It’s not surprising there’s stigma that surrounds gut health. Even though “everybody poops” it’s still a bit of a taboo topic, and don’t even get the general population to think about getting the dreaded colonoscopy. This is where the GH Foundation comes into play. Co-Founders, Dacia Heck and Kristin Lynn Grubehave both been personally impacted by gastro health in unique ways and their journeys inspired them to create a non-profit to help break down barriers and start critical, life-saving conversations.
According to the Crohn’s and Colitis Foundation, “patients with IBD appear to be at notably increased risk of colorectal cancer compared to the general population, with one recent study demonstrating a 7% colorectal cancer risk after 30 years of the disease. I had my first colonoscopy at age 21, which confirmed my Crohn’s disease diagnosis. Since 2005, I’ve had more scopes than I can count. I typically get a colonoscopy every year. While it’s not an enjoyable experience, it gives me peace of mind that I’m being proactive about my health. I’ll be getting my next scope in the coming months.
This week on Lights, Camera, Crohn’s we hear from Dacia and Kristin to learn more about their mission, the difference they hope to make, and how you can get involved and feel supported.
The personal connection
Until your gut starts causing health problems, chances are you don’t often think about it. Kristin was diagnosed at age 27 with Serrated Polyposis Syndrome (SPS), which is characterized by the occurrence of multiple polyps throughout the colon and/or rectum that can develop into colorectal cancer (CRC). She discovered this through a colonoscopy.
Kristin Lynn Grube, co-Founder of the GH Foundation
“My diagnosis has taught me to be my own relentless health advocate and speak up for myself. I continue to learn how to cope with SPS’s ongoing effects – emotionally, physically, and spiritually. Some days are easier than other days.”
Dacia lost her healthy, active sister from Stage IV colon cancer. Her sister was diagnosed at age 43 and passed away less than 4 months later.
Dacia Heck, co-founder of the GH Foundation.
“My sister’s diagnosis was a complete shock, as we didn’t have a family history of colorectal cancer and she was well below the screening age of 50 at the time of her diagnosis.”
The inspiration behind the GH Foundation
While Dacia and Kristin have different stories and experiences, they are both passionate about bringing important resources to the general public and are adamant about making gastrointestinal (GI) conversations not only more accessible, but also more mainstream, in order make the path to GI wellness and cancer prevention easier for others.
“We truly believe we can make a difference – one conversation at a time. As Kristin and I discussed where we wanted to focus our time and energy, we kept circling back to the “stigma” associated with GI diseases. That stigma often delays people talking to their family or medical provider about GI-related conditions. We decided the way we could make the biggest impact was to create GH Foundation and focus our mission on breaking that stigma,” said Dacia.
The GH Foundation’s main mission is to destigmatize conversations around GI, or gastro, health issues. 1 in 16 people in America will get CRC and 0 in 16 like talking about it. The GH Foundation encourages everyone to start the conversation. True prevention starts with educating the public on what is normal GI health and when to speak with a medical provider.
Discovering the loopholes in gastro health
As Dacia and Kristin did their research and spoke with different folks from all walks of life, they kept noticing that the conversations around gastro health have to start with a younger audience. Young adults in their late twenties to early forties are not discussing the importance of gastro health with their medical providers.
“We believe this is mostly due to the deeply rooted societal stigma surrounding gastro health. Given the uptick in early age onset (EAO) CRC, it may be too late to prevent a late-stage diagnosis once they qualify for screening. We want to focus on the very beginning and origin of it all – the conversation, whether it is with your family, friends, or network. Take that first step and reach out to someone, ask questions, make that list of symptoms you are experiencing, find out if you have a family history of GI diseases,” said Kristin.
While it’s intimidating, Dacia and Kristin guarantee that the first step will go a long way and may improve your quality of life, or even save your or someone else’s life.
“Our goal is to bridge the gap between the medical terminology and the general public’s knowledge about GI health. We are finding ways to make medical terminology and information accessible to the public. We encourage everyone to listen to their body, and to get the tools to empower them to speak up if they have issues,” said Dacia.
Taking their mission into action
The GH Foundation works to meet people where they are and find different ways to overcome the stigma. For some people, it’s learning about the basics of gastro health through an educational webinar, for others, it is hearing a survivor’s story and becoming inspired to take that first step.
“It’s connecting at a social gathering and finding a space where you can share your day-to-day challenges that you thought you were experiencing alone. Other times, we just want to have fun – we play GI trivia games and entertain each other with the Poo Squad mascots (more on that later in this interview). With all our events, we create an environment where it is safe to ask any questions. There is never TMI; we can talk about poop all day if you like,” said Kristin.
The Three Main Pillars of the GH Foundation’s Advocacy
Gastro Health
Inform and educate the public about the importance of GI health. So far, the GH Foundation has focused on the human GI anatomy, common myths and facts about GI health, ostomy facts, and CRC-related information. You can find out more about resources and past events on the GH Foundation website.
Proactive Advocacy
Proactively provide information and strategies to create positive shifts in how we communicate and influence others. Using what they’ve learn from other organizations, medical providers, patients, and cancer survivors, the GH Foundation has created educational content to then share with the public. Be on the lookout, you may just see their Mascots or Bristol Stool Charts popping up more and more near you!
Impact/Prevention
Educate and inspire people to take action to live a healthier life by fostering an open environment where no topic or question is off limits. Kristin and Dacia lead by example by first sharing something about themselves or asking someone at an event if they would like to share their experiences. They want to help people become as comfortable as possible about talking with their medical providers so they can get the most accurate information about their symptoms and find the best treatment for them.
Making a Difference
Since launching the GH Foundation, Kristin and Dacia have heard from many people that they scheduled their colonoscopy after attending one of their events or receiving one of their resources.
“People have also spoken with family members about their family history to get genetic testing and have said they felt more prepared about what to ask their medical provider at their next visit. People have approached us and expressed a sense of relief that we are creating an environment where they can ask any question, as uncomfortable or personal as it may be. Our mascots have received positive feedback as well. Seeing Sir Colon has taught them what the “colon” looks like,” said Dacia.
Through their initiative “GHF on Campus” they bring gastro health conversations to the forefront of young adult minds through a series of captivating events exclusively tailored to undergraduate students.
“One of our main approaches at the GH Foundation is targeting who we call the “pre-screening community”. Young adults under the age of 45 need to be made aware of common myths and facts on GI health, CRC signs and symptoms to keep watch, and what to ask if CRC symptoms emerge. GHF on Campus has a dual impact: Not only are they learning for themselves, but they can go back home and share what they have learned with family and friends. They can ask about their family history and encourage their family members to act, like scheduling a colonoscopy,” said Kristin.
So far, the GH Foundation has collaborated with the vibrant student communities at the University of Iowa and Northwestern University. Kristin and Dacia are looking to expand campus programming—if you’re reading this and would like to learn more, click here.
Finding humor through the message
You must meet people where they are. One of the ways they are doing that is with a sense of humor.
“We have designed our GHF mascots that bring some fun and lightness to topics that can be very overwhelming and serious,” said Kristin.
The GH Foundation’s mascot crew features: The Poo Squad (from left to right)—Ms. TP, Plungy, Mr. Poo and Sir Colon.
They will show up in different ways. One of the ways is our “Check your Colon” t-shirt with our very own Sir Colon. You can purchase a shirt here.
You can register now for a virtual webinar panel discussion entitled, “Destigmatizing Ostomy 101” taking place Tuesday, February 20th, 2023 at 6:30 pm CT. The discussion will feature Wound Ostomy RNs Jennifer Bart, MSN, RN, CWOCN, and Aimee Sheddan, BSN, RN, CWOCN.
Getting Involved with the GH Foundation
Talk – Initiate the conversation with your family, friends, and colleagues. Educate your loved ones about the risk of neglecting their gastro health. It may seem like a small step but can change the trajectory of life.
Volunteer – Help connect your community to life-saving resources about GI health.
Donate – Your donation directly funds our efforts to distribute educational materials and health guidance to the public.
Engage – Reach out to us! We welcome new ideas on how we can break the stigma.
Follow us on our socials so we continue to reach more and more people.
Connect with the GH Foundation on social media and follow the amazing work they’re doing:
When you have IBD and need a biologic, it used to be all infusions or self-injections. But starting in March 2022 (for ulcerative colitis) and May 2023 (for Crohn’s) a daily pill known as Rinvoq (Upadacitinib), entered the game. Rinvoq is the first approved oral product to treat Crohn’s. This once-daily pill is prescribed for those with moderately to severely active IBD who have had a lackluster response or an intolerance to one more TNF blockers (such as Humira and/or Remicade). Rinvoq is also prescribed for rheumatology and dermatology conditions, such as rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, non-radiographic axial spondylarthritis.
Doses range from 15 mg, 30 mg, or 45 mg. According to AbbVie’s website, “Rinvoq is a selective JAK inhibitor based on enzymatic and cellular assays. Rinvoq works with your body to fight the inflammation that can lead to IBD symptoms. Rinvoq stops the activity of some inflammatory proteins known as Janus kinase (JAK) to help reduce inflammation.
This week on Lights, Camera, Crohn’s we talk with 29 IBD patients about their personal experience on Rinvoq, along with Dr. Uma Mahadevan about key information for those in the family planning stages of their lives.
What patients have to say about the induction dose and the quick improvement in symptoms
Rinvoq is the first JAK inhibitor medication that Brooke tried and she didn’t know what to expect. She started Rinvoq in July and says her body has done a complete 180.
“All of my immediate issues have healed, and my long-standing symptoms have begun to fade. In the beginning during the loading dose, I felt a bit more tired. But after two weeks, I had more energy and have experienced less symptoms. Most of my extraintestinal manifestations have cleared up.”
Brooke says she has caught two colds since being on it, so she’s still masking and being diligent around crowded spaces, especially during flu season. She advises fellow patients to talk to their physicians about the dosage they need.
“Because of how much I’ve been flaring, I’m on a higher dose longer than I may have been if I started in a healthier place. Make sure you and your care team agree on a dosage that is not only good for you, but also that you agree with.”
Brooke sets alarms to take her meds because she is used to an infusion or subcutaneous injection, and it’s important not to miss a dose of Rinvoq.
Tonya: I’m only two weeks in, so still on the induction dose, but this is the first time my symptoms have been somewhat controlled in four years.”
Sarah: “I just started Rinvoq and it’s helping me come out of a flare up.”
Melissa: “My 17-year-old son has been on Rinvoq for about six months after Xeljanz failed him. He’s doing great on it and it’s super easy since it’s a pill once a day. He has also been on Humira and Entyvio in the past. Rinvoq has been the easiest transition so far.
Jennifer L.: “I went on Rinvoq after Remicade failed me and then went on Cyclosporine to bridge the gap before I could switch to Rinvoq. I started it in December of last year and this has been the one drug that has subsided a lot of the symptoms. No nocturnal bowel movements, the only major side effects I’ve had is some acne, but I would say it’s hardly noticeable. I did have to come off hormonal birth control as a side effect can also be blood clots, so you can’t have two drugs that increase your risk of that together. I’m single and wasn’t really thinking about dating coming out of a huge flare, so it was a no brainer for me there. If you’re looking to get pregnant, I’ve heard you can’t be on it because studies have shown birth defects, so that’s a concern potentially for some women or for contraceptive options given that you’re only limited to non-hormonal options while on this.”
Krista: “My fiancé just started Rinvoq and after one day he was feeling better. His energy is up, he has an appetite again, and is showing significantly less signs of inflammation. We still have a journey, but it’s been a miracle drug for him.”
Lizzie: “I have been on this now for 3 months after Humira and Stelara stopped working. So far, my Crohn’s symptoms have subsided. I’m no longer flaring. I would say since taking Rinvoq, I feel more fatigued, but apart from that, I feel really good.”
Marla: “I started Rinvoq 24 days ago, so I don’t have a lot to tell you. I don’t think it’s anything bad. It’s hard to tell if the medication is working yet. I do blood work in November.”
Lauren: “I’ve been on Rinvoq for about one year now. Didn’t work at first, but found out I simultaneously had C-diff. I was on vancomycin and Rinvoq for about 4 months and was scoped for the first time in 4 years because I was in remission. I ended vancomycin and flared again. I will be transitioning to Skyrizi soon, but even though I’m not in remission, Rinvoq has been the only thing that has gotten me in the best place I’ve been in 4 years. I love the ease of one pill a day, no infusions, no shots, etc.”
The main reason Lauren can’t stay on Rinvoq is that it’s not safe for pregnancy and she hopes to have another child. She’s bummed this medication is the only thing that’s shown her improvements and that she needs to switch.
Amber: “I just started Rinvoq last week, so perhaps it’s too early. I am adding Rinvoq to Entyvio for fistulizing Crohn’s. The one thing we are trying to figure out is how it works with an ileostomy. I tend to have a fast track and has passed pills in the past and Rinvoq is an extended release.”
Dana: “I’m currently on Rinvoq! Although I’ve only been on it for 3 weeks, I don’t have any real side effects so far.”
Lindsay: “I’ve only been on Rinvoq for about 3 weeks. I was hoping for a more dramatic change based on things I have read. My fevers have gone away, and I feel like I have more energy, but I still go to the bathroom just as much and the urgency has not changed. I also had to give up breastfeeding to start Rinvoq, so that was hard!”
Sarah: “I started Rinvoq after Humira was not putting me in remission after 1.5 years on it (even with methotrexate added to help). I saw an immediate improvement in my stools. I might have a few pimples as a side effect. It’s only been 3 weeks, but so far, so good!”
Erica: “I’ve been on Rinvoq since May. I haven’t had any improvement. I was hoping when I started that it would work for me. I heard so many people call it their miracle drug. I was scared to try it at first because of all the warnings, but once I started it, I was hopeful. Unfortunately, it was not my miracle drug and I had to add Skyrizi to it…I’m still not better.”
