Kids are more intuitive than we tend to give them credit for. They are always watching us and even before they’re able to speak in sentences they have an innate sense of empathy and understanding. As an IBD mom of three, whose kids are almost 7, 5, and 2.5, I’ve started to think more lately about how to explain my Crohn’s disease to them in a way that will educate them, without scaring them. It can be a difficult balance.
I know my older two know mama gives herself shots, often needs to run to the bathroom, and gets “tummy aches” but I haven’t yet dropped the term “Crohn’s” or “disease” to them quite yet. It can be hard to explain and sometimes when I start trying to share more, I feel like it’s still going over their heads. Their concerned eyes when I’m in pain and how they watch me do my Humira injections is a reminder to me that they are aware something is going on. As we potty train my youngest, he commends himself for going on the potty by saying he’s “just like mama” …ah, what a great analogy!
This week on Lights, Camera, Crohn’s hear from several IBD parents about how they transparently communicate their experiences with Crohn’s disease and ulcerative colitis. It can be a fine line educating and being open, while also trying not to overwhelm and scare kids. I’ve found it extremely helpful tapping into the community and gaining input from others and I hope you do, too!
Helpful Guidelines for Navigating the conversation with your kids
Choose the right time. Pick a time when you won’t be interrupted and can focus on the conversation. Ensure it’s a moment when you and your children are feeling calm, at ease, and open to discussion. My recommendation as an IBD mom would be to have this conversation on a “feel good” day—rather than when you’re flaring or in the hospital.
Prepare yourself. Decide in advance how much detail you want to share based on your child’s age and maturity level. IBD is complicated, be ready for a range of emotions including sadness, fear, and even anger.
Use age-appropriate language. Explain your IBD in a way that is understandable to your child. Avoid using confusing or technical terms. For younger kids, it might be helpful to compare your illness to something they already understand.
Be honest but reassuring. You can be transparent and truthful, but also reassure them about all you do to manage and control your IBD. Empathize with the aspects of your daily life that won’t change, to provide them with a sense of stability and comfort.
Focus on practical impacts. Explain how your IBD might affect your daily routine or activities with them in a straightforward way. Use examples such as—“Mommy’s Crohn’s can be unpredictable, I may say we’re going to the park, but then I don’t feel well so we have a movie date and snuggle instead and plan to go to the park another day.”
Encourage questions. Allow your children to ask questions and express their feelings and know this will be an ongoing conversation throughout life. Go into the conversation without expectations. It’s ok to admit if you don’t have all the answers. You can explore some of the questions together.
Provide continuous support. Let your kids know that it’s okay to have and express their feelings about your IBD. Offer them ongoing support and reassurance. Let them know they can always come to you with questions or concerns at any time.
Seek support when needed. Consider enlisting the help of a therapist or a counselor, especially if you or your children are struggling to cope. Joining support groups and tapping into the online patient community and connecting with fellow IBD families in similar situations can be beneficial.
Keep the conversation going. Check in with your children regularly about your IBD and how you’re feeling. Be casual about it. Share when you see an opportunity to teach or calm fears that your kids may be internalizing.
Highlight the positives. While acknowledging the challenges, also focus on the positive aspects, such as the strength of your family unit or the support you have from friends and community. I always tell my kids when I’m doing my injection that mommy is strong, and we can all do hard things.
By approaching the conversation with honesty, sensitivity, and openness, you can help your children understand and cope with your chronic illness in a healthy way.
My 2-year-old trying to make me smile during a rough day in the bathroom.
IBD as a family disease
There’s a common saying in our community that IBD is a family disease, in that whether you have Crohn’s or ulcerative colitis or not, if someone in your nuclear family has it, the disease impacts your living experience in some way.
Emily and her husband have IBD and so do their three daughters, so discussions about IBD are frequent in their home since it’s a living reality for all five of them. She tells me the conversations tend to fall in one of the following categories:
1) Explanations of IBD details, procedures, surgeries, or diet needs for a member (or members) of the family.
2) Discussions to calm anxieties in one child about the presentation of IBD in themselves or in another family member.
She says the second category tends to be the more challenging conversations, by far.
“In the first category, we tend to stick to factual, age-appropriate explanations. For example, when our five-year-old needed to know about scopes and surgeries, we explained that a specific family member has “belly problems” and the doctor is helping by taking pictures of their belly and fixing the parts that were causing trouble,” explained Emily.
As the girls have gotten older, Emily says they add details about how the doctors do different procedures – always led by their child’s level of interest and desire for the knowledge.
“We are always honest about pain or discomfort related to medical procedures. Many things are NOT painful, and we want them to trust us that something does not hurt if we tell them. This has served us well. When surgery was needed for one daughter, we discussed how she would be sore afterwards, but we had ways to help the pain until it would subside. This was undoubtedly a challenging time for us, but our daughter did amazing,” Emily said.
As Emily’s girls have gotten older, as a preteen and teen, they understand more about their parents,’ and their own, IBD. They have lived through surgeries and many medical procedures in their family. Emily says now the more challenging conversations have started, related to knowing the possibilities around IBD.
“For example, I had a colon perforation following a routine monitoring scope for my IBD. It was a rare event that we are all warned about prior to a colonoscopy. It resulted in a more significant repair surgery and several days in the hospital. My daughters are old enough to realize that they also have scopes regularly and we had to have some discussions about the chance that the same thing could happen to them. It was challenging for our family for a few rounds of scopes!”
Emily says they addressed this topic mostly by focusing on the “helpers” as the iconic Mr. Rogers would! Yes, bad things can happen, but she reminded her daughters that they are so lucky to have doctors and medical professionals to “fix” these problems. She reminds them that they are lucky to have family and friends to help when they are not feeling well. She also talks about how they are lucky to have each other – who understand the ups and downs of this disease.
“This narrative has gotten our family through many challenges! I talk with my oldest daughter much more now about the details of her IBD. She is a teen and has had more than her fair share of IBD troubles. She has watched me deal with my challenges too. We are open with each other about the negative parts, and our frustrations having to deal with IBD. It is a double-edged sword to have her growing up! On the one hand – I hate that she is old enough to really understand the negatives. But she is also turning into an amazing young woman who is one of my closest confidants with this disease. We understand each other’s highs and lows like most cannot. We supported each other in challenging times and celebrate together for each win!”
Sari says she bought a couple of children’s books that feature a caregiver with chronic illness.
“One of them is titled ‘Some days’…it’s about a mom with multiple sclerosis, but it works for IBD, too. It goes over how some days are more exciting and others are simpler more restful days. If there are other kids’ books people have found, I’d love to hear about them!”
Kate also has a book by someone with Crohn’s, but says they’ve also always been very honest and open about it with her son.
“I always worried he would tell people too much, but I’ve found he’s incredibly respectful and it has made me feel less shame in my body because I talk to him so positively about it. Especially the perianal disease, which has been really hard to talk about with people. My son is six and understands my immune system attacks my digestive tract. We also have a puzzle of the body we have played with for years and he knows the colon, intestines, rectum, etc. because of that.”
Becca says one of her favorite memories as an IBD mom is when her daughter was learning body parts and said, “Mommy and I have vulvas, Daddy has a penis, Daddy and I have butts, and mommy has a bag!” She also often asks to see her “cut” on my belly (c-section scar), but I constantly remind her that she shares her “cut” with a lot of intestine.”
Becca also says for the longest time her daughter thought that EVERY mom gets an ostomy bag when they’ve had a baby.
“She didn’t realize I had mine for four years before she was born!”
As an IBD Dad, Brandon said he stumbled upon a video series when his son was around age five that provided a solid explanation. At the time his son had a broken arm.
“The video explained people have booboos you can’t see. I explained that I had what the girl in the video has. Nowadays, I show both my boys’ photos from my colonoscopies.”
You can watch the video Brandon showed his son here.
Here are additional books about chronic illness that others have recommended:
Did you know within the next decade, one in three IBD patients will be over age 60 and that right now, adults over 60 make up the greatest portion of the IBD population? As someone who was diagnosed with Crohn’s disease at age 21, who is now 40, I’ve started to think more about what managing and living with IBD will look like as I continue to age. Managing IBD in older adults is complex and requires considering each person’s individual risk of complications and co-morbidities.
This week on Lights, Camera, Crohn’s a look at the research that’s available and what we can expect as an aging patient population. Before we get started, it’s important to note there are two groups—adult-and-pediatric onset IBD who are getting older and then a group of people who are diagnosed later in life (after age 60) referred to as “elderly-onset IBD”. Every review I saw online uses age 60 as the benchmark to differentiate these two groups. Elderly onset makes up about 10-20% of patients who are newly diagnosed with IBD.
Unfortunately, there’s limited data and studies that have followed patients for 20-plus years, so we don’t know a ton about how aging impacts patients who were diagnosed as pediatrics or as younger adults compared to those who are in their later years. While there’s a well-known belief that IBD can “burn out” as we age, meaning that symptoms for some quiet down, that is of course not the case for all.
Considerations when treating IBD in older age
Have you ever talked to your GI about how your IBD will be managed as you age? I know I haven’t. I feel that there’s so much to focus on in the “now” it can be overwhelming to think about how we’ll take care of ourselves 20-40 years from now! As we surpass age 50, there are important discussions to be had.
What patients and providers need to consider:
Risk of disease and treatment related complications
Tolerability of IBD therapies, which is unique to each person’s personal experience
Drug metabolism and how it alters with aging
Body composition changes which include a reduction in total body water and an increase in total body fat.
The delicate balance of disease-related risks vs. treat-related complications.
Risk of adverse events from medications vs. benefit shift (higher rates of infections, malignancy, and drug intolerance).
Given these factors alone, the way in which IBD is managed in older age isn’t as clear cut as when we’re younger. With both thiopurines and biologics, older patients are more likely to discontinue treatment. Older adults may value symptomatic remission (and quality of life) more than mucosal healing.
This study entitled, “The elderly IBD patient in the modern era: changing paradigms in risk stratification and therapeutic management” states, “Despite elderly onset IBD presenting with a less extensive or aggressive phenotype than adult-onset IBD, its disease course is not necessarily more benign. In Everhov et al.’s work, 22% of elderly onset Crohn’s patients underwent surgery by 5 years, although the rate was lower in UC patients (6%). Similarly, the cumulative probability of surgery at 10 years was 32% in Crohn’s patients compared with 8% in UC in another population-based study.”
According to an article in Time called “The Connection Between IBD and Aging”, whereas IBD was once thought as a disease with two spikes in onset—20s to 30s and 40s to 50s—doctors are learning there is a third spike that begins later in life. For those of us who are diagnosed when we are younger, our bodies have lived with decades of damage the disease has caused, often we’ve had surgery, been on medications with serious side effects, and ongoing flare-ups for much of our lives. For those who get IBD after 60, rather than seeing damage in various parts of the intestinal tract, more activity is seen in the colon.
The article goes on to say, “It’s no surprise IBD causes chronic inflammation, and so does aging. So, as we age with IBD, we’re at greater risk for inflammation linked-health issues, including cardiovascular disease, cancer, hypertension, chronic obstructive pulmonary diseases, chronic kidney diseases, obesity, skin issues, blood clots, arthritis, dementia, and skeletal muscle loss.”
Comorbidities and IBD
According to the Crohn’s and Colitis Foundation, people who have Crohn’s may also have a better quality of life as they age, partly thanks to modern medications and less use of steroids long term, which can trigger bone loss and cataracts over time, among other symptoms. Steroids are the most dangerous medication we have to treat IBD, sometimes of course they are necessary, but long-term use should be avoided at all costs.
People over 60 are more prone to infections and have a greater likelihood of being on medications for additional health conditions. They also often have visual, cognitive impairments, risks for falls, and surgery complications.
Underrepresentation in clinical trials
One of the main reasons we lack data about IBD in older age is because this population of patients is often excluded from clinical trials. This study from The Lancet Gastroenterology & Hepatology says, “A deeper understanding of biological and functional age, dynamic risk stratification strategies (including frailty-based risk assessment tools), comparative effectiveness and safety of current therapies and treatment strategies, and shared decision making to inform treatment goals and targets is needed to improve outcomes in older adults with IBD.”
A Crohn’s and Colitis Foundation study found that clinical trials for biologics only included 1% of people over age 65. How can patients feel safe about being put on biologics when there isn’t research to back up the safety and efficacy of these heavy-duty medications when they reach that age bracket?
As far as menopause goes, we still don’t know much yet about how this impacts women and the role it plays in disease course. Some small studies have found a modest protective role for estrogen-replacement therapies for IBD activity. But there’s more research needed in this area. According to the Crohn’s and Colitis Foundation menopause may begin earlier in IBD patients, but this does not appear to have any negative effect on disease activity or progression. Women with IBD are at greater risk for osteoporosis in menopause, this is why it’s so important we’re proactive in younger age by getting bone density tests and taking calcium and vitamin D supplementation (if labs show you’re deficient). I have taken 50,000 IU of Vitamin D once a week for years to help combat bone loss and this past year I started seeing a Bone Health Doctor to keep a close eye on my osteopenia. My GI told me during my clinic visit this month he wants me to take 2 Tums a day for added calcium.
As far as men, aside from methotrexate, IBD medications do not usually cause erectile dysfunction. Ileal pouch anal anastomosis (IPAA or J-Pouch) surgery, while sometimes associated with loss of sexual function, is not associated with erectile dysfunction. There’s also no known connection between IBD and prostate cancer.
Patient inputfrom those who are 60-plus
Patti says her age has changed how she manages her IBD.
“I’m 60 years old. Mostly, I compartmentalize social outing to 2 hours at a time. If I extend it, I’m exhausted and feel crummy for the entire next day or two. If there’s a situation where I know it will have to be more than three hours, I make sure to rest and eat less the day before, and then eat minimally until the last hour or so of the outing. This way, I don’t have to feel like I’m running on empty during the entire outing, and I can prepare to be home for whatever the food decides to do, in addition to the exhaustion and pain that I know are coming.”
Patti went on to say that she feels her Crohn’s brought on menopause sooner, but also that her Crohn’s may have masked menopause symptoms because she was used to low-grade fevers and sleep interruptions.
“I found out I was post-menopausal at 50 and I basically missed the transition (the symptoms). I took that as a win (ha), but I do feel like my body is older than my age. I can’t really explain why, but the constant inflammation, plus my body trying to resolve it—I believe it’s taken a toll on my aging. But recently turning 60 feels AMAZING. TO be sick since I was 8 years old and have fought my way to my sixth decade feels like I climbed a mountain! I’m proud of how hard I’ve fought all these years, while still thoroughly enjoying life, my marriage, my daughters, and my career!”
Heidi was diagnosed with Crohn’s at age 50 after years of being told she had IBS. She found out in July 2023 that she had a” severe Crohn’s reoccurance after 5 years on Stelara. Her options were Skyrizi or Rinvoq since she has a history of TNF inhibitors failing her. Even though Rinvoq had a slightly better chance of putting her in remission, her and her care team thought Skyrizi would be a safer option due to her age. Rinvoq has a warning regarding increased cardiovascular events, such as heart attack, stroke, or death in people 50 years or older, along with risk of blood clots.
