This article was sponsored by ImYoo. All thoughts and opinions shared are my own.
Precision medicine is a common term we hear when it comes to treating IBD now and into the future. But have you heard about citizen science as it relates to IBD? Citizen science gives everyone a chance to play an active role in research. Whether that’s coming up with research ideas or taking part in the experiments themselves, citizen science makes it possible for you to have a direct impact. A company spun out of Caltech is taking citizen science to a whole new level. ImYoo is debugging the human immune system by using at-home blood collection kits and single RNA sequencing to discover insights about autoimmune diseases.
Tatyana Dobreva and her co-founder, David Brown, worked at NASA prior to switching gears from space to focus on biotech.
“The COVID-19 pandemic accelerated the process and highlighted for us what was missing. Since the pandemic, people are paying more attention to their immune systems. Immunology is still as much a mystery as outer space, so that was the next frontier we wanted to get involved in. We feel that the best way to take on that challenge is by building a database across time, for every individual – that is what can make personalized medicine possible and that is why we’re so focused on making this research accessible.”
Since IBD presents uniquely in each person and changes over time, it’s a rollercoaster journey of highs to lows, flares to remission. With all the twists, turns, and complexities that ulcerative colitis and Crohn’s create for each of us in the patient community, following a roadmap can seem impossible.
“Precision medicine tries to apply scientific tools to take out some of this guesswork. A lot of those tools look at the genetic material you inherited from your parents. We’re adding another tool to that kit by looking at the expression of those genes. For IBD, we want to figure out which genes and cells are acting up during a flare,” said Tatyana.
By answering these key questions, clinicians have told Tatyana that it will help gastroenterologists make more informed decisions when it comes to treating and managing IBD and patients can feel more empowered every step of the way. While making the decision to start a biologic can be overwhelming for patients, precision medicine is a way to have powerful data to support the choice to move forward with that treatment plan.
Tracking the immune system over time
ImYoo’s focus is tracking a person’s immune system over time. Researchers do this by looking at RNA expression. Tatyana shared a fantastic analogy with me. She said that DNA is like the menu you get at a restaurant, RNA is your order, and proteins are your final meal.
“There are a lot of companies that look at your blueprint, or in this case your menu – all the possibilities. Our team at ImYoo looks at your cells’ orders over time. That way we can capture how the different immune cells in your blood are changing,” said Tatyana.
IBD flareups are of specific interest to both clinicians and patients. Even after living with Crohn’s disease for more than 17 years, the unpredictability of the disease is still one of my main struggles. The looming thoughts of a flare are always with you.
“There is not much literature on what happens in the immune system during a flare, and we think there are a lot of powerful biomarkers that could be discovered if IBD patients could track themselves during flares and when they feel “normal.”Our IBD study will ask IBD warriors to sample themselves both during and outside of flares,” said Tatyana.
ImYoo built a solid foundation for studying autoimmunity because researchers were able to build a database of “normal” immune systems.
“Being the first to do this for single-cell data means we can provide a helpful reference to enable more single-cell studies for the future. By having a large database of “healthy” immune systems, we can provide more context as to what having a flare means with respect to dysfunctional immune systems.”
How IBD Patients Can Participate
ImYoo’s IBD study was inspired by conversations researchers had across Reddit and in a Facebook group. Patients in the community offered invaluable insights about what to research.
Emily Harari works as a liaison between the scientific team at ImYoo and the patient community. She says if a person demonstrates interest in participating in the study, a screening process will take place to determine eligibility.
If you qualify, you are enrolled under an ethics-approved study protocol and sent a kit that includes a virtually painless capillary blood self-collection device called TAP II. The device allows you to participate in immune studies in the comfort of your home and send capillary blood samples directly to the ImYoo lab. The TAP II is placed on the upper arm and sticks with the help of a gentle adhesive, it barely penetrates the inner layer of your skin and feels like a suction cup.
“For the IBD study, we ask you to collect a few samples when you’re feeling well and a few samples when you’re flaring. The TAP II device is virtually painless and takes just a couple minutes to use. You’ll mail us the tube of your sample with the packaging we provide. After several weeks we’ll report updates from the lab and several weeks after that we’ll release our study’s findings to the community. Since the community is crowdsourcing the study for us, the least we can do is share what we discover. For example, we may find a new gene or an immune cell marker that helps your doctor better treat your flares,” said Emily.
The Power of Crowdsourcing
The best part about a crowdsourced study is that anyone can make a difference. By visiting the ImYoo crowdsourcing page and selecting “Participate in this Study!” you are making a powerful impact. The more people with IBD who join, the more attention we can attract for crowdfunding.
“If you’re eligible for the IBD study, we’ll reach out after we’ve hit our crowdfunding goal. To help us reach our goal, you can express an interest to participate or pitch in a donation to one of our Champions’ campaigns. There’s a network effect we’re going for, one person tapping into their community can open so many doors.”
If you’ve ever been told your labs or scopes look normal or there’s nothing more to do when you’re suffering through IBD, it’s simply not true. Everyone is on their own health journey and deserves a chance to take control of it.
“That’s why ImYoo is excited to put innovative science in peoples’ hands. This research isn’t possible without the IBD community, which is why we invite IBD Warriors to pitch in however they can – skip a coffee and donate $5, express interest to participate, or simply share to your network,” said Emily.
“Our goal is to empower the IBD community with more powerful tools. One of the biggest questions we hear from IBD folks is, “Am I in remission yet?” You might be feeling fine and think you’re good, meanwhile your immune system could be attacking your colon,” explained Tatyana. “We hope to help people track their immune systems when they are most vulnerable.”
By enabling the IBD community to crowdsource our own studies, the power is in our hands. ImYoo wants to explain their research findings every step of the way and keep people engaged, because it really is a partnership. From this IBD study, the ImYoo team wants to prove that the IBD community can make their own research happen. By studying flares, the hope is that sequencing the state of individual immune cells will uncover predictors and targets for more accessible precision medicine.
Connect with ImYoo, Follow and Participate in the Research
It’s been 6,207 days since my life changed forever. On July 23rd, 2005, I was diagnosed with Crohn’s disease at age 21. Since that time, I’ve evolved and changed in ways I may not have if it weren’t for my IBD. After living in silence with my condition while working in television news for a decade, I decided to use my love for storytelling and speaking to be the voice I needed to hear upon diagnosis as I navigated the many crossroads of young adulthood (finding love, a fulfilling career, and having a family).
July 23rd also marks the day I launched my blog, Lights, Camera, Crohn’s. Since 2016, I have shared fresh content, every single Monday (sometimes even twice a week!). 336 articles on my site alone. More than a quarter-million visitors and more than 387,000 views.
It’s been a labor of love and a mission project that continues to fill my cup and implore me to constantly want to learn more and shed light on topics that are often not talked about. Every day of every week since my blog began, I’m constantly thinking about story ideas, topics of interest, people to interview, ways to word content, images that are needed…the list goes on.
This photo was taken at a wedding July 23, 2016, right after I pressed “Publish” on the first Lights, Camera, Crohn’s article. I found out I was pregnant two days later.
The weekend I started my blog in 2016, I was one month into married life and found out days later I was pregnant with my first child. Since then, I am now a stay-at-home mom of three children (ages 5, 3, and 1). Life has gotten way more hectic and busier with each year that passes, but I’ve held tightly onto fulfilling my promise to the patient community, and to myself, to deliver new content each and every week. I’ve been organized through the years—often having an article written days before my Monday deadline, but this past year, with another baby added to the mix, it’s been more of a stress on me. I’ve spent many Sunday nights finishing my articles. At times it’s felt like a lot to juggle. I haven’t wanted to let anybody down, including myself. And I haven’t wanted my content to start lacking in any way.
Don’t worry, Lights, Camera, Crohn’s is not going anywhere
My blog has grown into more than I ever thought possible. It’s so rewarding to know my words have helped comfort and guide so many in the IBD community. I need to cut myself some slack and give you a heads up that moving forward there may not always be an article on Mondays. It pains me to say that, but at this point in my life, in this season of IBD motherhood, I need to start taking time to rest and relax. Since having my third baby last summer, I get my kids down for the night and START to work around 830 pm. It’s just constant. I truly rarely get a break. I’ve been in remission since August 2015, and I don’t want the stress to get the best of me.
You may not be aware—but my blog is only one aspect of my advocacy work. I also spend a great deal of time working with digital healthcare companies, patient-centered non-profit organizations, sitting on advisory boards and patient engagement teams, communicating with patients in need online and over the phone, and do freelancing work on the side, all without childcare.
I laugh as I write this because I already have three articles lined up for August…so there will be months where there IS an article every Monday. Just not always. My commitment and desire to serve as a patient leader is not waning in any way—I just want to be honest with you, my loyal readers, that this mama needs to lighten the load and take a little self-imposed stress off my shoulders.
I started contemplating this a few months ago, and almost changed my mind this week about sharing, but it’s time. We had an AMAZING 6-year streak of constant new content. I’m excited to see what this coming year brings in the way of patient stories, research, and perspectives. Having extra time to work on articles will really allow me to do more special reports and expand my “IBD Motherhood Unplugged” and “Patient Experience” series.
Thank you for giving me so much to talk and write about, always. There are endless topics that need to be brought to the forefront and I love providing a platform for others to share their journeys and experiences with the community. As always, please reach out if you have a story idea you want me to cover. Lights, Camera, Crohn’s has truly evolved from being a blog about my IBD experience to an award-winning and well-respected site that has highlighted hundreds of different patient stories and physician perspectives—and I love that. There’s no greater compliment then when I hear a gastroenterologist uses my blog to educate their patients.
Excited to see what 2022-2023 brings! Thanks for the love, support, and understanding and for making the first six years of Lights, Camera, Crohn’s what it was.
This blog post is sponsored by Wave Health. Thoughts and information shared are my own.
