Traveling with inflammatory bowel disease (IBD) is rarely as simple as packing a suitcase and showing up. It’s logistics, emotions, planning, and flexibility. It takes a bit of hypervigilance. This layered on top of a disease that doesn’t take vacation days. But it is possible. And for many of us, it becomes one of the most empowering reminders that life with IBD can still be adventurous, and rich with new experiences.
This week on Lights, Camera, Crohn’s you’ll hear from two incredible IBD advocates, Kelly Dwyer and Rachel Verbanac. They both open up about their diagnoses, their anxieties, their coping strategies, and their go-to travel essentials. Their honesty and wisdom offer a roadmap for anyone who wants to explore the world without letting IBD call all the shots.
Meet Kelly: 21 Years of Symptoms, 7 Years Diagnosed
Kelly may have been diagnosed with Crohn’s disease in 2018, but she’d been living with severe perianal fistulizing ileal Crohn’s since the early 2000s.
“Before diagnosis, I avoided significant travel whenever possible because I was so ill. And when I did travel, I tried so hard to plan for every single scenario that it became stressful for me and everyone around me.”
Now in deep remission thanks to medication, Kelly still plans intentionally, but the difference is that the planning empowers her instead of holding her back.
She structures trips around:
Her injection schedule
The time of day she flies or drives
What foods she eats before travel
How to pace her energy
And what she needs to stay healthy while surrounded by crowds
“I wear a mask, use sanitizer constantly, wash my hands as much as I can… it all helps me feel like I’m doing what I can to set myself up for success.”
Kelly on Travel Anxiety: The Trauma Stays with You
Despite years of remission, Kelly still carries fear rooted in lived experience.
“I constantly worry about not making it to a bathroom. Even though it has not happened in years, that trauma stays with you.”
Kelly also experiences nausea, anxiety and a whole lot of gas and burbling guts when she travels.
“Finding the right medication cocktail that keeps things calm and in order in my guts (and brain!) took a lot of trial and error, but was worth it for me to find a combination to give me confidence that I’ll feel like I’ve done everything I can to get the trip off on the right foot. I would recommend you ask your doctor or GI about Zofran, anti-anxiety medications in small doses, Gas-x, antacids, and other OTC medications that might help you to make sure they’re safe for you to take.”
She’s built a system that helps her feel confident when she’s traveling:
Depends or heavy-duty panty liners on days she’s unsure
Change of clothes and wipes in her purse, not her carry-on
Imodium and emergency meds ready to go
Small meals before and during travel days
Medication for nausea, anxiety, gas, and gut discomfort
“I had to learn to relax into the chaos of travel and not panic when plans change. Travel is unpredictable—but so is Crohn’s.”
The Power of Protection: Insurance (Both Emotional and Literal)
Kelly is adamant that travel insurance is non-negotiable.
“I have used travel insurance many times for flare-related cancellations. It can be heartbreaking to miss something important, but it’s not your fault. This is your reality, and you’re doing your best.”
She also communicates openly with travel companions, so expectations are clear and compassionate from the start.
“Find as much peace as possible. Asking for everyone’s understanding and compassion, is so important. I remind myself that it’s not my fault that I am unwell. It’s not anything I did to cause the flare. This is simply my reality, and I am trying my very best, even if it doesn’t always work out the way I’d hoped.”
“Treat yourself with compassion, always. Build in extra time everywhere. Your comfort is worth it. Having a few extra hours at the airport to sit and read a magazine is much preferable to rushing through security lines and not being able to use the bathroom before getting on the plane because you’re late.”
Meet Rachel: A Travel-Lover Who Refused to Stop Exploring
Rachel was diagnosed with Crohn’s disease in 2021, right as she was going back to nursing school. Before that, she spent months living a nomadic lifestyle in New Zealand and expected to spend her twenties exploring the world. Her diagnosis meant rethinking what travel could look like. Requiring infusions changed everything.
“Hiking the Appalachian Trail used to be a dream, but with the need for insurance, pharmacy authorizations, infusion clinics, and access to university health systems… that lifestyle just wasn’t realistic anymore.”
But Rachel didn’t stop traveling. She adapted.
How Rachel Travels Now
Rachel describes herself as someone who “packs her anxieties,” but in a productive way.
Her prep includes:
Bringing a med kit stocked with small doses of essential meds
Monitoring hydration closely on travel days
Planning meals and bowel habits ahead of time
Understanding bathroom access in each country
Carrying small local currency bills for paid restrooms
Bringing a letter from her provider outlining her diagnosis and meds
“After many international trips, I’ve proven to myself that how I feel at home reflects how I feel on the road.”
Rachel also buys comprehensive travel insurance that covers pre-existing conditions, often from TinLeg, and encourages others to read the fine print carefully, especially regarding upfront payment rules.
“I feel much more secure knowing all medical bills will be paid for should I need anything abroad. Beyond health insurance, I have used the insurance for trip interruption and costs of delays. I also have my provider write me a letter stating my disease, common side effects, and my current medications. This letter can be useful when seeking care at a new clinic or if TSA should ever give you a difficult time (I have never experienced this). I like having the physical letter in the med kit.”
Bathroom Access: A Cultural Learning Curve
When traveling with others, Rachel gives them a heads up that access to bathrooms is a priority for her. Especially when traveling in Europe.
“Europe often requires a purchase to use a restroom. You cannot just run into a McDonald’s.”
Her strategy?
Plan ahead
Carry cash: Having a few small bills in the local currency is helpful to make a quick sale or pay at public bathroom stations in some countries.
And she always tried to keep everything in perspective, even when the unexpected happens.
“Accidents are embarrassing, but you will most likely never see these people again. It is okay. You are okay.”
Travel Anxiety: You’re Not Alone
Rachel acknowledges the fears that come with IBD, but her message is clear:
Do not let IBD keep you from seeing the world. Start small and your confidence will grow.
She now travels to Mexico annually and cannot imagine winters without it.
Nurse-Approved Safety Tips from Rachel
Some of her favorite reminders:
Even healthy travelers get GI bugs—be cautious with food and water. Taking general precautions like only drinking bottled water in areas where the water might not be safe to drink, sanitizing your hands often, and avoiding touching your eyes and mouth are still the best ways to prevent infections.
Avoid buffet sushi
Choose made-to-order stations
Read resort and food reviews. She checks out Google reviews, TripAdvisor, and Hotels.com to see what people have to say before she books a trip.
Wear an N95 on flights to avoid illness and see if your travel companions will do the same to help keep germs at bay.
Advocate for yourself with travel companions
Read Google reviews quickly if you’re unsure of a restaurant, locals and travelers will share if they got sick eating there. Look for highly frequented places.
As a nurse, Rachel has these words of wisdom for our community, “Don’t let IBD keep you from seeing places and experiencing new cultures. Often as patients we have anxiety and unknown destinations can seem overwhelming and scary. Start small and your confidence will grow, promise.”
Rachel’s Travel Med Kit
She carries:
Doctor’s letter
Hand sanitizer
Tylenol
Imodium
Pepto
Tums
Fiber
Gas-X
Benadryl
Dramamine (also helpful for intense nausea)
Zofran
Liquid I.V.
Band-Aids that are a few sizes
Contact solution or small vial of artificial tears (I wear contact lenses)
A few doses of Dayquil and Zyrtec—when changing the container medication comes in, be sure to write the dose (mg or ml or the number of pills) and how often you take it.
A tube of triple antibiotic ointment and hydrocortisone ointment (for scrapes and bug bites)
Final Thoughts: You Deserve to Experience the World
Traveling with IBD takes more planning, more flexibility, and more courage than most people will ever understand. But as Kelly and Rachel show, it’s possible and it can even become empowering.
As someone who was diagnosed with Crohn’s more than 20 years ago traveling can still make me feel a bit uneasy. I always keep pain medication, Zofran, and Dramamine in my carry on. If you have to pack your biologic medication, keep that on you as well. It’s important to check how long your injection can be out of the fridge. Nowadays, Humira for example, can be unrefrigerated for up to 14 days. If you have to do your injection while away from home, make sure to have alcohol swabs and an ice pack (if you are used to using one).
I never drink caffeine prior to flights or long road trips, and I eat very light until I am at my destination. I try to dress as comfortably as possible, and do not restrict my belly in any way. The moment I get to my hotel room I take off my travel clothes and shower. If you are traveling and feeling symptomatic, it can be helpful to alert your care team at home and also do research beforehand about local hospitals so you have a game plan in place should you be facing an acute flare that may require a trip to the emergency room.
Whether you are taking a weekend road trip or boarding a long-haul flight, remember:
You’re allowed to take up space. You’re allowed to prioritize your needs. You’re allowed to choose comfort over speed. You’re allowed to protect your energy.
And most importantly:
You deserve to make memories that reach far beyond the walls of your disease.
Community and chronic illness can be thought of as a beautiful tapestry. Our lives and experiences, while unique, become intertwined, and once we recognize we don’t have to embark on the isolating journey alone, we are forever changed. We are so much stronger together. Johnson & Johnson’s published White Paper developed through IBD Social Circle entitled, “The Power of Community in Inflammatory Bowel Disease: Coming Together to Reduce physical and psychosocial impacts” highlights key touchpoints of the patient and caregiver experience and shows the ripple effect of Inflammatory Bowel Disease and how complexity and intricacies of Crohn’s and ulcerative colitis reach far beyond the gut. IBD impacts our careers, our relationships, our identities, our mental and emotional health, and it often dictates how our life stories unfold.
This week on Lights, Camera, Crohn’s, I’ll walk you through the valuable insights from the white paper and show what the research uncovered when it comes to stigma, mental health, online communities, and more. You’ll hear heartfelt reactions from IBD patients and caregivers about the findings and hear what two leading gastroenterologists have to say about the research.
Leaning on the lifeline of community
Jessie Magaro was diagnosed with IBD when she was 15 years old. Her reaction to the white paper speaks volumes.
“I was almost in tears reading this research. When I was first diagnosed as a child, there was no readily accessible community to lean on. It was isolating, depressing, and incredibly lonely. But when my disease returned in adulthood after years of remission, I realized the world had changed,” she recalls. “Suddenly, there was visibility. People sharing their stories openly online, entire communities forming on social media. For the first time, I could connect with others who were like-minded and like-bodied, people who understood my fears, my choices, and my fight.”
That connection wasn’t just comforting; it was lifesaving. It became essential to Jessie’s mental health and gave her the strength to make the hard, necessary decisions about her body and her health that helped her survive.
The white paper digs deep into how and why patients and caregivers crave additional information and resources within the IBD community. According to the survey, “Nearly all people with IBD (95%) are looking for IBD information and resources beyond what their physician provides or discusses with them.” The survey found:
42% of people with IBD have participated in online IBD support groups
37% have engaged with social media forums or group chats on platforms like Facebook and Reddit
28% have followed influencers who share their IBD journey on social media platforms.
Dr. Jami A. Kinnucan, MD, is an IBD specialist at the Mayo Clinic Florida. She says, “This research is profoundly impactful for the IBD community, as it highlights many of the challenges that patients experience but often do not share with friends, family, or even their healthcare team. It opens the door for important conversations within the IBD community and reinforces the need for clinicians to explore the broader effects of disease beyond physical symptoms.”
The pediatric caregiver perspective
Cindy Hancock’s daughter was diagnosed with Crohn’s at age eight, she tells me if there can be a “best” part of being an IBD caregiver, it is “absolutely the online community she’s been so grateful to find and learn from.”
As a result of how heavily her and her daughter have leaned on and benefited from the support of others who “get” the reality of life with IBD, Cindy was not surprised by the findings of this white paper that highlight the power of community.
“The courage to seek out a second opinion, and bring info shared by the second-opinion gastroenterologist to our established gastroenterologist? CHECK. Information about how to interpret iron blood work that helped me advocate for transformational care for my daughter, CHECK. Learning what intestinal ultrasound is, and why it presents an amazing opportunity for IBD care and joining forces with other patients to informally advocate for its increased usage in the U.S., CHECK. Anecdotes about drug interactions via lived experiences of other people with IBD, CHECK. Recommendations about favorite heating pads, CHECK. Learning from another Crohnie that gummy bears who aren’t red or purple are part of a colonoscopy prep diet, CHECK!! I could go on and on all day!” says Cindy.
She feels fortunate that her daughter has a good team of physicians, and they always seek their opinions first of course. But Cindy feels the tidbits they’ve gleaned from the IBD community online are what have transformed her daughter’s quality of life with Crohn’s. “The impact is incalculable.”
Cindy credits patient advocates for helping guide healthcare decisions, saying “the IBD community is akin to a warm blanket. We very rarely interact with people in the “real” world who live with IBD, but every day we get to interact virtually with people just like us who understand this life… and that sense of community is priceless.”
Bridget Brown’s daughter was diagnosed with Crohn’s two years ago when she was eight. She says, “Humans are built for connection—but when you’re handed a diagnosis that isn’t widely understood, it can feel incredibly isolating. Most families reach an IBD diagnosis after some really dark, confusing months and years. The IBD community brings the light back in.”
She says as a parent, hearing other people’s stories and experiences is everything.