Denise: “I’ve been on Rinvoq for about 7 years. I’ve been part of a clinical trial. I don’t think I have anything bad to say about it. I was so sick with few options, so I took a risk, and it fixed me. I don’t think I’ve had any side effects. I still get scoped annually as part of the study and my intestines have looked great. Sure, I still have tummy troubles, but not the main Crohn’s ones! I get blood work done every 3 months and everything has been normal there as well.”
Abigail was prescribed Rinvoq in late August 2022. At the time, she was hospitalized with the worst flare she’s ever had and was admitted 3 separate times for a 37 day stay. She was facing steroid and Remicade failure and running out of time before requiring emergency surgery. Abigail was given the option of trying Rinvoq for 2 weeks. If it didn’t work, surgery would be required to remove her colon. Her care team got insurance to approve it and she started it right away. Abigail took a double loading dose. Usually, you do 45 mg for 8 weeks, but she did it for 16 weeks instead.
“This medication not only saved my colon, but arguably my life, as I had faced death twice during that hospitalization. I was able to get off steroids. I now take 30 mg of Rinvoq daily and I’m in clinical remission. My next colonoscopy is at the end of this month, so it may show even further remission. I was nervous to start Rinvoq, since it is so new, but given the circumstances, I agreed to it. I am honestly so glad I did. The only side effect I have experienced is high cholesterol. My care team will be addressing this after my colonoscopy. I am forever grateful to Rinvoq for giving me my life back. I choose to do medication and therapeutic diet (SCD). For me, this combination has really helped.”
The visible side effects
Jessie started on Rinvoq to treat her Crohn’s before it was FDA approved because of a flare she couldn’t get under control. She was put on the 45 mg dose for 2 months and saw quick improvements in how she was feeling. After years and years of being poked and prodded for infusions and labs she says she’s so grateful to give her body a rest and just take a daily pill.
“Rinvoq has been like a miracle drug for me. Despite the side effects of weight gain, constipation, and acne on my face and body, I don’t even care because it’s the best I’ve felt in more than 5 years. I’ll take the acne and backne any day.”
Jessie spent hundreds of dollars on skin products and through patient support groups she was recommended CeraVe Moisturizing Cream with Salicylic Acid and CeraVe Body Wash with Salicylic Acid and has noticed a huge improvement. Both products are available over the counter.
Madison: “I am on Rinvoq and I hate it. Let’s say first, it works fast. Within 48 hours, my symptoms were gone, and it’s done a great job at keeping my UC in check. However, the side effects are awful. Acne is the most common side effect and I have it everywhere. My face used to be dry, but now it’s VERY oily. My cholesterol has gone up, which is a known side effect and doctors are keeping close tabs on it. Lastly, weight gain. Weight gain was recently acknowledged as a side effect and I’ve had that, too. The first-generation JAK inhibitors were notorious for weight gain, so I’m not sure why it wasn’t acknowledged in this second generation.”
Madison adds that it’s hard to acknowledge that Rinvoq is working well, but it comes with its fair share of side effects. While the side effects are annoying, she says they are not as bad as a flare.
Alexandra: “I took Rinvoq for 5 months. It did absolutely nothing for my UC, but it gave me horrible acne.”
Lisa: “I was on 45 mg for 3 months. I hated it. I had some sort of infection the entire time and had bruises everywhere. I started Skyrizi three days ago.”
Elizabeth: “I’ve had great results on Rinvoq, I take 30 mg along with Entyvio. My only complaint with Rinvoq is the acne.”
Jenna: “I just stopped Rinvoq. I had a horrible face rash as a side effect. It seemed like an acne flare when it started back in early August and no matter what I tried, it got worse and worse. My dermatologist and doctors both believed it was some sort of rash caused by being on immunosuppressant drugs and stopped my Rinvoq. I took an anti-parasitic and the acne is mostly cleared up.”
Kelly: “I started Rinvoq and only completed 6 weeks (the loading dose and start of the treatment). Insurance issues were part of the reason why I stopped taking it. I also knew that I wanted another child. If I was able to…and there were minimal to no studies for a safe pregnancy. The only symptoms I had were small rashes on my hands and feet, kind of pimple like, not painful or concerning…just something I noticed.”
Jennifer V.: “On Rinvoq and love it!! It’s a pill so it’s easy and it has put me mostly into a therapeutic remission. The cons: weight gain, fatigue, elevated liver enzymes, and anemia. All in all, if you are not having any more children, I would highly recommend this medication. I would need to see more time and research if I were to recommend it prior to pregnancy.”
Jennifer V. had to go off Rinvoq last week while she was taking Paxlovid to clear up Covid and she lost weight for the first time in ages. Now she says she’s back on Rinvoq and the weight is coming right back.
Emily: “I have had Crohn’s and lupus since 2020 and I took the highest dosage of Rinvoq, and it didn’t do much to help me. While I was on it, I thought I saw some improvements, but as soon as I went off it, I realized it wasn’t doing much good. It made my skin break out really bad. I often would pass the pill whole when going to the bathroom. It’s a big pill, easy to see. I’m on Skyrizi now and hoping to reach remission.”
Kendall: “I’ve been on Rinvoq about 3 months. My symptoms have improved, but I’m surprised at how many of the side effects I have experienced: styes, mouth sores, cold sores, and acne. I’m planning to stay on it. My IBD is not stable yet, but I’m hopeful Rinvoq will get me there. Afterwards, I’ll see if diet and lifestyle can maintain remission. It’s nice that you can start and stop Rinvoq!”
Implications for pregnancy and breastfeeding to consider
Sarah: “I just started Rinvoq and it’s helping me come out of a flare up. I am wrapping up my third month. I started to feel improvement after two weeks. It’s such a relief to take a pill after self-injecting for the past 15 years. So far, I don’t have any bad side effects. The only thing that stresses me out is that you can’t be pregnant while taking it, so as a 34-year-old, ready to have a second child, it’s in the back of my mind—how am I going to get off (and back on this), how will I keep my Crohn’s under control when I’m pregnant next? But, in the meantime, I’m grateful that it’s helped me get control over a bad flare that caused me to take a medical leave from my job.”
Allie: “I feel like I had a good experience on Rinvoq. I would say the good is that it works very fast. I was starting to feel better from my flare within 3 days. I was able to get off prednisone because it worked so quickly. The bad is that Rinvoq made me gain weight that I haven’t been able to lose, but my doctors won’t confirm it’s related to the medication. I also felt very bloated all the time. I did not like having to take a pill every day (going from being on Entyvio), so I would sometimes forget to take it. The last thing for me is that I’m still hoping to have another child and it’s not safe for pregnancy, so it was not a long-term option for me, even though it helped me achieve healing from a flare.”
Carmen started taking Rinvoq in February after multiple biologics and non-biologics failed to treat and manage her ulcerative colitis. So far, she says her experience has been very positive. She went into clinical remission within the first month of being prescribed 45 mg.
“I’ve since been tapered down to 15 mg and it’s still looking very positive. Bloods, calprotectin, and how I generally feel has massively improved, along with my quality of life. The negatives I’ve experienced so far have been some mild skin issues, mainly rashes on my face, chest, and upper back, this is currently controlled by over-the-counter salicylic acid face and body wash. I’ve also picked up a few fungal infections and have lost my big toenail because of one of the infections that required antibiotics. For me, these are minor issues and outweigh the overall treatment plan. My GI believes as we’ve decreased the dose to 15 mg, that these minor side effects will disperse over time.”
Carmen says taking a once daily pill is much simpler than some of the other biologic drugs that require visiting an infusion center and taking multiple other medications either intravenously or orally. The cost for me is relatively high for Rinvoq at $150 a month, but this will depend on what medical insurance and copay you have. All in all, Carmen says Rinvoq has been a positive experience and has done what other medications have failed to do.
Important Considerations Regarding Family Planning While on Rinvoq
Dr. Uma Mahadevan, MD, Director of Colitis and Crohn’s Disease Center at University of California San Francisco and lead investigator of the Pregnancy in IBD and Neonatal Outcomes study (PIANO) says when it comes to Rinvoq, the medication has been associated with birth defects in animals at the same dose as given to humans (30 mg), so she avoids prescribing this in pregnancy.
“I do not prescribe Rinvoq to someone who is about to get pregnant. However, Rinvoq is generally given to people who have not responded to anti-TNF, so if Rinvoq is the best medicine for them, I do not hold the fact that they are a woman of child-bearing age against them and give them the therapy to best put them in remission.”
Dr. Mahadevan says if a woman is on Rinvoq and becomes pregnant she has successfully transitioned patients to Skyrizi. This can be more challenging with UC as there are fewer options. The PIANO study is currently researching the safety and efficacy of these drugs. There are several Skyrizi patients being monitored right now and 2 Rinvoq patients so far. You can learn more about being a part of PIANO here. I participated in PIANO with my youngest child as an IBD mom who is on Humira. Being a part of this research is invaluable for our community and helps current and future families.
It’s believed that Rinvoq crosses into breastmilk, so you should avoid feeding your baby that way if you are taking this medication.
Rinvoq Complete Patient Support
Much like other biologics, there are patient support services in place that you want to be aware of. RINVOQ Complete provides personalized patient support when you need it. With RINVOQ Complete, you get 1-to-1 assistance with finding potential ways to save on the cost of your prescription and more. I use Humira Complete for my prescription needs.
You can also get help making sense of your insurance and finding ways to fit Rinvoq into your everyday routine.
If you have commercial insurance, you may be eligible to pay as little as $5 a month for your prescription with the RINVOQ Complete Savings Card. Click here to sign up for your RINVOQ Complete savings card.
Final thoughts
It’s important to remember that just because someone has a miraculous experience or a terrible one with a specific drug, does not mean that you will. I will say, with all the biologics that I’ve covered on Lights, Camera, Crohn’s the visible side effects (weight gain and acne specifically) were the most widespread and common among the patient population. So many of you said you felt guilty feeling “vain” about not wanting to be on a drug because of that, and I want you to know those feelings are valid and matter. At the end of the day, we all must measure risk vs. benefit and what matters most when it comes to keeping our IBD in check.
You can check out other Patient Experience articles that I’ve covered here:
It can feel like a bad break up. You build trust and rapport with a medical specialist who feels like family after overseeing your complex chronic health condition for years and then boom out of nowhere you find out they are moving away. Or maybe you’re relocating and trying to rebuild your dream team of health care providers. Whether this change is brought on by you or your care team it can feel a bit overwhelming to start anew.
My gastroenterologist of 8 years announced she was leaving on the Patient Portal in August. I was out running errands with my kids when a fellow IBD patient and friend texted me and shared the news. My heart sank and my stomach dropped, it never crossed my mind that she would ever leave. What do you mean SHE’S leaving? The doctor who finally got me into remission and has kept me there for nearly a decade. The doctor who oversaw all my family planning, pregnancies, and postpartum. The doctor whose rooted me on after each scope and always had an aggressive and thoughtful game plan no matter what twists and turns we face.
Unfortunately, this is the nature of the beast. I wrote a heartfelt “thank you” explaining my genuine gratitude for her efforts to always go above and beyond and all that she did to be extremely responsive and attentive to my needs. For the past 8 years when I send a Portal message, I always received a phone call from her—whether she was in clinic or on her cell. This time was different. This time there was radio silence and a one line canned thank you message from a nurse in the office. Just like that our worlds were not interconnected. I made a point to get my routine safety labs the Monday of her last week so that she could provide insight one last time. This time she didn’t comment on any of them and left September 15th without saying goodbye. It felt a bit like a slap in the face and stung.
As a chronic illness patient, we tend to feel a sense of comfort by care providers who help manage so much of our lives. This was a reminder to me that at the end of the day it’s a job for many and that even though we may feel that closeness, that bond may just be a façade. At the same time, I’ve also learned that some medical settings don’t allow doctors to communicate with patients, so who knows.
This week on Lights, Camera, Crohn’s I share tips for how I’m navigating finding a new GI that I think may help you along the way. I’m still feeling a bit lost and don’t know what the future is going to hold or what IBD Center I am going to land at, but I want to take you along for the ride.
The first steps to take
If a care provider is leaving the office or moving out of state, you will generally be placed with another doctor from the same team. This is not always a seamless transition though. Each doctor has a reputation. Some people want to be seen by a female care provider; others want a male. Years of experience and the college they graduated from and where they did residency may be of utmost importance to you. Just because the office says you can see “so and so” now, doesn’t mean you can’t speak up and advocate for what you’re looking for. In the realm of the healthcare world, you’re back to being “single” now and you can find who is the right match for you. Don’t feel pressured into anything. The long-term goal here is for a long-lasting relationship with a care provider who makes you feel like more than a number.
I have seen three different GIs in my 18+ years since my Crohn’s disease diagnosis. The first was incredible. I just so happened to meet him during my initial hospital stay, the day after I was diagnosed in the emergency room. He practices in my hometown (a Chicago suburb) and oversaw my care for a decade—even when I lived in Minnesota and Wisconsin while I was a news reporter and anchor.
When I moved to St. Louis in 2014 and my Crohn’s was flaring, I knew I needed to find a local provider. So once again, during a hospitalization for a bowel obstruction, I connected with the GI who was doing rounds at the hospital and loved his bedside manner. I felt safe and like I had found another great doctor. Unfortunately, while under his care I was very sick. We couldn’t figure out why my Crohn’s was so out of control. By the third hospitalization in 15 months, even while ramping up Humira injections to every week, and after several ER visits, his partner called me while I was in the hospital and said I needed an MRE to get to the bottom of what was happening. I did the MRE and was called back by that same doctor (not my GI) and he coldly told me over the phone that I needed a bowel resection—either the next day or in 10 days. He said I could go home and build up my strength. I chose to wait the 10 days. My actual GI never visited me in the hospital, never followed up…I knew it was time to drop him like a bad habit.
