Traveling with inflammatory bowel disease (IBD) is rarely as simple as packing a suitcase and showing up. It’s logistics, emotions, planning, and flexibility. It takes a bit of hypervigilance. This layered on top of a disease that doesn’t take vacation days. But it is possible. And for many of us, it becomes one of the most empowering reminders that life with IBD can still be adventurous, and rich with new experiences.
This week on Lights, Camera, Crohn’s you’ll hear from two incredible IBD advocates, Kelly Dwyer and Rachel Verbanac. They both open up about their diagnoses, their anxieties, their coping strategies, and their go-to travel essentials. Their honesty and wisdom offer a roadmap for anyone who wants to explore the world without letting IBD call all the shots.
Meet Kelly: 21 Years of Symptoms, 7 Years Diagnosed
Kelly may have been diagnosed with Crohn’s disease in 2018, but she’d been living with severe perianal fistulizing ileal Crohn’s since the early 2000s.
“Before diagnosis, I avoided significant travel whenever possible because I was so ill. And when I did travel, I tried so hard to plan for every single scenario that it became stressful for me and everyone around me.”
Now in deep remission thanks to medication, Kelly still plans intentionally, but the difference is that the planning empowers her instead of holding her back.
She structures trips around:
Her injection schedule
The time of day she flies or drives
What foods she eats before travel
How to pace her energy
And what she needs to stay healthy while surrounded by crowds
“I wear a mask, use sanitizer constantly, wash my hands as much as I can… it all helps me feel like I’m doing what I can to set myself up for success.”
Kelly on Travel Anxiety: The Trauma Stays with You
Despite years of remission, Kelly still carries fear rooted in lived experience.
“I constantly worry about not making it to a bathroom. Even though it has not happened in years, that trauma stays with you.”
Kelly also experiences nausea, anxiety and a whole lot of gas and burbling guts when she travels.
“Finding the right medication cocktail that keeps things calm and in order in my guts (and brain!) took a lot of trial and error, but was worth it for me to find a combination to give me confidence that I’ll feel like I’ve done everything I can to get the trip off on the right foot. I would recommend you ask your doctor or GI about Zofran, anti-anxiety medications in small doses, Gas-x, antacids, and other OTC medications that might help you to make sure they’re safe for you to take.”
She’s built a system that helps her feel confident when she’s traveling:
Depends or heavy-duty panty liners on days she’s unsure
Change of clothes and wipes in her purse, not her carry-on
Imodium and emergency meds ready to go
Small meals before and during travel days
Medication for nausea, anxiety, gas, and gut discomfort
“I had to learn to relax into the chaos of travel and not panic when plans change. Travel is unpredictable—but so is Crohn’s.”
The Power of Protection: Insurance (Both Emotional and Literal)
Kelly is adamant that travel insurance is non-negotiable.
“I have used travel insurance many times for flare-related cancellations. It can be heartbreaking to miss something important, but it’s not your fault. This is your reality, and you’re doing your best.”
She also communicates openly with travel companions, so expectations are clear and compassionate from the start.
“Find as much peace as possible. Asking for everyone’s understanding and compassion, is so important. I remind myself that it’s not my fault that I am unwell. It’s not anything I did to cause the flare. This is simply my reality, and I am trying my very best, even if it doesn’t always work out the way I’d hoped.”
“Treat yourself with compassion, always. Build in extra time everywhere. Your comfort is worth it. Having a few extra hours at the airport to sit and read a magazine is much preferable to rushing through security lines and not being able to use the bathroom before getting on the plane because you’re late.”
Meet Rachel: A Travel-Lover Who Refused to Stop Exploring
Rachel was diagnosed with Crohn’s disease in 2021, right as she was going back to nursing school. Before that, she spent months living a nomadic lifestyle in New Zealand and expected to spend her twenties exploring the world. Her diagnosis meant rethinking what travel could look like. Requiring infusions changed everything.
“Hiking the Appalachian Trail used to be a dream, but with the need for insurance, pharmacy authorizations, infusion clinics, and access to university health systems… that lifestyle just wasn’t realistic anymore.”
But Rachel didn’t stop traveling. She adapted.
How Rachel Travels Now
Rachel describes herself as someone who “packs her anxieties,” but in a productive way.
Her prep includes:
Bringing a med kit stocked with small doses of essential meds
Monitoring hydration closely on travel days
Planning meals and bowel habits ahead of time
Understanding bathroom access in each country
Carrying small local currency bills for paid restrooms
Bringing a letter from her provider outlining her diagnosis and meds
“After many international trips, I’ve proven to myself that how I feel at home reflects how I feel on the road.”
Rachel also buys comprehensive travel insurance that covers pre-existing conditions, often from TinLeg, and encourages others to read the fine print carefully, especially regarding upfront payment rules.
“I feel much more secure knowing all medical bills will be paid for should I need anything abroad. Beyond health insurance, I have used the insurance for trip interruption and costs of delays. I also have my provider write me a letter stating my disease, common side effects, and my current medications. This letter can be useful when seeking care at a new clinic or if TSA should ever give you a difficult time (I have never experienced this). I like having the physical letter in the med kit.”
Bathroom Access: A Cultural Learning Curve
When traveling with others, Rachel gives them a heads up that access to bathrooms is a priority for her. Especially when traveling in Europe.
“Europe often requires a purchase to use a restroom. You cannot just run into a McDonald’s.”
Her strategy?
Plan ahead
Carry cash: Having a few small bills in the local currency is helpful to make a quick sale or pay at public bathroom stations in some countries.
And she always tried to keep everything in perspective, even when the unexpected happens.
“Accidents are embarrassing, but you will most likely never see these people again. It is okay. You are okay.”
Travel Anxiety: You’re Not Alone
Rachel acknowledges the fears that come with IBD, but her message is clear:
Do not let IBD keep you from seeing the world. Start small and your confidence will grow.
She now travels to Mexico annually and cannot imagine winters without it.
Nurse-Approved Safety Tips from Rachel
Some of her favorite reminders:
Even healthy travelers get GI bugs—be cautious with food and water. Taking general precautions like only drinking bottled water in areas where the water might not be safe to drink, sanitizing your hands often, and avoiding touching your eyes and mouth are still the best ways to prevent infections.
Avoid buffet sushi
Choose made-to-order stations
Read resort and food reviews. She checks out Google reviews, TripAdvisor, and Hotels.com to see what people have to say before she books a trip.
Wear an N95 on flights to avoid illness and see if your travel companions will do the same to help keep germs at bay.
Advocate for yourself with travel companions
Read Google reviews quickly if you’re unsure of a restaurant, locals and travelers will share if they got sick eating there. Look for highly frequented places.
As a nurse, Rachel has these words of wisdom for our community, “Don’t let IBD keep you from seeing places and experiencing new cultures. Often as patients we have anxiety and unknown destinations can seem overwhelming and scary. Start small and your confidence will grow, promise.”
Rachel’s Travel Med Kit
She carries:
Doctor’s letter
Hand sanitizer
Tylenol
Imodium
Pepto
Tums
Fiber
Gas-X
Benadryl
Dramamine (also helpful for intense nausea)
Zofran
Liquid I.V.
Band-Aids that are a few sizes
Contact solution or small vial of artificial tears (I wear contact lenses)
A few doses of Dayquil and Zyrtec—when changing the container medication comes in, be sure to write the dose (mg or ml or the number of pills) and how often you take it.
A tube of triple antibiotic ointment and hydrocortisone ointment (for scrapes and bug bites)
Final Thoughts: You Deserve to Experience the World
Traveling with IBD takes more planning, more flexibility, and more courage than most people will ever understand. But as Kelly and Rachel show, it’s possible and it can even become empowering.
As someone who was diagnosed with Crohn’s more than 20 years ago traveling can still make me feel a bit uneasy. I always keep pain medication, Zofran, and Dramamine in my carry on. If you have to pack your biologic medication, keep that on you as well. It’s important to check how long your injection can be out of the fridge. Nowadays, Humira for example, can be unrefrigerated for up to 14 days. If you have to do your injection while away from home, make sure to have alcohol swabs and an ice pack (if you are used to using one).
I never drink caffeine prior to flights or long road trips, and I eat very light until I am at my destination. I try to dress as comfortably as possible, and do not restrict my belly in any way. The moment I get to my hotel room I take off my travel clothes and shower. If you are traveling and feeling symptomatic, it can be helpful to alert your care team at home and also do research beforehand about local hospitals so you have a game plan in place should you be facing an acute flare that may require a trip to the emergency room.
Whether you are taking a weekend road trip or boarding a long-haul flight, remember:
You’re allowed to take up space. You’re allowed to prioritize your needs. You’re allowed to choose comfort over speed. You’re allowed to protect your energy.
And most importantly:
You deserve to make memories that reach far beyond the walls of your disease.
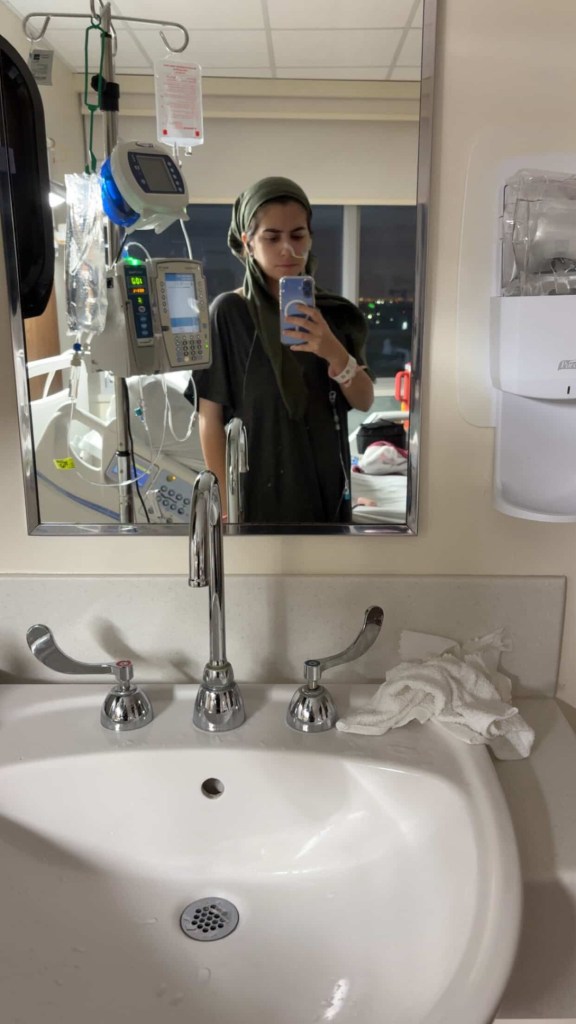
When you live with Inflammatory Bowel disease, there’s no telling if or when you’re going to need an NG tube (nasogastric tube) to help stabilize your symptoms, deliver nutrition, and help your body heal. In my 20-plus years living with Crohn’s disease, and despite many hospitalizations for bowel obstructions, I have never needed one (yet). Recently, a fellow IBD mama on Instagram shared about getting one as she’s hospitalized right now (with a new/additional diagnosis-Gastroparesis), and her experience inspired this article.
This week on Lights, Camera, Crohn’s, a guide that breaks down what to expect, what helps, and how we can best cope from fellow patients and caregivers who have lived through it. Whether you are facing your first tube placement or supporting someone who is, the fear of the unknown can often feel bigger than the procedure itself.
Understanding the Process (and Why It’s So Intense)
NG tube placement can feel overwhelming because it involves an extremely sensitive area: your nose, throat, and gag reflex. It is quick, but not exactly pleasant. Knowing what is coming can dramatically reduce anxiety.
An NG tube is typically used for:
Bowel rest and decompression during IBD flares
Relieving bowel obstructions
Nutrition support
Medication delivery
And while the experience varies widely, preparation and honest communication with your care team make a huge difference.
Before Placement: Preparing Your Mind and Body
Ask for numbing options: Most hospitals can use lidocaine spray or gel in your nostril to make the initial insertion more tolerable. It is worth requesting.
Practice slow breathing: Focusing on deep, steady inhales through your nose helps decrease the gag reflex and keeps your body relaxed.
Sit upright with your chin slightly tucked: This position straightens the path the tube travels and can make the process smoother.