“I don’t know what it feels like to live inside my daughter’s body, but the insight gathered from the online IBD community helps me support her better. There’s real strength in shared stories, and there is nothing more valuable than being heard from someone who truly gets it.”
Dr. Hilary Michel, MD is a pediatric gastroenterologist at Nationwide Children’s Hospital in Ohio. She says in reading this white paper she could not help but think about how the concepts also apply to children and adolescents with IBD.
“In addition to physical symptoms, youth with IBD are also at increased risk for anxiety and depression and school absenteeism. In a period of life characterized by marked changes in development, independence, and relationships, the diagnosis of a chronic disease like IBD can be incredibly impactful,” says Dr. Michel. “Access to the IBD community for education and support is likely to be equally as important to young people with IBD and already exists in formats including in person and online groups, advocacy efforts, and camps, such as Camp Oasis. Just knowing they are not alone with IBD is so powerful. Additional attention should be paid to privacy and safety concerns when developing interventions for young people.”
Dr. Michel also feels support for parents and caregivers of youth with IBD is essential.
“Parents are at risk for missed work themselves and experience immense guilt and stress related to caring for their child. Connecting with other parents who have “been there,” sharing tips and tricks to navigate their journey, or simply having a listening ear can go so far in allowing parents to feel supported.”
The Power of the IBD Social Circle: A Veteran’s Perspective
Suzy Burnett is an IBD mom of three and blogger at Crohnie Mommy was diagnosed with Crohn’s in 2008. She says when the white paper was published, she read, and re-read, the IBD Social Circle’s latest report.
“The first reading left me stunned by the raw reality encapsulated in the statistics. The second reading became a series of nods: “Yes, that’s me,” I found myself thinking with every single finding. I found the white paper to be fascinating, maddening, raw, and often heartbreaking. Mostly, because I have personally walked down, or known someone in the IBD community who has walked down, every single path described. Simply put, this report is SPOT ON.”
Suzy says her own patient experience deeply resonated with the segment that focused on the critical role our community plays in every aspect of life with IBD: from the shock of diagnosis and the struggle with relationships to the relentless search for answers and navigating new medications.
The Birth of a Community
“When I was first diagnosed, Crohn’s disease was relatively unknown. The internet was not the wealth of knowledge it is today,” explains Suzy. “I was handed a packet of paper, told there was no cure, and left to grapple with denial, depression, and severe flares for years.”
As Suzy grappled with her disease and the years ticked on by, she felt as though the IBD community was born.
“Or we all simply started emerging from the woodwork, bloggers, patient advocates, and a growing number of patients sharing their stories. It felt as if we made an invisible pact: to stick together, stay strong, and fight for each other. It felt like a window of hope opened: I found others. Others like me.””
Suzy says the research done in this report should be shared with every newly diagnosed patient and every “old veteran”.
“We are IBD warriors, and this white paper embodies that truth to the core. It is an invaluable resource for all who suffer from IBD, as well as for the caregivers and family members who stand by their side.”
Recognizing the importance of treating the whole self
Katie Connelly has lived with Crohn’s disease for more than 20 years. She says hearing that patients are afraid to share their emotional burdens with their HCPs is defeating and eye-opening.
“As someone who is lucky enough to have one of those GI specialists who sees me as a whole person, it is imperative that I let her know how I am feeling about my quality of life. It helps her gauge where I am both physically and emotionally with the treatments I am on,” she shares. “With the mind/gut connection being such a real thing, it needs to be instilled in every HCP’s practice to inquire on how their patients feel in life. The responsibility cannot always fall to the patient to disclose everything.”
As a woman living with perianal fistulizing Crohn’s disease, Katie knows firsthand how isolating and complicated the patient journey can be. She credits the patient community for helping her cope and get educated about the questions she has had about intimacy and sexual dysfunction.
“I have had fistula for six years now and have both dated and ended up married while living with them. It has been far from easy, and there is a lack of understanding and communication around it. I hope to start bringing up my own sexual experiences and helpful tips through my own community, Badass with a Bad Ass in hopes to help lower those numbers. I just want us all to feel less isolated in this.”
Being wary of misinformation shared online and in person
Kelly Dwyer says she’s benefited from both in person and online IBD communities over the many, many years of living with her disease. While she’s grateful for community support, she believes misinformation is one of the greatest threats to IBD patients.
“When I attended my first support group after I was diagnosed, I found a community of people who were anti-biologic and unsupportive of many questions I had about treatments and medical care for IBDers. I was so dismayed to see that they were the only in-person support community in one of the US’s largest metropolitan areas, and promoting non-science backed theories of IBD care,” recalls Kelly. “Commitment to strict content moderation and upholding science-backed information is one of the reasons that support communities affiliated with national IBD organizations are an essential part of IBD care and connection.”
While she agrees the online community is beneficial, she also wants patients and caregivers to always have their guard up and be aware of the misinformation and opportunists who go after vulnerable IBDers by attempting to spread fake cures and push “snake-oil” treatment to a make a quick buck.
“As with many chronic illness communities, the newly diagnosed are uniquely susceptible to bad actors because of the desperation and grief that comes with being diagnosed with this incurable, devastating disease,” says Kelly.
While she believes many patient advocates seek to promote accurate and data-driven information, such as advocates like Tina Aswani-Omprakash and Brooke Abbott Abron who are cited in this study, Kelly wants to warn others that just as many others are publicly sharing their support for dangerous treatments, unregulated supplements, and potentially harmful lifestyle and diet choices.
“National organizations, physicians, patient advocates, and support communities like IBD Social Circle are doing their best to create easily accessible, data-driven, and science-backed resources for education for IBDers at all levels of managing their disease, and from diverse cultural and racial backgrounds. Making sure these resources speak loudly and spread far online will be a vital step to combatting the harms of misinformation. We all need to do as much as we can to educate and inoculate fellow IBDers against the dangers of anti-science rhetoric,” advises Kelly.
The financial trade-off and workplace woes with IBD
Ian Goldstein has lived with Crohn’s since 16 years old. The white paper’s discussion on disclosing diagnosis in the workplace and requesting accommodations hit home for him.
“I was fearful of mentioning my disease on job interviews and at work because I did not know if my co-workers would view me differently, if they would think I was less equipped for my role or more expendable. For a long time, I had to get weekly iron infusions, and I don’t know if my employer didn’t like that I worked remotely because of this, says Ian.
The white paper highlights a 2024 survey from the Crohn’s & Colitis Foundation that found more than 40% of people with IBD have made significant financial trade-offs to afford their healthcare, including giving up vacations or major household purchases, increasing credit card debt, and cutting back on essential items such as food, clothing, and basic household items.
“YES! 1000% YES. If I ever take a vacation, it is a weekend trip upstate because I need to make sure I have money set aside to afford my one thousand dollar a month health insurance premium in addition to the deductible and copay costs. If healthcare didn’t cost so much, my life would look quite different,” says Ian.
Everything from career impact to diet resonated with Ian. The focus in the research on foods and beverages that are staples for most but may be on the list of foods people with IBD should avoid (such as fried or greasy foods, spicy foods, sugar-sweetened drinks, and whole-fat dairy). Ian believes it’s important that people understand that it is not just the “unhealthy” or “junk” foods that can exacerbate symptoms.
“For 10 years I avoided vegetables and nuts completely because they put me at risk of having a bowel obstruction. The same foods that would make me healthy could also send me to hospital,” explains Ian.
Falling back on community for overall well-being and treatment decisions
The white paper highlights that, through IBD community engagement and support, patients have reported positive impacts on:
Physical well-being and treatment decisions
39% reported that it has helped them identify ways to make improvements in their physical health and well-being
39% learned how to improve their ability to communicate with their HCPs
39% became more informed about IBD treatment options, including different treatment options they did not know about before
32% learned how to better advocate for themselves with their HCPs
Ian couldn’t agree more, “Community has been a game changer for me. Because of two friends I met from social media, I learned about an amazing surgeon in New York who did an outstanding job with me in 2025, and I haven’t felt this good in years.”
He puts on comedy shows in New York centered around healthcare and because of one show called, “The Autoimmune Saloon,” Ian crossed paths with an audience member who mentioned Intestinal Ultrasound. “No doctor had ever mentioned it to me, but this random audience member did. Because of her, I’m able to get this test, which is much less invasive and informative when it comes to my Crohn’s. This is how community makes an impact: we teach others what we know, things that doctors may never think to tell us.”
Facing the music and fighting the stigma across all races and cultures
According to the white paper, up to 84% of adults with IBD feel that there is perceived disease-related stigma against them, which results in social stereotypes making them seem unreliable or antisocial.
IBD has historically affected White populations at a higher prevalence than other groups; however, the research shows the incidence of IBD is increasing in all races and ethnicities across the US, including in people who are Black, Hispanic, Latino, and East or Southeast Asian. Research also suggests that Black, Asian, and Hispanic individuals with IBD may have a higher incidence of more severe disease.
Kimberly Hooks says, as a Black woman living with IBD, she knows exactly what it feels like to be dismissed, overlooked, and told that her symptoms didn’t fit the picture.
“I was diagnosed late, and even after that, there were delays in getting the medication I truly needed for my severe Ulcerative Colitis. That delay cost me my colon. My story isn’t unique; it reflects what so many Black and Brown patients experience when our pain is minimized or our symptoms aren’t taken seriously,” Kimberly shares. “That’s why this research matters so much. It confirms what we’ve been living. IBD does not discriminate, and our communities are being affected at rapidly increasing rates. This is why I advocate, because visibility saves lives, and every person deserves to be heard, believed, and treated with quality care.”
Kimberly went on to say how incredibly grateful she is for the IBD Social Circle creating a safe space for patient voices and grounding this work in real lived experiences.
“Partnering with advocates to highlight our real stories and pairing those stories with research exploring the physical and psychosocial factors impacting patient care is powerful. It shows the benefits of community and how connection can support people with IBD in every part of their disease management. This kind of work gives me hope. When patients and community come together, we don’t just raise awareness, we help shape a better, more equitable future for everyone living with IBD,” she says.
Acknowledging the struggles IBD can present in motherhood and beyond
As a patient leader and an IBD mom of two small kids, Michelle Pickens appreciates the white paper for a multitude of reasons, especially the notion that we can appear “fine” even while we’re struggling. She also valued the discussion around the wide range of symptoms patients face and how this variability can delay diagnosis and access to support.
“That “in-between” period—when someone is sick but unsure where they fit or where to turn—is incredibly challenging. You experience symptoms consistent with IBD, yet you don’t quite feel part of that community without a formal diagnosis,” Michelle explains.
The section of the white paper on remission really resonated with Michelle. There is often an expectation that once you begin treatment, you will immediately feel better, but that is not always the case. She says it’s important to acknowledge the need for community support when clinical measures indicate remission, but physical symptoms persist.
“I was glad to see the impact on the family unit addressed, especially in areas such as domestic responsibilities and parenting. These are areas where I personally struggle at times. In the workplace, accommodations can be requested to help manage IBD symptoms, but parenting offers no such structure,” Michelle shares. “As a mother, it can be difficult to find someone who can step in and keep things running the way you would, so the responsibilities often fall back on you, even when you’re unwell. This contributes to significant “mom guilt,” and while mom communities exist, the parenting experiences of those without chronic illness differ greatly from my own.”
Addressing mental health struggles
The white paper reveals that more than half (52%) of people with IBD consider the impact of IBD on their mental well-being as negative. Other research studies have shown that individuals also experience depression and anxiety—with as many as 40% and 30%, respectively, experiencing these comorbidities, even while in remission.
The body image issues that stem from IBD such as weight loss, hair loss, steroid-related weight gain, ostomy bags, fistula, and other extraintestinal manifestations make life feel like a minefield. We are constantly up against the unpredictable nature of living with a disease that can rear its ugly head at any given moment. We are constantly forced to pivot and make decisions that often have a direct impact on our overall body image. I remember when I was in college (prior to my Crohn’s diagnosis) that I loved being on camera, working in TV news. Fast forward to five months post-graduation and three months post-diagnosis, and I was mortified anytime anyone tried to take a picture of me. Looking in a mirror was a stark reminder of what I was now and what I used to be.
These photos were taken 3 months apart. Pre-diagnosis and while on 22 pills a day.
Please know that if you struggle with this, you are not alone. As the white paper notes, “as many as 75% of women and 50% of men experience body image issues because of their IBD.”
Final thoughts
This white paper is a gift to the IBD community. As someone who was diagnosed with Crohn’s in 2005, I would have given anything to have a resource like this at my fingertips to validate my struggles and recognize my fears. We are at a pivotal point in patient advocacy and leadership where we can help shape the future of what it means to live with IBD and thrive despite the dark days.
Dr. Matthew Ciorba, MD, a gastroenterologist at Wash U in St. Louis says, “This work offers patient-identified, doctor-approved insight. It brings together perspectives that clinicians alone often cannot fully grasp. The document fills a unique niche in the IBD space. It bridges the lived experience of patients with the expertise of leading clinician advocates. There is truly nothing else quite like it.”
Our community, everyone from patients to caregivers, and medical providers, is so unique. For many of us, these connections and friendships (whether online or in person) have helped us to reclaim a sense of purpose within our disease journeys. My hope is that medical providers and GI psychologists use this research to empower and educate the community by providing this incredible research to patients and caregivers.