Enter in my most recent GI. Everyone raved about her. My colorectal surgeon and friends from the local Crohn’s and Colitis Foundation chapter all said she was the one to go to. So, I did…and now 8 years later I feel a bit stressed about starting the hunt for a great doctor all over again.
Amazing doctors can fall right into your lap, but sometimes you need to do some digging and research.
The behind-the-scenes work
At the end of the day, I find the most helpful advice comes from fellow IBD patients. There are several ways you can approach this.
Look up GIs in your area who specialize in IBD. This is key. You don’t want a run of the mill GI, if you have Crohn’s or ulcerative colitis you need a GI who specializes in IBD.
Check out online reviews and what people have to say about them.
Do a call out on your social media and see if anyone locally has any recommendations or personal experience. You want to hear the good, the bad, and the ugly. I have gained incredible insight this way. I had one fellow IBD friend message me about her experience with the provider I made an appointment with—and it made me a bit concerned. This week during my well woman visit, another IBD mom, who happens to work as a nurse practitioner in my OB’s office, told me about her awesome GI who is in the same group—so I plan to switch my appointment per her recommendation. This insight is GOLD.
Interview several GIs. Don’t feel pigeon-holed by only meeting with one possible new provider. Make a few appointments and see who jives the best with you. I have two appointments in January with two new GIs. My last clinic appointment was March 2023. I was supposed to be seen in October…that’s the soonest I can be seen.
Come up with a list of questions and see whose responses give you peace of mind and make you feel empowered to take on your IBD.
Be mindful of the office staff and how they treat you on the phone.
Make a pros and cons list of staying with your current GI team or starting fresh.
Decide if the doctor’s gender matters to you. I’ve had two male GIs and one female. I personally enjoyed having a female during my family planning and pregnancies, but now that my family complete it’s not *as* important to me, but still preferred.
To switch offices all your records and a referral will be needed by your current office, so make sure all your ducks are in a row and that the two offices have communicated. I made it clear with my current office that I am being seen by both IBD Centers, to see who is the best fit for me.
What questions to ask possible new providers
You may be wondering what to ask a new doctor or where to even start with your saga-long health history. We all know how rushed clinic appointments can feel. Here are some of the questions I plan to ask in January once we get the basic health questions out of the way.
How often will you be seeing me in clinic?
How often do you like patients to get labs? What kind of labs will you draw?
Will I keep my current medication regiment (ex. Biologic)? Will I stay with the originator/reference product biologic or are you planning to switch me to a biosimilar. Note: For you to be switched, your GI has to write a script for that to happen.
What days of the week are you in the clinic to see patients? If you have childcare or work conflicts, this can help so you know if their schedule/availability matches with your needs.
What hospital(s) do you treat at?
Are you apart of any research studies going on?
How often do you like patients to get a colonoscopy?
If I need pain medication to manage my symptoms, will you prescribe it? My last GI refused to—and I found that to be ridiculous.
Do you perform intestinal ultrasound here and if you don’t yet, when do you plan to?
If I run into insurance issues, will you go to bat for me and write an appeal letter or do what it takes to make sure I receive my medications on time?
Final thoughts
It’s jarring and takes a lot of time and energy to find a new provider but stay positive and know there are so many incredible gastroenterologists out there who genuinely care about patients and about helping our community out in any way they can. You are not civilly bound or married to your doctor—it’s not about hurting feelings or trying not to be a bother, be bold and do what’s best for you. I’m grateful to be in remission right now. My heart hurts knowing so many patients going through this same ordeal, while flaring, don’t have the luxury of taking their time or the privilege of living near an IBD Center with options. I always try and tell myself and I think this perspective will help bring you clarity, too—think of yourself at your sickest, lying in a hospital bed. Would you want that person leading your care? If there is any doubt or hesitation, keep looking for the right doctor for you.
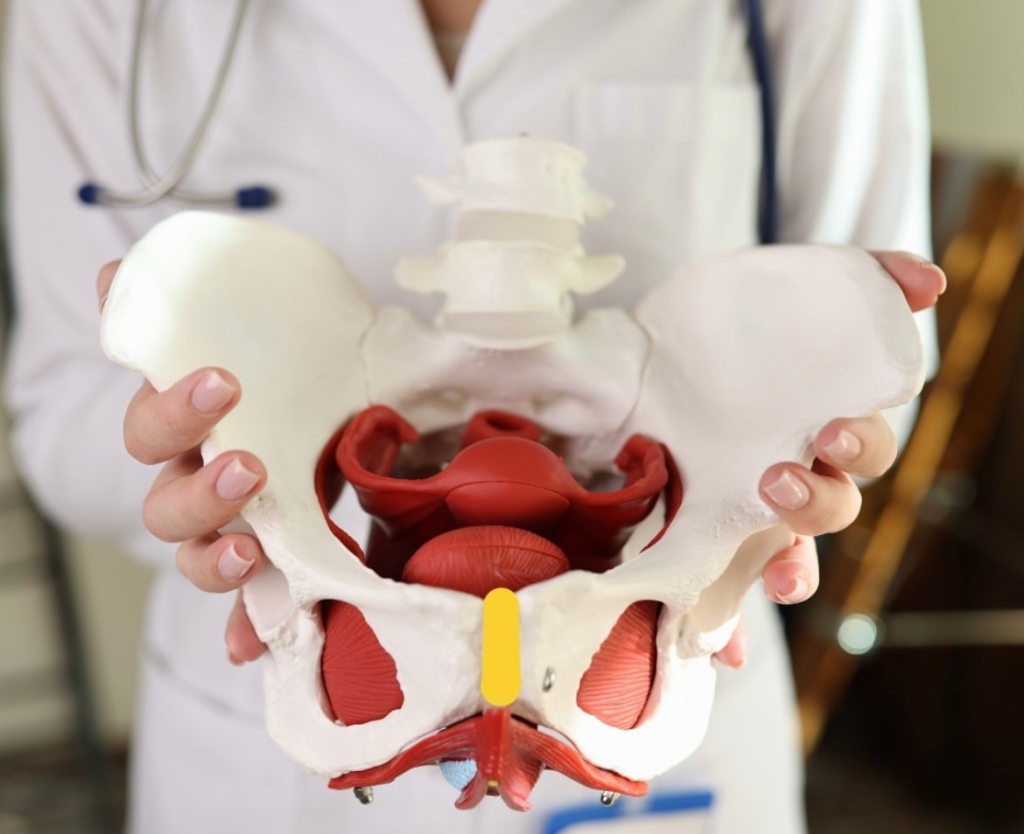
Chances are you’ve heard of Pelvic Floor Therapy but may not know what this entails or why so many people in the IBD community are talking about it. Individuals with IBD can have persistent symptoms of fecal incontinence, constipation, rectal discomfort, and diarrhea, despite having their IBD in remission with medical therapy. These persistent and often debilitating symptoms can have a major impact on your wellbeing and quality of life.
This week on Lights, Camera, Crohn’s we hear from two gastroenterologists from Mayo Clinic along with several IBD warriors who provide insight, helpful guidance, and information about pelvic floor therapy.
What exactly is Pelvic Floor Therapy?
Pelvic floor therapy is a treatment program performed by pelvic floor therapists to retrain the pelvic floor muscles to address underlying issues such as constipation, fecal incontinence, or urgency. Many patients with IBD in remission may develop pelvic floor dysfunction which is usually diagnosed from a digital rectal examination in combination with an anorectal manometry test.
“During an anorectal manometry, a small catheter with sensor probes and a balloon is placed into the rectum and is connected by a wire to the computer. During the test you are lying on your side and asked to perform maneuvers to determine how your pelvic floor muscles work. At the end of the test, they inflate a balloon in the rectum to help evaluate for sensation and then ask you to simulate having a bowel movement by pushing the balloon out,” explained Dr.Katie Dunleavy, MB BCh BAO, Gastroenterology Fellow, Mayo Clinic.
Based on normal values for your age and gender, you may be diagnosed with a pelvic floor dysfunction. Dr. Dunleavy went on to say that in IBD, there is less research on the benefits of pelvic floor therapy.
“But we have seen benefit in up to 80% for patients in remission who continue to have symptoms of constipation, urgency, or incontinence once active inflammation is fully ruled out. Similarly, some patients with IBD undergo total proctocolectomy with ileal pouch anal anastomosis (IPAA) may also benefit from pelvic floor therapy if they have issues emptying their pouch,” said Dr. Dunleavy.
Additionally, those with IBD who’ve had pelvic floor surgeries might experience sexual dysfunction and this type of therapy directed towards relaxation of the pelvic floor can lead to a better sexual experience.
Pelvic Floor Dysfunction does not discriminate across genders
Any person can develop pelvic floor dysfunction and may benefit from treatment with pelvic floor therapy in the right setting.
“While most studies describe pelvic floor in females, I believe individuals from all genders deserve evaluation of their pelvic floor the recommendation for pelvic floor therapy. Furthermore, individuals of a transgender experience, might undergo gender affirming surgery that impacts their pelvic floor muscles, and would benefit from pelvic floor therapy,” said Dr. Victor Chedid, M.D., M.S., Gastroenterologist at Mayo Clinic.
Dr. Dunleavy says, “As many as 50% of people with chronic constipation have pelvic floor dysfunction, which means there is impaired relaxation and coordination of the pelvic floor and abdominal muscles during evacuation. Some common symptoms include straining with hard bowel movements, a feeling of incomplete evacuation, pain with intercourse, or urinary symptoms.”
Certain risk factors make it more likely for men or women to develop pelvic floor dysfunction, this includes instrumented vaginal deliveries, chronic constipation with straining, prior surgery, prolapse, and age. It is important for men and women to discuss symptoms with their doctor to ensure they get the appropriate testing and treatment.
Apprehensive about getting looked at?
It is important for people diagnosed with pelvic floor dysfunction to seek out a qualified pelvic floor therapist who is specialized in GI and evacuation disorders. These are generally physical therapists or occupational therapists who complete extra training in pelvic floor therapy.
“You should find a therapist you trust and will feel comfortable with during your therapy sessions. The therapists who work in this area are fantastic and work diligently to explain what they will be doing. My patients tell me that the relief they feel from therapy well exceeds the apprehension they had prior to starting sessions,” said Dr. Dunleavy.
It’s important for patients to feel comfortable talking with health care providers and addressing concerns they may have on this topic. Dr. Chedid typically discusses the benefits of pelvic floor therapy with patients during clinic visits as a beneficial treatment option that does not require surgery. He provides patients with exercises and techniques to do at home that will have a major impact on general wellbeing and health.
“Individuals with IBD experience significant “negative” experience with the bathroom and with defecation that can be quite traumatizing, and therefore when they get in remission, they still have a negative association with the bathroom and might have “fear of defecation” despite being in remission. I equate that to “PTSD of the pelvic floor”, which is not a medical term, but an analogy I use. Therefore, pelvic floor therapy is essential to reverse this negative experience with the bathroom and make their bathroom experience a healthier and satisfying experience. Almost all patients who I describe this to get it right away and understand the importance of pelvic floor therapy,” said Dr. Chedid.
He adds that it’s imperative health care providers communicate with patients and ensure that the therapy session will be a safe space with at rained physical therapist who is trained in empathetic and trauma informed care. This is essential in putting a person’s mind at ease, as many patients might have experienced sexual trauma in their lifetime that makes pelvic floor therapy triggering for them.
The impact of Pelvic Floor Therapy post operatively and after IBD pregnancy
If you’ve had a total proctocolectomy and an ileal pouch anal anastomosis (IPAA), you might experience non-relaxing pelvic floor dysfunction or pouch evacuation disorder. This is similar to the rectal evacuation disorder in individuals with pouches.
“Typically, this is identified by history, physical exam, pouchoscopy, anorectal manometry and dynamic imaging of pouch evacuation. Additionally, someone who has had any form of trauma to the pelvic floor, including Perianal Crohn’s disease or surgeries for Perianal abscesses or fistulas or lacerations due to vaginal deliveries after pregnancy, these patient might experience rectal evacuation disorders after recovering and healing. In the proper patient, if identified by history, physical exam and the right testing, these patients will benefit from pelvic floor therapy,” said Dr. Chedid.
At the same time, there isn’t a lot of research on pelvic floor therapy in the post-operative state or following pregnancy in patients with IBD.
“There have been several attempts to find normal values for patients with IPAA who have undergone colectomy to help diagnose pouch related pelvic floor dysfunction. We generally recommend patients wait until the anastomosis following surgery is completely healed prior to having an evaluation with a balloon to ensure no complications. Similarly, patients who have recently undergone delivery from pregnancy will likely require time to heal. I would discuss this with your doctor to have more personalized information,” advised Dr. Dunleavy.
If your GI recommends pelvic floor therapy for your personal symptoms and struggles the overall response is tremendous.
“Recommending pelvic floor therapy to everybody, without identifying the right patient who would benefit from it is not typically beneficial. Therefore, in the right patient, pelvic floor therapy is extremely effective,” said Dr. Chedid.
What IBD patients have to say
Stacey has ulcerative colitis and went from having an ostomy to becoming a j-poucher. She’s a big proponent of Pelvic Floor Therapy. After her 3-step surgery to j-pouch in 2021, she knew she needed at least an evaluation from a pelvic floor physical therapist (PFPT) after urination became a challenge and inserting tampons became impossible during her takedown recovery.
“My surgeon wouldn’t write me a referral, citing that the anorectal manometry tests prior to surgery were all normal. My GI doctor didn’t want to go against the clinical judgement of my surgeon, so I couldn’t get one from her either, and finally I received a referral from my OB/GYN after explaining that penetrative sex was impossible (and felt unsafe to me) to even attempt,” Stacey explained.