“If I don’t respond well enough to Skyrizi, we will then try Rinvoq, but the safety profile seemed better especially for me being over 60, and that’s important to me. I also worry about what is going to happen when I retire and my medical insurance goes from commercial to Medicare! I think they often have a deductible that is much higher than commercial insurance.”
Heidi was also diagnosed with osteoporosis in her 50’s and took treatment for it for 5 years.
“My risk for fracture still increases as I age, so my GI ensures I have DEXA scans every 2 years.”
Brenda had diverticulitis for a few years, and beginning in December 2011 she started having other bowel problems. She went straight to her general practitioner, and he ordered a colonoscopy, which confirmed her Crohn’s disease diagnosis at age 63.
“After many failed medications, I had part of my colon removed and I had a temporary ileostomy. Unfortunately, I got an abscess which made me really sick and in 2015 I had more colon removed and the stoma was made permanent. Since that surgery, I’ve been quite well and basically get on with my life without any IBD medication.”
Brenda is now 75 and worries about getting sick again and needing additional surgeries. She also worries that as she ages that one day she may not be able to deal with her ostomy bag herself and that concerns her.
Keith has ulcerative colitis and his wife was diagnosed in her 20s with ulcerative colitis. Her IBD was under control for years until she was hospitalized 20 years ago. She underwent her first operation then and it was successful. Fast forward two decades and she flared and required additional surgery.
“She’s doing ok now, but both surgeries were a result of her bowel narrowing.”
Jody is on Remicade and is currently in remission. She started with colitis in her 20s and then her diagnosis shifted to Crohn’s in her 60s. She’s in her early 70s now. She’s tried several biologics and medications.
“Not sure when I started Remicade. I have tried a few before and they were either too expensive or I had issues with them. I am in the United States so our insurance is not easy. I also have taken Mesalamine for years for colitis, which has worked great but it’s another expensive drug, so the prescription was cut in half due to cost a few years ago.
Sherry hasn’t changed much in her 44 years of living with Crohn’s, but has more of a focus on an overall healthy lifestyle.
“I’ve gotten better at avoiding trigger foods and being more diligent taking necessary vitamins. I’ve always been active (weight training, golf, and skiing) and remain so if not more these days. The introduction of biologics has obviously been a game changer a huge benefit.
Jeff says gastroenterologists seem to believe you more as you age.
“As you get older, more things in your body are broken. It’s a balancing act as to what is most critical. You also start running into unknown territory for GI docs, as many treatments do not have much data, if any, for seniors. GI docs do seem to believe you more when you need help.
Kanchan is currently 74. She has had a J-Pouch since 1989.
“For the last 4-5 months I am making probiotic yogurts at home and the last month I started making Kefir. I’m hoping for good results.”
Sherri– “I was diagnosed with IBD in 2015 when I was 56. I’m tired of the whole thing. What’s going to happen when I can’t look after myself?”
Closing Thoughts
It’s important for us to work closely with our healthcare teams, not only gastroenterologists, but all specialists, to manage IBD effectively as we age. It is beneficial to check in with a registered IBD dietitian, as aging may affect the body’s ability to absorb nutrients. I often wonder if when my kids are in high school or college (my youngest is 2.5!), if I’ll play a little Russian Roulette and try going off my biologic. I’ve been in surgery-induced remission since August 2015 and if this continues (God willing), I think I will try. Right now, as an IBD mom of 3 kids (ages 6, 5, and 2.5), I don’t feel confident enough that I won’t flare and need to pull out all the stops I can, so I can be present and well for my young family.
There’s a delicate balance with each decision we make along the way and the best we can do is advocate for ourselves, be proactive and take measures now to be healthy, do our research, and stay as educated as we can about what’s coming down the pipeline for the IBD community as we age. By controlling inflammation in our younger years, we can help improve our future quality of life and prevent age-related symptoms.
When you’re diagnosed with Crohn’s disease or ulcerative colitis it’s a lot to process. When I started this blog in 2016 and after living with Crohn’s for nearly 19 years, my focus has always been to be the voice I needed to hear upon diagnosis and what it was like to experience young adulthood with a chronic illness. As a 21-year-old, fresh out of college, I had to navigate my career, finding love, and becoming a mom with IBD on my own. The first decade I wasn’t publicly sharing my story and didn’t know there was a patient community to tap into online for support.
The first week I started experiencing Crohn’s symptoms-March 2005, Senior Spring Break in the Bahamas
Often as the years go by and we get beyond the initial shock of hearing the news and what this means for our lives, we tend to forget the challenges we faced to gain our footing. This week on Lights, Camera, Crohn’s I share some tokens of knowledge I’ve gained along the way that I hope will help you on your own journey, no matter where you find yourself at this moment.
Healing—physically, mentally, and emotionally is not linear. We all experience IBD uniquely—some people’s disease course is milder, others have it severe. We all cope differently with knowing and living with a chronic illness. Give yourself grace in the difficult moments. It’s ok to feel resentment or anger. It’s understandable to wonder at times “why me.” It’s “normal” to feel scared and anxious whether you’re a few weeks or a few decades in. Sometimes it’s taking things one hour at a time, other times it’s taking them one day at a time. Because of how quickly a flare up can strike, I try to live in the now and not worry about tomorrow.
You didn’t have control of getting your chronic illness, but you can control how you react and choose to heal from it. It’s easy to feel like you may be to blame if your health takes a turn for the worse. But understand this is not your fault. The unpredictability of IBD makes it feel like we’re often in the passenger seat and spiraling in circles, but this disease cannot control how you react, respond, and choose to heal from it. No matter what, you’re in control of the healing process. Whether it’s finding support through fellow patients and caregivers or through professional therapy, you won’t look back and you’ll be setting yourself up to take this on to the best of your ability.
There is no comparison game. Since the majority of people are diagnosed with IBD in their teens and into their 30s, it can be easy to try and measure your timeline and accomplishments to that of your peers who do not have chronic illness. It can also be tempting to look at people in the patient community who seem to have the world by the tail, when you’re struggling to get out of bed each day. This isn’t a competition of the sickest or a ploy to see who can smile through the pain and get more done. The only person you need to answer to, is who you see looking back in the mirror. You determine what you’re capable of and what you want in life. Your roadmap is yours and you’re right where you’re meant to be.
You set the benchmark for what’s possible. Your IBD is part of you, but it’s not your entire identity. Remember that even patient advocates are posting somewhat of a highlight reel. Even those who are working, in love, and parenting are dealing with their own struggles, too. My best advice would be to think about what you hope for in life (don’t even think of your IBD as part of the equation) and go after it. Yes, your health may cause some detours and roadblocks, but you won’t find your way unless you try.
No one knows your body better than you. I don’t care how many letters someone has after their name, they aren’t living in your body and experiencing what you feel each moment of every day. Be vocal when you need to be. Communicate as much as you can with your care team and paint the clearest picture of your reality. If you keep parts of your struggles to yourself or dumb down the severity of your day-to-day life, the only person you’re hurting is yourself. Learn about nutritional bloodwork and advocate for yourself to be tested for a full iron panel with Ferritin and Vitamin D. Get labs every 3-4 months so you can keep a finger on the pulse of what’s going on with your body. If you feel like your provider is being lackadaisical, don’t hesitate to get a second opinion. Take ownership of your health and find a provider who in your darkest moments you would feel most comfortable by your bedside in the hospital.
Make sure your GI specializes in IBD. There are gastroenterologists and there are gastroenterologists who specialize in Crohn’s and ulcerative colitis. Once you’re diagnosed with IBD, it’s imperative you try to find a GI who is an IBDologist. This can be tricky if you live in a rural area, it may mean you need to travel several hours to find a provider who fits the bill. If you move or are unsure of a good GI to check out, it’s helpful to reach out to your local Crohn’s and Colitis Foundation chapter and often they can help point you in the right direction.
Diet and stress levels matter. Read that again. Any doctor who tells you diet, and stress doesn’t impact your disease process is wrong. There are incredible registered dietitians throughout the US who specialize in IBD, and many of them have IBD themselves! Before you start restricting yourself or your child, make an appointment—most provide virtual options and this will help you get educated on what works best for you. What is a trigger for one person, isn’t necessarily a trigger for another. There isn’t a one-size-fits-all diet or else we would all do it.
Emotions will strike when you least expect them. Even almost 19 years in, I’ll sometimes break down and cry when I think about my Crohn’s or how it makes me feel. Just because you become a veteran patient doesn’t necessarily mean you fully ever heal from the hurt life with a chronic illness causes. It’s ok to have these moments where you may feel like you’re allowing your disease to control your emotions, you’re not. You’re human. It’s healthy to feel frustrated and to get emotional about what your life is like because you have IBD.
You’ve endured more than you give yourself credit for. As chronic illness patients we go through so much that often we don’t even bat an eye over experiences that would be extremely painful or stressful to the average person. Think about what a bad ass you are and how that carries over into each and everything you do in life. If you’re newly diagnosed you will get there—but even those initial weeks and months, you’re enduring more than the people who have their IBD under control and have a good handle on their body. No matter how many surgeries, scopes, scans, and IVs I’ve had, I always get a little teary eyed because it brings me back to 21-year-old me and then all the trauma that comes along with living with Crohn’s for 19 years. While those tears are sad, they also come from the strength of reflecting on what I’ve gone through to bring me to now.
Stay in tune with how your body is speaking to you through symptoms, do not ignore them. It can be challenging to communicate what you’re feeling to someone who does not have IBD. I get that. But by protecting loved ones, friends, and doctors from what you’re experiencing you’re preventing them from stepping in before it’s too late and before you know it your flare has gotten out of control and requires hospitalization. I used to be that person all the time. I would always internalize the pain, silently fighting through each day, doing anything possible to stay out of the hospital until the symptoms were simply unavoidable and required medical intervention. One hospitalization always sticks out in my mind. It was May 2009. I was a 25-year-old morning news anchor in Wisconsin. I was solo producing a 2-hour morning show dealing with horrible abdominal pain that kept making me throw up in the garbage can next to my desk in the newsroom as I struggled to put together the show. Finally, I couldn’t take it anymore and I had to call my co-anchor, who rushed me to the hospital. I was released from the ER hours later after my parents had driven from Chicago in the middle of the night only to return to the hospital that afternoon and have my dad carry me in his arms through the automatic doors. I was finally admitted and given the medical intervention I needed. Take it from me, you’re creating even more of an uphill climb for yourself if you don’t start speaking up when you initially notice something is awry.
The worst moments are just that, moments. When you hit your breaking point, when the pain seems overwhelming, and you can’t see the forest through the trees try to breathe. Go to your happy place. Recognize this is one day, one moment, I always tell myself “This too shall pass.” Go to your happy place mentally. Do mindfulness exercises. Shut out the outside world and focus on your breath. Detach from your body as best you can. Think of people who inspire you and bring you joy. Everything is fleeting. Each flare, each recovery, each prep, procedure, and surgery…it has a start and a finish. One day it will be a memory you talk about.
Pay attention to who is there when you when are quiet and when you’re going through the thick of it. IBD is too big to deal with alone. Lean on people you can trust, who you genuinely feel safe sharing your health woes with. This will be fewer people than you’d ever imagine. Be prepared to realize that many of the people you thought would be front and center to support you will be non-existent. It’s fine to mourn those friendships or relationships, but don’t waste your time or energy on them. Your disease will give you the ability to see who loves you and who wants to be present in not only the good times, but the bad. You can’t change people. Hold on tightly to the people who show up consistently, expecting nothing in return. Those are your people.
Emmanuel Acho shared a reel on Instagram recently that really hit home for me and caused me to reflect a bit on the people in my life and their roles. In the video he explains that friendship is like a house. You have your window, door, and floor friends. Window friends are outside looking in, they don’t know what’s going on in your house. They don’t have intimate access to what’s going on in your life. You can only let so many people into your house. Door friends come in and out of your life depending on the season. When life gets too hard or when your world turns cold, they might exit. Your friends might not be equipped for that season. Floor friends—aren’t going anywhere. You might track mud, but they will last regardless of the season. They are there to catch your tears and hear your fears. Remember—a house has more windows than it has doors and more doors than it does floors…if it has one good floor, you’re set.
Just because you need medication does not mean you’re taking the easy way out. I’ve been where you are. I remember lying helpless in a hospital bed and what it felt like to be told I needed to “break out the big guns” and start a biologic medication back in 2008 when there were only two options on the market for those with IBD. In that moment, we all naturally want to learn about side effects and what this could possibly mean for the long term. But please try and focus on the actual risk versus the benefit. As someone who has been on Humira since July 2008, I’m so grateful for my medication for allowing me to live a full life, bring babies into this world, and be a present, able-bodied, and active mom. It’s not all medicine, or all diet and lifestyle, often for many of us who have moderate to severe IBD we need a mix of both, and that’s ok. You can still thrive and be healthy, despite being on a medication with a black box label.
You are not a burden, and you deserve love. Any romantic partner who makes you feel less than, isn’t present when you need them most, or doesn’t show any empathy or interest in your daily reality isn’t going to stand the test of time. Use your IBD to your advantage to see your partner’s true colors. Be honest and upfront when you start dating and if you ever feel like you need to defend their actions or make excuses consider that a major red flag. Dating and marrying a person with a chronic illness isn’t for everyone, and that’s fine—but when it comes to people like you and me, we need a partner who is willing to take the challenge on beside us every step of the way. Find someone who you feel comfortable communicating openly with, who sees you for more than your disease.
IBD is not a battle to be “won” or “lost.” One of my pet peeves with any health condition or disease is when people say “so and so lost their battle”…they didn’t lose shit. Diseases are not a game. Oftentimes reaching remission is due to luck, disease severity, or surgery. I spent a decade of my life with active disease and have been in remission (thanks to surgery) for almost nine years. I don’t give myself credit for that, I’m not “winning.” It’s because of my efforts to stay diligent with my biologic, vitamins, safety labs, daily decisions, and check-ins with multiple specialists, but I also don’t think I’m at this point because of something special I’m doing compared to someone else. We’re all dealt a different hand of cards in life. Your IBD isn’t a win or lose situation—you’ll celebrate big victories and small ones, too, your disease can rob you at times, it’s a never-ending exchange and game of back and forth. You are not less than because you are flaring. You are not lazy for taking medication or failing because you struggle to follow a strict, regimented diet that may or may not help you. Once you stop thinking of everything as a “fight” it takes a bit of the stress, anger, and onus off your shoulders. IBD is a chronic illness, until there’s a cure, we’re in this situation until the day we die…that’s simply too long to be “fighting” anything.