Check out the Executive Summary of the White Paper
When you’re diagnosed with Crohn’s disease or ulcerative colitis it’s a lot to process. When I started this blog in 2016 and after living with Crohn’s for nearly 19 years, my focus has always been to be the voice I needed to hear upon diagnosis and what it was like to experience young adulthood with a chronic illness. As a 21-year-old, fresh out of college, I had to navigate my career, finding love, and becoming a mom with IBD on my own. The first decade I wasn’t publicly sharing my story and didn’t know there was a patient community to tap into online for support.
The first week I started experiencing Crohn’s symptoms-March 2005, Senior Spring Break in the Bahamas
Often as the years go by and we get beyond the initial shock of hearing the news and what this means for our lives, we tend to forget the challenges we faced to gain our footing. This week on Lights, Camera, Crohn’s I share some tokens of knowledge I’ve gained along the way that I hope will help you on your own journey, no matter where you find yourself at this moment.
Healing—physically, mentally, and emotionally is not linear. We all experience IBD uniquely—some people’s disease course is milder, others have it severe. We all cope differently with knowing and living with a chronic illness. Give yourself grace in the difficult moments. It’s ok to feel resentment or anger. It’s understandable to wonder at times “why me.” It’s “normal” to feel scared and anxious whether you’re a few weeks or a few decades in. Sometimes it’s taking things one hour at a time, other times it’s taking them one day at a time. Because of how quickly a flare up can strike, I try to live in the now and not worry about tomorrow.
You didn’t have control of getting your chronic illness, but you can control how you react and choose to heal from it. It’s easy to feel like you may be to blame if your health takes a turn for the worse. But understand this is not your fault. The unpredictability of IBD makes it feel like we’re often in the passenger seat and spiraling in circles, but this disease cannot control how you react, respond, and choose to heal from it. No matter what, you’re in control of the healing process. Whether it’s finding support through fellow patients and caregivers or through professional therapy, you won’t look back and you’ll be setting yourself up to take this on to the best of your ability.
There is no comparison game. Since the majority of people are diagnosed with IBD in their teens and into their 30s, it can be easy to try and measure your timeline and accomplishments to that of your peers who do not have chronic illness. It can also be tempting to look at people in the patient community who seem to have the world by the tail, when you’re struggling to get out of bed each day. This isn’t a competition of the sickest or a ploy to see who can smile through the pain and get more done. The only person you need to answer to, is who you see looking back in the mirror. You determine what you’re capable of and what you want in life. Your roadmap is yours and you’re right where you’re meant to be.
You set the benchmark for what’s possible. Your IBD is part of you, but it’s not your entire identity. Remember that even patient advocates are posting somewhat of a highlight reel. Even those who are working, in love, and parenting are dealing with their own struggles, too. My best advice would be to think about what you hope for in life (don’t even think of your IBD as part of the equation) and go after it. Yes, your health may cause some detours and roadblocks, but you won’t find your way unless you try.
No one knows your body better than you. I don’t care how many letters someone has after their name, they aren’t living in your body and experiencing what you feel each moment of every day. Be vocal when you need to be. Communicate as much as you can with your care team and paint the clearest picture of your reality. If you keep parts of your struggles to yourself or dumb down the severity of your day-to-day life, the only person you’re hurting is yourself. Learn about nutritional bloodwork and advocate for yourself to be tested for a full iron panel with Ferritin and Vitamin D. Get labs every 3-4 months so you can keep a finger on the pulse of what’s going on with your body. If you feel like your provider is being lackadaisical, don’t hesitate to get a second opinion. Take ownership of your health and find a provider who in your darkest moments you would feel most comfortable by your bedside in the hospital.
Make sure your GI specializes in IBD. There are gastroenterologists and there are gastroenterologists who specialize in Crohn’s and ulcerative colitis. Once you’re diagnosed with IBD, it’s imperative you try to find a GI who is an IBDologist. This can be tricky if you live in a rural area, it may mean you need to travel several hours to find a provider who fits the bill. If you move or are unsure of a good GI to check out, it’s helpful to reach out to your local Crohn’s and Colitis Foundation chapter and often they can help point you in the right direction.
Diet and stress levels matter. Read that again. Any doctor who tells you diet, and stress doesn’t impact your disease process is wrong. There are incredible registered dietitians throughout the US who specialize in IBD, and many of them have IBD themselves! Before you start restricting yourself or your child, make an appointment—most provide virtual options and this will help you get educated on what works best for you. What is a trigger for one person, isn’t necessarily a trigger for another. There isn’t a one-size-fits-all diet or else we would all do it.
Emotions will strike when you least expect them. Even almost 19 years in, I’ll sometimes break down and cry when I think about my Crohn’s or how it makes me feel. Just because you become a veteran patient doesn’t necessarily mean you fully ever heal from the hurt life with a chronic illness causes. It’s ok to have these moments where you may feel like you’re allowing your disease to control your emotions, you’re not. You’re human. It’s healthy to feel frustrated and to get emotional about what your life is like because you have IBD.
You’ve endured more than you give yourself credit for. As chronic illness patients we go through so much that often we don’t even bat an eye over experiences that would be extremely painful or stressful to the average person. Think about what a bad ass you are and how that carries over into each and everything you do in life. If you’re newly diagnosed you will get there—but even those initial weeks and months, you’re enduring more than the people who have their IBD under control and have a good handle on their body. No matter how many surgeries, scopes, scans, and IVs I’ve had, I always get a little teary eyed because it brings me back to 21-year-old me and then all the trauma that comes along with living with Crohn’s for 19 years. While those tears are sad, they also come from the strength of reflecting on what I’ve gone through to bring me to now.
Stay in tune with how your body is speaking to you through symptoms, do not ignore them. It can be challenging to communicate what you’re feeling to someone who does not have IBD. I get that. But by protecting loved ones, friends, and doctors from what you’re experiencing you’re preventing them from stepping in before it’s too late and before you know it your flare has gotten out of control and requires hospitalization. I used to be that person all the time. I would always internalize the pain, silently fighting through each day, doing anything possible to stay out of the hospital until the symptoms were simply unavoidable and required medical intervention. One hospitalization always sticks out in my mind. It was May 2009. I was a 25-year-old morning news anchor in Wisconsin. I was solo producing a 2-hour morning show dealing with horrible abdominal pain that kept making me throw up in the garbage can next to my desk in the newsroom as I struggled to put together the show. Finally, I couldn’t take it anymore and I had to call my co-anchor, who rushed me to the hospital. I was released from the ER hours later after my parents had driven from Chicago in the middle of the night only to return to the hospital that afternoon and have my dad carry me in his arms through the automatic doors. I was finally admitted and given the medical intervention I needed. Take it from me, you’re creating even more of an uphill climb for yourself if you don’t start speaking up when you initially notice something is awry.
The worst moments are just that, moments. When you hit your breaking point, when the pain seems overwhelming, and you can’t see the forest through the trees try to breathe. Go to your happy place. Recognize this is one day, one moment, I always tell myself “This too shall pass.” Go to your happy place mentally. Do mindfulness exercises. Shut out the outside world and focus on your breath. Detach from your body as best you can. Think of people who inspire you and bring you joy. Everything is fleeting. Each flare, each recovery, each prep, procedure, and surgery…it has a start and a finish. One day it will be a memory you talk about.
Pay attention to who is there when you when are quiet and when you’re going through the thick of it. IBD is too big to deal with alone. Lean on people you can trust, who you genuinely feel safe sharing your health woes with. This will be fewer people than you’d ever imagine. Be prepared to realize that many of the people you thought would be front and center to support you will be non-existent. It’s fine to mourn those friendships or relationships, but don’t waste your time or energy on them. Your disease will give you the ability to see who loves you and who wants to be present in not only the good times, but the bad. You can’t change people. Hold on tightly to the people who show up consistently, expecting nothing in return. Those are your people.
Emmanuel Acho shared a reel on Instagram recently that really hit home for me and caused me to reflect a bit on the people in my life and their roles. In the video he explains that friendship is like a house. You have your window, door, and floor friends. Window friends are outside looking in, they don’t know what’s going on in your house. They don’t have intimate access to what’s going on in your life. You can only let so many people into your house. Door friends come in and out of your life depending on the season. When life gets too hard or when your world turns cold, they might exit. Your friends might not be equipped for that season. Floor friends—aren’t going anywhere. You might track mud, but they will last regardless of the season. They are there to catch your tears and hear your fears. Remember—a house has more windows than it has doors and more doors than it does floors…if it has one good floor, you’re set.
Just because you need medication does not mean you’re taking the easy way out. I’ve been where you are. I remember lying helpless in a hospital bed and what it felt like to be told I needed to “break out the big guns” and start a biologic medication back in 2008 when there were only two options on the market for those with IBD. In that moment, we all naturally want to learn about side effects and what this could possibly mean for the long term. But please try and focus on the actual risk versus the benefit. As someone who has been on Humira since July 2008, I’m so grateful for my medication for allowing me to live a full life, bring babies into this world, and be a present, able-bodied, and active mom. It’s not all medicine, or all diet and lifestyle, often for many of us who have moderate to severe IBD we need a mix of both, and that’s ok. You can still thrive and be healthy, despite being on a medication with a black box label.
You are not a burden, and you deserve love. Any romantic partner who makes you feel less than, isn’t present when you need them most, or doesn’t show any empathy or interest in your daily reality isn’t going to stand the test of time. Use your IBD to your advantage to see your partner’s true colors. Be honest and upfront when you start dating and if you ever feel like you need to defend their actions or make excuses consider that a major red flag. Dating and marrying a person with a chronic illness isn’t for everyone, and that’s fine—but when it comes to people like you and me, we need a partner who is willing to take the challenge on beside us every step of the way. Find someone who you feel comfortable communicating openly with, who sees you for more than your disease.
IBD is not a battle to be “won” or “lost.” One of my pet peeves with any health condition or disease is when people say “so and so lost their battle”…they didn’t lose shit. Diseases are not a game. Oftentimes reaching remission is due to luck, disease severity, or surgery. I spent a decade of my life with active disease and have been in remission (thanks to surgery) for almost nine years. I don’t give myself credit for that, I’m not “winning.” It’s because of my efforts to stay diligent with my biologic, vitamins, safety labs, daily decisions, and check-ins with multiple specialists, but I also don’t think I’m at this point because of something special I’m doing compared to someone else. We’re all dealt a different hand of cards in life. Your IBD isn’t a win or lose situation—you’ll celebrate big victories and small ones, too, your disease can rob you at times, it’s a never-ending exchange and game of back and forth. You are not less than because you are flaring. You are not lazy for taking medication or failing because you struggle to follow a strict, regimented diet that may or may not help you. Once you stop thinking of everything as a “fight” it takes a bit of the stress, anger, and onus off your shoulders. IBD is a chronic illness, until there’s a cure, we’re in this situation until the day we die…that’s simply too long to be “fighting” anything.
Get ready to be extra proactive with your health. Due to the nature of our IBD and the medications many of us take, we are at greater risk for additional health problems. It’s important to get annual skin checks at the dermatologist. Make sure whether you have good vision or not that you’re seeing an eye doctor. Get cleanings at the dentist at least every six months. If you’re a female, make sure you get your well woman visits. We are greater risk for cervical cancer because many biologics don’t allow our bodies to fight off HPV, this may mean annual Pap smears. We’re also at an increased risk for breast cancer, so don’t delay your mammogram. Get a bone scan every 3-4 years, get one as close to diagnosis as you can so you have a baseline. Your GI may say it’s not necessary, it is. Steroids put us at risk for osteopenia and osteoporosis from an early age, this may mean you need to see a bone health doctor (yes, those exist). Those of us with IBD are at greater risk for pelvic pain, it can be helpful to see a Pelvic Floor Therapist who addresses those unique needs.
Faith can give you added strength and comfort. I understand faith is very individualized and looks different for each of us, but I can tell you as someone who is Greek Orthodox who has always been a faithful and prayerful person that I rely on my faith to guide me through my IBD each and every day. There’s a sense of comfort and hope that comes with believing God is watching over you through the good, the bad, and everywhere in between. When you’re diagnosed or flaring, it can test your faith. Hold on tightly to what you believe and lean on that (however it looks for you). I truly believe God gives his toughest lessons to his greatest teachers. One of my biggest fears as an IBD mom of 3 is that one of my children will get my disease one day. Each night before bed, I always pray with them and say, “keep my babies healthy, safe, and strong.”
My why. My motivation to push through each and every day.
Family planning takes time and effort. Just because you have IBD does not mean you can’t be a biological mom or dad one day. The journey will look a bit different, but this disease does not necessarily need to rob you of the experience if that’s what you want in your life. Communicate these desires with your GI so they can help prep your body for a baby. This can mean starting a prenatal vitamin and folic acid several months before trying. I had a colonoscopy before every pregnancy so that I could be given the ‘green light’ by my GI that we were cleared to try for a baby. When I was pregnant, my care was overseen by my OB, a maternal fetal medicine OB (high risk), and my GI. Unless you have perianal disease, you can have a vaginal birth, but oftentimes this is a discussion left to you and your care team. I personally chose to have 3 scheduled c-sections, because while I don’t have perianal Crohn’s, I didn’t want to risk tearing or causing a fistula to form. I would make the same choice if I had to do it all over again. I also stayed on my biologic through conception, pregnancy, and breastfeeding. These are all personal choices but there are many, many research studies available that show the safety and efficacy of doing so. If you feel you could have internal scarring due to past surgeries that could hinder your fertility, check in with a fertility specialist and have them help you investigate if there could be issues.