These delays resulted in 5 months of significant pelvic pain that she felt ill-equipped and under-supported to handle, and this time could’ve been saved if she had gone into surgery with a referral to see PFPT from the get-go, even if she didn’t need to use the referral; it would’ve been nice to have.
“It’s so wild to me that orthopedic surgery has extensive PT rehabilitation protocols, and yet I was met with such resistance to gain access to the professionals who could help support my muscular recovery, even after such extensive GI surgeries,” she said.
During Stacey’s initial encounter with the PFPT, she spent the majority of the visit trying to gain a strong understanding of her entire pelvic and holistic health history, everything from sexual health to physicality to surgery, and all the in-between.
“She asked for consent prior to any invasive exams and explained them in thorough detail, reminding me that I was in control and could always choose to stop an exam if I felt unsafe. She continued to breathe with me during the exams and communicated her findings in real-time, which made me feel at ease. At the conclusion of our visit, I was told that I was experiencing hypertonic pelvic floor dysfunction from a decade of clenching for dear life trying to make it to the bathroom with mod-severe UC, even before my surgeries. The tightness of the muscles, coupled with three extensive pelvic surgeries, contributed to the pain and issues I was experiencing,” said Stacey.
During the visits with the PFPT, Stacey discovered she had no awareness of her pelvic floor muscles whatsoever. She could not distinguish the relaxation of the muscles from the contraction, and the entire area felt numb to her, like it was a holy, empty space. She says this made the exercises challenging to understand initially. She was prescribed specific exercises, not Kegels, including strategies to gain awareness of supportive muscle groups so she could begin to engage with this part of her body and start to heal.
“What I did not expect, however, was for this experience to be as enlightening and empowering as it was. Slowly but surely, the little life things showed me that they’re the big life things: being able to fully urinate in under 20 minutes, FINALLY being able to use tampons again- these were MASSIVELY important to my quality of life, and they became possible through the help and support of a PFPT and my adherence to their prescribed exercise regimen. I even realized one day while holding one of my exercise poses that I could feel the muscles DEEP in my abdomen! They felt heavy, full of pressure, as if they fired on to greet me, and then suddenly… I could feel them gently, slowly, RELEASE. I cried tears of relief realizing that I had been fearful of reconnecting with these muscle groups, and it really was safe and okay to be in my body.”
Stacey says she had NO idea these muscles existed, yet here they were. Had they been here all along?! She says she numbed them out from years of associating the deepest parts of her with pain from UC; and that her brain was protecting her. I truly wonder. All she knows is the day that she could FEEL her body experience relaxation and safety with FULL awareness of these pelvic muscles is the day that she knew that healing from these surgeries was going to be possible.
After one year of PFPT, Stacey “graduated,” not free of pain, but with the tools to know how to live within the ebbs and flows of pain. She tells me she still relies on the tools and bodily awareness that she gained through the experience.
Jessie was diagnosed with Crohn’s disease when she was 15 years old and after more than 22 surgeries later, at the age of 38, she says she completely underestimated how much her pelvic floor was affected over the years by the inflammation, surgeries, and her pregnancy.
“I was “guarding” badly (a response to pain) and so weak. I was having bladder issues, pelvic pain, rectal pain and so much more. After 2 years of being consistent going to pelvic floor therapy and doing the exercises I can say I’m about 85% better. I can’t say enough how much of a HUGE difference pelvic floor therapy made in my life and my IBD journey. My therapist explained it to me like this “you don’t have orthopedic surgery on your knee, wrist, ankle, spine, etc. and not get prescribed physical therapy. Same with an injury. It’s just standard procedure. But, for some reason, even though your pelvic floor consists of tons of muscles, ligaments, tendons, bone, etc. the same process is not considered – but IT SHOULD BE!” Your pelvic floor needs to be rehabbed after any injury, strain, surgery, etc. just like any other muscle/tendon/ligament/bone in your body,” explained Jessie.
Claire started PFPT because all imaging and tests showed that while her inflammation is under control, she still experiences extreme pain.
“I was tested, and they found I have dyssynergic defecation. This was caused by my chronic pain due to long-lasting fissures as well as chronic constipation. I’m grateful my GI thought to have me tested for this, as many don’t make that connection since the symptoms are so similar to Crohn’s. During PT, I have learned that my muscles do not relax and are constantly tense, so we work on trying to get them relaxed in order to successfully pass bowel movements. Like all other PT, one downside is that it is a lengthy process and takes up a lot of time. I have a one-hour appointment every week for 12 weeks and an hour or two of exercises and stretches on my own every day.”
She says she’s started to notice improvements and found ways to make her pain more bearable, though it’s something she will have to continue working on for a long time.
Tiffany has accessed pelvic floor therapy for herself and having previously been a physio and a fellow Crohnie, she recommends people speak with their doctors because it can make a world of difference, especially after surgery, hospitalization, or a flare.
“The neural connection we have to our trunk and pelvic muscles can be re-trained and strengthened, allowing less pain, and for me an improved sense of control over urgent bowel movements.”
Preslie was diagnosed with Crohn’s in June 2016, and after two years of battling severe symptoms, she had a colonoscopy that showed she was in remission. It may sound like lovely news, except Preslie was still living with a ton of pain, so her and her care team started digging for answers.
“This led to an Endometriosis diagnosis in August 2018. That was great news, except I STILL was not getting relief, and started having severe burning anytime I urinated, but always tested negative for UTIs. I went to a male urologist who told me I was just constipated, which was not the case. After well over a year of extremely painful sex, constant pain, and burning when I peed, I went to a urogynecologist who talked with me for less than 10 minutes and had the diagnosis: Interstitial Cystitis and Levator Ani Syndrome. I finally felt heard. I started pelvic floor therapy shortly after and immediately felt relief.”
Rocio says pelvic floor therapy was recommended to her by a home health physical therapist who was treating her for neuromuscular issues after bowel resection surgery for her Crohn’s in 2020.
“During my resection recovery, I was struggling tremendously with constipation, which was unfortunately always my issue with my IBD. Although uncommon, it’s been my reality for the last 20-plus years. The reason I share this is because I wish someone would have recommended pelvic floor therapy to me over all those years.”
She began seeing a pelvic floor therapist in January 2021 and completed two years of treatment. During that time, Rocio says she learned a lot about the intricacies of all the muscles, the nerves, the internal blood flow, and so much more. Because of two fistulotomies and a stricturplastly, she has numerous anatomical issues which prevent her from having normal bowel movements.
“Pelvic PT changed that completely and I have normal/formed BM’s every single day, without any signs of constipation and without any straining. I’ve learned ways in which I can help relax and release the pelvic floor should I face issues in the future.”
Separately, Rocio has learned how beneficial pelvic floor therapy is for many IBD patients post-operatively, including the ileal resection she had. Her therapist worked on her abdomen significantly during appointments to prevent adhesions and scar tissue. She says there are so many benefits to pelvic floor therapy that it does make her wonder why more IBD health care providers aren’t encouraging patients to pursue care.
Annie started pelvic floor therapy two weeks ago. She was referred based on suspected interstitial cystitis, not her IBD. She was shocked to learn during her first appointment that treatment was for all conditions that involve urgency of any kind.
“The game changer was the pelvic exam itself, I never realized what my PT noticed right away, which is that my first layer of pelvic muscles are unnaturally sensitive. This is massively helpful for IBD and IC, but the most validating part was having a lifetime of excruciating intercourse and painful pap smears and knowing the reason. My PT told me this is not how my life has to be. After just two weeks of exercising my pelvic muscles with a vaginal wand and daily targeted yoga, my urgency, both with my Crohn’s and IC, has gotten so much more manageable. I started this journey running to the restroom every 30 minutes (even at night), now I feel like I’m starting to get my life back.”
Jasmine says pelvic floor therapy helped her a ton following j-pouch surgery.
“I truly believe it should be integrated into post-op care plans, I had to seek it out and ask for it.”
Amy says that while she doesn’t have experience yet with PFPT, she has a complicated Crohn’s history for the past 25-plus years. Now that she’s over 40 and has had three vaginal births, she recently asked her doctor about pelvic floor therapy.
“Because of all the IBD women sharing their journey with this on the Internet, it inspired me to look into therapy for myself. In my first request, the response was that it might be a fantastic idea, but to wait and see. My next visit is in a couple of weeks and I’m looking forward to utilizing this article to share and take with me to help me advocate for myself.”
A look at the insurance piece
Yes, pelvic floor therapy can be covered by insurance, but it can vary based on the type of insurance. It is also important to ask about coverage for biofeedback therapy which is an essential part of the therapy based on prior research studies. Many insurance companies will need proof of diagnosis using an anorectal manometry with balloon expulsion test or defecating proctogram.
“If the proper indication based on testing is identified with the referral to pelvic floor therapy with a script written by someone’s GI provider, then typically insurance should cover it,” said Dr. Chedid.
Closing thoughts on Pelvic Floor Therapy and IBD
It is important to discuss with your doctor if pelvic floor therapy is right for you. Once patients with pelvic floor dysfunction have these basic tools, they can begin retraining the pelvic floor muscles with biofeedback. Biofeedback provides auditory and visual feedback to help retrain the pelvic floor and relax the anal sphincter. Biofeedback training is the treatment of choice for medically refractory pelvic floor constipation, with some studies showing improvement in more than 70 percent of patients. Patients also learn to identify internal sensations associated with relaxation and long-term skills and exercises for use at home.
At Mayo Clinic patients have had more than 70% response at 3 months following initiation of pelvic floor therapy. The response usually takes weeks to months to see a clinical difference and requires patients to practice their exercises and biofeedback at home.
“Although many centers are familiar with retraining techniques to improve pelvic floor dysfunction, few have the multidisciplinary expertise to teach patients with constipation how to appropriately coordinate abdominal and pelvic floor muscles during defecation, and how to use bowel management techniques, along with behavior modification, to relieve symptoms. Because pelvic floor dysfunction can be associated with psychological, sexual, or physical abuse and other life stressors, psychological counseling is often included in the evaluation process,” said Dr. Dunleavy.
If you have chronic pain, you may also need to see a physician to have these issues addressed prior to starting pelvic floor therapy.
Key takeaways from fellow IBD patients
PTs are an excellent resource, but just like getting an IBD-ologist is superior to a general GI doctor, PFPTs are an even stronger resource, ESPECIALLY in the context of chronic GI disease where so many of our deepest muscles are constantly working on our behalf.
You can always say “no thanks!” You don’t need to agree to any sort of exams or exercises that you’re not ready for, and a compassionate PFPT will empower you to make decisions and communicate in alignment with your body’s needs.
ANYONE can benefit from PFPT: any age, any gender.
Normalizing pain and discomfort is a survival instinct, but it’s not necessarily serving you for the GOOD life- it’s okay to get evaluated if you’re concerned about sexual pain or dysfunction, pain with periods, or if you also have IBD and simply want to be sure that you’re supporting your pelvic and spinal muscles the best you can so that you can, especially in the bathroom!
YOU get to decide! Having an evaluation may be all you have the capacity for, and that’s okay! You can return for a plan of attack later, or you can wait until you have the capacity to dive in head-first! There’s no one right way.
If you decide while talking to a PFPT before they do ANY manual evaluations that something doesn’t feel right- YOU GET TO CHOOSE, and you can always, always say, “nevermind”. Advocating for your body is always progression in your healing journey, every single time.
SPEAK UP! It’s RIDICULOUS that patients have to ask and ask and ask for the bare minimum, but if it helps your quality of life and it’s within your capacity- it’s certainly worth it.
A big deterrent for patients can be cost, but the investment is worth it, if you can swing it. You would be surprised how much every system of your body is so connected and feeds off one another!
Helpful resources to check out
Find a Pelvic Floor Therapist Close to Home
Utilize the “Section on Women’s Health” or the “Herman & Wallace” websites. Both these groups train therapists who specialize in pelvic floor disorders.
The Section on Women’s Health (SOWH) website has a “PT Locator” tab. You can enter search criteria including your geographic location (e.g., zip code) and specialty (e.g., constipation) to identify a therapist closer to home.
The Herman & Wallace website has a “Resources” tab under which you will find a “Practitioner Directory.” Use the map features to locate a therapist near you.
Utilize the “find a provider” section of www.pelvicrehab.com for a local PT by zip code.
The therapists who work with pelvic floor disorders may be in Gastroenterology, Urology, Gynecology, Physical Medicine, and/or Women’s Health, etc. You may be able to find someone through your local physicians or contacts.
For those in Canada, check out the Canadian Physiotherapy Association. It has a “Find a Physiotherapist” tab which allows you to connect with the sites of participating provinces/territories. By specifying a “Women’s Health” therapist or equivalent, you may find someone who specializes in the field of incontinence, pelvic pain, constipation, etc.
The benefit of pelvic floor therapy also involved patient education, relaxation exercises, diaphragmatic breathing, and correction of maladaptive toileting behaviors. Some studies have shown improvement in quality of life relating to symptoms, and mental health.
To receive biologic infusions at home or within a medical setting? That is the question. As an IBD mom of three who has done self-injections for 15-plus years, it’s intrigued me to see how many people in the IBD community now receive at-home infusions. This inspired me to dig deeper and hear firsthand what fellow patients have to say about their experience. When polled on Instagram—out of 260 votes, 55% of IBD patients prefer at home infusions compared to 45% who would like to receive their medication in a medical setting. This week on Lights, Camera, Crohn’s hear advice, guidance, the role insurance plays in all of this, and perspective on treating your IBD at home versus at an infusion clinic or hospital. I learned a lot and I think you will, too!