Have emotional support: Whether it is a partner, parent, friend, or even someone on speakerphone, having a familiar voice can ease anxiety.
During Placement: Strategies That Actually Help
Swallow as the tube advances: If the nurse allows, sipping water and swallowing as the tube moves downward helps guide it into the esophagus rather than the airway.
Anchor your eyes on one spot: A visual point of focus reduces the instinct to pull back or panic.
Choose a mantra: Something like “This is temporary” or “Every swallow gets me closer” can center your mind.
Ask your nurse to narrate the steps: Knowing what is happening and when it will be over prevents surprises and makes the process feel more controlled.
What Patients and Caregivers Have to Say
Hindy: “I would say to request the thinnest tube possible. It is really awful.”
Ashley: “It’s a horrible experience. I’m glad I didn’t know what to expect before getting one placed, because I don’t think I would’ve been able to handle it. I don’t think there’s anything that could have prepared me for it.”
Amy has IBD and her four-month-old daughter does not, but she has had an NG tube for two months, due to issues with strength, stamina, and desire to eat after being born prematurely.
“She was diagnosed with Failure to Thrive, and her NG tube has been lifesaving! I can guarantee she gets the nutrients she needs to grow and thrive. She tolerates the NG tube very well. She has pulled it out multiple times, but thankfully we live close to the GI clinic and a great Children’s hospital.”
Amy has found there are certain strategies to limit the number of times she pulls the NG tube out, such as taping it closer to her nose. She says it can be stressful at times, but luckily with her medical background she knows how to clean the tube 8 times a day. Even though her daughter has handled the NG tube like a champ, Amy and her husband have decided to transition to a G-tube, since their baby girl will need nutritional support for a little bit longer, which Amy thinks will aide in comfort and speech development.
Alexis: “Get a little white board so that you can write what you want to say as talking is so uncomfortable.”
Karen: “Taking anti-anxiety + pain medication to help with the uncomfortable pain and anxiety that NG’s cause. I refuse NG tubes now without serious meds, the trauma, pain, and discomfort they cause must be treated and I think providers really underestimate how traumatizing it is to have one, especially if it’s put in while you’re awake.
Amanda: “Ask for some nebulized lidocaine before insertion.”
Abbie: “Ask for throat numbing spray!!! I was given it my first time and then every other time I’ve had to ask, but I’m so appreciative the first nurse I had gave me some so I knew to ask for it in the future.”
Sarah: “I didn’t even know what an NG tube was until it was already inserted. I suppose the shock of how quickly the insertion went shielded me from the pain and discomfort. Numbing spray was the only way I could cope with the tube irritating my throat. Mine was in for three days while I had a bowel obstruction and the day it came out felt like FREEDOM.”
Becca: “They are the f***ing worst. You can quote me.”
Melissa: “I had one they put in while I was awake and after SIX tries, I was adamant on getting something to relax me. They put a little something in my IV and then it went down without an issue. I also had a smaller one, more child-sized than adult.”
Dana: “I wish I had something positive to say about NG tubes, frankly I didn’t cope at all until they gave me Ativan and eventually a muscle relaxer. Sometimes they can give you a numbing throat spray to help with irritation. After the first few days, it gets little more tolerable as your body gets used to it.”
Jennifer: “OMG. 26 years with Crohn’s and nothing traumatizes me more than the mention of an NG tube. I was about 95 pounds the first time I got one. I’m almost 5 feet tall, and after two tries of me not being able to breathe they realized I needed a child-size tube.”
Mayara: “When I had my NG tube, I used to suck on ice chips/cubes to help ease my sore throat.”
Claire says she’s been through the wringer with NG tubes. There was a point where she had 10 in one year!
She says, “Regardless of how awful NG tubes are and the damage (long or short term) they can do, they have saved my life repeatedly. I am no stranger to bowel obstructions. Developing strictures seemed to be a favorite past time for my small intestines. The NG tube is supposed to decompress the obstruction and stop or at least reduce the amount of vomiting (also helps to prevent aspiration). I will never forget how nervous I was before my first NG placement and even now as an NG vet, I still get very nervous. I always ask the doctor for IV Ativan or IV Valium beforehand.
Claire also says even if a doctor does not want to give a benzo after an opiate that they will usually give her a dose right before placement.
“Don’t be afraid to ask for what you need. I also won’t sugarcoat it; you will most likely gag and vomit during the placement. Ask for an emesis bag or basin. It sounds counterintuitive, but if the nurse doing the placement is experienced, they will be able to utilize you gagging/vomiting to get the tube in faster. Nosebleeds are also very common.”
After NG Placement: Getting Comfortable
Secure the tube well: Do not be shy about asking for gentler tape, extra adhesive, or adjustments. A well-secured tube is less irritating and less likely to tug.
Soothe nasal irritation: Saline spray, warm compresses, or a tiny amount of water-based lubricant around the nostril can reduce soreness in the first day.
Experiment with sleeping positions: Many find sleeping slightly elevated or on their back with a supportive neck pillow helps keep the tube comfortable.
Be comfortable: Wear loose tops, zip-up hoodies, or scarves if you want to conceal the tube and prevent snagging on straps or bags. Obviously, many people are choose to stay in their hospital gown.
Protect it in the shower: A bit of cling wrap or a small waterproof dressing keeps the tape from falling off.
Move with intention: Sharp head turns or bending forward quickly can tug the tube and cause discomfort. Slow and steady helps.
Support for Caregivers: What Helps Most
As a caregiver, it can be easy to feel helpless on the sidelines as you watch your child or a loved one or friend go through this. Here is how you can help ease that burden:
Watch for tension or kinks: If the tube starts pulling, the patient may feel nausea or pressure.
Track symptoms: Be mindful of any changes you may notice with coughing, reflux, or fullness. This can mean the tube has shifted.
Learn how to flush the tube: If this is a long-term situation, educate yourself so you can help prevent blockage and avoid urgent care visits.
Offer emotional space, not pressure: Let your loved one set the tone. Everyone is different. Some want distraction, others want quiet, some want humor. Follow their lead. You know them best, trust that instinct and know that even if they may seem frustrated or short, that anger is not geared towards you, but rather the difficult circumstance and situation they are enduring.
The Emotional Side: What We Don’t Talk About Enough
Having an NG tube can stir up fear, embarrassment, frustration, sadness, or anger. All these feelings are normal.
Many patients say:
They feel “less like themselves.”
They are worried about how they look.
They are afraid to sleep.
They are overwhelmed by the sensation of the tube at first.
These feelings tend to ease within 24–48 hours as the body adjusts. Give yourself grace. This is a medical tool, not a reflection of strength, identity, or dignity. It is ok to feel all the feelings.
Celebrate the small wins
Take this one like you do with all things IBD. Give yourself credit where credit is due! It is not easy and it is important to celebrate all the wins, no matter how “small” they may seem. You are making strides and growing through this journey, whether you realize it or not. What you are experiencing matters and your resiliency deserves celebrating!
The first time you swallow without noticing the tube
Sleeping through the night
Getting out of bed more comfortably
Tolerating feeds or feeling abdominal relief
When to Call Your Care Team
You may wonder what is “normal” and what deserves pushing the nurses light or alerting your care team. You should reach out immediately if any of the following happen:
You have trouble breathing or persistent coughing
The tube appears to be slipping out
There’s significant nasal bleeding
You feel intense nausea or vomiting
The tube becomes clogged and flushing does not help
You should never hesitate to call. NG tubes are temporary but important, your team expects questions. Classic example of better safe than sorry. You are not a burden to anyone.
Final Thoughts
An NG tube can feel intimidating, and while extremely unpleasant, they can help give you some relief while allowing your doctor to keep finding answers for you. With preparation, the right coping strategies, and the support of a caregiver or medical team, you can make the experience more manageable. Always remember you are never alone in your fears and setbacks and that your ability to cope and your voice matters.
It is an exciting and transformative time for the IBD community when it comes to family planning and pregnancy. For years, patients and providers faced uncertainty and conflicting guidance about everything from fertility to medication safety. Now, with the publication of the Global Consensus on IBD and Pregnancy, we finally have a unified, evidence-based roadmap created by leading experts worldwide.
This groundbreaking research, jointly published across multiple top journals, is more than just a collection of data—it’s a lifeline for patients, caregivers, and clinicians seeking clarity and confidence. And for the first time, that guidance comes to life through a series of 12 videos now available online. As the sole U.S. Patient Ambassador and Group Lead for patient advocates worldwide, I was honored to contribute not only to this historic project, but also to share my own journey in the video series—bringing the patient perspective directly into the global conversation.
Grateful for Dr. Uma Mahadevan and the entire team for their incredible work on the Global Consensus.
Check out the video series
Following the release of the research from the 2025 Global Consensus Conference on IBD, a series of 12 videos were also published on the PIANO (Pregnancy in IBD and Neonatal Outcomes website), featuring experts speaking on best practices, emerging data, and consensus statements.
Among those 12, my Patient Perspective video is unique. It’s the only video in the lineup where you hear firsthand experience from an IBD mom. During my unscripted 18-minute video, I share openly about the tough decisions I faced personally, the hopes and worries I encountered while bringing babies into this world, and what I want fellow patients and doctors to know. As an IBD mom of three kids (now ages 8, 6, and 4) who were all exposed in utero to Humira, I have a unique perspective to share.
I know what it’s like when you’re 32 weeks pregnant and have to do a biologic injection while you see your baby’s foot kicking at your belly. I know how stressful it is when you don’t know if you’re going to flare while pregnant or shortly thereafter. I know how complicated and overwhelming it can feel when you’re juggling a chronic illness along with pregnancy and motherhood.
Having a patient video placed alongside expert commentaries is a statement: our lived experience is essential to understanding how guidelines work in the real world. I hope my words leave you feeling seen and empowered.
Preconception Counseling and Contraception for Patients with IBD
The Patient Perspective
Why These Videos Matter
Each video is a piece of a bigger puzzle. Together they tell a story about where we are now, where we need to go, and how patients can be—and must be—central to that journey.
Bridging gaps between patient, clinician, and researcher. These videos are designed not just for patients, but for caregivers, physicians, policy makers, and anyone interested in improving IBD care. Seeing things through the patient lens can spark better communication, more empathic care, and guidelines that address what matters most.
Empowerment through shared experience. Whether it’s coping with symptoms, navigating treatment decisions, or facing uncertainty, this research will make you feel more confident in every decision you make along the way. Rather than feeling like there’s an overwhelming amount of gray area, you can see the roadmap of decision-making created from the Consensus that will help you each step of the way.
How to Watch & What To Do Next
Watch the videos: Listen firsthand and educate yourself. An educated patient is an empowered patient. It’s one thing to read a published medical study, it’s especially helpful to see these videos and watch the research come to life.
Join the conversation: Use these videos as conversation starters, take what you learned into clinic visits, have conversations with your partner/family/friends, or on social media. When you’re talking about family planning, make sure your GI and Maternal Fetal Medicine doctors are aware of the Global Consensus on IBD and Pregnancy to ensure they are up-to-date on the very latest research.
Join the PIANO study. This is a great way to become a citizen scientist and use your journey to motherhood as a way to pave the way for others. I participated in PIANO with my youngest child, and he will continue to be “followed” until age 18. It does my heart good to know we’re helping bridge the gaps in understanding so women with IBD now and in the future can feel more comfortable about staying on medication in pregnancy and during breastfeeding.
Too often, patient voices are an afterthought or an add-on. Being featured as an integral voice, not a sidebar, is a powerful shift. The fact the Global Consensus Conference team made such a point to incorporate patients like myself who are IBD moms, from around the world, goes to show just how inclusive and comprehensive this research is.
Final Thoughts
Living with IBD means navigating uncertainty, physical challenges, and emotional strength, but it also means being part of a community that continues to push boundaries in care. These videos highlight not only the science and data, but the lived realities that bring those numbers to life. Patient voices don’t just complement medical expertise, they help shape the future of care. By placing my perspective alongside global experts, the Consensus reminds us that guidelines are most powerful when they reflect both evidence and experience.
