Kids are more intuitive than we tend to give them credit for. They are always watching us and even before they’re able to speak in sentences they have an innate sense of empathy and understanding. As an IBD mom of three, whose kids are almost 7, 5, and 2.5, I’ve started to think more lately about how to explain my Crohn’s disease to them in a way that will educate them, without scaring them. It can be a difficult balance.
I know my older two know mama gives herself shots, often needs to run to the bathroom, and gets “tummy aches” but I haven’t yet dropped the term “Crohn’s” or “disease” to them quite yet. It can be hard to explain and sometimes when I start trying to share more, I feel like it’s still going over their heads. Their concerned eyes when I’m in pain and how they watch me do my Humira injections is a reminder to me that they are aware something is going on. As we potty train my youngest, he commends himself for going on the potty by saying he’s “just like mama” …ah, what a great analogy!
This week on Lights, Camera, Crohn’s hear from several IBD parents about how they transparently communicate their experiences with Crohn’s disease and ulcerative colitis. It can be a fine line educating and being open, while also trying not to overwhelm and scare kids. I’ve found it extremely helpful tapping into the community and gaining input from others and I hope you do, too!
Helpful Guidelines for Navigating the conversation with your kids
Choose the right time. Pick a time when you won’t be interrupted and can focus on the conversation. Ensure it’s a moment when you and your children are feeling calm, at ease, and open to discussion. My recommendation as an IBD mom would be to have this conversation on a “feel good” day—rather than when you’re flaring or in the hospital.
Prepare yourself. Decide in advance how much detail you want to share based on your child’s age and maturity level. IBD is complicated, be ready for a range of emotions including sadness, fear, and even anger.
Use age-appropriate language. Explain your IBD in a way that is understandable to your child. Avoid using confusing or technical terms. For younger kids, it might be helpful to compare your illness to something they already understand.
Be honest but reassuring. You can be transparent and truthful, but also reassure them about all you do to manage and control your IBD. Empathize with the aspects of your daily life that won’t change, to provide them with a sense of stability and comfort.
Focus on practical impacts. Explain how your IBD might affect your daily routine or activities with them in a straightforward way. Use examples such as—“Mommy’s Crohn’s can be unpredictable, I may say we’re going to the park, but then I don’t feel well so we have a movie date and snuggle instead and plan to go to the park another day.”
Encourage questions. Allow your children to ask questions and express their feelings and know this will be an ongoing conversation throughout life. Go into the conversation without expectations. It’s ok to admit if you don’t have all the answers. You can explore some of the questions together.
Provide continuous support. Let your kids know that it’s okay to have and express their feelings about your IBD. Offer them ongoing support and reassurance. Let them know they can always come to you with questions or concerns at any time.
Seek support when needed. Consider enlisting the help of a therapist or a counselor, especially if you or your children are struggling to cope. Joining support groups and tapping into the online patient community and connecting with fellow IBD families in similar situations can be beneficial.
Keep the conversation going. Check in with your children regularly about your IBD and how you’re feeling. Be casual about it. Share when you see an opportunity to teach or calm fears that your kids may be internalizing.
Highlight the positives. While acknowledging the challenges, also focus on the positive aspects, such as the strength of your family unit or the support you have from friends and community. I always tell my kids when I’m doing my injection that mommy is strong, and we can all do hard things.
By approaching the conversation with honesty, sensitivity, and openness, you can help your children understand and cope with your chronic illness in a healthy way.
My 2-year-old trying to make me smile during a rough day in the bathroom.
IBD as a family disease
There’s a common saying in our community that IBD is a family disease, in that whether you have Crohn’s or ulcerative colitis or not, if someone in your nuclear family has it, the disease impacts your living experience in some way.
Emily and her husband have IBD and so do their three daughters, so discussions about IBD are frequent in their home since it’s a living reality for all five of them. She tells me the conversations tend to fall in one of the following categories:
1) Explanations of IBD details, procedures, surgeries, or diet needs for a member (or members) of the family.
2) Discussions to calm anxieties in one child about the presentation of IBD in themselves or in another family member.
She says the second category tends to be the more challenging conversations, by far.
“In the first category, we tend to stick to factual, age-appropriate explanations. For example, when our five-year-old needed to know about scopes and surgeries, we explained that a specific family member has “belly problems” and the doctor is helping by taking pictures of their belly and fixing the parts that were causing trouble,” explained Emily.
As the girls have gotten older, Emily says they add details about how the doctors do different procedures – always led by their child’s level of interest and desire for the knowledge.
“We are always honest about pain or discomfort related to medical procedures. Many things are NOT painful, and we want them to trust us that something does not hurt if we tell them. This has served us well. When surgery was needed for one daughter, we discussed how she would be sore afterwards, but we had ways to help the pain until it would subside. This was undoubtedly a challenging time for us, but our daughter did amazing,” Emily said.
As Emily’s girls have gotten older, as a preteen and teen, they understand more about their parents,’ and their own, IBD. They have lived through surgeries and many medical procedures in their family. Emily says now the more challenging conversations have started, related to knowing the possibilities around IBD.
“For example, I had a colon perforation following a routine monitoring scope for my IBD. It was a rare event that we are all warned about prior to a colonoscopy. It resulted in a more significant repair surgery and several days in the hospital. My daughters are old enough to realize that they also have scopes regularly and we had to have some discussions about the chance that the same thing could happen to them. It was challenging for our family for a few rounds of scopes!”
Emily says they addressed this topic mostly by focusing on the “helpers” as the iconic Mr. Rogers would! Yes, bad things can happen, but she reminded her daughters that they are so lucky to have doctors and medical professionals to “fix” these problems. She reminds them that they are lucky to have family and friends to help when they are not feeling well. She also talks about how they are lucky to have each other – who understand the ups and downs of this disease.
“This narrative has gotten our family through many challenges! I talk with my oldest daughter much more now about the details of her IBD. She is a teen and has had more than her fair share of IBD troubles. She has watched me deal with my challenges too. We are open with each other about the negative parts, and our frustrations having to deal with IBD. It is a double-edged sword to have her growing up! On the one hand – I hate that she is old enough to really understand the negatives. But she is also turning into an amazing young woman who is one of my closest confidants with this disease. We understand each other’s highs and lows like most cannot. We supported each other in challenging times and celebrate together for each win!”
Sari says she bought a couple of children’s books that feature a caregiver with chronic illness.
“One of them is titled ‘Some days’…it’s about a mom with multiple sclerosis, but it works for IBD, too. It goes over how some days are more exciting and others are simpler more restful days. If there are other kids’ books people have found, I’d love to hear about them!”
Kate also has a book by someone with Crohn’s, but says they’ve also always been very honest and open about it with her son.
“I always worried he would tell people too much, but I’ve found he’s incredibly respectful and it has made me feel less shame in my body because I talk to him so positively about it. Especially the perianal disease, which has been really hard to talk about with people. My son is six and understands my immune system attacks my digestive tract. We also have a puzzle of the body we have played with for years and he knows the colon, intestines, rectum, etc. because of that.”
Becca says one of her favorite memories as an IBD mom is when her daughter was learning body parts and said, “Mommy and I have vulvas, Daddy has a penis, Daddy and I have butts, and mommy has a bag!” She also often asks to see her “cut” on my belly (c-section scar), but I constantly remind her that she shares her “cut” with a lot of intestine.”
Becca also says for the longest time her daughter thought that EVERY mom gets an ostomy bag when they’ve had a baby.
“She didn’t realize I had mine for four years before she was born!”
As an IBD Dad, Brandon said he stumbled upon a video series when his son was around age five that provided a solid explanation. At the time his son had a broken arm.
“The video explained people have booboos you can’t see. I explained that I had what the girl in the video has. Nowadays, I show both my boys’ photos from my colonoscopies.”
You can watch the video Brandon showed his son here.
Here are additional books about chronic illness that others have recommended:
When you’re diagnosed with Crohn’s disease or ulcerative colitis it’s a lot to process. When I started this blog in 2016 and after living with Crohn’s for nearly 19 years, my focus has always been to be the voice I needed to hear upon diagnosis and what it was like to experience young adulthood with a chronic illness. As a 21-year-old, fresh out of college, I had to navigate my career, finding love, and becoming a mom with IBD on my own. The first decade I wasn’t publicly sharing my story and didn’t know there was a patient community to tap into online for support.
The first week I started experiencing Crohn’s symptoms-March 2005, Senior Spring Break in the Bahamas
Often as the years go by and we get beyond the initial shock of hearing the news and what this means for our lives, we tend to forget the challenges we faced to gain our footing. This week on Lights, Camera, Crohn’s I share some tokens of knowledge I’ve gained along the way that I hope will help you on your own journey, no matter where you find yourself at this moment.
Healing—physically, mentally, and emotionally is not linear. We all experience IBD uniquely—some people’s disease course is milder, others have it severe. We all cope differently with knowing and living with a chronic illness. Give yourself grace in the difficult moments. It’s ok to feel resentment or anger. It’s understandable to wonder at times “why me.” It’s “normal” to feel scared and anxious whether you’re a few weeks or a few decades in. Sometimes it’s taking things one hour at a time, other times it’s taking them one day at a time. Because of how quickly a flare up can strike, I try to live in the now and not worry about tomorrow.
You didn’t have control of getting your chronic illness, but you can control how you react and choose to heal from it. It’s easy to feel like you may be to blame if your health takes a turn for the worse. But understand this is not your fault. The unpredictability of IBD makes it feel like we’re often in the passenger seat and spiraling in circles, but this disease cannot control how you react, respond, and choose to heal from it. No matter what, you’re in control of the healing process. Whether it’s finding support through fellow patients and caregivers or through professional therapy, you won’t look back and you’ll be setting yourself up to take this on to the best of your ability.
There is no comparison game. Since the majority of people are diagnosed with IBD in their teens and into their 30s, it can be easy to try and measure your timeline and accomplishments to that of your peers who do not have chronic illness. It can also be tempting to look at people in the patient community who seem to have the world by the tail, when you’re struggling to get out of bed each day. This isn’t a competition of the sickest or a ploy to see who can smile through the pain and get more done. The only person you need to answer to, is who you see looking back in the mirror. You determine what you’re capable of and what you want in life. Your roadmap is yours and you’re right where you’re meant to be.
You set the benchmark for what’s possible. Your IBD is part of you, but it’s not your entire identity. Remember that even patient advocates are posting somewhat of a highlight reel. Even those who are working, in love, and parenting are dealing with their own struggles, too. My best advice would be to think about what you hope for in life (don’t even think of your IBD as part of the equation) and go after it. Yes, your health may cause some detours and roadblocks, but you won’t find your way unless you try.
No one knows your body better than you. I don’t care how many letters someone has after their name, they aren’t living in your body and experiencing what you feel each moment of every day. Be vocal when you need to be. Communicate as much as you can with your care team and paint the clearest picture of your reality. If you keep parts of your struggles to yourself or dumb down the severity of your day-to-day life, the only person you’re hurting is yourself. Learn about nutritional bloodwork and advocate for yourself to be tested for a full iron panel with Ferritin and Vitamin D. Get labs every 3-4 months so you can keep a finger on the pulse of what’s going on with your body. If you feel like your provider is being lackadaisical, don’t hesitate to get a second opinion. Take ownership of your health and find a provider who in your darkest moments you would feel most comfortable by your bedside in the hospital.
Make sure your GI specializes in IBD. There are gastroenterologists and there are gastroenterologists who specialize in Crohn’s and ulcerative colitis. Once you’re diagnosed with IBD, it’s imperative you try to find a GI who is an IBDologist. This can be tricky if you live in a rural area, it may mean you need to travel several hours to find a provider who fits the bill. If you move or are unsure of a good GI to check out, it’s helpful to reach out to your local Crohn’s and Colitis Foundation chapter and often they can help point you in the right direction.
Diet and stress levels matter. Read that again. Any doctor who tells you diet, and stress doesn’t impact your disease process is wrong. There are incredible registered dietitians throughout the US who specialize in IBD, and many of them have IBD themselves! Before you start restricting yourself or your child, make an appointment—most provide virtual options and this will help you get educated on what works best for you. What is a trigger for one person, isn’t necessarily a trigger for another. There isn’t a one-size-fits-all diet or else we would all do it.