Get ready to be extra proactive with your health. Due to the nature of our IBD and the medications many of us take, we are at greater risk for additional health problems. It’s important to get annual skin checks at the dermatologist. Make sure whether you have good vision or not that you’re seeing an eye doctor. Get cleanings at the dentist at least every six months. If you’re a female, make sure you get your well woman visits. We are greater risk for cervical cancer because many biologics don’t allow our bodies to fight off HPV, this may mean annual Pap smears. We’re also at an increased risk for breast cancer, so don’t delay your mammogram. Get a bone scan every 3-4 years, get one as close to diagnosis as you can so you have a baseline. Your GI may say it’s not necessary, it is. Steroids put us at risk for osteopenia and osteoporosis from an early age, this may mean you need to see a bone health doctor (yes, those exist). Those of us with IBD are at greater risk for pelvic pain, it can be helpful to see a Pelvic Floor Therapist who addresses those unique needs.
Faith can give you added strength and comfort. I understand faith is very individualized and looks different for each of us, but I can tell you as someone who is Greek Orthodox who has always been a faithful and prayerful person that I rely on my faith to guide me through my IBD each and every day. There’s a sense of comfort and hope that comes with believing God is watching over you through the good, the bad, and everywhere in between. When you’re diagnosed or flaring, it can test your faith. Hold on tightly to what you believe and lean on that (however it looks for you). I truly believe God gives his toughest lessons to his greatest teachers. One of my biggest fears as an IBD mom of 3 is that one of my children will get my disease one day. Each night before bed, I always pray with them and say, “keep my babies healthy, safe, and strong.”
My why. My motivation to push through each and every day.
Family planning takes time and effort. Just because you have IBD does not mean you can’t be a biological mom or dad one day. The journey will look a bit different, but this disease does not necessarily need to rob you of the experience if that’s what you want in your life. Communicate these desires with your GI so they can help prep your body for a baby. This can mean starting a prenatal vitamin and folic acid several months before trying. I had a colonoscopy before every pregnancy so that I could be given the ‘green light’ by my GI that we were cleared to try for a baby. When I was pregnant, my care was overseen by my OB, a maternal fetal medicine OB (high risk), and my GI. Unless you have perianal disease, you can have a vaginal birth, but oftentimes this is a discussion left to you and your care team. I personally chose to have 3 scheduled c-sections, because while I don’t have perianal Crohn’s, I didn’t want to risk tearing or causing a fistula to form. I would make the same choice if I had to do it all over again. I also stayed on my biologic through conception, pregnancy, and breastfeeding. These are all personal choices but there are many, many research studies available that show the safety and efficacy of doing so. If you feel you could have internal scarring due to past surgeries that could hinder your fertility, check in with a fertility specialist and have them help you investigate if there could be issues.
Educate yourself on insurance, prior authorizations, specialty pharmacies, and Pharmacy Benefit Managers (PBMS). Unfortunately, with IBD we are forced to do so much behind-the-scenes work to simply receive treatment and medication. You will waste countless hours and endless energy on the phone as these people give you the run around. Nobody ever seems to want to take ownership. Work with your gastroenterologist if you are denied a medication so they can write an appeal letter to insurance and go to bat for you. Stay on top of everything, don’t worry about annoying anybody. You gotta hustle. You gotta be frank and assertive. It’s not about hurting feelings; it’s about making sure people are doing their jobs and ensuring your course of treatment doesn’t get delayed because someone fumbles some paperwork. Our medications are time sensitive. Light a fire under people’s ass if you’re not getting responses you deserve. One of my friends on social media posted this over the weekend, “Managing specialty medications in January is an annual slap in the face to chronically ill people.” It sure is. This week will mark the first time I’ve ever received my injections late in the mail, due to a misstep in my GI office that I had to follow up on for over a week. Be extra proactive at the start of each year. Make sure your GI informs you about all the patient savings programs available, these can help you not only emotionally, but also financially.
You get the final say. No one but you gets to say what you do with your body. If a doctor wants you to do an enema before a scope and you don’t want to, don’t. If you don’t feel comfortable with taking a certain medication and your care provider keeps pushing it, they can’t physically make you pop a pill, take an injection, or receive an infusion. You must do your research, educate yourself every day, feel empowered by all you know and be ready to deal with the ramifications if you go against the grain or determine you want to try something differently. There’s not one “right” way to live with IBD. Be honest with your provider. Don’t say you’re taking a medication and then not take it, that’s not helping anyone or anything. Be a compliant patient, but an educated and empowered one at the same time. Measure all the risks and benefits and what your hopes and dreams are for your present life and for your future. Don’t ever feel like someone else can or should dictate what path your journey takes. Just because one biologic is a magic bullet for one person doesn’t mean it will be for you. You never fail treatments, they fail you. If a provider says “oh, you failed Remicade” … please correct them. “No, Remicade failed me.”
I write this as a 40-year-old mom of three—ages 6, 5, and 2.5 years old, married for almost 8 years, who has been on a biologic since 2008, who was diagnosed at age 21 in 2005. So much has changed for the better regarding the patient experience since that time. My perspective has come a long way. I used to be right where you are, so many are living your current reality. Instagram is the bread and butter for the patient community, that’s where you’ll find the most patients and caregivers transparently sharing. Follow the accounts, send a DM, comment on reels and posts, get engaged. Never hestitate to connect and reach out to me–natalieannhayden. Educate yourself through lived experiences and people who have paved the way for you, rather than Google. You don’t need to recreate the wheel, but this is your experience and your story. You get the final word on how you want each chapter to play out. Know each time you fall you will bounce back and that there’s a massive community of support here to catch you and cheer you on every step of the way as you rise once again.
It’s no surprise IBD impacts so much more than just our guts. Not only is there the gut and brain connection, but also the complex nature of our chronic illness(es) that can cause serious anxiety, depression, and mental health issues. The isolating nature of Crohn’s disease and ulcerative colitis, the unknowingness of what the next day holds, and the never-ending laundry list of procedures, labs, scans, and surgeries, year after year is a lot for any person to go through.
Even though I’ve lived with Crohn’s disease for more than 18 years, and have seen three different gastroenterologists in that time, not once has my mental health been brought up during a clinic appointment. When treating a person for IBD, the health of the whole person needs to be considered. I ran a poll on Instagram asking the IBD community if they’ve ever been to therapy. Out of 185 respondents, 70% seek therapy, 18% have not, and 12% are considering it.
I did an article in September 2020 about why a specific public bathroom at a grocery store I used to shop at triggers me and shared tactics for coping. You can read the article that featured Dr. Tiffany Taft here.
This week on Lights, Camera, Crohn’s we hear from those in our community about the advice that’s resonated with them the most since receiving their IBD diagnosis.
The words that have made a lasting impact
Olivia: “3% effort is still effort. You’re not going to be able to give 100% every day and that’s OK. Your best can look different from day to day.”
Julie: “It’s not your fault, you didn’t do anything wrong.”
Kristen: “You can’t drive forward if you’re always looking in the rearview mirror.”
Sarah: “Medical trauma is trauma and to give myself credit for all I have overcome.”
Cindy: “Remove all IBD related stressors from the bedroom to avoid impacting sleep. In our case, this meant no Humira injections for my daughter while sitting on the bed or nearby it.”
Tina: “Imitation is the best form of flattery.”
Lauren: “Don’t Google things you’re worried about, like symptoms.”
Jennifer: “Stay in the present.”
Heather: “Sometimes you just need to take a nap!”
Myisha: “If it’s not going to matter in five years, don’t give it five minutes of your energy.”
Kate: “It’s not your fault.”
Susan: “I’ve never seen a therapist, but I always tell myself it could always be worse.”
Stacey said: “You can’t control how seriously people take Covid. You can only control how you protect your physical and mental health. You have to put your health first. And, if people don’t agree with your choices, then that’s their problem. You can’t risk your health just to make it easy for others or to placate them. You come first in your life.”
Robin: “The “things” I do—my work advocating for others, supporting others, helping others face challenges with their diseases—I deserve that, too. Not from other people, but from myself. The beauty in therapy is that you’re receiving a non-biased/outsider opinion. This person that has no side and will sometimes say something you’ve heard 1,000 times in a way you’ve never heard before or even in a better way that allows you to really listen to what’s being said. To absorb it. Even to say it multiple times with no judgement if that’s what’s needed. Also, EMDR, which is a whole other thing and only part of the therapy experience.”
What is EMDR therapy?
Several people said EMDR therapy was their favorite and has been lifechanging. So, what exactly is it? Eye movement desensitization and reprocessing (EMDR) is a fairly new, non-traditional type of psychotherapy that’s popular for treating post-traumatic stress disorder. EMDR focuses on the natural tendencies our brains have for healing from traumatic memories. There are mental blocks (such as feelings of self-esteem issues and powerlessness) that can prevent us from healing. During EMDR, you are allowed to process the bad memories and experiences to start healing yourself. This helps our brains process challenging thoughts and feelings in a healthier way. Chances are through your patient journey you’ve endured several vivid and significantly painful moments that you haven’t been able to process and heal from.
Supportive Resources about managing mental health and IBD
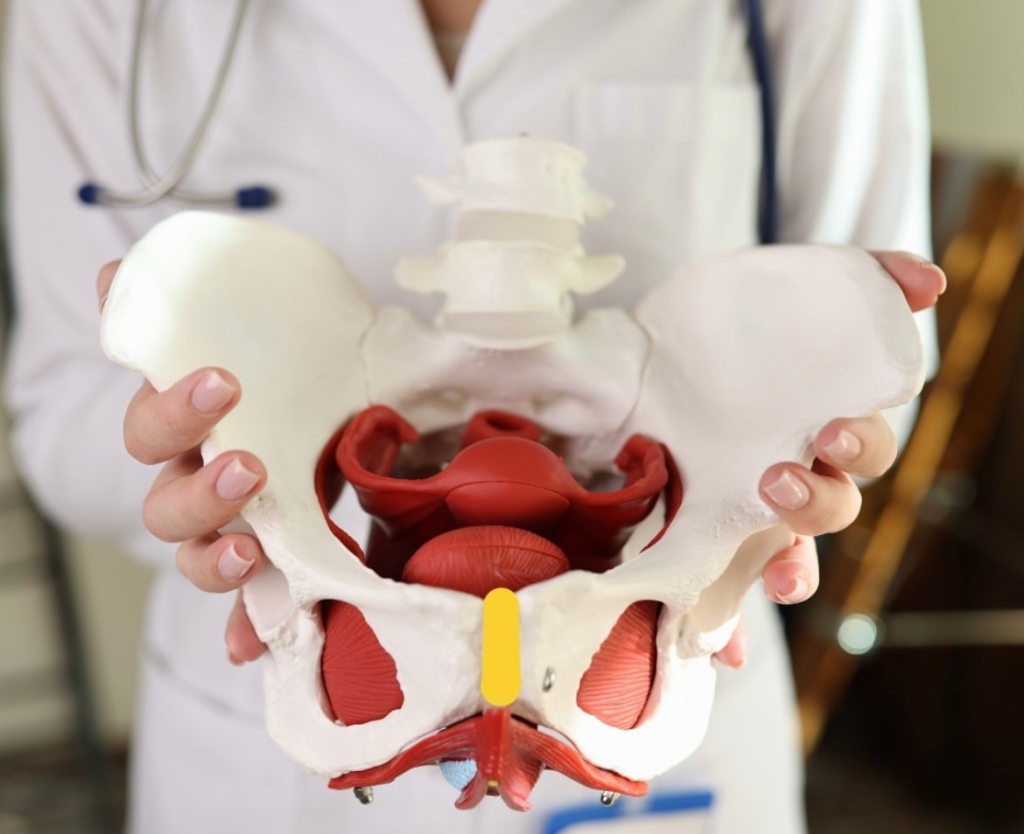
Chances are you’ve heard of Pelvic Floor Therapy but may not know what this entails or why so many people in the IBD community are talking about it. Individuals with IBD can have persistent symptoms of fecal incontinence, constipation, rectal discomfort, and diarrhea, despite having their IBD in remission with medical therapy. These persistent and often debilitating symptoms can have a major impact on your wellbeing and quality of life.
This week on Lights, Camera, Crohn’s we hear from two gastroenterologists from Mayo Clinic along with several IBD warriors who provide insight, helpful guidance, and information about pelvic floor therapy.
What exactly is Pelvic Floor Therapy?
Pelvic floor therapy is a treatment program performed by pelvic floor therapists to retrain the pelvic floor muscles to address underlying issues such as constipation, fecal incontinence, or urgency. Many patients with IBD in remission may develop pelvic floor dysfunction which is usually diagnosed from a digital rectal examination in combination with an anorectal manometry test.
“During an anorectal manometry, a small catheter with sensor probes and a balloon is placed into the rectum and is connected by a wire to the computer. During the test you are lying on your side and asked to perform maneuvers to determine how your pelvic floor muscles work. At the end of the test, they inflate a balloon in the rectum to help evaluate for sensation and then ask you to simulate having a bowel movement by pushing the balloon out,” explained Dr.Katie Dunleavy, MB BCh BAO, Gastroenterology Fellow, Mayo Clinic.
Based on normal values for your age and gender, you may be diagnosed with a pelvic floor dysfunction. Dr. Dunleavy went on to say that in IBD, there is less research on the benefits of pelvic floor therapy.
“But we have seen benefit in up to 80% for patients in remission who continue to have symptoms of constipation, urgency, or incontinence once active inflammation is fully ruled out. Similarly, some patients with IBD undergo total proctocolectomy with ileal pouch anal anastomosis (IPAA) may also benefit from pelvic floor therapy if they have issues emptying their pouch,” said Dr. Dunleavy.
Additionally, those with IBD who’ve had pelvic floor surgeries might experience sexual dysfunction and this type of therapy directed towards relaxation of the pelvic floor can lead to a better sexual experience.
Pelvic Floor Dysfunction does not discriminate across genders
Any person can develop pelvic floor dysfunction and may benefit from treatment with pelvic floor therapy in the right setting.
“While most studies describe pelvic floor in females, I believe individuals from all genders deserve evaluation of their pelvic floor the recommendation for pelvic floor therapy. Furthermore, individuals of a transgender experience, might undergo gender affirming surgery that impacts their pelvic floor muscles, and would benefit from pelvic floor therapy,” said Dr. Victor Chedid, M.D., M.S., Gastroenterologist at Mayo Clinic.
Dr. Dunleavy says, “As many as 50% of people with chronic constipation have pelvic floor dysfunction, which means there is impaired relaxation and coordination of the pelvic floor and abdominal muscles during evacuation. Some common symptoms include straining with hard bowel movements, a feeling of incomplete evacuation, pain with intercourse, or urinary symptoms.”
Certain risk factors make it more likely for men or women to develop pelvic floor dysfunction, this includes instrumented vaginal deliveries, chronic constipation with straining, prior surgery, prolapse, and age. It is important for men and women to discuss symptoms with their doctor to ensure they get the appropriate testing and treatment.
Apprehensive about getting looked at?