As an IBD mom, I think about what this progress means for my three children and for the next generation of families impacted by this disease. I volunteer my time and energy for these projects because they are at the heart of my patient advocacy and genuinely matter so much to me. The inclusion of patient voices today paves the way for a future where no one feels alone in their decisions about pregnancy and IBD. Together—patients, clinicians, and researchers are building a roadmap that will make the journey clearer, safer, and more hopeful for those who come after us.
Living with Inflammatory Bowel Disease (IBD) often means juggling more than one health condition. For some, that includes managing Attention-Deficit/Hyperactivity Disorder (ADHD). Both conditions can significantly impact daily life, and when it comes to treatment, it’s important to understand how ADHD medications may interact with IBD and its therapies. This week on Lights, Camera, Crohn’s we hear from more than 25 people who are juggling both and share their impactful advice.
The Overlap Between ADHD and IBD
While ADHD and IBD are separate conditions, research shows that people with chronic illnesses, especially those that begin in childhood or young adulthood may experience higher rates of ADHD or ADHD-like symptoms. Brain fog, fatigue, and difficulty concentrating are also common in IBD, which can make it challenging to distinguish what’s driving certain symptoms.
For those diagnosed with both conditions, ADHD medications can be life-changing, improving focus, energy, and daily functioning. But because IBD involves a sensitive gastrointestinal (GI) system, it’s important to weigh the potential effects ADHD medications can have on digestion and disease activity.
Appetite suppression: Stimulants often decrease appetite, which may be concerning for IBD patients who already struggle to maintain weight or adequate nutrition.
GI side effects: Nausea, abdominal pain, and diarrhea can occur, sometimes making it difficult to know whether a flare or medication side effect is to blame.
Sleep disruption: Poor sleep can worsen IBD symptoms and overall inflammation. Timing doses earlier in the day can help.
Slower onset: These may be less likely to cause GI upset but can take weeks to become effective.
Potential side effects: Constipation, abdominal pain, and fatigue are possible, which can overlap with IBD symptoms.
Impact on Gut Motility
Both stimulant and non-stimulant ADHD medications can influence gut motility (how fast or slow food moves through the digestive tract). For those with Crohn’s or ulcerative colitis, this may complicate symptom management, particularly if diarrhea or constipation is already a challenge.
Key Considerations for Patients with IBD
Collaborative Care is Essential Make sure your gastroenterologist and psychiatrist (or prescribing physician) are aware of all your medications. This helps prevent drug interactions, especially if you’re on biologics, immunosuppressants, or steroids.
Monitor Nutritional Status If stimulants suppress appetite, work with a dietitian to find calorie-dense, IBD-friendly foods and snacks that can help you maintain strength and body weight.
Track Symptoms Carefully Keep a journal noting when you take your ADHD medication, what you eat, and how your GI symptoms present. This can help differentiate between medication side effects and IBD flare activity.
Adjusting Doses and Timing Sometimes, smaller, or extended-release doses can reduce side effects. Timing medication with meals or adjusting when you take it can also ease GI discomfort.
Mental Health Matters ADHD itself can heighten stress and anxiety, which are known triggers for IBD flares. Finding a treatment balance that supports both brain and gut health is critical for overall well-being.
An IBD mom and therapist shares her advice
Sammi is an IBD mom who works as a therapist. In her experience, both personally and professionally, she has valuable input to share about taking ADHD medications when you have Crohn’s or UC. Sammi took a low dose of Adderall (5 mg, sometimes 10 mg) in graduate school for her anxiety and ADHD.
“My appetite was extremely impacted I’m sad to say. I did not feel hungry until my stomach was physically giving me intense hunger cues. I was only a couple of months into Humira at that point so I too, was struggling with maintaining my weight and didn’t want that to be impacted.”
Here are a few things Sammi did to make it manageable:
1. ALWAYS eat before you take ADHD medications. Eat a big breakfast, if possible, protein and carbs (if you can tolerate generally, of course). As a therapist, many of my clients struggle with taking meds early enough at times. And inferring a good meal ahead of time can feel like a barrier so I just want to hold space for that. However, it is so imperative to be really fueled and in a good place stomach wise / eating wise before taking for the day.
2. Plan your meals out as much as possible. Since hunger cues were lessened for me, I was in the mood for nothing. So  it would be hard to decide what I was going to eat, and then I would not have to decide when I was feeling fatigued and overwhelmed.
3.Snacks are clutch. I say snacks because sometimes that’s just the easiest thing to eat, especially when you don’t want to think about food or you’re not actively thinking about food because your appetite is suppressed. I have Crohn’s disease and one of my biggest triggers is my stomach getting too empty whether it’s because I’ve waited too long to eat or I haven’t eaten enough that day. It will give me such a bad stomachache so that was happening to me pretty frequently when I first started taking the Adderall.
4.Take your ADHD medicines early in the day. This is my BIGGEST piece of advice and clinical recommendation for anyone who is considering taking ADHD medication. Take it early in the day so your sleep isn’t impacted. As we know with IBD- sleep can already be difficult this is so important!
More from the patient community
“My advice is to take it early in the morning so that you can eat more in the afternoon and evening. I don’t have a problem with dropping weight; I had the problem of retaining! Transparently, now I’m on GLP-1 (GI approved) medication, and I’ve lost 38 pounds. Best I’ve ever felt! But, when I take my Adderall too late in the day, I don’t eat and that’s not good either. I take my ADHD meds twice a day, as prescribed. Once at 7 am and once around noon.”
“I have IBD, and I currently take Adderall for my ADHD. I have been on it for a few months, and in my experience, my biggest issue is that it suppresses your appetite for quite some time. I’ve been struggling to gain weight for awhile due to my IBD, so taking something that makes it hard for me to eat all day has been a big challenge. I am thinking about asking my doctor to switch me to a new treatment plan to hopefully find something that doesn’t suppress my appetite!”
“I feel like it never affected me very much with eating and I don’t think there was any interactions between anything with ADHD meds and my UC!”
“I’ve heard fellow moms with kids on these medications recommend eating a big breakfast before ADHD meds kick in, having a snacky lunch, and a late dinner after they wane.”
“There are non-stimulant ADHD meds. Stimulants are the ones that suppress appetite. You can ask your doctor about these and ask to start on the very lowest possible effective dose, if stimulants are required.”
“I don’t take ADHD medications now, but in college I did. I did not find it impacted anything with my Crohn’s. Depending on the ADHD med, it could impact appetite but didn’t interfere with how I manage my IBD.”
“I’m on mental health meds for anxiety and depression, along with ADHD meds, and I do think I’ve had a slight decrease in appetite. I also naturally have a lower appetite than most. A family friend of mine has been on Ritalin for longer than me, and I think he has struggled more in that aspect than I have though.”
“I have a j-pouch with a post-pouch diagnosis of Crohn’s, and I take Vyvanse for ADHD. I take 30 mg a day, I don’t feel like it impacts my appetite at all.”
“I take stimulants for my ADHD, and I don’t have any decrease in appetite. It just depends on the person.”
“The best advice is eating a big breakfast, having snacks for lunch, and then eating a big dinner. I have also reached out to my Crohn’s dietitian to have more creative ideas for small meal ideas! The issue with choosing what medicines is that they all aren’t covered immediately—I’m starting on Adderall, which is one of the suppressants—my doctor doesn’t plan to keep me on that long term, but due to insurance, I have to start there. I have also have to find out what exactly is covered and is not covered (as IBD patients we’ve been there before, right!?)”
“I have Crohn’s and just started to take Vyvanse about two months ago. Even on a low dose, while also being on a high dose of prednisone, I’ve had little appetite. It has helped me to eat something small as soon as I’m able in the morning, before taking the medicine. It helps me have more of an appetite throughout the day, though I have smaller meals now.”
“I have Crohn’s and ADHD. I take an extended release 10 mg Adderall and find that my appetite is fine, a little less, but not dramatically so. I hadn’t really thought about it until my GI went through my meds. I have found that if I take 20 mg (we played around with the dose to find which works best), I do experience a loss of appetite. I think if you can find the therapeutic dose, it should be ok! I’m just a case study of one, but I would also add that ADHD meds have the benefit of supporting healthier time management skills, so I’m more inclined to stop and eat, which my scattered self sometimes didn’t do.”
“I don’t take my ADHD meds every day, but I take Vyvanse and when I do take it, I notice appetite suppression, but it’s nothing severe. I don’t have a j-pouch or struggle with being underweight. When I take them, I usually notice mid-day appetite suppression the most. I tend to eat breakfast before it’s fully kicked in and the effects have waned by dinner time.”
“I have been on Vyvanse, and it has been the best on my stomach and ADHD. I was diagnosed early this year. I tried Adderall, and it made me anxious and over stimulated. Concerta had me nauseated all day, everyday…Vyvanse is the way to go!”
“I have been on Ritalin for the last 2.5 years (finally) and even started an anxiety med that also helps with my chronic pain.”
“I’m on 10 mg of Focalin for ADHD and on Imuran (max dose), Entyvio infusions, and other meds for anxiety and depression. I never had a big appetite regularly, so I haven’t noticed a big difference. The benefit for me has been that I am calmer now and don’t get that ADHD stress. I’m 45 and was just diagnosed with ADHD last November. I’ve had Crohn’s since age 14 with many surgeries between then and 2022.”
“I have IBD and take ADHD meds. I never had the lack of appetite side effect, so I might be an outlier. I usually eat breakfast before taking my pills. Sometimes I need to set timers to eat though if I’m hyperfocusing.”
“I recommend keeping snacks in view. If you don’t feel like eating, drink a protein shake. My Crohn’s symptoms improved a bit with ADHD meds, too.”
“I can’t speak to the loss of appetite, but I was diagnosed with ADHD a few months ago. I tried Adderall for three days, but each day it upset my gut. I had way more bowel movements than normal, even though I was not flaring, and my gut was sore after each one. So, I stopped taking the Adderall and everything went back to normal. I’ve just been self-medicating with caffeine ever since.”
“It helps to eat when you take your ADHD meds and then eat smaller meals throughout the day. It’ll make you not thirsty, so make sure you’re mindful about hydrating. I recommend taking little breaks from it, during weekends and things.”
“I just started my ADHD medications again post-baby and have noticed a huge drop in appetite. I tried a few different meds before settling on extended-release Ritalin. I will say immediate release Adderall severely exacerbated my Crohn’s and gave me horrible stomach cramps. The stomach cramp thing is common with that one, even if you don’t have IBD.”
“I stopped my ADHD medication. It absolutely destroyed my belly. They are a stimulant and make you go to the bathroom more an also affect blood flow to the colon. It’s been awful.”
“Personally, it’s never been enough to make me lose weight. But I do tend to front load—eat my biggest meal in the morning. Also, the come down from stimulants will have you ravenous by the end of the day.”
Finding the Right Balance
Every person’s IBD and ADHD journey looks different. What works well for one person may not for another. The key is to be proactive, keep your healthcare team in the loop, and advocate for adjustments when needed.
Managing IBD is already a full-time job. Adding ADHD into the mix can feel overwhelming, but with the right treatment plan, many people find that their ADHD medications not only improve focus but also help them feel more in control of their health overall.
Whether you’ve experienced one colonoscopy or 20, you know the process is far from enjoyable. This past week while scrolling through Instagram I came across a story an IBD caregiver posted as her young daughter prepped for her scope. During the video she explained how her husband rolls dice, and whatever number it lands on is how many sips their daughter has to take of prep. I was amazed at this brilliant trick to ease the struggle of getting the prep down, and it inspired me to dig a little deeper and ask the IBD community what their “tips and tricks” are.
This week on Lights, Camera, Crohn’s read firsthand advice from caregivers and patients of all ages. My hope is that you find comfort and maybe even a new idea or two to make your next prep a little less stressful.
Firsthand advice for pediatric IBD caregivers
Mara’s daughter has IBD and has already been through eight colonoscopies in just five years. She says the dice game was a huge success for their family the first time around:
“She was at the perfect age for a little competition as motivation with a reward at the end for the winner…of course she always won. It was honestly so easy to prep her I was shocked.”
However, being NPO (derived from the Latin saying ‘nil per os’ or nothing by mouth/no food or drink) after midnight was NOT easy.
“There were lots of tears and anger directed at us. We bought her a special blanket and stuffed animal, which helped diffuse some of that anger.”
