**This article has also been published on Tina’s blog: Own Your Crohn’s**
As two bloggers and patient thought leaders in the IBD community, we were thrilled and honored to attend and speak at the Advances in IBD conference in December 2024 in Orlando, Florida. In the article below, we come together to summarize key learnings for our IBD patient and caregiver community.
Management of Crohn’s Disease
Crohn’s can be a very progressive disease, meaning it can worsen over time and cause complications, often leading to fistulae, strictures, and therefore surgery and bowel loss. In a debate between two of the co-chairs, Dr. Miguel Regueiro and Dr. Corey Siegel, as well as throughout AIBD, a key theme was to understand if all Crohn’s patients need advanced therapies (biologics or small molecules) to prevent complications. A good suggestion was to identify those few patients who could be closely monitored but not necessarily put on an advanced therapy. The doctors agreed that almost all patients do need an advanced therapy to prevent progression of the disease. Dr. Siegel brought up an interesting point about risk-stratifying patients via a new blood test called CD-PATH, which allows physicians to better understand if a patient might be low-, medium-, or high-risk for progression of Crohn’s disease.
The conclusion at the conference was that early intervention has made a big difference in terms of improving long-term outcomes for patients. It was shown that there is an optimal time for treatment and missing that window can lead to progression of disease and potentially complications.
From stem cells for perianal Crohn’s to more options for fibrostenotic Crohn’s, many patients are waiting for more therapeutics to gain better quality of life. Patients, however, are also clamoring for more therapies for mild Crohn’s disease. There is a real void in treatment options for mild Crohn’s outside of dietary therapies and occasional use of steroids (< 1-2x a year). As patients ourselves, we advocate for more options whether that’s looking at S1Ps or new therapeutics that can help patients feel safe & comfortable that their disease is being treated.
Management of Ulcerative Colitis
In Dr. Millie Long’s talk on Defining Disease Severity in UC, she shared many pearls. Primary indicators of severity include appearance severity of disease on endoscopy and frequency of use of steroids (more often means another long-term therapy may be needed to quell inflammation). She said to also consider biomarkers (fecal calprotectin, C-reactive protein, etc.) and to keep in mind what prior therapies have been used. Dr. Long emphasized that UC can also progress like Crohn’s, and it is important to use treat to target strategies, including initiating therapy early, monitoring for disease activity using biomarkers and intestinal ultrasound, and aim for mucosal healing.
In Dr. Maia Kayal’s talk on what meds to consider if Mesalamine doesn’t cut it in UC, her key take-home message was, “Your first shot is your best shot.” She said it was important to plan wisely if you have mild to moderate UC and work carefully with your gastroenterologist to identify medication options. Dr. Kayal emphasized that certain biologics may be more effective as a first-line therapy rather than being used after one or two biologics haven’t worked, so to choose carefully. Even if mesalamine doesn’t work, there are multiple biologic options from anti-TNF agents to anti-IL-23 medications, and S1P receptors.
CurQD & IBD
Throughout the conference, CurQD received many notable mentions, which in randomized clinical trials showed efficacy in mild to moderate UC when mesalamine hasn’t cut it. CurQD is a naturally sourced formula. Cura is gut-directed form of curcumin that has been found to reduce inflammatory cytokines, restore barrier function, and positively alter the composition of the gut microbiome. QD (Qing Dai) is an extract of Indigo plants found in clinical trials to relieve bleeding, inhibit inflammation, and promote mucosal regeneration (Naganuma et al, Gastroenterology 2018, Ben-Horin et al, CCFA 2023). Dr. Kayal shared this placebo-controlled trial, that found CurQD was effective for inducing response and remission in active UC patients and has the ability to significantly decrease urgency.
Dr. David Rubin also touted CurQD as an adjunctive IBD therapy option, rather than a singular therapy, much like diet. He said while it may be beneficial, patients need to be cautious about sudden pain or obstructive-like symptoms and communicate how they’re feeling with their doctor.
Insurance barriers
Patients and providers have an uphill climb when dealing with insurance barriers, which makes managing IBD exceptionally challenging and at times frustrating for everyone involved. These proverbial hula hoops we’re all constantly forced to jump through often lead to delays in treatment and unnecessary stress. One key challenge discussed during this session was how to deal with insurance companies denying patients who have not tried 5-ASAs or steroids. Solutions shared included the GI office providing detailed documentation on the following:
listing previously tried and failed medications including steroids,
recent objective findings on endoscopy, imaging, blood tests,
sharing symptoms experienced by the patient,
referencing guideline recommendations, and
outlining the risks to the patient and the costs to the insurance company if treatment is not initiated soon.
Patients can also proactively reach out to their insurance company to determine their preferred advanced therapies and pass that intel along to their IBD team.
Another common roadblock discussed was finding out a medication is not covered or no longer covered by insurance—whether it be biologic vs. biosimilar of off-label dosing.
Patients can discuss appealing the decision with their IBD team during clinic appointments, over the Patient Portal, or over the phone. If your first appeal is denied, keep close tabs on your quality of life moving forward. If you are forced to switch, keep a detailed journal of all your symptoms to paint a clear picture of your reality.
Ask about having your GI submit a letter written by you about your patient experience, along with theirs, and make sure a doctor with knowledge of immune-mediated conditions is reviewing the appeal at the insurance company.
Providers can be supportive by showing empathy, following the latest research and including studies within insurance appeal letters. If a person is symptomatic, it would be important to rule out whether it’s active disease or an adverse reaction to medication.