Emotions will strike when you least expect them. Even almost 19 years in, I’ll sometimes break down and cry when I think about my Crohn’s or how it makes me feel. Just because you become a veteran patient doesn’t necessarily mean you fully ever heal from the hurt life with a chronic illness causes. It’s ok to have these moments where you may feel like you’re allowing your disease to control your emotions, you’re not. You’re human. It’s healthy to feel frustrated and to get emotional about what your life is like because you have IBD.
You’ve endured more than you give yourself credit for. As chronic illness patients we go through so much that often we don’t even bat an eye over experiences that would be extremely painful or stressful to the average person. Think about what a bad ass you are and how that carries over into each and everything you do in life. If you’re newly diagnosed you will get there—but even those initial weeks and months, you’re enduring more than the people who have their IBD under control and have a good handle on their body. No matter how many surgeries, scopes, scans, and IVs I’ve had, I always get a little teary eyed because it brings me back to 21-year-old me and then all the trauma that comes along with living with Crohn’s for 19 years. While those tears are sad, they also come from the strength of reflecting on what I’ve gone through to bring me to now.
Stay in tune with how your body is speaking to you through symptoms, do not ignore them. It can be challenging to communicate what you’re feeling to someone who does not have IBD. I get that. But by protecting loved ones, friends, and doctors from what you’re experiencing you’re preventing them from stepping in before it’s too late and before you know it your flare has gotten out of control and requires hospitalization. I used to be that person all the time. I would always internalize the pain, silently fighting through each day, doing anything possible to stay out of the hospital until the symptoms were simply unavoidable and required medical intervention. One hospitalization always sticks out in my mind. It was May 2009. I was a 25-year-old morning news anchor in Wisconsin. I was solo producing a 2-hour morning show dealing with horrible abdominal pain that kept making me throw up in the garbage can next to my desk in the newsroom as I struggled to put together the show. Finally, I couldn’t take it anymore and I had to call my co-anchor, who rushed me to the hospital. I was released from the ER hours later after my parents had driven from Chicago in the middle of the night only to return to the hospital that afternoon and have my dad carry me in his arms through the automatic doors. I was finally admitted and given the medical intervention I needed. Take it from me, you’re creating even more of an uphill climb for yourself if you don’t start speaking up when you initially notice something is awry.
The worst moments are just that, moments. When you hit your breaking point, when the pain seems overwhelming, and you can’t see the forest through the trees try to breathe. Go to your happy place. Recognize this is one day, one moment, I always tell myself “This too shall pass.” Go to your happy place mentally. Do mindfulness exercises. Shut out the outside world and focus on your breath. Detach from your body as best you can. Think of people who inspire you and bring you joy. Everything is fleeting. Each flare, each recovery, each prep, procedure, and surgery…it has a start and a finish. One day it will be a memory you talk about.
Pay attention to who is there when you when are quiet and when you’re going through the thick of it. IBD is too big to deal with alone. Lean on people you can trust, who you genuinely feel safe sharing your health woes with. This will be fewer people than you’d ever imagine. Be prepared to realize that many of the people you thought would be front and center to support you will be non-existent. It’s fine to mourn those friendships or relationships, but don’t waste your time or energy on them. Your disease will give you the ability to see who loves you and who wants to be present in not only the good times, but the bad. You can’t change people. Hold on tightly to the people who show up consistently, expecting nothing in return. Those are your people.
Emmanuel Acho shared a reel on Instagram recently that really hit home for me and caused me to reflect a bit on the people in my life and their roles. In the video he explains that friendship is like a house. You have your window, door, and floor friends. Window friends are outside looking in, they don’t know what’s going on in your house. They don’t have intimate access to what’s going on in your life. You can only let so many people into your house. Door friends come in and out of your life depending on the season. When life gets too hard or when your world turns cold, they might exit. Your friends might not be equipped for that season. Floor friends—aren’t going anywhere. You might track mud, but they will last regardless of the season. They are there to catch your tears and hear your fears. Remember—a house has more windows than it has doors and more doors than it does floors…if it has one good floor, you’re set.
Just because you need medication does not mean you’re taking the easy way out. I’ve been where you are. I remember lying helpless in a hospital bed and what it felt like to be told I needed to “break out the big guns” and start a biologic medication back in 2008 when there were only two options on the market for those with IBD. In that moment, we all naturally want to learn about side effects and what this could possibly mean for the long term. But please try and focus on the actual risk versus the benefit. As someone who has been on Humira since July 2008, I’m so grateful for my medication for allowing me to live a full life, bring babies into this world, and be a present, able-bodied, and active mom. It’s not all medicine, or all diet and lifestyle, often for many of us who have moderate to severe IBD we need a mix of both, and that’s ok. You can still thrive and be healthy, despite being on a medication with a black box label.
You are not a burden, and you deserve love. Any romantic partner who makes you feel less than, isn’t present when you need them most, or doesn’t show any empathy or interest in your daily reality isn’t going to stand the test of time. Use your IBD to your advantage to see your partner’s true colors. Be honest and upfront when you start dating and if you ever feel like you need to defend their actions or make excuses consider that a major red flag. Dating and marrying a person with a chronic illness isn’t for everyone, and that’s fine—but when it comes to people like you and me, we need a partner who is willing to take the challenge on beside us every step of the way. Find someone who you feel comfortable communicating openly with, who sees you for more than your disease.
IBD is not a battle to be “won” or “lost.” One of my pet peeves with any health condition or disease is when people say “so and so lost their battle”…they didn’t lose shit. Diseases are not a game. Oftentimes reaching remission is due to luck, disease severity, or surgery. I spent a decade of my life with active disease and have been in remission (thanks to surgery) for almost nine years. I don’t give myself credit for that, I’m not “winning.” It’s because of my efforts to stay diligent with my biologic, vitamins, safety labs, daily decisions, and check-ins with multiple specialists, but I also don’t think I’m at this point because of something special I’m doing compared to someone else. We’re all dealt a different hand of cards in life. Your IBD isn’t a win or lose situation—you’ll celebrate big victories and small ones, too, your disease can rob you at times, it’s a never-ending exchange and game of back and forth. You are not less than because you are flaring. You are not lazy for taking medication or failing because you struggle to follow a strict, regimented diet that may or may not help you. Once you stop thinking of everything as a “fight” it takes a bit of the stress, anger, and onus off your shoulders. IBD is a chronic illness, until there’s a cure, we’re in this situation until the day we die…that’s simply too long to be “fighting” anything.
Get ready to be extra proactive with your health. Due to the nature of our IBD and the medications many of us take, we are at greater risk for additional health problems. It’s important to get annual skin checks at the dermatologist. Make sure whether you have good vision or not that you’re seeing an eye doctor. Get cleanings at the dentist at least every six months. If you’re a female, make sure you get your well woman visits. We are greater risk for cervical cancer because many biologics don’t allow our bodies to fight off HPV, this may mean annual Pap smears. We’re also at an increased risk for breast cancer, so don’t delay your mammogram. Get a bone scan every 3-4 years, get one as close to diagnosis as you can so you have a baseline. Your GI may say it’s not necessary, it is. Steroids put us at risk for osteopenia and osteoporosis from an early age, this may mean you need to see a bone health doctor (yes, those exist). Those of us with IBD are at greater risk for pelvic pain, it can be helpful to see a Pelvic Floor Therapist who addresses those unique needs.
Faith can give you added strength and comfort. I understand faith is very individualized and looks different for each of us, but I can tell you as someone who is Greek Orthodox who has always been a faithful and prayerful person that I rely on my faith to guide me through my IBD each and every day. There’s a sense of comfort and hope that comes with believing God is watching over you through the good, the bad, and everywhere in between. When you’re diagnosed or flaring, it can test your faith. Hold on tightly to what you believe and lean on that (however it looks for you). I truly believe God gives his toughest lessons to his greatest teachers. One of my biggest fears as an IBD mom of 3 is that one of my children will get my disease one day. Each night before bed, I always pray with them and say, “keep my babies healthy, safe, and strong.”
My why. My motivation to push through each and every day.
Family planning takes time and effort. Just because you have IBD does not mean you can’t be a biological mom or dad one day. The journey will look a bit different, but this disease does not necessarily need to rob you of the experience if that’s what you want in your life. Communicate these desires with your GI so they can help prep your body for a baby. This can mean starting a prenatal vitamin and folic acid several months before trying. I had a colonoscopy before every pregnancy so that I could be given the ‘green light’ by my GI that we were cleared to try for a baby. When I was pregnant, my care was overseen by my OB, a maternal fetal medicine OB (high risk), and my GI. Unless you have perianal disease, you can have a vaginal birth, but oftentimes this is a discussion left to you and your care team. I personally chose to have 3 scheduled c-sections, because while I don’t have perianal Crohn’s, I didn’t want to risk tearing or causing a fistula to form. I would make the same choice if I had to do it all over again. I also stayed on my biologic through conception, pregnancy, and breastfeeding. These are all personal choices but there are many, many research studies available that show the safety and efficacy of doing so. If you feel you could have internal scarring due to past surgeries that could hinder your fertility, check in with a fertility specialist and have them help you investigate if there could be issues.
Educate yourself on insurance, prior authorizations, specialty pharmacies, and Pharmacy Benefit Managers (PBMS). Unfortunately, with IBD we are forced to do so much behind-the-scenes work to simply receive treatment and medication. You will waste countless hours and endless energy on the phone as these people give you the run around. Nobody ever seems to want to take ownership. Work with your gastroenterologist if you are denied a medication so they can write an appeal letter to insurance and go to bat for you. Stay on top of everything, don’t worry about annoying anybody. You gotta hustle. You gotta be frank and assertive. It’s not about hurting feelings; it’s about making sure people are doing their jobs and ensuring your course of treatment doesn’t get delayed because someone fumbles some paperwork. Our medications are time sensitive. Light a fire under people’s ass if you’re not getting responses you deserve. One of my friends on social media posted this over the weekend, “Managing specialty medications in January is an annual slap in the face to chronically ill people.” It sure is. This week will mark the first time I’ve ever received my injections late in the mail, due to a misstep in my GI office that I had to follow up on for over a week. Be extra proactive at the start of each year. Make sure your GI informs you about all the patient savings programs available, these can help you not only emotionally, but also financially.
You get the final say. No one but you gets to say what you do with your body. If a doctor wants you to do an enema before a scope and you don’t want to, don’t. If you don’t feel comfortable with taking a certain medication and your care provider keeps pushing it, they can’t physically make you pop a pill, take an injection, or receive an infusion. You must do your research, educate yourself every day, feel empowered by all you know and be ready to deal with the ramifications if you go against the grain or determine you want to try something differently. There’s not one “right” way to live with IBD. Be honest with your provider. Don’t say you’re taking a medication and then not take it, that’s not helping anyone or anything. Be a compliant patient, but an educated and empowered one at the same time. Measure all the risks and benefits and what your hopes and dreams are for your present life and for your future. Don’t ever feel like someone else can or should dictate what path your journey takes. Just because one biologic is a magic bullet for one person doesn’t mean it will be for you. You never fail treatments, they fail you. If a provider says “oh, you failed Remicade” … please correct them. “No, Remicade failed me.”
I write this as a 40-year-old mom of three—ages 6, 5, and 2.5 years old, married for almost 8 years, who has been on a biologic since 2008, who was diagnosed at age 21 in 2005. So much has changed for the better regarding the patient experience since that time. My perspective has come a long way. I used to be right where you are, so many are living your current reality. Instagram is the bread and butter for the patient community, that’s where you’ll find the most patients and caregivers transparently sharing. Follow the accounts, send a DM, comment on reels and posts, get engaged. Never hestitate to connect and reach out to me–natalieannhayden. Educate yourself through lived experiences and people who have paved the way for you, rather than Google. You don’t need to recreate the wheel, but this is your experience and your story. You get the final word on how you want each chapter to play out. Know each time you fall you will bounce back and that there’s a massive community of support here to catch you and cheer you on every step of the way as you rise once again.
When you have IBD and need a biologic, it used to be all infusions or self-injections. But starting in March 2022 (for ulcerative colitis) and May 2023 (for Crohn’s) a daily pill known as Rinvoq (Upadacitinib), entered the game. Rinvoq is the first approved oral product to treat Crohn’s. This once-daily pill is prescribed for those with moderately to severely active IBD who have had a lackluster response or an intolerance to one more TNF blockers (such as Humira and/or Remicade). Rinvoq is also prescribed for rheumatology and dermatology conditions, such as rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, non-radiographic axial spondylarthritis.
