant relief from her chronic pain. Going into surgery the plan from the start was to do a three-step surgical journey over 12 months that resulted in a j-pouch May 2012.
“There is so much help in the hospital that it was only the day I was leaving that it hit me that this was going to be something that would be hard to get used to. I was 22 and I was embarrassed to tell everyone and conscious of my looks, so there was a vanity piece that was hard to overcome. When I was home, I felt alone. I wanted to manage the bag all by myself, I didn’t allow anyone to see the stoma or my bags or anything. Looking back at my young self, I wish I had let my family and friends in more to help me, I didn’t need to hide it.”
Elissa was initially diagnosed with ulcerative colitis when she was 14 years old, back in 1994 and years later, Crohn’s, in her small intestine. Her diagnosis journey was a difficult one. She was told she was lactose intolerant, had food allergies, IBS, anxiety, and a nervous stomach.
When Elissa was 20, she underwent emergency surgery to remove her colon. She was one of the first patients to participate in a clinical trial for Remicade back in the day. Unfortunately, the medications kept failing her, she became dependent on high doses of steroids, and she had precancerous cells in her colon.
“I was in college at the time and didn’t feel comfortable telling most people. There were a few occurrences of my bag leaking (one especially memorable experience in the middle of a fraternity party), and I was mortified. However, my recovery also highlighted the thoughtfulness and generosity of my best friends and family members who would drive me to the pharmacy to pick up medical supplies, drive me to doctor appointments, even just sit with me and rest. People really come out of the woodwork – sometimes asking for help is the hardest part.”
At times Elissa felt very alone. She wishes she had known the Crohn’s and Colitis Foundation was available, along with support groups. She says, now, there are so many amazing resources available for people in recovery, including the forum j-pouch.org.
Dani was diagnosed with ulcerative colitis in 2005, when she was just 8 years old. She was initially managed on oral medication then switched to biologics and went through Remicade, Humira, Xeljanz, Stelara, and Entyvio.
“I always knew that surgery was on the table, and I felt like I was always buying time until a new medication came out. In January of 2021 I became extremely sick and was admitted to the hospital for IV cyclosporin to try to lessen my immune response. I was ok enough to leave the hospital and was feeling ok for about four days out of the hospital and then I started to become sick again. My surgeon came around a few times to check on me and introduce himself. He said, “I just want you to know that I’m not the scary man with a knife.” At that time, I didn’t know he would be my surgeon. When I started to get sick again after leaving the hospital, I knew that surgery was going to be the next step.”
From then on, Dani met with her GI doctor and Colorectal surgeon (who work together), and they scheduled her for a subtotal colectomy a few weeks later. She began the 3-step surgical process in March 2021.
“It was a huge adjustment. I constantly felt my bag and it felt so foreign to me. At the same time, it gave me an independence that I had never had before. My plan was to go through all 3 j-pouch surgeries to have an ostomy for nine months and then have a j-pouch. I felt confident that I could adjust to an ostomy again if necessary and that I wanted to give a j-pouch a try.”
Dani got her take down surgery J-pouch in December 2021.
The hope of reversing from the start
Jackie: “The plan was to reverse, but I did have a major panic moment a few months before I was supposed to have another surgery. A friend of mine who had started his journey to a -j-pouch around the same time I did, was one step ahead of me in his surgical sequence, and he was having some major problems. I figured the ostomy was the devil I know, better stick with what you know, because I was afraid of what the other side looked like. But I knew myself, and I knew I had to at least try for a reversal, otherwise I’d spend the rest of forever wondering how it would have gone.”
Jasmine: “From the start, the colectomy was presented to me as a step toward the larger goal of getting a j-pouch. I went into the first surgery planning to try the j-pouch.”
Elissa: “I knew the ostomy would be temporary, but I really had no idea what to expect as far as recovery was concerned. My doctors and surgeons did not explain any potential complications. I wish I had known more questions to ask.”
For Elissa, a pouch was created at the time of surgery that removed her colon. Three months later, she had reversal surgery during college spring break – unfortunately, the reversal failed, she caught an infection and ended up in the ICU. The ostomy was placed again for her body to recover from an additional open abdominal surgery. She then went on to have a successful reversal in July of 2000.