As many caregivers know, every prep is different. Mara recalls their second scope being much more difficult, requiring hospitalization and an NG tube after her daughter couldn’t keep the prep down. Now, they focus on giving their daughter as much autonomy as possible, letting her choose flavors, snacks, and activities.
“On prep days or days, she must be NPO, dad and I also follow that diet. It gives her a sense of belonging and that we are struggling right alongside her. We’ve done it for all eight scopes, and we will continue to do it if she needs us to.”
Over time, Mara says they let their daughter lead as much as they can. They give her a “yes” day.
“Whatever she wants (within reason) to eat or drink. Gummy bears, sure. Popsicles, sure. Want to try to mix three different Gatorades? Why not? She wants to watch TV while she preps or play hockey, absolutely.”
Emily’s Family Emily has three daughters with IBD (now ages 9, 12, and 15) who’ve been doing preps for over a decade. Their youngest had to prep for a scope when she was only 21 months old. Their top tips include:
Only prepare 8oz of the drinking mixture at a time. With MiraLAX prep, we let them pick a new flavor to mix each 8oz.
Think outside the box with the liquids for MiraLAX! One preferred water once! (With other electrolyte drinks that day.) One daughter does her whole prep with tea and chicken broth. (Add MiraLAX after the liquid is warmed.)
Use distraction!! This is our biggest piece of advice. We surprise the girls with a new activity the day of prep. They know there will be something fun to do – just not what it is. We have gotten Lego sets, multi-step craft projects, etc. We pick something that we can partition up and give them one part at a time in celebration for ounces drunk!
Keep them active. We have found that the girls tolerate the large amounts of liquids better if they get up and get moving! In the warmer months, they go walk laps around the driveway between cups of the prep.
Pick the “fun” liquids together ahead of prep day. Since they normally cannot have juice or soda, they pick out a few drinks that they are excited to have. This helps them to drink more, once the MiraLAX prep is complete.
I set timers for myself for the day of prep for every 10 mins or so. Just to check in on their drinking. It’s easy to lose track of time and accidentally go 30 mins (or more!) without drinking.
Pack a bag of supplies for the scope day. We always take extra clothes and baby wipes for any accidents. Games/books/crafts are great to keep the girls distracted during the wait before their procedure time. We take some water/light snacks for afterwards. (Check with your providers to see what/when your child can eat afterwards.) Chapstick is always requested by mine now too.
Remember that you can speak up and (nicely!) ask for what your child needs to make them comfortable. For example, at our hospital, the kids usually get their IV’s after they are sedated with some gases through their breathing mask. This is great to avoid needle anxiety for many kids. However, mine have taken a dislike to the masks and the smell of the gas. Since they get regular med infusions, they prefer to get their IV’s back in the holding area and then use the IV for their sedation to sleep. While not the normal procedure, the anesthesiologists and nurses have kindly worked with us to do it the way my kids prefer.
Cindy’s Perspective Cindy, mom to a teenage daughter with Crohn’s disease, says scheduling scopes early in the day is key. Even if you have a teen who likes to sleep in, sleeping in is worth nothing if you already feel like crud due to the prep. She emphasizes advocating during IV placement and following your gut as a caregiver:
“A parent’s intuition of how much is too much comes into play, and you’ve got to listen to that voice. Tell the nurse you (parent and child) did your best to complete as much of the prep as possible. If you can’t finish it to a T, they can still make it work. They know they are working with a child. If they are having trouble placing an IV, advocate for your kid. Give them two tries and then request another person to try. We’re still traumatized from watching them work for 10 minutes to get an IV into my dehydrated and scared 9-year-old, and I think that trauma will live with us both forever.”
She also believes in being honest with your child without over-preparing. Start the conversations when it’s time, but don’t talk about it for days or even hours beforehand.
“This is not going to be fun, and it won’t feel good. But I know you can do it and we are going to do it together because I will be beside you every step of the way. Here are the steps we will take and outline them in age-appropriate detail. Let’s think about how amazing this is going to be once it’s done! This is our focus for the next 24 hours… that moment when it’s done… that will be the best! As soon as you are done at XYZ time tomorrow, we can celebrate and go back to normal life, and you can eat whatever you want.”
Additional feedback for pediatric patients
“For pediatric prep, popsicles are necessary. Blue popsicles allow kids to “poop blue,” which many like. The Gatorade with the MiraLAX is the easiest for them to get down. We tried magnesium citrate once and it was a disaster. Gatorade is where it’s at. Also, we make it a party. Popsicle party. Jokes and TV while pooping. Anything to keep the mood light.”
“Turn the ordeal into a scavenger hunt by completing parts of the prep with small stickers to earn up to something whether it be completing a picture or something to distract when prep is working.”
“My daughter’s first prep at home didn’t go well, but prep while in-patient thru NG tube really worked.”
“If the hospital or your GI team has a Child Life specialist, they can send prep books to families ahead of time so they can help prepare kids for what to expect the day of the procedure.”
“Bribes! Lots of bribes! New toys or games. Legos keep little ones busy. Family doesn’t eat in front of them. Lots of snuggles. Clear your schedule to spend time with them. For young kids, put all food out of reach or lock the pantry so a hungry little one doesn’t get into something they can’t have and make you have to cancel the procedure, which is always my fear!”
“I have a prep approved Starbucks order—Mango Dragonfruit refresher, Venti, no ice, no Dragonfruit fruit inclusions, peach juice blend, in my personal cup … I like to line up cups so I can visually see how much is left and removing one feels like an accomplishment. A seasonal suggestion is using an advent calendar and dividing prep by 24 and opening one door after each one…just make sure the prizes are not food!”
“Arts and craft activities and projects can be a good distraction. Recently gave a sensory art bin to a VEO-IBD patient through their first scope as a kid it helped me to have new things to do.”
“My mom fasted with me when I was doing the prep as a kid! My tips now as a mom myself are to make Jello without Red 40. Ramen seasoning dissolved in water tasted way better than broth to me as a kid…I know that’s not good for you. I would make it a fun and relaxing day, so your kiddo is distracted. I would recommend not watching TV or YouTube because there are so many advertisements for food everywhere and it didn’t help distract me much. I advise having a movie marathon instead!”
“We didn’t eat out much when I was a kid, so eating out with my parents only was a big treat for me to look forward to after starving the day before! Back in the day, GIs used to do a combination of drinkable prep and suppositories for pediatric patients, and I’m glad my mom did the suppositories for me because it was not something else you had to drink. Ask pediatric GIs about low consumption prep so your child doesn’t throw up.”
“When I was a pediatric patient, my mom took me to the store to pick out different drinks for the mix, Jello flavors, etc.… which would make it fun picking it out myself and this also gave me a sense of control in a very out my control situation. My mom always fasted with me, which I appreciated not feeling alone in it. I was also able to pick the restaurant to go to after for something to look forward to!”
“Have your child drink their prep in a fun container., a Disney theme with a silly straw. For adults, use a wine glass or fun mug. Cheers!”
“My 12-year-old just had their first colonoscopy. As a Crohn’s patient myself, I have done one every other year for 25 years and it was hard to watch him go through it. He was tougher than me. The hardest part was him not eating! He had to do a full two days of clears only—per our doctor’s recommendation. That’s my hack as an adult, too. I start taking a Dulcolax dose and not eating a day or two earlier than recommended. You only have to drink the drink until it’s clear in the toilet. The milder/longer prep is easier on me and saves me drinking half the magnesium citrate drink.”
“My daughter couldn’t get any of the prep down at age 16 and by this summer, at age 19, she felt ready. This time we tried over the counter prep of MiraLAX and Dulcolax. The doctor said if she did it this way, she would need to fast for 48 hours instead of 24. She was fine with that. She started taking a couple of Dulcolax tablets at 5 pm the night before. Then, we put half a bottle of MiraLAX into Sprite. She drank a cup every 10 minutes until it was gone. We did the same thing a few hours later. She was clear before going to bed at night. It was easy and stress-free for her.”
“My parents would set me up with my iPad for movies, a desk chair, and a blanket in the bathroom so I could go back and forth from the toilet easier.”
“Make MiraLAX with white grape juice instead of Gatorade! Drink with a fun straw so you can put it on the back of your tongue and taste less. Put on headphones with loud music to distract your sense from the taste so you can drink the prep faster.”
“I confirmed with my child’s GI that colorless cotton candy is a clear liquid! Obviously in moderation, but this could be super helpful for kids and adults who need a different texture than liquid or gelatin.”
Prep Hacks for Adult Patients
Our IBD family had plenty of creative hacks for adults, too:
“The MiraLAX + Dulcolax prep hands down!! I’ve tried them all, and it’s tasteless and easiest.”
“Lemonheads or lemon jolly ranchers RIGHT after you get done drinking a dose!”
“Gummy bears and lifesavers! I love having stuff to chew. I also had pickle juice shooters, which gave me some salty/sour taste to balance all the sweet stuff. I also keep my schedule open for the remainder of the day and allow myself to relax.”
“I put my Suprep in the fridge (even though it says not to) and it makes it SUBSTANTIALLY easier to drink (and doesn’t seem to make it less effective in any way). I also buy myself a new book to read or save a special TV show episode, so I have something to look forward to when I’m drinking prep at 2 in the morning. Colonoscopies are miserable and until they figure out how to make them a nicer experience, it’s great to team together to gather the best tips.”
“Clear Gummy Bears!! This keeps it fun for all ages! Here’s a recipe!
“Drinking chicken broth throughout the day. This gives energy and takes away the bad taste of the prep drink. As a kid, my sister used to make a colonoscopy prep kit. Every 8 oz. I drank; there would be a little gift or activity to do. For example, after the first 8 oz., I got a nice bottle to drink the rest from. The next thing was a Lego kit or a paint by number.”
“I begin my prep four hours ahead of their suggested time, so I can sleep through the entire night. Getting up in the middle of the night, especially for children to complete round two of the prep is just borderline inhumane. What a nightmare. The catch is waking up and hydrating with enough water before the anesthesia cut-off which requires not to drink anything 2 hours before the procedure.”
“Wet wipes and diaper cream are super helpful!”
“A lot more MiraLAX than the prescription prep. And gummy bears (except red ones) are a gamechanger. They let you feel like you’re eating, but they liquify in your gut.”
“Rotate flavors and get some protein through broths. Have broth, then 2 hours later do Jello or change the texture and taste, then 2 hours later do broth and rotate.”
“Strain chicken noodle soup to just have the clear broth, it has more sodium.”
“Avoid eating vegetables/fruits/seeds three days before. Taking preps that you can take with a glass of water and then drink two liters of tea or water.”
“My son, Andrew, has autism and Crohn’s disease. When he has to do colonoscopy prep, he likes to listen to Disney music and use a timer. Andrew is almost 30 years old and has been having to do colonoscopies since he was 17. This past year, for the first time, he did the pill prep and loved it. He used a timer to tell him when to take the next pill. Andrew told me he will never go back to liquid prep. Pill prep was so much easier for him, especially with his sensory issues.”
“Take notes on all preps you’ve been assigned and take notes and photos of what it felt like. I found one that was less painful for me, and I always request it. I also alternate sips out of a straw with apple juice. I drink the prep in my kitchen, near a bathroom, and watch TikTok’s while drinking to distract myself.”
“I only eat soft foods 2-3 days before, make sure to hydrate, and follow the instructions they give about not eating things like seeds or nuts a week before.”
“Have a bidet and diaper cream ready.”
“Desitin, Gatorade that is the Frost Glacier Cherry flavor (not red) frozen or really cold to help me stay hydrated.”
“Make freezer pops out of the Gatorade prep mix.”
“For me—finding fun drinks, whether a tea at Starbucks or stocking up at the grocery store, really makes it feel less horrible. I started this as a teenager. I make a list of movies or shows I want to binge. If you’re comfortable with it, have a friend there to distract you—at 15 years old, my boyfriend stayed with me all day for my surgery prep which was the same as a colonoscopy and we watched movies and he distracted me/made me laugh and at times I forgot what was going on!.”
“Savory liquids to balance out the sweet!”
“Mix the prep with Crystal Light Lemonade—instead of the lemon mix the pharmacy provides. Drink the prep through a straw and suck on hard candy (e.g., Werther’s Originals) in between doses to get rid of the taste and have something to look forward to.”