Doses range from 15 mg, 30 mg, or 45 mg. According to AbbVie’s website, “Rinvoq is a selective JAK inhibitor based on enzymatic and cellular assays. Rinvoq works with your body to fight the inflammation that can lead to IBD symptoms. Rinvoq stops the activity of some inflammatory proteins known as Janus kinase (JAK) to help reduce inflammation.
This week on Lights, Camera, Crohn’s we talk with 29 IBD patients about their personal experience on Rinvoq, along with Dr. Uma Mahadevan about key information for those in the family planning stages of their lives.
What patients have to say about the induction dose and the quick improvement in symptoms
Rinvoq is the first JAK inhibitor medication that Brooke tried and she didn’t know what to expect. She started Rinvoq in July and says her body has done a complete 180.
“All of my immediate issues have healed, and my long-standing symptoms have begun to fade. In the beginning during the loading dose, I felt a bit more tired. But after two weeks, I had more energy and have experienced less symptoms. Most of my extraintestinal manifestations have cleared up.”
Brooke says she has caught two colds since being on it, so she’s still masking and being diligent around crowded spaces, especially during flu season. She advises fellow patients to talk to their physicians about the dosage they need.
“Because of how much I’ve been flaring, I’m on a higher dose longer than I may have been if I started in a healthier place. Make sure you and your care team agree on a dosage that is not only good for you, but also that you agree with.”
Brooke sets alarms to take her meds because she is used to an infusion or subcutaneous injection, and it’s important not to miss a dose of Rinvoq.
Tonya: I’m only two weeks in, so still on the induction dose, but this is the first time my symptoms have been somewhat controlled in four years.”
Sarah: “I just started Rinvoq and it’s helping me come out of a flare up.”
Melissa: “My 17-year-old son has been on Rinvoq for about six months after Xeljanz failed him. He’s doing great on it and it’s super easy since it’s a pill once a day. He has also been on Humira and Entyvio in the past. Rinvoq has been the easiest transition so far.
Jennifer L.: “I went on Rinvoq after Remicade failed me and then went on Cyclosporine to bridge the gap before I could switch to Rinvoq. I started it in December of last year and this has been the one drug that has subsided a lot of the symptoms. No nocturnal bowel movements, the only major side effects I’ve had is some acne, but I would say it’s hardly noticeable. I did have to come off hormonal birth control as a side effect can also be blood clots, so you can’t have two drugs that increase your risk of that together. I’m single and wasn’t really thinking about dating coming out of a huge flare, so it was a no brainer for me there. If you’re looking to get pregnant, I’ve heard you can’t be on it because studies have shown birth defects, so that’s a concern potentially for some women or for contraceptive options given that you’re only limited to non-hormonal options while on this.”
Krista: “My fiancé just started Rinvoq and after one day he was feeling better. His energy is up, he has an appetite again, and is showing significantly less signs of inflammation. We still have a journey, but it’s been a miracle drug for him.”
Lizzie: “I have been on this now for 3 months after Humira and Stelara stopped working. So far, my Crohn’s symptoms have subsided. I’m no longer flaring. I would say since taking Rinvoq, I feel more fatigued, but apart from that, I feel really good.”
Marla: “I started Rinvoq 24 days ago, so I don’t have a lot to tell you. I don’t think it’s anything bad. It’s hard to tell if the medication is working yet. I do blood work in November.”
Lauren: “I’ve been on Rinvoq for about one year now. Didn’t work at first, but found out I simultaneously had C-diff. I was on vancomycin and Rinvoq for about 4 months and was scoped for the first time in 4 years because I was in remission. I ended vancomycin and flared again. I will be transitioning to Skyrizi soon, but even though I’m not in remission, Rinvoq has been the only thing that has gotten me in the best place I’ve been in 4 years. I love the ease of one pill a day, no infusions, no shots, etc.”
The main reason Lauren can’t stay on Rinvoq is that it’s not safe for pregnancy and she hopes to have another child. She’s bummed this medication is the only thing that’s shown her improvements and that she needs to switch.
Amber: “I just started Rinvoq last week, so perhaps it’s too early. I am adding Rinvoq to Entyvio for fistulizing Crohn’s. The one thing we are trying to figure out is how it works with an ileostomy. I tend to have a fast track and has passed pills in the past and Rinvoq is an extended release.”
Dana: “I’m currently on Rinvoq! Although I’ve only been on it for 3 weeks, I don’t have any real side effects so far.”
Lindsay: “I’ve only been on Rinvoq for about 3 weeks. I was hoping for a more dramatic change based on things I have read. My fevers have gone away, and I feel like I have more energy, but I still go to the bathroom just as much and the urgency has not changed. I also had to give up breastfeeding to start Rinvoq, so that was hard!”
Sarah: “I started Rinvoq after Humira was not putting me in remission after 1.5 years on it (even with methotrexate added to help). I saw an immediate improvement in my stools. I might have a few pimples as a side effect. It’s only been 3 weeks, but so far, so good!”
Erica: “I’ve been on Rinvoq since May. I haven’t had any improvement. I was hoping when I started that it would work for me. I heard so many people call it their miracle drug. I was scared to try it at first because of all the warnings, but once I started it, I was hopeful. Unfortunately, it was not my miracle drug and I had to add Skyrizi to it…I’m still not better.”
Denise: “I’ve been on Rinvoq for about 7 years. I’ve been part of a clinical trial. I don’t think I have anything bad to say about it. I was so sick with few options, so I took a risk, and it fixed me. I don’t think I’ve had any side effects. I still get scoped annually as part of the study and my intestines have looked great. Sure, I still have tummy troubles, but not the main Crohn’s ones! I get blood work done every 3 months and everything has been normal there as well.”
Abigail was prescribed Rinvoq in late August 2022. At the time, she was hospitalized with the worst flare she’s ever had and was admitted 3 separate times for a 37 day stay. She was facing steroid and Remicade failure and running out of time before requiring emergency surgery. Abigail was given the option of trying Rinvoq for 2 weeks. If it didn’t work, surgery would be required to remove her colon. Her care team got insurance to approve it and she started it right away. Abigail took a double loading dose. Usually, you do 45 mg for 8 weeks, but she did it for 16 weeks instead.
“This medication not only saved my colon, but arguably my life, as I had faced death twice during that hospitalization. I was able to get off steroids. I now take 30 mg of Rinvoq daily and I’m in clinical remission. My next colonoscopy is at the end of this month, so it may show even further remission. I was nervous to start Rinvoq, since it is so new, but given the circumstances, I agreed to it. I am honestly so glad I did. The only side effect I have experienced is high cholesterol. My care team will be addressing this after my colonoscopy. I am forever grateful to Rinvoq for giving me my life back. I choose to do medication and therapeutic diet (SCD). For me, this combination has really helped.”
The visible side effects
Jessie started on Rinvoq to treat her Crohn’s before it was FDA approved because of a flare she couldn’t get under control. She was put on the 45 mg dose for 2 months and saw quick improvements in how she was feeling. After years and years of being poked and prodded for infusions and labs she says she’s so grateful to give her body a rest and just take a daily pill.
“Rinvoq has been like a miracle drug for me. Despite the side effects of weight gain, constipation, and acne on my face and body, I don’t even care because it’s the best I’ve felt in more than 5 years. I’ll take the acne and backne any day.”
Jessie spent hundreds of dollars on skin products and through patient support groups she was recommended CeraVe Moisturizing Cream with Salicylic Acid and CeraVe Body Wash with Salicylic Acid and has noticed a huge improvement. Both products are available over the counter.
Madison: “I am on Rinvoq and I hate it. Let’s say first, it works fast. Within 48 hours, my symptoms were gone, and it’s done a great job at keeping my UC in check. However, the side effects are awful. Acne is the most common side effect and I have it everywhere. My face used to be dry, but now it’s VERY oily. My cholesterol has gone up, which is a known side effect and doctors are keeping close tabs on it. Lastly, weight gain. Weight gain was recently acknowledged as a side effect and I’ve had that, too. The first-generation JAK inhibitors were notorious for weight gain, so I’m not sure why it wasn’t acknowledged in this second generation.”
Madison adds that it’s hard to acknowledge that Rinvoq is working well, but it comes with its fair share of side effects. While the side effects are annoying, she says they are not as bad as a flare.
Alexandra: “I took Rinvoq for 5 months. It did absolutely nothing for my UC, but it gave me horrible acne.”
Lisa: “I was on 45 mg for 3 months. I hated it. I had some sort of infection the entire time and had bruises everywhere. I started Skyrizi three days ago.”
Elizabeth: “I’ve had great results on Rinvoq, I take 30 mg along with Entyvio. My only complaint with Rinvoq is the acne.”
Jenna: “I just stopped Rinvoq. I had a horrible face rash as a side effect. It seemed like an acne flare when it started back in early August and no matter what I tried, it got worse and worse. My dermatologist and doctors both believed it was some sort of rash caused by being on immunosuppressant drugs and stopped my Rinvoq. I took an anti-parasitic and the acne is mostly cleared up.”
Kelly: “I started Rinvoq and only completed 6 weeks (the loading dose and start of the treatment). Insurance issues were part of the reason why I stopped taking it. I also knew that I wanted another child. If I was able to…and there were minimal to no studies for a safe pregnancy. The only symptoms I had were small rashes on my hands and feet, kind of pimple like, not painful or concerning…just something I noticed.”
Jennifer V.: “On Rinvoq and love it!! It’s a pill so it’s easy and it has put me mostly into a therapeutic remission. The cons: weight gain, fatigue, elevated liver enzymes, and anemia. All in all, if you are not having any more children, I would highly recommend this medication. I would need to see more time and research if I were to recommend it prior to pregnancy.”
Jennifer V. had to go off Rinvoq last week while she was taking Paxlovid to clear up Covid and she lost weight for the first time in ages. Now she says she’s back on Rinvoq and the weight is coming right back.
Emily: “I have had Crohn’s and lupus since 2020 and I took the highest dosage of Rinvoq, and it didn’t do much to help me. While I was on it, I thought I saw some improvements, but as soon as I went off it, I realized it wasn’t doing much good. It made my skin break out really bad. I often would pass the pill whole when going to the bathroom. It’s a big pill, easy to see. I’m on Skyrizi now and hoping to reach remission.”
Kendall: “I’ve been on Rinvoq about 3 months. My symptoms have improved, but I’m surprised at how many of the side effects I have experienced: styes, mouth sores, cold sores, and acne. I’m planning to stay on it. My IBD is not stable yet, but I’m hopeful Rinvoq will get me there. Afterwards, I’ll see if diet and lifestyle can maintain remission. It’s nice that you can start and stop Rinvoq!”
Implications for pregnancy and breastfeeding to consider
Sarah: “I just started Rinvoq and it’s helping me come out of a flare up. I am wrapping up my third month. I started to feel improvement after two weeks. It’s such a relief to take a pill after self-injecting for the past 15 years. So far, I don’t have any bad side effects. The only thing that stresses me out is that you can’t be pregnant while taking it, so as a 34-year-old, ready to have a second child, it’s in the back of my mind—how am I going to get off (and back on this), how will I keep my Crohn’s under control when I’m pregnant next? But, in the meantime, I’m grateful that it’s helped me get control over a bad flare that caused me to take a medical leave from my job.”
Allie: “I feel like I had a good experience on Rinvoq. I would say the good is that it works very fast. I was starting to feel better from my flare within 3 days. I was able to get off prednisone because it worked so quickly. The bad is that Rinvoq made me gain weight that I haven’t been able to lose, but my doctors won’t confirm it’s related to the medication. I also felt very bloated all the time. I did not like having to take a pill every day (going from being on Entyvio), so I would sometimes forget to take it. The last thing for me is that I’m still hoping to have another child and it’s not safe for pregnancy, so it was not a long-term option for me, even though it helped me achieve healing from a flare.”
Carmen started taking Rinvoq in February after multiple biologics and non-biologics failed to treat and manage her ulcerative colitis. So far, she says her experience has been very positive. She went into clinical remission within the first month of being prescribed 45 mg.
“I’ve since been tapered down to 15 mg and it’s still looking very positive. Bloods, calprotectin, and how I generally feel has massively improved, along with my quality of life. The negatives I’ve experienced so far have been some mild skin issues, mainly rashes on my face, chest, and upper back, this is currently controlled by over-the-counter salicylic acid face and body wash. I’ve also picked up a few fungal infections and have lost my big toenail because of one of the infections that required antibiotics. For me, these are minor issues and outweigh the overall treatment plan. My GI believes as we’ve decreased the dose to 15 mg, that these minor side effects will disperse over time.”