It is important for people diagnosed with pelvic floor dysfunction to seek out a qualified pelvic floor therapist who is specialized in GI and evacuation disorders. These are generally physical therapists or occupational therapists who complete extra training in pelvic floor therapy.
“You should find a therapist you trust and will feel comfortable with during your therapy sessions. The therapists who work in this area are fantastic and work diligently to explain what they will be doing. My patients tell me that the relief they feel from therapy well exceeds the apprehension they had prior to starting sessions,” said Dr. Dunleavy.
It’s important for patients to feel comfortable talking with health care providers and addressing concerns they may have on this topic. Dr. Chedid typically discusses the benefits of pelvic floor therapy with patients during clinic visits as a beneficial treatment option that does not require surgery. He provides patients with exercises and techniques to do at home that will have a major impact on general wellbeing and health.
“Individuals with IBD experience significant “negative” experience with the bathroom and with defecation that can be quite traumatizing, and therefore when they get in remission, they still have a negative association with the bathroom and might have “fear of defecation” despite being in remission. I equate that to “PTSD of the pelvic floor”, which is not a medical term, but an analogy I use. Therefore, pelvic floor therapy is essential to reverse this negative experience with the bathroom and make their bathroom experience a healthier and satisfying experience. Almost all patients who I describe this to get it right away and understand the importance of pelvic floor therapy,” said Dr. Chedid.
He adds that it’s imperative health care providers communicate with patients and ensure that the therapy session will be a safe space with at rained physical therapist who is trained in empathetic and trauma informed care. This is essential in putting a person’s mind at ease, as many patients might have experienced sexual trauma in their lifetime that makes pelvic floor therapy triggering for them.
The impact of Pelvic Floor Therapy post operatively and after IBD pregnancy
If you’ve had a total proctocolectomy and an ileal pouch anal anastomosis (IPAA), you might experience non-relaxing pelvic floor dysfunction or pouch evacuation disorder. This is similar to the rectal evacuation disorder in individuals with pouches.
“Typically, this is identified by history, physical exam, pouchoscopy, anorectal manometry and dynamic imaging of pouch evacuation. Additionally, someone who has had any form of trauma to the pelvic floor, including Perianal Crohn’s disease or surgeries for Perianal abscesses or fistulas or lacerations due to vaginal deliveries after pregnancy, these patient might experience rectal evacuation disorders after recovering and healing. In the proper patient, if identified by history, physical exam and the right testing, these patients will benefit from pelvic floor therapy,” said Dr. Chedid.
At the same time, there isn’t a lot of research on pelvic floor therapy in the post-operative state or following pregnancy in patients with IBD.
“There have been several attempts to find normal values for patients with IPAA who have undergone colectomy to help diagnose pouch related pelvic floor dysfunction. We generally recommend patients wait until the anastomosis following surgery is completely healed prior to having an evaluation with a balloon to ensure no complications. Similarly, patients who have recently undergone delivery from pregnancy will likely require time to heal. I would discuss this with your doctor to have more personalized information,” advised Dr. Dunleavy.
If your GI recommends pelvic floor therapy for your personal symptoms and struggles the overall response is tremendous.
“Recommending pelvic floor therapy to everybody, without identifying the right patient who would benefit from it is not typically beneficial. Therefore, in the right patient, pelvic floor therapy is extremely effective,” said Dr. Chedid.
What IBD patients have to say
Stacey has ulcerative colitis and went from having an ostomy to becoming a j-poucher. She’s a big proponent of Pelvic Floor Therapy. After her 3-step surgery to j-pouch in 2021, she knew she needed at least an evaluation from a pelvic floor physical therapist (PFPT) after urination became a challenge and inserting tampons became impossible during her takedown recovery.
“My surgeon wouldn’t write me a referral, citing that the anorectal manometry tests prior to surgery were all normal. My GI doctor didn’t want to go against the clinical judgement of my surgeon, so I couldn’t get one from her either, and finally I received a referral from my OB/GYN after explaining that penetrative sex was impossible (and felt unsafe to me) to even attempt,” Stacey explained.
These delays resulted in 5 months of significant pelvic pain that she felt ill-equipped and under-supported to handle, and this time could’ve been saved if she had gone into surgery with a referral to see PFPT from the get-go, even if she didn’t need to use the referral; it would’ve been nice to have.
“It’s so wild to me that orthopedic surgery has extensive PT rehabilitation protocols, and yet I was met with such resistance to gain access to the professionals who could help support my muscular recovery, even after such extensive GI surgeries,” she said.
During Stacey’s initial encounter with the PFPT, she spent the majority of the visit trying to gain a strong understanding of her entire pelvic and holistic health history, everything from sexual health to physicality to surgery, and all the in-between.
“She asked for consent prior to any invasive exams and explained them in thorough detail, reminding me that I was in control and could always choose to stop an exam if I felt unsafe. She continued to breathe with me during the exams and communicated her findings in real-time, which made me feel at ease. At the conclusion of our visit, I was told that I was experiencing hypertonic pelvic floor dysfunction from a decade of clenching for dear life trying to make it to the bathroom with mod-severe UC, even before my surgeries. The tightness of the muscles, coupled with three extensive pelvic surgeries, contributed to the pain and issues I was experiencing,” said Stacey.
During the visits with the PFPT, Stacey discovered she had no awareness of her pelvic floor muscles whatsoever. She could not distinguish the relaxation of the muscles from the contraction, and the entire area felt numb to her, like it was a holy, empty space. She says this made the exercises challenging to understand initially. She was prescribed specific exercises, not Kegels, including strategies to gain awareness of supportive muscle groups so she could begin to engage with this part of her body and start to heal.
“What I did not expect, however, was for this experience to be as enlightening and empowering as it was. Slowly but surely, the little life things showed me that they’re the big life things: being able to fully urinate in under 20 minutes, FINALLY being able to use tampons again- these were MASSIVELY important to my quality of life, and they became possible through the help and support of a PFPT and my adherence to their prescribed exercise regimen. I even realized one day while holding one of my exercise poses that I could feel the muscles DEEP in my abdomen! They felt heavy, full of pressure, as if they fired on to greet me, and then suddenly… I could feel them gently, slowly, RELEASE. I cried tears of relief realizing that I had been fearful of reconnecting with these muscle groups, and it really was safe and okay to be in my body.”
Stacey says she had NO idea these muscles existed, yet here they were. Had they been here all along?! She says she numbed them out from years of associating the deepest parts of her with pain from UC; and that her brain was protecting her. I truly wonder. All she knows is the day that she could FEEL her body experience relaxation and safety with FULL awareness of these pelvic muscles is the day that she knew that healing from these surgeries was going to be possible.
After one year of PFPT, Stacey “graduated,” not free of pain, but with the tools to know how to live within the ebbs and flows of pain. She tells me she still relies on the tools and bodily awareness that she gained through the experience.
Jessie was diagnosed with Crohn’s disease when she was 15 years old and after more than 22 surgeries later, at the age of 38, she says she completely underestimated how much her pelvic floor was affected over the years by the inflammation, surgeries, and her pregnancy.
“I was “guarding” badly (a response to pain) and so weak. I was having bladder issues, pelvic pain, rectal pain and so much more. After 2 years of being consistent going to pelvic floor therapy and doing the exercises I can say I’m about 85% better. I can’t say enough how much of a HUGE difference pelvic floor therapy made in my life and my IBD journey. My therapist explained it to me like this “you don’t have orthopedic surgery on your knee, wrist, ankle, spine, etc. and not get prescribed physical therapy. Same with an injury. It’s just standard procedure. But, for some reason, even though your pelvic floor consists of tons of muscles, ligaments, tendons, bone, etc. the same process is not considered – but IT SHOULD BE!” Your pelvic floor needs to be rehabbed after any injury, strain, surgery, etc. just like any other muscle/tendon/ligament/bone in your body,” explained Jessie.
Claire started PFPT because all imaging and tests showed that while her inflammation is under control, she still experiences extreme pain.
“I was tested, and they found I have dyssynergic defecation. This was caused by my chronic pain due to long-lasting fissures as well as chronic constipation. I’m grateful my GI thought to have me tested for this, as many don’t make that connection since the symptoms are so similar to Crohn’s. During PT, I have learned that my muscles do not relax and are constantly tense, so we work on trying to get them relaxed in order to successfully pass bowel movements. Like all other PT, one downside is that it is a lengthy process and takes up a lot of time. I have a one-hour appointment every week for 12 weeks and an hour or two of exercises and stretches on my own every day.”
She says she’s started to notice improvements and found ways to make her pain more bearable, though it’s something she will have to continue working on for a long time.
Tiffany has accessed pelvic floor therapy for herself and having previously been a physio and a fellow Crohnie, she recommends people speak with their doctors because it can make a world of difference, especially after surgery, hospitalization, or a flare.
“The neural connection we have to our trunk and pelvic muscles can be re-trained and strengthened, allowing less pain, and for me an improved sense of control over urgent bowel movements.”
Preslie was diagnosed with Crohn’s in June 2016, and after two years of battling severe symptoms, she had a colonoscopy that showed she was in remission. It may sound like lovely news, except Preslie was still living with a ton of pain, so her and her care team started digging for answers.
“This led to an Endometriosis diagnosis in August 2018. That was great news, except I STILL was not getting relief, and started having severe burning anytime I urinated, but always tested negative for UTIs. I went to a male urologist who told me I was just constipated, which was not the case. After well over a year of extremely painful sex, constant pain, and burning when I peed, I went to a urogynecologist who talked with me for less than 10 minutes and had the diagnosis: Interstitial Cystitis and Levator Ani Syndrome. I finally felt heard. I started pelvic floor therapy shortly after and immediately felt relief.”
Rocio says pelvic floor therapy was recommended to her by a home health physical therapist who was treating her for neuromuscular issues after bowel resection surgery for her Crohn’s in 2020.
“During my resection recovery, I was struggling tremendously with constipation, which was unfortunately always my issue with my IBD. Although uncommon, it’s been my reality for the last 20-plus years. The reason I share this is because I wish someone would have recommended pelvic floor therapy to me over all those years.”
She began seeing a pelvic floor therapist in January 2021 and completed two years of treatment. During that time, Rocio says she learned a lot about the intricacies of all the muscles, the nerves, the internal blood flow, and so much more. Because of two fistulotomies and a stricturplastly, she has numerous anatomical issues which prevent her from having normal bowel movements.
“Pelvic PT changed that completely and I have normal/formed BM’s every single day, without any signs of constipation and without any straining. I’ve learned ways in which I can help relax and release the pelvic floor should I face issues in the future.”
Separately, Rocio has learned how beneficial pelvic floor therapy is for many IBD patients post-operatively, including the ileal resection she had. Her therapist worked on her abdomen significantly during appointments to prevent adhesions and scar tissue. She says there are so many benefits to pelvic floor therapy that it does make her wonder why more IBD health care providers aren’t encouraging patients to pursue care.
Annie started pelvic floor therapy two weeks ago. She was referred based on suspected interstitial cystitis, not her IBD. She was shocked to learn during her first appointment that treatment was for all conditions that involve urgency of any kind.
“The game changer was the pelvic exam itself, I never realized what my PT noticed right away, which is that my first layer of pelvic muscles are unnaturally sensitive. This is massively helpful for IBD and IC, but the most validating part was having a lifetime of excruciating intercourse and painful pap smears and knowing the reason. My PT told me this is not how my life has to be. After just two weeks of exercising my pelvic muscles with a vaginal wand and daily targeted yoga, my urgency, both with my Crohn’s and IC, has gotten so much more manageable. I started this journey running to the restroom every 30 minutes (even at night), now I feel like I’m starting to get my life back.”
Jasmine says pelvic floor therapy helped her a ton following j-pouch surgery.
“I truly believe it should be integrated into post-op care plans, I had to seek it out and ask for it.”
Amy says that while she doesn’t have experience yet with PFPT, she has a complicated Crohn’s history for the past 25-plus years. Now that she’s over 40 and has had three vaginal births, she recently asked her doctor about pelvic floor therapy.
“Because of all the IBD women sharing their journey with this on the Internet, it inspired me to look into therapy for myself. In my first request, the response was that it might be a fantastic idea, but to wait and see. My next visit is in a couple of weeks and I’m looking forward to utilizing this article to share and take with me to help me advocate for myself.”
A look at the insurance piece
Yes, pelvic floor therapy can be covered by insurance, but it can vary based on the type of insurance. It is also important to ask about coverage for biofeedback therapy which is an essential part of the therapy based on prior research studies. Many insurance companies will need proof of diagnosis using an anorectal manometry with balloon expulsion test or defecating proctogram.
“If the proper indication based on testing is identified with the referral to pelvic floor therapy with a script written by someone’s GI provider, then typically insurance should cover it,” said Dr. Chedid.
Closing thoughts on Pelvic Floor Therapy and IBD
It is important to discuss with your doctor if pelvic floor therapy is right for you. Once patients with pelvic floor dysfunction have these basic tools, they can begin retraining the pelvic floor muscles with biofeedback. Biofeedback provides auditory and visual feedback to help retrain the pelvic floor and relax the anal sphincter. Biofeedback training is the treatment of choice for medically refractory pelvic floor constipation, with some studies showing improvement in more than 70 percent of patients. Patients also learn to identify internal sensations associated with relaxation and long-term skills and exercises for use at home.
At Mayo Clinic patients have had more than 70% response at 3 months following initiation of pelvic floor therapy. The response usually takes weeks to months to see a clinical difference and requires patients to practice their exercises and biofeedback at home.
“Although many centers are familiar with retraining techniques to improve pelvic floor dysfunction, few have the multidisciplinary expertise to teach patients with constipation how to appropriately coordinate abdominal and pelvic floor muscles during defecation, and how to use bowel management techniques, along with behavior modification, to relieve symptoms. Because pelvic floor dysfunction can be associated with psychological, sexual, or physical abuse and other life stressors, psychological counseling is often included in the evaluation process,” said Dr. Dunleavy.
If you have chronic pain, you may also need to see a physician to have these issues addressed prior to starting pelvic floor therapy.
Key takeaways from fellow IBD patients
PTs are an excellent resource, but just like getting an IBD-ologist is superior to a general GI doctor, PFPTs are an even stronger resource, ESPECIALLY in the context of chronic GI disease where so many of our deepest muscles are constantly working on our behalf.
You can always say “no thanks!” You don’t need to agree to any sort of exams or exercises that you’re not ready for, and a compassionate PFPT will empower you to make decisions and communicate in alignment with your body’s needs.
ANYONE can benefit from PFPT: any age, any gender.
Normalizing pain and discomfort is a survival instinct, but it’s not necessarily serving you for the GOOD life- it’s okay to get evaluated if you’re concerned about sexual pain or dysfunction, pain with periods, or if you also have IBD and simply want to be sure that you’re supporting your pelvic and spinal muscles the best you can so that you can, especially in the bathroom!