Educate yourself on insurance, prior authorizations, specialty pharmacies, and Pharmacy Benefit Managers (PBMS). Unfortunately, with IBD we are forced to do so much behind-the-scenes work to simply receive treatment and medication. You will waste countless hours and endless energy on the phone as these people give you the run around. Nobody ever seems to want to take ownership. Work with your gastroenterologist if you are denied a medication so they can write an appeal letter to insurance and go to bat for you. Stay on top of everything, don’t worry about annoying anybody. You gotta hustle. You gotta be frank and assertive. It’s not about hurting feelings; it’s about making sure people are doing their jobs and ensuring your course of treatment doesn’t get delayed because someone fumbles some paperwork. Our medications are time sensitive. Light a fire under people’s ass if you’re not getting responses you deserve. One of my friends on social media posted this over the weekend, “Managing specialty medications in January is an annual slap in the face to chronically ill people.” It sure is. This week will mark the first time I’ve ever received my injections late in the mail, due to a misstep in my GI office that I had to follow up on for over a week. Be extra proactive at the start of each year. Make sure your GI informs you about all the patient savings programs available, these can help you not only emotionally, but also financially.
You get the final say. No one but you gets to say what you do with your body. If a doctor wants you to do an enema before a scope and you don’t want to, don’t. If you don’t feel comfortable with taking a certain medication and your care provider keeps pushing it, they can’t physically make you pop a pill, take an injection, or receive an infusion. You must do your research, educate yourself every day, feel empowered by all you know and be ready to deal with the ramifications if you go against the grain or determine you want to try something differently. There’s not one “right” way to live with IBD. Be honest with your provider. Don’t say you’re taking a medication and then not take it, that’s not helping anyone or anything. Be a compliant patient, but an educated and empowered one at the same time. Measure all the risks and benefits and what your hopes and dreams are for your present life and for your future. Don’t ever feel like someone else can or should dictate what path your journey takes. Just because one biologic is a magic bullet for one person doesn’t mean it will be for you. You never fail treatments, they fail you. If a provider says “oh, you failed Remicade” … please correct them. “No, Remicade failed me.”
I write this as a 40-year-old mom of three—ages 6, 5, and 2.5 years old, married for almost 8 years, who has been on a biologic since 2008, who was diagnosed at age 21 in 2005. So much has changed for the better regarding the patient experience since that time. My perspective has come a long way. I used to be right where you are, so many are living your current reality. Instagram is the bread and butter for the patient community, that’s where you’ll find the most patients and caregivers transparently sharing. Follow the accounts, send a DM, comment on reels and posts, get engaged. Never hestitate to connect and reach out to me–natalieannhayden. Educate yourself through lived experiences and people who have paved the way for you, rather than Google. You don’t need to recreate the wheel, but this is your experience and your story. You get the final word on how you want each chapter to play out. Know each time you fall you will bounce back and that there’s a massive community of support here to catch you and cheer you on every step of the way as you rise once again.
Lights, Camera, Crohn’s: An Unobstructed View is officially SEVEN years old! If you told me when I started blogging what a labor of love this website would become for me, I never would have been able to imagine what it would become for my life, for the IBD community, and for patient advocacy efforts. I went into blogging blindly. I had no clue how to format the site, but I knew the types of stories I wanted to share and the messages from patients that I wanted to get across.
As a seasoned journalist who spent nearly a decade as a TV news anchor, reporter, and producer, I’ve used my love for storytelling to try my best to be the voice I so desperately needed to hear upon diagnosis, through my professional life, finding love, family planning, pregnancy, motherhood and beyond. It’s been quite the ride these last seven years. My first article went live July 23, 2016, on the 11th anniversary of my Crohn’s disease diagnosis. I found out I was pregnant with my now six-year-old, two days later. The first six years of Lights, Camera, Crohn’s (and 3 kids later), I shared a new article every single Monday.
Through these seven years, Lights, Camera, Crohn’s has been viewed half a MILLION times, by more than 320,000 people around the world. On this site alone, I’ve shared 368 articles, which does not account for the countless other IBD articles I’ve created for other websites. As I reflect on this milestone, I’m proud of what I’ve accomplished thus far, but know there’s much more work to be done.
This week I want to give you a behind-the-scenes look at how my storytelling process comes to life—I often get asked “how do you become a patient advocate?” and “how do you start blogging?” I hope this advice inspires you to take the plunge, as there are endless seats at the proverbial advocacy table and your voice, your story, your valid experiences, deserve to be heard.
Choosing What’s Newsworthy
It can be overwhelming trying to come up with content that is new and fresh for your blog and social media. I’ve found it extremely beneficial to have an editorial calendar that helps guide the stories that I share. My editorial calendar is in my email in the draft folder. I simply list out the dates (articles have always been shared on Mondays on Lights, Camera, Crohn’s…so I list out all the Mondays for the next 3-4 months). This serves as a reminder of my game plan and when I need to do outreach for the stories.
As a journalist you’re taught and it’s almost innate in some ways to always be on the lookout for a story. I’m always keeping my eye out for tweets and posts on Instagram, conversations in real life, experiences that happen to me when I see my GI or get a scope, that I think will resonate with our community. I think about the pain points I’ve felt along the way and the advice I wish I had when I was struggling in certain moments. I think about the questions I’ve had along the way when Google was scaring the bejesus out of me, and I just wanted real life advice from someone who understood my reality. Think about what uncertainty, questions, concerns you’ve had and what you want to learn more about and then go after the story.
Writing for the Reader
Everyone has a unique writing style, but one of the most common “mistakes” I tend to see with blogging is when writers go on and on and on about their own experience. The articles sound more like a diary entry—and if that’s what you’re going for, great—but usually, you’re wanting to draw readers in. To do this, I use my own experience as a foundation—a sentence or two in the intro and then the rest of the article is written to and for the reader. Try to write your blog articles like a news story. Use sub heads, get reliable sources, attribute studies, share credible information. Give readers in the chronic illness community news they can use. Empower others on their patient journeys so they learn something by checking out your content. Let others see that they are not alone in what they are going through and that you get where they are coming from. By including the expertise of medical professionals, it helps your articles really come to life and allows you to build a rapport and a reputation with the GI community. It’s always incredible to hear when a GI shares Lights, Camera, Crohn’s with their patients.
If you’re unsure how to reach a GI who is not your doctor, I advise going on Twitter and sending doctors a DM asking if they’d be interested in providing input for an article you’re working on. 9 out of 10 times you’ll get a yes. As we all know, doctors are busy, so try and give them a longer lead time to respond to interview questions. I like to include a headshot when I quote a doctor, so I have them send you one.
My Patient Experience articles have become one of my favorite parts of Lights, Camera, Crohn’s—these articles are a major labor of love. I interview 10-20 patients, along with physicians, and spend upwards of 20+ hours out of the goodness of my heart to create a resource that a patient and caregiver can have at their fingertips when they’re trying to make major decisions about how they choose to manage their disease. Topics range from biologics to infertility or life with an ostomy. Rinvoq is coming up next, folks…I just need a breather since I finished writing Skyrizi earlier this month. By crowdsourcing and sharing the good, the bad, and the ugly I’ve been able to provide a complete look at the reality patients face and provide background that shows more than just my experience.
The Art of Interviewing
Whether you’re interviewing a fellow patient or a healthcare professional, the same process goes a long way. Try thinking about the main points of the article and the flow before you write the questions. You almost must think backwards. I do all my interviews over email—for multiple reasons. The number one reason, is that as a mom of a 6-year-old, 4-year-old, and 2-year-old, I don’t get many breaks and trying to conduct an interview over the phone or Zoom and capturing the true essence of what someone is saying is nearly impossible. I also prefer email because it gives people a chance to articulate their responses and enables me to accurately share their quote—word for word, without paraphrasing. I rarely give interviews over the phone, as I like fellow writers/editors/journalists to have what I’m saying verbatim.
When I send the interview email for Lights, Camera, Crohn’s, I provide a deadline in bold and then list the questions. I always ask for a high-level explanation of a person’s patient journey so I have an understanding of what they’ve been through and so I can paint a clear picture for the reader. Try to never ask “yes” or “no” questions—you want people to give good explanations and descriptions.
An example of email outreach to a pediatric gastroenterologist for an article I worked on.
Often the most important question you can ask if “Anything you’d like to add?”—in TV, podcasts, you name it, this is when people let loose a little bit and can provide you with key nuggets of information.
Once I receive the interview responses, I open up Word, and take all the content and start compiling what’s going to be a quote and what’s going to be a part of my wording/storytelling. Then, much like journalists do in TV news, I write the story around the quotes.
Have a Copy Editor (aka family member/friend review your content)
It’s always helpful to have an extra set of eyes on your articles before you share them. Since the day I launched Lights, Camera, Crohn’s, my mom has been my “copy editor.” I email her a draft of the article along with an explanation of what I’m hoping to get across and then she goes through each article with a fine-tooth comb and provides edits and feedback. If I get too fired up about something, she may politely advise I take a certain line of the story out or re-think how I word a sentence. She’s been my voice of reason through this entire process and as my mom, she’s my biggest cheerleader in not just life with Crohn’s, but everything. As a nurse of more than 40+ years, she’s also well versed in medical situations, as well as grammar.
Be Vulnerable and Transparent
Despite how many people advocate for IBD, Crohn’s and ulcerative colitis still have stigmas. It can be daunting to put your words down on paper and share them with the world. I spent the first decade of my disease just telling close family members and friends. What I’ve found since blogging and being a vocal patient advocate, is that by being open, you open yourself up to endless support and camaraderie. There is such strength that comes from saying you’re not ok or need help. Tell it like it is and don’t sugarcoat your story. At the time same, one of the main pillars of my advocacy has to always been to be transparent, while also positive.
Back in the day when I was diagnosed, and those first 10 years when I was living in silence, most of the content I read was pretty doomsday. While I understand and empathize with the pain and horror Crohn’s can cause in one’s life, I’ve tried to never sit in that sadness for long. If anything, IBD has given me perspective and clarity about the fact that IBD doesn’t have to destroy your life or who you are. Yes, it can create major complications, unpredictable setbacks, and hurdles, but those detours don’t have to rob you of what you hope to accomplish or become. While it’s important to be real, I find it just as important to provide hope and inspiration for those who wonder what their futures may hold.
Keep on Swimming
Due to social media algorithms and the lack of engagement many of us see online, it can feel disappointing at times when you put all this effort into an article or a blog and feel like you’re talking or reaching no one. I’ve been there countless times. Don’t let the “likes” or the follows deter you. Know that your words and your stories just need to get into the hands of one person who needs them, and that makes all the effort, time, and energy worth it. Your articles have legs—meaning that once you post them, continue to post, and share for months and years to come because these “evergreen” articles are always timely and necessary. Try to collaborate with others when you can. If news outlets reach out for a quote or if a health website asks for your input, give it—and then ask for your blog to be a part of how you’re attributed in the quote. If you see someone’s Instagram story referring to an article topic you’ve covered, grab the link and send it their way over DM.
If you feel like you’re in a rut or if you’re having a tough time creating content—don’t force it. Ask your followers what topics they’d like you to cover. Use the timing of the year to help come up with stories (for example, navigating diet around the holidays or back to school time and being an IBD teacher). Support the content of fellow advocates—comment and share articles that intrigue you and help others get their words out and the same will be done for you. Rather than seeing advocacy as a competition, view others as your ally—we’re all doing this to help others, spread awareness, drive research, and together we can truly amplify the patient voice—one article at a time.
There’s no telling what Lights, Camera, Crohn’s will look like seven years from now, but I don’t plan to stop storytelling anytime soon. Thanks for all your kind words, for telling me when my stories have touched your life or helped you make a tough decision, and for being there for me when I need support. If you’d ever like to collaborate with me to share your story or if you have a topic you’d like me to write about—please don’t hesitate to reach out.
Here’s to another seven years of breaking stigmas, spreading awareness, and making everyone in the IBD community feel seen.
