The moniker “IBD Mom” is commonly used in the patient community. As a mom with Crohn’s disease who has three children, I focus a great deal of my advocacy efforts on family planning, pregnancy, and motherhood. But I recognize the decision and choice to have children isn’t for everyone. Studies on voluntary childlessness among people with IBD suggest a higher prevalence compared to the general population. Research has indicated that concerns about health, the impact of the disease on parenting ability, and the potential genetic transmission of IBD are significant factors influencing this decision.
So, what about the women who make the personal and often emotional decision not to have children or who didn’t have the option to choose, due to health complications? This week on Lights, Camera, Crohn’s a look at being childfree and the many factors that may deter people from becoming parents. You’ll hear from several women in the IBD community about their decision.
Key factors that influence being childfree
Disease Activity: Active IBD puts a halt on family planning, as women are told to be in remission 3-6 months prior to conception. The unpredictability of the disease can make finding the right timing to have a baby tricky. If a woman conceives while flaring, there is a much greater likelihood of flaring during pregnancy.
Medications: Some of the medications used to manage IBD can pose risks to a developing fetus. If a woman finally finds a treatment protocol that gets her IBD under control it can feel daunting to stop and risk losing remission.
Surgical History: Surgeries for IBD, especially those involving the intestines and rectum, can affect fertility and pregnancy outcomes.
Genetic Considerations: IBD has a genetic component, meaning there is a risk of passing the disease on to offspring. While this is a major deterrent for many, it’s important to understand what that risk is. For Crohn’s, there’s a 7% of passing on your disease and even less for ulcerative colitis. When both parents have IBD that number goes up astronomically.
Physical and Emotional Well-Being: Managing IBD is physically and emotionally demanding, trying to imagine what it is like to care for yourself and take care of a child can be overwhelming for many.
Firsthand accounts from the patient community
Kat: “This doesn’t mean I won’t change my mind in the future, but my health has had a huge impact on why I have decided not to have kids. I think a big part of not wanting to carry a baby anymore is because of the trauma my body went through when I was sick in my 20s.”
Rachel: “I was diagnosed with Crohn’s disease almost three years ago, and I’m on my second biologic. I’m 25 and have decided that I don’t want to carry my own children. Due to the currently unknown effects of biologic drugs on development, but also the risks for myself coming off a biologic and flaring. I have also considered the complications of having a c-section before or after other potential abdominal surgeries and the complications from that. The main one for me though is also the genetic chance of passing IBD on to my kids. I have always been open to adoption anyway and have decided this is the route I would pursue if I do decide to have children.”
Kate: “We are going through fertility treatments after five years of secondary infertility and I chose to stop to start Rinvoq and save my rectum. I am not having my eggs retrieved and frozen in the hopes that we find a gestational carrier for our embryos.”
Kendall: “I am 30 and single and haven’t made the firm decision to be childfree, but as I get older and my Crohn’s disease gets more challenging, it’s definitely something that I’ve been questioning. Wondering if I will have the health and energy to be able to take care of myself and my kids. I worry about the impact of pregnancy on my body and of course finances are also a consideration.”
Alesha: “I’ve questioned being a mother. I’m 33 and I was diagnosed with Crohn’s in 2022. After having a perforated small intestine in 2015, an ostomy for 6 months, and the reversal in 2016…only to suffer with so much pain from the scar tissue being so narrow. I’d visit the hospital a few times a year and try to work through the pain. Now, I’ve been on Stelara for a little over a year. It’s been helping, it’s just hard to be told that the medication will be lifelong. While I desire to be a mom, I just don’t know how my body will respond.”
Liz: “I have chosen not to have kids for many Crohn’s reasons: Having to come off meds to protect pregnancy, the risk of flares and them causing infertility anyway (my periods always stop in a flare), the massive risk from common childhood illnesses, adhesions due to surgery and just the added stress and time needed to devote to a kid to raise them is something I just can’t do on top of a career as a doctor.”
Meredith: “I’m currently in this situation now. My husband and I held off having kids until we were ready (different components here—moving, reaching career milestones, enjoying our lives as they were, but in the past few years we felt we were ready except my body wasn’t. I had a terrible flare that knocked me on my ass for about a year and then I was put on my methotrexate and was told I could not become pregnant, or I would need a medical abortion. I’ve since gotten off that medicine but was told to hold off trying until after my colonoscopy. I had another small flare, and my GI wants me to wait until I’m healthier. He says, “healthy mom, healthy baby” and I don’t think he’s wrong, but it isn’t what I want to hear. So now, I’m just waiting to see what happens.”
Sarah: “Not sure what I’m looking for because I have two kids, but I had them prior to my Crohn’s diagnosis at age 30. The diagnosis prevented us from having more children. We always planned on four kids, but because of my diagnosis, we didn’t continue to try and only have our two that I had before developing Crohn’s.”
Belinda: “We’ve decided not to have any kids. I know my history with my Crohn’s hasn’t been as bad as some other ladies who would struggle to conceive and carry a child. I might have been fine to. I had two resection surgeries, at age 24 and 39. The first one was very traumatic, and I was very sick for many, many years. I just didn’t ever feel I wanted to take a risk to “rock the boat” as I’m always trying to keep my health stable. I didn’t feel I had it in me to manage a potentially difficult or risky pregnancy or bad flare after the baby. I do think there might be other reasons why we’ve decided not to have kids, so it might not be fair to blame it all on my Crohn’s. I’ve never had the urge or yearning to be a mom. It’s very prevalent in my family, too. Three out of four cousins on my dad’s side have Crohn’s and my mom’s cousin does, too. The nature of the world, healthcare issues, and so many other issues make me wonder if it influences would-be mothers. Our health is already such a scary unpredictable element of our being…who has the capacity to navigate it all?”
Kelsey: “I’m childfree by choice! I’m a professional auntie. I was diagnosed with ulcerative colitis after I had already made that decision, but it has 100% solidified it. I’ve watched my other childfree friends waiver with their decisions and some choose to have children later in life.”
Deanna: “I got married in October and my husband and I talk about this a lot. I never expected I’d be childless, but I don’t have a strong drive to have children either. The fact that the decision was made for me is something I am trying to navigate emotionally.”
Jessica: “I was always on the fence about children, even when meeting my partner six years ago when we were 25. I decided a few years ago that I did not want to have children. While there were a few factors in my decision, my ulcerative colitis was a big decision to choose not to. Stress and lack of sleep (I need at least 8 hour a night) are a prime duo for flare ups for me. I knew that if I was going to be lacking sleep in the many stages of childhood, and stressed many times, I wouldn’t be able to care for myself, and therefore wouldn’t be able to truly take care of children. I know there are so many moms out there with IBD or another autoimmune disease that are rocking it, but this was the right choice for me.”
Courtney: “To be honest, having children was just never something that was on my mind in my twenties and thirties. I was diagnosed with ulcerative colitis in college and had a colectomy in graduate school. During most of that time, I was in a 10-year relationship. Towards the end, it became clear we had different ideas about where our futures were headed. He wanted a traditional family life in a small town, and I wanted to focus on my career and stay close to my medical team in an urban area.”
Ashley: “I’ve been really scared due to medical trauma and not feeling ready to trust my body. It’s hard because I have a strong desire to have a child, but it would also mean putting myself back into situations that genuinely scare me.”
Kaycie: “My IBD is one of the several reasons I decided to be childfree. I was so sick throughout my early to mid-20s when I finally went into remission in my late 20s, the last thing I wanted was to risk falling out of it to have a child. I’m in my mid-30s now, living abroad for work, traveling all the time, and able to have the freedom I craved in my 20s when I was chained to a toilet with my ulcerative colitis. A child just doesn’t fit the life I’ve built, and my husband and I are happy with that choice.”
Lauren: “I miscarried many years ago and was told I was high risk at the time and that it would be a battle to get pregnant and carry full term. After being diagnosed with Crohn’s, I didn’t think it would be healthy to try further with my body. With so many flares and surgeries, we decided if we had children we’d adopt. It was like grieving a major loss of something I’d always wanted. I love my life and my marriage. I had a few great years of remission and have been flaring for about one year now. I’m not comfortable adopting when my health is so on and off. I don’t think it’s fair to a child or my husband to not always be present.”
J: “For me, every time we were going to try for a second child, something my with health would come up. I’ve had a collapsed lung, broken rib, inflamed pleural pace, and IBD flares. Between all those health setbacks, coupled with chronic fatigue, it felt like I couldn’t get to a place healthy enough to support a second pregnancy and even if I could, I wouldn’t have the energy to survive the first three months postpartum with such little sleep going on. So, we opted to no go for more and be as present as we could for our existing child.”
Casey: “My husband and I have had a to delay trying to conceive due to a flare and were going to delay trying even further as I just had to switch from Humira to the biosimilar, Hyrimoz. I don’t want to be pregnant while navigating a chance in medication in case it doesn’t work the same.”
Hannah: “There is still quite a lot of taboo around being childfree and it isn’t something I feel I can share with everyone. I don’t have a strong desire to be a mother. It’s difficult to know how much of that is due to my challenging childhood and adolescence due to my Crohn’s. I have a vivid memory from when I was 11 years old watching my siblings playing outside from the bedroom window and of being very upset that I didn’t have the energy to join them. That memory is very poignant and painful for me. It’s one that has been at the forefront of my mind as a 34-year-old woman as I decide whether to remain childfree. I fear repeating that feeling of being at the periphery but this time as a mother, rather than as an 11-year-old girl. Another fear is that I might pass on Crohn’s to my child. While the risk is small, I would find that difficult to bear.”
Lizzy: “I’ve had IBD for almost two years. I am on Remicade and methotrexate. Since methotrexate can’t be taken during pregnancy, it would be concerning number one of having to switch to a pregnancy-safe alternative and hope it works as well as my current regimen. Additionally, periods make my Crohn’s symptoms worse, so I haven’t had a period in over a year due to birth control. Having to get off birth control and deal with horrible symptoms sounds miserable. I get sick when I don’t sleep, and it wouldn’t be fair to always make my partner get up in the middle of the night. I am also gay so going through the stress of IVF or artificial insemination when trying to maintain Crohn’s remission would be stressful.”
Sexual and reproductive considerations
Amy Bugwadia is an MD student with scholarly concentration in medical education/health equity and social justice at Stanford. She collaborated with some IBD patients and clinicians and authored a paper about sexual and reproductive health considerations. She says, “while we were writing and listening to patient feedback there were a few salient themes:”
Mis and dis-information
Stigma: patients being too shy or not knowing if this is a topic that they can or should talk to their GI about
Confusion about language: Doctors saying “you can’t get pregnant while on this med”—do they mean “difficulty getting pregnant” due to potential infertility or “should not get pregnant” due to potential medication impacts on the fetus.
Outdated information: Many patients (especially when young) have been on the certain medication for a long time, but as time has gone on, we have new/updated data on safety profiles that not all patients are up to date on, especially relevant for pediatric patients as they transition to young adulthood.
Voluntary childlessness or being childfree among individuals with IBD is a multifaceted issue influenced by health concerns, genetic considerations, quality of life, and psychosocial factors. As you heard from several IBD women, the decision to remain childfree is often a carefully considered and personal choice determined after talking with healthcare providers, significant others, family, and support networks. I hope after reading this you feel less alone if this is your reality—whether it’s something you’ve always wanted or if it’s a decision you struggle with.
It’s no surprise as a non-profit The Crohn’s & Colitis Foundation relies on donations to fund research to find cures for Inflammatory Bowel Disease (IBD) and sustain support programs for people living with Crohn’s and ulcerative colitis. But did you know there is a Do It Yourself (DIY) fundraising opportunity for anyone interested in raising money for the cause beyond their major campaigns like Take Steps and Team Challenge? This week on Lights, Camera, Crohn’s, here’s a look at how our community has risen to the challenge in the past and how you can get involved now.
How does DIY Fundraising Work?
If you’re interested in taking the reins and fundraising, you can create and manage your own fundraising activities based on your interests and motivation. The money you raise helps support research for finding a cure for) IBD. The Foundation staff offers one-on-one support, fundraising tools, and resources to help you along the way.
Michael Osso, President and CEO of the Crohn’s & Colitis Foundation says it is incredibly inspiring to see the Crohn’s and colitis community come together with such creativity and passion to raise awareness and funds for the mission to find cures and improve the lives of the 1 in 100 Americans with IBD.
“From walking 100 miles to hosting charity hikes in Alaska and livestreaming gaming events, our supporters have come up with innovative and impactful ways to turn their ideas into personalized fundraisers through our DIY program. I am deeply grateful for every person who gets involved because together we are unstoppable in our fight against IBD,” said Michael.
Melissa Scott serves as the National Marketing Manager for the Crohn’s & Colitis Foundation. She says volunteers have been hosting their own fundraisers since the Foundation’s inception. About four years ago, during the pandemic, the program was formalized, with a dedicated team, toolkits, and fundraising platform specifically for DIY fundraising.
“Every contribution, regardless of its size, plays a crucial role. The cumulative impact of our DIY fundraisers, big or small, is vital in our ongoing efforts to fund research and move closer to finding cures for Crohn’s disease and ulcerative colitis. Each fundraiser, by raising awareness and funds, helps us advance our goal of improving the lives of those affected by IBD,” said Melissa.
Inspiring DIY fundraising efforts
The sky is the limit and the options to raise money are, too. Oftentimes as IBD patients and caregivers, we may feel our well-being and health is out of our control. DIY Fundraising is a tangible way to make a difference and recognize how supported the IBD community is within your inner circle and among your peers. Not only are you raising money. but you’re raising awareness about your reality and educating others about IBD, which is priceless.
Stasia, an IBD warrior, hosted the “Alaska Hike for IBD Cures.” She made this happen by asking her network of friends, family members, and local businesses to donate in support of her mission and to join her on the hike. Stasia wants the IBD community to know that “Even if you don’t raise a lot of money that single dollar can pay for a test tube that might holds the cure.”
Robby founded “Gaming for Guts” 10 years ago. This is a team of online gamers who raise money for IBD and provide funds to support the Foundation’s mission. Robby says, “the first year we had two people participate, now we have a whole team and we’ve raised more than $20,000 for the cause.”