YOU get to decide! Having an evaluation may be all you have the capacity for, and that’s okay! You can return for a plan of attack later, or you can wait until you have the capacity to dive in head-first! There’s no one right way.
If you decide while talking to a PFPT before they do ANY manual evaluations that something doesn’t feel right- YOU GET TO CHOOSE, and you can always, always say, “nevermind”. Advocating for your body is always progression in your healing journey, every single time.
SPEAK UP! It’s RIDICULOUS that patients have to ask and ask and ask for the bare minimum, but if it helps your quality of life and it’s within your capacity- it’s certainly worth it.
A big deterrent for patients can be cost, but the investment is worth it, if you can swing it. You would be surprised how much every system of your body is so connected and feeds off one another!
Helpful resources to check out
Find a Pelvic Floor Therapist Close to Home
Utilize the “Section on Women’s Health” or the “Herman & Wallace” websites. Both these groups train therapists who specialize in pelvic floor disorders.
The Section on Women’s Health (SOWH) website has a “PT Locator” tab. You can enter search criteria including your geographic location (e.g., zip code) and specialty (e.g., constipation) to identify a therapist closer to home.
The Herman & Wallace website has a “Resources” tab under which you will find a “Practitioner Directory.” Use the map features to locate a therapist near you.
Utilize the “find a provider” section of www.pelvicrehab.com for a local PT by zip code.
The therapists who work with pelvic floor disorders may be in Gastroenterology, Urology, Gynecology, Physical Medicine, and/or Women’s Health, etc. You may be able to find someone through your local physicians or contacts.
For those in Canada, check out the Canadian Physiotherapy Association. It has a “Find a Physiotherapist” tab which allows you to connect with the sites of participating provinces/territories. By specifying a “Women’s Health” therapist or equivalent, you may find someone who specializes in the field of incontinence, pelvic pain, constipation, etc.
The benefit of pelvic floor therapy also involved patient education, relaxation exercises, diaphragmatic breathing, and correction of maladaptive toileting behaviors. Some studies have shown improvement in quality of life relating to symptoms, and mental health.
One of the worst aspects of life with IBD (in my opinion) are the side effects of the devil’s tic tacs aka steroids and what they do to your outward appearance. It’s a shock to the system to go from looking malnourished and thin to having a moon face and an insatiable appetite coupled with irritability, the shakes, acne, and insomnia. The weight fluctuations patients endure throughout their journey is a rollercoaster of unexpected twists and turns. Our bodies transform from being thin and sickly to healthy and in remission with weight we’re not used to. While IBD is called an “invisible” illness, our outward appearances take a hit more often than most might think. Those around us often compliment us when we’re “skinny” and stay silent when we’re a normal weight—this is detrimental because there is SO much more than meets the eye.
These photos are three months apart. Pre-diagnosis and on 22 pills a day (60 mg of prednisone).
This week on Lights, Camera, Crohn’s we peel back the layers of complexity regarding body image and self-esteem with IBD. Hear the candid commentary and often heartbreaking reality from 27 patients and caregivers.
The steroid struggle
I always know that after 3 weeks of prednisone my face and looks change dramatically. I went from someone with aspirations to work in TV news, on camera every day, to not letting my mom take pictures of me. I started in the TV business as a producer and once I was off prednisone and well managed, I got promoted to an on-air role, talk about messing with your head. I used to dread being a morning show anchor and returning to the news desk after being out for weeks. Nobody knew I had IBD or what my health struggles were, but they could see something was up. The calls to the newsroom and the comments were mortifying. I used to chew gum all day long while on prednisone to try and curb my appetite. My former GI told me to be careful doing that because the ingredient Sorbitol can cause stomach upset and diarrhea.
Katie: “The moon face with prednisone really did a number on my body image. I was in seventh grade and the kids and teachers would ask me what happened and why my face was like that. My school nurse, after I was out for two weeks because of a flare, came up to me and said, “Glad to see you, but honey, you look like crap.” I was in middle school when this happened, so I always just associated having Crohn’s with being ugly and that has been a long and hard battle. When you’re relapsing and you lose a lot of weight, people tell you that you look great, but when you’re healthy and in remission and you’ve gained weight back, people stop commenting about how good you look.”
Katie’s awful experience as a middle schooler inspired her to go into education. She is now a high school teacher. She says half the reason she went into teaching was to make sure students who have chronic illnesses, or who were absent, had someone who could empathize with them and just try to make sure that the experience never happens to anyone.
Danielle: “Prednisone destroyed my body image. When you look in the mirror and don’t recognize yourself, it’s really an emotional experience. In so many ways, prednisone is amazing, it got me out of my flare, but it turns my face into a swollen balloon. I can’t look at pictures of myself during that time. I am always so self-conscious when I’m on prednisone and feel like everyone can see it. IBD does many things, one of which is controls how you look which is a difficult part of the disease. I just got married and am in a minor flare and I delayed starting budesonide because I didn’t want to risk any moon face.”
Ross: “For me, what’s had the biggest negative impact is the side effects of steroid use, specifically back acne. This developed the first time I took steroids for my Crohn’s six years ago and it still has never gone away. It has had such a negative impact on my body image even though it’s not something anyone would really see. It has stopped me from taking my shirt off during summer months in public, or I’m self-conscious of having my top off at the gym changing room or even around friends or anyone I was dating. It’s something that I would almost always be conscious of these last six years. Even now, when it’s not too active, the scars and pigmentation and redness would stop me from taking my shirt off or make me very self-conscious around other people. I don’t think it will ever go away. It used to get me so down when I was already struggling with flare ups, etc.”
Laura: “Long-term steroid use was the most damaging for me. I was unrecognizable to myself and to others. I never found much support for those body changes and the mental health impact from ‘roids.”
Chanel: “I have struggled much more with weight gain from steroids and other medications than I ever have with the weight loss that is oftentimes common in IBD. Many informational graphics and articles out there about IBD always mention weight loss, but never the issue with weight gain. I’ve always had an unhealthy relationship with my body image because of the constant weight fluctuations due to medication.”
The fluctuations from being thin to gaining weight
I’ll never forget back in 2012 noticing that I was getting thinner and thinner by not eating any differently or increasing my physical activity. I was a morning news anchor at the time in Springfield, IL and I remember weighing myself each morning and seeing 1-2 pounds drop off each day…for weeks. At the time I wasn’t very well informed about IBD and didn’t realize that was a sign I was flaring. I was in my late twenties and gearing up for a trip to the Dominican for a childhood friend’s wedding. To be honest, I was happy, and I liked how my sickly body looked.
Fast forward to 2015, I was engaged and had bowel resection surgery. I had never weighed more than 127 pounds in my life and had dropped to the teens when I was unwell. My first post-op appointment with a new GI I gained seven pounds, and I wasn’t happy about it. My GI said, “this is what happens when you’re healthy and finally absorbing nutrients.” When you’re planning a wedding, healthy weight gain hits a bit differently.
Ever since then, I’ve been in remission and I’m so grateful for that, but my weight has been something I think about now—not only because of my IBD being in check, but after having three kids. My self-confidence and how I feel about my reflection in the mirror has taken a blow as the years have gone on.
Madison: “ When I was in a severe flare in 2020 after being diagnosed, I dropped 20 pounds unintentionally. I was normally around 127 pounds and during my worst flare I was down to 107 pounds. It was absolutely horrifying. I was devastated. I remember going to American Eagle to buy shorts in a 00 size because none of my clothes fit me. I felt sick and looked sick, which made everything 10 times worse. Not being able to eat food and constantly running to the bathroom in pain led me to be malnourished. I remember being at my GI appointment when we were trying to figure out a treatment plan and my nurse said after taking my blood pressure, “Madison are you eating?” I started to cry to her and said “everything hurts me. I can’t eat.”
While Madison was growing up, she always thought being thin was attractive. After being so severely sick, she now personally affiliates being thin with being sick.
“Being on prednisone to help was both a blessing and a curse as it helped get my flare under control, but also led to unwanted weight gain in my face, which makes me super self-conscious, especially in pictures. I know that side effects are temporary, but it can really hurt someone’s self-esteem.”
Fast forward to now—three years later, Madison is on a treatment plan that works for her and she’s proud of her body. She says she looks forward to being weighed at the doctor and at infusions appointments just to see a healthy weight.
“Weight and IBD is very fluid, and I constantly remind myself to give my body grace. When you’re losing weight on top of being sick, it can be detrimental to your mental health. You look in the mirror and see someone you don’t recognize.”
Ashley: “I’ve kept three different sized sets of clothes with my ulcerative colitis. My normal size, a smaller size for when I’m extremely sick, and a larger size for when I’m on prednisone. I’ve always been super self-conscious about my body size because a lot of time it’s out of my control. I also feel self-conscious when I’m so sick and lose weight and people comment about how good I look. I’ve felt guilty because I didn’t work out to “earn” that body. Then, I’ve felt frustrated because it made me mad that to look a certain way that got me compliments, I had to be extremely sick and unhealthy. Now, I have a permanent ileostomy. I am more confident in my body than I have ever been. I think that’s mainly because I’m so healthy now and I have more control over my body and life.”
Danielle: “So many things come to mind. I was 14 when I was diagnosed, and while I was sick prior to being diagnosed, I was judged for being too thin and accused of being anorexic or bulimic. Then upon diagnosis, I gained 30 pounds in 2 weeks from prednisone. At 14 years old, I was swollen and chubby and self-conscious. Since being diagnosed, I haven’t struggled with being “too thin” again, but with weight gain from prednisone and other medications. I’ve been told far too many times that “anyone can lose weight by eating right and exercising” but it’s not that easy with a chronic condition. Some mornings, I’m so fatigued and achy, I can’t get out of bed, and it takes my energy to get ready for work. My diet is extremely limited as I had a bowel resection and I’m allergic to dairy products. So, I live off protein and carbs which are not ideal for weight loss or even maintenance.”
Amber: “I have been on Stelara and have reached remission, but the thing people don’t talk about is after being in constant flares, you have no idea how much weight you might gain because of not flaring. It is a great thing and I’m so happy to be in remission, but now I must learn how to work on the nutrition aspect of it all. To be honest, all these years of being sick, I never had to worry about weight gain. I had to worry how much weight loss affected me and most people do more posting about that. Not the up sides of remission, but also what we do now to get onto a new lifestyle change. We have to learn a whole new way of nourishing our bodies.”
Stephanie: “I have found that when I’m flaring at my worst, I lose weight from not being able to eat and my body not retaining anything that I eat. I get so many compliments about the weight loss, but it breaks my heart because I might look good to others, but I’m at my sickest.”
Jennifer: “It’s crazy to know how jarring it can be to see your weight fluctuate so much so fast. Diagnosed with UC about a year ago and went through a huge flare, lost like 35 pounds. I hated looking at my body because I was under 100 pounds as an adult woman. Fast forward to now and I’m back to my “normal” weight, but still have issues with how my body looks as weight came back. It’s softer and less toned than before. I’m sure it’ll get back to the place where I was, but what if it doesn’t? Our bodies can go through so much and I’m thankful for its resilience, but the mental toll the fluctuations can be a lot to try and manage and reflect on as we navigate this journey.”
Louise: “I’m newly diagnosed and dealing with my second flare. I worry about the impact it has on me mentally because I am happier with my body when I’m very ill, and unhappy with it when I’m on steroids and feeling better. It can’t be good for us. Negative comments (from my mother!) when my face gets chubby on steroids and compliments from people when I’m not eating and very unwell are difficult to process. I get angry when they compliment me on how well I look just because I’m skinny, because I feel like it minimizes how bad things are and how unwell I am. I also like it because I like being slimmer. It is so messed up! When I get my appetite back, I try to fight the cravings and then binge and then feel awful for it. I have never been this way pre-IBD. I was always fit and healthy and in control of my relationship with food. There’s also a weird part of me that wants to look thinner because it’s an invisible illness, I want people to see how unwell I’ve been, so they don’t think I’m lying.”
Louise said it felt good to let it all out and that she’s never said any of this. Coping with big health issues comes first, but this annoys her during quiet moments. Her sentiments ring true for so many of us.
Myisha: “I struggle with body image a lot. I’m naturally 127 pounds, but with prednisone I got to 210 pounds and no longer recognized the person I was staring at in the mirror. I cried for weeks unable to recognize myself. I still cry now and I’m down to 139. My clothes still don’t fit, and I still have clothes that are a size 12-14 because I know that prednisone is an ongoing possibility and that I might get back to that size if I have a bad flare.”
Jessie: “The constant weight fluctuations have always made me self-conscious. It messes with your head too because when you lose weight from a flare, people say “oh my gosh you’re so skinny you look great, what did you do?”…but then when you gain weight (from medications not from becoming healthier) no one comments and you’re just self-conscious about it.”
Celia: “Before I was diagnosed, I was happy with losing weight. I was 13 and hated my body. I remember I had my diagnostic colonoscopy and the day after I took a picture of my stomach, it was as flat as it’s ever been. I felt good about how I looked, but keep in mind I was barely 100 pounds and 5’5’. I felt awful and I was tired all the time. As I started Humira and was gaining weight, I missed my old (very unhealthy) body. I constantly am reminded by loved ones that this weight gain is good. I just returned to the weight I was pre-symptoms almost 4 years later and I feel good overall! I still struggle with how I look and have developed a connection between food, weight gain and loss, and pain from Crohn’s that I still need to work on, but I’m doing my best. As a 17-year-old, we all tend to struggle with how we look, and I need to remember all my body has been through and done for me.”
Kindra: “Along with IBD, I also have Primary sclerosing cholangitis (PSC), so when I flare or I’m unwell, I lose weight and I can’t do anything to keep it on. I will eat all day long and you can count my ribs and see all my chest bones sticking out. I get compliments from people who don’t know me well about how thin I am/how they wished they could eat like me, and I never quite know what to say. When I am healthy and can gain weight and I have to shop for bigger clothes, I get a complex thanks to years of the American media diet culture.”
Leah: “I feel like weight gain after a flare has been challenging. All the body yo-yo and knowing the weight coming back on is so healthy and just what your body needs, but I believe it can be tough at times.”
Kelly: “I’m scared to go below a certain weight in fears of having a flare, but on the backside, I feel unattractive for my partner and fight with self-image.”
Bloating is a bitch
Even in remission, bloating is one of my main IBD symptoms. I often tell my husband, friends, and family, “you can physically see my pain right now. Feel how hard my stomach is. I look like I’m 5 months pregnant.” The reaction is always one of shock, raised eyebrows, and a bit of sympathy. Because of this I usually wear elastic waistbands or dresses. You’ll rarely ever see me wearing pants or shorts with a button. When I used to work in corporate America, my Crohn’s was out of control, and I would repeatedly have to unbutton my pants in the board room and lean back in my chair during meetings with co-workers. It was humiliating, but I always tried to make light of it. It’s amazing how we can wake up with a flat stomach and have a distended belly that truly looks like there’s a pregnancy going on by dinner.