Biosimilars now and in the future
The landscape for IBD therapies has changed immensely in recent years and will continue to do so in the years ahead. Stelara will join Remicade and Humira in 2025 with six biosimilar options for patients (and insurance companies). One of the main areas of improvement lies in patient education. Oftentimes we hear about the switch through a letter from our insurance company or we’re blindsided at an infusion appointment and told by our nurse that we’ll be receiving the biosimilar moving forward. As should be expected, this results in a great deal of uncertainty, skepticism, and pushback from the patient and caregiver population.
Biosimilars are biologic medical products that are highly similar to an already approved reference biologic, with no clinically meaningful differences in terms of safety, potency, or efficacy. Unlike generic drugs, which are chemically synthesized and identical to their branded counterparts, biosimilars are produced using living organisms and exhibit minor natural variability.
Dr. David Choi presented about how important proactive discussions with the patient community area to instill confidence and help educate about how safety and effective biosimilars are. Currently, four adalimumab and two Ustekinumab drugs have interchangeability, which is a designation from the FDA that allows for patients to be automatically switched (originator drug substituted) at the pharmacy level. Dr. Choi shared that providers can avoid this automatic substitution by selecting “dispense as written” on the original prescription. He went on to share that while improving access, there is also a major cost savings. Biosimilars across all disease spaces are expected to save $38-$124 billion from 2021 to 2025. The future of biosimilars is happening right now with exclusivity for golimumab and certolizumab over in 2024 and with more biosimilars in development.
Final thoughts from AIBD 2024
Overall, the main theme throughout all the educational sessions was that IBD needs to be more than just managed, it needs to be overcome with shared patient decision making. More work needs to be done to determine which patient is right for which therapy. There tends to be too much focus on the risk of therapies, rather than the risk of uncontrolled disease. The overarching goal is for providers to identify high-risk patients before we have severe disease and not be hesitant to use surgery as a treatment option when necessary. Emphasis on the importance of re-thinking the role of diet and nutrition and mental health care in conjunction with advanced therapy, looking at biomarkers 10+ years before diagnosis to see if we can prevent or diminish disease severity, utilizing intestinal ultrasound to measure drug response and disease activity in a non-invasive way, and continuing biologics in pregnancy (Healthy mom= healthy baby) were common themes throughout this fantastic conference.
As patients, we remain hopeful for the future of IBD and committed to improving patient outcomes. Lots of work still to be done, but it is impressive to see how far the science has come in the last 19-20 years since our diagnoses!
Getting a colonoscopy when you have Inflammatory Bowel Disease (IBD) carries a distinct set of challenges and trauma compared to the average person receiving a colon cancer screening scope. I underwent my 10th colonoscopy this past week as part of my Crohn’s disease surveillance and heard the word “trauma” on multiple occasions.
I received the following public comment on an Instagram post following my colonoscopy, “You seem to have trauma around colonoscopy prep. I get it, but I don’t. Childbirth is traumatic but colonoscopy prep is not. It sucks, but really not traumatic. The flu sucks, strep throat sucks, why is this so hard for people?”
…to which I responded, “Do you have IBD?”…radio silence.
*Side note—none of my 3 child births were even close to traumatic, they were all joyous, uneventful, and happy occasions. But I digress.*
I had a wonderful nurse get me ready for my scope and give my IV, I let her know I have terrible veins and that I’m a tough stick. Once the IV was started she said that it appeared I have trauma around IVs…which I said was correct. While I appreciated her recognizing this it also felt a little bit judgy. During a prior hospitalization it took EIGHT tries to get an IV started. These difficult medical experiences cause trauma. It should not come as a surprise to anyone dealing with an IBD patient that what may seem run of the mill to an average person is not the same for us. I have to tell myself not to roll my eyes when a 70-year-old tells me how “easy” and uncomplicated their colonoscopy was. Happy for them…but their experience is much different than mine.
My most recent colonoscopy experience inspired me to dig a bit deeper and help to articulate why it’s hurtful and not helpful when you try and compare a “healthy” person’s experience getting a scope compared to someone diagnosed with IBD.
Oftentimes we receive confirmation of our IBD diagnosis after a colonoscopy. The results of a colonoscopy can significantly impact treatment plans, which may heighten stress. The fear of bad news—such as disease progression or the discovery of dysplasia—can weigh heavily. We not only have to rule out colon cancer (due to our elevated risk), we also have the weighted worry about hearing we could have active disease and inflammation going on. If that’s the case we may need to stop our current treatment, start a new treatment, need surgery, etc.
Unlike the average person who may not need a scope until age 45 and then not for another 7-10 years after, we know we may need to go through the ordeal multiple times a year, annually, or every other year starting whenever we’re diagnosed (as a child/in our 20s). The frequency of needing to go through prep and the procedure is astronomical compared to the typical person and when you’re way younger than 45 and have to go through a scope it builds resentment against your body, something our healthy peers and caregivers can’t truly grasp unless they’ve lived it. The cumulative stress of repeated procedures can lead to heightened anxiety and emotional exhaustion.
Our digestion is different from yours. Prep can induce abdominal pain, nausea, vomiting, and bloating that mirrors flare symptoms to us and this in and of itself can feel traumatic. People with IBD frequently experience inflamed, ulcerated, or narrowed sections of the gastrointestinal tract. During a colonoscopy, these areas may be more sensitive, leading to increased pain and discomfort compared to individuals without the condition. The bowel preparation process—which involves consuming large amounts of laxatives to clear the colon—can be especially grueling for those with IBD. It may exacerbate symptoms like diarrhea, cramping, and dehydration, making the days leading up to the procedure particularly difficult.