As a high school student with IBD, Hala used her love for baking to drive donations. She hosted a bake sale as part of her senior project. “I knew I wanted to do a bake sale and DIY is so customizable, it was perfect for me to raise funds in a meaningful way,” she said.
Ilie, Mack, Charlie, Lawson, and Thompson created “Dilworth Kids for Crohn’s and colitis Cures” and hosted a lemonade stand during the Dilworth Historic Home Tour. With the help of the Foundation, the kids had marketing materials to help get the word out.
How to learn more and get involved
As a trustworthy source in the IBD community, The Foundation is the driving force in the development of next-generation treatments and personalized medicine for IBD. The Foundation has played a role in every major research and treatment breakthrough in IBD. DIY Fundraising is a vital tool in helping the Foundation continue its quest for better treatments and cures, while also allowing for our voices to be heard. By getting creative, taking the plunge, and seeing where it takes you, you may feel more empowered and supported on your patient journey.
You can learn more about the Foundation’s DIY program (including livestream and gaming opportunities) here. Interested in getting started? Email the DIY team directly: diy@crohnscolitisfoundation.org
Crohn’s disease and ulcerative colitis can cause symptoms both in and out of the gut. When our disease wreaks havoc on other parts of our body, outside of our intestines, it’s known as an extraintestinal manifestation (EIM) or complication. Did you know, according to the Crohn’s and Colitis Foundation, anywhere between 25-40% of people with IBD experience some type of EIM? EIMs arise in the joints, skin, eyes, bones, kidneys, and liver or as anemia. This week on Lights, Camera, Crohn’s a deep dive into the heavy toll of living with not only IBD but the EIMs that come along with them and how more than 30 patients manage these issues that can significantly impact the quality of life and overall health of IBD patients.
One of the most interesting quotes from a patient was that while one man doesn’t like EIMs, he’s grateful for them because that’s often the only time family, friends, and medical providers can see with their own eyes what a serious illness IBD is. It’s heavy, but it makes sense. IBD is so much more than a bathroom disease and EIMs go to show how severe Crohn’s and ulcerative colitis can be and how this is a full body disease.
The most common EIMs associated with IBD
Joint problems: This is the most common EIM and affects around 25% of IBD patients. The pain normally occurs in the knees, ankles, and wrists, but can also happen in the spine in the form of ankylosing spondylitis. For many of us, our biologics or biosimilars are approved to treat both IBD and rheumatoid arthritis and this can help alleviate joint pain.
Skin Conditions: The two main conditions are Erythema nodosum and Pyoderma gangrenosum. EN is characterized by tender red nodules that usually occur on the shins. PG is a more severe skin condition that causes painful ulcers. Those with IBD also have a greater chance of developing skin tags, anal fissures, and fistulas, both Enterocutaneous (from the intestine to the skin) and Perianal (around the anus that can drain blood, pus, and/or stool.
Eye Disorders: When those with IBD deal with red eyes, pain, and vision problems, uveitis and episcleritis tend to be the culprit.
Kidney complications: Medications tend to cause this, and serious kidney complications associated with IBD are rare, but still can happen in the way of kidney stones, hydronephrosis (an obstruction of the ureters, which connect the kidney to the bladder), and fistulas (abnormal connections between the intestines, bladder, or ureter). Amyloidosis (an abnormal deposit of protein in the kidneys) and Glomerulonephritis (inflammation in the kidney that limits its ability to filter properly) can also occur.
Liver and Biliary Tract Diseases: Primary sclerosing cholangitis (PSC) is a serious liver disease is most commonly seen in conjunction with ulcerative colitis. This is often discovered when lab works show liver markers are out of whack and it’s diagnosed with a liver biopsy to determine the stage and level of severity. Fatty Liver Disease, Hepatitis, and Gallstones are also considered EIMs.
Bone Health Issues: Osteoporosis and osteopenia can result from years of chronic inflammation, steroid use, and malnutrition. It’s a good idea to get a baseline DEXA bone scan and to get scans periodically to make sure you’re not experiencing this.
Lung Issues: While this is less common, lung involvement can include airway inflammation and interstitial lung disease.
Managing EIMs along with your IBD
Managing and treating EIMs is no easy feat and often necessitates a multidisciplinary approach, including your gastroenterologist, rheumatologist, dermatologist, and other specialists, depending on what organs are affected. Treatment strategies might include non-steroidal anti-inflammatory drugs (NSAIDs), immunosuppressive medications, and biological therapies which are tailored to reduce inflammation and manage symptoms.
You may wonder if there’s any way to prevent EIMs from happening in the first place. There are several strategies that can help reduce your risk, but much like anything with IBD, don’t blame yourself if EIMs keep happening to you and feel out of your control.
Effective IBD Management: Controlling your IBD through appropriate medical therapy is crucial, whether that’s in the way of aminosalicylates, steroids, immunomodulators, and biologics/biosimilars. The goal is to reach and sustain remission of your IBD, which can help reduce the risk of EIMs popping up.
Communicating when you see a change: Once you notice a possible EIM, it’s imperative you share this with your healthcare provider. Early detection and treatment of EIMs can prevent them from getting more severe. A simple message on the Portal to your GI addressing your concern or worry helps alert your doctor so they can take the appropriate measures before symptoms spiral out of control.
Lifestyle Modifications: Smoking is known to worsen the course of IBD and increase the risk of EIMs, especially in Crohn’s disease. Consulting with a dietitian who specializes in IBD can help ensure you are receiving adequate nutrition and getting regular exercise can help reduce inflammation, improve bone health, and enhance your overall wellbeing. Speaking of bone health, calcium and vitamin D supplements can help counteract the lasting effects of steroid use and malnutrition.
Collaborative Care: By branching out from your GI and seeking care from specialists, you have the best bet of ensuring EIMs are treated promptly and effectively. Talk with your GI about the potential signs and symptoms of EIMs so you know what to watch out for and have a game plan in place if one were to arise to feel more in control.
Medical gaslighting and EIMs
Unfortunately, far too many patients and caregivers feel symptoms are dismissed or not taken seriously by healthcare providers, which can be particularly discouraging and frustrating.
“I had a tough time getting my consultant to take me seriously. The eye problems were “probably just bad eye strain,” the mouth ulcers were “maybe the cups in the office not properly being cleaned, and the rashes were “probably a reaction to laundry detergent or maybe insects getting on my clothes while they are on the clothesline outside.”
Here are some helpful strategies to help you speak up in these situations and feel empowered to advocate for your health effectively:
Document Your Symptoms: You may think you’ll remember what’s going on, but life with chronic illness gets hazy and when we think back, we can lose sight of the actual frequency and intensity of what we’re going through. A detailed diary will help provide concrete evidence to discuss with your healthcare provider and may even help assist in identifying patterns that are relevant to your diagnosis and treatment.
Seek Second Opinions: If you don’t feel listened to or heard, don’t hesitate to get a second opinion, and find a provider you jive well with. Each doctor has varying levels of experience with IBD and EIMs, find the person who best understands your personal situation and is willing to get you to where you need to be, rather than dumbing down or belittling your experience.
Be Prepared for All Appointments: Write down a list of questions and concerns before your appointments. Bring your symptom diary and any other relevant medical records. By being prepared, you can better focus and ensure that you’re capitalizing on the one-on-one time you have with your doctor while you’re face to face.
Bring an Advocate: Having a trusted friend or family member at your appointment can provide support and help ensure that your voice is heard. That person can also help remember details on the appointment that you may not.
Be Clear and Assertive: There is a delicate balance between being assertive about your concerns without being confrontational. Be descriptive and transparent about the impact your symptoms have on your daily life, paint as clear a picture as you can and explain why it’s important for these symptoms to be addressed.
Educate Yourself: By understanding what EIMs are ahead of your appointment you can feel more confident about asserting your concerns and how best to improve your health. If you’re able to “talk the talk” with medical language about your condition, your healthcare professional will be more apt to listen.
Formal Complaints: If you repeatedly feel as though you’re dealing with an unprofessional doctor who has a dismissive attitude, or if you feel your care is compromised, it may be necessary to share a formal complaint with the medical facility.
Let’s hear from IBD patients and caregivers
Leah daughter was diagnosed with Crohn’s when she was five.
“Little did we know our most difficult days would come a few years later and be due to an extraintestinal manifestation of her IBD. It started off as bruises on my daughter’s shins. I thought it was related to her sledding on her knees with the recent snowfall. Unfortunately, I had never learned about Erythema nodosum being related to IBD and would later learn this is what she had. The spots on her legs grew and grew. They eventually got raised and painful. I emailed our GI nurse and thankfully she instantly knew and sent us for stat labs. My daughter was on Humira and wasn’t in remission, so the drug was increased. Week by week things got worse and more painful. The redness and swelling covered her entire shins. The bumps spread to the bottom of her feet and were extremely painful. Her feet swelled and she was crying in pain and no longer able to walk on them.”
Leah ended up taking her daughter to the ER where she got steroids and started on antibiotics as it looked like the spots had turned into cellulitis on her feet.
“I was not prepared that EN could be associated with IBD. I wish I had known earlier, so her condition could have been treated more aggressively from the beginning. It was many months before she healed, and her maintenance medication was switched.”
Emilie– “This is such an important topic and I wish it were discussed more! Most of my UC complications have revolved around extraintestinal manifestations (as opposed to typical UC symptoms). I have had arthritis and uveitis and for me, extraintestinal manifestations always come first, before a typical flare and always stay long after the typical UC symptoms have resolved. At times, I’ve just had extraintestinal manifestations without any typical UC flare symptoms. The most frustrating part about EIM symptoms is that most GI doctors aren’t super familiar with them and only think they happen after a UC flare. Thankfully, I’ve been followed by a rheumatologist since I was diagnosed (because I had EM symptoms long before I had typical UC symptoms and saw a rheumatologist first). My rheumatologist is always like, “we follow people with these symptoms to see if they develop IBD” and many of my GI doctors have said, “this can’t be because of your UC.”
Dina was diagnosed with UC in January 2022 after experiencing IBD-related symptoms six months prior. Since then, she’s had pneumonia, mono, CMV, RSV, and other illnesses. She went from weighing 150 pounds to 120 and was so weak she could barely walk. She was switched to Entyvio/Rinvoq as a combo therapy along with an anti-viral drug used to treat HIV to try and keep the CMV virus at bay. The CMV made her liver markers skyrocket, and it was discovered she has Stage 1 PSC, in addition to everything else.
“I consider this a blessing because once I went back on the full dose of anti-viral my liver counts normalized. We never would have known about the PSC until it got severe or at a later stage. My GI said he’s never seen PSC in this early stage, so I’m grateful we can start earlier than most to monitor it.
Lynette-“I’ve dealt with many EIMs. To manage my anemia, I take iron and having a hysterectomy helped. For my kidney stones, I stay hydrated with electrolytes daily. I had surgery for hemorrhoids and fistulas. I’m on medication to manage my joint pain and use my heating pad. I use a special toothpaste to prevent cavities and I floss daily. I do everything I can to reduce stress and anxiety—from breathwork, to meditation, and openly communicating with my family.
Madison-“My personal experience is severe joint pain and swelling, as well as erythema nodosum. My IBD flares typically begin with joint pain. At times, it can be so severe I can’t walk up and down stairs because my ankles are so swollen. When I was first diagnosed with Crohn’s, in addition to my joint pain, I started to develop red tender bumps all over my legs up to my knees. They were so painful to touch, and they were diagnosed as Erythema nodosum which only occurs in about 10-15% of Crohn’s patients. Once we got my IBD under control and found the underlying cause of my joint pain and erythema nodosum they thankfully got better.”
Myisha- “I experience inflammation in my eyes three to four times a year. I also deal with osteoarthritis. Mentally, I’ve checked out on my Crohn’s awhile ago. I just take it day by day. I have eye drops that I have to use daily to help with inflammation, but osteoarthritis is painful and some days I want to cut my limbs off. I always try to remind myself that someone out there has it worse and today might be a high pain day, but the darkness doesn’t stay around forever, eventually the sun will shine again, and I’ll have a low pain day.”
Christopher- “I’m 46. I was diagnosed with Crohn’s about two years ago. Three years before that I began having panic attacks and anxiety out of nowhere. I went from never having anxiety or panic to multiple incidents per week. At the same time, I had new joint pain in my knees, and developed arthritis in my shoulder joint as well as mild lower right quadrant pain. Now, looking back, these were all related to systemic inflammation from the undiagnosed Crohn’s. Now that I’m in remission, it’s all gone away.”
Vern– “OMG EIMs!?! I have so many. Along with Crohn’s, I have developed Gilbert’s Syndrome, short gut, Reynaud’s, rigors, kidney stones, skin problems, anemia, B12 and vitamin D deficiency, joint pain, fissures, fistulas, and hair loss. There’s not much to do when it comes to Gilbert’s, Reynaud’s, rigors, or skin…but with kidney stones I drink a lot of water everyday plus cranberry juice or tea every once in awhile. To manage my anemia, B12 and D, I take easily soluble supplements and B12 shots every month. I take Tylenol to manage my joint pain and rest. The fissures and fistulas have a mind of their own, so not much I can do until it’s taken care of surgically if it gets bad enough. The hair loss is from medication and even when I tried different treatments (home remedies) nothing worked until I was off the medication.”
Pao-“I have been experiencing skin issues for the last year and a half. I have a lesion under my armpit, behind my ear, and a gangrenous epidermis, which is healed. I had a biopsy on the lesion and then a corticosteroid cream healed it. The lesion on my ear won’t go away after months of putting cream on it.”
Kerry-“I deal with intense joint and muscle pain all over my body. My left hand got so swollen at one point that I tried to learn to write with my right hand. This was during my initial diagnosis. Once I started on Remicade it helped and now my joint pain is an indicator of disease activity for me. I log symptoms using the Wave app, I increase my rest, and use diclofenac gel as a topical analgesic. I also see a rheumatologist who has experience treating other IBD patients.”
Rocio: “One of my most debilitating and constant EIMs I’ve had over the last 20+ years is iron-deficiency anemia (IDA). The fatigue levels I live with are beyond frustrating. I know the disease itself can add to my fatigue, but even when at my healthiest, I’m constantly tired. And it’s the kind of tired no on understands. I’ve received countless IV iron infusions for my IDA as I can’t tolerate oral iron due to my previous history of chronic constipation. Fortunately, infusions and I’m able to go months without iron, but there have been times where I’ve received 5 infusions in 1 month – yikes!”