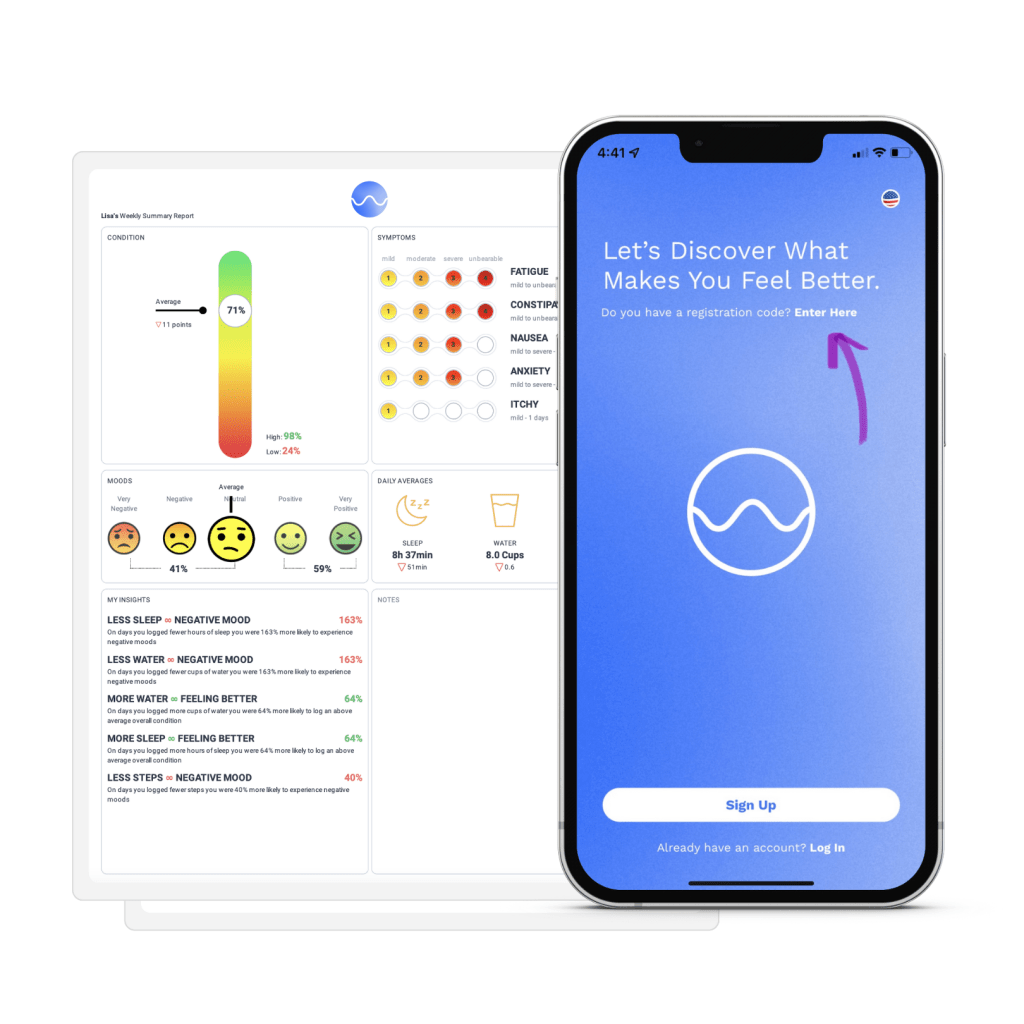
What started as an app designed for cancer patients in 2019, now spans more than 250 chronic health conditions, including inflammatory bowel disease. Wave Health is a free, easy-to-use, comprehensive tool that empowers patients to use their daily health data in practical and effective ways, while enabling those in our community to be more involved in their care and treatment decisions. This week on Lights, Camera, Crohn’s a look at the story behind how Wave Health came to be what it is today and how the app can be a transformative tool in how you take on your IBD.
Hear what Claudia Zhao, the Marketing and User Engagement lead at Wave, has to say about the inspiration behind their mission.
“Wave Health App was inspired by a personal patient experience. In 2013, one of Wave’s founding partners was diagnosed with non-Hodgkin’s lymphoma. During his treatment, Ric’s partner, Matt (now the CEO of Wave Health) began to record extensive data by hand — things like his diet, hydration, exercise, mental engagement — anything that might impact the side effects Ric faced during his chemo and drug therapy. With this information, they were able to provide their doctor with real-time, individualized information, and identify relationships between what Ric was doing and the side effects he was experiencing. Protocols were shifted and Ric began to feel better,” said Claudia.
Matt transformed his data analytics system into chemoWave, an app for cancer patients like Ric. Soon, they realized that anyone with a chronic illness would benefit from a health management and insights tool like chemoWave, and they created Wave Health App.
“Wave’s mission is simple: to help every patient take control of their own journey. Wave serves to empower patients to use their everyday data in ways that allow them to be better partners with their care team and ultimately improve their at-home and treatment decisions.”
What sets Wave apart from other IBD-related apps
Most IBD-related apps focus on tracking symptoms and a few other activities such as meals, bowel movements, and medications. Wave Health is different in that it serves as an all-in-one health diary.
“In addition to the more obvious activities to track in IBD management, Wave also lets you track vitals, sleep, menstruation, and even mindfulness activities like meditation and breathing. Wave then gives you personal insights, not only about your symptoms, but also about what’s impacting your moods and wellbeing. Wave helps you manage your IBD-related symptoms, but it also acts as your overall health companion.”
Having a companion to help guide the way you manage and treat your IBD can help ease the isolating nature of our disease. Often life gets busy, and we forget how much our Crohn’s disease or ulcerative colitis takes a toll on our day-to-day activities. It’s easy to generalize or downplay the struggle when it comes time to share how you’re feeling to your care team. Wave takes that guesswork out of picture and is a win-win for everyone involved.
A systemic review out of Cedars-Sinai Medical Center recently found the app to be the highest rated symptom and PRO tracker for cancer patients.
“This speaks to the fact that Wave is easy-to-use, while also providing real, tangible benefits to the patient journey. In addition to being rated the highest overall PRO tracking app, Wave also received the highest individual scores for both engagement and aesthetics, two very important pillars for any type of user experience. Since the review in 2020, Wave has also done a complete UI/UX redesign. With a more intuitive interface and new features that make health tracking even easier, the experience of using Wave is only getting better,” explained Claudia.
How Wave expanded beyond the cancer community
Beginning exclusively as a cancer app, Wave was expanded to serve all chronic illnesses because of the underlying challenges that patients face regardless of their specific health issue.
“The nature of most treatments is that they are standardized — protocols shift only after periods of trial and error. Wave identifies relationships effectively and quickly, so that treatments can be tweaked, and side effects can be alleviated or avoided more promptly.”
Another key focus of Wave is on filling the gap between doctor’s visits. Most of the patient experience occurs at home, not in the doctor office, and currently there is no sufficient system or way for patients to easily report their symptoms and other outcomes during these critical periods.
“Wave helps patients fill in their care team, whether it’s about how their symptoms have been improving or how many days they’ve missed their medications. With a comprehensive record of patients’ daily and treatment activities, doctors have a more complete picture of the patient and their journey and are enabled to make more-informed decisions from there.”
Wave can help anyone
You also don’t have to be “chronically ill” to use Wave and see its benefits. Tracking and getting Wave’s A.I. insights can help anyone improve how they feel. Wave is a health management tool for anyone looking to take control.
“The app empowers patients to take control of their own journey. Just by harnessing their own daily health data, they can get powerful information into what helps them feel better or worse and then adjust their at-home activities to optimize their wellbeing. Second, Wave helps patients communicated better with their doctors on what they’re experiencing between visits. Patients can share/email their logged data directly through the app, or they can receive easily shareable Wave Pro PDF reports,” said Claudia.
How Wave Pro Works and a 6-month FREE discount code
The reports summarize a patient’s important health data and insights from the week, allowing them to see both short-term and long-term trends and changes. Users can download these reports and bring them into their doctor’s visits. Wave Pro is available through a monthly ($10.99) or annual ($54.99) subscription, with a free 30-day trial at sign-up.
Enter the code LIGHTS right away at sign-up and receive 6 months of FREE Wave Pro reports.
Moving away for school. A future career. Relationships. Discovering your identity. Switching from a pediatric IBD care team to adult providers. All while living with a chronic illness. This is the stark reality for young adults living with Crohn’s disease and ulcerative colitis. Juggling all these major life milestones and having to get acclimated to new physicians while taking the lead on disease management is often met with anxiety and worry from young patients, their parents, and caregivers. IBD is a family disease. Even if only one person in the household personally lives with the issue, the disease impacts each person.
This week on Lights, Camera, Crohn’s we hear from patients and caregivers who have lived through the experience and from pediatric GI’s about how best families can be supported through the changes to make them as seamless as possible for everyone involved.
Input from those who have made the switch
Aging out of pediatric doctors can be a stressful time for everyone involved. Let’s start with input from those with IBD who have made the switch along with what some parents and caregivers had to say.
Start researching doctors early. Do your homework and see what insurance providers accept and what hospitals they are affiliated with.
Ask your current pediatric doctors for recommendations/referrals.
Before the first visit make sure the adult GI has received copies of medical records.
Have healthcare proxy and power of attorney papers on file.
“I just turned 20, but I’m still in pediatrics and plan on staying until I graduate from college, as that is the norm at my hospital. However, as an adult in peds, I found it important to have healthcare proxy and power of attorney papers on file so my mom can still help me and if something were to happen like while I’m away at school she is able to get information. I broke my arm this past fall and my body went into such shock that I couldn’t give the hospital any information. My friends were with me and contacted my mom, but because I was 19, the hospital couldn’t even confirm to her that I was in the building. This was a wake-up call. We started thinking about, “what if this was my IBD?” and decided it was necessary to have the papers on file just in case. I still ask my mom to be involved in my care, but we both have the understanding that I have the final say.”- Anna
Navigating the switch through college
Heidi was diagnosed with Crohn’s when she was 9. She’s now 41. When she reflects on the transition from a pediatric doctor to one who treats adults, she recalls the process being fairly simple and a change she welcomed with open arms.
“The best thing was being talked to directly and my opinions mattered more in my later teenage years with the new doctor. Of course, my parents had my best interests at heart, but appointments were so frustrating as a young girl. Another reason for the seamless transition was that my new doctors were amazing. I switched at 18 and then again at 22 when I graduated college and moved away from home. My care team listened to me and saved my life. I know I’m lucky to have found such a wonderful team of doctors.”
Katie wishes there had been a support group (even online) for teenagers back when she was phased into an adult GI. She says when she was diagnosed with IBD at age 15, she often felt uncomfortable discussing her symptoms and didn’t feel her pediatric GI was that great with kids.
“I felt detached from my GI until I was in my 20s and had the confidence to advocate for myself. I was so lost and refused to tell classmates what was wrong with me for fear of being made fun of. I ended up missing so much school I decided to drop out, get my GED, and go straight to college. It was a terrible time to be honest.”