Many of us take the prep a step further and start a liquid diet days before the actual prep to try and “ease” the process. I personally put myself on a full liquid diet 4-5 days prior to my scopes and then a clear liquid the day before. This takes a great deal of willpower, especially as an IBD mom making school lunches and meals for my kids, while not being able to eat any of it. Caring for a family while running on fumes is not for the faint of heart. It’s a challenge to have the energy to function while feeling hangry. Understand that we might feel irritable, fatigued, or anxious during the preparation and recovery process. Provide a judgment-free space for us to express our feelings. I’m not one of those people who feels comfortable eating a light breakfast the day before a scope, because I fear not being cleaned out enough and having to go through the experience again sooner than I need or want to.
How to Be Supportive
Acknowledge Their Experience: Validate their feelings and recognize that colonoscopies are more than a simple procedure for someone with IBD. Avoid dismissive comments like “It’s just routine.”
Offer Practical Help:
Assist with transportation to and from the procedure. Offer to babysit if the person has kids or needs help at home with childcare.
Help prepare supplies for the bowel prep process, such as clear liquids, electrolyte solutions, and soft toilet paper.
Offer to stay with them during recovery if needed.
My husband always makes a point to take our kids out to dinner or try and not eat in front of me while I’m prepping, this makes a world of difference. We also always go out for a big breakfast or lunch date immediately following the procedure.
Provide Distractions. During the prep period, suggest activities to keep their mind off the discomfort, such as watching movies, playing games, or listening to calming music.
Encourage Communication with Healthcare Providers. If they’re particularly anxious or in pain, encourage them to discuss these concerns with their doctor. Sedation options or anti-anxiety medications might help make the procedure more tolerable. I always make sure I have Zofran on hand to take prior to my prep to help with nausea. I still always vomit at least once, but it does help.
Respect Their Privacy: Everyone copes differently. Some people may want to talk about their experience and post about it on social media, while others may prefer to keep it private. Follow their lead and respect their boundaries.
Final thoughts
Colonoscopies are a critical tool in managing IBD and being proactive about colon cancer screening, but they can be uniquely challenging for those living with Crohn’s or ulcerative colitis. By understanding the physical and emotional toll of these procedures, friends and family can provide better support and help ease the burden.
My ask for friends, family members, and medical professionals with patients or loved ones who have IBD and are undergoing or gone through a colonoscopy is to refrain from comparing your own experience with us. Show compassion. Be kind. Remember that colonoscopies carry a sense of trauma for many of us, and for good reason. We are not weak. We are not complainers. If you lived our reality and been through what we have, I guarantee it wouldn’t feel like a walk in the park. Not many 41-year-olds I know have had 10 colonoscopies. With patience, empathy, and practical assistance, you can make a difficult experience a little more manageable for someone with IBD.
Inflammatory bowel disease is increasingly recognized as a condition associated with systemic complications beyond the gastrointestinal tract. Among these, cardiovascular (CV) complications stand out due to their potential impact on morbidity and mortality. One of the presentations I attended at the Advances in IBD conference that took place in Orlando this month explored the relationship between IBD and cardiovascular disease, focusing on the effects of disease activity and commonly used therapies. This week on Lights, Camera, Crohn’s a look at what we need to watch out for as a patient community and how we can be proactive with our providers.
Cardiovascular Risks in IBD
Meta-analyses indicate that IBD is associated with a 24% increased risk of ischemic heart disease. Moreover, there are higher rates of premature (under age 55) and extremely premature (under age 40) atherosclerotic cardiovascular diseases in our population. The underlying mechanisms are multifactorial, but persistent inflammation and disease activity are key drivers of arterial events.
Heart failure (HF) risk is also elevated among individuals with IBD. Notably:
The risk appears greater in patients with ulcerative colitis compared to Crohn’s disease.
Female patients with IBD demonstrate a higher predisposition to HF than their male counterparts.
Corticosteroid use further exacerbates the risk of HF in this population.
Cardiovascular Considerations for IBD Therapies
Anti-TNF Therapy
Anti-TNF agents (infliximab, adalimumab, certolizumab pegol, and golimumab) have been linked to worsening congestive heart failure (CHF). In patients with pre-existing heart conditions or known cardiomyopathy, baseline cardiac assessment is critical. Recommendations include performing a transthoracic echocardiogram (TTE) before initiating anti-TNF therapy and monitoring for new or worsening cardiac symptoms during treatment.
JAK Inhibitors
The use of Janus kinase (JAK) inhibitors ( Tofacitinib, filgotinib and Upadacitinib) raises concerns regarding cardiovascular risks, including:
Increases in low-density lipoprotein (LDL) and triglycerides.
Development or exacerbation of hypertension.
Major adverse cardiovascular events (MACE).
For patients starting on JAK inhibitors, clinicians should:
Discuss the patient’s cardiovascular history and risk factors.
Perform a baseline lipid profile, with a repeat evaluation at 8-12 weeks after initiating therapy.
S1P Receptor Modulators
Sphingosine-1-phosphate (S1P) receptor modulators, a newer class of therapies for IBD (ozanimod, etrasimod, fingolimod and laquinimod), can impact cardiac conduction. To mitigate risks:
Screen for symptoms suggestive of conduction abnormalities.
Review the patient’s drug history for concurrent use of anti-arrhythmic agents or drugs that prolong the QT interval.
Perform an electrocardiogram (ECG) prior to initiating therapy.