Carmen says taking a once daily pill is much simpler than some of the other biologic drugs that require visiting an infusion center and taking multiple other medications either intravenously or orally. The cost for me is relatively high for Rinvoq at $150 a month, but this will depend on what medical insurance and copay you have. All in all, Carmen says Rinvoq has been a positive experience and has done what other medications have failed to do.
Important Considerations Regarding Family Planning While on Rinvoq
Dr. Uma Mahadevan, MD, Director of Colitis and Crohn’s Disease Center at University of California San Francisco and lead investigator of the Pregnancy in IBD and Neonatal Outcomes study (PIANO) says when it comes to Rinvoq, the medication has been associated with birth defects in animals at the same dose as given to humans (30 mg), so she avoids prescribing this in pregnancy.
“I do not prescribe Rinvoq to someone who is about to get pregnant. However, Rinvoq is generally given to people who have not responded to anti-TNF, so if Rinvoq is the best medicine for them, I do not hold the fact that they are a woman of child-bearing age against them and give them the therapy to best put them in remission.”
Dr. Mahadevan says if a woman is on Rinvoq and becomes pregnant she has successfully transitioned patients to Skyrizi. This can be more challenging with UC as there are fewer options. The PIANO study is currently researching the safety and efficacy of these drugs. There are several Skyrizi patients being monitored right now and 2 Rinvoq patients so far. You can learn more about being a part of PIANO here. I participated in PIANO with my youngest child as an IBD mom who is on Humira. Being a part of this research is invaluable for our community and helps current and future families.
It’s believed that Rinvoq crosses into breastmilk, so you should avoid feeding your baby that way if you are taking this medication.
Rinvoq Complete Patient Support
Much like other biologics, there are patient support services in place that you want to be aware of. RINVOQ Complete provides personalized patient support when you need it. With RINVOQ Complete, you get 1-to-1 assistance with finding potential ways to save on the cost of your prescription and more. I use Humira Complete for my prescription needs.
You can also get help making sense of your insurance and finding ways to fit Rinvoq into your everyday routine.
If you have commercial insurance, you may be eligible to pay as little as $5 a month for your prescription with the RINVOQ Complete Savings Card. Click here to sign up for your RINVOQ Complete savings card.
Final thoughts
It’s important to remember that just because someone has a miraculous experience or a terrible one with a specific drug, does not mean that you will. I will say, with all the biologics that I’ve covered on Lights, Camera, Crohn’s the visible side effects (weight gain and acne specifically) were the most widespread and common among the patient population. So many of you said you felt guilty feeling “vain” about not wanting to be on a drug because of that, and I want you to know those feelings are valid and matter. At the end of the day, we all must measure risk vs. benefit and what matters most when it comes to keeping our IBD in check.
You can check out other Patient Experience articles that I’ve covered here:
It’s no surprise IBD impacts so much more than just our guts. Not only is there the gut and brain connection, but also the complex nature of our chronic illness(es) that can cause serious anxiety, depression, and mental health issues. The isolating nature of Crohn’s disease and ulcerative colitis, the unknowingness of what the next day holds, and the never-ending laundry list of procedures, labs, scans, and surgeries, year after year is a lot for any person to go through.
Even though I’ve lived with Crohn’s disease for more than 18 years, and have seen three different gastroenterologists in that time, not once has my mental health been brought up during a clinic appointment. When treating a person for IBD, the health of the whole person needs to be considered. I ran a poll on Instagram asking the IBD community if they’ve ever been to therapy. Out of 185 respondents, 70% seek therapy, 18% have not, and 12% are considering it.
I did an article in September 2020 about why a specific public bathroom at a grocery store I used to shop at triggers me and shared tactics for coping. You can read the article that featured Dr. Tiffany Taft here.
This week on Lights, Camera, Crohn’s we hear from those in our community about the advice that’s resonated with them the most since receiving their IBD diagnosis.
The words that have made a lasting impact
Olivia: “3% effort is still effort. You’re not going to be able to give 100% every day and that’s OK. Your best can look different from day to day.”
Julie: “It’s not your fault, you didn’t do anything wrong.”
Kristen: “You can’t drive forward if you’re always looking in the rearview mirror.”
Sarah: “Medical trauma is trauma and to give myself credit for all I have overcome.”
Cindy: “Remove all IBD related stressors from the bedroom to avoid impacting sleep. In our case, this meant no Humira injections for my daughter while sitting on the bed or nearby it.”
Tina: “Imitation is the best form of flattery.”
Lauren: “Don’t Google things you’re worried about, like symptoms.”
Jennifer: “Stay in the present.”
Heather: “Sometimes you just need to take a nap!”
Myisha: “If it’s not going to matter in five years, don’t give it five minutes of your energy.”
Kate: “It’s not your fault.”
Susan: “I’ve never seen a therapist, but I always tell myself it could always be worse.”
Stacey said: “You can’t control how seriously people take Covid. You can only control how you protect your physical and mental health. You have to put your health first. And, if people don’t agree with your choices, then that’s their problem. You can’t risk your health just to make it easy for others or to placate them. You come first in your life.”
Robin: “The “things” I do—my work advocating for others, supporting others, helping others face challenges with their diseases—I deserve that, too. Not from other people, but from myself. The beauty in therapy is that you’re receiving a non-biased/outsider opinion. This person that has no side and will sometimes say something you’ve heard 1,000 times in a way you’ve never heard before or even in a better way that allows you to really listen to what’s being said. To absorb it. Even to say it multiple times with no judgement if that’s what’s needed. Also, EMDR, which is a whole other thing and only part of the therapy experience.”
What is EMDR therapy?
Several people said EMDR therapy was their favorite and has been lifechanging. So, what exactly is it? Eye movement desensitization and reprocessing (EMDR) is a fairly new, non-traditional type of psychotherapy that’s popular for treating post-traumatic stress disorder. EMDR focuses on the natural tendencies our brains have for healing from traumatic memories. There are mental blocks (such as feelings of self-esteem issues and powerlessness) that can prevent us from healing. During EMDR, you are allowed to process the bad memories and experiences to start healing yourself. This helps our brains process challenging thoughts and feelings in a healthier way. Chances are through your patient journey you’ve endured several vivid and significantly painful moments that you haven’t been able to process and heal from.
Supportive Resources about managing mental health and IBD
Chances are you’ve heard of Pelvic Floor Therapy but may not know what this entails or why so many people in the IBD community are talking about it. Individuals with IBD can have persistent symptoms of fecal incontinence, constipation, rectal discomfort, and diarrhea, despite having their IBD in remission with medical therapy. These persistent and often debilitating symptoms can have a major impact on your wellbeing and quality of life.
This week on Lights, Camera, Crohn’s we hear from two gastroenterologists from Mayo Clinic along with several IBD warriors who provide insight, helpful guidance, and information about pelvic floor therapy.
What exactly is Pelvic Floor Therapy?
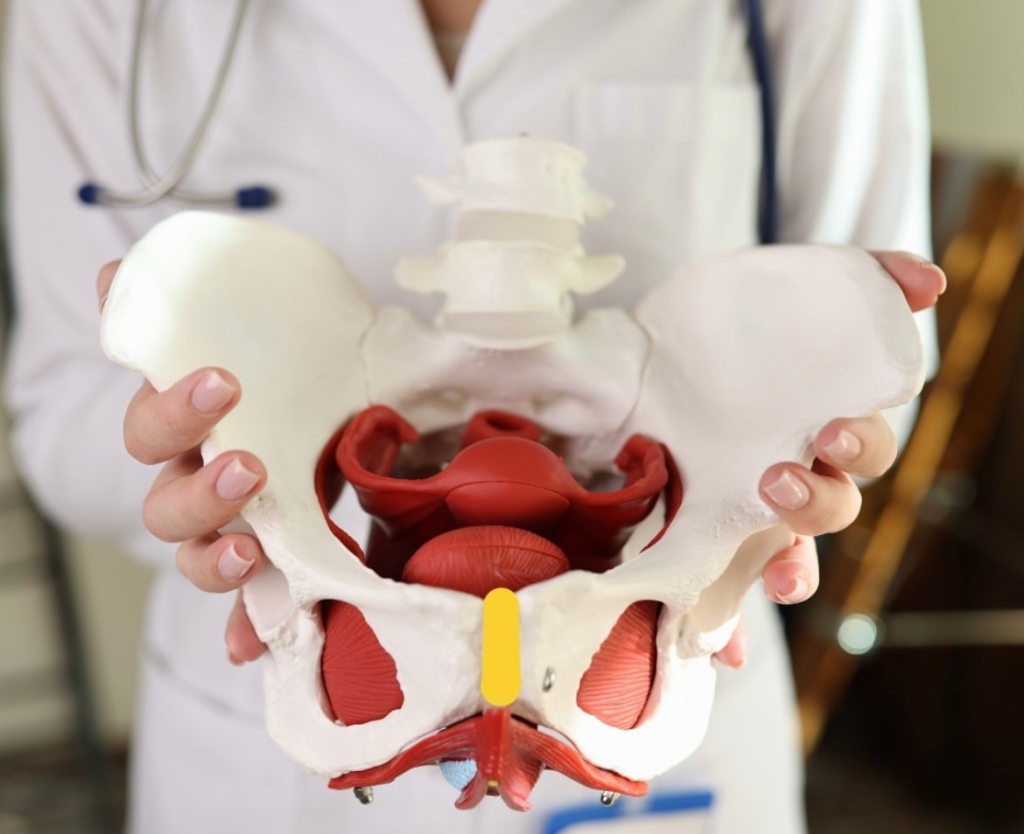
Pelvic floor therapy is a treatment program performed by pelvic floor therapists to retrain the pelvic floor muscles to address underlying issues such as constipation, fecal incontinence, or urgency. Many patients with IBD in remission may develop pelvic floor dysfunction which is usually diagnosed from a digital rectal examination in combination with an anorectal manometry test.
“During an anorectal manometry, a small catheter with sensor probes and a balloon is placed into the rectum and is connected by a wire to the computer. During the test you are lying on your side and asked to perform maneuvers to determine how your pelvic floor muscles work. At the end of the test, they inflate a balloon in the rectum to help evaluate for sensation and then ask you to simulate having a bowel movement by pushing the balloon out,” explained Dr.Katie Dunleavy, MB BCh BAO, Gastroenterology Fellow, Mayo Clinic.
Based on normal values for your age and gender, you may be diagnosed with a pelvic floor dysfunction. Dr. Dunleavy went on to say that in IBD, there is less research on the benefits of pelvic floor therapy.
“But we have seen benefit in up to 80% for patients in remission who continue to have symptoms of constipation, urgency, or incontinence once active inflammation is fully ruled out. Similarly, some patients with IBD undergo total proctocolectomy with ileal pouch anal anastomosis (IPAA) may also benefit from pelvic floor therapy if they have issues emptying their pouch,” said Dr. Dunleavy.
Additionally, those with IBD who’ve had pelvic floor surgeries might experience sexual dysfunction and this type of therapy directed towards relaxation of the pelvic floor can lead to a better sexual experience.
Pelvic Floor Dysfunction does not discriminate across genders
Any person can develop pelvic floor dysfunction and may benefit from treatment with pelvic floor therapy in the right setting.
“While most studies describe pelvic floor in females, I believe individuals from all genders deserve evaluation of their pelvic floor the recommendation for pelvic floor therapy. Furthermore, individuals of a transgender experience, might undergo gender affirming surgery that impacts their pelvic floor muscles, and would benefit from pelvic floor therapy,” said Dr. Victor Chedid, M.D., M.S., Gastroenterologist at Mayo Clinic.
Dr. Dunleavy says, “As many as 50% of people with chronic constipation have pelvic floor dysfunction, which means there is impaired relaxation and coordination of the pelvic floor and abdominal muscles during evacuation. Some common symptoms include straining with hard bowel movements, a feeling of incomplete evacuation, pain with intercourse, or urinary symptoms.”
Certain risk factors make it more likely for men or women to develop pelvic floor dysfunction, this includes instrumented vaginal deliveries, chronic constipation with straining, prior surgery, prolapse, and age. It is important for men and women to discuss symptoms with their doctor to ensure they get the appropriate testing and treatment.
Apprehensive about getting looked at?
It is important for people diagnosed with pelvic floor dysfunction to seek out a qualified pelvic floor therapist who is specialized in GI and evacuation disorders. These are generally physical therapists or occupational therapists who complete extra training in pelvic floor therapy.