The difference in pediatric vs. adult care
“The transition happened quite fast as I was being referred to an adult surgeon for my complications that the pediatric team were not experienced or educated enough to treat for Crohn’s. I was thrown in the water with no guidance when I started seeing physicians who treated adults with Crohn’s. The pediatric GI team would dumb some things down for me and make my problems not seem “as bad.” As soon as complications started arising, they threw the towel in and basically told me they couldn’t help me anymore and would be better off seeing a care team with more experience with my symptoms and complications.”-Chrissy
Natasha experienced the transition about 13 years ago. Her pediatric team helped her choose an adult GI. And the guidance didn’t stop there.
“My pediatric GI told me who she wanted for me and then went with me to interview the doctors in the adult team. Once I chose, my pediatric GI attended every appointment with me until we all agreed I was ready to move into the next step of my care, which luckily was quickly. And the two doctors stayed in communication. My advice—be open with your doctor.”
Natasha recommends asking yourself the following questions to help streamline the process and make it less nerve-wracking.
What are you looking for in your next step of care?
What are you looking for during the transition process?
What is important to you in a physician?
Do your own research
“I had an AMAZING pediatric GI when I switched, and I just went with who she recommended. Looking back, I wish I did my research because he is not who I would have chosen for myself. I would recommend doing your own research and make sure whoever you find is willing to work with you and thoroughly go through your medical history and all your results. Too many doctors seem to just think they know everything, but we know our bodies best and need to have a medical team who lets us advocate for ourselves.”-Danielle
Jennie has lived with IBD for nearly 20 years. She has a PhD, works in IBD care, and recognizes she has the privilege of a strong support network and insurance. As an IBD psychologist she recognizes how difficult the system and transition can be for everyone involved.
“I was diagnosed with IBD at 12 and transitioned to adult care around age 18. I was extremely sick at the time and ended up having a proctocolectomy within months of transitioning. I think the biggest things for me were the notable shift in culture between the peds and adult world, and the insurance pieces. It’s so much for kids and families. Lastly. I’ve noticed the transition is nuanced for my parents who were so good at being my advocates, they will still offer to call the doctor if I tell them I am not feeling well, and they have a tough time not having the same significant role they did when I was younger.”
Allie was diagnosed with Crohn’s disease when she was 12. Her mom attended all her appointments until she turned 18, and only stopped going then because she was out of state for college and seeing a pediatric GI there until she turned 22. Allie’s mom kept a medical binder of all her procedures, lab results, and details about her patient journey. She says when she phased out of pediatrics and started taking matters into her own hands, she found the binder her mom made to be beneficial—Allie found herself referring to it when she couldn’t remember everything.
“What helped the transition the most was going to appointments on my own when I turned 18. I felt more prepared to speak for myself when I switched to an adult GI.”
Allie’s mom also inspired her to ask the tough questions. After witnessing how her mom spoke up to doctors it empowered her to speak up and stop minimizing her struggles. By watching how her mom handled appointments, it inspired Allie to write down all her questions and concerns before doctor appointments, so she doesn’t forget anything.
“My mom asked me what fights I wanted her to fight for me and what I wanted to do myself. She guided me on what I might need to ask about when I had no clue—even as an adult she still offers to help call insurance companies to fight authorization battles. She gave me space to live my life when I turned 18. She worried, but she never hounded me for updates (are you taking your medication?, how are you feeling? Are you eating ok?”…but she always conveyed support (both my parents did) when I needed it most she showed up.”
Sari recommends young adults with IBD to ease into taking control of their care as early as possible.
“Things like refilling your own meds, scheduling your own appointments, and driving yourself to appointments goes a long way when it comes to learning how to stay organized and advocate for yourself. You don’t want to be doing all those things for the first time when you go to college or a start a new job—too many scary or unknown things at once!”
Check out what pediatric GI’s have to say about bridging the gap and ensure continuation of care.
Dr. Sandra Kim, MD, Associate Professor of Pediatrics, Director, Inflammatory Bowel Disease Center, UPMC Children’s Hospital of Pittsburgh, says, “Transition is the preparation process while the young adult/teens are still under the care of the pediatric team. Transfer of care is the actual “handoff” when the young adult moves from the pediatric GI team to the adult GI providers. Teens want independence but struggle with disease knowledge and self-management skills. Therefore, the pediatric GI team needs to help the teen (and the family, too!) by being active listeners, communicators, and educators. The healthcare team also should utilize things like transition tools.”
Dr. Kim went on to say that GI doctors need to assess how teens are doing on the road to greater independence and that shared decision-making helps build partnerships between adult and pediatric GI providers.
For the adult GI team:
Collaborate with the peds team in the initial stages of care transfer.
Anticipate existing gaps of knowledge and self – management skills
Prepare for more time during appointments for questions, additional education, and working with the family. Parents need help during this time of care transfer, too!
Woman patient signing medical documents discussing medication treatment with african american practitioner in hospital office during clinical consultation. Doctor physician explaining disease symptoms
Dr. Jonathan D. Moses, Assistant Professor of Pediatrics, Director, Pediatric Inflammatory Bowel Disease Program, UH Rainbow Babies and Children’s Hospital, explained how his hospital has a multidisciplinary pediatric IBD team that engages patients in a Health Maintenance Education Clinic as early as 11 years old.
“This allows them to build up the self-management skills needed for a successful transition to adult GI, when they are ready. In lieu of this resource, parents can engage their health care providers about ways to get their child more involved in their care and provide them with the autonomy, and support, to take over aspects of their care over a period of time.”
Dr. Hilary Michel, MD, Assistant Professor of Clinical Pediatrics, Nationwide Children’s Hospital, says a successful transition from pediatric to adult care requires that young folks have developed the knowledge and skills needed to understand and manage their disease independently.
“This knowledge and skill is not gained overnight, and ideally should be obtained gradually. Transfer to adult care should be planned in advance, when a patient is feeling well and has a good grasp on their disease management, so there are no gaps between peds and adult care. Parents and families can help the process by allowing teens to speak with their healthcare providers alone, gradually share care responsibilities, encourage them to learn about their disease, and highlight their successes.”
How this works in real time:
Patients can listen and participate in their visits.
Set goals with your healthcare team and work toward them, ask questions and share your opinions.
Healthcare teams can help by providing a non-judgmental space, listening attentively, encouraging young people’s success, engaging patients in decisions, checking for understanding, getting to know patients as people (talk about school, friends, activities), and connecting patients with resources
Dr. Whitney Marie Sunseri, MD, Pediatric Gastroenterologist, Assistant Professor of Pediatrics, UPMC Children’s Hospital of Pittsburgh, says “I always encourage a step-wise approach to transitioning to the adult world. I encourage patients to know their diagnosis, what medications they take and when, to recall their last scopes, and to be able to report all of their symptoms without the assistance of their parents. Then as they get older, and closer to the time of transition, I encourage them to look into different adult doctors. I give recommendations as well.”
Dr. Sunseri advises caregivers and patients to be proactive and look at reviews of doctors and who is in their insurance network. She says the most important visit is the one where patients follow up with her after their first adult visit to make sure it was a good fit and that they are in good hands.
“It’s bittersweet watching these children grow in so many ways and head off into the hands of another provider. Your heart swells with pride and breaks at the same time.”
Resources and Communities of Support
Sneha was diagnosed with Crohn’s at age six. She’s now 23 and still figuring out what her future will look like with IBD. As she grew up, she couldn’t find a community of young adults. This inspired her to create Generation Patient and the Crohn’s and Colitis Young Adults Network.
“Peer support during this transition is critical, so we host seven virtual community meetings. We have hosted over 250 of these peer support meetings over the last two years. I think peer support should be seen as essential during this transition period and it has been the best thing to come out of living with IBD.”
Generation Patient: Instagram–@generationpatient
CCYN: Instagram–@ccyanetwork
Join the American College of Gastroenterology Thursday, May 4, 2022 at Noon and 8 pm ET for a discussion about “Empowering Patients Through the Transition of Care in IBD”. Click here to register.
Whether you are a parent or not it’s heartbreaking to imagine how it would feel if you found out your child (no matter their age) was diagnosed with a chronic illness like inflammatory bowel disease. Of the more than six million people in the world diagnosed with Crohn’s and ulcerative colitis, approximately 25% of patients are diagnosed during childhood and adolescence, most of which are going through puberty. Impaired growth, pubertal delay, and low bone density are all common in children and teens with IBD. They can occur at diagnosis or at any time during a patient’s IBD journey.
As an IBD mom of three, who was not diagnosed until I was 21 years old, I personally don’t have the experience or perspective to share what it’s like to grow up with IBD or have a child diagnosed with it, so I tapped into several caregivers in our community, along with four leading pediatric gastroenterologists for input.
My hope is this article will serve as a helpful resource as you navigate the challenging waters of puberty with your loved one. Teen years are difficult enough without a chronic disease, taking a close look at how this impacts a young adult physically, emotionally, and mentally is something that deserves much more attention than a blog article.
Concerns from patients and caregivers
Before we get into the medical input, I want to share some of the messages I received this week from young patients and their caregivers so you can see firsthand how complicated this period of life is for everyone involved.
“I’m 14 years old. I was diagnosed with Crohn’s when I was 12, which marked an influential time in my life. It can be hard to cope with being diagnosed and having a chronic illness at that age. That year leading to my Bar Mitzvah, a cultural rights of passage from boyhood to manhood, was really challenging for me. At a time when changes are going on and puberty takes its course, learning to trust your body and that it is working is key. Rather than trusting my body, I had a lot trust issues. If my body could turn itself to work against me in my GI system, what’s to say it wouldn’t turn on me other ways? I am especially worried about my reproductive system. Since I was a little boy, I always knew I wanted to be a father when I grew up. Having kids and being a family man has always been my highest purpose in life. Since my Crohn’s diagnosis, I’ve felt anxious and worried about whether my Crohn’s or my body will stop me from fulfilling that dream.”
“I often worry about whether my son’s hormones will put him into a flare and wonder what the best way to approach the school about his Crohn’s is.”
“My biggest puberty concern is delayed growth or slowed growth and flares. I’ve heard a lot about puberty hormones really causing issues. Is there truth to this?”
“Will my almost 15-year-old son start puberty once his treatment kicks in or will he always look like a 12-year-old child?”
“My 15-year-old lost more than 15 pounds in the last year, we’ve checked all kinds of things, but can’t figure it out. He’s on renflexis (generic Remicade) and his colonoscopy came back clean. He gets full easily and deals with chronic constipation. I hope his IBD doesn’t stunt his growth.”