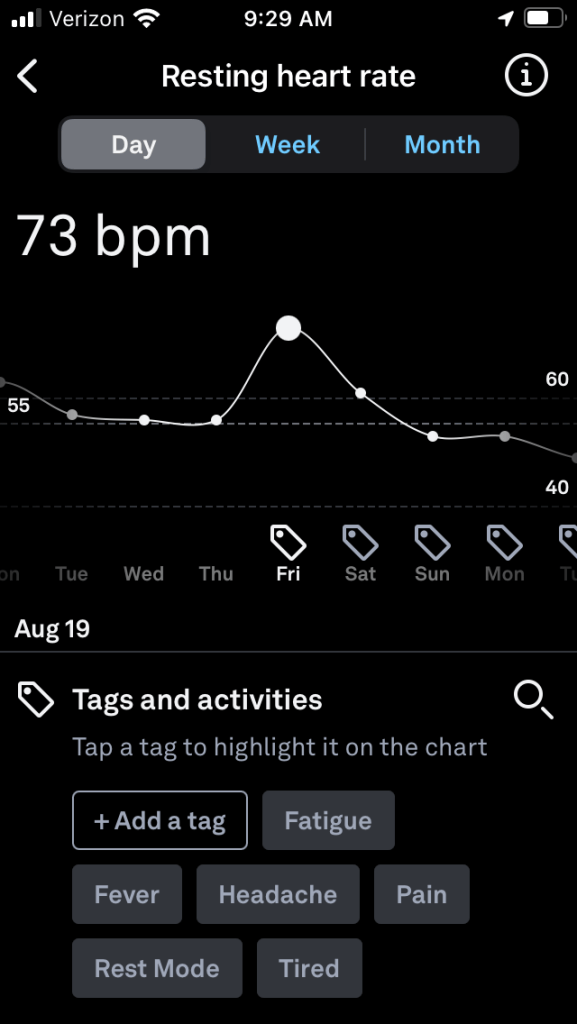
Raise your hand if you’ve ever been blindsided by an IBD flare. My Crohn’s has landed me in the hospital with zero warning on several occasions. The unpredictability of IBD is a huge challenge we all face. But what if a wearable device could signal when our disease course is going off the tracks? What if we had warnings long before we were face to face with our next flare?
An ongoing “Stress in Crohn’s” study out of Mt. Sinai’s IBD Center in New York and The John Radcliffe Infirmary/Oxford University in the United Kingdom has been investigating this since February 2021, with the help of 200 participants. The study wrapped up in June 2022 and was conducted in partnership with 4YouandMe and funded by a grant from The Leona M. and Harry B. Helmsley Charitable Trust to 4YouandMe.
The goal? To empower those with Crohn’s to monitor stress responses and early signs of impending illness worsening in between clinic visits, while providing a means to navigate life and mitigate the consequences stress has on our disease journey. While stress has long been known to somehow affect our IBD, the details of the relationship are poorly understood.
This week on Lights, Camera, Crohn’s we hear from an IBD mom and educator who recently participated in the Stress in Crohn’s study in hopes of taking action to help advance our knowledge of diseases like Crohn’s and ulcerative colitis.
The mission of the Stress in Crohn’s study
Wearables such as smart rings, smart watches, and smart scales, along with our phones, can collect information emanating from us. They can record our physiology and our routines that we are learning to weave together into “clinical symptoms”- such as fatigue, sleep, and stress.
“The main mission of 4YouandMe (nonprofit) is to empower individuals to navigate their own health by using wearables and apps while sharing their own health related data and insights for the benefit of all. This desire was birthed after working at Apple on their Special Projects team and grew out of asking “why can’t the data that emanates from each of us come back and help each person improve their health on a daily basis”,” said Stephen Friend, President 4YouandMe(nonprofit) , Visiting Professor of Connected Medicine, Oxford University.
Tina Aswani-Omprakash, MPH, Wearables Research Coordinator at Mount Sinai’s Susan & Leonard Feinstein IBD Center & Patient Advocate/Founder of the blog ‘Own Your Crohn’s’ says the promise of wearable devices in the prediction of IBD flares and drug response is real and something she’s excited about.
“As we know, IBD can be a progressive disease and it is important to shut down inflammation quickly to prevent complications. The wearable studies at Mount Sinai’s Susan & Leonard Feinstein IBD Center are looking to develop algorithms using measures such as heart rate variability, sleep duration & quality, essentially autonomic/ parasympathetic nervous system fluctuations via data collected through wearable devices. The hope is to help predict IBD flares and showcase drug response utilizing wearable device signatures,” said Tina.
Meet Nicole, Stress in Crohn’s study participant
Nicole Pavlin became a patient at the Mount Sinai IBD Center in New York and received an official diagnosis of Crohn’s disease of the ileum and jejunum in 2021, but her symptoms began more than 16 years prior. At the time Nicole was just beginning her teaching career and she was focused on raising her family. Once Nicole received her IBD diagnosis, she would often search GI research publications to better understand Crohn’s, along with the treatments and procedures available to patients.
“By educating myself about the disease, I’ve been able to communicate more efficiently with my healthcare team and advocate for my needs. The opportunity to participate in IBD research is always exciting to me, especially since the results could potentially help patients in the future,” said Nicole.
Nicole chose to participate in the “Stress in Crohn’s Study” from July 2021 to May 2022, which captured a period of time when her IBD symptoms took a turn for the worse. Nicole had bowel resection surgery that involved the removal of 6 inches of her ileum, including her Meckel’s diverticulum.
Getting recruited for the Stress in Crohn’s study
You may be wondering how Nicole got involved with this study. A Clinical Research Coordinator from the Mt. Sinai IBD Center reached out to Nicole to see if she’d be interested in participating. The researcher told her digital devices were being used to learn the relationship between Crohn’s disease symptoms and stress to try and predict the onset of flares.
“I was given detailed information about the study and instructions on downloading the app. The researchers provided me with an Oura ring, an Empatica EMBRACE wristband, and a Bodyport scale. I completed various surveys and tasks within the Stress Study app each day. Whenever I had a bowel movement, I would note the characteristics of the stool on the Pooply app based on the Bristol stool scale. The Rescue Time app was optional, and I chose not to use that one,” Nicole explained.
Daily points were awarded for wearing the Oura ring and Empatica wristband, using the Bodyport scale, answering survey questions, and completing tasks on the study app. Nicole received extra “boost points” for using the devices multiple days in a row.
“Every two weeks I gained points for completing a video diary and a cognition task. About five times during the study, I completed a Calprotectin stool sample at home through the IBDoc app. I had a support team and check-in calls each month to answer questions about my mental health and medications. There was also a study visit every three months to complete additional surveys about my health and Crohn’s disease.”
By the end of the study, Nicole earned more than 20,000 points for completing these tasks and eventually received 5 stars for being a “Groundbreaking Contributor” to science. She says the point system was a big motivator and a fun challenge. The study lasted 9 months. Nicole was compensated $400, and she got to keep the Oura ring.
Wearables provide a “new voice of objective data”
Up till now, those with chronic diseases have had to use their memory and feelings to convey their diseases. The wearables offer a new voice of objective data for themselves and for their physicians about what precisely occurred.
“In this study of Crohn’s disease, we were more interested in unlocking the link between stress and flares in Crohn’s. This is part of a larger set of feasibility studies to build for individuals a “Stress Load Navigator” for we note a tight connection between not just inflammatory bowel disease, but also diseases as diverse as diabetes, heart attacks, arthritis and even Alzheimer’s,” said Dr. Friend.
Marco Altini, Founder of HRV4Training, advisor at Oura, and Guest Lecturer at VU Amsterdam, says recent advancements in wearable technology are making it possible to move away from the lab and monitor our physiology continuously, in real life, when and where it really matters.
“In the context of many chronic conditions, the ability to monitor our own, individual changes in resting physiology over long periods of time, and in relation to symptoms or other makers, could finally help us better manage our health,” said Marco.Devices such as the Oura ring can monitor accurately resting heart rate and heart rate variability over time. These signals are tightly coupled to our stress response, which is often an important part of the picture when managing our health.
Participating in research as an IBD mom
Since there is a genetic component to IBD, Nicole says she worries that her children could show signs of the disease in the future. She’s been very open with her children about the challenges she’s faced with the disease.
“I want to model resilience for them so they can see how to navigate difficult situations. By participating in research, I want to show them that we have a chance to use these challenges to help others and make a difference in the future.”
Nicole says it’s encouraging that wearable devices could potentially predict the onset of flares, which might offer faster treatment to prevent the escalation of inflammation and disease progression.
The importance of contributing to IBD research
Nicole’s hope is that by sharing her experience, it will inspire others to participate in IBD research and encourage more funding for these types of initiatives.
“Our research contributions as chronic illness patients have so much potential to benefit others in the future. This study was fascinating, and it was truly a pleasure to participate in the research.”
She says by taking the daily surveys and performing the tasks, it made her feel like someone was paying attention to her struggles.
“It gave me an incentive to be strong, thinking that my challenges could be helpful to IBD research!”
Nicole’s final thoughts on wearable devices
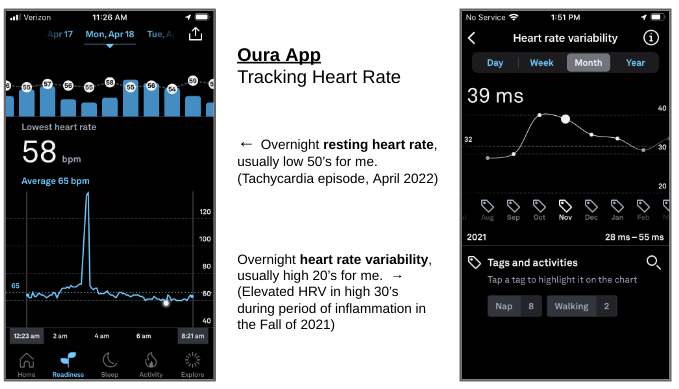
Wearable devices present a great opportunity for patients to monitor their health and provide feedback to healthcare professionals. “Since the study, I’ve continued to wear the Oura ring, and it’s been especially helpful to follow my progress as I rebuild and strengthen my body. Each morning I can check my readiness level to see how my heart has recovered from various activity levels. My sleep analysis has also been helpful for establishing a healthy sleep routine.”
The Oura ring has captured periods of strain on my body, and I can often tell when I’m getting sick with slight elevations in body temperature and resting heart rate. “During my Covid infection, the ring app even showed a fever spike along with elevated heart rate. I’ve also been able to monitor episodes of tachycardia with the help of the Oura ring and a KardiaMobile device, which is a single-lead portable EKG connected to a phone app. In addition, we have a pulse oximeter at home to monitor heart rate and oxygen saturation.”
With so much information to collect on our health, these devices can be overwhelming and anxiety provoking. “During the study, I was constantly monitoring my symptoms which led to a hyperfocus on my disease. Weighing myself each day also contributed to anxiety. Each time my weight dropped a little bit, I got worried and discouraged. The constant focus on weight can also contribute to issues with body image, and I’ve since decided to just weigh myself at medical appointments. For anyone considering wearable devices, it’s very important to keep moderation in mind.”
When we step out into the world, we need navigation tools. The same goes with wearable technologies. Soon, we’ll be able to use the data taken directly from our own bodies, during our day-to-day lives, to follow what is happening and help us to better navigate our own health paths. According to Dr. Friend, last year almost half of American adults were wearing some form of smart watch, and as of Spring 2022 more than 90% of smart watch users state they use health related apps to follow their health.
Interested in becoming a citizen scientist like Nicole? Learn about additional research opportunities:
In the future, Nicole plans to contribute to the Mount Sinai Million Health Discoveries Program which aims to understand how to treat different diseases in patients of all races, ages, and genders. She has also been invited to collaborate with Nutritional Therapy for IBD whose mission is to improve the lives and outcomes of patients with Crohn’s disease and ulcerative colitis through evidence-based nutrition.
Closing thoughts
The information collected from wearables can be a gamechanger for us as patients. Many of us call our doctors or go to the ER based on symptoms, but if we have remote monitoring via such devices, we could perhaps prevent this disease from spiraling. Kudos to Nicole and the many other research participants who are helping to push the needle and change the future of what it means to live with IBD.
“To me, that’s not just hope. That’s the future of managing this disease better and truly owning our Crohn’s or ulcerative colitis,” said Tina.
One in three people with inflammatory bowel disease (IBD) has iron deficient anemia. This common, but often underrecognized and undertreated extra-intestinal manifestation impacts so many of us. You may wonder why. The reason is three-fold.
First being that long-term irritation and inflammation in our intestines can interfere with our body’s ability to use and absorb vitamins and minerals properly. When our intestines don’t absorb enough iron, folate, B12 and other nutrients, our bodies are unable to create more red blood cells. Those with IBD are also at risk for blood loss—both visible and microscopic and we often don’t eat as much iron-rich foods. So, what can we do to boost our reserves and increase our energy? How as patients can we better advocate for ourselves to stay on top of screenings? This week on Lights, Camera, Crohn’s an in-depth look at anemia in both adult and pediatric patients and input from Dr. Alka Goyal, who recently co-authored a major study on pediatric anemia.
Symptoms to watch out for
As someone who was diagnosed with Crohn’s disease in July 2005, I experienced anemia long before my diagnosis. I often wonder if my anemia was a warning sign of the larger issue, my IBD. In fourth grade, I fainted on the teacher’s desk while waiting for her to look at an assignment. Throughout my life I’ve experienced light-headedness, weakness, black outs, and extreme fatigue. My symptoms were never addressed prior to finding out I had Crohn’s. A simple lab test would have shown all along. When I was diagnosed with IBD and hospitalized my hemoglobin was a 7. To give you an idea, people are given blood transfusions once they drop to 7 (or below). Throughout my 18 years with IBD, my hemoglobin was rarely ever in “double digits”—and I took over the counter iron supplements for years.