“You should find a therapist you trust and will feel comfortable with during your therapy sessions. The therapists who work in this area are fantastic and work diligently to explain what they will be doing. My patients tell me that the relief they feel from therapy well exceeds the apprehension they had prior to starting sessions,” said Dr. Dunleavy.
It’s important for patients to feel comfortable talking with health care providers and addressing concerns they may have on this topic. Dr. Chedid typically discusses the benefits of pelvic floor therapy with patients during clinic visits as a beneficial treatment option that does not require surgery. He provides patients with exercises and techniques to do at home that will have a major impact on general wellbeing and health.
“Individuals with IBD experience significant “negative” experience with the bathroom and with defecation that can be quite traumatizing, and therefore when they get in remission, they still have a negative association with the bathroom and might have “fear of defecation” despite being in remission. I equate that to “PTSD of the pelvic floor”, which is not a medical term, but an analogy I use. Therefore, pelvic floor therapy is essential to reverse this negative experience with the bathroom and make their bathroom experience a healthier and satisfying experience. Almost all patients who I describe this to get it right away and understand the importance of pelvic floor therapy,” said Dr. Chedid.
He adds that it’s imperative health care providers communicate with patients and ensure that the therapy session will be a safe space with at rained physical therapist who is trained in empathetic and trauma informed care. This is essential in putting a person’s mind at ease, as many patients might have experienced sexual trauma in their lifetime that makes pelvic floor therapy triggering for them.
The impact of Pelvic Floor Therapy post operatively and after IBD pregnancy
If you’ve had a total proctocolectomy and an ileal pouch anal anastomosis (IPAA), you might experience non-relaxing pelvic floor dysfunction or pouch evacuation disorder. This is similar to the rectal evacuation disorder in individuals with pouches.
“Typically, this is identified by history, physical exam, pouchoscopy, anorectal manometry and dynamic imaging of pouch evacuation. Additionally, someone who has had any form of trauma to the pelvic floor, including Perianal Crohn’s disease or surgeries for Perianal abscesses or fistulas or lacerations due to vaginal deliveries after pregnancy, these patient might experience rectal evacuation disorders after recovering and healing. In the proper patient, if identified by history, physical exam and the right testing, these patients will benefit from pelvic floor therapy,” said Dr. Chedid.
At the same time, there isn’t a lot of research on pelvic floor therapy in the post-operative state or following pregnancy in patients with IBD.
“There have been several attempts to find normal values for patients with IPAA who have undergone colectomy to help diagnose pouch related pelvic floor dysfunction. We generally recommend patients wait until the anastomosis following surgery is completely healed prior to having an evaluation with a balloon to ensure no complications. Similarly, patients who have recently undergone delivery from pregnancy will likely require time to heal. I would discuss this with your doctor to have more personalized information,” advised Dr. Dunleavy.
If your GI recommends pelvic floor therapy for your personal symptoms and struggles the overall response is tremendous.
“Recommending pelvic floor therapy to everybody, without identifying the right patient who would benefit from it is not typically beneficial. Therefore, in the right patient, pelvic floor therapy is extremely effective,” said Dr. Chedid.
What IBD patients have to say
Stacey has ulcerative colitis and went from having an ostomy to becoming a j-poucher. She’s a big proponent of Pelvic Floor Therapy. After her 3-step surgery to j-pouch in 2021, she knew she needed at least an evaluation from a pelvic floor physical therapist (PFPT) after urination became a challenge and inserting tampons became impossible during her takedown recovery.
“My surgeon wouldn’t write me a referral, citing that the anorectal manometry tests prior to surgery were all normal. My GI doctor didn’t want to go against the clinical judgement of my surgeon, so I couldn’t get one from her either, and finally I received a referral from my OB/GYN after explaining that penetrative sex was impossible (and felt unsafe to me) to even attempt,” Stacey explained.
These delays resulted in 5 months of significant pelvic pain that she felt ill-equipped and under-supported to handle, and this time could’ve been saved if she had gone into surgery with a referral to see PFPT from the get-go, even if she didn’t need to use the referral; it would’ve been nice to have.
“It’s so wild to me that orthopedic surgery has extensive PT rehabilitation protocols, and yet I was met with such resistance to gain access to the professionals who could help support my muscular recovery, even after such extensive GI surgeries,” she said.
During Stacey’s initial encounter with the PFPT, she spent the majority of the visit trying to gain a strong understanding of her entire pelvic and holistic health history, everything from sexual health to physicality to surgery, and all the in-between.
“She asked for consent prior to any invasive exams and explained them in thorough detail, reminding me that I was in control and could always choose to stop an exam if I felt unsafe. She continued to breathe with me during the exams and communicated her findings in real-time, which made me feel at ease. At the conclusion of our visit, I was told that I was experiencing hypertonic pelvic floor dysfunction from a decade of clenching for dear life trying to make it to the bathroom with mod-severe UC, even before my surgeries. The tightness of the muscles, coupled with three extensive pelvic surgeries, contributed to the pain and issues I was experiencing,” said Stacey.
During the visits with the PFPT, Stacey discovered she had no awareness of her pelvic floor muscles whatsoever. She could not distinguish the relaxation of the muscles from the contraction, and the entire area felt numb to her, like it was a holy, empty space. She says this made the exercises challenging to understand initially. She was prescribed specific exercises, not Kegels, including strategies to gain awareness of supportive muscle groups so she could begin to engage with this part of her body and start to heal.
“What I did not expect, however, was for this experience to be as enlightening and empowering as it was. Slowly but surely, the little life things showed me that they’re the big life things: being able to fully urinate in under 20 minutes, FINALLY being able to use tampons again- these were MASSIVELY important to my quality of life, and they became possible through the help and support of a PFPT and my adherence to their prescribed exercise regimen. I even realized one day while holding one of my exercise poses that I could feel the muscles DEEP in my abdomen! They felt heavy, full of pressure, as if they fired on to greet me, and then suddenly… I could feel them gently, slowly, RELEASE. I cried tears of relief realizing that I had been fearful of reconnecting with these muscle groups, and it really was safe and okay to be in my body.”
Stacey says she had NO idea these muscles existed, yet here they were. Had they been here all along?! She says she numbed them out from years of associating the deepest parts of her with pain from UC; and that her brain was protecting her. I truly wonder. All she knows is the day that she could FEEL her body experience relaxation and safety with FULL awareness of these pelvic muscles is the day that she knew that healing from these surgeries was going to be possible.
After one year of PFPT, Stacey “graduated,” not free of pain, but with the tools to know how to live within the ebbs and flows of pain. She tells me she still relies on the tools and bodily awareness that she gained through the experience.
Jessie was diagnosed with Crohn’s disease when she was 15 years old and after more than 22 surgeries later, at the age of 38, she says she completely underestimated how much her pelvic floor was affected over the years by the inflammation, surgeries, and her pregnancy.
“I was “guarding” badly (a response to pain) and so weak. I was having bladder issues, pelvic pain, rectal pain and so much more. After 2 years of being consistent going to pelvic floor therapy and doing the exercises I can say I’m about 85% better. I can’t say enough how much of a HUGE difference pelvic floor therapy made in my life and my IBD journey. My therapist explained it to me like this “you don’t have orthopedic surgery on your knee, wrist, ankle, spine, etc. and not get prescribed physical therapy. Same with an injury. It’s just standard procedure. But, for some reason, even though your pelvic floor consists of tons of muscles, ligaments, tendons, bone, etc. the same process is not considered – but IT SHOULD BE!” Your pelvic floor needs to be rehabbed after any injury, strain, surgery, etc. just like any other muscle/tendon/ligament/bone in your body,” explained Jessie.
Claire started PFPT because all imaging and tests showed that while her inflammation is under control, she still experiences extreme pain.
“I was tested, and they found I have dyssynergic defecation. This was caused by my chronic pain due to long-lasting fissures as well as chronic constipation. I’m grateful my GI thought to have me tested for this, as many don’t make that connection since the symptoms are so similar to Crohn’s. During PT, I have learned that my muscles do not relax and are constantly tense, so we work on trying to get them relaxed in order to successfully pass bowel movements. Like all other PT, one downside is that it is a lengthy process and takes up a lot of time. I have a one-hour appointment every week for 12 weeks and an hour or two of exercises and stretches on my own every day.”
She says she’s started to notice improvements and found ways to make her pain more bearable, though it’s something she will have to continue working on for a long time.
Tiffany has accessed pelvic floor therapy for herself and having previously been a physio and a fellow Crohnie, she recommends people speak with their doctors because it can make a world of difference, especially after surgery, hospitalization, or a flare.
“The neural connection we have to our trunk and pelvic muscles can be re-trained and strengthened, allowing less pain, and for me an improved sense of control over urgent bowel movements.”
Preslie was diagnosed with Crohn’s in June 2016, and after two years of battling severe symptoms, she had a colonoscopy that showed she was in remission. It may sound like lovely news, except Preslie was still living with a ton of pain, so her and her care team started digging for answers.
“This led to an Endometriosis diagnosis in August 2018. That was great news, except I STILL was not getting relief, and started having severe burning anytime I urinated, but always tested negative for UTIs. I went to a male urologist who told me I was just constipated, which was not the case. After well over a year of extremely painful sex, constant pain, and burning when I peed, I went to a urogynecologist who talked with me for less than 10 minutes and had the diagnosis: Interstitial Cystitis and Levator Ani Syndrome. I finally felt heard. I started pelvic floor therapy shortly after and immediately felt relief.”
Rocio says pelvic floor therapy was recommended to her by a home health physical therapist who was treating her for neuromuscular issues after bowel resection surgery for her Crohn’s in 2020.
“During my resection recovery, I was struggling tremendously with constipation, which was unfortunately always my issue with my IBD. Although uncommon, it’s been my reality for the last 20-plus years. The reason I share this is because I wish someone would have recommended pelvic floor therapy to me over all those years.”
She began seeing a pelvic floor therapist in January 2021 and completed two years of treatment. During that time, Rocio says she learned a lot about the intricacies of all the muscles, the nerves, the internal blood flow, and so much more. Because of two fistulotomies and a stricturplastly, she has numerous anatomical issues which prevent her from having normal bowel movements.
“Pelvic PT changed that completely and I have normal/formed BM’s every single day, without any signs of constipation and without any straining. I’ve learned ways in which I can help relax and release the pelvic floor should I face issues in the future.”
Separately, Rocio has learned how beneficial pelvic floor therapy is for many IBD patients post-operatively, including the ileal resection she had. Her therapist worked on her abdomen significantly during appointments to prevent adhesions and scar tissue. She says there are so many benefits to pelvic floor therapy that it does make her wonder why more IBD health care providers aren’t encouraging patients to pursue care.
Annie started pelvic floor therapy two weeks ago. She was referred based on suspected interstitial cystitis, not her IBD. She was shocked to learn during her first appointment that treatment was for all conditions that involve urgency of any kind.
“The game changer was the pelvic exam itself, I never realized what my PT noticed right away, which is that my first layer of pelvic muscles are unnaturally sensitive. This is massively helpful for IBD and IC, but the most validating part was having a lifetime of excruciating intercourse and painful pap smears and knowing the reason. My PT told me this is not how my life has to be. After just two weeks of exercising my pelvic muscles with a vaginal wand and daily targeted yoga, my urgency, both with my Crohn’s and IC, has gotten so much more manageable. I started this journey running to the restroom every 30 minutes (even at night), now I feel like I’m starting to get my life back.”
Jasmine says pelvic floor therapy helped her a ton following j-pouch surgery.
“I truly believe it should be integrated into post-op care plans, I had to seek it out and ask for it.”
Amy says that while she doesn’t have experience yet with PFPT, she has a complicated Crohn’s history for the past 25-plus years. Now that she’s over 40 and has had three vaginal births, she recently asked her doctor about pelvic floor therapy.
“Because of all the IBD women sharing their journey with this on the Internet, it inspired me to look into therapy for myself. In my first request, the response was that it might be a fantastic idea, but to wait and see. My next visit is in a couple of weeks and I’m looking forward to utilizing this article to share and take with me to help me advocate for myself.”
A look at the insurance piece
Yes, pelvic floor therapy can be covered by insurance, but it can vary based on the type of insurance. It is also important to ask about coverage for biofeedback therapy which is an essential part of the therapy based on prior research studies. Many insurance companies will need proof of diagnosis using an anorectal manometry with balloon expulsion test or defecating proctogram.