“The anxiety of managing IBD while combining that with the developmentally normal anxieties of the adolescent years can result in mental health issues that are hard to pinpoint. Body image issues that are normal as their bodies change, mixing with body image and food-related issues associated with IBD (good foods and bad foods, overly focusing on diet, etc.) which can lead into worrisome territory like disordered eating and worse. As children separate from their parents more with each passing year (which is normal), it becomes harder to monitor IBD symptoms and disease progression as a parent. As someone who has always been in the driver’s seat about IBD, this is a scary shift and I worry some symptoms will go unnoticed and become exacerbated.”
“That puberty will stop growth—growth has been severely impacted by Crohn’s before diagnosis and it did—hitting puberty early meant growth stopped and she only reached 4’9”/4’10”. Her periods also add to existing fatigue levels.”
“I worry about medication not working like it used to due to so much change in the body. I also worry about how she may feel about her image comparing herself to others at that age with so many scars or if she ever needs to have an ostomy bag. I worry her IBD will affect her cycles or make them more painful.”
“That my son will go into a flare requiring heavy intervention that goes far beyond our comfort zone, but we’ll feel trapped so he’s able to grow at the right time.”
“My 13-year-old son was diagnosed with Crohn’s a little over a year ago. He is doing ok now and on Humira bi-weekly. I’m mostly concerned about his growth, as he is small for his age. He has gained about 20 pounds in the last year, but he was malnourished as COVID made it difficult to get his diagnosis. Hoping he stays on track and continues growing and that his growth potential isn’t adversely affected by his IBD.”
“As a kid who went through being on high dose steroids while going through puberty, bless my mother!”
“Delayed puberty is a big thing. Also, how, and when is it appropriate to start transitioning responsibly for ultimate transfer of care. Mental health is often a concern for adolescents (anxiety/depression).”
“Flares. Many parents report puberty as being a challenging time for IBD. Imagine all the normal teen/puberty hormonal issues and then add IBD (and I say this as a lucky parent with our teens). I think every parent that makes it out alive should get a very long vacation. The #1 thing I hear from parents of kids with IBD is: “my heart breaks every single day”. Whether in remission or not, the disease is a persistent and heavy burden on patients and families. With all the noise, it’s important not to lose sight of this fact.”
“I was diagnosed with ulcerative colitis at age 13 and it all happened very quickly. I was in eighth grade – my body changed almost immediately after being put on prednisone. Being an early developer, puberty was a challenge for me. I didn’t look like most other girls in my grade. So when I started getting really bad acne and a swollen (moon) face from the meds, it was the icing on the cake. I remember ninth grade consisted of me coming home from school and crying to my mom because I felt what was happening to me was unfair. I’d have to excuse myself during classes to use the bathroom, so everyone knew what was happening. I was mortified. And although I was an “early bloomer”, I can’t help but wonder if I would have grown a bit more if I hadn’t been diagnosed, put on prednisone off and on for the first 3 years, or started on biologic treatment. There’s always the questions and mystery of what IBD has potentially taken away from me. But living with IBD also resulted in me growing up pretty quickly. I was able to navigate the healthcare system by the time I graduated from high school. I learned to talk about my body and my health – things that I don’t believe my peers could articulate by that time. So it came with some benefits – or at least things that I have been able to turn into positives. My experiences have made me a stronger person. And I’m thankful for that.”
Impaired Growth: Why it happens and what to watch out for
According to Dr. Sabina Ali, MD, Associate Clinical Professor, Director of IBD program, UCSF Benioff Children’s Hospitals, the most common extraintestinal manifestation of IBD in children is impaired growth, particularly in Crohn’s disease and that’s also what she hears from patients and their families when it comes to their greatest concern.
“Growth is a dynamic marker of overall health in children and adolescents, which occurs in 10-30% of cases. Short stature and failure to grow can precede IBD symptoms. It is important to monitor nutrition and growth closely and as this can lead to delayed puberty. Make sure the child is routinely getting height, weight and BMI measured. Growth impairment is more common in males than females with Crohn’s disease. It’s important to get disease in remission.”
Dr. Ali went on to explain that growth issues are more frequently seen in children who have never been in remission or for those who have dealt with flare ups in the pre-pubertal period.
“Pubertal delay may potentially decrease bone mineralization and affect quality of life in children who realize that their sexual maturation is different from their peers.”
Dr. Jonathan D. Moses,Assistant Professor of Pediatrics, Director, Pediatric Inflammatory Bowel Disease Program, UH Rainbow Babies and Children’s Hospital, agrees that remission is essential as a first step to ensure normal bone growth and pubertal development. Most of the time the concerns we hear about puberty and IBD is at the initial diagnosis when parents will note that young women have not started their menstrual cycle yet at the expected age or young men have not started their “growth spurt” yet.
“Growth is a key element of children diagnosed prior to puberty. Our goal is to provide the therapy that will allow them to be in continuous remission and achieve their final adult height and avoid any pubertal delays. If there are any concerns with this, we typically place a referral to the pediatric endocrinologist to help co-manage this.”
According to this University of California San Francisco study, boys are three times more likely than girls to deal with one of the conditions most devastating effects: the failure to grow normally. Researchers were surprised by this finding because the study also found girls had a more severe disease course than boys.
Dr. Ali says that a novel finding is that a high proportion of patients with ulcerative colitis exhibited continued growth, suggesting delayed skeletal maturation is also frequent in ulcerative colitis, contrary to common assumptions. For patients exhibiting continued growth, median final adult height was greater in males with ulcerative colitis than males with Crohn’s disease but did not differ significantly in females with ulcerative colitis, compared with females with Crohn’s disease. This finding supports the growing body of literature that statural growth impairment is more common in males than females with Crohn’s disease.”
Dr. Hilary Michel, MD, Assistant Professor of Clinical Pediatrics, Nationwide Children’s Hospital, explains the importance of monitoring pediatric GI patients’ weight, height, and pubertal development over time. She says measuring weight and height and asking about pubertal development helps make sure each patient is tracking along their growth curves and developing at an appropriate rate.
“In addition to monitoring IBD symptoms and checking labs, stool tests, and scopes, monitoring growth and pubertal development is another way to make sure we are treating IBD inflammation completely. If a patient is not going through normal stages of puberty, or is going through puberty more slowly than expected, it’s a hint that we should check on their IBD disease control! And if their disease is in control, then we need to think of other causes for delayed puberty and get them in to see the right experts to help.”
Dr. Sandra Kim, MD, Associate Professor of Pediatrics, Director, Inflammatory Bowel Disease Center, UPMC Children’s Hospital of Pittsburgh, says along with monitoring growth and nutritional status, it’s important to keep a close eye on emotional state and quality of life.
“It’s important children understand their disease, and for families and the care team to understand where the child is not only medically, but psychologically and developmentally. As a pediatric gastroenterologist, who focuses on the care of children and teens living with IBD, I know I have a unique relationship and responsibility as I watch “my kids” grow up.”
Dr. Kim says, “We see growth impairment in children and teens with Crohn’s much more so than with ulcerative colitis, especially with extensive involvement of the small intestine. Active inflammation in the small intestine can impact an individual’s ability to absorb nutrients. IBD also impacts appetite and can lead to inadequate nutrition.”
According to Dr. Kim, studies have shown up to 80% of children (males>females) have some degree of both weight and growth impairment when their Crohn’s is not controlled. While studies do vary in the range affected, it’s clearly a significant issue.
Medication and the pubescent years
In general all pediatric gastroenterologists try to limit and shorten the exposure of steroids in children.
Dr. Ali says, “Recent inception cohort studies in pediatric IBD have highlighted baseline phenotyping of patients to predict the severity of their disease course and help identify who will benefit the most from early biologic treatment. Biologic therapies have improved outcomes in pediatric IBD, including achieving mucosal healing as well as improved growth and pubertal development.”
Prior to this, the goals of treatment in Crohn’s disease were focused on controlling symptoms, enhancing quality of life, minimizing complications to prevent surgery, and restoring growth in pediatric patients. Evidence has shown that mucosal healing is associated with sustained corticosteroid-free clinical remission, reduced hospitalization, and lower surgery rates. According to Dr. Ali, biologics are the most effective in inducing and maintaining mucosal healing in this patient population.
Dr. Moses explains how biologics are decided upon with young patients.
“The age of the patient, in the context of the biologic era, does not seem to play a significant role at our center. If a child, regardless of age, needs a biologic medication, then we will typically proceed with this after shared decision making with the family. As a rule, for all ages, we work very hard to limit steroid exposure, both by planning out their maintenance therapy right away or using exclusive enteral nutrition (EEN) to induce remission in our patient with Crohn’s disease.”
Dr. Michel says it’s important to get IBD under control quickly since the window to achieve the goal of remission is so small.
“Because of this, growth and pubertal delay can be reasons to start a biologic as first line treatment. If steroids are used, they should be short-term (induction therapy only) to prevent negative impacts on growth and bone health. These patients may also be great candidates for exclusive enteral nutrition to treat their IBD, as it can help heal inflammation and address malnutrition without the side effects of steroids. Involving an experienced dietitian is key!”
While research has shown that disease activity may fluctuate with hormonal shifts (like those that happen with puberty, pregnancy, and even menopause), Dr. Michel says she is not aware of any specific data to connect loss of response to therapy because of puberty.
Puberty gets delayed
For pediatric patients in whom remission has never been achieved or for those who have frequent relapses, puberty is often delayed.
“The endocrine-hormonal mechanisms responsible for pubertal delay associated with inflammatory disease are incompletely understood. It is thought to be due to effect by both nutrition and inflammation,” said Dr. Ali.
Delayed puberty or delayed linear growth can be presenting signs of IBD to help clinicians make the diagnosis.
“Once these pre-teens achieve remission, they will begin to progress through puberty again and have improvement in their bone density, if it was low at baseline,” says Dr. Moses.
Dr Michel says, “The best way to ensure normal growth, weight gain, and pubertal development is to make sure their mucosa is healed. It’s also important we address low weight or malnutrition. If we’ve confirmed that IBD inflammation is resolved (through labs, stool tests like calprotectin, and scopes), and that patients are getting the nutrition they need, and we’re still seeing delayed puberty or slow growth or weight gain, this may prompt a referral to an endocrinologist, adolescent medicine doctor, or gynecologist to look for other causes of these problems.”