One of Rocio’s other debilitating EIMs is uveitis. She says it is truly one of the most excruciatingly painful manifestations.
“Despite having a high pain tolerance due to chronic illness, uveitis has been one experience I don’t wish upon anyone. And uveitis can progress to glaucoma or vision loss. I did have glaucoma along with my uveitis, but we treated it immediately. Due to recurrent uveitis flares and limited treatments that worked for me, I dealt with uveitis for nearly 3 years. The ophthalmological EIMs that can occur with IBD are not one to take lightly…we need our vision!”
The earliest EIM Rocio experienced were perianal fistulas – a common type of enterocutaneous fistulas. Unfortunately, she did not receive proper care initially, or her actual IBD diagnosis, for five years. She could have suffered far less had her fistulas been identified as an EIM of Crohn’s disease.
Jennifer-“So many doctors are just unaware or unwilling to see extraintestinal manifestations for what they are. When I was in my late teens and struggling with depression and a ton of stress in my first year of college, I was shamed by a doctor and told (without any testing) that I had herpes. Mind you, I had never been sexually active and never had symptoms before this point. I was in extreme pain and had painful ulcers from my mouth to my anus and genitalia. I left the appointment in tears and wanted to die. It was only years later that I learned of external manifestations of Crohn’s and had a doctor confirm that is what happening all those years earlier.”
Jennifer says she had far too many unpleasant encounters with doctors over the years. From doctors telling her that she was just a bored homemaker (because he felt my complaints were made up) to dentists shaming her in front of her kids (because her mouth health was in his opinion from lack of hygiene vs. effects of Crohn’s disease).
“I was also told by a GI doctor once that if my Crohn’s disease flared while pregnant that I should just have an abortion (for a pregnancy that I very much wanted). This is not a commentary on my stance on abortion, but rather the lack of empathy and respect that this male doctor had towards me, my health, and my choice in that moment.”
Becky- “Erythema nodosum is so scary and I had no idea what was happening to my legs. It was so painful to even walk. I’ve lived with Crohn’s for 30 years. I was admitted to the hospital and given steroids and the doctors drew black Sharpie circles around the red swollen lumps on my legs to see if they grew larger. I was there several days, and the doctor finally figured out what was going on based off my medical history. I was on steroids for awhile and then it finally cleared up.”
Liz- “Extraintestinal manifestations are one of the toughest parts of Crohn’s for me. I have joint aches, eye inflammation that is so painful and disruptive when it flares and chronic severe anemia. Each result in another doctor, another expensive treatment, and time not feeling well. Getting doctors to recognize that they are all connected is difficult as well.”
Anthony has lived with Crohn’s for almost 18 years and EIMs have been a big part of his journey. To him, they’re often a key indicator that a flare up is on the way and unfortunately EIMs have become a regular part of his life for the past decade.
“I get a lot of eye problems (swelling, overly sensitive to light, foggy vision). Once I woke up with my left eye swollen shut. I get a lot of ulcers on my gums, tongue, and in my throat along with rashes that break out on my arms, back, and hands. When I get ulcers, I have difficulty swallowing and need to consciously put effort into swallowing my tablets and often I’m forced to stay away from solid food and meals.”
Anthony goes on to say EIMs bring on depressive episodes for him, along with brain fog, and having issues concentrating and remembering.
“Some days I wake up at 4 or 5 in the morning with a cement block of sadness in my chest, preparing to go about a “normal” day and hoping not to feel the urge to burst out crying. Before I learned how to live with it and got mental therapy, I had to write almost everything down to the point of keeping a note on my phone with bus and train times that would get me to and from work or to various parts of the city because I’d draw a complete blank at times or couldn’t figure out the timetables. I am an engineer and almost had to give up my career because I couldn’t get through a workday.”
Deb– “I’ve had reoccurring Pyoderma Gangrenosum under the flange or baseplate of my ostomy to the point that the skin and tissue diminished and has now caused a very significantly sized peri stomall hernia. We haven’t landed on a treatment of late that has any amount of effect on the inflammation in my colon, so no hernia repair until we get the CRP way down.”
Courtney-“I’ve experienced blepharitis, which is an inflammation of the eyelid that may commonly be confused with pink eye. I’m not fully clear if it is an extraintestinal manifestation or side effect of immune suppression, but after 5 years “in the clear” it’s back. One of the few occasions when I actually “look sick” but feel fine. It’s treated with antibiotic eye drops. I saw a specialist who recommends a special cleanser with tea tree oil.”
Amanda-“During a particularly bad Crohn’s flare, I developed Erythema nodosum. They were painful welts that went up and down both legs. My legs got so swollen and covered with welts that I couldn’t bend them to walk. It was incredibly painful and difficult to need help just getting out of bed. They took awhile to go down and left bruises all over my legs. No one ever mentioned this to me as a possibility, so I didn’t even think to contact my GI, but my local emergency room doctor pointed me in the right direction.”
Krista– “Oof. Alopecia. I lost probably 50-75% of my hair. Now it’s thicker than it’s ever been. Very strange. I also have experienced bursitis and inflammation in my knees, but that’s only flared up once since my IBD diagnosis.”
Melanie-“I was diagnosed with IBD when I was 12 and by 15, I could no longer walk upstairs due to Crohn’s-related arthritis. I went on Remicade which got me walking again but have since been looking for options. Sometimes my Crohn’s and Arthralgia flare together, but in my experience, when I get one under control, I start having issues with the other one which can make disease management a challenge.”
Tish- “I got Uveitis and must always be on the watch for signs of it now. It was misdiagnosed as an eye infection, and I was sent to the eye and ear emergency, but they also misdiagnosed it. Thankfully, I was able to see my ophthalmologist who correctly identified and treated it properly. I also have very dry eyes, so I always use drops to avoid it leading to another Uveitis flare up.”
Eliza– “I’ve dealt with bone density issues related to my ulcerative colitis. I now take a prescribed high dose of D3 and incorporate calcium and other minerals as often as I can into my diet. I have been getting DEXA scans since I was 19!”
Allison-“Skin!! Why are there no IBD-expert dermatologists anywhere?! Why can’t my doctors give me more information about extraintestinal Crohn’s related skin issues? Are we really suggesting bleach baths as the only path for resolution because that feels insane. I’m struggling to find the right resources to help.”
Stacey-“I developed Type 2 diabetes as a result of the inflammation in my pancreas. In addition to diabetes, I also have Rosacea caused by my Crohn’s. We first thought it was an allergic reaction to my Stelara. However, the Rosacea persisted after I stopped Stelara. I saw a Dermatologist who made the diagnosis, and I was then able to get back on it. Like many IBD patients, I also deal with dry eyes, dry mouth, fatigue, and achy joints.
Dana– “I’ve struggled with cutaneous Crohn’s (perianal and elsewhere) and oral Crohn’s, including mouth sores, gum inflammation, and recession. I’ve been prescribed a lot of various topical medications (tacrolimus, taclonex, steroids…just to name a few). It causes a huge gluteal cleft fissure and a lot of damage to my skin in the perianal area in general, which was resolved when I had my proctocolectomy surgery. They had to cut my rectus abdominis muscle to create a flap and place it in the area where they had to cut out all the tissue and skin. Regarding oral Crohn’s, I have steroid ointment that I use as needed for inflammation/sores and I’ve had three gum graft surgeries so far.”
Gabriella-“I have chronic urticaria and dermatographia that was triggered by a rare reaction to the carrier protein used in Humira and Remicade. The reaction hasn’t gone away despite stopping those medications, and despite taking Xyzal and Benadryl daily. I still have extremely high IgE levels. I had had all the major inflammatory skin conditions associated with Crohn’s as well: Erythema nodosum, Pyoderma gangrenosum, and just general infections from “normal skin flora.” I’ve had multiple bad IBD flares where I’ve experienced inflammatory arthritis in all joints from my hips down.”
Ben-“I was diagnosed with gastroduodenal Crohn’s and UC over 30 years ago when I was six. Back then, it started with Erythema nodosum, which led to a colonoscopy, when then ended in my first polyps removed and a diagnosis. I still have issues with it today. I also picked up an obscure kidney cancer about five years back. My oncology and GI teams feel it is related to my Crohn’s/UC somehow, as they don’t see this type of cancer in patients under age 80. Crohn’s also gives me severe anemia.”
Stephane– “After 15 years of partial obstructions, during which I amazingly enough, managed to avoid diagnosis or treatment, it was the obviousness of an extra-intestinal manifestation, my left ankle swelling for no reason, which marked the beginning of the end of my epic denial. Over the summer, my knees swelled too, and walking became painful and slow. By September, I couldn’t walk at night because of the pain in my joints and had to crawl to the bathroom. Finally appearing in the ER, sent by my GP, ankles, and knees puffy and swollen, anemic, malnourished and down 30 pounds, the doc only needed to glance at my chart and test results to give me a diagnosis of Crohn’s.”
Amanda-“Extraintestinal manifestations I’ve dealt with include mouth ulcers, inflammation of my eyes (so red!), joint pain (specifically knees and hands), TMD (no classic clicking or popping, just mass inflammation of the joint and muscles), eczema, anxiety, slow wound healing, fatty liver (non-alcohol, I don’t drink, I am a fitness and nutrition professional so I know my lifestyle is on point), and kidney stones.
Amanda manages this by having exceptional oral hygiene. She brushes and flosses twice a day and uses Orajel mouth wash. She sees an Ophthalmologist to ensure she doesn’t have damage to her eyes and uses Lumify drops to combat the redness. Amanda takes a curcumin supplement (primary bioactive substance in turmeric) for its anti-inflammatory properties, which may also help with joint pain. She uses a bite splint and warm compresses for her TMD and eczema patches on her face, around her ears, eyes, and neck. Amanda has two different prescriptions from her dermatologist to address this: hydrocortisone cream and fluocinolone oil. She also uses Skin Smart antibacterial eczema spray every night. To deal with the remainder—she practices stress reduction when and where she can, continues to focus on her diet and weightlifting and keeps her sugar intake low. She doesn’t drink alcohol and only takes moderate caffeine each day. She’s also hyper focused on micronutrients, specifically fiber, vitamin D, iron, zinc, folate, and B vitamins for overall health and wound healing. Her Avsola infusion for her IBD also is approved to treat Rheumatoid Arthritis so she feels that helps her joints feel significantly better.
Dealing with the mental health challenges of EIMs
Much like IBD, EIMs take a toll on our mental and emotional wellbeing. By seeking mental health support from a psychologist or counselor trained in chronic illness management, you can receive valuable support. Cognitive behavioral therapy (CBT) is particularly effective for managing depression and anxiety associated with IBD. If this article has done anything, I hope it’s shown you that you are not alone and sadly how common these complications are in our community. By simply going on social media and looking up hashtags for your EIM, you will see so many others who are living your reality and can learn a thing or two and feel understood, seen, and heard. There’s so much power that comes from us joining forces as a shoulder to cry on and an ear to listen, even if we’re thousands of miles apart.
By educating yourself and being proactive about what could happen to your body now or in the future, it can help reduce fear and anxiety that is associated with these unexpected and often unruly symptoms.
Everybody copes and has their own unique tips and tricks for undergoing an MRE. I received more than 100 messages with recommendations, there was some overlap and similar advice—but I know our community could benefit from this information and find comfort in it. One of the most challenging aspects of undergoing medical scans and procedures is the mental health aspect—the wait, the wondering. Oftentimes these results do not go in our way and may indicate we are in a serious flare or need surgery. So, while the actual process of drinking contrast and dealing with claustrophobia can be intense, the challenges are often amplified by the dread of finding out the story behind our symptoms. Understand you are not alone in that. I try and just prepare myself for the worst, while hoping for the best. Nobody wants “bad” news, but once you go through the scan and have a better idea of what is going on and then you can go after the flare and get to feeling better.
Here’s the link to Part 1 of “Everything You Need to Know Before an MRE with IBD” in case you missed it.
Advice from the community to ease the MRE experience
“Whether it’s laying there saying prayers (like the Rosary) or focusing on doing something (like walking through Sun salutations or walking through doing something you love to do) that has helped me.”
“As a pediatric patient, my mom was allowed into the MRE room, and she held my foot (the only thing she could reach). Just feeling she was physically there helps my anxiety a lot. Ask for goggles that let you watch a movie are gamechangers because you can’t see anything but the movie, even if you tried!”
“I close my eyes and pretend that I’m lying on a beach and listening to country music. I feel comfortable knowing I can see my feet at the other end, and they can communicate with me. Honestly, I close my eyes and sing my heart out!”
“I listen to the loud banging noises and try to find melodies or patterns. Then, I repeat them back in my head and by the time I’ve done it a few times I’m in a meditative state or the test is over.”
“I try to look up/behind me if I start to feel claustrophobic and you can see outside! I also find it almost relaxing to count the loud clips and beeps. It gets your mind distracted.”
“Picture yourself someone you like; use deep breathing to help soothe your vagus nerve.”
“I know it’s not ideal, but if you are extremely overwhelmed you can always get the test under general anesthesia.”
“I focus on my breathing and imagine I’m in my favorite place.”
“Eye mask with no metal clasps and ear plugs (or music) helps to reduce the sensory overload for me.”
“Before you get in the tube, ask for a towel. Put it over your eyes and do not take it off until they let you out.”
“Deep breaths. Visualize you’re in your favorite place and ask for music. Ask your GI if moving forward Intestinal Ultrasound can replace getting an MRE.”
“I’m normally able to tilt my head up to see out the end of the tube. It helps me so much!”
“Breathing exercises can help.”
“Ask if there is a bariatric imaging machine so you have more room.”
“Slow deep breathing helps me prepare for it and calm down.”
“I close my eyes and envision being on a bench or somewhere hard but with open space for me.”
“Gadolinium has a high allergic reaction. Even if you have not had it before. Communicate with your care team and ask about taking Benadryl.”
“Meditation and Guided Imagery.”