Making the decision to go for a j-pouch
Jackie: “I knew that I could have chosen to keep my ostomy, but there was a real sense of “why wouldn’t you get a j-pouch” from the medical team. There was an undertone in what they said and did that insinuated the j-pouch was the more ideal situation and that I should clearly want to go that route. At the time, I was still regularly following most professional medical advice and didn’t really question it. But the option to keep the ostomy was never really discussed and it was always assumed I would reverse it.”
Jasmine: “Because I was young, otherwise healthy, and it had been confirmed many times through testing that I had ulcerative colitis, rather than Crohn’s disease, my doctors said I was a great candidate for j-pouch surgery. In general, my surgeon told me that close to 90% of j-pouch surgeries are successful, and I felt confident trying based on my background and the conversations with my medical team. By the time I’d had surgery, I’d only had ulcerative colitis for three years and had been in remission for two of them. The j-pouch felt like the best avenue for a life as close to normal as possible given the circumstances, and at 22, with (hopefully) a lot of life ahead of me, that sense of normality was important to me.”
How it felt leading up to reversal
Jackie: “I kept reading about all the things that could go wrong and it really freaked me out. I knew people personally who had some complications and it made it seem less like a potential statistic and more like a reality. The reality is that more people do well but are not often talking about it online. At that time there weren’t enough stories about people thriving after j-pouch surgery. I knew what life with the ostomy was like and I knew I could do that. Welcoming another major surgery and another major change just seemed really overwhelming.”
Jackie started the process in March 2010. She unfortunately had a few complications along the way which resulted in more surgeries and a longer sequence to the j-pouch, so her takedown occurred in mid-2012.
Jasmine: “I often worried something would go wrong that would prevent me from getting a j-pouch. Everything that could go wrong had gone wrong for me to even end up 22 and colon-less, and it was hard for me to imagine something could go “right.” I felt very distrustful after the variety of promises made to me by my medical team over the past year that never came to fruition and struggled with cynicism about what might happen. Coupled with all the negativity online about life with a j-pouch, I became very apprehensive about something either going wrong with my surgeries or my j-pouch failing.”
Jasmine’s j-pouch was created in December 2020 with a diverting loop ileostomy and was fully connected in February 2021.
Dani:“I had read about ‘butt burn’ and that when you first get a j-pouch you are going to the bathroom frequently, so I was concerned about that. I had just gotten used to being able to go where I wanted and not worry about the bathroom, and I was concerned that I was going to be putting myself back into a position where I was more limited.”
What j-pouch recovery was like
Jackie: “The takedown was one of the easier surgeries to recover from for me because that was the only thing they were doing in that surgery. Sometimes surgeons combine steps that can make certain parts more difficult to recover from, but for me it was just hooking up the plumbing, which had already been healing internally for months. Despite the complications I had that resulted in more surgery, it gave my body more time to heal, which I think is part of why my j-pouch has been so successful. The hardest part was understanding that the j-pouch can take a year or so to settle, which means you may still have some accidents here or there in the beginning. It wasn’t an immediate magical fix, but over time I learned to understand my j-pouch and to predict its behaviors.”
Jasmine: “J-pouch recovery is an exercise in endurance and mental fortitude, but I didn’t find it as terrifying as it seemed from reading online. From the beginning, I felt like I had far more control than I did with ulcerative colitis. There was almost no urgency, and I could take a minute or two to finish what I was doing before going to the bathroom, rather than having to drop everything and run. Although you do go to the bathroom quite often at the start, having that control makes a huge difference. One of the harder parts of recovery is the acidic stool – waste in the small intestine has more stomach acid in it, which usually gets broken down by the colon, however, without a colon, that acid creates burning on the skin. My skin was constantly raw and sore the first few weeks no matter how much butt cream or fluffy toilet paper I used. Sometimes the burning pain was so bad it would wake me up at night, but now, almost two years out, I rarely have butt burn.”
Aimee: “This was the hardest surgery because it was so long and so much handling of my intestines, my bowel lost function, so I vomited for eight days after my surgery. My doctors considered TPN, but luckily peristalsis started again, and I could eat!
Elissa: “Honestly, recovering from surgeries itself wasn’t too bad, especially after years of IBD flares. Getting rid of my colon provided almost immediate relief. I just had to be patient and let my body heal.”