Once I had my bowel resection surgery in 2015, my iron panel slowly started to improve. It takes time. Last month, I had my “highest” hemoglobin since diagnosis, ever—12.9 (which really isn’t that high, but I’ll take it!). It’s difficult to put the fatigue caused by anemia into words, but you can physically tell such a difference when your iron panel is where it needs to be.
When you have anemia, you have less blood carrying oxygen throughout your body. The most common symptom is feeling tired or lethargic. Other symptoms include dizziness, headaches, feeling cold, pale skin, being irritable, and shortness of breath. Not everyone experiences symptoms, so it’s important as a patient to speak with your GI about making sure that when you get labs, an iron panel is part of the workup.
Screening for Anemia
Anemia screening is driven by patient symptoms and/or a care provider’s recognition of lab abnormalities. It’s important to note that anemia is not *just* a low hemoglobin, all the lab figures matter. With iron deficiency anemia (IDA), red blood cells are smaller and paler in color. Your hematocrit, hemoglobin, and ferritin go hand in hand. Ferritin helps store iron in your body. Iron deficiency anemia is the most common type of anemia and is caused by a lack of iron-rich foods, malabsorption, and blood loss.
Other types of anemia include vitamin deficiency anemia and anemia of chronic disease. Vitamin deficiency anemia is a result of poor absorption of folic acid and vitamin B12. My GI has me on daily folic acid. Luckily my B12 has never been an issue, but it’s worth a discussion with your care team. If you’re deficient, you can receive B12 injections. Diseases such as IBD and other inflammatory diseases can interfere with the production of red blood cells. When this happens anemia can often only be resolved once remission is reached or inflammation calms down.
In order to address the need for improved patient management, the Crohn’s and Colitis Foundation created the Anemia Care Pathway (ACP) to standardize clinical management of anemia in IBD. This pathway helps to identify high-risk patients so that timely intervention and care can be provided. The hope is that this pathway will improve patient outcomes and our quality of life. Patients are assessed based on the severity of their anemia and iron stores to determine the type of iron therapy (intra-venous or oral) that is best suited.
The importance of accurately diagnosing the type of anemia you have
According to the PubMed study, Management of Anemia in Patient with Inflammatory Bowel Disease, despite iron deficiency anemia impacting one third of IBD patients, “more than a third of anemic ulcerative colitis patients are not tested for IDA, and a quarter are not treated with iron replacement therapy.” While oral iron tablets are effective for treating mild IDA, it’s not for everybody. The study also notes, “it is important to recognize that ferritin is elevated in chronic inflammatory states and among patients with active IBD, ferritin levels less than 100 are considered to be diagnostic of iron deficiency.” Iron infusions have a solid safety profile and can be used to help boost your iron stores and prevent future iron deficiency.
While treatment goals are well-defined, selecting a treatment is often not as straightforward. The PubMed study previously mentioned recommends that all IBD patients with IDA should be considered for oral supplement therapy, whereas someone with clinically active IBD, or someone who is not tolerant of oral iron, with hemoglobin levels below 10 g/dl be given IV infusions therapy. While oral iron is safe and affordable, some people experience GI issues from oral iron, it can also increase inflammation and contribute to flares in patients who are not in remission.
“Though intravenous (IV) iron is substantially underused, it’s considered first-line treatment for patients with active disease, severe anemia, oral iron intolerance, and erythropoietin (a hormone secreted by the kidneys that increases the rate of production of red blood cells in response to falling levels of oxygen in the tissues.)
Anemia in pediatric IBD patients
The most common cause of anemia in children with IBD is iron deficiency. It results from chronic blood loss, poor absorption, and less intake of foods that are rich in iron due to poor appetite, food selection or intolerance. According to the World Health Organization’s definition of anemia, prevalence in the pediatric IBD population ranges from 44% to 74% at diagnosis and 25% to 58% at 1 year follow-up.
Anemia can be both a biomarker of disease activity and a subtle or debilitating extraintestinal manifestation. According to, Anemia in Children With Inflammatory Bowel Disease: A Positi… : Journal of Pediatric Gastroenterology and Nutrition (lww.com), “newly diagnosed children with IBD are more likely to have IDA in contrast to anemia of chronic disease. No significant improvement in the hemoglobin was observed when patients were assessed after 13 weeks of induction therapy with conventional drugs that included nutritional therapy, azathioprine, steroids, and 5-ASAs. Despite the recognition of anemia, fewer than half of anemic patients received indicated iron therapy.”
Dr. Alka Goyal, MD, Clinical Professor of Pediatrics, and Interim Associate Chief of Clinical Affairs at Stanford University of Medicine, co-authored this study on pediatrics and tells me the key message is that anemia is the most common extraintestinal manifestation in patients with IBD.
“More than 2/3rd of children with IBD are anemic at the time of diagnosis. The treatment of IBD alone does not resolve anemia, which can be associated with a variety of symptoms. Persistent anemia indicates a more aggressive disease course,” said Dr. Goyal.
Hemoglobin levels across genders and race
According to the study, hemoglobin levels are similar in preteen boys and girls; however, after menstruation, the cutoff hemoglobin in girls is lower than in boys and is even lower in pregnant versus nonpregnant women. The African American population tends to have lower hemoglobin concentration compared with Caucasians.
“Although the normal range of hemoglobin varies with age, gender, and race, a hemoglobin level below 10 g/dL is considered to be consistent with moderate anemia and below 8 g/dL as severe anemia, whereas in young children below the age of 5 years and pregnant women, a hemoglobin level below 7 g/dL is deemed as severe anemia.”
Dr. Goyal says it’s important to monitor anemia regularly in all patients with IBD.
“Anemia can be an early indicator of active disease or an impending flare of IBD. When the body has inflammation, the iron stored in the body cannot be metabolized to help manufacture more hemoglobin and additionally there is suppression of normal blood production, resulting in anemia of chronic disease.”
Other causes include vitamin deficiency, medication side effects, or breakdown of red blood cells due to other inherited or disease-related complications.
“Patients should be monitored not just by symptoms, but also by blood tests like complete blood count, Ferritin, and markers of inflammation like CRP every 3 months when they have active inflammation and every 6 months when patients are in remission,” Dr. Goyal explains.
Bringing a dietitian on board to help
Registered dieticians who specialize in IBD can advise patients and families about foods that contain iron naturally. The iron in meats is more readily absorbed than that present in a plant-based diet.
Dr. Goyal says another important concept is food pairing.
“With food pairing, iron-rich foods like spinach, kale, and Swiss chard are ingested with citrus fruits, melons, or vegetables like bell pepper, broccoli, beans, carrots, tomato, etc. Avoid simultaneous ingestion of foods rich in dietary fiber, soy, cereals, coffee, tea, and animal protein like milk, and eggs. Children should consume at least three servings of iron-rich foods like fortified cereals, red meat, tofu, etc. The recommended daily intake of iron in healthy children is 7-11 mg daily,” says Dr. Goyal.
Treating anemia in the younger IBD population
When it comes to treating anemia, Dr. Goyal has helpful tips. She says it’s important to recognize and treat anemia along with the treatment of IBD and vice versa.
Oral iron can be tried in mild anemia when the hemoglobin is above 10 gm/dl, preferably given with juice or citrus fruits.
Avoid taking oral iron multiple times a day or in high doses.
Brush your child’s teeth after taking liquid iron.
If your child experiences side effects including abdominal pain, nausea, or constipation, and/or has no significant improvement with oral iron, it is safe to give intravenous iron.
Timely treatment may save a blood transfusion. excessive unabsorbed iron is not healthy for our digestive system, so avoid overdosing on oral iron.
Patients with persistent anemia lasting for three or more years were noted to have a higher prevalence of more severe and complicated disease (stricturing and penetrating phenotype) with a greater need for surgical intervention.
Whether you’re an adult patient or a caregiver to a child or young adult with IBD, be mindful of the importance of keeping tabs on whether anemia is creeping in and hindering you or someone you loves quality of life. Have the conversation with your GI and make sure you are being vigilant and proactive about doing all you can to prevent, manage, and treat anemia.
This article is sponsored by Atticus. All thoughts and opinions are my own.
Navigating federal disability like Social Security Disability Insurance or Supplemental Security Income with inflammatory bowel disease (IBD) can be complicated and overwhelming. Those with chronic illness in the United States face roadblocks when it comes to being on the receiving end of benefits. Did you know 80% of people are denied the first time they apply for federal disability benefits and an astounding 90% are denied during the next stage of appeal?!
This week on Lights, Camera, Crohn’s we hear from Sarah Ashmore, an attorney at Atticus who has Crohn’s disease. The firm’s core mission is to “tear down barriers between people in crisis and the aid they need.” The social safety nets that exist are quite difficult to access. Atticus strives to help people in the IBD community and beyond get the assistance they deserve.
Juggling a flare and disability benefits
Since being diagnosed with Crohn’s disease in 2005, luckily, I’ve only needed to utilize short term disability through my former employer after my small bowel resection. In the moment, surgery recovery and dealing with Human Resources unexpectedly from my hospital bed was stressful. I went from speaking at an all-employee event to blacking out from abdominal pain in the bathroom and going to the hospital. When I left my work office in July 2015, little did I know I would not be healthy enough to return for more than two months.
At the time, I was completely naïve to short term and long-term disability benefits and how to get the support I needed to fully recover from surgery and maintain my position at work, while receiving a portion of my salary. I was like a fish out of water, learning as I went. I received my benefits and didn’t have issues, but that’s often not the case. Luckily, I’ve never needed to explore this further, so I did not need to utilize Atticus’ services.
Sarah’s experience
Sarah was diagnosed with Crohn’s disease in 2019 after dealing with symptoms for a year that left her feeling weak and powerless.
“At the end of that year, my symptoms were so severe that I had to take short-term leave from my job and move in with my family to help take care of me: I was so sick that I couldn’t wash my dishes,” she said.
Sarah applied for short-term disability while awaiting her official diagnosis. Thankfully, once she received her IBD diagnosis and was put on medication, she was able to return to her old lifestyle and work.
“I think one of the biggest roadblocks is that applying for benefits requires organization, persistence, and patience and trying to access them on your own while dealing with the types of symptoms from an illness or injury that make it difficult for you to work can be extremely hard. I needed that support from my family and friends while I was applying for short-term disability and, for many people, applying for Social Security Disability Insurance (SSDI) is a harder and longer process.”
What makes someone eligible for disability?
There are multiple options and they get confusing fast! You may wonder Which Benefits Do I Qualify For? Both short-term and long-term disability are often private insurance policies, while SSDI and SSI are provided by the government.
Short-term disability, like what Sarah and I accessed, is generally private disability insurance that you purchased or was provided by your employer before you became disabled. It normally lasts 3-6 months and pays a percentage of your salary. There are also five states that offer short-term disability separately from private short-term disability. Long-term disability is very similar to private short-term disability, but it often pays a smaller percentage of your salary and, of course, lasts longer than private short-term disability.
Social Security Disability Insurance and Social Security Income are both federal programs and, really, where Atticus can help.
“Both Social Security Disability Insurance (SSDI) and Social Security Income (SSI) are federal programs designed for people with a diagnosed medical condition that will prevent them from working for at least 12 months. The technical eligibility (such as how much money you make or your age) is different for each program, as is what a beneficiary gets. The medical eligibility for both programs is the same: you must have a diagnosed medical condition that will keep you from working (although you can do some limited work) for at least a year,” explained Sarah.
The rules around eligibility are quite intricate and there are exceptions, if you are struggling to work due to your chronic condition or disability, make sure to talk to a lawyer about your specific situation to see if you’re eligible for coverage.
For SSDI a person should generally be making less than $1,350.00/month at a job, be younger than 66, and have worked about five of the last ten years. If you are awarded benefits, you get Medicare and up to $3,300.00/month depending on your work history.
For SSI, a person should generally be receiving less than $841.00/month from any source of income and have less than $2,000.00 in assets (not counting things like your home) if you are single. The income and asset limits are a bit higher for married couples. If a person is granted SSI, they get Medicaid and up to $841.00/month depending on your sources of income.
You can apply for both programs at the same time, and, in some cases, a beneficiary can be on both programs at the same time.
“While there are general rules for eligibility, the evaluation is involved and there are exceptions to the rules, so please reach out to us at Atticus to determine your eligibility because we can offer individualized advice based on the specifics of your situation,” Sarah said.
Dealing with the disability denial and when to seek counsel
Getting an initial denial does not mean that you won’t get benefits or that you have a bad disability case. Don’t let this stop you from going through the process. If you get a denial, Sarah tells me you should request reconsideration within 60 days. This is when it’s optimal to get legal counsel involved. The lawyers at Atticus can walk you through the next steps in detail and get you connected with someone who can help you.
“Ideally, legal counsel would not be necessary for getting disability benefits but, unfortunately, many people do need it. Although having a lawyer can be helpful at any stage of the process, if you are at the hearing stage, you are three times more likely to get benefits if you have an attorney or legal representative with you. Good lawyers will have the experience to understand what the Social Security Administration is looking for when determining whether to grant benefits: they should understand what documents you will need and what questions you will need to answer to help your application,” she said.