“I take deep breaths and remind myself I am going to be ok. It was quicker than I had expected.”
“Take extra Xanax! I take it for flying and always need more than I think.”
“If they let you pick the music, pick it! Having my music really helps me.”
“See if an Open MRI is available. Otherwise, a big dose of benzos.”
“I’ve been Twilight sedated before, it’s the only way to go!”
“I took Zofran. I also wear MRI safe clothes, so I don’t have to change. I make sure there’s no metal in my bra.”
“Focus on breathing. Close your eyes before being rolled in. Think of something like planning a party or a holiday.”
“I hate it. Hate it. Hate it. Someone told me just don’t open your eyes and it worked.”
“I take Ativan and do breathing exercises.”
“Always ask for a towel or wash cloth to cover your eyes.”
“Keep your eyes closed the whole time. Do not peek. And ask for your favorite music to play.”
“I keep my mind focused on other topics and talk to God.”
“Take anxiety meds! If I have to do this again, I will take something.”
“Let your care team know before you enter the room that you’re claustrophobic.”
“Say Affirmations or imagine being on a vacation on a sunny beach. Anything to divert your mind.”
“Last time my nurse gave me an orange smelling strip that helped so much.”
“I close my eyes and pray or sing songs I like the most in my mind.”
“Slow breathing and counting (in for 4 seconds and out for 4 seconds) or listening to music while in the tube.”
“I always have a Life Saver candy between the contrast drinks.”
“I asked them to bring me back far enough so I could tip my head back and see the ceiling.”
“My sister needs to take 3 anxiety pills for the MRE.”
“Try to find your happy place and go to that in the tube.”
“Have all the good and happy plans run through your mind and ponder them. Daydreams! Mantras!”
“I write stories in my head—like manifestations.”
“Think of a beach on a sunny day.”
“Make lists in your head.”
“Definitely have anxiety meds on hand.”
“Bring a personal blanket. This always helps me.”
“Bring ear plugs in case they don’t have some for you.”
“Use a wedge pillow for your legs (ask for it).”
“Visualize the best vacation, start to finish. Try to remember every detail. Distract your mind!”
“Ask for a heated blanket, it can be chilly in there.”
“When your mind wanders, count. Count breaths in (5) and out (5) and focus on the numbers.”
“Some MRI machines offer a mirror, almost like a periscope. It shows you the outside!”
“Fast paced work out music helps me.”
“I ask before we start that they give me a time update every 15 minutes.”
“It makes me less anxious when I hear the weird and terrible sounds the machine makes if I have NSYNC playing. Have them play music you like that’s also light and funny. (As in 90’s boy bands!)
“My office gives lavender stickers to help calm you to place on the robe. It helped me!”
“I’m SO claustrophobic but I always self-talk “I’m a mother and set the example for my kids.”
“Tell the tech you are nervous. Ask them to check in with you more than they usually would.”
“Remember you can squirm out of the bottom if you need to. Knowing that makes me feel less trapped.”
“Lavender essential oil.”
“I took half a Xanax and enjoyed every second…haha.”
“Take the meds and extra, if possible. I’ve taken up to 4-5 mg of Ativan!”
“They let you choose your radio station or podcast, which can help.”
“I’ve listened to the Hamilton soundtrack. I struggle more with getting the contrast down.”
“Meditation! I always do it before, during, and after.”
“Prepare a playlist or an audiobook and ask if the tech can play it over the speaker.”
“I pray the entire time, so I don’t panic.”
“Try not to investigate too much about the details, it may worry you too much.”
“It’s easier to go in feet first, I don’t know why…but it is.”
“Use the help/panic button and take a break midway through if needed.”
“Be prepared to hold your breath a lot—the tech will guide you.”
“Request a helmet with a mirror. It’ll help you see out of the tube.”
“Try and see how many song lyrics you can remember.”
“Tell them you are nervous. They are more understanding and will talk you through it more.”
“Make sure you give the anxiety meds at least 30 minutes to work their magic.”
“The pills help tremendously, but I also bring an eye mask.”
“Thank you for doing this article, I’ve canceled my MRE twice now out of fear.”
Nearly 19 years of living with Crohn’s disease and this past week I experienced an MRE (Magnetic Resonance Enterography) scan for the second time. I felt nervous, overwhelmed, and scared leading up to the test. The only other time I had an MRE was in July 2015 while hospitalized with a bowel obstruction. The scan was used to determine whether I needed surgery. I was out of it and have little to no recollection of the experience. The results from my MRE in 2015 informed my GI team back then that I needed 18 inches of my intestine removed. Fast forward to the present day, and after being in deep remission since that surgery, I started to experience a worrisome uptick in symptoms beginning in early March 2024.
It took a month to get in for the MRE, but I knew in my heart-of-hearts I needed to get answers. Leading up to the scan, I crowdsourced questions on Instagram and received an outpouring of support that helped make the experience nearly seamless for me. This week on Lights, Camera, Crohn’s I provide a behind-the scenes look at what it’s like to get an MRE and share firsthand advice from a patient advocate who is truly an “MRE pro”. Due to the amount of information, we’re breaking this bad boy up into two parts.
Walking you through the process
I had to arrive at the medical center at 10:15 am and was advised not to eat or drink four hours prior. I set my alarm for 6 a.m. and drank some water. When it was time to get in the car with my husband to head to my MRE, I took a Zofran to help prevent nausea from drinking all the contrast. After arriving at the imaging center, I was brought back to a room where I answered health questions and changed into a hospital gown and pants. I wore a sports bra without metal but was told I couldn’t wear it due to some synthetic fabrics. Then, I received my IV. The nurse took one look at my arms and grabbed a vein finder machine. For those who don’t know, this looks like a wand and puts a light over your arm to highlight veins so the nurse can pick the best option. My husband held the wand for her as she did my IV and she got it on the first try. That was a big win for me.
Once the IV was in, an MRI tech brought me three bottles of contrast (450 ml) to drink, about 46 ounces of fluids. I was told I had 20 minutes for each bottle and hopefully that I would have all three bottles down in an hour. Worst case the tech said I needed two. She told me not to chug too fast as that might make me nauseous. I took it with a straw and scrolled on my phone to distract myself. The contrast tasted like a super flat Sprite with a dull citrus taste. I’ve heard many people must do this in a public waiting room, I was grateful to be in a private room with my husband.
Due to my claustrophobia and anxiety about the test, my GI prescribed pre-meds for me that I picked up from Walgreens prior to the day of my test. He prescribed me four, 0.25 mg Xanax. I had never taken Xanax and did not know how it would make me feel. I called the Radiology center the day before the scan to ask whether I’d be able to get anything in my IV if I was too anxious, and they said if you’re outpatient you can only take anxiety meds orally.
Fellow IBD patients advised I take one Xanax the night before to have an idea of how it made me feel. I followed that advice and I’m so glad I did! Knowing how I responded took a bit of the stress off my shoulders. I took my first Xanax the moment I started the contrast (1 hour prior to the MRE) and then 30 minutes later I took .50 mg (2 pills) because I didn’t feel calm enough. For me, that was the perfect dosage. I felt completely coherent but chill and relaxed.
When I walked into the MRI room I asked if I could have headphones and listen to music. The techs asked me what kind of music I wanted; I said something upbeat like Taylor Swift. Then, I asked for a washcloth to put over my eyes. The scan took 45 minutes, I didn’t have one moment of fear or anxiety. There are lots of loud banging sounds and you hear the tech’s voice instruct you when to hold your breath and when to breathe. I felt very at ease and at the end started to doze off!
Since I had been NPO all day and it was 1 p.m. I was given a bag of pretzels and a bottled water after I changed back into my clothes. My husband had to leave during the scan to pick up our younger two from preschool, but the timing was perfect, and he swung back and grabbed me, so I did not have to drive after the scan. I felt tired afterwards.
After about 3 hours I started to get excruciating abdominal pain that I was not expecting. I’ve since been told by fellow patients that this is a result of the contrast and that it’s not unusual. I was very uncomfortable for about four hours. I spent a long time in the bathroom and on the couch with the heating pad. By about 9 p.m. I felt back to normal.
Guidance from a Veteran IBD Warrior and MRE Pro
Rocio Castrillon has lived with Crohn’s disease for more than 20 years and underwent countless MRIs specific to her IBD, but also for a multitude of other reasons including—Brain, Face/Sinus, Shoulder, Cervical Spine, Lumbar Spine, Legs, and Knee. She’s a true patient advocate in every sense of the word and someone I admire greatly. Through my recent experience, Rocio helped me immensely and even texted me the morning of my scan on her own accord, throughout my test as I drank the contrast, and after when I was stuck in the bathroom in pain. This is a true example of someone who goes out of their way behind the scenes to be a source of comfort and support for others. We have never met in person (yet!) and there’s this level of friendship between us.
“While MREs are specifically used for IBD patients, due to the contrast ingested, as well as injected, they are more complex than the traditional MRI and tend to be lengthier in time. Due to my anxiety and claustrophobia, I’ve had to utilize coping techniques to undergo MRIs and although they are still challenging, it’s yet another aspect of my IBD I’ve overcome. While these recommendations are primarily for IBD patients, many can be considered for a traditional MRI,” explained Rocio.
Check out Rocio’s step-by-step advice as your gear up for your next MRE:
PLANNING
At the time that an MRE is ordered by your gastroenterologist, there are a few considerations to keep in mind. MREs will require prior authorization which may take weeks. Fortunately, this time will allow you to explore options for locations.
In most cases, the MRE is ordered to be performed at the imaging facility that is affiliated with your provider, but you do not have to do your MRE there.
Oftentimes, there are private imaging centers, not affiliated with an academic institution, which can be more cost-effective.
MRI machines are now available in a wider bore design to help reduce anxiety and are recommended for claustrophobic patients. The feeling of a more “open” machine is beneficial. But to locate one, you must call around to determine if your recommended imaging facility has them and/or if you need to seek out an external facility.
At the time of your gastroenterologist appt., and if you have anxiety and/or claustrophobia, Rocio strongly suggests requesting a prescription for a sedative used for panic disorders, such as: Ativan, Klonopin or Xanax, which are short-to-intermediate in duration. While you will only need a prescription for one pill, keep in mind that there are many states that now require identification to pick up controlled substances.
Please note that if you do take a sedative, you will be required to have a driver to accompany you, as you will not be allowed to drive yourself.
Also, at the time of your gastroenterologist appt., and if you have nausea, Rocio strongly suggests requesting a prescription for Zofran to be utilized prophylactically.
Once the prior authorization for your MRE is approved, you will be able to schedule. Request an appt. time that works with your personal eating schedule. Because MREs require fasting, as well as contrast ingestion, patients may find it challenging to drink contrast early in the morning. Rocio tends to have more nausea in the mornings, so she prefers to schedule mid-day scans. While this does mean a longer fasting time, it also allows her to drink more contrast.
DAY BEFORE
Rocio eats a light diet the day before the MRE to prevent nausea as much as possible. While this is not necessary, she’s found it helps with nausea and vomiting.
HYDRATE…before AND after your MRE. While the technicians will explain the need to hydrate following an MRE, hydrating beforehand will allow for easy access to veins for the IV needed to inject the contrast. Hydrating after is crucial to eliminate the contrast from your body.
DAY OF MRE
Before leaving home, be sure to remove all jewelry and/or metal from your body. Because an MRI machine uses a magnetic field, you cannot have any metal on you. Women will be asked to remove their undergarments which have metal.
Additionally, if you continue masking in medical facilities, your mask will be switched out for a mask without metal that the technician will provide you.
An hour prior to the scheduled arrival time, take the prescription Zofran so it has time to kick in before needing to begin the contrast. It will help prevent/reduce the level of nausea and/or vomiting from the contrast.
Upon arrival at the imaging facility, you can take the sedative, as this will allow it time to kick in before you begin the imaging. Because there will be a window of time when you need to consume the contrast and when the imaging begins, this typically works well.
Contrast! While many academic institutions have shifted to a new contrast, Breeza, which is lemon-lime flavored, it is not always available to patients. In the past, Rocio has consumed other contrasts. She wholeheartedly agrees that Breeza is certainly better “tasting” than those in the past. But in full transparency, it still is contrast…haha.
For all her MREs, Rocio has been provided with three bottles of Breeza. Unfortunately, she cannot consume all of them, and at best, she’s drank a maximum of one bottle. While this is certainly not ideal from an imaging perspective, and is NOT medical advice, she’s been fortunate to have been “allowed” to perform the test with just one contrast bottle. The imaging that has resulted has sufficed for the radiologist to review and for her gastroenterologist to see results.
Insider Tip: While this may not be available to all patients at all facilities, Rocio always requests to sit near a bathroom and/or near a trash can if she is in the main waiting area. She says she already has enough anxiety about the MRE, and having people watch her drink contrast tends to make her more anxious. Note this is NOT always readily available, and you will have to adapt to what is available at your facility.
MRE START
Upon finishing the contrast, the technician will take you back to the MRI machine where you will be laid flat. If you have anxiety and/or claustrophobia, be sure to alert the technician as they can make you more comfortable in a few ways.
Typically, a technician will ask for your music preference as they’re able to control the music that you hear via headphones (provided to you)
Rocio prefers relaxation/spa music as it helps to keep her calm.
Depending on your facility, there are mirrors that can be placed to allow you to “see” the surroundings and not actually have a view of the MRI tube. It enables patients to have the “illusion” that they can see the outside – either images displayed on the ceiling, or the room where the technician is sitting. This has been a lifesaver for her!
During the MRE, the technician will explain everything to the patient through a speaker that you can hear in the machine. You will also be able to respond to the technician and they can always hear you. You will also be provided with an emergency panic button to press, should you need to come out of the machine for any reason.
During the MRE, the technician will advise when they are starting the contrast through your IV. You should not feel anything except a quick sensation of nausea that passes immediately. This doesn’t happen to everyone, but it’s common.
Rocio says for some patients, like herself, who have been unable to consume all the contrast or who have slow motility, sometimes an injection called Glucagon will be utilized. This improves the quality of the images, but it does cause side effects. You will be instructed to ease into resuming eating and avoid any high protein foods due to slow digestion.
At the conclusion of the exam, you will be instructed to hydrate and begin eating slowly. Much like post-colonoscopy, Rocio recommends light meals for a few hours.