Dani: “The recovery was the easiest in terms of there weren’t new incision spots. I had to get used to seeing my stoma hole as it closed in naturally and I was still very sore. I also was going to the bathroom frequently and wasn’t sleeping through the night for the first few weeks, which was hard. I was frustrated that I felt like I always needed to be near a bathroom, but that feeling was temporary. “
Pros and Cons of life with a j-pouch
Jackie: “Honestly…it has been so good. I have a total rockstar j-pouch. I eat anything I want (popcorn? yes! all the nuts? yes! spicy food? Yes, please!), I can hold my bowels for hours upon hours. I rarely have any urgency and in general have peace of mind that I can live my life, go where I want, and UC no longer can control that. The cons exist, but for me, they’re small. I’ve had pouchitis a few times, which feels like UC again, but it’s treated with antibiotics and then you’re back on your feet! I have accidents at night maybe once a year. I still use the bathroom more often than a person without IBD, but it’s mostly because I choose to for peace of mind. My digestive tract in no way resembles a normal one, it’s different how everything works now, but it’s not a detriment in my life.”
Jasmine: “My j-pouch has given me a level of freedom I never thought I’d experience with IBD. I don’t currently take any medications, and I don’t worry about flaring or failing a medication the way I would with my colon. Although I know there’s always the possibility of needing medication in the future, I’ve been given more freedom and autonomy over my life than I ever thought possible. I eat what I want when I want. I sleep through the night. I sit through meetings and classes without thinking about the bathroom. I go out with friends, travel, and exercise. For me, the j-pouch has brought me closer to my pre-IBD or deep remission self than anything else, and although there are permanent tradeoffs to having such major surgeries, I don’t regret my decision in the slightest. There is an adjustment phase and a new normal, but that new normal has enabled me to integrate IBD my life, rather than having my life completely consumed by my illness.”
Aimee: “I have had fistulae since at the anastomosis, so they have been tricky to manage, but Humira has been wonderful to me, keeping them at bay and giving me energy to live a full life. I also need to have the scar tissue at the anastomosis stretched surgically every 6 months.”
Elissa: “J-pouch life has been amazing! I was in the bathroom 20+ times a day before my surgeries and felt like a shell of a human being. I’m now 42 and have had my j-pouch for 22 years. I can do pretty much anything a “normal” healthy person can do, just need to take occasional extra precautions like electrolyte replenishment or dealing with occasional pouchitis or Crohn’s flares. (My Crohn’s diagnosis came after my j-pouch surgery).”
Dani: “The first few weeks/months with a j-pouch were tough. Your body needs to figure out how to function with a new man-made organ. I was only comfortable laying down for the first few weeks after the surgery. I really hit a turning point when I was able to start taking Imodium and Metamucil. They were helpful for me in the first few months and now I don’t need them. Three months after my final surgery, I had moved out of my house and was starting a new full-time job. So, the initial discomfort and increase in bowel frequency were very temporary!!”
What j-pouchers wish they knew prior to their reversal
Jackie: “I always say its trading a large set of problems for a smaller, more manageable set of problems. UC was awful for me and ended up being life threatening. It was no way to live. My j-pouch has given me my life back, but it’s not a cure. It’s not perfect. I still have some small problems here and there, but it’s all manageable and in no way resembles life before surgery.”
Jasmine: “It’s hard to find information on j-pouches, and I think many of us turn to the internet to learn about what life with one might be like. I personally found the internet to contain a lot of negative information, making me more fearful going into the surgeries than I would have been had I just listened to my surgeon. I would recommend limiting time spent online and trying to connect with individuals who have j-pouches/ostomies through your doctor or the Crohn’s and Colitis Foundation. These resources provide a more accurate peek into life with a j-pouch and can allow you to ask questions and connect with someone who’s been through the same thing. Most people who are healthy aren’t online complaining about their j-pouch, which skews the sample of information accessible to the rest of us. Whenever I started to feel overwhelmed by everything online, I reminded myself of something a nurse once said to me: the internet is a showcase of the best and the worse situations, more often than not, you’ll end up somewhere in-between.”
Aimee: “I was told this would be the end of treatment and medicine which wasn’t the case. As I had Crohn’s, not UC, I had many more hurdles ahead. Also, a new pouch is new so it’s behavior post op, is not your life. Your body adjusts to the pouch and output goes slower as the post-op weeks go by. The j-pouch is an alternative to an ostomy bag, but has to be adjusted to also. It’s different from having your colon. After a few months though, you will have longer periods between toilet runs and sleep through the night. I go 11pm to 6am with no pooping, which is so much better than those few months post-op when I thought oh dear, this is hard!”