“Take SUTAB (pill prep) and Zofran and then fall asleep. Your bowels will wake you up and you’ll avoid the nausea but start the pooping process. I do the same for the morning dose! If you vomit, at this point it’s fine, just hopefully after the nap and pills are digested!”
“Gummy bears/worms!”
“Pill prep has been a gamechanger for me!”
“Extending the clear liquid diet an extra half day or full day helps a ton with prep.”
“You have to have a movie downloaded on a device that you can have in the bathroom and a pillow for the toilet seat for your back. I’m a fan of disposable diapers because after the first several poopy poops, you get to the drizzle stage and then it’s annoying to have to get up every two seconds towards the end. They also come in handy when you’re sleeping and when you’re traveling to the procedure.
“Before I have a colonoscopy I write down positive affirmations and thoughts and there is like a Table of Contents that’s like “When you’re sad” or “When you need a good laugh” and it really helps me though the ups and downs, although it may sound silly. I choose what to drink and I always have my good luck drink which is blue Gatorade.”
“Use nuun electrolyte drink instead of Gatorade!”
“My personal hacks are to follow what you know works for you. I followed the timings of when to take what from the last instructions and it wasn’t the cleanest prep. I should have listened to my gut and started doing that earlier. I resort to drinking Ensure Plus instead of just relying on broth and soft foods to keep me feeling full. It’s helped me SO much. I know not everyone can tolerate it or like it, but when I was on a liquid diet about a year ago for two months, I only had Ensure Plus. I got used to it. It’s now a lifesaver, especially if I’m traveling or on the road and not sure what food I will have access to. It helps to start the diet a bit earlier, so mash and fish instead of just toast and pasta.”
“I mix apple juice with my Suprep! I also always buy bone broth or stock because the protein per cup is higher. I like the Zoup brand because there’s 3 or 4 gram of protein per cup. I also get the College Inn brand bone broth which has up to 10 grams of protein per cup.”
“Gummy bears!! Just not the red or purple ones. Just being able to chew something helps! Progresso Chicken Soup. Use a metal strainer to strain out all the solids and then sip the broth. It’s thicker and has more flavor than regular stock and it’s just more satisfying.”
“Remind yourself “this is only temporary.” Having loved ones supporting also helps to distract a little, which makes it easier to get through. Focusing solely on drinking cup after cup can seem very overwhelming.”
“Start a low residue diet a few days early even before your doc says to. Mix prep with Sprite. Have hard candies or gum to chew on while doing prep. Use a measuring cup or something to lines to indicate how much to drink.”
“I really love the Trader Joes less sugar lemonade mix with water for my prep. I chugged and it was so delicious! Also, ice pops like the good pop brand were yummy.”
“Gummy bears! Making ice cubes out of juice and chewing on the ice.”
“Make sure it’s cold! Drink with a straw, chew Juicy Fruit gym in between drinks, this helps cut the saltiness. Do two-step prep if your practitioner allows it (half the night before and the other half in the morning). Ask if you can use one of the lower volume prep or the MiraLAX and Gatorade prep.”
“For the MiraLAX prep I use two different flavors so I can alternate when I get sick of one.”
“Mix the prep early and put it in the fridge. Have music and TV on to help distract yourself.”
“While most people say to drink it cold, I prefer my prep at room temperature so I can chug it faster.”
“Always lots of ice and drinking thru a straw. Big gulps. Have a station in the bathroom with a laptop streaming Netflix. I also got a Bidet before my last one!”
“Gummy bears! I buy the Haribo ones and don’t eat the red ones. My favorite prep hack thus far. It’s great getting to chew something when everything else is liquid.”
“Lots of mint tea when the cold chills kick in a few hours before you have to go in for the procedure.”
“Use a Pedialyte jug and ensure it is very cold and drink the prep with a straw. The slower you drink, the worse it is. I always chug it super-fast through a straw and it gives me 10-15 minutes between each cup. Have lots of other drinks that you don’t normally consume to make it fun and have lots of juice, Jello, soda, and popsicles on hand!”
“I’ve turned prep days into self-care days. I binge shows, nap, relax, and try to take care of myself.”
“I like to alternate between sweet/cold beverages and salty/warm soups when I am trying to stay hydrated before starting prep. Sprite/popsicles/lemon ice and then chicken broth.”
“I chase my prep by sucking on approved colored Lifesavers. They truly are a lifesaver for me. I could never do it without them.”
“I recommend the pill prep instead of liquid prep if you’re neurodivergent or have issues with taste and textures. Maybe keep a backup on MiraLAX and Gatorade or juice in case you can’t tolerate the liquid prep. If you know you get nauseated, take prescription anti-nausea medication like Zofran before you begin the prep. I like Squatty Potty and having wipes to dab and pat my skin. A Peri Bottle can be useful. If you’re prone to hemorrhoids or know you have vascular issues like pelvic congestion syndrome, apply hemorrhoid cream in advance. Keep Zinc Oxide handy if it starts to burn or feel raw. Get into comfortable clothes that’s easy to get in and out of in the bathroom. I personally use a heating pad and Bentyl for intestine cramping. I usually make sure I’m scheduled first thing in the morning, and I ask for extra IV fluids.”
The Takeaway
Colonoscopy prep is a universal challenge in the IBD community, whether you’re a child facing your first scope or an adult whose been through dozens. But as the stories above reveal, there are countless ways to make it less daunting through creativity, distraction, teamwork, and sometimes sheer humor.
I personally start a full liquid diet 4-5 days before my scope to ease the actual prep. I make sure I have Zofran on hand to manage my nausea (I always vomit, regardless), and I prefer the SUTAB pill prep. I’ve done multiple preps since being diagnosed with Crohn’s disease in 2005, and my last three preps, SUTAB pills have been the “most tolerable.” While MiraLAX/Dulcolax is popular, I never enjoyed having to drink such a large volume of liquid. Having gummy bears on hand is also a necessity for me! My husband always takes the day off work, and we go out to breakfast and spend the day together afterwards as a reward for all I went through.
If you’re gearing up for a prep, remember you’re not alone. Thousands of IBD patients and caregivers are walking this same path and learning tricks along the way. Find what works for you (or your child), advocate for needs, and give yourself grace. And once it’s done? Celebrate that victory meal and the relief of getting through another milestone in your IBD journey.
When you live with Inflammatory Bowel Disease (IBD), you become an expert in knowing life can throw you curveballs at any given moment. Those curveballs are especially worrisome and scary during pregnancy and after you become a mom.
For one IBD mom who wishes to remain anonymous, that curveball came in the form of a rare and dangerous vitamin K deficiency that caused life-threatening complications for both her and her newborn son after delivery. Now, two years later, a published medical case study based on their experience is helping raise awareness of this rare issue, offering hope that future pregnancies in the IBD community might benefit from earlier detection and intervention.
Diagnosed Young, Navigating the Unknown
This mom was diagnosed with Crohn’s disease at age 13, and now at 34, she’s lived with IBD for more than 20 years. Her journey has included numerous medications, including a long stretch on Humira, which she remained on during her pregnancy, and four partial small bowel resections. She’s also undergone several exams under anesthesia due to complications like abscesses and fistulas.
Thankfully, during her pregnancy, her Crohn’s was well-controlled with no active disease, making the post-delivery complications much more shocking.
A Sudden Turn After Delivery
After giving birth to her son (we’ll call him “B”), what should have been a joyful moment quickly turned traumatic.
She spent 16 days in the hospital, including three in the ICU, while her newborn faced a 23-day NICU stay. The cause? A severe, undiagnosed vitamin K deficiency, which led to hemorrhaging in both mom and baby. The medical team was blindsided—none of them expected this.
Understanding Vitamin K Deficiency & IBD
Let’s get one important thing straight first. This situation is not about skipping the vitamin K shot that newborns typically receive. The mom explains:
“It’s imperative that newborns receive a vitamin K shot after they are born to prevent vitamin K deficiency bleeding. The American Academy of Pediatrics recommends that all newborns receive a single dose of vitamin K, because babies are naturally born with very little in their bodies. In our case, my son did get the shot—but because I was unknowingly severely deficient in vitamin K during pregnancy, his vitamin K levels in utero were dangerously low, leading to a brain hemorrhage before he was even born. The bleeding he experienced was similar to what some babies experience when they don’t receive the shot, but in our case, it happened earlier—and was not caused by withholding care. In fact, he needed far more vitamin K after birth to restore safe blood clotting levels.”
This vital distinction can prevent confusion and reinforce just how important that standard vitamin K shot is for all newborns.
What She Wants Other IBD Moms to Know
“Knowing what I know now,” she says, “I want fellow IBD women to understand a few key things about vitamin K deficiency during pregnancy:”
This is rare. Most pregnant people with IBD will never encounter this issue. “I hope that offers peace of mind. But as we all know, knowledge is power—especially when you live with IBD.”
If you’ve had bowel resections or are deficient in other fat-soluble vitamins (like A, D, or E), consider bringing this case study to your GI and OB/Maternal Fetal Medicine (MFM) doctors. Ask about checking vitamin K levels, as well as PT/INR and PTT, which monitor blood clotting.
You can develop a deficiency during pregnancy even if you’ve never had one before. “Outside of pregnancy, I had no clotting issues. But between my history of resections and my baby’s increasing demand for nutrients, my levels dropped—and no one knew.”
Looking Back: What She Wishes Had Been Done
“If we had been monitoring my vitamin K levels, PT/INR, and PTT throughout my pregnancy, we likely would have seen early warning signs,” she says. “These aren’t standard tests, but I hope someday they will be for IBD moms with similar risk factors.”
A Silver Lining in the Study
Despite the trauma, having their experience turned into a published medical case study brought a sense of closure.
“When they told us they wanted to publish it, I felt incredibly validated. This wasn’t just something we lived through—it’s now out in the world to potentially save lives. That’s the best-case scenario for us.”
The comprehensive care team—consisting of her OB, MFM, GI, hematologist, and PCP—remained closely connected throughout the experience. After both mother and baby were stabilized, Ohio State’s hematology team and Nationwide Children’s Hospital worked together to identify the deficiency as the root cause for both patients.
“They didn’t miss anything—they acted on the knowledge they had at the time, and when things went south, they sprang into action. I’ll always be grateful for that.”
“B” Today: A Story of Resilience
Despite a traumatic start, B is now a thriving, happy, and a miraculously healthy two-year-old.
“We were so worried about long-term impacts due to the hemorrhage in his brain, but he is now meeting and exceeding all his developmental milestones. He doesn’t need any additional support. It’s truly a miracle.”
His early care included close monitoring from neurology and the Early Development Clinic at Nationwide Children’s Hospital, along with early intervention specialists. Today, all those appointments are in the rearview mirror.
What About Future Pregnancies?
The reality is that this situation may recur if she decides to grow her family.
“My doctors believe I’d face similar risks, so we would monitor everything very closely: vitamin K levels, PT/INR, PTT and I’d likely receive IV vitamin K infusions throughout pregnancy to stay ahead of any deficiencies.”
Lifting the Tide for Others
After two decades of managing Crohn’s, she knows how isolating chronic illness can be.
“It’s hard. It’s lonely. It’s easy to feel invisible. But finding others who share their stories and who get it has been a game-changer for me. That’s why I’m sharing this now. Even if this specific challenge never affects you (and I truly hope it doesn’t), I hope you feel a sense of solidarity. A rising tide lifts all ships and if sharing our story lifts someone else’s experience just a little, it’s worth every word.”
If you’d like to contact this IBD Mom don’t hesitate to reach out to me, and I will connect you. It’s stories like this that help to pave the way for future families.
When you’re living with a chronic illness like Crohn’s disease or ulcerative colitis, it’s easy to become hyper-aware of every medication, every symptom, and every nutrient—or lack thereof. One essential mineral that often flies under the radar is magnesium.
Magnesium supports nerve function, hormone balance and how we respond to stress, so when levels drop, the nervous system can become overly reactive. For those with Inflammatory Bowel Disease (IBD), these symptoms can be even more noticeable because our bodies often struggles to absorb and retain magnesium properly.