Discussing Home Infusions with your Care Team
If receiving your infusion at home interests you, here’s what you can do to get the ball rolling on making it happen.
Talk with your GI about whether home infusions are an option in your area and if they feel comfortable with you doing so. Discuss the risks and benefits. Your GI will need to write a prescription.
Call your insurance and make sure home infusions are covered in your health plan.
Amanda has been doing Remicade infusions at home since the pandemic started and she says it’s been much better for her. Being able to receive her medication at home and cuddle with her 4-year-old daughter and dog are big wins for her. Recently, she also receives daily IV fluids, and thanks to her Port and home health, she’s been able to do it herself.
Amanda: “Home infusions have changed the game for me. They make me feel safer as someone whose immune compromised. I almost always have the same nurse, and I don’t have to commute before or after. How grateful am I!”
She says how you coordinate setting up home infusions is dependent on your insurance. Personally, after talking with her insurance she found a list of home health agencies within 30 miles of her house and called and spoke with a few.
“Some did not administer my medication, some charged separately for nursing fee, and some were not taking new patients. Once I found a good option for my family, the home health company reaches out to your GI doctor, who then sends the script to the Specialty Pharmacy, rather than to an infusion center.”
When Bad Veins and IV issues Set You Back
One of the main reasons I chose to do a self-injection rather than an infusion was because of how horrible my veins are. When I was told I needed to start a biologic during a hospitalization in July 2008, it was the same hospitalization where it took three people and eight tries to start an IV on me. To this day, I’m still a bit fearful of getting IVs because of that traumatic situation. Several people wrote to me with the same concerns—this is something to consider if you typically need a Vein Finder for hospital visits and procedures.
Olivia: “I initially loved the idea of doing infusions at home. My first one went smoothly, the nurse had a bit of trouble finding a vein and drawing blood, but no problems after that. The ability to do my infusion in my bed or on my couch was so much more comfortable than the hospital! But then, the next two infusions, the nurse had trouble getting a vein and one had to be rescheduled because of hospital policy. That infusion took over an hour to find a vein. After that, we spent a month trying to convince insurance to let me go back to the hospital so I could use the ultrasound to get IVs placed. Ever since, I’ve been doing infusions at the hospital. The idea of doing infusions at home was nice, but it didn’t work for my situation.”
Meredith: “I get my Entyvio infusion at home. I don’t love it. It is more convenient than having to go to the hospital/office, but nurses often have trouble starting IVs on me and at home they are the only option. There is no backup and I’ve had a few bad experiences. Things have gotten better because I now have in my profile that I need pediatric needles, but they aren’t the standard, so those types of needles are not always supplied. The insurance decided for me that I would receive my infusions at home because it’s cheaper and since I’ve never had allergic reaction. The service by me is different, but there is no future scheduling. You know around the date that your next infusion is and then you’re contacted one day beforehand with a time. I’m too high strung to be comfortable with that, but it is what it is.”
Much like Amanda, Meredith loves having her dog there for support. When she initially started getting home infusions her dog needed to stay outside the room because she was too interested in what was going on, but now she’s used to the process and equipment and can snuggle.
Heidi: “My insurance made me switch to home infusions. At first, I was nervous because I’m a hard stick and always require a vein finder. I also just felt safer in a hospital setting. But, I’ve been doing home infusions for three years and I love it. I have my “old faithful” vein and I like being in my own home with my own bathroom and other comforts. I also have wonderful nurses whom I look forward to seeing each time. Everything is so much more personal this way.”
Melissa: “Sadly my veins are awful, and I wouldn’t want to chance the one person who comes not being able to get an IV started.”
Concerns from the Community Regarding Home Infusions
Ashley: “With my ulcerative colitis, comes other chronic illnesses. Which is true for a lot of people in our community. I have POTS, so having my infusions done in a healthcare setting is more reassuring for me because there’s more safety nets in place.”
Emilie: “I don’t get my infusions at home anymore (I used to!) because I hated it. The nurse was always texting me to reschedule, I was always having to deal with CVS trying to get my medication delivered on time, and I had to store all the stuff. It also made me feel like a “patient” in my own home. Mentally it was incredibly stressful organizing and coordinating everything and feeling like I was constantly sick because the medical equipment was always around. I much prefer going to an infusion center, where I just show up and they have everything ready to go. Just another perspective—I know a lot of people love getting infusions at home and I’m in the minority, but there are cons to consider.”
Mary: “I don’t currently do an infusion medication, but I have in the past with Remicade. My GI office set home infusions up for me after I did the first few in the office. It was more convenient for me due to the office being about 1.5 hours away from where I live. I was provided with an IV pole to keep at home among other supplies and a nurse came to my house to do the infusion. It was awkward at first, but after a few times it got better. Unfortunately, during one infusion, I had an allergic reaction unexpectedly, during which the nurse had to give me Benadryl and another medication. After that happened, I couldn’t do them at home anymore and had to go to the office. After two more infusions, my GI discovered I wasn’t responding to Remicade anymore and I had to switch to Stelara. The cons are the risk of something happening and not being in a medical setting. Luckily, I had a great nurse who knew what to do.”
Adam: “I prefer the clinic and the reason is, when I was on Humira and had to self-inject, I always worried I didn’t get it in the right spot or the full injection and miss some of my medication. For me, it’s a piece of mind that my infusion is done properly.”
IBD Moms Experience
Miranda was diagnosed with Crohn’s during the height of the pandemic. When she started Entyvio it was in an infusion center, and she felt like she was putting herself and her family at risk each time she went in. By receiving infusions at home, you can potentially be exposed to fewer hospital-acquired infections. This is especially important for individuals with compromised immune systems, as it helps minimize the risk of additional health complications.
“I saw a few ladies (connections on Instagram) who were receiving home infusions, so I asked my doctor about it. He said it would be no problem to connect me with a company in Dallas that handles nursing and medications for in-home infusions. My only obstacle was seeing if my insurance company would approve home nursing. After calling them to go over benefits, my insurance informed me I could receive in-home nursing. I did have to escalate the call to get it pushed through. At the end of the day home infusions were approved. The same company that ships my meds provides nursing. I do have to make a phone call every January to make sure coverage is good, but other than that it’s a flawless process. The nurse and I are close friends.”
Christina: “I specifically told my GI I don’t want to get infusions at home because I like my “me” time in the infusion clinic. Two hours to read my Kindle in peace! I also decline the accelerated rate…perspective changes when you have kids. My nurse jokes they’re my spa days!”
Krista: “I moved to home infusions once I had my daughter. It was more convenient because I didn’t have to find someone to watch my daughter (I had nobody to help or to ask) so that I could attend my infusions. I had a pleasant experience, and the nurse was fantastic. Being able to do infusions in the comfort of my home was fantastic, especially needing an infusion only 2 weeks postpartum, while recovering from a c-section.”
Getting adjusted to receiving medication without support from fellow patients in the room
Kristi has been receiving Remicade at home monthly since January. Her GI office stopped doing infusions at their office due to staffing issues. After a time or two at the hospital-run infusion center, her insurance company called her to see if she’d be interested in home infusions. Since she had been driving an hour each way for years, she jumped at the chance!
“The idea of not having to worry about getting my infusion during a winter storm was enough for me. My doctor’s office was hesitant at first. I was always on board with the idea, and I was shocked to see the cost was similar to my doctor’s office but significantly less than an infusion center. Home infusions have allowed me more flexibility in scheduling. I also feel like my resting period post-infusion is much easier since I’m already home. While I love home infusions, there are some downsides. I don’t think I would have wanted this back years ago when I started infusions. There’s a lot to be said about the community and the support I received just by being in an infusion room with similar patients. It was also nice to be in my doctor’s office monthly, where I could easily report any symptoms, I was having health wise. I am the person that needs to have my house looking perfect before company comes over, so that adds an extra level of stress during an infusion week. It’s also a bit odd to have the nurse here for so many hours. However, I’ve had two nurses so far and they’ve always been very good and very respectful in my home and if I wanted quiet time. Overall, I don’t think I could go back to going somewhere.”
Kristi says now that she doesn’t have the infusion room support, she relies even more on the social media community and the IBD family online. She also loves getting to snuggle with her dog and use him as a heating blanket while she receives her infusion.
Final Thoughts
Balancing the risks vs. benefits. As you’ve read, home infusions are not a one-size-fits-all approach. What works for one person, doesn’t for another. While the benefit of being at home is a big one, having to worry about the sole nurse at your house finding a vein and not knowing if you’re going to have a bad reaction are just some of the cons that can make the experience worrisome for people.
The convenience of home. Home infusions offer the convenience of receiving treatment in the comfort of your own home. This eliminates the need to travel to a medical facility and allows you to maintain your daily routine more easily. For IBD parents and caregivers it alleviates the need of finding childcare. By fitting infusions into your daily life, it helps to reduce the disruption that may come with hospital or infusion center visits. So many of us deal with medical PTSD and having the comfort and familiarity of home can help to ease that burden a bit.
Kat: “I received home infusions for years for UC. My doctor’s office got them set up because I live in a rural area. The pros were the convenience and being in the comfort of my home. The cons were having a stranger in my home for over an hour. Dealing with the company’s billing department was also horrendous.”
A more personalized treatment experience. You can have a dedicated healthcare professional who gets to know you and your specific needs, creating a customized care plan to address your individual symptoms and concerns. Many IBD people I speak with have a close bond with the nurse who visits their home and feel supported during the process.
Jill started on Humira and was later switched to Remicade infusions. She started receiving infusions at the hospital and then her GI recommended she try home infusions to limit exposure to germs.
“My GI’s office took care of the paperwork and I had the choice between two home health companies. This has been a game changer for any guilt I felt around missing work, because the nurse comes to my home and I can continue working on my laptop, if needed. Or I schedule infusions to begin at the end of my work day. I have a great relationship with my home health nurse and she knows me and my veins so well now. I value the relationship and level of care as well as the flexibility I have found with this option. It’s a win for my mental health as well.
Matt received home infusions for seven years. If he could pass along any advice, he says to be even more proactive about your health.
“I had to always coordinate shipments, supplies, and the infusion schedule. The pros are the flexibility and comfort, but the cons are not being at an infusion center where you can unplug and be in your own thoughts.
It’s important to discuss the option of home infusions with your healthcare team to determine if it’s a suitable choice for you. Your care team can address any concerns or questions you may have, educate you on the process, and help you make an informed decision. Remember, you have options and support to manage your IBD effectively, even when it comes to receiving necessary infusions.
Lights, Camera, Crohn’s: An Unobstructed View is officially SEVEN years old! If you told me when I started blogging what a labor of love this website would become for me, I never would have been able to imagine what it would become for my life, for the IBD community, and for patient advocacy efforts. I went into blogging blindly. I had no clue how to format the site, but I knew the types of stories I wanted to share and the messages from patients that I wanted to get across.
As a seasoned journalist who spent nearly a decade as a TV news anchor, reporter, and producer, I’ve used my love for storytelling to try my best to be the voice I so desperately needed to hear upon diagnosis, through my professional life, finding love, family planning, pregnancy, motherhood and beyond. It’s been quite the ride these last seven years. My first article went live July 23, 2016, on the 11th anniversary of my Crohn’s disease diagnosis. I found out I was pregnant with my now six-year-old, two days later. The first six years of Lights, Camera, Crohn’s (and 3 kids later), I shared a new article every single Monday.
Through these seven years, Lights, Camera, Crohn’s has been viewed half a MILLION times, by more than 320,000 people around the world. On this site alone, I’ve shared 368 articles, which does not account for the countless other IBD articles I’ve created for other websites. As I reflect on this milestone, I’m proud of what I’ve accomplished thus far, but know there’s much more work to be done.
This week I want to give you a behind-the-scenes look at how my storytelling process comes to life—I often get asked “how do you become a patient advocate?” and “how do you start blogging?” I hope this advice inspires you to take the plunge, as there are endless seats at the proverbial advocacy table and your voice, your story, your valid experiences, deserve to be heard.
Choosing What’s Newsworthy
It can be overwhelming trying to come up with content that is new and fresh for your blog and social media. I’ve found it extremely beneficial to have an editorial calendar that helps guide the stories that I share. My editorial calendar is in my email in the draft folder. I simply list out the dates (articles have always been shared on Mondays on Lights, Camera, Crohn’s…so I list out all the Mondays for the next 3-4 months). This serves as a reminder of my game plan and when I need to do outreach for the stories.
As a journalist you’re taught and it’s almost innate in some ways to always be on the lookout for a story. I’m always keeping my eye out for tweets and posts on Instagram, conversations in real life, experiences that happen to me when I see my GI or get a scope, that I think will resonate with our community. I think about the pain points I’ve felt along the way and the advice I wish I had when I was struggling in certain moments. I think about the questions I’ve had along the way when Google was scaring the bejesus out of me, and I just wanted real life advice from someone who understood my reality. Think about what uncertainty, questions, concerns you’ve had and what you want to learn more about and then go after the story.
Writing for the Reader
Everyone has a unique writing style, but one of the most common “mistakes” I tend to see with blogging is when writers go on and on and on about their own experience. The articles sound more like a diary entry—and if that’s what you’re going for, great—but usually, you’re wanting to draw readers in. To do this, I use my own experience as a foundation—a sentence or two in the intro and then the rest of the article is written to and for the reader. Try to write your blog articles like a news story. Use sub heads, get reliable sources, attribute studies, share credible information. Give readers in the chronic illness community news they can use. Empower others on their patient journeys so they learn something by checking out your content. Let others see that they are not alone in what they are going through and that you get where they are coming from. By including the expertise of medical professionals, it helps your articles really come to life and allows you to build a rapport and a reputation with the GI community. It’s always incredible to hear when a GI shares Lights, Camera, Crohn’s with their patients.