Clinical Implications
Cardiovascular complications are common in patients with IBD, often presenting at a younger age than in the general population. The association between active disease and increased CV risk highlights the importance of maintaining disease control. Non-steroidal options for long-term management should be prioritized, as corticosteroids exacerbate both IBD and CV risks.
Therapeutic decisions should also account for the cardiovascular safety profile of IBD medications. High clinical suspicion and proactive monitoring are essential for detecting underlying or developing cardiovascular disease in IBD patients. Understanding the risks associated with specific therapies, such as anti-TNF agents, JAK inhibitors, and S1P receptor modulators, can guide personalized treatment plans and improve long-term outcomes. When meeting with your gastroenterologist communicate any concerns you may have about chest pain or your blood pressure.
Closing Summary
Cardiovascular complications in IBD patients necessitate a high level of vigilance from healthcare providers. Early detection and management of cardiovascular risks are paramount, particularly in young IBD patients who may already be vulnerable to inflammation-driven atherosclerotic changes. A tailored approach—balancing effective disease control with an awareness of therapy-specific cardiovascular risks—is critical to optimizing care in this complex patient population.
Nothing prepares you to hear that your child has Inflammatory Bowel Disease. For many, it’s the first time ever learning about what the weight of those words even means. Not only is a chronic illness at a young age an incredibly heavy burden to bear, it can feel isolating to not only the patient but the caregiver. This inspired The University of Chicago to launch the IBD Kids Club in February 2024. This week on Lights, Camera, Crohn’s learn more about how you can connect with others living your reality and find community, regardless of where you live.
Recognizing the need
Dr. Amelia Kellar, MD, MSc, FRCPC, Assistant Professor of Pediatrics, Director, Pediatric Intestinal Ultrasound University of Chicago Medicine/Comer Children’s Hospital says one of the most common concerns she hears from patients and their families is that they don’t know anyone else with IBD or where to go for support.
“I always refer my patients to Crohn’s and Colitis Foundation, but this also inspired me to create a community for these kiddos more locally…a place where they could authentically meet one another both virtually and in person, and know they are not alone.”
Dr. Kellar wants her patients to see kids who are older than them doing all the things they aspire to do and have examples of adults who are living and thriving with IBD. So far, the feedback has been extremely positive—families are grateful to meet one another where there’s no need to explain and there’s comfort in shared experiences.
Get connected to the IBD Kids Club
The group meets virtually every 2nd Tuesday of the month on Zoom at 6 pm CT. Dr. Kellar says it is tough to find a time that works for everyone, but she’s found the dinner hour allows for kids and parents to join together and chat. The next meeting is Tuesday, December 10th.
“I feel very fortunate as I have a great team of GI docs, nurses, dieticians and psychologists that join for different sessions and I co-lead with one of our adult IBD nurses who is also a counselor at Camp Oasis and openly talks to the group about her diagnosis of UC and journey through J-pouch surgery,” says Dr. Kellar.
When she started the group, Dr. Kellar polled participants for what they would like the group to be, whether they wanted to simply chat with one another and offer support, whether they wanted some guest speakers on topics or in person events… and they indicated they wanted a mix, so they have had some support/chat sessions, some guest speakers, and a live cooking class with their IBD dietician. There has not been an in-person event yet. I let Dr. Kellar know in the months ahead I would love to join one of the calls, meet the families, and share experiences.
Everyone is welcome
Dr. Kellar is looking to get the word out—and wants all pediatric IBD warriors and their caregivers to know they are welcome to join.
“I want this group to be open to everyone—regardless of where you live or where you receive care. I want the IBD community to know they are not alone. We talk a lot about how every single person in the world has something that is challenging and that they may or may not choose to share with others and you would never know when you see someone at school, work, on the street, what challenges they might be facing. At the same time, finding people who have faced or are facing similar challenges can offer a unique support system. Our hope is that this group unites children and families with IBD and fosters connections, friendships, and support so no one ever feels alone with their challenges,” says Dr. Kellar.
If it’s happened to you, you know the feeling all too well. When I received a letter in the mail informing me that the biologic injection, I had been on for 16 years was no longer going to be covered, my stomach flipped, and my heart sank. When you live with a complicated disease like Crohn’s or ulcerative colitis and find a therapy that keeps your health in check and your IBD well-controlled, it’s extremely stressful and daunting to face the worry of being forced to switch your medication to a biosimilar or a different biologic all together.
Like many patients, I asked my gastroenterologist to appeal the forced medication switch. Even though I was almost positive we would be denied, I did not want to go down without a fight. As expected, within days of my GI’s appeal, we were told by insurance that Humira would no longer be covered and that I would need to choose a biosimilar or a different drug class all together moving forward.
I chose to go on the biosimilar Hyrimoz for many reasons—the first being that anti-TNF drugs have worked well for me for YEARS, by choosing to go off it and switch to a different drug class, I ran the risk of building up antibodies and possibly not responding as well to treatment. I also have a comfort level with self-injections and know how I have typically responded to anti-TNF medication in the past.
The emotions and heartache of having to say goodbye to a medication that carried me through for 16 years, allowed me to bring three healthy babies into this world, and stay out of the emergency room and hospital since becoming a mom 7.5 years ago tore me apart. I sobbed. I stressed. I was anxious.