“If the proper indication based on testing is identified with the referral to pelvic floor therapy with a script written by someone’s GI provider, then typically insurance should cover it,” said Dr. Chedid.
Closing thoughts on Pelvic Floor Therapy and IBD
It is important to discuss with your doctor if pelvic floor therapy is right for you. Once patients with pelvic floor dysfunction have these basic tools, they can begin retraining the pelvic floor muscles with biofeedback. Biofeedback provides auditory and visual feedback to help retrain the pelvic floor and relax the anal sphincter. Biofeedback training is the treatment of choice for medically refractory pelvic floor constipation, with some studies showing improvement in more than 70 percent of patients. Patients also learn to identify internal sensations associated with relaxation and long-term skills and exercises for use at home.
At Mayo Clinic patients have had more than 70% response at 3 months following initiation of pelvic floor therapy. The response usually takes weeks to months to see a clinical difference and requires patients to practice their exercises and biofeedback at home.
“Although many centers are familiar with retraining techniques to improve pelvic floor dysfunction, few have the multidisciplinary expertise to teach patients with constipation how to appropriately coordinate abdominal and pelvic floor muscles during defecation, and how to use bowel management techniques, along with behavior modification, to relieve symptoms. Because pelvic floor dysfunction can be associated with psychological, sexual, or physical abuse and other life stressors, psychological counseling is often included in the evaluation process,” said Dr. Dunleavy.
If you have chronic pain, you may also need to see a physician to have these issues addressed prior to starting pelvic floor therapy.
Key takeaways from fellow IBD patients
PTs are an excellent resource, but just like getting an IBD-ologist is superior to a general GI doctor, PFPTs are an even stronger resource, ESPECIALLY in the context of chronic GI disease where so many of our deepest muscles are constantly working on our behalf.
You can always say “no thanks!” You don’t need to agree to any sort of exams or exercises that you’re not ready for, and a compassionate PFPT will empower you to make decisions and communicate in alignment with your body’s needs.
ANYONE can benefit from PFPT: any age, any gender.
Normalizing pain and discomfort is a survival instinct, but it’s not necessarily serving you for the GOOD life- it’s okay to get evaluated if you’re concerned about sexual pain or dysfunction, pain with periods, or if you also have IBD and simply want to be sure that you’re supporting your pelvic and spinal muscles the best you can so that you can, especially in the bathroom!
YOU get to decide! Having an evaluation may be all you have the capacity for, and that’s okay! You can return for a plan of attack later, or you can wait until you have the capacity to dive in head-first! There’s no one right way.
If you decide while talking to a PFPT before they do ANY manual evaluations that something doesn’t feel right- YOU GET TO CHOOSE, and you can always, always say, “nevermind”. Advocating for your body is always progression in your healing journey, every single time.
SPEAK UP! It’s RIDICULOUS that patients have to ask and ask and ask for the bare minimum, but if it helps your quality of life and it’s within your capacity- it’s certainly worth it.
A big deterrent for patients can be cost, but the investment is worth it, if you can swing it. You would be surprised how much every system of your body is so connected and feeds off one another!
Helpful resources to check out
Find a Pelvic Floor Therapist Close to Home
Utilize the “Section on Women’s Health” or the “Herman & Wallace” websites. Both these groups train therapists who specialize in pelvic floor disorders.
The Section on Women’s Health (SOWH) website has a “PT Locator” tab. You can enter search criteria including your geographic location (e.g., zip code) and specialty (e.g., constipation) to identify a therapist closer to home.
The Herman & Wallace website has a “Resources” tab under which you will find a “Practitioner Directory.” Use the map features to locate a therapist near you.
Utilize the “find a provider” section of www.pelvicrehab.com for a local PT by zip code.
The therapists who work with pelvic floor disorders may be in Gastroenterology, Urology, Gynecology, Physical Medicine, and/or Women’s Health, etc. You may be able to find someone through your local physicians or contacts.
For those in Canada, check out the Canadian Physiotherapy Association. It has a “Find a Physiotherapist” tab which allows you to connect with the sites of participating provinces/territories. By specifying a “Women’s Health” therapist or equivalent, you may find someone who specializes in the field of incontinence, pelvic pain, constipation, etc.
The benefit of pelvic floor therapy also involved patient education, relaxation exercises, diaphragmatic breathing, and correction of maladaptive toileting behaviors. Some studies have shown improvement in quality of life relating to symptoms, and mental health.
I remember the first phone call when I was pregnant with my oldest as a soon-to-be IBD mom. A researcher from Mother to Baby called me when I was newly pregnant and leaving work—I sat in my car in a parking lot, as she asked me several questions about my health, well-being, medication, and pregnancy thus far. That was Fall of 2016. Fast forward to now—and my oldest, Reid, just graduated from kindergarten. When I was diagnosed with Crohn’s disease at age 21 in 2005, one of my biggest fears was whether my chronic illness was going to rob me of motherhood. Back then, I was nowhere near ready to settle down, but the worry was always in the back of my mind.
When my husband and I got married in June 2016 and I was 10 months into surgical remission, we knew we needed to capitalize on my IBD finally being under control. Luckily, we got pregnant one month after getting married. Shortly thereafter, I started researching pregnancy studies for IBD moms. Lights, Camera, Crohn’s launched two days before I received a positive pregnancy test. I was fresh into my advocacy and had never been pregnant before. I didn’t have a community of IBD moms to lean on for questions or support as I navigated the unknown.
I came across information about Mother to Baby online and ended up being a part of their pregnancy studies for my first two children. The studies were different, but I had such a positive experience with Reid, that I decided to participate again with my daughter, Sophia. Reid’s study was a 5-year look at how Humira impacts babies in utero through kindergarten. When I was initially pregnant with him, this felt light years away. And here we are. Over the course of his pregnancy and until November 2022, I completed surveys, did phone interviews, had an in-person meeting with a doctor who came to my home and looked him over in front of me for any health anomalies, and most recently did an in-person cognitive neurobehavioral assessment at a nearby hotel with researchers.
We just got the results. While it’s rewarding to participate in IBD studies and interesting to learn, there’s always a part of you that worries about the findings and if mom guilt will ensue. It’s been reassuring and comforting to see my healthy kids, who were exposed to Humira in utero through the 3rd trimester, thrive and excel with milestones and in school.
The findings of the study
In November 2022, Reid and I met up at a nearby hotel with two researchers who provided neurodevelopmental behavioral evaluations for both of us. Reid’s assessment used a series of questions, games, and puzzles to help researchers determine his development of language ability, memory skills, and problem-solving abilities. The tests were selected to provide an evaluation of general mental ability and to describe specific abilities in areas of verbal knowledge and reasoning and visual-perceptual reasoning and organization. The tests were intense, I was proud of him for how he handled himself during the process.
Reid and I waiting to do our assessmentwith research administrators
According to Mother To Baby, “this battery of tests is best suited to examine the similarities and differences among groups of children. While it was not adapted for Reid’s individual characteristics, it can highlight general strengths and weaknesses in a child’s cognitive profile and indicate potential concerns when present.”
Behavioral Observations: “Reid was personable and interacted with both administrators on his arrival. He had a very positive attitude toward testing and quickly became comfortable with administration. He was engaged and attentive to the materials, listened attentively to the examiner and provided effortful responses even as questions became more difficult. Reid demonstrated good cooperation and attitude by following instructions and requiring minimal to no redirection from the administrators of his mother. He was focused and friendly for the full duration of testing.”
Summary of Assessment Results: “Tests were administered in a single testing session with one short break. The Wechsler Preschool and Primary Scale of Intelligence (WPPSI-IV) was selected to provide an evaluation of Reid’s general mental ability and to describe specific abilities in areas of verbal knowledge and reasoning and visual-perceptual reasoning and organization. This battery of tests is best suited to examine the similarities and differences in ability among similarly aged groups of children. While it was not adapted for Reid’s individual characteristics, it can highlight general strengths and weaknesses as well as potential concerns when present.”
The intelligence test was comprised of 10 subtests which measured a variety of verbal and nonverbal skills. Reid achieved a composite score in the average range. In the working memory category and spatial working memory, Reid performed in the high average range, which required him to remember and identify pictures that had previously been shown to him. On tasks that measured visual-spatial abilities, Reid scored below average. These tasks required him to synthesize visual stimuli to recreate block design.
“Reid was highly focused while processing visual stimuli. Overall, Reid is a bright and enthusiastic child. He was a pleasure to work with.”
Along with Reid’s assessment, I was also interviewed and performed tasks with an examiner on the other side of the room. I was assessed in the adjustment and life context. Tests included the Center for Epidemiological Studies Depression Scale and Parent Stress Index. My scores were within normal limits and my general mental ability also scored in the average range. Not gonna lie, the testing was challenging!
Reflecting on my experience
As an IBD mom of a 6-year-old, 4-year-old, and 22-month-old, who participated in pregnancy research during each of my pregnancies, I can’t begin to tell you how incredibly rewarding it is to know that your personal experience is helping to drive the future of care for women in our community who have hopes of one day being a mother. Sure, it takes a little bit of time and effort, but the data and research to show the safety and efficacy of medications while pregnant and breastfeeding is so needed. It’s comforting to know Reid is right where he needs to be cognitively and healthy physically, despite my high-risk pregnancy and exposure to Humira until 39 weeks gestation. We need more women to willingly step up to the plate and share their journeys to help guide the future of IBD motherhood and show all that’s possible despite our disease.
Opportunities to participate in research
Many people need to take medication during pregnancy to manage and treat their IBD. Yet, according to the Mother To Baby website, fewer than 10% of medications have enough information to determine their safety for use in pregnancy.
Do you have Crohn’s disease? Are you currently pregnant? If you answered “yes” to both questions, you may be able to help Mother To Baby advance the knowledge of how managing IBD in pregnancy impacts a developing baby. Click here to learn about how you can impact the health of future families by joining the Crohn’s Disease and Pregnancy Study.
July marks 15 years since I started my journey taking a biologic injection to manage and treat my Crohn’s disease. Since that time, I’ve had routine “safety labs” every 3-6 months, depending on my gastroenterologist. You may be familiar with safety labs, or you may wonder what I’m talking about. I’ve been seeing my current GI for almost 8 years, and she’s adamant that I get labs every 3 months to make sure my disease is closely monitored. If I fail to get labs every 3 months, per her orders, my prescription for Humira is unable to be filled by my specialty pharmacy.
I ran a poll on Instagram and asked, “If you are on a biologic, do you get safety labs every 3 months?” Of the 175 people who responded, 41% said “yes”, 36% said “no”, and 23% had no idea what safety labs are. This week on Lights, Camera, Crohn’s we take a closer look at the reasoning and purpose behind safety labs, and we hear from esteemed and world-renowned gastroenterologists Dr. David Rubin, MD, Section Chief of Gastroenterology, Hepatology, and Nutrition at the University of Chicago Medicine and Dr. Miguel Regueiro, MD, Chair, Digestive Disease and Surgery Institute, Professor in the Department of Medicine, Cleveland Clinic.
What is a safety lab?
Safety labs are to ensure that patients are not developing a complication from a medication that they may not feel.
“For example, kidney or liver function tests that may show an abnormality before a patient has damage to those organs, or problems. Or a white blood count that lowers in a patient on certain immunosuppressive therapy – something they may not “feel” until the immune system gets low enough to develop an infection,” explained Dr. Regueiro.
The periodicity of labs for “safety” are often taken from the clinical trial designs, rather than the likelihood that something is going to change within that period of time.
“Routine labs while on therapies for IBD is important and patients can and should keep track and ask for them at least twice a year for most of our therapies. For many of these, there are gaps in our understanding whether the interval (every 3 months for example) is the right one or makes a difference. We certainly know it takes time for patients to do this and costs money too. Some of my colleagues withhold refills as a safeguard to make sure patients get their labs. This may be more punitive than necessary, but it is one way to make sure this is getting done,” said Dr. Rubin.
When I get my labs done every 3 months the following blood tests are ordered by my GI:
CBC w/Auto Differential
Hepatic Function Panel (Liver Panel)
Vitamin D 25 Hydroxy (I am deficient, so we keep a close eye on this)
If there is concern about inflammation or anemia, then my GI also adds:
Sedimentation Rate, automated
High Sensitivity CRP
Iron Profile with IBC + Ferritin
In the past, if there’s concern about my response to Humira we do a “trough level” to see if I’ve built up antibodies to my therapy and to measure how much medication remains in my body right before I am scheduled to do another injection.