If you’re unsure how to reach a GI who is not your doctor, I advise going on Twitter and sending doctors a DM asking if they’d be interested in providing input for an article you’re working on. 9 out of 10 times you’ll get a yes. As we all know, doctors are busy, so try and give them a longer lead time to respond to interview questions. I like to include a headshot when I quote a doctor, so I have them send you one.
My Patient Experience articles have become one of my favorite parts of Lights, Camera, Crohn’s—these articles are a major labor of love. I interview 10-20 patients, along with physicians, and spend upwards of 20+ hours out of the goodness of my heart to create a resource that a patient and caregiver can have at their fingertips when they’re trying to make major decisions about how they choose to manage their disease. Topics range from biologics to infertility or life with an ostomy. Rinvoq is coming up next, folks…I just need a breather since I finished writing Skyrizi earlier this month. By crowdsourcing and sharing the good, the bad, and the ugly I’ve been able to provide a complete look at the reality patients face and provide background that shows more than just my experience.
The Art of Interviewing
Whether you’re interviewing a fellow patient or a healthcare professional, the same process goes a long way. Try thinking about the main points of the article and the flow before you write the questions. You almost must think backwards. I do all my interviews over email—for multiple reasons. The number one reason, is that as a mom of a 6-year-old, 4-year-old, and 2-year-old, I don’t get many breaks and trying to conduct an interview over the phone or Zoom and capturing the true essence of what someone is saying is nearly impossible. I also prefer email because it gives people a chance to articulate their responses and enables me to accurately share their quote—word for word, without paraphrasing. I rarely give interviews over the phone, as I like fellow writers/editors/journalists to have what I’m saying verbatim.
When I send the interview email for Lights, Camera, Crohn’s, I provide a deadline in bold and then list the questions. I always ask for a high-level explanation of a person’s patient journey so I have an understanding of what they’ve been through and so I can paint a clear picture for the reader. Try to never ask “yes” or “no” questions—you want people to give good explanations and descriptions.
An example of email outreach to a pediatric gastroenterologist for an article I worked on.
Often the most important question you can ask if “Anything you’d like to add?”—in TV, podcasts, you name it, this is when people let loose a little bit and can provide you with key nuggets of information.
Once I receive the interview responses, I open up Word, and take all the content and start compiling what’s going to be a quote and what’s going to be a part of my wording/storytelling. Then, much like journalists do in TV news, I write the story around the quotes.
Have a Copy Editor (aka family member/friend review your content)
It’s always helpful to have an extra set of eyes on your articles before you share them. Since the day I launched Lights, Camera, Crohn’s, my mom has been my “copy editor.” I email her a draft of the article along with an explanation of what I’m hoping to get across and then she goes through each article with a fine-tooth comb and provides edits and feedback. If I get too fired up about something, she may politely advise I take a certain line of the story out or re-think how I word a sentence. She’s been my voice of reason through this entire process and as my mom, she’s my biggest cheerleader in not just life with Crohn’s, but everything. As a nurse of more than 40+ years, she’s also well versed in medical situations, as well as grammar.
Be Vulnerable and Transparent
Despite how many people advocate for IBD, Crohn’s and ulcerative colitis still have stigmas. It can be daunting to put your words down on paper and share them with the world. I spent the first decade of my disease just telling close family members and friends. What I’ve found since blogging and being a vocal patient advocate, is that by being open, you open yourself up to endless support and camaraderie. There is such strength that comes from saying you’re not ok or need help. Tell it like it is and don’t sugarcoat your story. At the time same, one of the main pillars of my advocacy has to always been to be transparent, while also positive.
Back in the day when I was diagnosed, and those first 10 years when I was living in silence, most of the content I read was pretty doomsday. While I understand and empathize with the pain and horror Crohn’s can cause in one’s life, I’ve tried to never sit in that sadness for long. If anything, IBD has given me perspective and clarity about the fact that IBD doesn’t have to destroy your life or who you are. Yes, it can create major complications, unpredictable setbacks, and hurdles, but those detours don’t have to rob you of what you hope to accomplish or become. While it’s important to be real, I find it just as important to provide hope and inspiration for those who wonder what their futures may hold.
Keep on Swimming
Due to social media algorithms and the lack of engagement many of us see online, it can feel disappointing at times when you put all this effort into an article or a blog and feel like you’re talking or reaching no one. I’ve been there countless times. Don’t let the “likes” or the follows deter you. Know that your words and your stories just need to get into the hands of one person who needs them, and that makes all the effort, time, and energy worth it. Your articles have legs—meaning that once you post them, continue to post, and share for months and years to come because these “evergreen” articles are always timely and necessary. Try to collaborate with others when you can. If news outlets reach out for a quote or if a health website asks for your input, give it—and then ask for your blog to be a part of how you’re attributed in the quote. If you see someone’s Instagram story referring to an article topic you’ve covered, grab the link and send it their way over DM.
If you feel like you’re in a rut or if you’re having a tough time creating content—don’t force it. Ask your followers what topics they’d like you to cover. Use the timing of the year to help come up with stories (for example, navigating diet around the holidays or back to school time and being an IBD teacher). Support the content of fellow advocates—comment and share articles that intrigue you and help others get their words out and the same will be done for you. Rather than seeing advocacy as a competition, view others as your ally—we’re all doing this to help others, spread awareness, drive research, and together we can truly amplify the patient voice—one article at a time.
There’s no telling what Lights, Camera, Crohn’s will look like seven years from now, but I don’t plan to stop storytelling anytime soon. Thanks for all your kind words, for telling me when my stories have touched your life or helped you make a tough decision, and for being there for me when I need support. If you’d ever like to collaborate with me to share your story or if you have a topic you’d like me to write about—please don’t hesitate to reach out.
Here’s to another seven years of breaking stigmas, spreading awareness, and making everyone in the IBD community feel seen.
When you hear the word “Skyrizi,” you may think people are referring to an up-and-coming rapper or something fun, but in case you didn’t know, Skyrizi (risankizumab-rzaa) is a biologic drug that was approved to treat Crohn’s disease in June 2022. With the medication only being around for IBD less than 13 months, finding patient experiences wasn’t as “easy” as previous articles I have covered on Lights, Camera, Crohn’s about biologics, but I learned a lot writing this and I think you will gain a better understanding of Skyrizi after reading this, too.
Some background on Skyrizi
Skyrizi was previously approved for moderate to severe plaque psoriasis and active psoriatic arthritis. It’s worth noting that Skyrizi is the first treatment for Crohn’s that targets the interleukin-23 (IL-23) protein, which is responsible for inflammation in our bodies. By going after IL-23, Skyrizi helps reduce inflammation that can contribute to Crohn’s symptoms.
When it comes to dosing, patients receive an intravenous (IV) infusion that lasts about an hour at week 0, week 4, and week 8, followed by a self-administered subcutaneous injection with an on-body injector (OBI) at week 12 and every 8 weeks after that. This whole OBI situation is incredibly intriguing to me. I’ve been doing Humira injections for 15 years (!) this week, so I’m used to self-injecting, but knowing technology like the OBI exists gives hope to people who are fearful of needles and having to give themselves a shot. We’ll get into more about the OBI and what fellow patients have to say later in the article.
As far as safety, prior to starting Skyrizi, it’s advised that your GI order lab work that looks at your liver function. If results come back abnormal, this may not be the right drug for you. If you are in the family planning stages, pregnant, or breastfeeding, speak to your doctor. You can also enroll in the ongoing PIANO study, which looks at the safety and efficacy of IBD medications during pregnancy and beyond. Since Skyrizi is so new to the game, research is needed to help pave the way for IBD moms and their children.
Let’s hear from the patient perspective
Prior to starting Skyrizi in February (2023), Stelara failed Stéphane. I’m always careful with how I word this—and I wish all patients and healthcare providers would be conscious of not saying “the patient failed” anything—at the end of the day, it’s the drug that fails us. Stéphane says he didn’t start feeling a response until this month (July)—just before his second OBI (on-body injection). Although his calprotectin started to respond positively in May.
“The good is that I’ve responded and feel better. The bad is that we don’t know how long my response will last or how much it’ll stop inflammation and the formation of strictures. I’ve responded to Remicade, Entyvio, Stelara, but I’ve also developed strictures and had surgeries on all of them. I can hope that Skyrizi won’t continue this dire and disappointing record.”
Megan says before she started Skyrizi she was on the path to an ostomy. Entyvio had failed her, and she was experiencing perianal Crohn’s symptoms that were keeping her from being the mom, wife, and employee she wanted to be.
“My medical team and I decided to start Skyrizi and plan for a temporary ostomy to help my symptoms while we waited for the medication to take effect. After my second Skyrizi infusion, I noticed significant improvement in my symptoms! My bowel movements were more regular, there was a decrease in drainage from my setons, and I had less pain overall. Given my positive response to the medication, we were able to table ostomy surgery. I was extremely relieved and grateful that I had such a quick response to Skyrizi.”
Maha went on Skyrizi after the biologic she was on failed her after six years. As she was reeling from the reality that the biologic that had put her into clinical remission could suddenly not work anymore, she was hesitant and nervous about how to decide the next treatment options.
“After reviewing all of my options with my doctor, I chose Skyrizi based on data and evidence, and also on a gut feeling that this might be the right next step. I’m happy to report that I was right, and in the time that I’ve been on Skyrizi, I’ve achieved a state of remission I could only dream of, with no side effects!”
Elizabeth was in the clinical trial for Skyrizi. She says the biologic “changed her life.” After fighting a Crohn’s flare for seven years, it’s been the only medication that’s wrangled her disease under control.
Kelly started to flare last Fall, because of a loss of response to Remicade (infliximab). Her gastroenterologist suggested Skyrizi as an option that aligned with her drug priorities: namely safety and efficacy.
“The drug has very good data behind it, and she had heard of excellent response in the clinical trials. But it was very new to GIs across the US. It was a gamble, but one that we both thought was worth trying.”
Unfortunately, Kelly dealt with significant problems and delays with her prior authorization and needed to use the AbbVie Bridge Program to get her first infusion dose covered.
“My insurance company used my participation in the Bridge Program as a reason to deny my coverage for the drug. But AbbVie anticipated this issue and has several support programs that cover longer use of the drug and help with deductibles until insurance companies change their policies about drug coverage. I strongly believe that the months of stress and anxiety and daily hours-long phone calls to try to get this drug covered and delivered seriously exacerbated my flare symptoms,” said Kelly.
This cat and mouse game is something far too many of us can relate to. It’s sickening and ridiculous what chronic illness patients have to go through month after month, just to receive medication on time. Kelly was constantly anxious and worried about whether her Skyrizi would be covered.
Kelly tells me her first two infusions were easy and that she had almost zero side effects aside from very mild fatigue, like her normal Crohn’s baseline.
Kelly’s final Skyrizi induction infusion
“My third infusion was a little heavier hitting, like how Remicade infusions felt: a pronounced bit of fatigue, headache and brain fog that lasted less than a day. It was very tolerable. I didn’t have to premedicate before the infusions either, although my doctor had started me on budesonide to try to control the inflammation and keep the flare from getting worse while we waited for the Skyrizi to kick in.”
Cassandra says this is her third biologic and the whole experience in and of itself has been a bit nerve wracking. She lives in Canada and was the first to receive Skyrizi in her city.
“I didn’t love being the first, having the nurses learn on me, not knowing what to expect was difficult as I typically try finding online forums where others share their experiences. So far, I feel ok with it. Skyrizi hasn’t gotten me into remission, but we will see how it goes!”
The OBI (On-Body Injector)
Like anything new, getting used to a new medication and the mode of delivery can have a bit of an adjustment period. You wear the device on your thigh or abdomen for 5 minutes while the medication gets into your skin.
Kelly – “The neat thing about Skyrizi is the Obi, or on-body injector. It’s a brand-new device that is halfway between an infusion and an injection. It’s a small rectangular device with adhesive on the whole back that sticks to your leg. The needle in the device is tiny and I had zero sensation or pain. The button to trigger the needle is large and doesn’t have the same kind of chunky CLICK that the Humira pens do, which was nice and felt less aggressive and intimidating. Because the device infuses the medication into your body over several minutes, it uses an electronic pump. This means you cannot wear your fitness device or Apple watch or have your phone anywhere near it while you’re doing the injection.”
Kelly says she expected to have difficulty with the adhesive since it covered such a large area of skin and was strong. Other than mild discomfort while peeling it off (like taking off a band-aid), her skin didn’t have any other reaction.
Stéphane-“The written instructions for Skyrizi make the self-administering with the on-body injection unnecessarily complicated. I counted 33 warnings of what not to do, something that just generates anxiety. In fact, it’s simple and easy and the Skyrizi video they provide on the website is far more confidence-inspiring and useful.”
Stéphane says it’s helpful to watch the video after reading the instructions. He says the video is good at stripping the process down to essentials and showing that the injection process is in fact easy.
“The front of the thigh is simpler than the stomach because it naturally offers the flat, smooth, easily accessible space you need to place the injector. You clean the small end of the vial, stick it into the injector so it clicks, close injector door, clean area of skin, take the two strips off the back (top first), place it on your thigh and press down the adhesive, then press forcefully on button of injector,” he said.
Jessica made the switch to Skyrizi after being on Stelara. So far, she hasn’t experienced side effects and the medication has kept her Crohn’s in remission.
“The new on-body injector technology is weird and takes some getting used, but overall, it’s painless. It’s just been a little complicated to learn. If there’s a lump on your skin after you take the injector off. She says it goes away. While the needle doesn’t hurt, Jessica feels as the medicine goes into your system you start to feel more pressure.”
So far, Megan has completed two OBIs at home. She says the OBI is extremely easy to use. She’s done Humira, Stelara, Cimzia, and methotrexate in the past and says the OBI for Skyrizi is the easiest and least painful.