Switching to a biosimilar—the emotional and physical toll
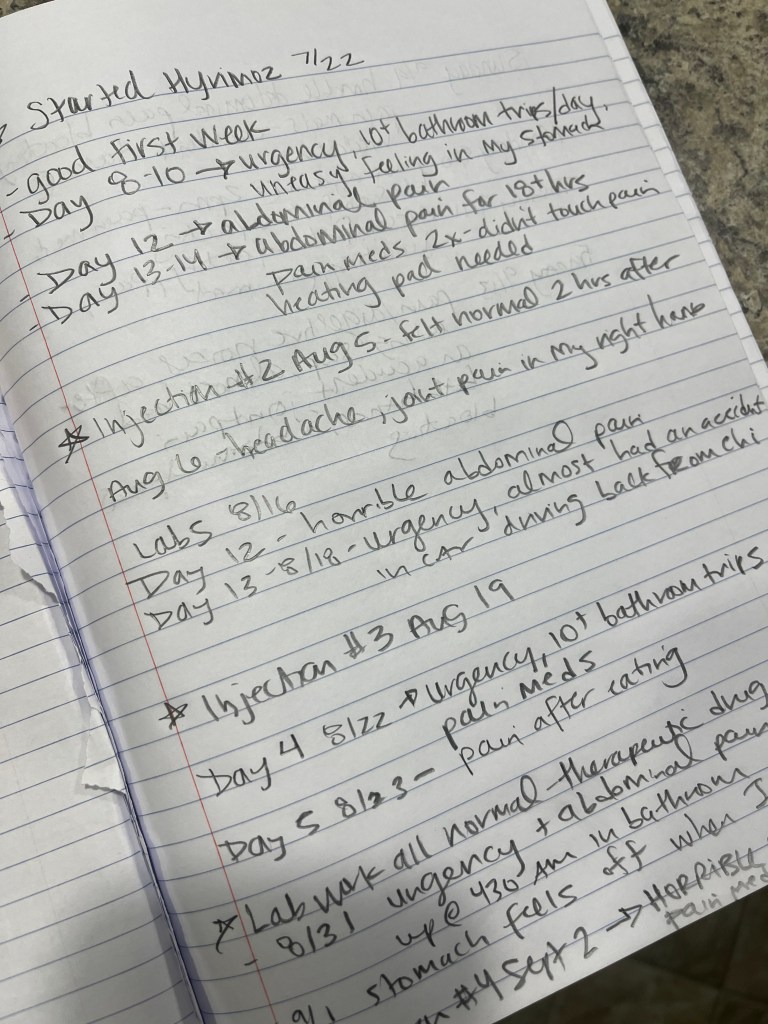
Much to my dismay, I started Hyrimoz in July 2024. The first eight days I felt the same and then my health began to crumble. I lasted four injections—and during that time I went from being in deep remission for years to needing pain medication to make it through elementary school PTO meetings and while coaching my kindergarten soccer team. I went from feeling well most of the time to running to the bathroom 15+ times a day and almost having accidents in public. I went from being able to eat whatever I wanted to worrying about how consuming anything was going to make me feel. I spent nights curled up in pain and days feeling bloated and on edge about whether every decision I made was going to make me unwell.
I knew something had to change. I refused to have my quality of life ripped from me without speaking up. I kept a detailed journal every single day since I started the biosimilar. I articulated my concerns to my care team repeatedly over the Patient Portal. We ran extra labs, I did a telehealth appointment, I spoke with GIs around the United States I have come to know and trust through my patient advocacy work. My care team told me that meeting in person for a clinic appointment or over telehealth would help build our case, as that carries more weight than just communicating over the Portal. Keep that in mind.
This week on Lights, Camera, Crohn’s I offer tips for building your case, writing your appeal letter, and making sure your voice is heard. Patients are constantly made to feel less than. It’s all about the profits and not about the patients. This needs to stop. Insurance companies and specialty pharmacies need to stop making our lives so damn difficult and start to recognize the havoc they cause by delaying treatment, blocking treatment options, and forcing us to change a medication that finally controls our disease. Living and managing chronic illness is a full-time job in this country. The hours and days wasted and spent on the phone dealing with all the red tape is an absolute nightmare, and unless you’ve experienced it, you have no clue the headaches it causes, the time suck it is, and how it puts the quality of our lives in jeopardy.
Keeping track of it all
When living with IBD, the bad days come and go and oftentimes we forget just how often or how horribly we feel because our “normal” is not normal. By journaling or writing in the Notes app on your phone anytime anything with your health is awry, this helps paint a clear picture for not only you, but your providers. If you can say, “On Tuesday, September 24th I went to the bathroom 10 times, I couldn’t eat, I had joint pain in my hands, and abdominal pain that required a heating pad”—this illustrates the complexity of your symptoms. Imagine having that type of intel for two months. These details help your appeal in a big way. My IBD Nurse told me that she believes my typed-out symptom journal made all the difference in winning our second appeal.
So, take notes and be as descriptive as possible. If you have a random headache and you’re not sure why, write it down. If you get new pain, you haven’t experienced before keep track of it. If you eat and must run right to the bathroom or start feeling pain jot it down.
Many of my symptoms I’ve dealt with since switching to the biosimilar feel exactly like a Crohn’s flare. After weeks of this, I started to freak out that I was losing my remission all because of a forced medication switch. A world-renowned GI took the time to call me as I was making dinner for my family one night to hear more about my situation. He did this out of the goodness of his heart to provide additional guidance and support. After hearing more about my situation, he believed it was my body having adverse side effects to the biosimilar rather than a Crohn’s flare, since my labs were checking out fine. Everything started to make sense. While he wasn’t sure our appeal would be granted, he listened and empathized with what I was going through.
Writing your own appeal letter
My IBD team recommended I also write a patient letter that they would include with their second appeal. I was happy to take the time to offer my voice and share what the experience of being on a biosimilar was like for me. At the same time, I had never written an appeal letter. Before I started I did my research on how to approach and craft the wording.