By adequately treating IBD and achieving mucosal healing, kids have the best chance to grow and develop normally and have healthy bones.
“Inflammation affects hormones important in growth and pubertal development, and delayed pubertal development is closely tied with poor bone health,” explained Dr. Michel. “Active inflammation can also worsen malnutrition and lead to low weight, which can delay puberty. These variables are often closely related; for example, a patient with active IBD may not feel well enough to eat regularly and lose weight or be malnourished. Or they may eat well but not be able to absorb the nutrients from their food. Or they may lose nutrients through stool or vomiting. So, treating inflammation and treating malnutrition are KEY to optimizing outcomes for kids and teens with IBD.”
Causes for the delay in puberty and decreased bone density can be multifactorial.
“Things we consider include nutritional deficiencies (not absorbing enough and/or not getting enough into your body), and the impact of inflammation (though pro-inflammatory cytokines – the “chemicals” produced by activated white blood cells – on sex hormone production, as well as growth hormone),” said Dr. Kim. “Other factors that can specifically impact bone density – decreased physical activity which leads to decreased muscle mass.”
When determining a course of therapy, a child’s quality of life and the impact of active IBD must be taken into consideration.
Dr. Kim explains, “Steroids have a great deal of side effects: external appearance (“moon” facies), psychological (can exacerbate underlying anxiety and depression; can impact sleep), bone health (decrease bone density and increasing risk of fractures), impact on wound healing, increased risk if long term on the GI tract (i.e. perforation), increased blood sugar (hyperglycemia), high blood pressure.”
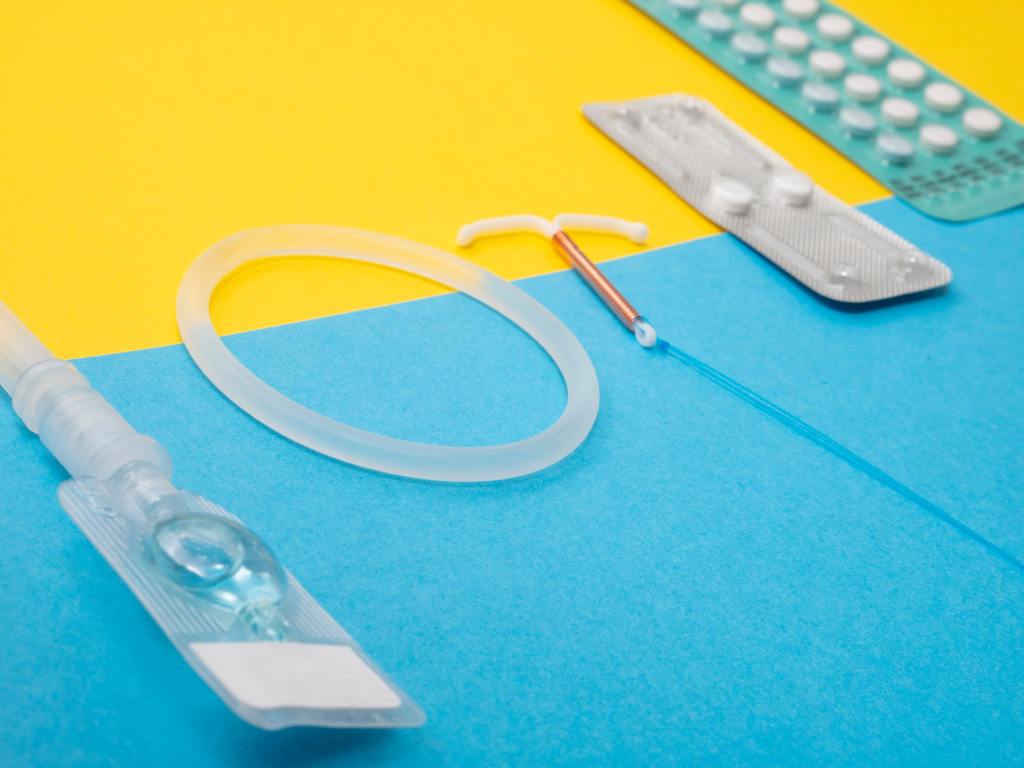
What’s the deal with birth control and IBD?
Each pediatric gastroenterologist featured in this piece says they have heard from both patients and parents about oral contraceptives aggravating IBD. Dr. Ali says oral contraceptives are consistently linked to an increased risk of IBD.
Dr. Michel says since menstruating is a normal part of development for female patients, active inflammation, low weight, and malnutrition, can all play a role in delaying the onset of it. If a patient is flaring, they might have irregular periods or stop getting their period for some time. Once the problem is addressed—inflammation controlled, normal weight achieved, and malnutrition treated, menses typically resumes. IBD symptoms can also be exacerbated during menses for some women.
When it comes to choosing to go on birth control, and what birth control to choose, Dr. Michel advises patients and parents to be clear about their goals and weigh the risks and benefits.
“Goals for starting birth control can include regulating heavy periods or bad cramps, preventing pregnancy, improving premenstrual symptoms (mood, headache, fatigue), or even managing acne. There are some data about birth control pills increasing the risk of developing IBD, but research is conflicting about whether they increase the risk of flare. I would encourage any patient who is interested in starting birth control to talk with her gastroenterologist about what options might be best for her. An adolescent medicine doctor or gynecologist can also be extremely helpful to have these conversations, weigh pros and cons, and help young women and their families make informed decisions.”
Dr. Kim is no stranger to hearing concerns about the impact of oral contraceptives. She says it’s tough to determine whether birth control specifically aggravates disease.
“Women who have increased diarrhea and cramping around their cycles may have improvement in these symptoms when on birth control. Currently, there is not enough data to suggest birth control directly leads to aggravation of underlying IBD. However, there are other issues to consider when a young woman chooses the type of birth control. There is increased risk of venous thromboembolism (increased risk of forming blood clots) in individuals with IBD. There also is an increased risk for clots associated with combination oral contraceptives whether a young woman has IBD or not. Therefore, a woman who has IBD and goes on oral contraceptives not only has a higher risk of forming significant blood clots, but with more significant consequences from this.”
Dr. Kim’s recommendation? Avoid oral contraceptives with an estrogen component, if possible. Depo-Provera is an alternative, but you need to be aware that it can impact bone density. She says IUDs are safe and highly effective
How best to support young patients
Support groups: Discuss concerns regarding how a patient is coping with the IBD team. A social worker or psychologist on the IBD team can be a great resource.
Psychosocial assessments
Care coordination
Supportive counseling
Connection to resources
“As a pediatric gastroenterologist, my contribution is to manage their therapy as best I can to achieve remission. After that, we rely on our multidisciplinary team to address the psychosocial aspect of the disease and how this affects them at this stage in life,” said Dr. Moses. “Finally, we encourage the families to get involved with the Crohn’s and Colitis Foundation and attend Camp Oasis, if possible, to meet other children their age who also have IBD. This builds up their social support network in a way that can be life changing for them.”
Dr. Michel says, “I try to normalize their feelings, and reassure them that with effective treatment and achieving remission, we are working toward them reaching their full potential. I also think it’s a great time to involve experts like psychologists and child life specialists to help work through these concerns. Parents will often also ask about future fertility (kids and teens usually aren’t thinking of this yet)! It’s always a huge relief for families to learn that we expect normal fertility for our young folks with IBD and that the best way to ensure this is to get good control of disease.”
She advises parents to acknowledge how challenging it can be to go through puberty with IBD.
“Any feelings they’re feeling – frustration, anger, sadness – are ok. Then, I would encourage parents and patients to share these emotional and physical struggles with their healthcare team. Many centers have fantastic psychologists, social workers, and child life specialists that can help young people understand their disease, explore their emotions, and develop healthy coping skills that will serve them now and into adulthood. There are also fantastic resources online through ImproveCareNow and the Crohn’s and Colitis Foundation,” said Dr. Michel.
Dr. Kim advises parents and patients not to be afraid to ask pediatric gastroenterologists and their healthcare team for help.
“I really believe it takes a collective effort to support our children and teens. We are living in an unprecedented time with the COVID 19 pandemic (which has led to social isolation and new stressors with school, peers, and family dynamics),” she said. “Seeking our behavioral health resources (psychology, psychiatry, counseling, social work) is NEVER a sign of weakness – quite the opposite. One thing I would love to see: elimination of any perceived stigma when addressing issues around mental health. It is so crucial to address stress, anxiety, and depression. Besides the obvious impact on quality of life, we know that anxiety and depression can negatively impact an individual’s IBD itself. For the parents out there, I tell them they must check their own guilt at the door. The parents did NOT do anything to cause their child to develop IBD. I always say that you can be mad at the disease but never at themselves.”
Connect with these physicians on Twitter:
Dr. Sabina Ali: @sabpeds
Dr. Hilary Michel: @hilarymichel
Dr. Jonathan Moses: @JonathanMoses77
Dr. Sandra Kim: @SCKimCHP
Let this piece serve as a conversation starter as you discuss your child’s health with their care team. Ask the questions. Get empowered by learning and educating yourself more. As chronic illness patients and parents, it’s a constant learning curve—with each setback and triumph we gain newfound understanding and perspective. Stay tuned for an upcoming article on Lights, Camera, Crohn’s with guidance regarding making the transition from pediatrics to adult doctors.
As the weeks of war go by in Ukraine, our IBD patient advocate extraordinaire, Elena Skotskova, continues to do all she can to ensure those with Crohn’s disease and ulcerative colitis are feeling supported in the face of the unknown. Elena and I have become pen pals of sorts over email. A world away. Our worlds so different. But our understanding of what it’s like to live with IBD very much the same. Here’s Elena’s latest update sent April 13th, 2022. She remains about 30 minutes outside of Kyiv at her mother in law’s home.
Dear Natalie! Now we are engaged in the distribution of humanitarian aid, which came to us from Dr. Falk (a German pharmaceutical company). I want to share with you the information about helping Ukrainian patients with IBD. Ever since we received the medicine from Dr. Falk we did a great job: 1. We sent medicines to 12 hospitals in different cities of Ukraine, where patients with IBD are treated; 2. We have collected more than 400 applications from patients who currently do not have the opportunity to go to their doctor. 3. We have sent more than 200 packages of medicines to patients throughout Ukraine who do not have access to a doctor 4. There are still about 200 parcels left to send, and I think we can do it before the end of the week.