“I like to head to a secluded area, so I don’t chance my son trying to wrestle or play and accidentally knock it out of place. (IBD mom hack!) While I still have hard days and I’m not symptom-free, my hard days are much less frequent than before starting Skyrizi!”
Cassandra-“The OBI is amazing. I have been getting IVs monthly/every other month for 9 years, so to not have to get an IV has been wonderful. I have grown to really hate them and have had some bad experiences getting IVs so to not have to face that has made a world of difference. The OBI is so simple, so quick, and relatively painless (though I have felt some slight pinching/stinging). All in all, it’s very simple and I find the mechanism very innovative and cool! I haven’t had any side effects yet, aside from injection site swelling and redness the day of.”
Maha-“The best part is the ease with which I can do my Skyrizi injections via the on-body injector: it’s painless, quick, and honestly I forget that I have to do them until my next injection rolls around.”
Benefits of utilizing the Nurse Ambassador Program Much like other biologics on the market, patients can tap into the free Nurse Ambassadors on hand to help ease the transition to Skyrizi. These nurses provide invaluable guidance and comfort every step of the way. Not only is utilizing these programs beneficial for patients, but also caregivers who may be helping to administer medication.
Kelly-“The device is so new, and the instructions can be long and a little complicated, but AbbVie has a nurse ambassador program that is free for all patients. I cannot recommend the program enough. My nurse ambassador came to my house before I even received the first infusion dose and answered all my hundreds of questions about the expected side effects, the rate of response, and showed me a demonstration with the OBI. It was helpful to get comfortable with the training device. My nurse ambassador also showed up to my house for my first injection and walked me through each step and was excellent at providing support.”
Natalie started Skyrizi infusions in May, 2 infusions down, 1 more to go before she starts with the OBI. She says while she hasn’t experienced huge benefits yet, she’s still hopeful. This is her first biologic and she’s appreciative of how helpful the AbbVie nurse has been through the process.
“I am still pretty new to this myself, but talking with the Skyrizi nurse has helped a great deal, especially getting their co-pay program and just having someone to check in on you.”
Jessica– “AbbVie has an amazing support system, and you can always have a nurse ambassador visit you in person or Facetime you. When I FaceTime the nurse, she guides me through it. Just talking to her while the injector is on for five minutes has made a difference.”
Cassandra-“I live in Canada, so things may be different elsewhere, but Skyrizi is the first biologic where I was sent a “Welcome package” which had a little health/wellness goal setter, appointment tracking sheets, a large needle disposable cartridge for my used injectors, and a mini cooler with reusable ice packs. I was super impressed, and it was fun and cute to receive. I have used the nurse ambassador a few times, especially at the beginning. It’s nice to ask questions or voice concerns with them. Having a nurse ambassador gives me peace of mind.”
Maha-“I really appreciate AbbVie’s commitment to patient education and support through their Skyrizi Hub which provides insurance specialists, nurse ambassadors, and an on-call line to help with any medical or financial concerns! My nurse ambassador walked me through my first injection and has followed up with me regularly to check on my progress both in terms of clinical symptoms and also quality of life!”
Struggling with the “newness” of being a biologic the first year it’s approved for IBD
Kelly ended up flaring badly between her third induction infusions and the fourth dose (her first at home injection). She met with her GI several times, discussing what to do. Since Skyrizi is such a new IBD drug, there really isn’t any extensive anecdotal evidence or patient stories about whether it be worth it to continue the drug, or if she would be considered a “primary non-responder.”
“We struggled with what criteria to use to determine if I just needed to wait longer or if I needed to switch drugs. My GI reached out to the Skyrizi sales rep for their practice and was told not to give up on the drug before 24-26 weeks because clinical trials did show that a non-trivial number of outliers did capture response to the drug later than the expected 8-12 weeks that was seen with most primary responders. At 14 weeks, I could tell that I wasn’t seeing any response to the drug because I was tracking my symptoms, daily bowel movements and pain. It was helpful to have that data to show us in black and white that I wasn’t doing well.”
Looking at the reality of the data and watching her symptoms escalate and her inflammation creep higher and higher despite the steroids and Skyrizi, Kelly and her care team made the decision to discontinue Skyrizi and move to another drug.
“It’s hard to hear from so many medical professionals that a drug with only about a 40% response rate is considered a raving success in the GI community. For me, that’s an enormous number of people who did not respond to this drug. I wish very much I had been one of them, because it’s scary and upsetting when you burn through a drug and cannot go back to it in the future because of possible antibody development.” says Kelly.
Ultimately, the decision to try a medication is a highly personal decision, one that should be made well-informed and jointly with your GI healthcare provider.
Maha says, “My experience with Skyrizi has affirmed that there is hope in all the new therapeutic modalities that are coming out, and that they can offer patients a strong quality of life while delivering treatment as minimally invasive as possible.”
Interested in reading previous Light’s Camera Crohn’s Patient Experience articles about other biologics?
I remember the first phone call when I was pregnant with my oldest as a soon-to-be IBD mom. A researcher from Mother to Baby called me when I was newly pregnant and leaving work—I sat in my car in a parking lot, as she asked me several questions about my health, well-being, medication, and pregnancy thus far. That was Fall of 2016. Fast forward to now—and my oldest, Reid, just graduated from kindergarten. When I was diagnosed with Crohn’s disease at age 21 in 2005, one of my biggest fears was whether my chronic illness was going to rob me of motherhood. Back then, I was nowhere near ready to settle down, but the worry was always in the back of my mind.
When my husband and I got married in June 2016 and I was 10 months into surgical remission, we knew we needed to capitalize on my IBD finally being under control. Luckily, we got pregnant one month after getting married. Shortly thereafter, I started researching pregnancy studies for IBD moms. Lights, Camera, Crohn’s launched two days before I received a positive pregnancy test. I was fresh into my advocacy and had never been pregnant before. I didn’t have a community of IBD moms to lean on for questions or support as I navigated the unknown.
I came across information about Mother to Baby online and ended up being a part of their pregnancy studies for my first two children. The studies were different, but I had such a positive experience with Reid, that I decided to participate again with my daughter, Sophia. Reid’s study was a 5-year look at how Humira impacts babies in utero through kindergarten. When I was initially pregnant with him, this felt light years away. And here we are. Over the course of his pregnancy and until November 2022, I completed surveys, did phone interviews, had an in-person meeting with a doctor who came to my home and looked him over in front of me for any health anomalies, and most recently did an in-person cognitive neurobehavioral assessment at a nearby hotel with researchers.
We just got the results. While it’s rewarding to participate in IBD studies and interesting to learn, there’s always a part of you that worries about the findings and if mom guilt will ensue. It’s been reassuring and comforting to see my healthy kids, who were exposed to Humira in utero through the 3rd trimester, thrive and excel with milestones and in school.
The findings of the study
In November 2022, Reid and I met up at a nearby hotel with two researchers who provided neurodevelopmental behavioral evaluations for both of us. Reid’s assessment used a series of questions, games, and puzzles to help researchers determine his development of language ability, memory skills, and problem-solving abilities. The tests were selected to provide an evaluation of general mental ability and to describe specific abilities in areas of verbal knowledge and reasoning and visual-perceptual reasoning and organization. The tests were intense, I was proud of him for how he handled himself during the process.
Reid and I waiting to do our assessmentwith research administrators
According to Mother To Baby, “this battery of tests is best suited to examine the similarities and differences among groups of children. While it was not adapted for Reid’s individual characteristics, it can highlight general strengths and weaknesses in a child’s cognitive profile and indicate potential concerns when present.”
Behavioral Observations: “Reid was personable and interacted with both administrators on his arrival. He had a very positive attitude toward testing and quickly became comfortable with administration. He was engaged and attentive to the materials, listened attentively to the examiner and provided effortful responses even as questions became more difficult. Reid demonstrated good cooperation and attitude by following instructions and requiring minimal to no redirection from the administrators of his mother. He was focused and friendly for the full duration of testing.”
Summary of Assessment Results: “Tests were administered in a single testing session with one short break. The Wechsler Preschool and Primary Scale of Intelligence (WPPSI-IV) was selected to provide an evaluation of Reid’s general mental ability and to describe specific abilities in areas of verbal knowledge and reasoning and visual-perceptual reasoning and organization. This battery of tests is best suited to examine the similarities and differences in ability among similarly aged groups of children. While it was not adapted for Reid’s individual characteristics, it can highlight general strengths and weaknesses as well as potential concerns when present.”
The intelligence test was comprised of 10 subtests which measured a variety of verbal and nonverbal skills. Reid achieved a composite score in the average range. In the working memory category and spatial working memory, Reid performed in the high average range, which required him to remember and identify pictures that had previously been shown to him. On tasks that measured visual-spatial abilities, Reid scored below average. These tasks required him to synthesize visual stimuli to recreate block design.
“Reid was highly focused while processing visual stimuli. Overall, Reid is a bright and enthusiastic child. He was a pleasure to work with.”
Along with Reid’s assessment, I was also interviewed and performed tasks with an examiner on the other side of the room. I was assessed in the adjustment and life context. Tests included the Center for Epidemiological Studies Depression Scale and Parent Stress Index. My scores were within normal limits and my general mental ability also scored in the average range. Not gonna lie, the testing was challenging!
Reflecting on my experience
As an IBD mom of a 6-year-old, 4-year-old, and 22-month-old, who participated in pregnancy research during each of my pregnancies, I can’t begin to tell you how incredibly rewarding it is to know that your personal experience is helping to drive the future of care for women in our community who have hopes of one day being a mother. Sure, it takes a little bit of time and effort, but the data and research to show the safety and efficacy of medications while pregnant and breastfeeding is so needed. It’s comforting to know Reid is right where he needs to be cognitively and healthy physically, despite my high-risk pregnancy and exposure to Humira until 39 weeks gestation. We need more women to willingly step up to the plate and share their journeys to help guide the future of IBD motherhood and show all that’s possible despite our disease.
Opportunities to participate in research
Many people need to take medication during pregnancy to manage and treat their IBD. Yet, according to the Mother To Baby website, fewer than 10% of medications have enough information to determine their safety for use in pregnancy.
Do you have Crohn’s disease? Are you currently pregnant? If you answered “yes” to both questions, you may be able to help Mother To Baby advance the knowledge of how managing IBD in pregnancy impacts a developing baby. Click here to learn about how you can impact the health of future families by joining the Crohn’s Disease and Pregnancy Study.
July marks 15 years since I started my journey taking a biologic injection to manage and treat my Crohn’s disease. Since that time, I’ve had routine “safety labs” every 3-6 months, depending on my gastroenterologist. You may be familiar with safety labs, or you may wonder what I’m talking about. I’ve been seeing my current GI for almost 8 years, and she’s adamant that I get labs every 3 months to make sure my disease is closely monitored. If I fail to get labs every 3 months, per her orders, my prescription for Humira is unable to be filled by my specialty pharmacy.
I ran a poll on Instagram and asked, “If you are on a biologic, do you get safety labs every 3 months?” Of the 175 people who responded, 41% said “yes”, 36% said “no”, and 23% had no idea what safety labs are. This week on Lights, Camera, Crohn’s we take a closer look at the reasoning and purpose behind safety labs, and we hear from esteemed and world-renowned gastroenterologists Dr. David Rubin, MD, Section Chief of Gastroenterology, Hepatology, and Nutrition at the University of Chicago Medicine and Dr. Miguel Regueiro, MD, Chair, Digestive Disease and Surgery Institute, Professor in the Department of Medicine, Cleveland Clinic.
What is a safety lab?
Safety labs are to ensure that patients are not developing a complication from a medication that they may not feel.
“For example, kidney or liver function tests that may show an abnormality before a patient has damage to those organs, or problems. Or a white blood count that lowers in a patient on certain immunosuppressive therapy – something they may not “feel” until the immune system gets low enough to develop an infection,” explained Dr. Regueiro.
The periodicity of labs for “safety” are often taken from the clinical trial designs, rather than the likelihood that something is going to change within that period of time.
“Routine labs while on therapies for IBD is important and patients can and should keep track and ask for them at least twice a year for most of our therapies. For many of these, there are gaps in our understanding whether the interval (every 3 months for example) is the right one or makes a difference. We certainly know it takes time for patients to do this and costs money too. Some of my colleagues withhold refills as a safeguard to make sure patients get their labs. This may be more punitive than necessary, but it is one way to make sure this is getting done,” said Dr. Rubin.
When I get my labs done every 3 months the following blood tests are ordered by my GI:
CBC w/Auto Differential
Hepatic Function Panel (Liver Panel)
Vitamin D 25 Hydroxy (I am deficient, so we keep a close eye on this)
If there is concern about inflammation or anemia, then my GI also adds:
Sedimentation Rate, automated
High Sensitivity CRP
Iron Profile with IBC + Ferritin
In the past, if there’s concern about my response to Humira we do a “trough level” to see if I’ve built up antibodies to my therapy and to measure how much medication remains in my body right before I am scheduled to do another injection.
It’s important to know, since I started seeing my GI two months after my bowel resection surgery in 2015, I have been in remission. So, the concern about inflammation and needing to take fecal calprotectin tests has been few and far between. When we were in the middle of the pandemic, rather than an annual colonoscopy, my doctor had me do a fecal calprotectin test at home to limit my risk of being exposed to germs in a hospital setting while my disease was well-managed.
“We recommend certain labs on patients taking IBD medications. Each medication will require a different safety lab monitoring strategy. Some brief examples, for mesalamine, checking kidney function tests within a couple of months of starting a medication and then once or twice a year. For thiopurines (6MP and Imuran) and methotrexate more frequent blood work initially, e.g., complete blood count and liver function tests weekly to every other week in the first two months after starting and then every few months thereafter,” said Dr. Regueiro.