I made sure not to come off angry or accusatory. I kept the letter as professional as possible, while also explaining very clearly how horribly I was responding to the medication. I backed up my letter with science and attributed research that’s been done regarding biosimilars. I learned from research published in the Journal of Crohn’s and Colitis (2020) that while around 80% of patients have a seamless transition, 10-20% have a negative response. It’s important to note that just because you are switched to a biosimilar, does not mean your health will deteriorate. Many people thrive and don’t notice a difference, but the issue is—you don’t know how you are going to respond. I went into the transition with an open mind and as positive as possible, but the unknown looms over and it’s emotionally draining to constantly wonder if you are going to feel unwell because of the forced switch.
Tips for expressing yourself in the appeal letter
I will use Humira as an example since that was my experience, but this goes for any biologic/medication.
Start with basic information—your name, date of birth, insurance ID number, and the policy number.
Provide the name of the medication you’ve been switched from (in my case Humira) and the one you’ve been switched to (Hyrimoz).
Mention the date when the change was made.
Clearly state the purpose of the letter. For example, “”I am writing to formally appeal the decision to switch my Crohn’s treatment from Humira to Hyrimoz.”
Briefly provide an overview of your health history with IBD, diagnosis date, and the treatments you’ve tried, hospitalizations/surgeries. If you’ve been on the same treatment for years and it’s helped you, highlight how effective the therapy has been. Mention the stability you’ve achieved with Humira—humanize your story. For instance, “While on Humira I was able to work full-time, have three healthy pregnancies and babies, and be a mom without my health holding me back.”
Reference any previous experiences with other medications that may have failed you or caused side effects.
Emphasize the risk of switching medications after long-term success. For IBD patients, changing medications can result in loss of response, worsening of symptoms or disease progression, potential adverse reactions.
Have your gastroenterologist provide their own letter that emphasizes the risks of switching, the stability you’ve achieved, and their professional recommendation. They will reference any studies that are available and be able to provide medical records showing your history on the medication.
If applicable, reference and cite insurance company policies that include provisions for medical necessity, or any pre-authorization that was previously approved.
Emphasize the impact on your health and finances and highlight the potential cost to both your health and your insurance provider if switching leads to disease flare ups, complications, hospitalizations, or the need for additional screenings, scopes, or treatments.
Close with a strong, respectful request. End the letter with a clear statement, such as:
“For the reasons stated above, I respectfully request that you reconsider your decision and allow me to remain on Humira as prescribed by my doctor.”
I signed my letter:
My family deserves more and so do I.
Sincerely,
Natalie Hayden
Ironically, when I wrote my appeal letter I was dealing with horrible abdominal pain, lying in bed with a heating pad.
Finding out we won the appeal
Once my appeal letter and journal of symptoms were finalized, I sent them to my GI and IBD nurse over the Patient Portal. I was on pins and needles wondering what was going to come next. I sent over the materials on a Friday morning and the following Monday, I received word from my nurse over the Portal that the insurance denied the 2nd appeal because back in June when my GI submitted the first appeal, he deemed it “urgent”—in doing so, the insurance company considers those appeals “2nd level appeals”—if those are denied, they consider the case closed. Imagine that— “closing a case” before a patient has even started a different medication. Makes sense…right?! Can’t make this stuff up. When I heard this, I felt incredibly defeated.
My care team was unaware of that and asked for a clinician to review our materials—the insurance company agreed and said there would be a decision in 72 hours. That same night, while I was making dinner for my family, I received an email from CVS Specialty pharmacy saying my prior authorization for Humira had been approved. I couldn’t believe my eyes. I’ll never forget how it felt to see those words and read that email.
My kids all smiled and laughed and danced with me, no idea what was really going on. But the celebratory moment was so incredibly jubilant they were smiling ear to ear. These last two months they’ve witnessed me unwell way too many times. It’s a side of my Crohn’s I’m not sure they even knew existed prior to now.
This past Friday night the same abdominal pain I’ve been dealing with began as the kids got off the bus. I had to take a pain pill before an advocacy call that was ironically about How to Deal with Insurance—for an upcoming panel discussion at a medical conference I’m speaking at in December. After my call and rushing through a makeshift meal, I took all three of my kids to my son’s soccer practice and told my friends on the sidelines how sick I felt. I came home and had to take another pain pill, had difficulty with the bedtime routine, and laid on the couch with a heating pad. But it helped to know these shitty days will hopefully be ending.
Looking to the future
This blog article is coming out the same day as I go back on Humira after winning my insurance appeal. While it’s a big win for me, it’s a small win for our community because at the end of the day an incomprehensible number of people are forced off their medications or denied off-label dosing, all so insurance companies see a better bottom line. As patients we can’t stand for this. Medical providers should and need to have the FINAL say in what medications their patients are on and they should always be willing to go to bat for their patients and appeal even if they “know they’ll get denied.” I hear all too often from fellow patients that their GI won’t even appeal in the first place and does not empathize with the fear of being forced on a biosimilar.
For those providers, I ask…can you guarantee, 100%, no doubts whatsoever that your patient will thrive and do just as well on a biosimilar as they did their originator biologic? Does the benefit really outweigh the risk? Should IBD patients who already live with an unpredictable and complicated chronic illness have to endure the stress, medical trauma, and anxiety that result from forced medication switches or denials related to off-label dosing?
