As temperatures rise, so can the challenges of living with Crohn’s disease and ulcerative colitis. For people with inflammatory bowel disease (IBD), summer heat (and heat in general) isn’t just uncomfortable, it can amplify symptoms, increase dehydration risk, worsen fatigue, and make everyday activities feel far more difficult.
And while everyone is told to “drink more water” during the summer, hydration with IBD is often much more complicated than that. Living in St. Louis, I’m no stranger to extreme heat and humidity!
Between diarrhea, ostomies, inflammation, medication side effects, and nutrient absorption issues, those of us with IBD are already operating at a hydration deficit before stepping outside into 90-degree-plus weather. This week on Lights, Camera, Crohn’s a look at what patients need to know about staying safe, hydrated, and feeling their best during the hottest months of the year.

Why People With IBD Are More Vulnerable to Dehydration
Dehydration happens when your body loses more fluids than it takes in. While that can happen to anyone in the heat, people with IBD face unique risks.
Some of the biggest contributors include:
- Frequent diarrhea
- Active inflammation
- Vomiting
- Excessive sweating
- Reduced appetite
- Short bowel syndrome
- Ileostomies or J-pouches
- Certain medications
- Avoiding fluids due to bathroom anxiety
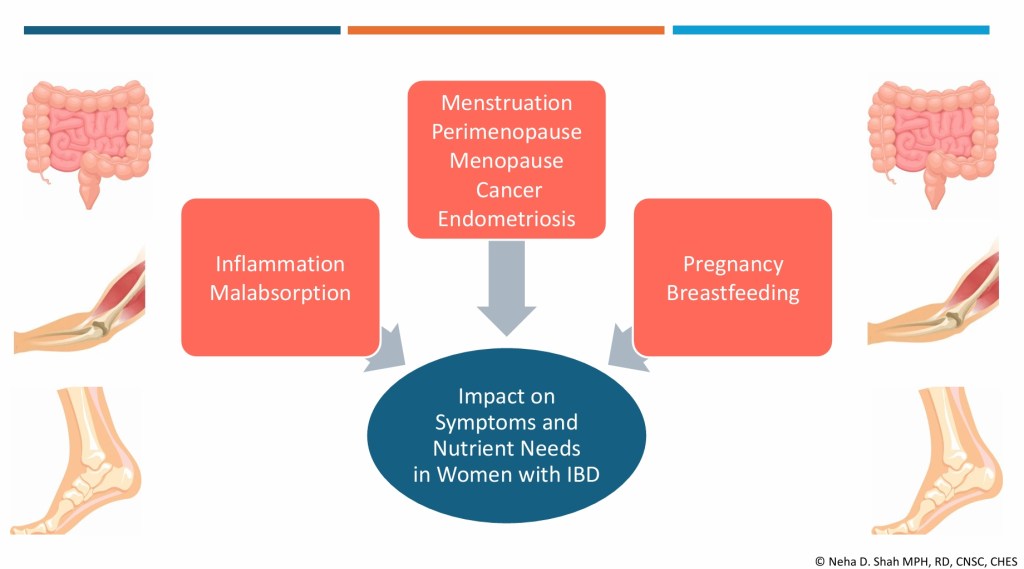
For patients with Crohn’s disease affecting the small intestine, the body may also struggle to absorb fluids and electrolytes efficiently. Meanwhile, people living with an ostomy can lose significant amounts of sodium and fluids throughout the day, especially in extreme heat. The result? We can become dehydrated faster than we realize.
Signs of Dehydration Can Look Different in IBD
Many symptoms of dehydration overlap with symptoms those with IBD already experience regularly, which can make it harder to recognize when something is wrong.
Common warning signs include:
- Dizziness or lightheadedness
- Fatigue or weakness
- Headaches
- Muscle cramps
- Dry mouth
- Rapid heartbeat
- Brain fog
- Dark urine
- Nausea
- Increased GI symptoms
For some, dehydration can trigger a vicious cycle: diarrhea leads to fluid loss, dehydration worsens fatigue and weakness, and patients feel too sick to adequately rehydrate.
Why Water Alone May Not Be Enough
One of the biggest misconceptions about hydration is that drinking plain water is always sufficient.
In reality, many IBD patients lose electrolytes (especially sodium and potassium) along with fluids. Drinking large amounts of water without replacing electrolytes can sometimes leave us feeling even worse.
Electrolytes help the body:
- regulate fluid balance
- support muscle function
- maintain blood pressure
- keep nerves functioning properly
That’s why your gastroenterologist may recommend oral rehydration solutions or electrolyte drinks during flares, illness, travel, heat exposure, or high-output ostomy periods.
Be mindful that some sports drinks contain large amounts of sugar or artificial sweeteners that can aggravate symptoms. I’ve personally had luck with DripDrop and Liquid IV.
Summer Activities Can Add Another Layer of Stress
Summer doesn’t just bring heat; it brings logistical anxiety. Long car rides and flights for fun travel. Outdoor festivals. Pool days. Sporting events. Theme parks. Beach vacations. Going to parks with the kids that don’t have bathrooms. The list goes on and on. I know I feel extremely anxious every time I get on my in-law’s boat and just pray, I don’t run into any bathroom issues!
We often become hyper-aware of where bathrooms are located, whether they’ll have access to safe foods, and how quickly heat exhaustion could escalate symptoms. And unlike others, people with chronic illness often can’t simply “push through” dehydration or fatigue.