Safety labs as a disease monitoring strategy
Generally, safety labs are done for medical health reasons to make sure that everything is ok while taking the medication.
“Safety labs are “driven” by the physician or provider caring for the patient. The insurance company may require certain labs before starting or continuing a medication. For example, a tuberculosis (blood) test before starting an anti-TNF medication and then yearly while a patient is on the medication. Otherwise, the insurance company usually does not require safety labs for medication approval or continuation. Each case is different, and each insurance company is different,” said Dr. Regueiro.
“More important than pharma-drive lab recommendations—is that every patient should have a customized strategy to monitor their disease stability to detect relapses before there are clinical consequences. This is my new take home message for most of my lectures- in addition to “treating to a target” we must have “disease monitoring” as something that every patient has as part of their care,” said Dr. Rubin.
Chronic diseases like IBD tend to “drift away from control”, so it is good to keep an eye on things and this enables proactive preventive care.
Getting my safety labs in the thick of the pandemic
“For low-risk patients, that might be once a year, but for those who are on advanced therapies (biologics and the novel targeted small molecules), they likely need this approach more frequently. It is true that “knowledge is power,” and knowing that the disease has activated enables much better care,” explained Dr Rubin.
Disease monitoring may involve blood or stool markers (calprotectin) or depending on where you live, intestinal ultrasound. Colonoscopy or CT scan/MRI is also recommended. Dr. Rubin tells me the key is identifying what is appropriately benchmarked and reliable and which approach is feasible and makes the most sense for the patient.
Why the onus is often on us
As you can imagine, 3 months comes quickly. If you’re like me, I see my GI in clinic two times a year (every 6 months). When I was pregnant, she would see me in the office every 3 months. Given that I see her twice a year, that checks off two of my four lab visits. As an IBD mom juggling life with three young kids, time can often slip away. I’ve found I must alert my nurse and GI about when and where they need to submit lab orders so I can take care of them the other two times a year at a Quest or LabCorp nearby. In the past there have been a few times where I’ve dropped the ball.
Coordinating life with chronic illness can truly feel like a full-time job. Just this week I spent an hour on the phone with my specialty pharmacy trying to organize my next shipment because there was an issue with my patient savings card. At the time, all three of my kids were running around like little banshees, yelling, and making it hard for me to hear the phone representatives. At one point, I had to lock myself in my laundry room. These aren’t calls that can wait. Patients need their medication; we can’t just hang up and re-visit the snafu at another time because it can mean we receive our biologic shipment late. This is one small example—of a behind-the-scenes look at life with IBD as a mom.
While getting labs four times a year may not seem like a lot, it does involve planning, time, and coordination for patients. My kids have joined me countless times in the stroller as I get labs done. Then, reading the results on the Patient Portal and seeing certain results too low or too high can cause anxiety and added stress. It’s a never-ending cycle.
Talking with your care team
If you’re only getting labs done once or twice a year, it may be worth having a conversation with your GI about the reasoning why and what you feel most comfortable with. Your care is not a one-way street. If you feel like you need a more hands-on approach, talk about this with your doctor. In talking with fellow IBD patients, many who are on infusions every 8 weeks, tell me they get labs every 16 weeks.
If you’re only getting labs done once a year, Dr. Regueiro says you don’t necessarily need to be alarmed.
“For a patient who has been on a medication like mesalamine or a TNF inhibitor for a long time, in remission, and doing well without prior lab test abnormality, once per year lab testing may be ok. However, a patient on Imuran or 6MP may need lab testing more frequently.”
As a veteran patient, who was diagnosed with Crohn’s nearly 18 years ago, safety labs have become part of how I manage my IBD. While annoying at times, these labs also give me a sense of relief. One final recommendation I have—don’t try and get labs done before or after your colonoscopy—I’ve tried this twice to try and kill two birds with one stone, and with being so dehydrated, it was not a pleasant experience. Being closely monitored through safety labs takes away much of the stress and worry that can come because of being on a biologic, and the possible side effects that can happen now and into the future.
A special thank you to Dr. David Rubin and Dr. Miguel Regueiro who took the time to offer their expertise for this article on the heels of Digestive Disease Week (a HUGE conference they both actively participate and present at). Having their insight on topics like this that matter to patients means so much.
One in three people with inflammatory bowel disease (IBD) has iron deficient anemia. This common, but often underrecognized and undertreated extra-intestinal manifestation impacts so many of us. You may wonder why. The reason is three-fold.
First being that long-term irritation and inflammation in our intestines can interfere with our body’s ability to use and absorb vitamins and minerals properly. When our intestines don’t absorb enough iron, folate, B12 and other nutrients, our bodies are unable to create more red blood cells. Those with IBD are also at risk for blood loss—both visible and microscopic and we often don’t eat as much iron-rich foods. So, what can we do to boost our reserves and increase our energy? How as patients can we better advocate for ourselves to stay on top of screenings? This week on Lights, Camera, Crohn’s an in-depth look at anemia in both adult and pediatric patients and input from Dr. Alka Goyal, who recently co-authored a major study on pediatric anemia.
Symptoms to watch out for
As someone who was diagnosed with Crohn’s disease in July 2005, I experienced anemia long before my diagnosis. I often wonder if my anemia was a warning sign of the larger issue, my IBD. In fourth grade, I fainted on the teacher’s desk while waiting for her to look at an assignment. Throughout my life I’ve experienced light-headedness, weakness, black outs, and extreme fatigue. My symptoms were never addressed prior to finding out I had Crohn’s. A simple lab test would have shown all along. When I was diagnosed with IBD and hospitalized my hemoglobin was a 7. To give you an idea, people are given blood transfusions once they drop to 7 (or below). Throughout my 18 years with IBD, my hemoglobin was rarely ever in “double digits”—and I took over the counter iron supplements for years.
Once I had my bowel resection surgery in 2015, my iron panel slowly started to improve. It takes time. Last month, I had my “highest” hemoglobin since diagnosis, ever—12.9 (which really isn’t that high, but I’ll take it!). It’s difficult to put the fatigue caused by anemia into words, but you can physically tell such a difference when your iron panel is where it needs to be.
When you have anemia, you have less blood carrying oxygen throughout your body. The most common symptom is feeling tired or lethargic. Other symptoms include dizziness, headaches, feeling cold, pale skin, being irritable, and shortness of breath. Not everyone experiences symptoms, so it’s important as a patient to speak with your GI about making sure that when you get labs, an iron panel is part of the workup.
Screening for Anemia
Anemia screening is driven by patient symptoms and/or a care provider’s recognition of lab abnormalities. It’s important to note that anemia is not *just* a low hemoglobin, all the lab figures matter. With iron deficiency anemia (IDA), red blood cells are smaller and paler in color. Your hematocrit, hemoglobin, and ferritin go hand in hand. Ferritin helps store iron in your body. Iron deficiency anemia is the most common type of anemia and is caused by a lack of iron-rich foods, malabsorption, and blood loss.
Other types of anemia include vitamin deficiency anemia and anemia of chronic disease. Vitamin deficiency anemia is a result of poor absorption of folic acid and vitamin B12. My GI has me on daily folic acid. Luckily my B12 has never been an issue, but it’s worth a discussion with your care team. If you’re deficient, you can receive B12 injections. Diseases such as IBD and other inflammatory diseases can interfere with the production of red blood cells. When this happens anemia can often only be resolved once remission is reached or inflammation calms down.
In order to address the need for improved patient management, the Crohn’s and Colitis Foundation created the Anemia Care Pathway (ACP) to standardize clinical management of anemia in IBD. This pathway helps to identify high-risk patients so that timely intervention and care can be provided. The hope is that this pathway will improve patient outcomes and our quality of life. Patients are assessed based on the severity of their anemia and iron stores to determine the type of iron therapy (intra-venous or oral) that is best suited.
The importance of accurately diagnosing the type of anemia you have
According to the PubMed study, Management of Anemia in Patient with Inflammatory Bowel Disease, despite iron deficiency anemia impacting one third of IBD patients, “more than a third of anemic ulcerative colitis patients are not tested for IDA, and a quarter are not treated with iron replacement therapy.” While oral iron tablets are effective for treating mild IDA, it’s not for everybody. The study also notes, “it is important to recognize that ferritin is elevated in chronic inflammatory states and among patients with active IBD, ferritin levels less than 100 are considered to be diagnostic of iron deficiency.” Iron infusions have a solid safety profile and can be used to help boost your iron stores and prevent future iron deficiency.
While treatment goals are well-defined, selecting a treatment is often not as straightforward. The PubMed study previously mentioned recommends that all IBD patients with IDA should be considered for oral supplement therapy, whereas someone with clinically active IBD, or someone who is not tolerant of oral iron, with hemoglobin levels below 10 g/dl be given IV infusions therapy. While oral iron is safe and affordable, some people experience GI issues from oral iron, it can also increase inflammation and contribute to flares in patients who are not in remission.
“Though intravenous (IV) iron is substantially underused, it’s considered first-line treatment for patients with active disease, severe anemia, oral iron intolerance, and erythropoietin (a hormone secreted by the kidneys that increases the rate of production of red blood cells in response to falling levels of oxygen in the tissues.)
Anemia in pediatric IBD patients
The most common cause of anemia in children with IBD is iron deficiency. It results from chronic blood loss, poor absorption, and less intake of foods that are rich in iron due to poor appetite, food selection or intolerance. According to the World Health Organization’s definition of anemia, prevalence in the pediatric IBD population ranges from 44% to 74% at diagnosis and 25% to 58% at 1 year follow-up.
Anemia can be both a biomarker of disease activity and a subtle or debilitating extraintestinal manifestation. According to, Anemia in Children With Inflammatory Bowel Disease: A Positi… : Journal of Pediatric Gastroenterology and Nutrition (lww.com), “newly diagnosed children with IBD are more likely to have IDA in contrast to anemia of chronic disease. No significant improvement in the hemoglobin was observed when patients were assessed after 13 weeks of induction therapy with conventional drugs that included nutritional therapy, azathioprine, steroids, and 5-ASAs. Despite the recognition of anemia, fewer than half of anemic patients received indicated iron therapy.”
Dr. Alka Goyal, MD, Clinical Professor of Pediatrics, and Interim Associate Chief of Clinical Affairs at Stanford University of Medicine, co-authored this study on pediatrics and tells me the key message is that anemia is the most common extraintestinal manifestation in patients with IBD.
“More than 2/3rd of children with IBD are anemic at the time of diagnosis. The treatment of IBD alone does not resolve anemia, which can be associated with a variety of symptoms. Persistent anemia indicates a more aggressive disease course,” said Dr. Goyal.
Hemoglobin levels across genders and race
According to the study, hemoglobin levels are similar in preteen boys and girls; however, after menstruation, the cutoff hemoglobin in girls is lower than in boys and is even lower in pregnant versus nonpregnant women. The African American population tends to have lower hemoglobin concentration compared with Caucasians.
“Although the normal range of hemoglobin varies with age, gender, and race, a hemoglobin level below 10 g/dL is considered to be consistent with moderate anemia and below 8 g/dL as severe anemia, whereas in young children below the age of 5 years and pregnant women, a hemoglobin level below 7 g/dL is deemed as severe anemia.”
Dr. Goyal says it’s important to monitor anemia regularly in all patients with IBD.
“Anemia can be an early indicator of active disease or an impending flare of IBD. When the body has inflammation, the iron stored in the body cannot be metabolized to help manufacture more hemoglobin and additionally there is suppression of normal blood production, resulting in anemia of chronic disease.”
Other causes include vitamin deficiency, medication side effects, or breakdown of red blood cells due to other inherited or disease-related complications.
“Patients should be monitored not just by symptoms, but also by blood tests like complete blood count, Ferritin, and markers of inflammation like CRP every 3 months when they have active inflammation and every 6 months when patients are in remission,” Dr. Goyal explains.
Bringing a dietitian on board to help
Registered dieticians who specialize in IBD can advise patients and families about foods that contain iron naturally. The iron in meats is more readily absorbed than that present in a plant-based diet.
Dr. Goyal says another important concept is food pairing.
“With food pairing, iron-rich foods like spinach, kale, and Swiss chard are ingested with citrus fruits, melons, or vegetables like bell pepper, broccoli, beans, carrots, tomato, etc. Avoid simultaneous ingestion of foods rich in dietary fiber, soy, cereals, coffee, tea, and animal protein like milk, and eggs. Children should consume at least three servings of iron-rich foods like fortified cereals, red meat, tofu, etc. The recommended daily intake of iron in healthy children is 7-11 mg daily,” says Dr. Goyal.
Treating anemia in the younger IBD population
When it comes to treating anemia, Dr. Goyal has helpful tips. She says it’s important to recognize and treat anemia along with the treatment of IBD and vice versa.
Oral iron can be tried in mild anemia when the hemoglobin is above 10 gm/dl, preferably given with juice or citrus fruits.
Avoid taking oral iron multiple times a day or in high doses.
Brush your child’s teeth after taking liquid iron.
If your child experiences side effects including abdominal pain, nausea, or constipation, and/or has no significant improvement with oral iron, it is safe to give intravenous iron.
Timely treatment may save a blood transfusion. excessive unabsorbed iron is not healthy for our digestive system, so avoid overdosing on oral iron.
Patients with persistent anemia lasting for three or more years were noted to have a higher prevalence of more severe and complicated disease (stricturing and penetrating phenotype) with a greater need for surgical intervention.
Whether you’re an adult patient or a caregiver to a child or young adult with IBD, be mindful of the importance of keeping tabs on whether anemia is creeping in and hindering you or someone you loves quality of life. Have the conversation with your GI and make sure you are being vigilant and proactive about doing all you can to prevent, manage, and treat anemia.