Why Atticus is completely free to clients
All SSDI and SSI attorneys and legal representatives get paid on contingency, so they only get paid if they win their client’s case. If they don’t win, the attorneys (and Atticus) get nothing. The federal government actually sets how much an SSDI/SSI attorney can get paid so it is the same across the board: 25% of only the first check that someone gets from the Social Security Administration should they win their case, capped at $7,200.
“Atticus gets paid by the attorneys that we refer a case to the same way the attorneys get paid by the Social Security Administration. If the attorney or legal representative wins, we get 25% of whatever the attorney got from SSA. That is never passed on to the client (so the amount of money taken out of the client’s first check is always the same). Getting paid this way allows us to provide free advice and resources to folks we speak with whether or not they are eligible, want an attorney, or end up using our services,” Sarah explained.
Click here to connect directly with an attorney at Atticus.
Coming to grips with the emotional struggle of realizing you need help
The stress of life and career can make this entire ordeal feel endless. As we all know it can be humbling to have to express how sick you are to those who often don’t understand the severity and complexity of IBD. There’s no need to suffer. There’s no need to be a martyr. Recognize when you need to wave the white flag and realize needing disability, whether SSDI, SSI, or short term does not make you less than your co-workers or peers.
Much like myself, Sarah and I don’t consider our Crohn’s a “disability” per se, but we did know that we could not work or live the way we were when we needed support.
“It’s a common theme we hear a lot from our clients. Especially if they don’t identify with the term ‘disability;’ or if someone feels like they are taking a government hand out after spending years working hard to make it on their own. SSDI is forced insurance designed for people who can’t work due to an injury or illness. Most workers have been paying into it every time they get FICA taxes taken out of their paycheck. It is designed to be there when you need it. If you would feel comfortable using private insurance, you should feel comfortable using SSDI. Asking for help can be hard but doing it can be so good for you in the long run,” she said.
Demystify the process of applying for disability benefits
Atticus’ goal is to get as many eligible people connected with federal disability benefits (SSDI and SSI) as they can.
“We function as the equivalent of a patient navigator for anyone in the disability application process. We are like a primary care physician, but for legal issues: someone will often come to us and say something like “I have this medical condition or had this injury; I can’t work anymore, and I am not sure what to do next,” Sarah said.
When someone calls Atticus for assistance, they will speak with an intake specialist who can help determine what benefits they are eligible for and recommend next steps.
If you want to continue the application process on your own, Atticus can provide resources and input on next steps for applying (for example, letting folks know they should get specialist care and then call back or apply).
“We give out our Guide to Applying for SSI to folks doing their initial SSI application. If they are not eligible, we can often point them in the right direction for other resources they may be looking for (for example, help with housing or signing up with Medicaid).”
If you are eligible and want legal help for the process, Atticus connects you with a legal representative or attorney who they think would be a good fit based on the specifics of their case, such as: location, case stage, medical condition, etc.
“We only work with attorneys that we have hand-picked and vetted. Those attorneys and legal representatives don’t pay to join our network or sign up for a membership with us; we thoroughly vet every lawyer and representative we work with and form relationships with only those we trust and respect,” Sarah explained.
Testimonials from IBD warriors
Jeremiah: “I have been dealing with IBD for 13 months. Atticus was able to help me with my legal issues while I was too sick to fight for my own rights. I was able to receive the best representation while becoming healthy again. They fought for me and today I am receiving SSI and disability for my condition. These programs are dedicated to people like us, who are suffering. Now I do not have to fear the future or what I will do when I flare again. I’m able to focus on my health and live my life. I urge anyone to ask for help, it’s out there. Atticus is one phone call or e-mail away.”
Joni: “I was diagnosed with Crohn’s almost 2 years ago, but lived with IBD for years not knowing what it was. Treatment is not 100% as I still tend to get flare ups that usually put me in a hospital, missing work. With that and other health issues, I decided to apply for SSD, being denied twice, I reached out to Atticus to get legal help/representation. I emailed them and within an hour they reached out. By the end of the day, I had an attorney representing me. They’ve been a great and fast help! Very professional!”
The article discusses how teenage girls and young women post upsetting footage and commentary on social media about their “invisible illnesses” to gain attention and “likes” and bashes “Spoonies” for giving people a behind-the-scenes look at the reality of their chronic condition. Hold UP. As someone who has lived with Crohn’s disease for more than 17 years, who is patient advocate, and works tirelessly to empower and educate others about life with inflammatory bowel disease, by candidly sharing on social media and through my blog, I find it incredibly disheartening and worrisome that a story of this nature is in circulation.
The ableist mentally shines bright
How disappointing that a “news outlet” takes the time to belittle people who are battling debilitating and unpredictable illnesses and sharing their struggles not for attention, but for support and camaraderie. Unless you have a chronic illness, you don’t have the slightest clue about what it’s like to wake up each day and not know what the next hour is going to bring. Unless you have a chronic illness, you can’t begin to imagine the stress, worry, and anxiety that comes along with diseases that limit us and often set us up for failure when it comes to trying to keep up with the rest of society. Unless you have a chronic illness, you have no idea how isolating and overwhelming it can be to be young and unhealthy, different than your peers, while fearing what your future is going to hold. Unless you have a chronic illness, you can’t fathom what it’s like to juggle multiple specialists, appointments, medications, insurance, specialty pharmacies, and screening tests… just to survive. It’s imperative those with invisible chronic illnesses share their stories and show others that what they are going through.
Articles like this are extremely damaging and triggering to those who suffer in silence, the newly diagnosed, and furthers the fear of what could happen if you decide to come out of the “proverbial closet” publicly and share about your health struggles.
Patient communities NEED you to share
When I was diagnosed with Crohn’s disease at age 21 in July 2005, Facebook hadn’t even been out for a year. No one was going on social media and sharing they had a disease. I felt like I was on a desert island, all alone with a diagnosis that flipped my world as I knew it upside down. As an aspiring TV journalist, two months out of college graduation, I had no idea how I was going to function and follow my dreams. Nobody wants a chronic illness diagnosis. Nobody asks for this. Nobody wants to suffer so they can have “likes” and attention on social media, trust me. Never in my life have I seen people encouraging others to lie to their doctors about getting the diagnosis that they want.
With diseases like inflammatory bowel disease, this is not something you can fake. A diagnosis is received after scopes, scans, and labs, reflect that this is in fact the case. You don’t just walk into a doctor’s office and say you aren’t feeling well and exaggerate abdominal pain. It’s not a competition of who is “sickest,” people are sharing what they are going through for a variety of reasons. When someone is in a hospital bed, they may share for support, advice, and prayers. When someone is gearing up for a colonoscopy, they may share so they can get tips for easing the prep or coping with the worry of the unknown. When someone is pregnant and flaring, they may share to hear from other IBD moms who have been there before. The examples are endless. Patients are not haphazardly concocting up social media content and lies about their medical struggles to see who is going to get more attention. This is not “attention” people want.
By claiming we share for attention it goes against everything we stand for and belittles the lifechanging work patient advocates are doing to support and comfort their peers. As a patient advocate myself, I do so much behind the scenes “work” to guide those in the IBD community and help them every step of the way. It’s about helping others from the bottom of your heart and being the voice you needed to hear upon diagnosis and through milestones in life. It’s genuinely finding connections with those who are not just strangers on the internet, but quickly become your closest confidantes and resources. Since coming out and sharing I had Crohn’s disease in 2015, I went from having family and friends who didn’t have Crohn’s offering me support, to an army of thousands of members in the IBD family I can rely on who “get it” and are available right at my fingertips. THIS IS PRICELESS.
Sorry not sorry for the “upsetting content”
The article states “thousands of teens are banding together on social media as part of the movement” to support the Spoon theory. Imagine what it’s like to be living this reality versus just having to view a post on social media. Can you pause and put yourself in the hospital bed or on the operating table or on the couch about to do a painful injection and think about the pain and suffering those with chronic illness are forced to endure just to survive like the rest of society? It’s privileged to lash out against those who are doing all they can to show others what their lives consist of rather than bottling everything up—THAT is damaging, THAT is not healthy. Must be nice to have the privilege to keep scrolling and living your healthy life and only see a few seconds on your screen.
Should chronic illness patients be smiling as they’re suffering in hospital beds? Is it not normal to be crying when you’re worried and scared and can’t help but get emotional with all that’s on your shoulders? No one is complaining. It’s the stark reality. It’s heavy. It’s no surprise that more than 30% of people with IBD also deal with mental health issues and anxiety because life with the disease is so heavy.
It’s not about the money
Can we all pause and laugh about the fact the article claims those with chronic illness post on social media for the money. Hilarious. Get a grip. Even as a well-established and trusted “health influencer” within the IBD community, when companies reach out to me, it’s often to try products, not get a paycheck. When I am paid for my advocacy work it’s working diligently like your job as a journalist to write articles, create social media copy, and educate others about what my life is like with Crohn’s. I get compensated like any other human for using my skills and expertise, along with my precious time and energy, to sit on advisory boards and offer input and perspective for marketing and awareness campaigns. My job is not to be a patient, my “job” is to take what I’ve learned and use it to make a difference and help others.
This is not for show. Digging up past medical trauma and flare ups is not enjoyable. If businesses and pharmaceutical companies want to collaborate with chronic illness patients, they should be paying us for our invaluable intel and understanding. The article states patients have adopted “victim mentalities” …wow…and “communities of grievances” … when medical professionals are out of line or treat patients without respect, you better believe your ass they should be called out. How is change going to happen and life for chronic illness patients going to improve if we sit quietly. Be loud, my friends. Don’t allow articles like this to stop you from sharing. We NEED your valid experiences. You deserve to be heard. You matter. Even though the rest of society may be rolling their eyes or trying to stop us, they won’t, and they can’t.
I don’t want to go back to 2005 when I was all alone in my struggles with Crohn’s disease. I want to stay in 2022 when I can post whatever I want, whenever I want about my trials and triumphs as a woman, mother, and wife with Crohn’s disease and not fear judgement. Sometimes I’m thriving, sometimes I’m struggling. It’s vital that those with chronic illness continue to honestly share their stories on social media to provide clarity, education, and connection to those who relate wholeheartedly.
So, dear Emma, from one journalist to another, please start sharing stories that matter—don’t go after stories for attention or follow the adage, “it bleeds, it leads.” Seems like you are the one going after the likes. You should know better.
Sign the Petition
There has been outrage in the chronic illness community about this article—many feeling triggered and upset by the accusations and the claims made about Spoonies. An online petition has been created to have this Daily Mail article taken down—you can sign the petition by clicking here.
Life with IBD impacts our careers in many ways. Our disease can often dictate what path our future takes. As students, teachers, and families gear up for another school year, I thought it would be interesting to hear from educators who have IBD about what it’s like to lead a classroom while living with an unpredictable chronic illness. This week on Lights, Camera, Crohn’s hear the inspiring stories and perspectives of four unsung heroes who don’t allow their IBD to rob them of their career aspirations.
Sarah Rife has been a teacher for seven years, she’s also an IBD mom and an ostomate. She’s currently teaching eighth grade math in the Chicagoland area, but previously taught high school Geometry and Algebra.
“I have taught through many highs and lows Crohn’s wise. For the first 5 years, there wasn’t a single year that I didn’t use every single sick day I had (and then some unpaid days). I believe four out of five of those first years, I had at least one hospitalization where I missed consecutive days, as well. In this time, I was on four different medications and tried a clinical trial.”
While this was going on Sarah says she rarely ate at school and if she did, she stuck to 3-4 “safe foods” to help get through the day.
“I constantly taught with an escape plan in the back of my mind. You can’t just leave a room full of 28-32 kids sitting unsupervised, so I constantly had to think about things like ‘Who will I have cover my class?’ ‘What if I am gone more than 5-10 minutes?’ ‘What can they work on that they will know how to do if I have to step out in the middle of teaching them something new?”
Sarah is open about her IBD with students and their families and says having IBD has made her a more compassionate educator since she understands when students need to miss school.
“When I was younger, I was the student missing multiple days of school. I remember the things that some of my favorite teachers did that helped me to not stress when I felt like I had mountains of missing work. Whenever I have a student gone for health reasons, physical or mental, my standard answer when they come back is “Worry about everything else first, and then I’ll talk to you about what we can do to bring you up to speed in math class. Don’t stress, I will work with you on it.”
One year while being evaluated by her principal during a drop-in visit. He walked into her room, sat down, and started typing. He was aware of her Crohn’s, but Sarah panicked when she knew she needed to make a mad dash to the bathroom while he was in her classroom observing her.
“I ended up going over to him and asking “I really need to step out and use the bathroom. Do you want me to grab someone like I usually do, or do you just want to watch them since you are here” He agreed to watch them, and I ran out to go to the bathroom. Whenever I had to step out, I was also conscious of what time it was. This time, there were about 30 minutes of class left. In my head, I needed to get back ASAP because THE PRINCIPAL was in there and he was supposed to be observing me. When I heard the bell ring and I was still on the toilet, I panicked – I’m talking instant tears. I was able to finish and tried to hurry back to my room. My path crossed his on the way back and I started to say, “I’m sorry, I didn’t know I would be that long.”