Due to Rocio’s extreme nausea and vomiting, she typically does not tolerate the contrast after the exam and tends to get sick shortly after. This is NOT the norm, but she recommends having an emesis bag in your car. As a reminder, if you have taken a sedative, you will not be allowed to drive yourself.
Considerations regarding contrast
While the actual scan experience was more pleasant than I had anticipated, about 3 hours after getting home I started getting terrible stabbing pains in my abdomen and had to run to the bathroom multiple times. At one point my husband came upstairs to check on me because I had been in the bathroom for so long. I was not aware or told that the contrast could cause this type of response. When sharing this on Instagram and after talking with Rocio, I learned how common this is within our community, especially for those who are symptomatic.
An IBD mom whose daughter has Crohn’s shared helpful insight for those who are on special diets or have difficulty tolerating contrast drinks.
Kristen tells me for MRE’s her daughter mixes Miralax in a specific amount of water that the MRI tech recommends, if she had to guess 40-60 oz over an hour. She says this helps prevent stomach cramping and uptick in symptoms. Kristen says some patients on the Specific Carbohydrate Diet (SCD) also drink pineapple juice (Lakewood brand or another organic fresh pressed brand) with Miralax.
“I found through this experience with my daughter that there was not much knowledge about how what you put in your body in the way of contrast, may affect inflamed intestines. Large amounts of sugar alcohol in contrast causes my daughter terrible pains for hours afterwards. Everyone is obviously different, and this disease is unique to each person, but I did a lot of research and we have found that the combo of a biologic plus SCD diet has really helped my daughter maintain remission, for now anyway.”
Kristen’s daughter had bowel resection surgery to remove strictures in her terminal ileum 7 years ago when she was 13 years old. She’s added some food back, but she’s strict with eating only whole foods and great about taking her medication.
Tomorrow on Lights, Camera, Crohn’s hear input and helpful MRE advice from 80 IBD warriors along with how to cope with the mental health aspect of going into a test and not knowing how the results are going to impact your life. As I was working on this article, I found out from my IBD nurse that my MRE results were within normal limits and that there is no evidence of active inflammatory bowel disease. While I’m thrilled and grateful to receive this news, it’s always perplexing when you’re more symptomatic than normal and your labs and scans don’t reflect a reason why.
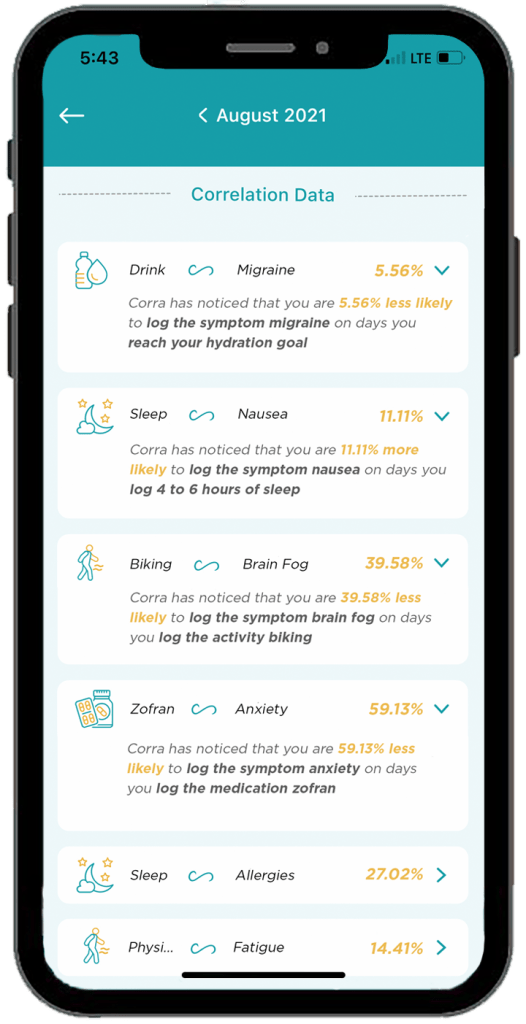
This post is sponsored by Corra. All thoughts and opinions shared are my own.
For as long as Elya Lane can remember she had signs and symptoms of a health condition. It wasn’t until college that she received her official diagnosis of Ehlers Danlos Syndrome and POTS. She says her poor health started to spiral with other comorbidities popping up, the worst of which was chronic UTIs that left her whole body in crippling, burning pain and weak from the antibiotics. Elya’s personal journey with chronic illness inspired her to create the Corra App. This week on Lights, Camera, Crohn’s we learn about how she made her dream a reality and how she hopes to improve peoples’ lives.
The breaking point
“I was constantly plagued with fears of antibiotic resistance, infection complications, or complications from long term antibiotic use. I got to the point where I was so sick that I wrote letters to my kids and my family in case something happened to me. I started tracking all our passwords and making videos for my husband on where our important files were, how different things were stored, all the kids’ data, etc. While I tried to face this potential outcome bravely, I was devastated imagining my kids growing up without a mom,” said Elya.
As she navigated these dark and daunting days, the despair caused her to think about how she could fight back and regain control of her health.
“I started to religiously track my health in journals before transferring to Excel spreadsheets. I was so frustrated by how exhausting and impossible it felt to crunch that much data, so I turned to searching for a symptom track and correlative software to help me. I downloaded and tried every single one I could find – but none met my needs. Some even gave me back faulty data which made me angry. That’s when I decided to create a solution myself,” she explained.
In 2020, after losing access to all her healthcare management tools, and with her health declining rapidly, she decided to create Corra.
The meaning of Corra
There are quite a few chronic illness apps on the market, some that even attempt to offer correlative insights. Corra is short for correlations. Elya wanted to identify correlations in her health so that she could find her triggers and optimize her lifestyle.
Here’s what sets Corra apart from other chronic illness apps on the market:
The algorithm was custom built by Corra’s chief data scientist, Simeon Wilson, who has a master’s in quantitative economics from UCLA. “We are not aware of any software that exists that compares to what Corra is currently offering with our correlative algorithm.”
Corra was designed by individuals with chronic illness. “Not just me! While the idea and original designs are all mine, we brought on more than 200 beta testers with various chronic illnesses to provide their feedback and help us tailor the app to the needs of the chronic illness community. Even now, we continue to rely on the insights and feedback from the community to enhance and adjust the app. I want Corra to always be designed by and created for our community.”
We correlate with nutrition in an accurate and helpful way. “I believe nutrition plays a massive role in our health so one of our key focuses with our algorithm was to be able to correlate seamlessly with nutrition inputs.”
Corra does not sell user’s data. “We don’t scrape your data from your device or browsing history, we don’t use your data to sell you anything, we don’t share your data with third parties. Your data is yours alone. As an individual with a chronic illness who often feels more like a commodity than a person, making sure people can receive personalized insights into their health without signing away their privacy is incredibly important to me.”
Corra’s bells and whistles to check out
The ability to track health data in one place without having to use five different apps to log information. “My favorite part of Corra is of course the correlations, because getting detailed insights like that about my health is equivalent to having a team of data scientists run extensive tests on my health and provide me reports. It’s life changing to be able to learn about my health overtime and create a custom-built lifestyle that caters to my future.”
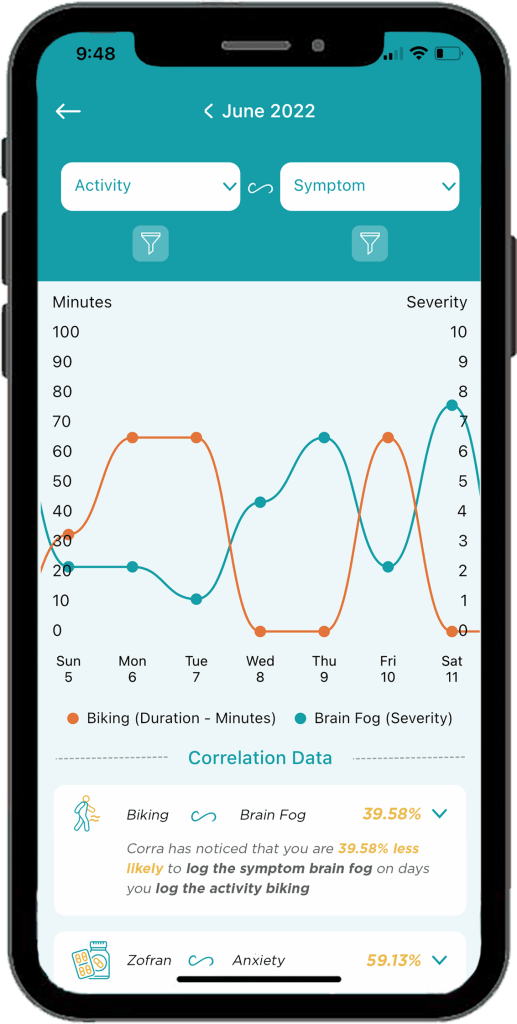
Discovering positive and negative correlations. “You may receive insight that something has x% chance of increasing or decreasing a symptom. I think being able to get data on the things that are helping is just as important as being able to identify triggers.”
The ability to log appointments, download PDFs of your data to share with my doctor, track medications and supplements, track mood and stress levels, etc. “I’m also extremely excited about all the upcoming integrations we have in the works! Soon we will be connected to Fitbit and Apple Health with Garmin, Cronometer, Weather data, and hopefully Oura coming shortly after! Over time we will continue to integrate with as many devices and apps as possible so users can have all their data in one location!”
A promising future
Elya says being able to learn what foods, activities, supplements, and medications help or cause symptoms has enabled her to have a much better understanding of how best to manage her health conditions.
“I’ve been told to go vegan, cut out red meat, don’t eat dairy, sugar, gluten, eat paleo, try a carnivore diet, go vegetarian, and try cutting out leafy greens… what I found with Corra is that I didn’t need to make these drastic nutrition changes, I only needed to cut out some foods in each of those categories. For example, I discovered that I have a high trigger correlation with ground beef. I can eat steak and other red meat, but not ground beef. Similarly, chicken thighs are a trigger for me, but chicken breast is not. Same with gluten, there are some gluten products that are triggering for me, but not all gluten triggers me. Being able to identify exactly which foods to cut out, rather than willy nilly cutting out entire food groups or going on drastic diet changes, has been an absolute game changer.”
Elya has also discovered that cold and flu medications like Mucinex are major triggers for her. This helped her realize why she would get a horrible flare a few days after coming down with a cold or flu.
“Now, I try to manage my colds and flus with other medicine to try to prevent the flare on top of the cold. It’s also important to note that I’m not cured! I have to manage my diet and my activities and my supplements every day. The difference is, I’m no longer throwing shots in the dark, I now have the information I need to manage my condition to the best of my ability.”
Information really is power, and it has given Elya control over her life and reduced her anxiety. Because of Corra, she is now coming up on two years without the need for daily antibiotics. It’s been over 2 years since she visited the emergency room.
“I’ve found that medical providers are far more willing to accept unbiased data from an algorithm than trust my verbal expression of my experience, so in that way Corra becomes my advocate and backs up my statements,” said Elya.
She says her health conditions have caused her to go through depression, isolation, and hopelessness. But her hope for Corra is two-fold.
“First, I believe it can help others identify their triggers and optimize their life so that their conditions can become more manageable, but I also hope that Corra can be a beacon of light for those struggling to see they are not alone. There are so many steps between the start of symptoms and any kind of treatment let alone cure (depending on if your condition is even curable)… and I want to be the one that goes into the trenches and helps people who are suffering the most. So many people in the chronic illness community get forgotten or left with “your test results are normal” when they know there is something wrong with them. I want to create a company that comes alongside them and lifts them up and allows them to have their voices heard.”
Downloading Corra
You can download Corra directly from the App store or the Android playstore. There is a free version as well as premium access. The premium version is $7.99/month or $24.99 if you enroll for a 6-month subscription. Elya is looking for Corra Insiders who are interested in getting free access to the app. By joining the Insiders group, you get a first look at upcoming features. This provides you the opportunity to share feedback on what you do/don’t like or would like to see improved or added in the future. Sign up for the Corra Insiders program here.
It’s the first of its kind program dedicated to training dietitians about IBD-focused nutrition. Cedars Sinai Hospital in Los Angeles, California launched its IBD Dietitian Apprenticeship in July 2023.
Registered IBD dietitian Stacey Collins was the first registered dietitian to be selected, participate, and complete the program. I’ve been amazed at all she does for our community and been excited to dig deep and learn what her key takeaways have been from this experience. As someone whose lived with ulcerative colitis since 2012, when she was 21-year-old, Stacey has a unique perspective and approach.
This week on Lights, Camera, Crohn’s we’ll hear about her firsthand experience and why this Apprenticeship program is just what our community needs. The hope is that registered dietitians who participate in the program can take their knowledge from the experience and be able to plug themselves into an IBD Center to build and strengthen an IBD program.
Going up against lack of education and funding
Stacey tells me there is little to no education that they receive in dietitian training on how to do nutrition specific to gastroenterology, much-less IBD, and she says this Apprenticeship program fills the gaps and then some.
“So much of what I learned was through self-study before this program. But in the Apprenticeship, whether I was part of the team rounding on patients in the hospital, or seeing a newly diagnosed patient in clinic, or sitting on the floor with a 3-year-old patient asking about their Paw Patrol toys, I left every encounter feeling that special kind of discomfort and gratification that comes with growth and learning. This was truly a hands-on learning experience from many different sides of the IBD rubix cube, and I’m so grateful I wasn’t learning it all by reading slides from a PowerPoint and taking a test- who learns that way anyway?!”
Addressing the unmet needs
Once registered dietitians complete the Apprenticeship they can work in an academic center or a private practice that values IBD nutrition and has the financial backing to justify the need for a dietitian.
“There are institutions and people in places of power who are advocates for the profession of IBD RDs, and this work is simply impossible without them. IBD RDs have the potential to support patients throughout their journey as an accessible, consistent member of their multidisciplinary care team. Unfortunately, a lot of this potential is systemically handicapped by the lack of funds: RDs are investments rather than quick money-makers for a clinic without physician advocates and creativity, and we NEED people at institutions to see our value,” said Stacey.