We have received a large number of letters of thanks from patients who have received medications. We tried to ensure that all patients had enough treatment for at least two months. Earlier we received two parcels from our Greek friends, which were sent via Poland. Everything that was in those parcels (medical food, colostomy bags, medicines, etc.) we distributed to patients and hospitals.
On Monday, April 11, we got a big package from Estonia with colostomy bags and stoma care products. We also send colostomy bags to patients who need it.
I have a lot of work now, and I am constantly in touch with patients. We have a lot of requests from patients from different parts of Ukraine. Particular pain is the regions that are occupied by Russia. It is impossible to deliver medicines there, it is impossible to help patients. I hope that someday they will be able to get out through humanitarian corridors, and then they will receive medical assistance.
This is Galina, our volunteer, a doctor who herself sent more than 300 packages of medicines to patients. She lives in Lviv, where humanitarian aid comes from Europe. This charming lady herself takes heavy boxes, sorts them, forms packages, and sends them out to patients. She does this at night 🙂 And during the day she treats people. I am very grateful to her, she is an irreplaceable person in our team.
I also wanted to share information with you we set up on our “Full Life” site that gives people around the world the ability to make donations using credit cards. You can do it from the link https://www.gofulllife.com.ua/donate/ Scroll down and click the: “Help the project” (Допомогти проекту) button. Once there, you will be directed to choose a currency. (USD or EUR, depending on which currency the credit card supports) and write the sum.
A pre-war photo of Elena and her friend and fellow volunteer, Alexandra.
The money raised will be used to buy medical nutrition for children with IBD and to buy medicine for IBD patients who have lost their jobs and incomes.
My husband and I are going to go to Kyiv on Saturday (April 16). We need to meet the humanitarian cargo from Lviv. And also, I need to deal with colostomy bags that came from Estonia and send them to patients.
Many people are already returning to Kyiv, I hope that my hairdresser will also come back and cut my hair 🙂 During the war, it is a great happiness for us just to get a haircut or get medicine. We have such small military joys.
As she fears for her life each day and every night in her homeland of Ukraine, ElenaSotskova thinks back to when her body started going to war against ulcerative colitis. She was 21 years old. Now, as a 47-year-old IBD mom, she shares firsthand experience of what it’s like to live in absolute chaos and devastation while trying to manage a chronic illness like IBD. Every morning Elena and her family wake up at 6 a.m. to the sound of explosions and gunfire. Oftentimes the internet and electricity go in and out, with repair workers constantly having to restore power.
Before we get into the utter heartbreak and unthinkable sadness, here’s some background. This isn’t the first time Elena has had to run from her home to try and reach safety. Shortly after her ulcerative colitis diagnosis, she fled with her 3-month-old daughter to Kyiv from Crimea, to avoid an abusive husband. At the time, she had the equivalent of 25 U.S. dollars in her pocket. Prior to becoming a mom, Elena worked for one of the largest banks in Ukraine, so she was confident she’d be able to land back on her feet in no time and support herself and her daughter. The stress of the divorce and being forced to start anew exacerbated her IBD.
“My condition was worsened by constant diarrhea, bleeding, low hemoglobin, and as a result, constant fatigue. I tried not to pay attention to it as I needed to work and make money for myself and the baby. My ulcerative colitis limited what I could do and where I could go. I used to be unable to go for walks unless I know where the restrooms were. I always had spare clothes with me and wet wipes, in case I did not make it in time.”
Since then, Elena has managed her ulcerative colitis with Mesalamine, in large doses (6-8 grams per day).
“In Ukraine at that time there was no biological therapy, and even clinical studies of such therapy did not take place. All that was available to patients were hormones and mesalamine. In addition, in Ukraine there is no compulsory insurance medicine (until now), there are no state programs for the treatment of patients with ulcerative colitis and Crohn’s disease, so I and other patients must buy drugs with our own money. And they are, as you know, not cheap. Compared to the level of income in Ukraine, it is expensive.”
How love found its way
Elena says she was working to buy her medicine. It felt like a vicious, never-ending cycle. But Elena’s luck in the love department took an amazing turn.
“I was lucky, I met a wonderful man, named Leonid who has a son. Leonid later became my second husband. I immediately told him about my illness. He accepted me, my IBD, and my child. He wouldn’t turn away from me or be ashamed when I had an accident at an event or in a public place. He helped me and supported me. And as a result, I stopped being nervous about my ulcerative colitis. I stopped worrying, and after I became calmer, the disease slowly began to subside.”
Leonid also started to take care of all the costs associated with her IBD treatments. Elena credits him for reviving her medically and emotionally, allowing her to reach remission after chasing after it for years. She was able to travel comfortably away from home and see the world through a different lens.
Prior to the war with Russia, Elena had big plans for herself. She aspired to begin her MBA and travel to English-speaking countries.
When the explosions hit
“All plans collapsed at 4 a.m. on February 24, 2022. We woke up to the explosions, saw the message “The Russians are bombing Kyiv, the war has begun.” That was more than a month ago, but it seems like we’ve been living in this nightmare for ages.”
Elena’s daughter, Alina, had recently arrived in Poland to study, but she happened to be home in Ukraine with family when the war started. Prior to this happening her travel plans were to fly back on February 27th. Of course, that all changed.
“She was supposed to fly back to Warsaw on Sunday, but war broke out on Thursday. Immediately, air traffic over Ukraine stopped. And hell began. Kyiv was bombed from the very beginning, we sat in the bathroom during the air raid, went down to the basement or went to the shelter. We did not turn on the lights in the apartment and taped the windows with duct tape so that they would not be knocked out by the explosions. We walked the dog for 5-10 minutes, near the house, so that if the shelling started, we could quickly hide. We live in Kyiv on the 7th floor, and most of all I was afraid that a bomb would hit our house, and we would either be overwhelmed or burned in a fire.”
Elena says for days on end she sat with her husband and daughter in their apartment. Alina would constantly cry. They learned that evacuation trains were leaving Kyiv for western Ukraine. At this point, they decided to send Alina back to Poland.
Nights spent at the railway station
“The most terrible were the three days that Alina and I spent in the basement of the railway station in Kyiv. There is a curfew, you cannot go outside in the evening, in addition, it was dangerous to go outside, because they are constantly shelling. My daughter and I got to the train station and decided to wait here until she could take the train to safety. My husband and son stayed home with the dog.”
The trains to leave Ukraine were like something out of a horror movie. Instead of a train car fitting the usual four people, they were packed with 20-plus people. People were ready to stand for an entire day just to leave Kyiv.
“Alina could not get on the train that was going to Warsaw, and we stayed overnight at the station. At night, the air alarm did not cease, explosions were heard, we went to the shelter (basement) of the station, which for three days turned into a home for us. We tried to sleep on the floor, it was warm, but the main thing was that it was safe. Finally, on the second day, we managed to put Alina on the train to Lviv. She left, and I was standing on the platform crying and praying that the train on the way would not be shelled, and my daughter would reach Lviv intact.”
Elena had to stay alone at the train station for an additional night because of the curfew in Kyiv. She was afraid her IBD would start acting up from the overwhelming stress and worry and terrified she was going to be killed.
“My gut understood me, it “behaved quietly”, and did not give me cause for concern. During the 21 years of illness, I learned to negotiate with him. On the fourth day, when the curfew was lifted, I was finally able to return home, wash myself and clean myself up. And my daughter had already reached Poland and was safe. We thought that somehow, we could adapt to this situation. We had food, water, gas, electricity, and Internet. We thought that we could somehow live in Kyiv. But this turned out to be unrealistic, as soon as dusk came, the city was pierced by an air alarm, it turned on several times during the night.”
Deciding to leave Kyiv
Bombing began each morning between 3 and 4. Elena and her family stayed in their clothes and didn’t sleep. She would take her dog and lock herself in the bathroom while her husband and son were standing in the hallway where there were no windows.
“Then a cruise missile hit a television tower, close to our house. It was afternoon, her son had just gone out to the store for bread, and there was an explosion, a crash, a fire. People who were nearby were killed. My husband said that we needed to leave Kyiv, it was extremely dangerous.”
So that’s what they did. They left for Elena’s mother-in-law’s house who lives in a village outside of Kyiv. There are no military or infrastructure facilities there, so they are hopeful it will not be bombed. As you are reading this, Elena is still there.
“In the village it is calmer, the battles are 30-40 kilometers (20-30 miles) away, we constantly hear artillery shots, gunfire, explosions, and flying missiles. But there is no air raid alarm, which was so exhausting in Kyiv. It’s still impossible to sleep normally. We are afraid that we will be occupied, and we are not where there are active battles.”
Running out of IBD medicine
But, Elena now faces another major issue. She will run out of her IBD medication this week and there is no way to buy it or receive it. Since the war started, she’s heard from countless other patients in the same bind. Doctors have fled, there’s no place to safely receive treatment, and for those who are now refugees or without jobs, they struggle to afford their medications. Elena knew she had to do something.
“I began to write to the European Crohn’s and Colitis Association, manufacturers of drugs, everyone who I could, to find out how to help our patients. Poland and Estonia immediately responded. They understand if Ukraine does not resist, the war will go on, to Poland, and the Baltic countries may also suffer. Now we are in constant contact with our European colleagues and are waiting for humanitarian assistance from them. Packages from Greece are supposed to arrive any day now.”
While Elena’s ulcerative colitis is under control now, she’s been forced to reduce her daily medication dose by half to try and keep medication in her body for as long as she can. She’s starting to feel that reminiscent pain we all know too well when our intestines are making themselves known. The pain, bloating, and diarrhea have been more consistent for her, but she doesn’t feel she’s flaring yet.
“I’m very scared that if I go into a flare, there will be no one and no place to treat me. I am afraid that this war will drag on for a long time, and then it is impossible to predict the condition of either mine or our other Ukrainian patients.”
Her friend was able to find her mesalamine in Kyiv. She bought the medication, but it’s been a week now and the package has not arrived to Elena’s new address. Tomorrow (March 31), Elena’s husband will venture back to Kyiv to try and get Elena the medicine she relies on.
She tells me she no longer cries or has emotions and that every day feels like déjà vu. Sometimes she feels like a robot in an out of body experience. Elena says the Ukrainian people are steadfast, strong, and remain hopeful they will be victorious in the end.
Tomorrow on Lights, Camera, Crohn’s you’ll learn about Elena’s inspiring patient advocacy prior to the Russian invasion, how she co-founded an IBD organization to support the patient community, and how she’s working day and night right now to help the approximate 11,000 Ukrainians who live with IBD and are struggling to manage a disease while living through a war.