According to Hollie King, Founder of Sweet Bee Organics, this humble mineral could be one of the most powerful tools in the IBD toolkit. This week on Lights, Camera, Crohn’s Hollie explains why magnesium matters so much for people in our community.
While I was working on this article, I did an Instagram poll asking the IBD community if they take a magnesium supplement. Of the 245 people who responded, 34% said “yes”, 29% said “no”, and 37% replied “should I be?”
The power of Magnesium
“Magnesium is one of those quiet powerhouses in the body,” Hollie explains. “It’s often overlooked, but absolutely essential. It plays a role in over 300 biochemical reactions, helping muscles relax, supporting proper nerve function, balancing hormones, and aiding energy production.”
When magnesium levels drop, your body knows it—but it doesn’t always scream it out loud. Instead, it whispers. Symptoms like anxiety, poor sleep, muscle cramps, low energy, and even restless legs may emerge. But there are subtler signs too: eye twitching, heart palpitations, tingling sensations, and a hypersensitivity to noise or stress.
For those with IBD, particularly Crohn’s disease, magnesium deficiency can be even more pronounced. “When the gut is inflamed or damaged, it struggles to absorb nutrients properly,” Hollie shares. “And magnesium is one of the first to drop.”
The Magnesium–IBD Connection
Recent research, like the article “Magnesium—A Potential Key Player in Inflammatory Bowel Diseases?” published in the Journal of Inflammation Research, highlights the strong link between magnesium deficiency and IBD. But knowing you’re deficient and being able to do something about it are two very different things, especially if your gut can’t absorb it well.
That’s where Sweet Bee Organics comes in. Rather than relying on supplements taken by mouth, Hollie and her team focus on transdermal support—a method that completely bypasses the digestive system.
“Our Sweet Sleep Magnesium Butter delivers highly absorbable magnesium chloride directly through the skin,” Hollie says. “You simply massage it into your chest, feet, lower back, or even your tummy before bed. It’s not just about topping up magnesium—it’s about calming the nervous system, supporting sleep, and helping the body reset.”
The Sweet Sleep Magnesium Butter isn’t just effective—it’s a best-seller across the U.S. and U.K. for a reason. “We’re obsessed with packing as much magnesium as possible into our balm,” says Hollie. “It’s not easy, but we’re committed to delivering a product that works—and works quickly.”
For people with Crohn’s or ulcerative colitis, the benefits of restoring magnesium levels can be profound. Balanced magnesium supports better digestion, improves sleep, reduces muscle tension, steadies mood swings, and even eases PMS symptoms. You sleep better. You feel calmer. Your energy becomes more stable, and your muscles feel less tight or twitchy.For IBD patients in particular, it can help calm inflammation and improve nutrient absorption—essential steps in managing the day-to-day symptoms of the disease.
“It’s not a magic fix, but it’s one of those foundational nutrients that helps everything else work better. The biggest thing people notice? They just feel more like themselves again,” Hollie explains.
Hollie’s Health Journey
This mission is deeply personal for Hollie, who was diagnosed with aggressive cervical cancer and had to completely reimagine how she cared for her body. “Magnesium became an important part of my healing journey. It wasn’t just about sleep or stress—it was about helping my body heal, rebuild, and feel safe again.”
Screenshot
Hollie happens to be my husband’s first cousin—and witnessing her health transformation and all she’s accomplished since her cancer diagnosis has been awe-inspiring. We’re not only family, but friends and I admire her and the genuine work she’s doing. We’ve wanted to collaborate for awhile and when Hollie saw the recent published medical study regarding magnesium and IBD we knew this was the perfect opportunity.
Hollie and I took our kids trick or treating this past Halloween when she was back in the States
Her empathy extends to the IBD community. “For anyone living with IBD, I truly see you. I know how exhausting it can be to manage symptoms, juggle treatments, and wonder if your body is even absorbing what it needs. That’s why I created Sweet Bee. Magnesium might seem like a small thing, but sometimes the smallest shifts are the ones that change everything.”
How is Magnesium Measured—and Why the Standard Test Might Miss the Mark
Many of us assume a blood test will tell the full story, but Hollie points out that traditional serum magnesium tests only measure about 1% of the magnesium in your body.
At my clinic visit with my GI last week, my doctor included magnesium in my lab work and the results were within range, but he also told me there would be no harm in using the transdermal magnesium discussed in this article.
For people with IBD, especially those experiencing persistent symptoms, your GI may suggest testing beyond the standard serum magnesium draw or even recommend supplementation based on symptoms alone. This may be something you want to bring up during your next clinic visit or over the Patient Portal.
How to Naturally Raise Your Magnesium
While supplements are helpful, diet is still key. Magnesium-rich foods include:
Pumpkin and chia seeds
Almonds, cashews, and peanuts
Beans and legumes
Spinach, broccoli, and potatoes with skin
Whole grains like oats and brown rice
Avocados, bananas, raisins
Milk, yogurt, and soy milk
Salmon, halibut, chicken, beef
Fortified cereals
That said, people with IBD often can’t rely solely on food due to absorption challenges. This is where topical support like Sweet Bee’s magnesium products truly shine.
Can You Take Magnesium with Crohn’s or Colitis?
Yes, but with care. Magnesium—especially in forms like citrate—can cause loose stools, which is problematic for IBD patients. That’s why topical magnesium is often a safer, more effective choice.
Always consult with your gastroenterologist before starting new supplements, especially if you’re in an active IBD flare, dealing with kidney disease or if you’re concerned about the medication(s) you are on.
Final Thoughts
In the landscape of IBD care, it’s easy to feel overwhelmed. But as Hollie reminds us, simple, natural tools—when thoughtfully applied—can offer real relief. Whether you’re struggling to sleep, feel calm, or just want to feel like yourself again, magnesium might be what your body’s been craving.
“You deserve to feel strong, rested, and well in your body. Replenishing magnesium levels in a gentle, non-irritating way can make a real difference in how you feel, both physically and emotionally,” Hollie says. “And we’re here to support that every step of the way.”
Learn More About Sweet Bee Organics
To explore Sweet Sleep Magnesium Butter and other clean wellness products created with love and integrity, click here. Use code NATALIE15 for 15% off sitewide.
Sweet Sleep was recently spotlighted on The View Co-Host’s Favorite Things for Mother’s Day. Check out the segment here.
Disclaimer: This article was not sponsored, but the content is for informational purposes only and does not replace professional medical advice. Always consult your healthcare provider before starting any new supplement.
When House Bill 544 passed the Montana Legislature and was signed into law May 1, 2025, it marked more than just a policy victory—it became a symbol of hope and action for families affected by Inflammatory Bowel Disease (IBD), especially those navigating the challenges of very early onset (VEO) IBD.
In the latest article on Lights, Camera, Crohn’s, we hear from the Founder and Executive Director of VEO Guardians, Rachel Markovich. She is not only a caregiver, but a passionate advocate behind the bill. Rachel shares the impact this is expected to have on families, the journey to getting the bill passed, and her hopes for this to set a precedent for the rest of the country.
What is House Bill 544, and why does it matter?
HB 544 is a transformative piece of legislation designed to eliminate two of the biggest hurdles families face when managing IBD: access to timely treatment and the threat of retroactive insurance denials.
The bill ensures that when a medical provider can present two efficacy studies showing a biologic treatment works in children of a comparable age, insurance companies must approve the request. This provision reduces dangerous delays in treatment— a common and deeply frustrating barrier for caregivers and physicians alike. Click here to see the news coverage.
The second part of the bill protects all Montanans by prohibiting insurers from denying coverage retroactively after a medication has already been approved. In the unpredictable world of chronic illness, this gives families something they often lack: peace of mind.
How did this caregiver become involved?
For Rachel as a mom of a son with VEO-IBD, this fight is personal.
“My son was diagnosed with VEO IBD at just 22 months old,” she shared. “Thankfully, his health has stabilized, and that gift gave me the time and perspective to help others.”
What began as outreach soon turned into a movement. With the support of VEO Guardians and a network of dedicated advocates, she testified in Helena and worked tirelessly to humanize the legislation. “It was an emotional and transformative journey—one built on compassion and resolve. It’s not just about celebrating a win—it’s about raising awareness for what this means for families across the state.”
The mission of VEO-Guardians was previously featured on Lights, Camera, Crohn’s, you can check out that article here.
Kim Longcake is an Advanced Nurse Practitioner in Montana. She says, “It is such an honor to be a part of this amazing organization. I am proud of the work we have done to protect access to care for Montana children and grateful to have a resource for families in their greatest time of need.”
Will this bill inspire similar legislation across the country?
Yes—and momentum is building.
“We’ve been in touch with national organizations like the EveryLife Foundation and the Crohn’s & Colitis Foundation. They’re excited about what we’ve accomplished here in Montana, and we’re developing a strategy to help other states follow suit.”
For those interested in bringing similar legislation to their own communities, the message from Rachel is clear: “We’re here, and we’re ready to help.”
How can people get involved, especially if they don’t live in Montana?
“Stay connected with us,” she urged. VEO Guardians regularly shares updates, advocacy tools, and family stories through their social media channels and newsletter.
Anyone can reach out directly for guidance, support, or to get involved in expanding the model elsewhere. “We want to help others navigate this path.”
What has VEO Guardians accomplished so far?
The organization recently helped a family avoid a $6,200 charge when a job loss disrupted their child’s insurance—ensuring timely infusion treatment. They’ve signed a reimbursement agreement with Community Medical and are working to secure similar partnerships with Montana’s two other major hospitals.
They’ve also welcomed a new board member with expertise in family counseling and plan to launch free counseling services and 504 plan support on their website soon. And for children newly diagnosed with IBD, a teddy bear delivery program is already in motion.
“Every step we take is rooted in our mission to support, uplift, and empower the IBD community.”
Final Thoughts
“In the darkest moments, we often find the strength to shine the brightest,” she said. “This bill is proof of what compassion and community can accomplish. To anyone facing this diagnosis—you’re not alone. There is a path forward, and we’re walking it together.”
Rachel tells me local gastroenterologists in Montana whom she’s spoken with are thrilled the bill has been signed because it removes the red tape and allows doctors to do what they do best—treat their patients. It’s a win for everyone.
“It fills me with pride, gratitude, and hope,” Rachel said. “What once felt like a long shot is now a new reality for countless families. I know it will ease the road for many who follow.”
To stay up to date or get involved, follow VEO Guardians on Facebook and Instagram, or visit their website to sign up for their newsletter.
When most kids were running around their middle schools full of energy and excitement, Taylor Gautney was quietly fighting an invisible battle. In sixth grade, while his classmates joined extracurriculars and laughed through lunch breaks, Taylor was barely making it through the day. Many afternoons were spent passed out on the couch after going the entire day without eating. One day, after skipping lunch again, he collapsed on his way back to class. That moment changed everything.
At first, doctors suspected celiac disease. He was placed on a gluten-free diet after an initial endoscopy, but nothing improved. For years, the mystery lingered—until a more thorough examination revealed the real culprit: Crohn’s disease. A new diagnosis, a new treatment—Humira—and a new outlook on life began to take shape.
Now in remission and attending Arizona State University (ASU), Taylor has transformed his story from one of struggles to one of strength. But it wasn’t always easy. This week on Lights, Camera, Crohn’s a firsthand look at what it was like to be diagnosed with IBD at such a young age and how his first year of college went living across the country from his family.
“Just Keep Fighting”
Looking back, Taylor wishes he could tell his younger self one thing: “Just keep fighting and enjoying the positives in life.” Being diagnosed with a chronic illness at age 11 felt like a devastating detour. He admits that it changed the way he viewed the world and himself. “I started to think of every aspect of life as negative,” he recalls. But over time, Taylor learned to embrace small joys, and most importantly, to appreciate the unwavering support of his family.
Taylor’s mom, Anna, says, “It’s crucial to advocate for your child and speak up for them if medications are not working. It is also important to showcase to your child that you are in this with them, help them find a community, such as the Crohn’s and Colitis Foundation. This way, they can meet people who have what they have and formulate a sense of belonging.”
Holding On Through the Hard Days
Taylor wants young people diagnosed with IBD to know that while the patient experience is incredibly challenging—often filled with procedures and surgery, flare days, and quiet battles with your own body, it doesn’t define who you are. “People can’t see the diagnosis from the outside, they see your personality and exterior self,” he says. “Just be yourself, let people come to you and support you, especially during a rough time like an IBD diagnosis.”