Courtney: “Being emaciated from poor nutrient absorption, but bloated from gas and inflammation at the same time can lead to a confusing relationship with food. I don’t think it’s quite the same psychology as an eating disorder, but when eating causes you pain, or makes you literally change your pant size pre and post meal, it can be easy to want to postpone meals if you have plans, eat little in social situations, and can create an unhealthy relationship with food. Food is not the enemy, it’s a necessity—it’s all about finding the proper treatment and lifestyle to manage your IBD.”
Courtney adds that living with an ostomy is a huge adjustment with major impacts on how you perceive your body and appearance.
“My first ostomy was such a shock to the system. It feels almost surreal to see a piece of your intestine outside your body. If you have no control over output timing, which can leave you feeling broken and helpless during bag changes. It wasn’t until my second ostomy that I was able to recognize and be grateful for the benefits it affords me. I now live a healthy, active, pain-free life and couldn’t be more grateful.”
Patti: “My everyday bloated belly is like a giant dark cloud that blankets my self-image. I really try to embrace the rest of my healthy body and be grateful that I’m able to leave the house and do some functional activities and can sometimes hide my ugly belly if I’m completely emptied out, but my typical mantra is that I look disgusting because of my belly. I know this is negative thinking and messes with my mental health, but after dealing with Crohn’s for the past 51 years, I’m not sure I can ever stop that thinking.”
Alyson: “Bloat makes a girl feel AWFUL. Add in intestinal dysmotility with Crohn’s and I literally start the week at a size 8 and end in a size 10. Then we just switch to those wide leg pants with the elastic. Prior to my diagnosis, I never had to unbutton pants before or after eating. Now, it’s the first move the second we get in the car to leave because, ouch. It really makes you feel cute.”
Alannah: “For me weight fluctuation is my biggest struggle. One week I’m slim with minimal bloating then the next I’m bigger and bloating more. My partner has always struggled with confidence with his stoma due to weight gain even though he’s perfect as he is. He will never go without a top off ever.”
Naima: “Bloating is the worst. I am getting married in three weeks and I’m so worried about being bloated or gassy or having a minor flare. It’s hard to feel pretty when you can’t control how your body is feeling. Some days I feel strong and look lean—other times I hate how I look.”
Post surgery swelling, scars, and ostomies
Sabrina: “I’ve struggled with my body image after being diagnosed and going through three surgeries in a matter of two years. Seeing myself with a bag was hard and the changes that came with post-surgery swelling, scars, and fluid buildup. Body image and my new body will always be something I struggle being comfortable with.”
Mark: “I’ve had Crohn’s for more than 37 years and in that time multiple operations. I have many scars, but they are a part of my life and badges of honor in my constant battle with this disease. My IBD has thrown everything at me including short bowel syndrome, liver failure, osteoporosis, broken vertebrae, septicemia, lymphoma, coma, hepatic encephalopathy, and the list keeps growing. When I see my scars, it reminds me to keep fighting. Crohn’s will not win or stop me from living a full life. If someone asks me about them, I don’t hide. I tell them it’s battle scars. Body image is important to me, and it reflects how strong I am, and no one can take that away. I’ve worked all my life and traveled the world. This year (one year after coming out of a coma) I’ve been on a Pole-to-Pole journey.”
Martin says body image is both how you feel and how you look to others, as well as yourself in the mirror. In his early days post-diagnosis, as a young adult starting a career, he felt anxious and angry, but looked normal.
“Post surgery and with time came the additional stress of looking and behaving differently and additional comorbidities that accompany IBD. This included dental and bone issues. I was hugely lucky to have found my lifetime soul mate before my Crohn’s became active, illness and surgery haven’t changed anything for us. I have been various shades of ill with Crohn’s all my adult life and it hasn’t helped self-love, including self-image on any level. I survived and thrived because of my family’s support and very little real-world commentary on my body from others, although I sometimes preempt this by joking about looking like Homer Simpson these days. I now face further life changing surgery and I worry about the impact of my quality of life on my family. I no longer care about how others see me.”
From a caregiver perspective
Cindy: “My daughter is so deeply at war with her body, and I know thanks to chronic illness it’s so much more complex than simple teenage-girl-in-the-age-of-Insta feelings of “I don’t like my shoulders” or “I should watch my calories” (both of which are things she thinks). It is rooted in a real fear of and discomfort with her body and what it puts her through. She has so many years to live in her body and I wish more than anything I could give her peace with it…the same relative peace and confidence I have always had with my body. I just can’t relate.”
Keyla and her teenage son have IBD: “The struggle is real. Not only do we have a condition that there is stigma about, then we have constant weight issues, scars, bruising, and so much more that leaves us with body image issues. Our bodies have been through enough and done so much for us. Let’s care for it, nourish it, nurture it, and be kind to it.”
Taking on body image one day at a time
Focus on strength and resilience. Recognize your ability to navigate through challenges and adapt to changing circumstances. Once you’ve been through the flare and recovery process once, you know what to expect. Find comfort in knowing you’ve done this before and know most of the unpleasant side effects are temporary.
Seek support. Surround yourself with a strong support system of family, friends, or support groups who understand and empathize with your experiences. Sharing your thoughts, concerns, and emotions with others who have similar experiences (hello online IBD fam!) can help you feel heard and supported. Surround yourself with people and media that promote positive body image and self-acceptance. Be selective in the content you consume, ensuring it supports a healthy perspective and challenges unrealistic beauty standards.
Educate yourself. Learn more about IBD and its impact on the body. Understanding the reasons behind changes in your body and recognizing that they are a result of the disease, not a reflection of your worth, can assist in developing a more positive body image.
Practice self-care. Engage in activities that promote self-care and boost your self-confidence. This can include hobbies, exercise, meditation, or anything that brings you joy and helps you connect with your body in a positive way. Oftentimes our fatigue can hinder what type of daily activity we feel capable of, take everything in stride and don’t overdo. Start with a 10-minute walk and build up from there. The fresh air and simple movement will do wonders.
Focus on what your body can do. Shift the focus from how your body looks to what it can do. Appreciate the functionality of your body, such as its ability to heal, fight illness, and carry you through daily activities.
Reece was diagnosed with Crohn’s disease in 2014. Since then, he’s endured countless surgeries, flares, and setbacks, but chooses to focus on the beauty his life still bestows despite the challenges.
“I’m a shell of my former self, but I am okay with it. I’m grateful for my life. I have people who love me and care for me. When I look in the mirror, I see a fighter. All of the marks and scars are just evidence of my battles. It was not easy to get here, but here I am. I will never be the person I was before Crohn’s, but my disease has taught me so much about myself and life.”
Communicate with your healthcare team. Discuss any concerns or insecurities related to body image with your healthcare team. They can provide guidance and offer resources to support you in addressing these concerns. Therapy may help you cope with these struggles and provide helpful tools for living with the uncertainties and challenges.
Remember, your worth is not defined by the physical changes caused by IBD. Surround yourself with positivity, celebrate your strengths, and prioritize self-care to foster a positive body image and improve overall well-being. Most importantly, after reading this I hope you feel seen and realize that your struggles and insecurities are not unique to you.
There’s not a magic bullet for helping us cope with these insecurities, I know it can be a daily challenge. I truly believe we are our own toughest critics. If family members or friends compliment you when you’re unintentionally thin, respond by saying it’s because your IBD is out of whack. Speak up and inform those who have no idea what’s going on in your mind, with your body, when you look in the mirror, get on a scale, or have to think about how your outfit choice could impact your physical symptoms every day…it’s a lot. You are beautiful. You are strong. You are capable. There’s no one like you in the world. Your body, no matter the size, is working overtime with IBD, please take a moment to show yourself and it, some love.
Healthcare for those with IBD in the LGBTQIA+ community looks a bit different. IBD often affects young adults, many of whom are just beginning to become comfortable in their sexuality and gender identity. This can be especially hard for LGBTQIA+ folks, who have already had to work through stigma and discrimination, and then have the additional burden of a new diagnosis of IBD. The LGBTQIA+ community is a big, diverse group of people and each person is unique.
This Pride Month on Lights, Camera, Crohn’s a close look at the most common concerns and patient experiences, helpful guidance to support the LGBTQIA+ community, tips for finding and communicating with your care team about your sexual orientation, and exciting news about how the University of California-San Francisco Medical Center is working to provide a safe space for patients.
You may not be aware that IBD symptoms can affect sexual function, colectomy and J-pouch surgeries can impact receptive anal sex, transgender people with active pelvic inflammation may have issues undergoing bottom surgery as part of gender affirming, and much more. The mere act of communicating with your care team can be an overwhelming and daunting experience.
Coming soon: An IBD Clinic specifically serving the LGBTQIA+community
Dr. Justin Field, MD, University of California, San Francisco, is passionate about supporting IBD patients who are part of the LGBTQIA+ community, as a gay man himself, he’s on the forefront of making the UCSF Medical Center one of the first in the country to have an IBD clinic geared towards treating IBD in the LGBTQIA+ community.
Currently there are two other clinics in the U.S. that specialize in treating LGBTQIA+ IBD patients, the Mayo Clinic in Rochester, Minnesota, run by Dr. Victor Chedid and Capital Digestive Care in Washington D.C. Dr. Jessica Korman, MD, specializes in LGBTQIA+ patients with all GI issues, including IBD. She also does anal cancer screenings.
“The clinic at UCSF is set to open this Fall and will offer comprehensive IBD care to anyone who is interested and will be a safe and inclusive environment where everyone involved in patient care will have special training in the unique needs and concerns of LGBTQIA+ patients. The clinic will offer screening for anal cancer, which is increased in patients with IBD, in men who have sex with men (MSM), patients living with HIV, those who have receptive anal sex, patients with prior cervical or vaginal cancers, and in those on long term immunosuppression,” said Dr. Field.
The clinic will also offer coordination between Gastroenterology and other specialties such as Colorectal Surgery and Transgender Care. For people who are interested, UCSF will offer the ability to participate in research that adds to the knowledge base about the unique needs of LGBTQIA+ people who have IBD.
“This clinic came from the realization that LGBTQIA+ folks often have unique needs that aren’t always addressed in other traditional settings. Also, patients often feel hesitant to fully discuss their sexual orientation and gender identity with healthcare providers due to fear of stigmatization or being treated differently. I wanted to create a safe space where patients can feel comfortable and empowered to be open with their healthcare team, and where they can receive the relevant expertise to meet their needs,” says Dr. Field.
Because LGBTQIA+ people have so often been left out of research (by not including sexual and gender diverse identities in research studies), having a dedicated LGBTQIA+ IBD clinic helps improve medical knowledge about how IBD affects LGBTQIA+ individuals, by allowing more patients to choose to participate in research.
“I have received incredible support from the University of California – San Francisco to start the clinic. The clinic continues to be a work in progress, and I’m continuing to seek out a wide variety of patient and provider input to ensure the clinic effectively serves the community,” explained Dr. Field.
Living with the stigma of IBD and being LGBTQIA+
CC Springhetti was diagnosed with ulcerative colitis when she was 12. She’s has an ileostomy and says sometimes she jokes that the universe keeps punishing her with stigmatized labels.
“I’m a woman, gay, AND I have a disability now?! In all seriousness, I try to view all my labels as gifts. They each make me who I am, and though it’s taken me some time to get to this point, I’ve learned to be proud of who I am and what I have. I know that sharing my life helps normalize and de-stigmatize IBD and queerness. Representation is so important, and being able to show up exactly as I am to show that you can be queer with IBD and still live a full life is a precious gift I have been given.”
CC and her wife share their life online and have been the target of extreme hate and prejudice. They’re received hundreds of threats.
“It can be draining to keep up with the amount of comment/message removal needed to keep our internet pages safe for young viewers and it’s incredibly disheartening on a regular basis. I sometimes give myself several days away from social media just to clear my mind – the hate and threats cause so much stress, and it can be difficult to separate internet life from real life. Those of us with IBD know how stress can affect our bodies, so this is a constant issue I am still working through every day.”
CC says when she’s admitted to the hospital, she’s dealt with the stress of her partner not being taken seriously of being allowed to make big decisions during emergency situations.
“We live in the south in the United States – it sometimes can be difficult for us to know who is able to separate their work life from their personal beliefs. When you’re in a hospital setting there really is no knowing, and this is something we always try to stay vigilant about and are very communicative with our care teams about what our needs and wishes are.”
The impact of IBD on sexual function
Brad Levy started to experience IBD symptoms in January 2022. He was diagnosed with Crohn’s the following month. His dad has ulcerative colitis, which sped up the diagnosis process significantly. Along with having Crohn’s Brad is a married gay man and a dad. Shortly after his diagnosis, Brad started to worry about how his disease would impact not only his life in general, but his intimacy with his husband.
Dr. Field explains why IBD can have such a big impact on the sex lives of LGBTQIA+ people.
“Receptive anal sex is an important part of sexuality for both LGBTQIA+ and non-LGBTQIA+ people but is especially important in this community. IBD often involves inflammation around the anus or in the rectum and this can make sex difficult or painful. For transgender folks, active inflammation in the pelvic area can affect their ability to undergo gender affirming surgery, so it’s especially important to address any pelvic inflammation.”
Brad says, “There is some shared stigma around IBD and being a gay receptive partner. Specifically, within the gay community there can often be some unrealistic expectations about how “cleaned” out you should be before engaging in receptive sex. The reality is though that shit happens, quite literally. The shame and judgment around a critical and natural bodily function such as elimination needs to end.”
Overcoming the fear of judgement and finding a care team you can openly communicate with
Talking about sex, sexual orientation, and gender identity can be scary as a patient, because often those in the LGBTQIA+ community have prior experiences telling people about their sexual orientation or gender identity which may have been met with rejection or judgement.
“Historically, the medical community has treated the LGBTQIA+ community poorly and considered LGBTQIA+ identities as pathologic. This historical context is important because there are very logical reasons patients aren’t comfortable talking about this with their doctors. In some areas, it truly isn’t safe for LGBTQIA+ individuals, especially the trans and non-binary community,” said Dr. Field.
Now more than ever, there are lots of affirming healthcare providers. Individual providers and practices can take measures to ensure a LGBTQIA+-friendly healthcare setting (For example, by following these recommendations put forward by the American Medical Association.
Demonstrating to patients that they are in a safe space to talk about their sexuality or gender identity can go a long way in facilitating sensitive conversations. Providers can seek additional education on sexual health in gender and sexual minority patients, so that they feel more capable of addressing the needs of the IBD community.
Dr. Fields says, “Providers should know it’s ok to make mistakes when it comes to addressing diverse sexual orientations and gender identities. What’s most important is that we acknowledge the mistake, apologize, and move on.”
CC is a firm believer that your doctor should be someone you never lie to. Honesty will help you navigate problems and solutions in a sensitive manner.