The main programmatic goals are to provide a structured, supervised training program for dietitians to learn a model wherein dietitians work together with physicians and advanced practice providers for the care of adults and children with IBD.
Places do exist (and many are coming) that support this multidisciplinary model of healthcare delivery, but there’s such an unmet need, especially for people who don’t have access to these IBD centers. The hope is for this Apprenticeship program to fill the gaps of that unmet need by signaling to physician advocates at these institutions that a nutrition professional with intense training and experience DOES exist, ESPECIALLY for more complex patients who have IBD.
So much to be done for patients Registered IBD dietitians can assess people for malnutrition regardless of their stage of IBD, which is common even in remission and linked to poor health outcomes, along with so much more. Stacey says:
We can help catch micronutrient deficiencies or insufficiencies that many other care team members might miss, and we can correct and monitor them.
We can help patients experiencing food insecurity find ways to nourish themselves within their budget constraints with an eye toward prevention of other comorbidities.
We can help nutritionally prepare patients for surgery.
We can help patients in need of a medical or therapeutic diet intervention find a way to make it a sustainable intervention for themselves.
We can help patients nourish themselves using a whole-person approach, whether they are juggling multiple diagnoses, starting a new job, headed off to college, or too tired to eat: we have tools for helping patients feeling like they can handle it all
We can help prevent re-hospitalizations from small bowel obstructions or dehydration by giving patients IBD-specific tools for understanding their body.
We can save physicians time by inheriting questions about nutrition and/or supplementation regimens, and we can personalize these for each patient.
We can even show GI or IBD Fellows what it’s like to feel spoiled working with an IBD dietitian, and hopefully they’ll advocate to hire one of us wherever they make their final clinical stop
She’s confident IBD dietitians can make nutrition an accessible tool when it so often feels inaccessible with IBD!
Stacey’s top apprenticeship moments that left a lasting impression
Six months is a long time to pick up your life, move to another state temporarily, and fine tune your knowledge and expertise on nutrition and IBD. Here are the key takeaways Stacey says she took away from the experience:
1. Patience with patients is key; everyone is on their own timeline.
“I got to see a doctor celebrate with a patient who finally quit smoking cigarettes for good. After that encounter, he told me that he had been pleading with that patient for 20 years to stop, but he never blamed the patient for having a tough time stopping. He really was empathetic to the fact that they had a lot going on, and he knew they’d get around to it once life allowed. That was really enlightening to see: patients really are doing their best. How can I support them, especially if their timeline looks differently than the expectations that I have?”
2. It doesn’t have to be all-or-nothing; don’t let perfection be the enemy of good nutrition.
“One day I was with Erin Feldman, RD (Cedar’s Pediatric GI and IBD RD). She was listening to a worried mom talk about how she didn’t want her kid to eat sugary cereal, but that’s ALL they would eat for breakfast: it was the sugary cereal, or it was nothing at all. The child was exercising their choice autonomy and exploring what that looked like around mealtimes, and it was a challenge for the parents. Erin had a rapport established with the family, and I could see that they really trusted her. Plus, Erin is a mom, too, so she speaks the same first language as parents, and she really empathizes with the fact that many IBD parents are blamed for their child’s symptoms or disease. She truly met the parents right where they were at that moment.”
“Instead of focusing on the PERFECT breakfast with beautifully-balanced macronutrients and color that the child certainly would refuse, she said, “What if you just added PLAIN Cheerios and a couple of raspberries to their sugary cereal, that way they’re getting some antioxidants from the berries and a more diverse source of grains into their breakfast?” It was TOO easy, and the parents were like, “YES. We can do that.” and just like that: not a perfect solution, but a practical intervention that would work for where the child is right now.”
And that’s the power in having multiple touchpoints to a dietitian: next time they see the doctor again, they’ll see Erin, too, and they can make more adjustments for how life is being lived around food at that stage, too. So often people have the ambitious idea of going from zero to specific carbohydrate diet (SCD) all in one encounter, and the reality is that often multiple conversations and coordination of resources are needed, and meeting patients where they are looks different for everyone.
3. Nutrition interventions can be hard, and multidisciplinary support really is key.
“So often as dietitians, it’s easy to get stuck in the weeds of research and to get excited over interventions that have promising outcomes. This happened with a patient needing Exclusive Enteral Nutrition, but ~5-7 days into it, they were uncomfortable, and they really missed food. I was able to have a conversation with the patient alongside their doctor in the same room, who patiently reiterated our rationale behind the intervention and said, “not if it compromises your mental health. Let’s stop it if your brain is telling you we need to stop- we need to respect that. You should be proud that you tried this, and now you know!” And I could tell the patient was so relieved to have reassurance from their doctor that no matter what THEY chose for THEIR body they’d be supported by their doctor and by their dietitian. It really does take a team.”
4. GI Doctors REALLY do not get exposure to solid nutrition in their training
Kelly Issokson, MS, RD (Clinical Nutrition Coordinator, Course Director: DIET Executive program, Apprenticeship Director) arranged for Stacey to lead a learning session with the GI Fellows at Cedars, and in a room full of some of the smartest and most compassionate clinicians.
“They wanted to know all about the different nutrition interventions that we can recommend for patients. It felt like they had been rewarded for being the best of the best all by themselves their whole lives, and now they had an opportunity to learn more about how to collaborate effectively. They were all so enthusiastic.”
Stacey noticed after that session that the GI Fellows felt comfortable texting her while on rounds if she wasn’t there to ask if she’d stop by a patient’s room, or they’d text to ask about B12 supplementation after remembering to screen for a deficiency.
“They really understood the value that IBD RDs bring, and it’s not because I’m a great public speaker (I’m really not); it’s that they had this additional exposure to working with a dietitian with specialized training. This really made everything click for me: doctors don’t always know the right questions to ask patients about our nutrition needs, because most of them haven’t had the education OR the exposure to team members with the expertise to be truly helpful for patients. Working in silos keeps patients isolated, and I’m hopeful that the GI Fellows, when/if they leave Cedars become physician advocates to ensure that their patients have access to an IBD experienced RD.”
Plans for the future
When Stacey completed her Apprenticeship this winter, she did not envision returning full-time to her online private practice. She thought she’d start working at an academic institution, because the purpose of the program is for the dietitian to seamlessly integrate into a multidisciplinary GI care team.
“I am still holding out on hope that one day I could have both (but I’ll never give up my private practice- I love it so much). Truthfully, I’m thrilled to be back with such a passion for teaching patients how to implement some of the skills that I’ve learned into their own life, plugging it into their existing care teams, even if I’m on my own in private practice. I already helped patients through perioperative nutrition before this program, but now I’ve got some RICH resources to help make IBD surgery and nutrition really make sense for patients now in a much clearer way,” Stacey explained.
She’s able to take the research that they did from the perioperative IBD Nutrition program that exists at Cedars and put it into practice with her patients, and it’s a bit of a full-circle moment for her, having lived through IBD surgery with limited support.
“I’m a much better listener than I was before this program, a skill I learned from Kelly Issokson, MS, RD (Clinical Nutrition Coordinator, Course Director: DIET Executive program, Apprenticeship Director). Additionally, I’m more practical in my approaches and meeting patients where they really are, too, a skill I learned from Erin. I’m working on some ways to expand IBD RD accessibility, too. I’m a much more confident advocate on behalf of my patients now, too.”
Advice for the newly diagnosed
If you’re reading this and you or a loved one was recently diagnosed with IBD, ask your GI doctor to hire an IBD Dietitian. Stacey knows this doesn’t exist in most places, and as a patient, she understands how silly it is to constantly be burdening patients with requests. But the field of IBD Nutrition exists because enough patients asked, “What can I eat?” and enough doctors paid attention to it to be documented research. This is the next piece of the puzzle.
If your care team provides a registered dietitian who doesn’t specialize in IBD, that’s not going to cut it. Be assertive in asking your GI office to hire an IBD Dietitian, or invest in training their Dietitian, if they really want to help their patients.
Stacey advises patients and caregivers to stay off online forums. There’s so much food fear there, and life is bigger than that. Lastly, she advises reaching out for help. Even if Stacey may not be a good fit for you, she’s happy to provide patients with other RDs that she’d enthusiastically see, because an informed decision is a good one.
During her Apprenticeship, Stacey chose to do a research project to examine the effects of malnutrition and perioperative nutrition supplementation on surgical outcomes in people getting IBD surgery, whether that be for j-pouch, permanent ostomy, lysis of adhesions, or a resection.
“We had a small sample size (n=25). Regardless, we found that perioperative nutrition supplementation had a statistically significant impact on decreasing the length of stay, meaning that greater adherence to the nutrition supplementation protocol was associated with a shorter time spent in the hospital. Regardless of nutrition status (malnourished or not), everyone seemed to benefit from the nutrition supplementation protocol that we recommended for before and after surgery.”
Stacey is hopeful that more research with an even larger sample size will help inform these results so that this can be a resource more widely available for patients!
The future is bright
“If I dared to dream about what this could look like in the future, the closest possible model in existence is at UCLA under Dr. Niru Bonthala who is the Director for Women’s Health in IBD. Basically, I see the RD’s role evolving to cover every nutritional aspect of IBD with specialized knowledge to support patients in each life circumstance: from surgical prehabilitation to home nutrition support (TPN or EEN) and transitioning back to eating; to the overlap of eating disorders; to fertility and perimenopause; from anywhere along the spectrum of LGBTQIA+ care and/or transgender care; from peds transitioning to adult care, and even adults to aging adults; even athletics and/or eating disorders.”
There’s a rich opportunity within all these Venn-diagrams for a specialist interest and training to exist in IBD Nutrition, and this learning opportunity exists at Cedars.
“I’d also love to see the RD in an outpatient clinic even able to do community outreach: teaching basic cooking skills, procuring menu items for their medical diet (and beyond), and even showing patients and their families what this could look like by partnering with local food banks. Again, this is just me dreaming here in a world that I think should exist for people who have IBD and for RDs who are trained in IBD Nutrition,” said Stacey.
The current IBD Apprentice Yi Min Teo (@herbsandfood) came from both clinical and private practice backgrounds like Stacey. Yi Min will finish her training in July 2024. The program is supported by a grant from Leona M. and Harry B. Helmsley Charitable Trust.
In addition to dietitians wanting more IBD nutrition education, there’s also an Executive Program for MDs/DOs, APPS, and includes both virtual and in-person learning opportunities. You can apply here.
This blog post is sponsored by the Alliance for Access to Care. All thoughts and opinions are my own.
Going head-to-head with insurance companies goes hand in hand with managing chronic illness. The amount of time wasted, and energy exhausted over the course of a patient’s journey is incomprehensible. But the Alliance for Access to Care is looking to change that with the help of its latest campaign known as Healthcare Here. This coalition of healthcare associations has shared concerns about the way that insurance companies have adopted and implemented practices and policies that impede timely decisions related to treatment coverage at the expense of patient care. The burden of these practices, as we know all too well, not only falls on patients, but also on local hospitals that make up the backbone of community care that so many people rely on.
This week on Lights, Camera, Crohn’s we hear from Sr. Mary Haddad, RSM, President and Chief Executive Officer, Catholic Health Association, about the key issues and how she’s leading the charge.
The mission of Healthcare Here
Sr. Mary says the mission of the Catholic Health Association of the United States (CHA) is to advance Catholic health in caring for people and communities. Recently they also adopted a new vision statement that highlights why they are so passionate about health care reform: We Will Empower Bold Change to Elevate Human Flourishing.
“We are keenly aware that the United States’ health care system is in dire need of bold change, and this needed change is long overdue. Commercial insurance companies that profit from the delay and denial of health care stand in direct opposition to our mission of caring for people. How can a person flourish, or even survive, if their basic health care needs are not being met?”
As a faith-based organization, they believe that their ministry echoes that of Jesus Christ, who spent his time on earth providing compassion care for those in need.
“This cause is not only central to our mission and vision; it’s core to who we are,” she said.
Local hospitals in financial distress
When commercial insurance companies continually delay or deny coverage for care to those who need it, the cost of that care is passed to local hospitals. Not-for-profit hospitals have policies in place to ensure that those burdened by financial challenges receive either free or discounted care.
“As an example, on average, members of CHA provide free care to individuals and families who are under 200 percent of the federal poverty level guidelines. They also provide discounted care for those making up to 350 percent of the federal poverty level guidelines,” explained Sr. Mary.
The role of AI and medical decisions made by insurance companies
The CHA has seen several examples of commercial insurers utilizing automated systems to quickly process claims that may require greater scrutiny.
“For example, a recent ProPublica article found that Cigna spent an average of 1.2 seconds per individual case to deny more than 300,000 claims. They used an automated system to do this and, in doing so, saved millions of dollars for themselves. NaviHealth, which is a UnitedHealth Group subsidiary, is currently being investigated for trying to align rehab stays for Medicare Advantage patients to within 1% of days projected by an algorithm,” she said.
There are other examples, but the overall trend is telling enough. According to Change Healthcare, denial rates increased by 23 percent from 2016 to 2020. Meanwhile, profits from commercial insurance companies continue to rise.
A call to action for patients and caregivers
It can feel helpless as a patient, feeling as though your health and well-being is in the hands of your insurance company. I relate to this on many levels. Since my Crohn’s disease diagnosis in 2005, I’ve had to deal with everything from insurance telling me I’m too young for my annual colonoscopy to deciding the biologic injection I’ve been on since 2008 needs to switch to a biosimilar, not for medical reasons, but because of insurance coverage.
“We must advocate for change in the health care system, specifically as it relates to commercial insurers. On Healthcarehere.org, the CHA has pre-written a message that patients and advocates can send to their local, state and federal elected officials that gets the message across loud and clear: local hospitals are important and need to be protected,” said Sr. Mary.
Rural hospitals at risk
Not-for-profit hospitals are experiencing dire financial straits. More than 30 percent of the United States’ rural hospitals are at risk of closing. Per-patient hospital expenses have increased. At the same time, commercial insurance premiums are increasing at twice the rate as the annual rise in hospital prices.