As patients, caregivers, and medical providers we are a team. We know what’s right. Doctors and nurses should not have to waste so much energy on fighting for off-label dosing, necessary treatments, and keeping their patients on medications that are working. A HUGE thank you to all the providers and nurses who go above and beyond and out of their way to fight for us and do everything in their power to make sure we receive the medical treatments we need to keep our IBD in check. Your efforts, whether successful or not, are not going unnoticed.
At the end of the day, the big argument is all about “accessibility” and “cost savings” in the United States, but are patients really reaping this benefit here? I paid at most 0-$5 for Humira injections, I paid $0 for Hyrimoz. Do you know how I paid? I paid with living more than two months with health issues that would bring the average person to their knees. I went from being in deep remission to re-living the trauma of how unpredictable life with IBD can be. I paid by being on a biosimilar for 71 days and spending more than half of them with debilitating pain and symptoms.
Big pharma can step up to the plate and lower their absurd pricing on biologics (originator drugs) so that biosimilars are of no monetary benefit to pharmacy benefit managers. Let’s make it an equal playing field and see what happens. Would Big Pharma rather lose all their patients because their biologic is being removed from the insurance formulary or keep patients, lower their costs of the drugs, and keep insurance companies from choosing biosimilars because it saves them money?
As a vocal IBD patient advocate and leader, I understand and feel for those who haven’t been able to go back on therapies or receive different dosage recommendations they depend on for their well-being. While I’m thrilled to be back on my biologic, now I have the worry about whether my body will respond the same as it did previously.
The medication I’ve depended on for 16 years to bring me comfort is finally back in my fridge and going to be back in my body today. The prior authorization lasts one year, so I’m not sure what the future will bring, but I’m focused on getting my health back on track right now and worrying about that later. I’m grateful my energy in dealing with my own appeal is over and now I can pour my efforts into trying to drive change for our community. We all deserve so much more. Let’s go after what is right and make forced medication switching and off-label dosing delays and denials by insurance companies illegal in the United States.
Ever have a feeling in your gut that says you can trust someone or to make a certain decision? Get diarrhea or constipation when you’re under a lot of stress or anxiety? Your gut is so sensitive and smart scientists call it your “second brain! The human body is a complex ecosystem, with various systems interconnecting in intricate ways. One of the most fascinating of these connections is between the gut and the brain, often referred to as the “gut-brain axis.” This communication network plays a crucial role in maintaining our overall health, influencing everything from mood and cognition to immune function and digestive health. Emerging research indicates that the gut-brain axis may significantly influence the development and progression of IBD. The big question being—how?
This week on Lights, Camera, Crohn’s a look into how the Gut-Brain Axis works and what this means for the future of IBD treatment and care. Whether it’s stress, people pleasing, avoiding emotions, or anxiety—there are many triggers aside from food.
The Gut-Brain Axis: A Two-Way Street
Before we get started, it’s helpful to understand what the gut-brain axis involves and the multiple pathways it impacts, including the nervous system, the endocrine system, and the immune system. The primary components of this axis are:
The Enteric Nervous System (ENS): Think of this as how it feels when you get “butterflies in your stomach”. The ENS is a vast network of neurons (nerve cells that send messages all over your body to allow you to do everything from breathing to talking, eating, walking, and thinking) embedded in the walls of the gastrointestinal tract. It operates independently of the central nervous system but communicates with it via the vagus nerve, which runs from the brainstem to the abdomen.
Neurotransmitters and Hormones: The gut produces and responds to various neurotransmitters and hormones, including serotonin, dopamine, and cortisol. These chemicals are crucial for regulating mood, stress responses, and digestive functions.
The Microbiome: Trillions of microorganisms reside in the gut, forming a complex and dynamic community known as the microbiome. These microbes play a critical role in digestion, immune modulation, and even the production of neurotransmitters.
The Gut-Brain Connection and IBD
Chronic inflammation in IBD can affect the enteric nervous system, leading to alterations in gut motility and sensitivity. Those of us with IBD often experience abdominal pain, cramping, and changes in bowel habits, which are partly mediated by the nervous system. Conversely, stress and psychological factors can exacerbate IBD symptoms. Stress activates the hypothalamic-pituitary-adrenal (HPA) axis, leading to the release of cortisol and other stress hormones, which can, in turn, promote inflammation in the gut.
The Role of the Microbiome
The gut microbiome is crucial in maintaining intestinal health and regulating immune responses. For those with IBD, the composition and diversity of our gut microbiomes are often disrupted, a condition known as dysbiosis. Dysbiosis can contribute to the chronic inflammation seen in IBD by impairing the gut barrier function and promoting an overactive immune response. Interestingly, the microbiome also communicates with the brain through the production of metabolites and neurotransmitters, which influences mood and cognitive function.
You can optimize your gut microbiome with diet by eating:
Low sugar fruits (avocado, bell peppers, cucumber, tomato, zucchini, limes, and lemons)
*Before altering your diet or incorporating foods that could trigger disease activity, please talk with your care team and discuss this further with a registered dietitian who specializes in IBD.
Psychological Factors and IBD
IBD is often associated with psychological conditions such as anxiety and depression. According to the Crohn’s and Colitis Foundation, we’re two to three times more likely to deal with anxiety and depression than the general population. These mental health issues can both contribute to and result from the physical symptoms of IBD. For instance, chronic pain and discomfort can lead to increased stress and anxiety, while anxiety and depression can exacerbate gut inflammation and symptom severity. It’s a vicious cycle that can often feel out of our control.