“I remember I was nervous to share with my gastroenterologist that I was gay. Whenever I referred to my partner and he responded back to me with questions or comments, he would always say “boyfriend” or refer to my partner as “he”. It felt scary to correct him (especially after all of these years) so I just didn’t. I was nervous it would embarrass him or make him feel silly, and I always want to protect people from that when I don’t feel they deserve it,” she said.
Then one day, CC was at a different doctor and she made sure to share to share that she was married to a woman and had been in a same-sex relationship exclusively for a number of years.
“I had this doctor add this information to the top of my medical chart. Now when I go to any doctor and they pull up my chart, they can see that I’m gay and can provide sensitivity to me in that way when speaking to me.”
Seeking out LGBTQIA+ affirming healthcare providers
Patients can feel empowered to seek out LGBTQIA+ affirming healthcare providers like Dr. Field.
Find providers with a special interest in LGBTQIA+ health. Patients can also look at lists such as the LGBTQIA+ Healthcare Directory.
Patients should feel empowered to be their own advocate. It’s a patient’s right to have their sexual health needs met and to receive care that is affirming of all genders.
Patients can bring a list of items that they want to discuss to a visit, and it’s best to mention those at the beginning of a visit to help set the agenda. It’s also always ok to seek a second opinion if you feel like your provider hasn’t gotten a satisfactory answer to your questions or if you feel another provider perspective would be helpful.
“Having a GI doctor you trust and feel comfortable enough to discuss your sexuality with is so important. When having receptive anal sex, things happen sometimes, such as tears, and you want to be able to talk with your GI doc openly so you can triage whether something is related to your IBD or not,” said Brad.
Additional IBD screenings for the LGBTQIA+ community
According to Dr. Field, men who have sex with men that are living with HIV should be screened for anal cancer.
“Other at-risk groups for anal cancer are men who have sex with men over age 40, people with prior cervical or vulvovaginal squamous cell cancer, patients that have receptive anal intercourse, and those with multiple sexual partners,” he said.
The risk of anal cancer is increased in patients with IBD, and doctors are continuing to learn more about this risk through ongoing research studies. Screening for anal cancer is with a rectal exam and a swab of the anal canal, called an anal pap smear. If these are abnormal, they must be followed by a procedure called a High Resolution Anoscopy, which is the best test for detecting anal cancer and its precursor.
“Anal cancer is caused by HPV, and there is a vaccine against HPV. Anybody who has not received the HPV vaccine, regardless of age or gender, can talk to their doctor about HPV vaccination. Currently, the CDC recommends HPV vaccination regardless of gender up to age 26 to prevent HPV related cancers, and the vaccine can be given up to age 45 on a case-by-case basis, if it’s felt it would benefit,” said Dr. Field.
Brad lives in the Chicago suburbs. As a result, he says the attitudes towards the LGBTQIA+ community are generally that of acceptance and love.
“I have always had a gay primary care physician because I want to make sure I am comfortable discussing any health issues with them. My GI is also aware of my sexuality, and we’ve had candid conversations about what intimacy looks like during a flare and what vaccines I should consider. For example, my GI recommended I receive the Gardasil HPV vaccine based on my sexuality and increased risk.”
Other cancer screenings to keep in mind are Colon cancer screening for all patients, Cervical cancer screening for patients who have a cervix, and skin cancer screening for all patients who have received immunomodulators, small molecules, and biologics.
“Much of the existing research on things like sexual health and surgery in IBD didn’t ask participants about their gender identity, sexual orientation, or typical sexual practices. This can leave both patients and providers at a loss for answers to sexual concerns,” said Dr. Field.
More and more, sexuality and gender identity are being included in research studies, and this will paint a clearer picture about how many LGBTQIA+ people are impacted by IBD, and how the course or experience of IBD is similar or different between LGBTQIA+ and non-LGBTQIA+ individuals.
Juggling a love life and fatherhood with IBD
Brad and his husband have been together for 13 years, so luckily communicating about his IBD has come easy.
“But I can recognize for others, in shorter relationships or dating, this isn’t always the case. All I can recommend is transparency and having a partner you feel you can be honest with. There will be times (such as a flare) where intimacy will look different. You want your partner to know that it’s because of your IBD activity and not because of them or some issue with your relationship,” said Brad.
As the years go by, Brad says the more authentically he lives, the happier he is. For him, that means living as an out gay man who has an amazing family. It also means living with Crohn’s disease, Anxiety, and Depression. Brad is open about his health struggles with family, friends, and close colleagues/bosses. He says transparency has served him and his relationships well.
As an IBD Dad to a five-year-old girl who is on the spectrum, Brad says focusing on self-care to help manage stress makes all the difference.
“Focusing on self-care enables me to show up as an active and healthy dad. My self-care includes hopping on my Peloton (#ThatDadBrad for the Peloton readers), bi-weekly therapy, monthly massages, and getting my nails professionally done. While not all these activities are for everyone, I strongly encourage folks to pour into their own cup or put on their own mask first. You can’t fully show up for you me kids and your family if you’re not grounded and the healthiest version of yourself, whatever that looks like for you.”
Brad wants to reiterate that his experience as a cis gay white man is “only one voice (and a privileged one at that) out of the vast and vibrant LGBTQIA+ community.” You can connect with Brad on Instagram at: @bssl.
CC says there are a number of ways our IBD community can show support. You can follow CC on Instagram at: @ccspringhetti.
“We’re all human, and I would encourage the IBD community just like I would encourage any community to show your support during Pride month and all year long through any means appropriate for your situation. Support LGBTQIA+ owned businesses, hang a Pride/Progress flag, post your support on social media, or even attend your local Pride events! If you’re ever looking to support a good LGBTQIA+ charity, I always suggest The Trevor Project.”
Certain roadblocks and issues that are a concern to one person, may not bother another. Just like every IBD patient, regardless of sexuality, the experience is unique. We all need to feel seen, understood, and respected, as one united IBD family.
Dr. Field’s views are his own and do not represent the University of California San Francisco.
I remember the first phone call when I was pregnant with my oldest as a soon-to-be IBD mom. A researcher from Mother to Baby called me when I was newly pregnant and leaving work—I sat in my car in a parking lot, as she asked me several questions about my health, well-being, medication, and pregnancy thus far. That was Fall of 2016. Fast forward to now—and my oldest, Reid, just graduated from kindergarten. When I was diagnosed with Crohn’s disease at age 21 in 2005, one of my biggest fears was whether my chronic illness was going to rob me of motherhood. Back then, I was nowhere near ready to settle down, but the worry was always in the back of my mind.
When my husband and I got married in June 2016 and I was 10 months into surgical remission, we knew we needed to capitalize on my IBD finally being under control. Luckily, we got pregnant one month after getting married. Shortly thereafter, I started researching pregnancy studies for IBD moms. Lights, Camera, Crohn’s launched two days before I received a positive pregnancy test. I was fresh into my advocacy and had never been pregnant before. I didn’t have a community of IBD moms to lean on for questions or support as I navigated the unknown.
I came across information about Mother to Baby online and ended up being a part of their pregnancy studies for my first two children. The studies were different, but I had such a positive experience with Reid, that I decided to participate again with my daughter, Sophia. Reid’s study was a 5-year look at how Humira impacts babies in utero through kindergarten. When I was initially pregnant with him, this felt light years away. And here we are. Over the course of his pregnancy and until November 2022, I completed surveys, did phone interviews, had an in-person meeting with a doctor who came to my home and looked him over in front of me for any health anomalies, and most recently did an in-person cognitive neurobehavioral assessment at a nearby hotel with researchers.
We just got the results. While it’s rewarding to participate in IBD studies and interesting to learn, there’s always a part of you that worries about the findings and if mom guilt will ensue. It’s been reassuring and comforting to see my healthy kids, who were exposed to Humira in utero through the 3rd trimester, thrive and excel with milestones and in school.
The findings of the study
In November 2022, Reid and I met up at a nearby hotel with two researchers who provided neurodevelopmental behavioral evaluations for both of us. Reid’s assessment used a series of questions, games, and puzzles to help researchers determine his development of language ability, memory skills, and problem-solving abilities. The tests were selected to provide an evaluation of general mental ability and to describe specific abilities in areas of verbal knowledge and reasoning and visual-perceptual reasoning and organization. The tests were intense, I was proud of him for how he handled himself during the process.
Reid and I waiting to do our assessmentwith research administrators
According to Mother To Baby, “this battery of tests is best suited to examine the similarities and differences among groups of children. While it was not adapted for Reid’s individual characteristics, it can highlight general strengths and weaknesses in a child’s cognitive profile and indicate potential concerns when present.”
Behavioral Observations: “Reid was personable and interacted with both administrators on his arrival. He had a very positive attitude toward testing and quickly became comfortable with administration. He was engaged and attentive to the materials, listened attentively to the examiner and provided effortful responses even as questions became more difficult. Reid demonstrated good cooperation and attitude by following instructions and requiring minimal to no redirection from the administrators of his mother. He was focused and friendly for the full duration of testing.”
Summary of Assessment Results: “Tests were administered in a single testing session with one short break. The Wechsler Preschool and Primary Scale of Intelligence (WPPSI-IV) was selected to provide an evaluation of Reid’s general mental ability and to describe specific abilities in areas of verbal knowledge and reasoning and visual-perceptual reasoning and organization. This battery of tests is best suited to examine the similarities and differences in ability among similarly aged groups of children. While it was not adapted for Reid’s individual characteristics, it can highlight general strengths and weaknesses as well as potential concerns when present.”
The intelligence test was comprised of 10 subtests which measured a variety of verbal and nonverbal skills. Reid achieved a composite score in the average range. In the working memory category and spatial working memory, Reid performed in the high average range, which required him to remember and identify pictures that had previously been shown to him. On tasks that measured visual-spatial abilities, Reid scored below average. These tasks required him to synthesize visual stimuli to recreate block design.
“Reid was highly focused while processing visual stimuli. Overall, Reid is a bright and enthusiastic child. He was a pleasure to work with.”
Along with Reid’s assessment, I was also interviewed and performed tasks with an examiner on the other side of the room. I was assessed in the adjustment and life context. Tests included the Center for Epidemiological Studies Depression Scale and Parent Stress Index. My scores were within normal limits and my general mental ability also scored in the average range. Not gonna lie, the testing was challenging!
Reflecting on my experience
As an IBD mom of a 6-year-old, 4-year-old, and 22-month-old, who participated in pregnancy research during each of my pregnancies, I can’t begin to tell you how incredibly rewarding it is to know that your personal experience is helping to drive the future of care for women in our community who have hopes of one day being a mother. Sure, it takes a little bit of time and effort, but the data and research to show the safety and efficacy of medications while pregnant and breastfeeding is so needed. It’s comforting to know Reid is right where he needs to be cognitively and healthy physically, despite my high-risk pregnancy and exposure to Humira until 39 weeks gestation. We need more women to willingly step up to the plate and share their journeys to help guide the future of IBD motherhood and show all that’s possible despite our disease.
Opportunities to participate in research
Many people need to take medication during pregnancy to manage and treat their IBD. Yet, according to the Mother To Baby website, fewer than 10% of medications have enough information to determine their safety for use in pregnancy.
Do you have Crohn’s disease? Are you currently pregnant? If you answered “yes” to both questions, you may be able to help Mother To Baby advance the knowledge of how managing IBD in pregnancy impacts a developing baby. Click here to learn about how you can impact the health of future families by joining the Crohn’s Disease and Pregnancy Study.
Parenthood when you live with a chronic illness like IBD can make you feel anxious, worried, and uneasy. As an IBD mom of three, I often connect with and share the stories of fellow women with Crohn’s disease or ulcerative colitis who have brought life into this world, despite their disease.
This week on Lights, Camera, Crohn’s we hear from a soon-to-be IBD Dad, Brad Watson-Davelaar. He was diagnosed with Crohn’s in 2001 at age 17. His name and face may look familiar, as I featured him in an article entitled: IBD Dads: What these patient heroes have to say about fatherhood. In that article, Brad was recently married and discussed his hopes for the future. Those hopes came to fruition, as he and his wife are awaiting the arrival of a baby girl in late June!
Leading up to the pregnancy, Brad was a bit scared of what fatherhood would look like while living with an unpredictable disease. Like many of us, Brad fears when his IBD will rear its ugly head again and cause him not to be as present as he wants to be, hindering his ability to be a “proper teammate” for his wife.
“Prior to my wife being pregnant, I think I was scared. I’ve wanted to be a dad for some time, but with the way my health has been over the last several years, the prospect of having kids while I was in that physical state freaked me out. Not because I didn’t want kids, but because I was worried I wasn’t going to be enough for them.”
Finding out he was going to be a dad
When Brad found out his wife was expecting he was elated. They had been trying for a few months and he was only a couple months post-op from his ileostomy and barbie butt surgery. While Brad knows life as an IBD Dad will have its ups and downs, he knows the highs will far outweigh any of the difficult days.
“I’m so thankful for Shawn, my stoma, for coming in and giving me a new lease on life. I feel ready to tackle this new chapter of our life and all that comes with it. The good, the bad, the ugly, and the beautiful.”
Since he’s lived with IBD for nearly 22 years and has been an ostomate for 6 months, Brad feels his patient journey has conditioned him to deal with the unexpected. He hopes to connect with fellow IBD dads who have paved the way before him and shown all that’s possible.
Discussing IBD with his daughter in the future
As his daughter grows up, Brad plans to be an open book about his battle with Crohn’s.
“I want to help her understand what IBD and ostomies are. Especially ostomies. It will take time, but I believe in being open and not hiding things. I want her to see that my IBD does not define me and show her how important it is to advocate for yourself.”
As Brad and his wife gear up to become a family of three, they are overjoyed and excited about the new chapter in their lives that is about to begin.
“I’ll be there to look after this wee little one, which will fill my heart with warmth. Being able to focus on her achievements will be a brilliant way to get through the rough days. In the past, it was the little things that got me through. Now, I’ll have all the little moments to continually push me.”
His wife, Sydney, feels so lucky to have Brad by her side as they experience this adventure.
“He had struggled so much over the last couple decades, especially these last couple of years and his perseverance and strength through it all makes me know that nothing is too big for him to overcome. I know he is going to be an amazing dad with so much love, nerdiness and laughter. His Crohn’s is a part of him, but his IBD does not define him. I know no matter what we can get through it together. Brad’s last surgery has definitely given him a new lease on life. With a baby on the way, his ostomy will help him be more present, active, playful, adventurous and helpful. I cannot wait to see him hold our little girl for the first time,” she said.
Mental health often takes a major hit when you’re diagnosed and live with a chronic illness like IBD. I ran a poll on Instagram and Twitter this past week and the results were extremely eye-opening. Not only for the patient community, but for any caregivers, friends, or family who know people with Crohn’s disease or ulcerative colitis.
On Instagram—out of 350 people polled over 24 hours, a resounding 93% responded “yes” to IBD impacting their mental health and causing depression and anxiety. On Twitter, I ran the same poll for 48 hours, of the more than 205 votes, 86% of people responded “yes”.