“We’re approaching a point where a dam is going to break. And the ones left dealing with the shortfall of coverage will be patients and the local hospitals that they rely on for care. Ideally, all sectors of the healthcare system should be working together to deliver affordable, accessible, and high-quality care for patients. Through this campaign, we want the public and the policymakers they elect to understand how profit-driven actors are manipulating the health care system, which in turn is harming patients and the local hospitals that care for them,” she said.
Sr. Mary went on to say chronic illness patients need to know they are safe and welcome at their local hospitals.
“We want patients to understand that they have a voice which needs to be heard. Coupled with the advocacy efforts of the Alliance for Access to Care, patient testimonials are a powerful tool in standing up to the commercial insurance industry that would profit off their illnesses. Too many have been victimized by this broken system of care. The stories need to be told and change must happen now.”
If you have a story of denials to care through commercial insurers, send them to story@healthcarehere.org. We want policymakers to understand that this isn’t a battle between hospitals and insurers. This is an issue that affects real people. Your stories and experiences matter and deserve to be heard. Lives are at stake.
Did you know within the next decade, one in three IBD patients will be over age 60 and that right now, adults over 60 make up the greatest portion of the IBD population? As someone who was diagnosed with Crohn’s disease at age 21, who is now 40, I’ve started to think more about what managing and living with IBD will look like as I continue to age. Managing IBD in older adults is complex and requires considering each person’s individual risk of complications and co-morbidities.
This week on Lights, Camera, Crohn’s a look at the research that’s available and what we can expect as an aging patient population. Before we get started, it’s important to note there are two groups—adult-and-pediatric onset IBD who are getting older and then a group of people who are diagnosed later in life (after age 60) referred to as “elderly-onset IBD”. Every review I saw online uses age 60 as the benchmark to differentiate these two groups. Elderly onset makes up about 10-20% of patients who are newly diagnosed with IBD.
Unfortunately, there’s limited data and studies that have followed patients for 20-plus years, so we don’t know a ton about how aging impacts patients who were diagnosed as pediatrics or as younger adults compared to those who are in their later years. While there’s a well-known belief that IBD can “burn out” as we age, meaning that symptoms for some quiet down, that is of course not the case for all.
Considerations when treating IBD in older age
Have you ever talked to your GI about how your IBD will be managed as you age? I know I haven’t. I feel that there’s so much to focus on in the “now” it can be overwhelming to think about how we’ll take care of ourselves 20-40 years from now! As we surpass age 50, there are important discussions to be had.
What patients and providers need to consider:
Risk of disease and treatment related complications
Tolerability of IBD therapies, which is unique to each person’s personal experience
Drug metabolism and how it alters with aging
Body composition changes which include a reduction in total body water and an increase in total body fat.
The delicate balance of disease-related risks vs. treat-related complications.
Risk of adverse events from medications vs. benefit shift (higher rates of infections, malignancy, and drug intolerance).
Given these factors alone, the way in which IBD is managed in older age isn’t as clear cut as when we’re younger. With both thiopurines and biologics, older patients are more likely to discontinue treatment. Older adults may value symptomatic remission (and quality of life) more than mucosal healing.
This study entitled, “The elderly IBD patient in the modern era: changing paradigms in risk stratification and therapeutic management” states, “Despite elderly onset IBD presenting with a less extensive or aggressive phenotype than adult-onset IBD, its disease course is not necessarily more benign. In Everhov et al.’s work, 22% of elderly onset Crohn’s patients underwent surgery by 5 years, although the rate was lower in UC patients (6%). Similarly, the cumulative probability of surgery at 10 years was 32% in Crohn’s patients compared with 8% in UC in another population-based study.”
According to an article in Time called “The Connection Between IBD and Aging”, whereas IBD was once thought as a disease with two spikes in onset—20s to 30s and 40s to 50s—doctors are learning there is a third spike that begins later in life. For those of us who are diagnosed when we are younger, our bodies have lived with decades of damage the disease has caused, often we’ve had surgery, been on medications with serious side effects, and ongoing flare-ups for much of our lives. For those who get IBD after 60, rather than seeing damage in various parts of the intestinal tract, more activity is seen in the colon.
The article goes on to say, “It’s no surprise IBD causes chronic inflammation, and so does aging. So, as we age with IBD, we’re at greater risk for inflammation linked-health issues, including cardiovascular disease, cancer, hypertension, chronic obstructive pulmonary diseases, chronic kidney diseases, obesity, skin issues, blood clots, arthritis, dementia, and skeletal muscle loss.”
Comorbidities and IBD
According to the Crohn’s and Colitis Foundation, people who have Crohn’s may also have a better quality of life as they age, partly thanks to modern medications and less use of steroids long term, which can trigger bone loss and cataracts over time, among other symptoms. Steroids are the most dangerous medication we have to treat IBD, sometimes of course they are necessary, but long-term use should be avoided at all costs.
People over 60 are more prone to infections and have a greater likelihood of being on medications for additional health conditions. They also often have visual, cognitive impairments, risks for falls, and surgery complications.
Underrepresentation in clinical trials
One of the main reasons we lack data about IBD in older age is because this population of patients is often excluded from clinical trials. This study from The Lancet Gastroenterology & Hepatology says, “A deeper understanding of biological and functional age, dynamic risk stratification strategies (including frailty-based risk assessment tools), comparative effectiveness and safety of current therapies and treatment strategies, and shared decision making to inform treatment goals and targets is needed to improve outcomes in older adults with IBD.”
A Crohn’s and Colitis Foundation study found that clinical trials for biologics only included 1% of people over age 65. How can patients feel safe about being put on biologics when there isn’t research to back up the safety and efficacy of these heavy-duty medications when they reach that age bracket?
As far as menopause goes, we still don’t know much yet about how this impacts women and the role it plays in disease course. Some small studies have found a modest protective role for estrogen-replacement therapies for IBD activity. But there’s more research needed in this area. According to the Crohn’s and Colitis Foundation menopause may begin earlier in IBD patients, but this does not appear to have any negative effect on disease activity or progression. Women with IBD are at greater risk for osteoporosis in menopause, this is why it’s so important we’re proactive in younger age by getting bone density tests and taking calcium and vitamin D supplementation (if labs show you’re deficient). I have taken 50,000 IU of Vitamin D once a week for years to help combat bone loss and this past year I started seeing a Bone Health Doctor to keep a close eye on my osteopenia. My GI told me during my clinic visit this month he wants me to take 2 Tums a day for added calcium.
As far as men, aside from methotrexate, IBD medications do not usually cause erectile dysfunction. Ileal pouch anal anastomosis (IPAA or J-Pouch) surgery, while sometimes associated with loss of sexual function, is not associated with erectile dysfunction. There’s also no known connection between IBD and prostate cancer.
Patient inputfrom those who are 60-plus
Patti says her age has changed how she manages her IBD.
“I’m 60 years old. Mostly, I compartmentalize social outing to 2 hours at a time. If I extend it, I’m exhausted and feel crummy for the entire next day or two. If there’s a situation where I know it will have to be more than three hours, I make sure to rest and eat less the day before, and then eat minimally until the last hour or so of the outing. This way, I don’t have to feel like I’m running on empty during the entire outing, and I can prepare to be home for whatever the food decides to do, in addition to the exhaustion and pain that I know are coming.”
Patti went on to say that she feels her Crohn’s brought on menopause sooner, but also that her Crohn’s may have masked menopause symptoms because she was used to low-grade fevers and sleep interruptions.
“I found out I was post-menopausal at 50 and I basically missed the transition (the symptoms). I took that as a win (ha), but I do feel like my body is older than my age. I can’t really explain why, but the constant inflammation, plus my body trying to resolve it—I believe it’s taken a toll on my aging. But recently turning 60 feels AMAZING. TO be sick since I was 8 years old and have fought my way to my sixth decade feels like I climbed a mountain! I’m proud of how hard I’ve fought all these years, while still thoroughly enjoying life, my marriage, my daughters, and my career!”
Heidi was diagnosed with Crohn’s at age 50 after years of being told she had IBS. She found out in July 2023 that she had a” severe Crohn’s reoccurance after 5 years on Stelara. Her options were Skyrizi or Rinvoq since she has a history of TNF inhibitors failing her. Even though Rinvoq had a slightly better chance of putting her in remission, her and her care team thought Skyrizi would be a safer option due to her age. Rinvoq has a warning regarding increased cardiovascular events, such as heart attack, stroke, or death in people 50 years or older, along with risk of blood clots.
“If I don’t respond well enough to Skyrizi, we will then try Rinvoq, but the safety profile seemed better especially for me being over 60, and that’s important to me. I also worry about what is going to happen when I retire and my medical insurance goes from commercial to Medicare! I think they often have a deductible that is much higher than commercial insurance.”
Heidi was also diagnosed with osteoporosis in her 50’s and took treatment for it for 5 years.
“My risk for fracture still increases as I age, so my GI ensures I have DEXA scans every 2 years.”
Brenda had diverticulitis for a few years, and beginning in December 2011 she started having other bowel problems. She went straight to her general practitioner, and he ordered a colonoscopy, which confirmed her Crohn’s disease diagnosis at age 63.
“After many failed medications, I had part of my colon removed and I had a temporary ileostomy. Unfortunately, I got an abscess which made me really sick and in 2015 I had more colon removed and the stoma was made permanent. Since that surgery, I’ve been quite well and basically get on with my life without any IBD medication.”
Brenda is now 75 and worries about getting sick again and needing additional surgeries. She also worries that as she ages that one day she may not be able to deal with her ostomy bag herself and that concerns her.
Keith has ulcerative colitis and his wife was diagnosed in her 20s with ulcerative colitis. Her IBD was under control for years until she was hospitalized 20 years ago. She underwent her first operation then and it was successful. Fast forward two decades and she flared and required additional surgery.
“She’s doing ok now, but both surgeries were a result of her bowel narrowing.”
Jody is on Remicade and is currently in remission. She started with colitis in her 20s and then her diagnosis shifted to Crohn’s in her 60s. She’s in her early 70s now. She’s tried several biologics and medications.
“Not sure when I started Remicade. I have tried a few before and they were either too expensive or I had issues with them. I am in the United States so our insurance is not easy. I also have taken Mesalamine for years for colitis, which has worked great but it’s another expensive drug, so the prescription was cut in half due to cost a few years ago.
Sherry hasn’t changed much in her 44 years of living with Crohn’s, but has more of a focus on an overall healthy lifestyle.
“I’ve gotten better at avoiding trigger foods and being more diligent taking necessary vitamins. I’ve always been active (weight training, golf, and skiing) and remain so if not more these days. The introduction of biologics has obviously been a game changer a huge benefit.
Jeff says gastroenterologists seem to believe you more as you age.
“As you get older, more things in your body are broken. It’s a balancing act as to what is most critical. You also start running into unknown territory for GI docs, as many treatments do not have much data, if any, for seniors. GI docs do seem to believe you more when you need help.
Kanchan is currently 74. She has had a J-Pouch since 1989.
“For the last 4-5 months I am making probiotic yogurts at home and the last month I started making Kefir. I’m hoping for good results.”
Sherri– “I was diagnosed with IBD in 2015 when I was 56. I’m tired of the whole thing. What’s going to happen when I can’t look after myself?”
Closing Thoughts
It’s important for us to work closely with our healthcare teams, not only gastroenterologists, but all specialists, to manage IBD effectively as we age. It is beneficial to check in with a registered IBD dietitian, as aging may affect the body’s ability to absorb nutrients. I often wonder if when my kids are in high school or college (my youngest is 2.5!), if I’ll play a little Russian Roulette and try going off my biologic. I’ve been in surgery-induced remission since August 2015 and if this continues (God willing), I think I will try. Right now, as an IBD mom of 3 kids (ages 6, 5, and 2.5), I don’t feel confident enough that I won’t flare and need to pull out all the stops I can, so I can be present and well for my young family.
There’s a delicate balance with each decision we make along the way and the best we can do is advocate for ourselves, be proactive and take measures now to be healthy, do our research, and stay as educated as we can about what’s coming down the pipeline for the IBD community as we age. By controlling inflammation in our younger years, we can help improve our future quality of life and prevent age-related symptoms.
When you’re diagnosed with Crohn’s disease or ulcerative colitis it’s a lot to process. When I started this blog in 2016 and after living with Crohn’s for nearly 19 years, my focus has always been to be the voice I needed to hear upon diagnosis and what it was like to experience young adulthood with a chronic illness. As a 21-year-old, fresh out of college, I had to navigate my career, finding love, and becoming a mom with IBD on my own. The first decade I wasn’t publicly sharing my story and didn’t know there was a patient community to tap into online for support.
The first week I started experiencing Crohn’s symptoms-March 2005, Senior Spring Break in the Bahamas
Often as the years go by and we get beyond the initial shock of hearing the news and what this means for our lives, we tend to forget the challenges we faced to gain our footing. This week on Lights, Camera, Crohn’s I share some tokens of knowledge I’ve gained along the way that I hope will help you on your own journey, no matter where you find yourself at this moment.
Healing—physically, mentally, and emotionally is not linear. We all experience IBD uniquely—some people’s disease course is milder, others have it severe. We all cope differently with knowing and living with a chronic illness. Give yourself grace in the difficult moments. It’s ok to feel resentment or anger. It’s understandable to wonder at times “why me.” It’s “normal” to feel scared and anxious whether you’re a few weeks or a few decades in. Sometimes it’s taking things one hour at a time, other times it’s taking them one day at a time. Because of how quickly a flare up can strike, I try to live in the now and not worry about tomorrow.
You didn’t have control of getting your chronic illness, but you can control how you react and choose to heal from it. It’s easy to feel like you may be to blame if your health takes a turn for the worse. But understand this is not your fault. The unpredictability of IBD makes it feel like we’re often in the passenger seat and spiraling in circles, but this disease cannot control how you react, respond, and choose to heal from it. No matter what, you’re in control of the healing process. Whether it’s finding support through fellow patients and caregivers or through professional therapy, you won’t look back and you’ll be setting yourself up to take this on to the best of your ability.
There is no comparison game. Since the majority of people are diagnosed with IBD in their teens and into their 30s, it can be easy to try and measure your timeline and accomplishments to that of your peers who do not have chronic illness. It can also be tempting to look at people in the patient community who seem to have the world by the tail, when you’re struggling to get out of bed each day. This isn’t a competition of the sickest or a ploy to see who can smile through the pain and get more done. The only person you need to answer to, is who you see looking back in the mirror. You determine what you’re capable of and what you want in life. Your roadmap is yours and you’re right where you’re meant to be.