When you think about IBD and motherhood, you may instantly imagine a woman who has dealt with her disease for years before getting pregnant. But that’s not always the case. This week on Light’s, Camera, Crohn’s we hear from IBD mom, Angela Knott. She was diagnosed with ulcerative colitis when she was 17 weeks pregnant with her second child in December 2020. While a circumstance like this is rare, it is possible and complicated.
Between navigating the pandemic and a chronic illness, this diagnosis rocked her world. Angela was living in Australia (away from all family and friends) because her husband is a U.S. Navy pilot. They were on orders for a pilot exchange program in Adelaide, South Australia. Angela and her family now live in Texas.
She reflects on her journey as a woman and mother with ulcerative colitis and how it felt to receive a chronic illness diagnosis while trying to bring a baby safely into this world. Prior to being diagnosed with IBD, Angela was in perfect health. She never had a cavity or even broke a bone. She grew up being extremely active and is in excellent shape. Her first pregnancy in 2018 was flawless and uneventful. She carried her daughter to term and had no issues. But everything started to change when she was 15 weeks pregnant with her son.
“During this time, I experienced severe fatigue, anemia, stomach pain, stomach cramps, and weight loss (I lost 15 pounds over two weeks). After a few days of symptoms, I went to my doctor, and I told him all about my symptoms and how I was concerned something might be off with my pregnancy. He told me I was lactose intolerant and that I needed to limit my dairy intake. I did this for three days and then I went back to the doctor because my symptoms were getting worse.”
Angela was then tested for salmonella poisoning and two days later, the test result was negative. By this time, she had already lost 10 pounds and she was becoming scared that something was wrong with her baby. She got a second opinion and was told she likely had irritable bowel syndrome (IBS). That doctor wrote a referral for a gastroenterologist.
“That same evening, I ended up in the hospital due to my symptoms worsening and I was scared my baby’s health was declining since I was so ill. I was told to immediately go to the Women and Children’s Hospital to have the baby monitored (in Australia, this is a hospital for pregnant women, children, teens, and babies). I was more concerned about my baby’s health rather than my own which, is why I went to a hospital that assisted pregnant women.”
While at the hospital, Angela’s baby was monitored and doing well. She was given IV fluids to help with dehydration and she started to feel better. She went home and rested, again being told she likely had IBS.
“Shortly after getting home, I started vomiting and this continued for the next two hours. After speaking with my husband, we decided I needed to go to the ER because something was seriously wrong, and I needed treatment.”
Seeking emergency care during Covid
Due to Covid restrictions in December 2020, Angela’s husband had to drop her off at the emergency room and could not go in, only adding to an already stressful and worrisome situation.
“After reviewing my blood work and hearing about my symptoms, a gastroenterologist at the hospital stated I may have colon cancer, ulcerative colitis, or Crohn’s disease. I knew what IBS was, but I had never heard of UC or Crohn’s before. On top of being told I may have an autoimmune disease or cancer, he told me I needed to have an endoscopy to check for potential inflammation in my colon and that this procedure could result in me miscarrying since I was going to be put under. I had never been so scared in my life.”
Angela underwent the endoscopy in the morning and sure enough, she was diagnosed with ulcerative colitis. She was close to having a toxic mega colon.
“It was a blessing that I went to the ER when I did because if I had waited a day longer, my colon would have become toxic, and my organs would have potentially shut down thus impacting my baby’s life. Later that afternoon, I met with another gastroenterologist, and he gave a thorough explanation of UC and my treatment options. He explained to me I would need Remicade infusions every 6 weeks throughout my pregnancy until I was 36 weeks pregnant. Within the next hour, I received the Remicade infusion.”
She stayed in the hospital for one week and was released on December 23, 2020. Angela received another infusion on Christmas Eve and stayed on a special diet for the next week. Within two weeks, her symptoms had drastically decreased, and miraculously remission seemed to be on the horizon.
“When I started the biologic, I was extremely nervous about how it would affect my baby’s health as well as mine. I was told it was safe for pregnancy, but it was scary knowing that my baby would be exposed to an immunosuppressant drug. I was very cautious during my first pregnancy as well as the first few months of Henry’s pregnancy, so it went against everything I had prepared for and wanted. On the flip side, I also was concerned about how malnourished I was from being so sick. I didn’t want to cause any more issues to my body or cause something to go wrong with my pregnancy.”
Initiating Remicade while pregnant
When Angela was 28 weeks pregnant remission became a distant thought, as her body was rejecting the infusion and she started flaring, again. She had a flexible sigmoidoscopy which showed she had severe amounts of inflammation in my colon.
“At 30 weeks pregnant, my bloodwork showed that my colon was nearing toxic levels and that I needed to have my baby early to ensure my organs didn’t shut down. A few days later, I was admitted to the hospital and my baby, and I were monitored for a week. I was given fluids and steroids to assist with the inflammation (a steroid shot was also given to me for my baby’s lungs). At this point, I had to switch OBs and delivery hospitals since I was admitted to a hospital that dealt with high-risk patients. This was the best decision possible since I was given an amazing team of doctors and specialists.”
Angela and her son were monitored closely. Four medical teams were on board to do all they could to ensure a healthy delivery—NICU, colorectal team, OB, and gastroenterology.
Her miracle baby, Henry, arrived 8 weeks early via an elective c-section April 1, 2021. Angela had a classical c-section (vertical incision on her abdomen) because after she delivered the colorectal team had to check her colon for inflammation.
Luckily, the inflammation was “only” considered mild to moderate. Angela’s bloodwork the day before had showed her colon was near toxic levels. She had been prepped for a possible ostomy. Fortunately, she still has her colon.
How Henry was after birth
Angela’s son was born extremely healthy and came out breathing on his own. He spent the first six weeks in the NICU to assist with growing and feeding and remained in the hospital for an additional week.
“I received another Remicade infusion a few hours after delivering as well as an additional infusion a few days later. Within 24 hours of delivering Henry, I felt like my old self again (pre-UC diagnosis) and I was almost immediately in remission. It was determined my UC was most likely dormant for years and my pregnancy triggered it. Additionally, my initial pregnancy flare started shortly after my second trimester and the Remicade failed when I started my third trimester. My medical team thinks my pregnancy hormones caused a lot of my issues.”
Postpartum as a newly diagnosed IBD mom
In the months following Henry’s birth, Angela was relieved to be feeling more like herself. The fear of a looming flare worried her as a stay-at-home mom. She ended up losing 30 pounds during her pregnancy and was recovering from a very painful c-section.
“Fortunately, I did receive counselling services throughout my pregnancy (after I was diagnosed) and postpartum which helped.”
Due to being on so many different medications and having a stressful birth, Angela had a low milk supply and therefore breastfed, pumped, and supplemented with formula the first few months.”
“I was grateful my baby and I are alive; every day I rejoice thinking of how far we have come, and I am extremely grateful he is healthy and happy. I now have a deep understanding of how short life is and I no longer stress about life’s minor hiccups. I constantly count my blessings and greatly appreciate my health which I took advantage of before my chronic condition. I am a mentally strong person now and I have amazing coping skills because of my diagnosis.”
Angela still receives Remicade infusions every 6 weeks and is extra mindful of her health. She works out a few times a week, eats healthy, watches her stress levels, and makes sleep and rest a priority.
“I am doing everything I can to stay in remission and have been flare-free for almost a year. Every three months, I see my gastroenterologist and have bloodwork taken to ensure my health is on track. Prior to staying home with my kids, I was a teacher and I plan to return to the classroom soon. I am blessed to know I have biologic options to help me stay in remission so I can be successful in the classroom.”
Despite only being diagnosed with ulcerative for 15 months, some days Angela feels like it has been years.
Here’s Angela’s advice for other women dealing with an IBD diagnosis prior to getting pregnant, while pregnant, or after delivering:
Seek out mental health assistance during challenging times and find a support group either locally or through social media to connect with others who live with IBD and understand your reality. Angela’s favorite Facebook group is: Ulcerative Colitis Support Group, which has 36,000 members.
Ask all the questions. Don’t hesitate to reach out to your care team whenever you’re unsure about something or want clarity. Do all you can do educate yourself on your condition.
Get a second opinion. Don’t feel bad about seeking care from multiple specialists to ensure you are making the best decisions for yourself.
If you’re a faithful person, lean heavily on prayer and trust that God will watch over you through the highs and the lows of your illness.
Communicate as best you can with family and friends. Angela is grateful for the love and support of her husband.
With mask mandates ending for most states across the country and the CDC once again changing its guidance about masking, it’s a cause for concern for many who are immunocompromised or considered higher risk for Covid-19. As an immunocompromised mom of three kids under age 5, I feel a bit uneasy about the shift in measures, even though I had Covid-19 in January. I contacted my GI this week to ask her opinion on the mask mandates lifting and navigating this time as an IBD mom. She didn’t hesitate for a second and told me to keep masking—not only for myself but because of my kids. She herself hasn’t stopped masking in public and doesn’t plan to anytime soon.
I polled my followers on Twitter and Instagram by asking: “Do you still wear a mask in public, indoor spaces?” Nearly 500 people responded. On Instagram, 69% responded “yes” to still wearing masks and 31% responded “no”. On Twitter, 88% responded “yes” and 12% responded “no”.
This led me to dig a bit deeper and hear what several top gastroenterologists who specialize in inflammatory bowel disease had to say on this controversial and politicized issue.
Dr. Aline Charabaty, MD, Assistant Clinical Director of the GI Division at Johns Hopkins School of Medicine, and the Director of the Inflammatory Bowel Diseases Center at Johns Hopkins-Sibley Memorial Hospital, offered several fantastic analogies for the IBD community. The one that really hit home to me was talking about family planning and remission in Crohn’s and ulcerative colitis. If you are flaring and want to start a family, the rule of thumb is to be off steroids for at least six months to ensure disease activity is calm. We JUST got through the rampant spike in omicron cases last month. In her opinion, going maskless this soon after that highly contagious variant is premature. She believes we need to wait longer to make sure we are out of the woods and that conditions need to be more stable for a longer period of time. Until then, she recommends those who are more susceptible in the IBD community continue to mask as an extra safety net.