Elissa: “When I had my surgeries, I was 20. No doctors discussed potential fertility issues. My daughter was born via IVF 9 years ago, though all additional efforts have failed. This is something I wish I had known about – I always wanted kids and would have frozen my eggs. Obviously, every person is different. Also, I still go to the bathroom 6-7 times a day. This is apparently normal (though again, everyone has different experiences).”
Dani: “I can eat salad for dinner with no problem!”
Advice for ostomates on the fence about going for a j-pouch
Jackie: “If you feel healthy and strong both physically and mentally, I would say, try it. I know it’s more complicated than giving a new restaurant a try, but I knew that I’d always have wondered. I knew on the bad days I would have idolized a life with a j-pouch, and I needed to know that it either would or wouldn’t work. I felt like the worst-case scenario was that my j-pouch would fail, and I’d return to an ostomy, which I already knew I could do, and I liked those odds.”
Jasmine: “I think it’s a personal decision dependent on the history and circumstances of each person’s illness. Going through the j-pouch surgeries means additional time spent in the hospital and recovering, which is worth it for some, but not others. Although I can share my experiences, everyone’s body is different, and you can’t always predict how someone else will respond. I think the best thing to do is find a colorectal surgeon skilled in these procedures and discuss whether they think you’re a viable candidate. Finding a skilled surgeon is the best way to hedge against future problems and increase chances of success. Beyond that, I would advise talking to as many people as possible with a j-pouch and permanent ostomy, to get questions answered and hear the pros and cons of each route. Having this information should help you feel more confident in your decision, and if you’re still undecided, you can always put off the decision until you’re ready.”
Aimee: “Tell them to get support, don’t expect instant results, give yourself time to adjust to yet another way of going to the toilet…reach out to the online community.”
Dani: “I think this is a very personal decision and there is validity to both sides. An important thing for me was to remember that people are more likely to write online if they have a bad outcome rather than a good outcome. Everyone’s instinct is to research things online and at some point, I felt like reading everything (both good and bad) was too overwhelming.”
Post-op expectations with a j-pouch
Like any surgery, recovery takes time and patience. The Crohn’s and Colitis Foundation shares the following on their website:
Some patients may experience an increased number of bowel movements, sometimes up to 12 times per day. This will typically decrease over time.
Some male patients may experience sexual dysfunction as a result of nerve damage.
Some female patients may develop scar tissue that surrounds their ovaries and fallopian tubes, which may lead to infertility.
Both men and women should discuss sexual function with their surgeon and ask when it is safe to resume sexual activity.
Ask your healthcare providers what supplies you may need at home, especially if you have a temporary ileostomy.
Your healthcare team will advise you on how to manage your temporary ostomy and how to keep it clean.
Final Thoughts
Jackie: “This is a weird one, but I had to use brain power the first time I had to poop after my takedown. It had been almost 2 years since I had used my butt, and I had to really think about how to use those muscles again. It was a little funny at the time.”
Jasmine: “In terms of recovery, the most important thing to remember is j-pouch surgery completely alters one of the body’s major systems and adjusting takes significant time. Recovery doesn’t happen overnight, and it can feel frustrating. I tried to give my body some grace and the time it needed to heal, while reminding myself that life with a j-pouch during the first few week’s post-op isn’t indicative of what living with a j-pouch will be like long-term.”
Aimee: “It’s a journey. I have a few good months, a few bad months. Part of me knows that quality of life could be better with an ostomy, but I’m not ready to say goodbye to my pouch yet. I have been unlucky with the scar tissue, but those small procedures are like going to the dentist for me, I’m so used to them.”
Elissa: “Do it! Healing takes time, but you will feel like a new person. Life is too short to be in pain all the time. So many improvements have happened over the past 10-15 years and awareness is absolutely the key. “
Dr. Holubar wants to remind patients, “The J-pouch cannot save your life – it is a lifestyle operation like cosmetic surgery in some way. Overall quality of life is excellent with both a pouch and with a permanent end ileostomy. Finally, we should think of surgery as an excellent “medical” therapy in patients suffering from colitis despite modern medicines. One of my expressions is that a good ileostomy (or pouch) is better than a bad colon, rectum, or anus (and a good ileostomy is better than a bad pouch). The great news is you cannot make a wrong choice.”