You set the benchmark for what’s possible. Your IBD is part of you, but it’s not your entire identity. Remember that even patient advocates are posting somewhat of a highlight reel. Even those who are working, in love, and parenting are dealing with their own struggles, too. My best advice would be to think about what you hope for in life (don’t even think of your IBD as part of the equation) and go after it. Yes, your health may cause some detours and roadblocks, but you won’t find your way unless you try.
No one knows your body better than you. I don’t care how many letters someone has after their name, they aren’t living in your body and experiencing what you feel each moment of every day. Be vocal when you need to be. Communicate as much as you can with your care team and paint the clearest picture of your reality. If you keep parts of your struggles to yourself or dumb down the severity of your day-to-day life, the only person you’re hurting is yourself. Learn about nutritional bloodwork and advocate for yourself to be tested for a full iron panel with Ferritin and Vitamin D. Get labs every 3-4 months so you can keep a finger on the pulse of what’s going on with your body. If you feel like your provider is being lackadaisical, don’t hesitate to get a second opinion. Take ownership of your health and find a provider who in your darkest moments you would feel most comfortable by your bedside in the hospital.
Make sure your GI specializes in IBD. There are gastroenterologists and there are gastroenterologists who specialize in Crohn’s and ulcerative colitis. Once you’re diagnosed with IBD, it’s imperative you try to find a GI who is an IBDologist. This can be tricky if you live in a rural area, it may mean you need to travel several hours to find a provider who fits the bill. If you move or are unsure of a good GI to check out, it’s helpful to reach out to your local Crohn’s and Colitis Foundation chapter and often they can help point you in the right direction.
Diet and stress levels matter. Read that again. Any doctor who tells you diet, and stress doesn’t impact your disease process is wrong. There are incredible registered dietitians throughout the US who specialize in IBD, and many of them have IBD themselves! Before you start restricting yourself or your child, make an appointment—most provide virtual options and this will help you get educated on what works best for you. What is a trigger for one person, isn’t necessarily a trigger for another. There isn’t a one-size-fits-all diet or else we would all do it.
Emotions will strike when you least expect them. Even almost 19 years in, I’ll sometimes break down and cry when I think about my Crohn’s or how it makes me feel. Just because you become a veteran patient doesn’t necessarily mean you fully ever heal from the hurt life with a chronic illness causes. It’s ok to have these moments where you may feel like you’re allowing your disease to control your emotions, you’re not. You’re human. It’s healthy to feel frustrated and to get emotional about what your life is like because you have IBD.
You’ve endured more than you give yourself credit for. As chronic illness patients we go through so much that often we don’t even bat an eye over experiences that would be extremely painful or stressful to the average person. Think about what a bad ass you are and how that carries over into each and everything you do in life. If you’re newly diagnosed you will get there—but even those initial weeks and months, you’re enduring more than the people who have their IBD under control and have a good handle on their body. No matter how many surgeries, scopes, scans, and IVs I’ve had, I always get a little teary eyed because it brings me back to 21-year-old me and then all the trauma that comes along with living with Crohn’s for 19 years. While those tears are sad, they also come from the strength of reflecting on what I’ve gone through to bring me to now.
Stay in tune with how your body is speaking to you through symptoms, do not ignore them. It can be challenging to communicate what you’re feeling to someone who does not have IBD. I get that. But by protecting loved ones, friends, and doctors from what you’re experiencing you’re preventing them from stepping in before it’s too late and before you know it your flare has gotten out of control and requires hospitalization. I used to be that person all the time. I would always internalize the pain, silently fighting through each day, doing anything possible to stay out of the hospital until the symptoms were simply unavoidable and required medical intervention. One hospitalization always sticks out in my mind. It was May 2009. I was a 25-year-old morning news anchor in Wisconsin. I was solo producing a 2-hour morning show dealing with horrible abdominal pain that kept making me throw up in the garbage can next to my desk in the newsroom as I struggled to put together the show. Finally, I couldn’t take it anymore and I had to call my co-anchor, who rushed me to the hospital. I was released from the ER hours later after my parents had driven from Chicago in the middle of the night only to return to the hospital that afternoon and have my dad carry me in his arms through the automatic doors. I was finally admitted and given the medical intervention I needed. Take it from me, you’re creating even more of an uphill climb for yourself if you don’t start speaking up when you initially notice something is awry.
The worst moments are just that, moments. When you hit your breaking point, when the pain seems overwhelming, and you can’t see the forest through the trees try to breathe. Go to your happy place. Recognize this is one day, one moment, I always tell myself “This too shall pass.” Go to your happy place mentally. Do mindfulness exercises. Shut out the outside world and focus on your breath. Detach from your body as best you can. Think of people who inspire you and bring you joy. Everything is fleeting. Each flare, each recovery, each prep, procedure, and surgery…it has a start and a finish. One day it will be a memory you talk about.
Pay attention to who is there when you when are quiet and when you’re going through the thick of it. IBD is too big to deal with alone. Lean on people you can trust, who you genuinely feel safe sharing your health woes with. This will be fewer people than you’d ever imagine. Be prepared to realize that many of the people you thought would be front and center to support you will be non-existent. It’s fine to mourn those friendships or relationships, but don’t waste your time or energy on them. Your disease will give you the ability to see who loves you and who wants to be present in not only the good times, but the bad. You can’t change people. Hold on tightly to the people who show up consistently, expecting nothing in return. Those are your people.
Emmanuel Acho shared a reel on Instagram recently that really hit home for me and caused me to reflect a bit on the people in my life and their roles. In the video he explains that friendship is like a house. You have your window, door, and floor friends. Window friends are outside looking in, they don’t know what’s going on in your house. They don’t have intimate access to what’s going on in your life. You can only let so many people into your house. Door friends come in and out of your life depending on the season. When life gets too hard or when your world turns cold, they might exit. Your friends might not be equipped for that season. Floor friends—aren’t going anywhere. You might track mud, but they will last regardless of the season. They are there to catch your tears and hear your fears. Remember—a house has more windows than it has doors and more doors than it does floors…if it has one good floor, you’re set.
Just because you need medication does not mean you’re taking the easy way out. I’ve been where you are. I remember lying helpless in a hospital bed and what it felt like to be told I needed to “break out the big guns” and start a biologic medication back in 2008 when there were only two options on the market for those with IBD. In that moment, we all naturally want to learn about side effects and what this could possibly mean for the long term. But please try and focus on the actual risk versus the benefit. As someone who has been on Humira since July 2008, I’m so grateful for my medication for allowing me to live a full life, bring babies into this world, and be a present, able-bodied, and active mom. It’s not all medicine, or all diet and lifestyle, often for many of us who have moderate to severe IBD we need a mix of both, and that’s ok. You can still thrive and be healthy, despite being on a medication with a black box label.
You are not a burden, and you deserve love. Any romantic partner who makes you feel less than, isn’t present when you need them most, or doesn’t show any empathy or interest in your daily reality isn’t going to stand the test of time. Use your IBD to your advantage to see your partner’s true colors. Be honest and upfront when you start dating and if you ever feel like you need to defend their actions or make excuses consider that a major red flag. Dating and marrying a person with a chronic illness isn’t for everyone, and that’s fine—but when it comes to people like you and me, we need a partner who is willing to take the challenge on beside us every step of the way. Find someone who you feel comfortable communicating openly with, who sees you for more than your disease.
IBD is not a battle to be “won” or “lost.” One of my pet peeves with any health condition or disease is when people say “so and so lost their battle”…they didn’t lose shit. Diseases are not a game. Oftentimes reaching remission is due to luck, disease severity, or surgery. I spent a decade of my life with active disease and have been in remission (thanks to surgery) for almost nine years. I don’t give myself credit for that, I’m not “winning.” It’s because of my efforts to stay diligent with my biologic, vitamins, safety labs, daily decisions, and check-ins with multiple specialists, but I also don’t think I’m at this point because of something special I’m doing compared to someone else. We’re all dealt a different hand of cards in life. Your IBD isn’t a win or lose situation—you’ll celebrate big victories and small ones, too, your disease can rob you at times, it’s a never-ending exchange and game of back and forth. You are not less than because you are flaring. You are not lazy for taking medication or failing because you struggle to follow a strict, regimented diet that may or may not help you. Once you stop thinking of everything as a “fight” it takes a bit of the stress, anger, and onus off your shoulders. IBD is a chronic illness, until there’s a cure, we’re in this situation until the day we die…that’s simply too long to be “fighting” anything.
Get ready to be extra proactive with your health. Due to the nature of our IBD and the medications many of us take, we are at greater risk for additional health problems. It’s important to get annual skin checks at the dermatologist. Make sure whether you have good vision or not that you’re seeing an eye doctor. Get cleanings at the dentist at least every six months. If you’re a female, make sure you get your well woman visits. We are greater risk for cervical cancer because many biologics don’t allow our bodies to fight off HPV, this may mean annual Pap smears. We’re also at an increased risk for breast cancer, so don’t delay your mammogram. Get a bone scan every 3-4 years, get one as close to diagnosis as you can so you have a baseline. Your GI may say it’s not necessary, it is. Steroids put us at risk for osteopenia and osteoporosis from an early age, this may mean you need to see a bone health doctor (yes, those exist). Those of us with IBD are at greater risk for pelvic pain, it can be helpful to see a Pelvic Floor Therapist who addresses those unique needs.
Faith can give you added strength and comfort. I understand faith is very individualized and looks different for each of us, but I can tell you as someone who is Greek Orthodox who has always been a faithful and prayerful person that I rely on my faith to guide me through my IBD each and every day. There’s a sense of comfort and hope that comes with believing God is watching over you through the good, the bad, and everywhere in between. When you’re diagnosed or flaring, it can test your faith. Hold on tightly to what you believe and lean on that (however it looks for you). I truly believe God gives his toughest lessons to his greatest teachers. One of my biggest fears as an IBD mom of 3 is that one of my children will get my disease one day. Each night before bed, I always pray with them and say, “keep my babies healthy, safe, and strong.”
My why. My motivation to push through each and every day.
Family planning takes time and effort. Just because you have IBD does not mean you can’t be a biological mom or dad one day. The journey will look a bit different, but this disease does not necessarily need to rob you of the experience if that’s what you want in your life. Communicate these desires with your GI so they can help prep your body for a baby. This can mean starting a prenatal vitamin and folic acid several months before trying. I had a colonoscopy before every pregnancy so that I could be given the ‘green light’ by my GI that we were cleared to try for a baby. When I was pregnant, my care was overseen by my OB, a maternal fetal medicine OB (high risk), and my GI. Unless you have perianal disease, you can have a vaginal birth, but oftentimes this is a discussion left to you and your care team. I personally chose to have 3 scheduled c-sections, because while I don’t have perianal Crohn’s, I didn’t want to risk tearing or causing a fistula to form. I would make the same choice if I had to do it all over again. I also stayed on my biologic through conception, pregnancy, and breastfeeding. These are all personal choices but there are many, many research studies available that show the safety and efficacy of doing so. If you feel you could have internal scarring due to past surgeries that could hinder your fertility, check in with a fertility specialist and have them help you investigate if there could be issues.
Educate yourself on insurance, prior authorizations, specialty pharmacies, and Pharmacy Benefit Managers (PBMS). Unfortunately, with IBD we are forced to do so much behind-the-scenes work to simply receive treatment and medication. You will waste countless hours and endless energy on the phone as these people give you the run around. Nobody ever seems to want to take ownership. Work with your gastroenterologist if you are denied a medication so they can write an appeal letter to insurance and go to bat for you. Stay on top of everything, don’t worry about annoying anybody. You gotta hustle. You gotta be frank and assertive. It’s not about hurting feelings; it’s about making sure people are doing their jobs and ensuring your course of treatment doesn’t get delayed because someone fumbles some paperwork. Our medications are time sensitive. Light a fire under people’s ass if you’re not getting responses you deserve. One of my friends on social media posted this over the weekend, “Managing specialty medications in January is an annual slap in the face to chronically ill people.” It sure is. This week will mark the first time I’ve ever received my injections late in the mail, due to a misstep in my GI office that I had to follow up on for over a week. Be extra proactive at the start of each year. Make sure your GI informs you about all the patient savings programs available, these can help you not only emotionally, but also financially.
You get the final say. No one but you gets to say what you do with your body. If a doctor wants you to do an enema before a scope and you don’t want to, don’t. If you don’t feel comfortable with taking a certain medication and your care provider keeps pushing it, they can’t physically make you pop a pill, take an injection, or receive an infusion. You must do your research, educate yourself every day, feel empowered by all you know and be ready to deal with the ramifications if you go against the grain or determine you want to try something differently. There’s not one “right” way to live with IBD. Be honest with your provider. Don’t say you’re taking a medication and then not take it, that’s not helping anyone or anything. Be a compliant patient, but an educated and empowered one at the same time. Measure all the risks and benefits and what your hopes and dreams are for your present life and for your future. Don’t ever feel like someone else can or should dictate what path your journey takes. Just because one biologic is a magic bullet for one person doesn’t mean it will be for you. You never fail treatments, they fail you. If a provider says “oh, you failed Remicade” … please correct them. “No, Remicade failed me.”
I write this as a 40-year-old mom of three—ages 6, 5, and 2.5 years old, married for almost 8 years, who has been on a biologic since 2008, who was diagnosed at age 21 in 2005. So much has changed for the better regarding the patient experience since that time. My perspective has come a long way. I used to be right where you are, so many are living your current reality. Instagram is the bread and butter for the patient community, that’s where you’ll find the most patients and caregivers transparently sharing. Follow the accounts, send a DM, comment on reels and posts, get engaged. Never hestitate to connect and reach out to me–natalieannhayden. Educate yourself through lived experiences and people who have paved the way for you, rather than Google. You don’t need to recreate the wheel, but this is your experience and your story. You get the final word on how you want each chapter to play out. Know each time you fall you will bounce back and that there’s a massive community of support here to catch you and cheer you on every step of the way as you rise once again.