Medications Can Complicate Heat Tolerance
Certain medications commonly used in IBD management may affect how patients tolerate heat. Steroids can increase sweating and cause fluid shifts within your body, some medications can cause nausea (Zofran to the rescue!), and fatigue from chronic inflammation can worsen when temperatures rise (especially if you’re anemic)!
Tips for Staying Hydrated With IBD This Summer
While every patient is different, experts often recommend:
Hydrating Before You Feel Thirsty. Thirst can be a late sign of dehydration. Consistent hydration throughout the day is key. I make a point of making a water bottle for myself before I even have breakfast or my coffee each morning. As an IBD mom, we can get so busy taking care of everyone else that we can put eating and drinking on the backburner for ourselves.
Focus on Electrolytes During High-Risk Situations
Especially:
- outdoor events
- travel days
- exercise
- active flares
- ostomy output increases
- stomach illnesses
Carry “Safe” Hydration Options: Many people find certain drinks are easier to tolerate than others. Trial and error matters. What may help someone else, may not sit well with you.
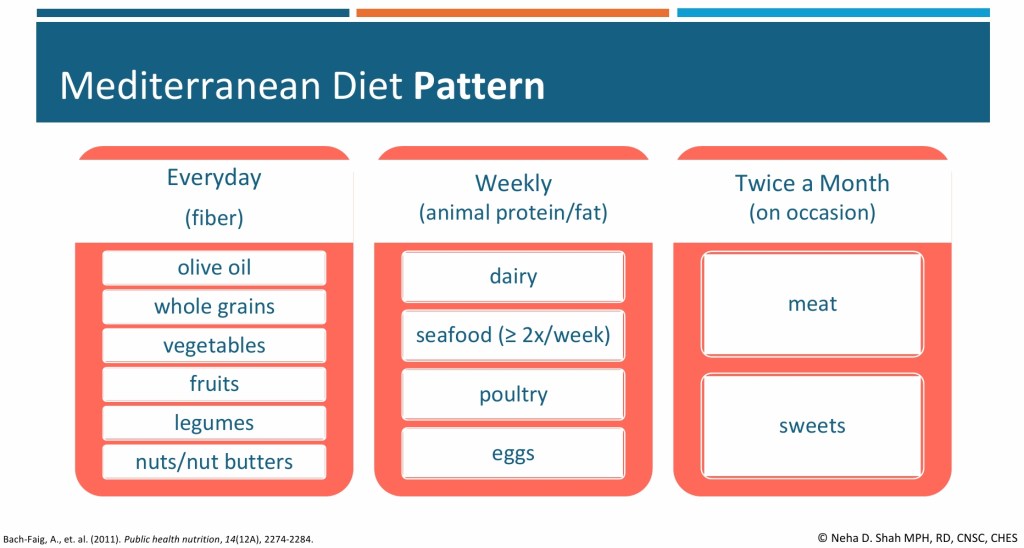
Eat Hydrating Foods: Foods like watermelon, lettuce, celery, zucchini, bell peppers, cucumbers, broth-based soups, smoothies, and fruits can contribute to fluid intake. If you’re currently flaring or have active stricturing disease, talk with a registered dietitian about how to navigate this (ex. Cooking the veggies so they’re tender or chewing to applesauce consistency).
Be Careful with Alcohol and Excess Caffeine: Both can worsen dehydration for some people.
Watch for Heat Exhaustion: If symptoms escalate to severe dizziness, fainting, confusion, rapid heartbeat, or inability to keep fluids down, medical attention may be necessary. Be vigilant and proactive as best you can.
The Emotional Side of Summer With Chronic Illness
There’s also a mental load that comes with navigating summer while living with IBD.
Many of us want to participate fully in vacations, outings, and family activities, but may quietly spend the entire day navigating bathroom access, our energy levels, finding safe foods, and staying on medication schedules. That invisible planning can be exhausting.
And for parents with IBD, summer can feel even more physically demanding. I’m gearing up for that with my three kids! The combination of heat, disrupted routines, increased outdoor activities, and caring for children often leaves little room for rest and recovery. Now that my kids are 9, 7, and almost 5, I know that everyday doesn’t need to be an adventure and that low-key days at home can be just as fun for everyone, too. There’s all this hype about bringing back the 90’s summer. Listen to your body and if it means staying home and having the kids ride their bikes, run through the sprinkler, and have popsicles versus going to parks, pools, and amusement parks—that’s ok. Give yourself grace, your body will thank you!

The Bottom Line
Hydration isn’t just a wellness trend for people with IBD, it’s a critical part of symptom management and overall health and something to discuss with your care team.
As summer temperatures climb, patients may need to be more proactive about fluids, electrolytes, rest, and recognizing the early signs of dehydration. As always, listen to how your body speaks to you through symptoms and do your best to address those needs before they become an acute issue.
Because while summer is often portrayed as carefree, many people living with Crohn’s disease and ulcerative colitis are dealing with an entirely different reality behind the scenes: one that requires constant awareness, preparation, and self-advocacy just to feel well enough to participate.
News You Can Use
Electrolytes and Hydration for IBD: What You Need to Know — Stacey Collins Nutrition
The Connection Between Ulcerative Colitis and Dehydration
Inflammatory bowel disease (IBD): Staying hydrated – AGA GI Patient Center