The Power of Family
Taylor credits his parents for being the steady foundation beneath his feet throughout the rollercoaster of diagnoses and treatments. “My mom has been my rock,” he says. She’s been by his side at almost every appointment and has researched tirelessly to understand Crohn’s. Taylor’s dad always makes time to show Taylor the world with family trips and unshakable support. “They have given everything to me and made my life so much easier after the diagnosis.”
Life at ASU with IBD
Taylor’s transition to college life came with its own set of hurdles, including logistical nightmares like getting his medication delivered to campus. But he’s found his rhythm. “It’s definitely not as hard as I thought it would be,” he says. One surprising blessing? His roommate. “He also had a medical condition that required shots, pills, and daily maintenance,” Taylor says. Their shared experiences helped them form an instant bond, even leading to grocery trips for IBD-friendly dorm snacks.
Taylor’s professors and friends have also shown deep compassion. He remembers an English professor who read about his condition in a personal essay and went out of her way to learn more about Crohn’s. “She made me feel really special and seen,” he says. His friends check in on him, make sure he’s got his injections, and understand when he needs to sit out from social events. “I thank my friends at ASU for their understanding and empathy.”
A Voice for the Voiceless
Studying sports journalism, Taylor dreams of becoming a play-by-play broadcaster for Major League Baseball—ideally for the Atlanta Braves. But his passion extends beyond sports. He wants to use his voice to make an impact and tell meaningful stories. One of the most pivotal moments in his life came when he was asked to be the Pediatric Honored Hero for the Crohn’s & Colitis Foundation’s Birmingham walk. “That one event gave me confidence to speak in public and really sparked my love for communication,” he says.
Now connected with the Arizona-New Mexico chapter of the Foundation, Taylor is committed to giving back. His mission? To reach kids and teens who are newly diagnosed and remind them they are not alone.
Final thoughts
Taylor and I connected after he was doing research for a college project and reached out to interview me about my patient experience and advocacy work. During our initial Zoom interview, I was so blown away by his positive attitude and how he takes on life with IBD. I asked him during the call if I could have the honor of sharing his story. While there are male patient advocates—we need more who are willing to share their story.
Taylor is wise beyond his years, so articulate, genuine, and kind. The sky is truly the limit when it comes to his future. If anything, living with Crohn’s disease since age 11 has helped show him all he’s capable of despite his disease.
You can connect with Taylor by following him on Instagram: @t.gautney or by emailing him: tgautney@asu.edu.
It feels like a punch to the gut. Even though you’re anticipating it, the experience is not easy for anyone. For patients with inflammatory bowel disease (IBD), stability is everything. Whether living with Crohn’s disease or ulcerative colitis, finding a medication that keeps symptoms under control is often the result of years of trial and error. So, when insurance companies or healthcare systems mandate a switch from a familiar biologic like Humira to a biosimilar such as Hyrimoz or Amjevita, the decision can feel sudden, confusing, and unsettling. As of right now (May 2025) there are 22 FDA-approved biosimilars on the market for infliximab (Remicade), adalimumab (Humira), and Ustekinumab (Stelara) with many more coming down the pipeline.
It’s easy for providers to rely solely on the science that says it should be a “seamless,” effortless transition for patients and caregivers—but that’s not always the case, nor is it ever a guarantee. This week on Lights, Camera, Crohn’s we hear from more than 30 patients who have lived this reality. While many people seem to do well clinically, it’s imperative that we also discuss the mental and emotional toll this forced non-medical switch takes on people with chronic, debilitating illnesses and their caregivers. This blog aims to demystify biosimilars, highlight the emotional and clinical complexity of switching therapies, and provide guidance for healthcare providers and patients navigating this challenging transition.
As someone who was forced off my Humira after being on it for 16 years and put on Hyrimoz, I empathize with how complicated this is for patients. Not only was I petrified to switch—but I had a God-awful experience that resulted in going from deep remission to dealing with an adverse response for two months of my life, while trying to be a mom to three young kids.
I don’t take this subject lightly and frankly; I don’t care who I piss off by sharing this patient experience transparently. I angered some donors from a Pharmacy Benefit Manager (PBM) when I spoke on stage in front of a large crowd last fall genuinely thanking my IBD nurse who went to bat for me countless times to help me win my appeal to get back on Humira—this isn’t about profit, it’s about patients. We don’t owe anyone an apology for being uncertain about being told we need to switch our heavy-duty drug therapy not by a doctor, but by someone working in corporate America.
Biosimilars are not generics
First things first, I must clear the air on this. Almost every direct message I receive from patients refers to biosimilars as “generics” …and that’s a common misconception that needs to be done away with.
Unlike generic drugs, which have identical active components, biosimilars are comparable but not identical to their originator drugs. According to the US-FDA, a biosimilar is a biological product that is potent, pure, and safe and that is “highly similar to and has no clinically meaningful differences from an existing US-FDA-approved reference product”. In other words, biosimilars are equivalent to the reference biologics regarding safety and efficacy.
When you hear the terms “originator” or “reference” biologics—that means Infliximab (Remicade), adalimumab (Humira), and Ustekinumab (Stelara). There are many other biologics of course, but so far, these three biologics have biosimilars approved by the FDA. You can familiarize with their names that I’ve listed below so if you see one listed in a letter it’s not foreign to you.
Infliximab Biosimilars:
Inflectra (infliximab-dyyb)
Renflexis (infliximab-abda)
Avsola (infliximab-axxq)
Ixifi (infliximab-qbtx)
Zymfentra (infliximab-dyyb)
Adalimumab Biosimilars:
Amjevita (adalimumab-atto)
Cyltezo (adalimumab-adbm)
Abrilada (adalimumab-afzb)
Hadlima (adalimumab-bwwd)
Hulio (adalimumab-fkjp)
Hyrimoz (adalimumab-adaz)
Idacio (adalimumab-aacf)
Yuflyma (adalimumab-aaty)
Yusimry (adalimumab-aqvh)
Simlandi (adalimumab-ryvk)
Ustekinumab Biosimilars:
Wezlana (ustekinumab-auub)
Selarsdi (ustekinumab-aekn)
Otulfi (ustekinumab-aauz)
Imuldosa (ustekinumab-srlf)
Yesintek (ustekinumab-kfce)
Pyzchiva (ustekinumab-ttwe)
Steqeyma (ustekinumab-stba)
Important note: While these biosimilars have received FDA approval, the availability of some may be subject to patent litigation settlements or market launch agreements, potentially delaying their commercial availability.
Let’s look at the real-life numbers
While working on this article, I ran several polls on Instagram asking the IBD community about their personal experiences. Some of the findings surprised me:
Have you received a letter saying you have to switch? Of the 265 respondents, 64% of patients said “yes”, and 36% said “no”.
Did you appeal before switching to a biosimilar? Out of 200 responses, 33% responded “yes” and 67% responded “no”.
For those who switched was the transition seamless—or did you notice an uptick in symptoms? Of the 140 responses, 51% had a seamless transition and 49% noticed an uptick in symptoms. This right here speaks volumes.
If you responded poorly to your biosimilar and your GI appealed insurance, what was the outcome of the appeal? Out of 75 responses—38% of patients were denied, 32% were put back on the originator drug (biologic), and for 30% after multiple appeals they finally won and returned on their biologic.
Let’s hear directly from patients
Bre: “I was taken off Humira after the New Year and placed on Simlandi for my ulcerative colitis. I was nervous as I had just come out of a two-year flare and had finally found a drug that worked and even though I was reassured that this was as good as Humira, I still had my doubts. Thankfully, I have had a positive experience and have remained in remission since starting Simlandi in January. I hope this story helps others feel less afraid of the potential outcomes when they get the dreaded non-coverage letters.”
Kyrsten: “Back in April I was forced off Stelara to the biosimilar, Yesintek. I went into it with an open mind because my Crohn’s has been in remission for about a year and a half. Unfortunately, I am now experiencing more symptoms that I’m documenting and oral manifestations of Crohn’s and need to see an oral medicine doctor now.”
Stefanie: “I’ve had to switch biosimilars twice at this point, this second time, while I was pregnant. I’m doing just fine!”
Alexandra: “I was first afraid of Humira, then I grew into being afraid of not having it; so, when my insurance mandated the switch to Hyrimoz late last summer, I was so worried (as all are/were)! In September, I was starting to feel some symptoms pop in, so we did all the tests, which indicated that I was still in clinical remission. Thankfully, I am doing ok now with no issues.”
Christina: “It was first recommended to me by my GI a couple of months after diagnosis in 2021 to start on biologics, since the oral medications had stopped working for me. We collectively decided the best option for me would be Remicade, however when it was brought to my insurance company, they immediately denied it. Insurance said it wasn’t their “preferred method” and wanted me to try and fail Humira first. When my GI tried to get the Humira approved, my insurance company ended up denying that, too, and this time, their excuse was it “wasn’t medically necessary.” It took my GI a couple of months to get a biologic approved and I almost ended up back in the hospital as a result.”
After receiving her first injection, Christina ended up developing an allergic reaction and had to be switched to something else. After another month of fighting insurance, Christina’s GI was able to get Remicade approved.
Christina goes on to say, “I did very well on that for about a year, until my body developed antibodies, and I had to switch once again. I then started Entyvio infusions which I have been on ever since, and so far, I’ve been doing well on it.”
Audrey: “I was forced to switch from Remicade to Inflectra a few years ago due to insurance coverage. My job at the time was horribly stressful and very time-consuming and getting the news then about my medication no longer being covered and that my next infusion was delayed because of this change over the phone from my infusion clinic was terrible. I remember sitting in the workplace cafeteria when my phone rang, and I burst into tears and was pleading with the pharmacist that gave me the news prior to receiving the letter.”
At this point, Audrey was receiving Remicade every seven weeks. With the delay and having to wait for Inflectra to be shipped, she was pushed out an extra week.
“The thing that made me so angry, was that I had already received my Remicade shipment, the nurses just weren’t allowed to mix and dispense it because of the insurance change. I refused to toss that Remicade dose until the vials expired, since I knew how costly it was. I called so many charity pharmacies for low-income folks to see if they could take the vials and since its temperature controlled, they couldn’t. Such a waste,” said Audrey.
Thankfully, Audrey tells me she hasn’t had any issues with the switch, and she’s stayed in remission—even during and after her first pregnancy. But she says the stress and frustration that occurred impacted her mental health at the time.
Kelly: “I just got the letter. Been on Stelara since 2017. I also take it every four weeks, even though the recommended dose is every eight weeks. I get my insurance through my husband and our insurance turns over on 6/31/25. The new policy begins July 1st. I’m really concerned and honestly don’t want to deal with this.”
Sandi: “I was forced to change from Remicade that had me in remission for several years to Inflectra and the outcome was not good. I had multiple Crohn’s flares a month, which was not happening when I was in remission. My GI appealed and after a year, insurance started to cover my Remicade again. Since getting back on Remicade, I’m in deep remission, again.”
Britt: “I was diagnosed with Crohn’s in 2011 at the same time I was diagnosed with Primary Sclerosing Cholangitis (PSC), a rare liver disease. I was on Remicade and was switched to Avsola. For a while, I was quite skeptical, but we stayed the course. I had some ups and downs with my health, but I was just told I am in histological remission by my GI! After five years of struggles to find the right medication, my health finally seems to have aligned. I also take 6mp to reduce antibody development to the Avsola.
Danielle: “I went into my pregnancy in remission and my first and second trimesters were lovely. About halfway through my pregnancy, insurance decided it was the right time to swap my medications. Two weeks following that change, I was already struggling. I ended up finishing my pregnancy on two different rounds of methotrexate and iron infusions. I had a scheduled C-section at 39 weeks, and I think my care team hoped that my body was just struggling balancing pregnancy and Crohn’s…that was not the case at all.”
Danielle says she tried two more Inflectra infusions after her daughter was born and saw no improvement. She required a round of prednisone and that didn’t help either. She was then switched to Humira injections every two weeks and they seemed to work wonderfully and she started to feel better.