“We are not out of the pandemic. Sure, there are less deaths and fewer severe cases, but people are still getting sick. We saw this happen when we let our guard down and delta hit…then omicron. When you are driving, you wear a seatbelt, follow the speed limit, try not to tailgate, and follow the rules of the road. These are all precautions to drive safely to your destination and avoid an accident. You don’t just do one thing to prevent a car accident. With Covid, we got the vaccines, we’re wearing masks, we’re limiting exposure to large crowds, and measuring risk versus benefit for each of our decisions. It’s not a pick and choose situation of how to keep ourselves and others out of harm’s way.”
Dr. Charabaty went on to say why get sick with something when we really don’t know the long-term effects. We already see Covid can cause a higher risk of depression, heart disease, and autoimmune issues.
“Wearing a mask is such a simple measure. If it adds a benefit, I don’t see why people are saying no to this. This virus can really change your body. Why not add another layer of protection to prevent illness? There are no downsides to wearing a mask, so why not wear it? When you are out and about there are people with weakened immune systems, cancer patients, organ transplant recipients, people on multiple IBD medications…why put these people at risk of infection? The more Covid is transmitted, the higher the risk of mutation, which will cause yet another spike. Each variant has been a result of people letting their guard down to soon with their decision making.”
Dr. Neilanjan Nandi, MD, FACP, Associate Professor of Clinical Medicine, Gastroenterology, Penn Medicine, agrees that while case numbers going down is reassuring, that we are not out of the woods yet. To him, a mask is a sign of empathy for others.
“It’s not about us…whether it’s a caregiver or a family member or friend, this shouldn’t be looked at as an encroachment on our freedom, but rather about showing respect for those around us. The best thing we can do is mask up. Wearing a mask in public, indoor spaces is a smart move because you don’t know the immunization status or exposures of people you don’t know. If you are planning to see family or friends and know people’s vaccination status or if they’ve recently had Covid, you might feel more comfortable not wearing a mask.”
Pre-pandemic photo-May 2019 with Dr. Nandi at Digestive Disease Week in San Diego.
Dr. Nandi reiterated the fact that we’ve learned over the course of the last two years that most of our IBD medications don’t cause an increased risk and may even be protective. While this is reassuring, if you are on 20 mg of prednisone or higher, he highly recommends you mask up as you are more susceptible to illness.
Dr. Uma Mahadevan, MD, Professor of Medicine, and Director of the UCSF Colitis and Crohn’s Disease Center, says every region of the country is different and that your location should be taken into account.
“In the Bay Area we have a high vaccination rate and a low hospitalization rate. You also have to consider the patient’s personal risk and risk aversion.”
Here’s what Dr. Mahadevan tells her patients.
Follow local guidelines for masking
If you are vaccinated and boosted and are in a low-risk area with no mask mandate, its ok to not mask, particularly outdoors. Indoors in crowded shopping areas, etc., I would still consider masking. However, again, low risk patient in a low-risk region, it’s ok not to mask.
For high-risk patients on steroids, double biologics, severely active disease, etc. I still recommend masking.
Dr. Miguel Regueiro, MD, Chair, Digestive Disease and Surgery Institute, Chair, Department of Gastroenterology, Hepatology & Nutrition, Cleveland Clinic, is hopeful we’re headed to what we see with influenza. While of course flu can still be serious and deadly, with enough people vaccinated and exposed to Covid, we can have herd immunity.
“We’re all learning as we go and there’s a lot of “grey” with nothing very “black or white.” For now, I am recommending IBD patients continue to mask. For those who are immunocompromised, wear a mask in indoor spaces, especially crowded spaces such as airports. In outdoor spaces, it is less clear, but masks are probably a good idea when social distancing is not possible.”
Pre-pandemic photo-May 2019 with Dr. Regueiro at Digestive Disease Week in San Diego
Dr. Peter Higgins, MD, Ph.D., M.Sc., Director of the IBD Program at the University of Michigan, says if a person is unvaccinated, masks are a must. He encourages you to talk with your doctor about Evusheld, a monoclonal antibody against Covid-19 for immunocompromised people and those who cannot be vaccinated for medical reasons.
“If the county you live in is below 10 cases per 100,000 people (CDC is saying 200/100,000 for the non-immunosuppressed), then you can consider not wearing a mask. But admittedly, this is an arbitrary number and 200 cases for every 100,000 people seems too high for the immunocompromised population. Especially if you are around kids, the elderly, or those who have not been able to be vaccinated, showing solidarity and wearing a mask is highly recommended.”
He explained that eating indoors with good ventilation is OK, but that is it hard to prove unless you have a CO2 monitor that can show a consistent CO2 ppm (parts per million) < 650. To give you an idea, Las Vegas casinos have good ventilation systems in place to keep restaurants free of smoke and those measure between 400-450 ppm. Dr. Higgins still recommends people do a rapid test within 12 hours of gathering with friends and family. He adds that as we learn more about long Covid and new variants guidance may once again shift.
Dr. Harry J. Thomas, MD,Austin Gastroenterology in Texas, also recommends patient who are immunocompromised (especially those on anti-TNF’s, prednisone, and other immunosuppressants) to mask up.
“I empathize with people who are worried about being judged by others and I recommend that they share — if they feel comfortable — that they (or their family member) have a chronic disease that places them at higher risk. I do feel that abandoning masks right now is premature, especially here in Texas as well as in other parts of the country with lower vaccination rates. I’m not sure if/when there will be another spike, but we still have about 2,000 COVID deaths each day which is really tragic and indicates that the pandemic is far from over.
My personal take
Personally, my husband and I still wear masks in public, indoor spaces. Our children who are in preschool are one of the few who are still wearing masks at their school. While I understand each person has the right to make their own personal decision for themselves and for their families, it’s disheartening and honestly disappointing to see the lack of care for others who are not fortunate to have the luxury of being healthy. I can’t tell you when I’ll feel safe enough to go into a grocery store or the mall without a mask on, it’s going to take time and assurance from my care team that I’m not making a rash decision that could put myself, my family, or even strangers at risk. It’s complicated. I get it.
My daughter at preschool this week. Still masked up.
When you’ve lived with a chronic illness like Crohn’s disease for nearly 17 years and been on immunosuppressive drugs ever since, your perspective shifts. You quickly realize you are not invincible. You recognize and empathize with those who have health struggles and depend on the greater good to make sound decisions. It’s a small act of kindness for the sake of health and safety. Talk with your care team about navigating this new normal. Don’t base your judgements on social media, the news, or your political beliefs. This is an ever-evolving discussion. It’s been a long two years. We’re all tired. But that doesn’t mean apathy is the answer. You may not care, but you are making a statement to those who are vulnerable when you go maskless indoors.
It’s ok to be unsure. It’s normal not to want to be judged or feel your kids will be outcasts if they’re the only ones at school masking. It’s understandable to feel a bit lost about what is best. But if a mask makes you feel comfortable, safer, healthier, you do you. Know that the medical community and so many others stand in solidarity with you.
When Marquis Ellison met and began dating his wife, Tasheia, in 1999, they were juniors in high school. The couple tied the knot 13 years ago. One year into marriage, Marquis started to experience weight loss, fatigue, anemia, abdominal pain, stomach cramps, and loss of appetite. He dropped to 100 pounds! They were on an anniversary trip to Los Angeles when his symptoms started to become unbearable. After the trip, Marquis was diagnosed with Crohn’s disease. He was 26 years old.
“Upon being diagnosed, I felt a sigh of relief in knowing what the condition was and starting on the right medications. I owned it and decided to beat it by how I live, educate and inspire others.”
Tasheia has been by Marquis’ side every step of the way. Every colonoscopy. Every flare. Every doctor appointment. He thanks God every day for a wife who truly exemplifies what it means to be a partner in sickness and in health.
Focusing on faith and family
Marquis keeps busy as a husband, father, and personal trainer. He gives all the credit to God.
“Faith is the cornerstone of who I am and why I have the outlook I have with Crohn’s. If God wants to completely heal me, I know He can. But if not, I know He’ll give me the strength to endure and I’m at ease with that. There’s always a greater good for what we go through and if my journey living with Crohn’s disease can inspire and encourage others, all praise to the Most High!”
Since becoming a father three years ago, Marquis says his faith and his son are his “why” …why he’s so enthusiastic about doing all he can to take care of his body and controlling what he can.
“Being a dad is the greatest gift and blessing. Knowing this little person is your responsibility. I want my son to see that while I have IBD, I don’t let it stop me and set the example he can follow when faced with life’s unpredictability. My son witnessed me running the marathon cheering me on at mile 22 and the finish line. When we got back home, he wanted to wear my medal. I asked him if he wanted to run a marathon in which he replied, ‘yes’. That was a great feeling knowing I’ve inspired my son despite my condition.”
Shout out to IBD men
When you hear about people’s IBD journeys, it’s more common to hear from women, even though Crohn’s disease and ulcerative colitis impact genders equally. Marquis wants men to recognize they are not alone and to speak up and tell their stories.
“Your story matters. Your voice matters. Speaking about your health and opening up doesn’t make you any less of a man, it only enhances it.”
As a Black man, the lack of representation, and health disparities, span far and wide. Marquis wants you to know you are not alone in your struggles.
“Our voices matter. The more we advocate, the more we’ll show that Black and Brown communities are affected with IBD and should be represented more often. I’m proud to be an ambassador with Color of Crohn’s and Chronic Illness (COCCI), where we’re working to bridge the gap and lack of representation.”
Running for a reason
Marquis recently completed the New York City Marathon in November. He says it was the toughest and most victorious accomplishment he’s ever experienced. His race shirt read, “Mr. Crohn’s Fighter” to represent all IBD warriors and show that you can still do remarkable things, despite your disease. Life with IBD is a marathon, not a sprint. That mentality prepared Marquis for the race.
“Living with IBD is unpredictable. The unpredictability of a flare up or foods not agreeing with you always feels like something is looming. When running, you never know how the course or weather will be. You can train hills or in the rain, but you may still face adversity you didn’t prepare for. With running and with Crohn’s disease, it’s all about mindset and the ability to adapt and repeatedly overcome. Focus on your current reality and not on what hasn’t happened or what could happen.”
He’s currently training to run the New York City Half March 20th, 2022.
Focusing on what you can control
Marquis manages his IBD through fitness, nutrition, mindset, and by taking Cimzia, a monthly self-injection. He’s all about controlling what you can and not succumbing to your circumstances.
“Life is 20% of what happens to you and 80% of how you respond to it. I choose to focus on the 80% by controlling what I can. I always say, I have Crohn’s disease, it doesn’t have me. IBD may try and take me down, but it will never knock me out.”