It’s important to know, since I started seeing my GI two months after my bowel resection surgery in 2015, I have been in remission. So, the concern about inflammation and needing to take fecal calprotectin tests has been few and far between. When we were in the middle of the pandemic, rather than an annual colonoscopy, my doctor had me do a fecal calprotectin test at home to limit my risk of being exposed to germs in a hospital setting while my disease was well-managed.
“We recommend certain labs on patients taking IBD medications. Each medication will require a different safety lab monitoring strategy. Some brief examples, for mesalamine, checking kidney function tests within a couple of months of starting a medication and then once or twice a year. For thiopurines (6MP and Imuran) and methotrexate more frequent blood work initially, e.g., complete blood count and liver function tests weekly to every other week in the first two months after starting and then every few months thereafter,” said Dr. Regueiro.
Safety labs as a disease monitoring strategy
Generally, safety labs are done for medical health reasons to make sure that everything is ok while taking the medication.
“Safety labs are “driven” by the physician or provider caring for the patient. The insurance company may require certain labs before starting or continuing a medication. For example, a tuberculosis (blood) test before starting an anti-TNF medication and then yearly while a patient is on the medication. Otherwise, the insurance company usually does not require safety labs for medication approval or continuation. Each case is different, and each insurance company is different,” said Dr. Regueiro.
“More important than pharma-drive lab recommendations—is that every patient should have a customized strategy to monitor their disease stability to detect relapses before there are clinical consequences. This is my new take home message for most of my lectures- in addition to “treating to a target” we must have “disease monitoring” as something that every patient has as part of their care,” said Dr. Rubin.
Chronic diseases like IBD tend to “drift away from control”, so it is good to keep an eye on things and this enables proactive preventive care.
Getting my safety labs in the thick of the pandemic
“For low-risk patients, that might be once a year, but for those who are on advanced therapies (biologics and the novel targeted small molecules), they likely need this approach more frequently. It is true that “knowledge is power,” and knowing that the disease has activated enables much better care,” explained Dr Rubin.
Disease monitoring may involve blood or stool markers (calprotectin) or depending on where you live, intestinal ultrasound. Colonoscopy or CT scan/MRI is also recommended. Dr. Rubin tells me the key is identifying what is appropriately benchmarked and reliable and which approach is feasible and makes the most sense for the patient.
Why the onus is often on us
As you can imagine, 3 months comes quickly. If you’re like me, I see my GI in clinic two times a year (every 6 months). When I was pregnant, she would see me in the office every 3 months. Given that I see her twice a year, that checks off two of my four lab visits. As an IBD mom juggling life with three young kids, time can often slip away. I’ve found I must alert my nurse and GI about when and where they need to submit lab orders so I can take care of them the other two times a year at a Quest or LabCorp nearby. In the past there have been a few times where I’ve dropped the ball.
Coordinating life with chronic illness can truly feel like a full-time job. Just this week I spent an hour on the phone with my specialty pharmacy trying to organize my next shipment because there was an issue with my patient savings card. At the time, all three of my kids were running around like little banshees, yelling, and making it hard for me to hear the phone representatives. At one point, I had to lock myself in my laundry room. These aren’t calls that can wait. Patients need their medication; we can’t just hang up and re-visit the snafu at another time because it can mean we receive our biologic shipment late. This is one small example—of a behind-the-scenes look at life with IBD as a mom.
While getting labs four times a year may not seem like a lot, it does involve planning, time, and coordination for patients. My kids have joined me countless times in the stroller as I get labs done. Then, reading the results on the Patient Portal and seeing certain results too low or too high can cause anxiety and added stress. It’s a never-ending cycle.
Talking with your care team
If you’re only getting labs done once or twice a year, it may be worth having a conversation with your GI about the reasoning why and what you feel most comfortable with. Your care is not a one-way street. If you feel like you need a more hands-on approach, talk about this with your doctor. In talking with fellow IBD patients, many who are on infusions every 8 weeks, tell me they get labs every 16 weeks.
If you’re only getting labs done once a year, Dr. Regueiro says you don’t necessarily need to be alarmed.
“For a patient who has been on a medication like mesalamine or a TNF inhibitor for a long time, in remission, and doing well without prior lab test abnormality, once per year lab testing may be ok. However, a patient on Imuran or 6MP may need lab testing more frequently.”
As a veteran patient, who was diagnosed with Crohn’s nearly 18 years ago, safety labs have become part of how I manage my IBD. While annoying at times, these labs also give me a sense of relief. One final recommendation I have—don’t try and get labs done before or after your colonoscopy—I’ve tried this twice to try and kill two birds with one stone, and with being so dehydrated, it was not a pleasant experience. Being closely monitored through safety labs takes away much of the stress and worry that can come because of being on a biologic, and the possible side effects that can happen now and into the future.
A special thank you to Dr. David Rubin and Dr. Miguel Regueiro who took the time to offer their expertise for this article on the heels of Digestive Disease Week (a HUGE conference they both actively participate and present at). Having their insight on topics like this that matter to patients means so much.
This article is sponsored by Health Beacon. All thoughts and opinions shared are my own.
When I think back about the scariest moments I’ve experienced since my Crohn’s disease diagnosis more than 17 years ago, doing self-injections and the loading dose process tops the list. To go from being someone who didn’t rely on a biologic medication to function and treat my chronic illness, to mustering up the strength to inflict pain on myself, it took getting used to, to say the least.
I’ll never forget what it was like when I was first told I would need to choose between a self-injection and an infusion while lying in a hospital bed with a hardcore flare. It felt like trying to pick the lesser of two evils at the time. I chose self-injection for privacy reasons because at the time I was a television news anchor and hadn’t shared that I had inflammatory bowel disease (IBD) publicly. I also have terrible veins and the thought of having to get IVs and be hooked up for hours to a medication seemed less convenient and like more of a reminder that I was unwell. During that hospital visit it took 8 tries to start my IV, so the trauma of that helped guide my choice to do injections instead.
Going the self-injection route
When I started my biologic in 2008, there were only two medications on the market to manage and treat Crohn’s disease – Humira and Remicade. The injection (I was prescribed) at the time had a reputation for being painful and the loading dose involved four injections, back-to-back in one sitting. When my mom and I walked into my gastroenterologist’s office so the nurse could instruct me on how to give myself shots, I was shaking like a leaf. In the moment I wasn’t sure how I was going to muster up the strength not knowing how it would feel. My palms felt sweaty holding the foreign injector pen in my hand. I wasn’t sure how badly it was going to hurt. I was fearful of the side effects and what the heavy-duty medication was going to make me feel like. I wanted the nurse to do the first injection for me, and she wouldn’t. In the moment that made me upset, but now I am so grateful she put the onus and trust on me. I’ve never had anyone do my injections but myself.
I pressed the button and instantly felt the liquid fire pain shoot into my leg. I couldn’t believe I was expected to do that three more times. But I did. When the appointment was over, my mom and I hugged in the hallway. I felt like I had been through battle. It was terrible. Knowing that I had to do another two injections in two weeks loomed over me. Unfortunately, my initial loading dose made me very sick. As my body got acclimated to the medication, I felt weak and could barely walk up 13 stairs to my apartment. I had to miss work and social functions as my body got used to medicine.
Going through another round of loading doses
Fast forward to 2015. I had bowel resection surgery that involved the removal of 18 inches of my small intestine, appendix, and Meckel’s diverticulum. My care team had me go off my medication for three months—prior to surgery and after. Because of that, I had to do another loading dose and re-start the process. Even though I was already more than 8 years into doing the same injection, when my GI told me I would need to do another loading dose, my mind immediately raced back to 2008 and what I went through. I was so emotional I had to call into work sick that day. Luckily, this time around was a lot less scary, and I had more confidence in the process and knew exactly what to expect. I didn’t have any side effects after this loading dose, and I was back on track to my normal injection routine.
The shift to “pain-free” injections
The first couple years I did my injection, I would count down the days until the next one was due with dread and worry. I spent more than a decade on the painful version of the medication. In 2018, the formula for the medication was changed for patients in the United States, taking out the sting and making the gauge of the needle smaller. The loading dose now “only” involves two injections versus the four.
The “pain-free” version of the medication has completely changed my patient experience for the better. I no longer dread my shot. The process feels simple and nearly effortless. Even though I’ve been lucky to be afforded the opportunity and access to this version of the medication, I can still remember how it used to feel. The anxiety and emotions the injection would cause, and what I dealt with for 10 years of my life every other Monday.
Self-injection through pregnancy and motherhood
I am an IBD mom with three young children. Ages 5, 3, and 15 months. When I was first pregnant in 2016, it took a lot of guts and felt like an emotional rollercoaster injecting a biologic knowing there was a life growing inside of me. As the weeks turned to months and my belly got bigger and bigger it became more emotional feeling kicks and movement in my stomach while I was pressing the button to give myself the shot. Until my son was 1.5 years old, he witnessed how upset the injection would make me at times and would hug me and watch with empathetic eyes from a very young age.
When I tried the pain-free injection in 2018, I shot a video the first time I experienced it. This time around, I was pregnant with my second child. You can watch the emotional video here. As I express in the video, it was lifechanging to know that throughout future pregnancies and through motherhood, my children wouldn’t ever see their mom crying or scared while doing injections anymore. Now, when I do my shots, I have a big smile on my face and my children see their mom through a much different lens.
Keeping your eye on the prize
Whether you are gearing up for your loading dose or a veteran self-injector, it’s an experience that can be hard to put into words unless it’s your reality. It’s normal to grieve and be upset about your situation. Try to breathe. Go to your happy place. Get a focal point to focus on and know that you are doing all you can to help keep your disease under control and live the fullest life possible. Short term pain, long term gain in every sense of the word. Being scared no matter where you are in your patient journey is understandable, but like all pain and fearful experiences, they too shall pass.
Click here to learn more tips about self-injecting.
The article discusses how teenage girls and young women post upsetting footage and commentary on social media about their “invisible illnesses” to gain attention and “likes” and bashes “Spoonies” for giving people a behind-the-scenes look at the reality of their chronic condition. Hold UP. As someone who has lived with Crohn’s disease for more than 17 years, who is patient advocate, and works tirelessly to empower and educate others about life with inflammatory bowel disease, by candidly sharing on social media and through my blog, I find it incredibly disheartening and worrisome that a story of this nature is in circulation.
The ableist mentally shines bright
How disappointing that a “news outlet” takes the time to belittle people who are battling debilitating and unpredictable illnesses and sharing their struggles not for attention, but for support and camaraderie. Unless you have a chronic illness, you don’t have the slightest clue about what it’s like to wake up each day and not know what the next hour is going to bring. Unless you have a chronic illness, you can’t begin to imagine the stress, worry, and anxiety that comes along with diseases that limit us and often set us up for failure when it comes to trying to keep up with the rest of society. Unless you have a chronic illness, you have no idea how isolating and overwhelming it can be to be young and unhealthy, different than your peers, while fearing what your future is going to hold. Unless you have a chronic illness, you can’t fathom what it’s like to juggle multiple specialists, appointments, medications, insurance, specialty pharmacies, and screening tests… just to survive. It’s imperative those with invisible chronic illnesses share their stories and show others that what they are going through.
Articles like this are extremely damaging and triggering to those who suffer in silence, the newly diagnosed, and furthers the fear of what could happen if you decide to come out of the “proverbial closet” publicly and share about your health struggles.
Patient communities NEED you to share
When I was diagnosed with Crohn’s disease at age 21 in July 2005, Facebook hadn’t even been out for a year. No one was going on social media and sharing they had a disease. I felt like I was on a desert island, all alone with a diagnosis that flipped my world as I knew it upside down. As an aspiring TV journalist, two months out of college graduation, I had no idea how I was going to function and follow my dreams. Nobody wants a chronic illness diagnosis. Nobody asks for this. Nobody wants to suffer so they can have “likes” and attention on social media, trust me. Never in my life have I seen people encouraging others to lie to their doctors about getting the diagnosis that they want.
With diseases like inflammatory bowel disease, this is not something you can fake. A diagnosis is received after scopes, scans, and labs, reflect that this is in fact the case. You don’t just walk into a doctor’s office and say you aren’t feeling well and exaggerate abdominal pain. It’s not a competition of who is “sickest,” people are sharing what they are going through for a variety of reasons. When someone is in a hospital bed, they may share for support, advice, and prayers. When someone is gearing up for a colonoscopy, they may share so they can get tips for easing the prep or coping with the worry of the unknown. When someone is pregnant and flaring, they may share to hear from other IBD moms who have been there before. The examples are endless. Patients are not haphazardly concocting up social media content and lies about their medical struggles to see who is going to get more attention. This is not “attention” people want.