“Then my insurance threatened to switch me to a Humira biosimilar, but Humira failed me right when that was supposed to happen, so I was transitioned to Entyvio. For six months I saw no improvement on Entyvio…more prednisone and still NO improvement. Finally when my daughter was 14 months old (so over a year and a half of feeling like absolute garbage and having no energy) I got bowel resection surgery and switched to Stelara.”
Danielle went on to say she’s been in remission since December 2021, and she still wonders if switching to the Remicade biosimilar caused all this to happen.
“I truly feel like that change took part of the joy of pregnancy away from me and also took a lot of special time away from my daughter the first 14 months of her life. I spent her second Christmas in the hospital unable to see her for two weeks. I was on so many pain medications for so long before the surgery that I don’t remember her first birthday. I lost a lot simply because someone was trying to cut costs and making decisions they are not educated about.”
Brooke: “I was on Remicade for 15 years, then I was forced to switch to Inflectra. I was incredibly stressed and tried to appeal but lost that battle. I’ve now been on Inflectra for 3 years and I am doing well! I still hate that we are forced to change when something is going well. The amount of stress, anxiety, and time I spent fighting the insurance company took a toll on me.”
Brooke went on to say that she got pregnant and had a daughter while on Inflectra. Her GI and OB had no concerns with the biosimilar during pregnancy.
Maya: “At the beginning of March, I was told by my insurance that Stelara will no longer be covered and that I would be put on Yesintek. I’ve only gotten one dose of it so far, but I very much empathize with all the emotions that come with getting the letter. So far, I haven’t noticed any additional symptoms or changes in how I feel. I’m hoping Yesintek works for me and that I continue to feel ok!”
Maria: “I live in Sweden where Humira is covered by the State since no private insurance is needed, the last year though I was recommended from doctors to switch to a biosimilar. So, in autumn of last year, I decided to try Hyrimoz. I noticed no difference in the first three months, but after that, I saw an increase in symptoms, especially for my rheumatoid arthritis. My doctor recommended that I take the injection weekly instead of biweekly, but that didn’t help at all. Since I haven’t developed any antibodies, my doctor switched me back to Humira and I felt the difference right away.”
Sadly, Maria recently got the news that Humira will no longer be covered in Sweden starting in August, so she will either have to pay out of pocket or find another medication.
“You can imagine how that feels. Humira has been my trusted friend since 2008, managing my Crohn’s and RA so well. Hard to think of life without it,” Maria said with a tearful emoji.
Kenzie: “I’ve been on two different biosimilars of Remicade. Inflectra was seamless—no issues. Then, a few years later, I got new insurance, and they made me switch to Avsola, which I had an allergic reaction to. No allergic reactions to Remicade or Inflectra, after being on them for more than six years. Now I’m on Cimzia injections (not a biosimilar) because it’s safe for nursing and that just seemed like the better option for me right now. I’ve only been on Cimzia for 10 weeks, but so far, my Crohn’s and RA seem slightly better.”
Audrey: “I switched to a biosimilar (Inflectra) in January 2022. I got pregnant in June 2024 and delivered a healthy baby boy this March. No disease issues thus far.”
Tara: “I was on a biosimilar when I conceived and throughout my entire pregnancy. I’m on Hulio and everything went well. I stayed in remission throughout the pregnancy and postpartum.”
Amanda: “I was able to conceive and am currently pregnant on a biosimilar. Everything is going great, thankfully I was on Humira for about six years and then got the dreaded letter to switch. I went on Hyrimoz at the end of last summer and was on it for five months prior to getting pregnant.”
Lauren: “I conceived and was pregnant with my now 3-week-old all while on Inflectra. I stayed in remission the whole time.”
Katie: “I was able to conceive while on Avsola, a biosimilar to Remicade. I haven’t experienced any issues related to pregnancy. I did develop some antibodies though and had to escalate my dose while pregnant. I also take premeds of Solumedrol and Benadryl before every infusion now. I got hives during the Avsola infusion while I was pregnant.”
Erica: “My doctor wouldn’t appeal it. I was put on Amjevita. Thank goodness and knock on alllll the wood…it’s been going well. I haven’t noticed any difference in symptoms. It’s been a little over a month, so I pray it stays that way.”
Jessica: “Conceived and pregnant on Inflectra infusions. I just had a healthy baby girl one month ago, and I’m now breastfeeding. No problems at all.”
Marla: “I switched to Hyrimoz while pregnant and I did not notice a change. However, I will say I’ve been in remission since getting pregnant with my first child and I don’t always take my medicine on time, so I don’t know if the transition was seamless because the medicine is truly fine or if it’s because my body just does well while I’m pregnant and breastfeeding (which I basically have been the past four years having three babies). I will say it’s an ABSOLUTE nightmare trying to get my medication each month. Constant bills I’m having to fight and constant new prescriptions and prior auths from my doctor for the SAME medication. It’s literally unreal. I blame that on CVS Specialty pharmacy.”
Amanda: “While I was pregnant, my OB appealed because insurance would no longer cover my Delzicol for ulcerative colitis. I won but was only allowed to stay on it until I delivered, then I had to switch to a generic mesalamine.”
Christine: “Pregnancy is what got me a temporary appeal. Once the baby was born, I had to switch, but it was peace of mind not having to make the transition during pregnancy. I was anxious that it was just a regular infusion, there wasn’t a loading dose or a slow rate or anything. They just infused the Inflectra the same way they infused the Infliximab. About two years after making the switch, I had to go from every 7 weeks to every 6, but I will never know if it was due to the biosimilar or if after 10 years on a biologic/biosimilar, my body just needed the drug at more regular intervals.”
Danielle: “I was pregnant (in remission), and my GI decided that was the correct time to switch me to Inflectra from Remicade…it did NOT go well.”
Jordyn: “I found out I was pregnant around the same time I had my first biosimilar infusion. I went through my whole pregnancy on the biosimilar and only noticed an uptick in symptoms around 10ish weeks, which a course of steroid foam resolved. Postpartum is when I noticed the return of symptoms the most. After 2 or 3 infusions (I get them every 4 weeks) with no improvement, I asked for an appeal, and it was granted for me to go back on Remicade.”
Natalie: “I got pregnant the month after switching to Avsola. I made the switch November 2022 to the biosimilar and found out I was pregnant December 29th. Pregnancy went fine, delivered in August 2023, all my problems started in February 2024. I went back on Remicade at that point because my GI suspected I had serum sickness for months on end, and to this day, they still aren’t sure if the serum sickness initiated my problem of Crohn’s attacking my joints.”
Angie: “We were told we would have to switch, but the doctor office contacted them, and they will be covering me at least until September for Humira…then we will renew the prescription and hope that it will be covered, again.”
Jasmine: “I’m on Avsola (biosimilar for Remicade) and I wasn’t trying to get pregnant, but did, and had a perfectly healthy pregnancy.”
Allie: “My specialists appealed saying I was going through fertility treatments and then insurance approved my Remicade for another year.”
Malea: “I got my insurance letter recently and have been meaning to reach out as I remember your Humira nightmare. I have not appealed yet, partly because my GI office is incredibly dysfunctional and hard to get ahold of. I am on Stelara, which is the first thing to have kept my Crohn’s in remission and they want me to switch to Selarsdi, which I can not find any patient experiences/anecdotal evidence about.”
Georgia: “I was on Humira last summer when Accredo tried to switch me to a biosimilar without notification. I had a letter saying that my Humira was still covered. I worked with my GI who told me they are seeing this a lot and if the person doesn’t push back, they just switch them to a biosimilar. But, if the person pushes back, the GI calls Accredo with a code (DW1 Brand Medically Necessary) to block it. That’s what I did, and they therefore had to send me my Humira since my insurance was still covering it. I want to let others know in case they have a prior authorization from their insurance saying they will cover Humira, despite the pharmacy trying to switch them!”
Jessica: “I so appreciate you talking about this. For my daughter, I went to refill her Humira, and insurance said the doctor allowed the switch. I asked the doctor, and they said no…it’s insurance. I had to use one of my daughter’s biosimilar pens while mine was being shipped, and I noticed more pain and burning. I advocated for my daughter to be on brand name only and they approved the request. When it came to my biologic, my letter had the same wording and once again it was insurance, not my doctor.”
Jessica’s GI said despite her being in remission for so long, she would need to try the biosimilar, then if any symptoms occurred then they could fight for return to the originator drug.
The Emotional Toll of a Forced Switch
For many patients, switching medications, especially after long-term remission, can trigger anxiety, mistrust, and a profound sense of vulnerability. Here are a few of the emotional and psychological responses patients may face:
Fear of Flare-ups: Patients often fear that a new medication might not work as well, risking disease recurrence and potentially hospitalization. So many of us have been relying on our biologic as a crutch for several years if not decades, it’s worrisome when you find a medication that works and have to change simply because insurance decides it’s necessary.
Loss of Control: Being told to switch due to non-medical reasons (like insurance mandates) can feel disempowering.
Medical Trauma: Those who’ve experienced years of instability before finding an effective treatment may associate medication changes with setbacks and suffering.
Distrust in the System: Patients may feel like financial decisions are being prioritized over their health and well-being.
How to Comfort and Support Patients Through the Transition
Healthcare providers and care teams play a critical role in guiding patients through these difficult changes. Here are some key strategies to help:
Educate With Compassion: Clearly explain what biosimilars are, how they’re tested, and what the current evidence says about their safety and effectiveness in IBD. Emphasize that switching is based on clinical research and real-world data, not just cost. Have discussions about biosimilars with patients in clinic even if they haven’t received a letter in the mail yet so they are prepared.
Validate Their Concerns: Avoid minimizing fears. Instead, acknowledge them openly. Saying, “I understand why you’re anxious about this” creates space for honest discussion and trust-building.
Advocate When Necessary: If a patient is stable and deeply concerned about switching, advocate on their behalf. Some payers allow exemptions if a provider makes a strong clinical case for staying on the original biologic. It may take extra paperwork, but the effort can mean everything to the patient, especially for pediatric patients and women who have family planning considerations.
Encourage Peer Support: Connecting patients with others who have made similar transitions can provide reassurance and reduce feelings of isolation. Patient communities, both online and in-person, can be powerful.
Navigating the Complexity of Informed Consent
True informed consent means patients understand not just the science, but the context of their decision. It’s more than ticking a box—it’s about creating space for dialogue, questions, and partnership. When I received the letter saying Humira would no longer be covered, I alerted my GI team not to sign the new script, as that gives the pharmacy/insurance the ability to switch you. A biosimilar is not able to be prescribed until your doctor signs off on it, remember that.
A thoughtful approach might involve:
Discuss what will happen if symptoms worsen after switching. My GI called me multiple times to comfort me and even prescribed a couple of Xanax pills to ease my anxiety leading up to the switch.
Review the process for switching back (if possible). Have a game plan in place so you’re not scrambling if you notice a change in your health.
Ensure patients know they won’t be left to manage complications alone. Support every step of the way makes all the difference.
Research articles to help you feel informed about biosimilars
An informed patient is an empowered patient. I did some research to help do the homework for you. By reading the articles below you should feel better educated on biosimilars so you feel more comfortable with the switch (if it’s a necessity) and about discussing this further with your care team:
Switching from a biologic to a biosimilar can feel like stepping into the unknown—but it doesn’t have to be done in fear or isolation. With transparency, empathy, and collaboration, patients can be empowered to make informed decisions, feel supported during the process, and maintain confidence in their care.
While some people feel more confident switching from a biologic to a different drug class (for example, Humira to Skyrizi or Stelara to Entyvio) to dodge the biosimilar, others are fearful of building up antibodies to a drug class that is otherwise working. You must weigh the pros and cons and do what you feel most comfortable doing. It’s important to remember it’s only a matter of time until all biologics for IBD have biosimilars, so by switching drug classes you are most likely just delaying the inevitable.
If you are planning to become pregnant or you are currently pregnant and on a biologic or a biosimilar please check out the PIANO registry so you can help pave the way for future IBD families and contribute to research so we have more information about the safety of these medications in pregnancy.
The science behind biosimilars is promising. But the human side of medicine—the fear, uncertainty, and trust involved in change, must be just as carefully managed. I hope after reading this article you feel less alone and supported in your personal health decisions.