Sarah says her mind was racing with crazy thoughts about her abilities as a teacher and what she was capable of. The principal could see she had been crying and more tears were starting to fall, and he interrupted her and said, “Sarah, I am not worried about it. This is your third year here and we know this happens. I am worried about what I see when you are able to be in the classroom and what I saw meets and exceeds our expectations. Please don’t worry about it.” – This reassured her so much more than even he will ever know, but the story replays in her head every time an administrator pops in her room for an unannounced observation – even 4 years later.
When Sarah taught high school, she was nowhere near remission, forcing her to be extremely transparent with her students.
“I told them that I had a disease called Crohn’s and that in a nutshell, my immune system was attacking itself, specifically my intestines. They knew that me having to step out of class and disappear to the bathroom was a possibility and witnessed it multiple times a week, sometimes in the same class period. They were also aware that often these bathroom breaks would result in pain, nausea, and exhaustion.”
Whenever Sarah would have an episode, she says the students went above and beyond to be empathetic and understanding.
“I had students volunteer to work out examples on the board so I could sit down, and they were extremely good at switching gears and changing the plan if I needed to do something with less walking around, standing, or talking – for example work on a worksheet instead of doing notes or bringing questions to me at my desk over me walking around offering help. I really do think high school students are more resilient and compassionate than people give them credit for.”
Since her ostomy surgery, Sarah’s life in the classroom has changed for the better.
“I feel like a completely different teacher. My energy isn’t nearly as much of an issue, I can teach without constantly having an escape plan or worrying how long I’ll be stuck in the bathroom, I can eat lunch at school like a normal person, without worry or only packing the same 3 things, and for the first time in my teaching career, I had paid sick days left at the end of the year. I had a chance to worry about the content I was teaching first and my health second, which I had never been able to do in the past.”
Sadly, this past week, Sara’s ostomy leaked while she was in the middle of teaching 30 thirteen-year-old students. Luckily, she works less than one mile from home so she yanked her shirt down as far as it could go and told the admin she’d be back in 15 minutes.
Sara Margolin of New York has been a professor of psychology for 15 years, with a focus on neuropsychology, cognition, and aging. She says her experience with ulcerative colitis and two other autoimmune conditions has made her more understanding toward her students. Sara says, “Robin Roberts said it best, “everybody has something.” And she’s right. I’m not the only person with a chronic illness. Many of my students struggle or someone they love struggles. Understanding that they deserve the compassion that I wish to have has only made me a better professor.”
Sara has had to leave the classroom on multiple occasions to urgently use the bathroom.
“I will either quickly show a film if I have one at hand or pretend to get a call from my children’s school and “need to leave to take it.” But in my smaller classes, where the discussion leads us there — in the discussion of medical trials, medications for chronic illness, or psychological issues stemming from chronic illness, I’ve discussed my condition. And there have been a handful of students over the years who have been diagnosed while in my class, and I share with them that I understand what they are going through. We bond over that.”
Now that classes are back to in person this fall, she has some concerns knowing she is not fully in remission and not able to teach remotely anymore.
“When I was teaching at home, I had a time or two where I turned my camera off and taught from the bathroom…. EEK! … and knowing that I may be in the position to need to do that but not be able to is nerve wracking. But I know that my colleagues will fill in for me if I do need them to.”
Madison Laspisa of New York has taught fourth grade for four years. She was diagnosed with Crohn’s disease in June 2020, during her first year of having her own classroom. Not only were schools shutting down when her severe symptoms began, but she was dealing with school closures and remote teaching, on top of being diagnosed with a chronic illness.
“My life was flipped completely upside-down to say the least. I was truly devastated at everything that was happening around me and to me. My first year in my own classroom should have been the most memorable part of my career (in a good way), but I sadly cannot say that. My life changed before I had a minute to truly process what was happening. However, since we were forced to stay home because of the Covid-19 pandemic I had the availability to see doctors and get procedures done as needed. Had it been a normal school year I would have had to take a leave of absence during my very first year of teaching.”
Since then, Madison says her IBD has impacted her experience as an educator in more ways than she’d like to admit.
“Aside from needing to take days off to receive my infusion, there have been days where I needed to take a last-minute half day because I desperately needed to see my doctor. At times, this can leave the main office scrambling to find a substitute for my class with an already existing shortage. Not to mention the schedule change my students have to now adjust to with their teacher leaving mid-day.”
Madison says the toughest challenge for her is the amount of time she needs to take off to receive her medication and meet with her care team. She does her best to schedule doctor appointments after school hours, but sometimes it’s not realistic. Right now, she receives her biologic every four weeks, which was changed from every eight weeks.
“This required change in my treatment plan will now require me to miss time in my classroom with my students twice as often. It’s not as simple as “taking a day off” as it is very time consuming to create thorough substitute plans on the days, I am absent. It makes me feel like I’m a “bad teacher” because I have to take time away from my students and classroom. I feel guilty when I’m making substitute plans because I know I am going to be absent the next day and my students have no idea.”
Madison says the weight of the unpredictability of her Crohn’s makes her anxious. She worries about waking up one morning and not being physically able to go into work and do her job.
“I love what I do with a passion and anything that can hinder my ability to do my job to the fullest breaks me. Having the summer months off allows me to slow down and take a break from my rigorous work schedule. In a sense, it provides me with some relief because I know being home, I don’t have to worry about missing work because of my IBD.”
Madison hopes that if someone reading this article aspires to work in education, that they don’t allow their IBD to deter them from taking the leap.
“Teaching and being with my students is my escape from my reality with IBD sometimes. IBD has robbed me of so much and I refuse to let it rob me of my dream job. Do not let IBD dictate what you can and cannot do. Being a teacher and having IBD are both full-time jobs and can be extremely overwhelming at times but loving what you do makes all the difference.”
Krista Deveau has been a teacher in Canada for seven years, she recently became a mom and is an ostomate. She currently teaches kindergarten but has also taught third grade and worked as an intervention specialist helping students with literacy and numeracy. She started her teaching career three months after having a bowel resection surgery. She ended up landing back in the hospital three months later, weighing under 100 pounds, in one of the worst flares of her life.
“My GI team told me that I had to work part time if I was able to or else my chances of being back in a hospital bed were quite high. Working part time has really given me a work- life balance where I can take care of my health and myself and also focus on my career.”
Prior to receiving her ostomy, Krista tells me it was difficult to teach, as she was having accidents almost daily and was vomiting in a garbage can outside of her classroom. During her first year of teaching, she had a meeting with an administrator after school and happened to have an accident. Krista had forgotten to bring a change of clothes.
“I was so embarrassed that I stayed behind my desk all afternoon so students couldn’t smell me. I cleaned up at recess as best as I could. After school I went to meet with admin and told them I had to leave because I had had an accident and didn’t have a change of clothes. I had already told them about my situation and how I was experiencing incontinence, so it wasn’t a big deal, but I was humiliated.”
Krista says teaching is a stressful and demanding job—and that it’s important to be honest with your admin team so there are no surprises along the way.
“Make sure to take care of yourself. Don’t stay late every day. Work smarter, not harder. Collaborate and share plans with other teachers so you aren’t reinventing the wheel. Lean on your coworkers. Find one good coworker friend that will have your back. Don’t work on weekends. Don’t take on too much of the extras, it’s okay to say no. Try to have a healthy work life balance. And find a school/school board that’s a good fit for you and where you feel supported.”
Helpful Tips for Educators with IBD
Be flexible and rework plans, not just in terms of being absent, but also what you can do instead if your energy level is too low to actively teachon your feet or if you need to talk for an hour straight multiple times a day.
For example: Create PowerPoint slides where every single step of a math problem animates itself with the click of a button so you can be sitting instead of standing up, exerting energy.
Teaching is a pleasant distraction. Teaching enables you to get your mind off your IBD and do what you love. Regardless of what you do professionally, your IBD is going to be a part of you, why let it take more from you than it already has? Enjoy the thing you can enjoy.
Make the appropriate accommodations for yourself. Once you are hired or work in a school district, provide school administrators with medical documentation as to why you are unable to work on a certain date. At the start of the school year, it can be helpful to turn in a letter stating your treatment plan along with a request to use the bathroom when needed stating your medical condition. Typically, teachers use the bathroom on their scheduled breaks, but this accommodation allows that in the event you need emergency use of a bathroom, someone will need to cover your class at any given time. This type of documentation for my district must be renewed every school year.
For example, if a typical teacher instructs five classes with an hour to plan and a 25-minute lunch, split with a 25-minute study hall, inquire about keeping your schedule consistent year after year and teaching two classes, then having a plan period, teaching two more classes, and then a ‘duty-free lunch’—meaning you get the entire 56 minutes for lunch, instead of having a study hall to give you a buffer for a bathroom trip along with minimal interruption to other classes.
Request a classroom close to a bathroom and department office so that there are people nearby in case you need someone to cover your class on a moment’s notice.
Try not to fear the worst. Being hospitalized is beyond your control and whether you have a chronic illness like IBD or not, life happens, and co-workers will need help from time to time. Rather than stress about who gave up what time to help you, focus on how to pay it forward and help other teachers when you feel well and when someone else is in need.
Teaching takes a village. Everyone is more than willing to help you out if you let them. Besides, it all becomes so much easier when you don’t feel like you must hide such a huge part of who you are. The sooner you realize people are willing to help you and you don’t have to try and keep it hidden, the easier teaching with IBD becomes.
It’s been 6,207 days since my life changed forever. On July 23rd, 2005, I was diagnosed with Crohn’s disease at age 21. Since that time, I’ve evolved and changed in ways I may not have if it weren’t for my IBD. After living in silence with my condition while working in television news for a decade, I decided to use my love for storytelling and speaking to be the voice I needed to hear upon diagnosis as I navigated the many crossroads of young adulthood (finding love, a fulfilling career, and having a family).
July 23rd also marks the day I launched my blog, Lights, Camera, Crohn’s. Since 2016, I have shared fresh content, every single Monday (sometimes even twice a week!). 336 articles on my site alone. More than a quarter-million visitors and more than 387,000 views.
It’s been a labor of love and a mission project that continues to fill my cup and implore me to constantly want to learn more and shed light on topics that are often not talked about. Every day of every week since my blog began, I’m constantly thinking about story ideas, topics of interest, people to interview, ways to word content, images that are needed…the list goes on.
This photo was taken at a wedding July 23, 2016, right after I pressed “Publish” on the first Lights, Camera, Crohn’s article. I found out I was pregnant two days later.
The weekend I started my blog in 2016, I was one month into married life and found out days later I was pregnant with my first child. Since then, I am now a stay-at-home mom of three children (ages 5, 3, and 1). Life has gotten way more hectic and busier with each year that passes, but I’ve held tightly onto fulfilling my promise to the patient community, and to myself, to deliver new content each and every week. I’ve been organized through the years—often having an article written days before my Monday deadline, but this past year, with another baby added to the mix, it’s been more of a stress on me. I’ve spent many Sunday nights finishing my articles. At times it’s felt like a lot to juggle. I haven’t wanted to let anybody down, including myself. And I haven’t wanted my content to start lacking in any way.
Don’t worry, Lights, Camera, Crohn’s is not going anywhere
My blog has grown into more than I ever thought possible. It’s so rewarding to know my words have helped comfort and guide so many in the IBD community. I need to cut myself some slack and give you a heads up that moving forward there may not always be an article on Mondays. It pains me to say that, but at this point in my life, in this season of IBD motherhood, I need to start taking time to rest and relax. Since having my third baby last summer, I get my kids down for the night and START to work around 830 pm. It’s just constant. I truly rarely get a break. I’ve been in remission since August 2015, and I don’t want the stress to get the best of me.
You may not be aware—but my blog is only one aspect of my advocacy work. I also spend a great deal of time working with digital healthcare companies, patient-centered non-profit organizations, sitting on advisory boards and patient engagement teams, communicating with patients in need online and over the phone, and do freelancing work on the side, all without childcare.
I laugh as I write this because I already have three articles lined up for August…so there will be months where there IS an article every Monday. Just not always. My commitment and desire to serve as a patient leader is not waning in any way—I just want to be honest with you, my loyal readers, that this mama needs to lighten the load and take a little self-imposed stress off my shoulders.
I started contemplating this a few months ago, and almost changed my mind this week about sharing, but it’s time. We had an AMAZING 6-year streak of constant new content. I’m excited to see what this coming year brings in the way of patient stories, research, and perspectives. Having extra time to work on articles will really allow me to do more special reports and expand my “IBD Motherhood Unplugged” and “Patient Experience” series.
Thank you for giving me so much to talk and write about, always. There are endless topics that need to be brought to the forefront and I love providing a platform for others to share their journeys and experiences with the community. As always, please reach out if you have a story idea you want me to cover. Lights, Camera, Crohn’s has truly evolved from being a blog about my IBD experience to an award-winning and well-respected site that has highlighted hundreds of different patient stories and physician perspectives—and I love that. There’s no greater compliment then when I hear a gastroenterologist uses my blog to educate their patients.
Excited to see what 2022-2023 brings! Thanks for the love, support, and understanding and for making the first six years of Lights, Camera, Crohn’s what it was.