By claiming we share for attention it goes against everything we stand for and belittles the lifechanging work patient advocates are doing to support and comfort their peers. As a patient advocate myself, I do so much behind the scenes “work” to guide those in the IBD community and help them every step of the way. It’s about helping others from the bottom of your heart and being the voice you needed to hear upon diagnosis and through milestones in life. It’s genuinely finding connections with those who are not just strangers on the internet, but quickly become your closest confidantes and resources. Since coming out and sharing I had Crohn’s disease in 2015, I went from having family and friends who didn’t have Crohn’s offering me support, to an army of thousands of members in the IBD family I can rely on who “get it” and are available right at my fingertips. THIS IS PRICELESS.
Sorry not sorry for the “upsetting content”
The article states “thousands of teens are banding together on social media as part of the movement” to support the Spoon theory. Imagine what it’s like to be living this reality versus just having to view a post on social media. Can you pause and put yourself in the hospital bed or on the operating table or on the couch about to do a painful injection and think about the pain and suffering those with chronic illness are forced to endure just to survive like the rest of society? It’s privileged to lash out against those who are doing all they can to show others what their lives consist of rather than bottling everything up—THAT is damaging, THAT is not healthy. Must be nice to have the privilege to keep scrolling and living your healthy life and only see a few seconds on your screen.
Should chronic illness patients be smiling as they’re suffering in hospital beds? Is it not normal to be crying when you’re worried and scared and can’t help but get emotional with all that’s on your shoulders? No one is complaining. It’s the stark reality. It’s heavy. It’s no surprise that more than 30% of people with IBD also deal with mental health issues and anxiety because life with the disease is so heavy.
It’s not about the money
Can we all pause and laugh about the fact the article claims those with chronic illness post on social media for the money. Hilarious. Get a grip. Even as a well-established and trusted “health influencer” within the IBD community, when companies reach out to me, it’s often to try products, not get a paycheck. When I am paid for my advocacy work it’s working diligently like your job as a journalist to write articles, create social media copy, and educate others about what my life is like with Crohn’s. I get compensated like any other human for using my skills and expertise, along with my precious time and energy, to sit on advisory boards and offer input and perspective for marketing and awareness campaigns. My job is not to be a patient, my “job” is to take what I’ve learned and use it to make a difference and help others.
This is not for show. Digging up past medical trauma and flare ups is not enjoyable. If businesses and pharmaceutical companies want to collaborate with chronic illness patients, they should be paying us for our invaluable intel and understanding. The article states patients have adopted “victim mentalities” …wow…and “communities of grievances” … when medical professionals are out of line or treat patients without respect, you better believe your ass they should be called out. How is change going to happen and life for chronic illness patients going to improve if we sit quietly. Be loud, my friends. Don’t allow articles like this to stop you from sharing. We NEED your valid experiences. You deserve to be heard. You matter. Even though the rest of society may be rolling their eyes or trying to stop us, they won’t, and they can’t.
I don’t want to go back to 2005 when I was all alone in my struggles with Crohn’s disease. I want to stay in 2022 when I can post whatever I want, whenever I want about my trials and triumphs as a woman, mother, and wife with Crohn’s disease and not fear judgement. Sometimes I’m thriving, sometimes I’m struggling. It’s vital that those with chronic illness continue to honestly share their stories on social media to provide clarity, education, and connection to those who relate wholeheartedly.
So, dear Emma, from one journalist to another, please start sharing stories that matter—don’t go after stories for attention or follow the adage, “it bleeds, it leads.” Seems like you are the one going after the likes. You should know better.
Sign the Petition
There has been outrage in the chronic illness community about this article—many feeling triggered and upset by the accusations and the claims made about Spoonies. An online petition has been created to have this Daily Mail article taken down—you can sign the petition by clicking here.
They call themselves “Propellers.” They’re a team of volunteers, made up of IBD patients and caregivers who created a non-profit called Propel a Cure for Crohn’s in 2016. They are laser focused on preventing and curing Crohn’s disease and, on the heels of their first research project funded at Stanford University in the world-renowned lab of Professor Mark Davis, they’re now determined to make a meaningful difference through their Roadmap to a Cure for Crohn’s effort. During this month (September 2022), they’re aiming to raise $50,000 to help get their latest project off the ground and to provide a solid foundation to bring their global team together.
This is a grassroots effort fueled by patient and parent volunteers. Patients and caregivers have an opportunity right now to directly influence a brighter future without Crohn’s! This is a peer-to-peer fundraiser—it’s not just about the monetary donations, but also sharing the message with others far and wide. Not only are international researchers involved, there are people all over the globe participating. In addition to the English-language campaign, there are also Swedish and Portuguese online campaigns running as well.
The Patient/Caregiver Perspective
Ildiko Mehes recalls what it was like when her 9-year-old daughter received her lifechanging Crohn’s disease diagnosis in 2017.
“As a parent, a serious diagnosis like Crohn’s is a huge shock, and it’s absolutely devastating and heartbreaking. Even during periods of remission, we are always on high alert and waiting for the other shoe to drop. At diagnosis, my whole world stopped, literally and figuratively. As irrational as it sounds, as a parent, you wish the rest of the world stopped with you to help you address the crisis. You wish that all of modern medicine rolled up their sleeves and urgently worked together to precisely diagnose the problem and bring her back to long-term health.”
As a caregiver, Ildiko has a unique sense of urgency and determination. She feels we need and can do better for IBD patients.
“When an otherwise healthy child, with no prior medical history, suddenly presents with IBD symptoms during a routine winter virus, you ask yourself “what caused this switch to be flipped?” Not having any answers to the underlying mechanism of disease onset or perpetuation, having a trial-and-error approach to disease management, and being forced to consider serious immunosuppressive medications with modest clinical trial benefits feels unacceptable as a parent. This is what drives me.”
As a pharmaceutical executive with more than 20 years of experience, Ildiko uses that unique skill set to go after complex and difficult goals with Propel a Cure and feels a deep sense of obligation to help our community.
“While there is excellent research ongoing in IBD, it happens in silos. It lacks global coordination and a plan. We don’t yet understand many basic things about Crohn’s. We are all just hoping for a “eureka moment” that hasn’t come over the last 100 years. We are continuously enticed with headlines of a “promising” new pathway or new drug candidate, usually in mice. And then that great idea sits there, with no progress made, a decade or more later. I know we can do better,” she said.
Natalie Muccioli Emery was diagnosed with Crohn’s disease in 2011 and she’s also a Propel a Cure Board member. She started dealing with abdominal issues 26 years ago. Being a veteran patient has provided her with perspective about how far treating and managing IBD has come and how far we still have to go.
“Propel a Cure was the first organization whose mission resonated with me. I appreciate their mission to cure Crohn’s Disease, but I even more appreciate the fact that they have laid out a plan as to what the areas of knowns and remaining unknowns are in their Roadmap to a Cure for Crohn’s project. Complex issues like Crohn’s Disease will take a collaborative and systematic approach to address, and this cause has captured that,” said Natalie.
Not only is Natalie an IBD mom, she’s also an IBD aunt!
“I believe that as an adult with IBD, the way I embody the role of a “Crohn’s Warrior” is not for myself it is for the next generation. I have “been there and done all that” with Crohn’s. But just because I did it with Crohn’s doesn’t mean the next generation should have to. I grow increasingly concerned when I see the rising rates of IBDs like Crohn’s in younger people. I believe the rising rates of Crohn’s should create a sense of urgency and a desire for a better future.”
Putting the puzzle pieces together
The Roadmap to a Cure is an ambitious project but one that is needed to drive real progress toward cures and prevention of IBDs, not just talk about “cures” in some very distant future. Ildiko says the brilliant clinicians and scientists she has gotten to know all tell her that getting to a cure will take a grassroots effort, global collaboration, and involvement of patients and caregivers.
“We at Propel a Cure are deeply committed to doing exactly that. The first step in our project is to systematize what we already know about Crohn’s today. We know a great deal, thanks to research. But when we are talking about complex fields like genetics, epigenetics, immunology, microbiology, epidemiology, multi-omics platforms and artificial intelligence, etc. there is no way any one person or group can know everything. We need a large global group of dedicated and brilliant experts to put all the puzzle pieces we already have on one table so we can begin to then put the pieces together,” she explained.
Grabbing the attention of medical professionals and researchers
Propel a Cure grabbed the attention of Dr. Bram Verstockt, MD, PhD, Department of Gastroenterology and Hepatology, University Hospitals Leuven, on social media.
“I truly like the concept of joined forces across various stakeholders, including patients and caregivers. As clinicians and scientists, we can have ideas about how to move forward based on experiences and interactions with patients on a daily basis. However, the next step really is to involve patients actively in many of these projects, as is currently the case with Propel a Cure,” said Dr. Verstockt.
The “Roadmap to a Cure” aims to bring together expertise across many different fields and niches in IBD.
“Over the past decades, a lot of scientific evidence has been generated in multiple domains of Crohn’s disease, so now it’s time to bring all that evidence together and truly connect the dots. Only by doing so, one might unravel knowns and unknowns and highlight where the remaining key gaps are, and we can define the priorities and strategies of how to fill these gaps to significantly advance the field, to improve the lives of patients with Crohn’s disease,” said Dr. Verstockt.
Where the roadmap can take us
After the initial step of putting together the state of the art, the next step is identifying gaps in our knowledge: what puzzle pieces do we still need? The third step is to develop the plan, or the Research Roadmap, to get from what we know today to developing cures and prevention strategies.
“We truly believe in a future where we can prevent and cure Crohn’s and eliminate so much patient and family suffering,” said Ildiko.
The reason this requires a grassroots effort and all of us patients and caregivers to fund it, is that otherwise the current system largely doesn’t provide incentives for new ideas or cures or global collaborative efforts of this magnitude. A recent paper discusses how the same ideas have been funded for decades, with limited progress and that we urgently need new directions.
Ildiko believes the current research incentive model is broken. “If we want true progress and cures for Crohn’s and other IBDs, we need a new collaborative model among IBD foundations/nonprofits, patients, caregivers, researchers, clinicians, and others. I believe this can become a model for other chronic and immune-mediated diseases.”
Click here to watch a video where Ildiko explains the Roadmap to a Cure project further.
Hopes for the future
“I would really like to see more key opinion leaders be brave about acknowledging the risks and limitations of current therapies, avoid putting lipstick on a pig when discussing some newer drug candidates in trials with lackluster results and the same mechanisms, dispense with biased headlines like “safe and effective” when the data is much more nuanced or unclear, and openness to “outside-the-box” ideas, like microbiome manipulation, including via diet, infectious triggers like Epstein-Barr virus in Multiple Sclerosis, vagus nerve stimulation, Fecal Microbiota Transplant (FMT), hyperbaric oxygen, etc. and also adopt routine monitoring via intestinal ultrasound for many patients,” said Ildiko.
As of now (September 12, 2022)—more than $26,609 has been raised!
“I have been overwhelmed by the response so far, as has the entire Propel team. People are really connecting with our mission. We are getting donations from so many states and countries! We have received more messages of profound thanks and hope than I can recount. This fuels us so much,” said Ildiko.
Natalie feels a wide range of emotions each time she sees a donation come in or the campaign shared across social media.
“I go from feeling hopeful, to introspective, to sad. I truly wish we did not have to do this campaign and that in 2022 we knew what the underlying cause(s) of Crohn’s are, and that safe, effective, reliable treatments were available for all Crohn’s patients. But here we are. Crohn’s is still very much part of the lives of patients and caregivers, and we need to take action to change that. I am so grateful for the outpouring of support we have received so far, but there is more work to be done!”
Propel a Cure has virtually no overhead fees or salaries, so every single dollar donated to Roadmap for a Cure goes to research.
“We are all volunteers who work out of our homes. The donations will be put towards collaborative research teams worldwide. Each team will lead a contributing area to the development of Crohn’s Disease (environment, microbiome, immune system etc.) and highlight where the gaps in knowledge remain,” said Natalie.
“The ultimate dream obviously would be to cure and if not, to significantly improve the quality of life for millions of patients worldwide,” said Dr. Verstockt.
Click here to donate to this incredible cause or to join their team.