Dr. Yezaz Ghouri, MD, Director of Inflammatory Bowel Disease Services, University of Missouri School of Medicine at Columbia, offered helpful insight on the topic. I had the pleasure of meeting “Dr. ZaZ” (as he commonly goes by) in person at the Crohn’s and Colitis Foundation’s Mid-America Chapter Gala in November. Dr. ZaZ was awarded the 2022 Catalyst for Mission Advancement award and I was so inspired and intrigued by his work as I was emceeing the event, that I knew we would have to collaborate on Lights, Camera, Crohn’s! We made it happen.
Here’s my interview with Dr. ZaZ about how our IBD can impact our mental health.
NH: “During the first day of the Crohn’s and Colitis Congress 2023 conference it was shared that rates of anxiety and depression are about twice as high in the IBD community compared to the general population–why is that?”
Dr. ZaZ: “The exact cause of IBD is not known. There are some common theories that have been suggested, these include genetic factors, changes in gut microbiome, alteration in immune function of the body, and effect of certain environmental factors. Interestingly, some of these factors have also shown to be associated with mental disorders like anxiety and depression. The gut-brain axis is a nervous system-based pathway that connects the nerve cells from the brain to the gut. This gut-brain axis has been found to play a role in the release of nerve cell chemicals (or neurotransmitters) in the intestines. One such neurotransmitter is Serotonin, which has a well-established role in several psychiatric disorders like anxiety, depression, bipolar disorder, etc. Studies have pointed out an alteration in serotonin activity in the intestines of patients with IBD 1.
The gut microbiome comprises of trillions of species of organisms mainly consisting of bacteria. The healthy gut-microbiome is altered in individuals with several conditions like anxiety, depression, Alzheimer’s, Autism, etc. This alteration is also seen in IBD and has been a subject of active research to better understand the various changes in the bacteria of the gut. Some of these bacteria produce chemicals that can serve as neurotransmitters in the gut. It is unclear if these chemicals could influence the gut-brain axis and contribute towards the occurrence of mental disorders. Last year we published a study that showed this association of increased prevalence of anxiety and depression among IBD patients 2. The added burden and distress was not just limited to IBD patients, the study also showed an overall increased healthcare cost and burden to hospital systems. It is in the best socio-economic interest of the government and the public to address mental health issues in society, especially among those with chronic illnesses like IBD.”
NH: “How can patients best articulate their concerns and communicate with their doctor about their mental health?”
Dr. ZaZ: “IBD patient sometimes suffer from anxiety, depression, sleep disturbances, and other mental conditions like eating disorders. Your GI doctor hopefully has established a healthy physician-patient relationship where you are comfortable to bring up any issues that you would like to discuss with your GI specialist. During my clinic visits apart from addressing the medical aspects of IBD, I frequently have a friendly conversation about my patient’s life in general with a focus on their overall well-being, including talking about their mental health. In addition, several individuals have a primary care provider (PCP) with whom they generally have a good relationship and feel comfortable bringing up any health-related concerns.
Psychiatric conditions can manifest with sleep disturbances, fatigue, loss of appetite, lack of interest in activities that you previously enjoyed, depressed mood, suicidal thoughts, etc. Sometimes IBD flares can contribute to some of these symptoms, especially sleep disturbances due to night-time diarrhea or constant abdominal pain. Use of biological medications can be frequently associated with fatigue that may last a day or two after taking the biologic. In a large-scale UK based study, presence of a diagnosis of IBD was associated with a higher likelihood to cause deliberate self-harm, anxiety, depression, and insomnia. Interestingly, the risk was higher among those with Crohn’s disease than with ulcerative colitis 3.
Remember, mental stress can also contribute to an IBD flare. Frequently I see some of my IBD patients go through an uncontrolled spell of psychological stress, maybe related to personal relationships or their place of employment. This when unchecked can precipitate an IBD flare, and in some cases develop psychiatric illnesses like anxiety or depression. Hence, it is important to have a stress-free life or mitigate stress to minimize its effect on your mind and body.”
NH: “I know you see a lot of college students; how do you navigate these concerns as their care provider? Do you tend to see this more with your younger patients—or is it across the board?”
Dr. ZaZ: “College life of a freshman can be quite stressful. The move away from the comforts of their homes to a new city or town and being surrounded by strangers can be overwhelming. This can cause psychological stress which may precipitate an IBD flare. Moving to college can also disrupt the continuity of care received from their established pediatric or adult GI specialist. Students may skip their medications due to storage issues, changes in insurance, feeling of shame of having IBD or fear of not being able to ‘fit-in’. All these factors can contribute to inadequate management of their underlying IBD. We at the University of Missouri try our best to accommodate college students in our clinics so they are cared for and IBD flares are prevented from occurring. The student health clinics are efficient in recognizing students with chronic illnesses and referring them to GI clinics. I frequently encourage students that they continue to see their primary GI specialist but also establish care in our clinic/hospital system, so in case there is a medical emergency or if they experience a flare, we will be well-informed beforehand about their medical history and have a plan in place to adequately treat them.
In a large study comprising of more than one million IBD patients, it was shown that being a female, having diagnosed with IBD as a child or a young adult and having a diagnosis of Crohn’s disease have been associated with higher likelihood of suicide attempts and suicide death 4.
Mental disorders in IBD are seen across all age groups but are somewhat more pronounced in those individuals whose disease is not well controlled or have not achieved remission since their initial diagnosis. Majority of IBD cases are generally diagnosed at a young age, several times in college students. Unfortunately, we also see frequent occurrence of mental disorders in younger age groups. Students have additional mental stressors when they have a chronic bowel condition like IBD. Many feel that they the lack of freedom in choosing to eat anything they like when they go out with friends or their need for frequent bathroom breaks, which can sometimes hinder them from participating in activities they choose or in making new friends. Many feel embarrassed to disclose their medical conditions to new friends or acquaintances, this perhaps cannot be stressed enough among those with an ostomy bag.
This leads to a state of inadequate social/family support which may push at risk students into developing mental conditions like depression, anxiety or eating disorders.”
NH: “Any advice for caregivers of young patients–who may have concerns about their child/teen/young adult and are unsure how to make sure their child is not dealing with anxiety/depression, but don’t want to overstep or upset their loved one?”
Dr. ZaZ: “It is very important for not just the physicians but also the caregivers involved in managing IBD in young patients to recognize signs of depression or other mental disorders. Do not always assume that if an individual is constantly tired, has disturbed sleep or looks depressed, that it is due to their IBD. Several times these are early signs of depression, and these young individuals need the support and help that they deserve to address these issues. Perhaps adult patients who have depression may recognize it and seek help, but kids or teens generally do not perceive these signs as an abnormal expression of behavior and may not even disclose them to their loved ones. Caregivers who attend clinic visits with pediatric specialists should bring up any unusual behavior they notice about their child and discuss it with the provider.”
NH: “How can mental health issues exacerbate IBD symptoms?
Dr. ZaZ: “Studies have shown that individuals with mental disorders who have IBD have a higher chance of developing IBD flares, they require escalation of their therapy and have increased incidence of death 5. (See Reference 5) This is quite alarming and should be brough to the attention of providers who take care of IBD patients. “Providers are not just prescribers”, simply writing prescriptions for medications, some of which are very expensive, is not enough to heal the patient. IBD is a chronic disease which lasts a lifetime, and medications alone cannot be the solution. Providers need to step up and participate in the mental well-being of their patients. If they are not able to address the mental health related issues themselves then referring to experts in the field is perhaps the best alternative approach. Depression may cause patients to skip their infusion visits or physician visits, uncontrolled anxiety or paranoid states may make them apprehensive about any therapy that they have been appropriately prescribed and may even stop the treatment. IBD patients with eating disorders may starve themselves or eat uncontrollably causing worsening of their bowel condition. These eating disorders are commonly present among young and female IBD patients who have body image disturbance 6.”
NH: “How is anxiety and depression typically managed in patients with IBD? (Medication, talking to a psychologist, etc.?)”
Dr. ZaZ: “The first step to treating anxiety and depression is to approach a provider with whom you are comfortable to freely express your medical complaints, problems, or any issues that you would like to discuss. Psychotherapy or behavioral therapy is probably the preferred approach in mild cases but in individuals with more profound symptoms, medications may be preferred in addition to psychotherapy. Finding a good therapist and setting up sessions at frequent intervals is important. In severe cases with suicidal ideations or attempts perhaps hospitalization may be required.
Multiple medications are commonly used for treating anxiety and depression. A PCP or psychiatrist may be able to find the right one for you, and please make sure you follow up with these providers since these medications may need to be monitored for their side effects and to adjust the dosage. Sometimes GI physicians may feel comfortable to prescribe these medications, but that may generally not be true for majority of gastroenterologists.”
NH: “As a GI, how do you try and facilitate positive relationships with your patients to help ensure they feel at ease with taking on their disease, managing it, overcoming flares/surgery, etc.?”
Dr. ZaZ: “My first step towards approaching IBD is to make sure that the symptoms that my patients are complaining of are truly from IBD and not from IBS or any other illness. Once IBD is diagnosed, I have a detailed visit with my patient with their new diagnosis. I usually encourage them to read up as much as they can and write down questions about their illness prior to this clinic visit. During the visit I start by giving a broad overview of what IBD is and the mechanism of disease process.I do this little exercise of talking about mechanisms by which IBD develops because I have noticed in my experience that several patients feel guilty about having their illness, and believe that in some way it was ‘their fault’ that they developed IBD. We then focus our attention on what are the available treatments why I think the recommended treatment would be a good fit, so the patients can make an informed decisions about their choice of therapy. I highlight the signs or symptoms they need to look out for that could suggest a complication or flare up of IBD. We provide them access to communicate with our clinic team if they have any questions; if they are concerned about a flare or if they suspect side effects from their therapy. Next, I answer questions they may have come up with during my discussion or from their personal research prior to the visit. Once the questions are answered I provide them with written material about their illness. I frequently encourage our patients to join patient support groups and direct them to online sources for information about IBD like the website for the Crohn’s and Colitis Foundation.”
NH: “Why is it so important to focus on whole person care–and recognize that IBD impacts more than the GI tract?”
Dr. ZaZ: “If we understand the mechanism by which IBD develops in the body, we can say that a dysfunctional immune system perhaps has the central role in the disease process. This immune system is connected to the entire body, it’s in our blood, guts, and other organs. Abnormal functioning of this immune system is likely to affect the entire body, although in IBD this abnormality primarily targets the bowels. But we frequently encounter what are called the “extra-intestinal manifestations of IBD”. These are referred to conditions that cause joint pains, skin rashes, eye redness, oral ulcers, liver disorders and other symptoms or signs that can be encountered in patients with IBD. Beyond these, patients with IBD are shown to be associated with higher incidence of mental disorders, pregnancy-related complications, chronic fatigue, and vitamin/mineral deficiencies. The effect on the bowels by this disease has a major impact on what one can eat, thereby limiting their nutritional intake. It is only fitting to treat these individuals as a whole, and not just their bowels. In terms of methods of treatment, apart from allopathic medical therapies, several other modalities of treatment are now being explored and accepted. Addressing diet and exercise is an important aspect to maintain healthy lifestyle in general, and especially so in patients with IBD. Running or other forms of cardio-based exercises have been shown to have a positive impact on the disease. Consuming healthy dietary supplements, like probiotics have been shown to be beneficial. Relaxation techniques and meditation also help keep oneself stress free, and perhaps prevent development of mental disorders as well.
One last thing we must also remember is that in today’s world social media can contribute to a lot of mental stress and anxiety, especially where disinformation campaigns can lead to confusion and poor choices in life. Hence it is important to have reliable resources to gain knowledge about IBD and its therapies. Sources like the Crohn’s and Colitis Foundation and its members like Natalie have been leading in educating several individuals through various platforms. In summary, eat healthy, exercise regularly, educate yourself about IBD, try to relieve stress and follow up with your doctor for medical care.”
I hope this article sparks a conversation and allows you to feel less alone in your mental health struggles. The findings show it’s anything but “just in your head.” Your feelings, fears, and struggles are valid. You are loved. You are not a burden. You are worth it. You matter. We need you here. Remember that.
If you’re thinking about suicide, are worried about a friend or loved one, or if you would like emotional support, call 988 any day of the week, any time. The 988 Suicide and Crisis Lifeline (formerly known as the National Suicide Prevention Lifeline) provides free and confidential emotional support to people in suicidal crisis or emotional distress 24 hours a day, 7 days a week, across the United States.
Reference Guide List
1: Coates, M. D., Mahoney, C. R., Linden, D. R., Sampson, J. E., Chen, J., Blaszyk, H., Crowell, M. D., Sharkey, K. A., Gershon, M. D., Mawe, G. M., & Moses, P. L. (2004). Molecular defects in mucosal serotonin content and decreased serotonin reuptake transporter in ulcerative colitis and irritable bowel syndrome. Gastroenterology, 126(7), 1657–1664. https://doi.org/10.1053/j.gastro.2004.03.013
2: Tarar, Z. I., Zafar, M. U., Farooq, U., Ghous, G., Aslam, A., Inayat, F., & Ghouri, Y. A. (2022). Burden of depression and anxiety among patients with inflammatory bowel disease: results of a nationwide analysis. International journal of colorectal disease, 37(2), 313–321. https://doi.org/10.1007/s00384-021-04056-9
3: Umar, N., King, D., Chandan, J. S., Bhala, N., Nirantharakumar, K., Adderley, N., Zemedikun, D. T., Harvey, P., & Trudgill, N. (2022). The association between inflammatory bowel disease and mental ill health: a retrospective cohort study using data from UK primary care. Alimentary pharmacology & therapeutics, 56(5), 814–822. https://doi.org/10.1111/apt.17110
4: Xiong, Q., Tang, F., Li, Y., Xie, F., Yuan, L., Yao, C., Wu, R., Wang, J., Wang, Q., & Feng, P. (2022). Association of inflammatory bowel disease with suicidal ideation, suicide attempts, and suicide: A systematic review and meta-analysis. Journal of psychosomatic research, 160, 110983. https://doi.org/10.1016/j.jpsychores.2022.110983
5: Fairbrass, K. M., Gracie, D. J., & Ford, A. C. (2022). Relative Contribution of Disease Activity and Psychological Health to Prognosis of Inflammatory Bowel Disease During 6.5 Years of Longitudinal Follow-Up. Gastroenterology, 163(1), 190–203.e5. https://doi.org/10.1053/j.gastro.2022.03.014
6: Stoleru, G., Leopold, A., Auerbach, A., Nehman, S., & Wong, U. (2022). Female gender, dissatisfaction with weight, and number of IBD related surgeries as independent risk factors for eating disorders among patients with inflammatory bowel diseases. BMC gastroenterology, 22(1), 438. https://doi.org/10.1186/s12876-022-02526-0