Therapeutic Implications
Understanding the gut-brain connection opens new avenues for the way we treat IBD. Traditional treatments focus on reducing inflammation and managing symptoms through medications and lifestyle changes. However, addressing the gut-brain axis could provide additional therapeutic benefits. Some potential approaches include:
Probiotics and Prebiotics: These can help restore a healthy balance in the gut microbiome, potentially reducing inflammation and improving gut health. Talk with GI about their thoughts on this, as each provider has their own opinion.
Psychological Interventions: Cognitive-behavioral therapy (CBT), mindfulness-based stress reduction (MBSR), and other stress-management techniques can help manage the psychological aspects of IBD, potentially reducing symptom severity. Tools such as breath work and gut-directed hypnotherapy can help to improve GI systems, while improving your mood and decreasing stress. This works by softening the body’s stress response, inhibiting the secretion of cortisol, decreasing inflammation, and supporting the immune system.
Dietary Modifications: Certain diets, such as the low-FODMAP diet, can help manage symptoms by reducing gut irritation and inflammation. Personalized nutrition plans based on an individual’s microbiome composition are also being explored. Connecting with a registered IBD dietitian can provide you with a personalized plan geared to where you’re at on your patient journey—this will differ if you’re recovering from surgery, pregnant, flaring, the list goes on. Diet is not a one size fits approach, it’s unique to you. Before you start eliminating entire food groups and putting difficult limitations on yourself, talk with a professional.
Pharmacological Treatments: Medications that target the gut-brain axis, such as those that modulate neurotransmitter levels, are being investigated for their potential to treat both the psychological and physiological aspects of IBD.
Final thoughts
Our gut and brain are in constant contact through nerves and chemical signals, and taking care of our mental health and our gut health goes hand in hand. The relationship between our gut and brain is a fascinating and complex one that significantly influences our overall health, playing a pivotal role in everything from mood and cognition to immune response and digestive health. For those of us living with IBD, understanding and addressing this connection can provide new insights into the management and treatment of our disease.
As research continues to uncover the complexities of the gut-brain axis, we move closer to a holistic approach to IBD care that considers the intricate interplay between mind and body. Know that there are psychologists who specialize in gastrointestinal illnesses as well as dietitians who do as well. By adding specialists like this to your care team, you’ll be better equipped to manage the unpredictability of life with Crohn’s and ulcerative colitis.
Imagine a medication that not only helps shed unwanted pounds but also holds the promise of alleviating the painful and debilitating symptoms of inflammatory bowel disease (IBD). For millions battling the dual challenges of IBD and weight management, this could be a game-changer. Some reported data suggest approximately 15 to 40% of IBD patients experience obesity. As obesity has been linked to more severe disease activity, anti-obesity medications, such as GLP-1 (glucagon-like peptide-1) receptor agonists (RA), could be a novel treatment strategy for IBD.
Recent research into GLP-1RA medications, primarily known for their role in weight loss and diabetes management, suggests they might have unexpected benefits for those with Crohn’s disease and ulcerative colitis. Could these medications pave the way for a new era in IBD treatment? This week on Lights, Camera, Crohn’s let’s dive into the intriguing possibilities that lie at the intersection of weight loss and inflammatory bowel disease management. You’ll hear from gastroenterologist and researcher Dr. Aakash Desai, along with 25 people who have IBD and have tried or are currently taking GLP-1RA medications.
What is a GLP-1RA medication?
GLP-1 (glucagon-like peptide-1) medications are primarily known for their role in managing type 2 diabetes and obesity. GLP-1 agonists, such as liraglutide (Victoza), semaglutide (Ozempic), and dulaglutide (Trulicity), mimic the action of the endogenous hormone GLP-1. These drugs enhance insulin secretion, inhibit glucagon release, slow gastric emptying, and promote satiety, thereby aiding in blood glucose control and weight loss.
The majority of these drugs are subcutaneous injections, with only one currently available orally. The frequency of taking the medication varies with each GLP-1RA and can be weekly, daily, or twice daily. But, the typical dose is a weekly self-injection, which can be done in your stomach, upper arm, buttocks, or thigh.
The Mechanistic Link to IBD
Anti-inflammatory Properties: GLP-1 receptors are present in the gastrointestinal tract and on immune cells. Activation of these receptors has shown anti-inflammatory effects in preclinical studies. This suggests that GLP-1 medications could theoretically modulate immune responses and reduce inflammation in the gut.
Mucosal Healing: Animal models have demonstrated that GLP-1 agonists can promote mucosal healing in the intestines, a critical aspect of managing IBD. This potential for enhancing intestinal barrier function and reducing inflammation holds promise for IBD therapy. Scroll to the bottom of the article to check out the latest research.
Considerations between providers and patients
Dr. Aakash Desai, MD, Allegheny Health Network in Pittsburgh, Pennsylvania says that before discussing if GLP-1RA is appropriate for his patients, he tries to understand their weight loss journey on a case-by-case basis.
“This is unique for every patient, so it’s important for the physician to understand where they’re at and the efforts that have been made. I like to ask what type of dietary and lifestyle modifications they have attempted, exercise (finding out actual numbers, number of days/minutes per week of exercise, moderate/strenuous intensity), prior consultations with nutrition and/or weight loss specialist, and prior exposure to weight loss medications. It’s also important to consider comorbidities, especially history of pancreatitis, gallbladder disease, type 2 diabetes mellitus, and psychiatric diseases including eating disorders.”
He tells me a “good” candidate is a patient who is obese or overweight with weight-related complications who is willing to undergo lifestyle interventions in close collaboration with nutrition and a weight loss specialist. From an IBD standpoint, before starting on this type of medication, Dr. Desai likes to see his patients in remission.
“GLP-1RA medications have several GI side effects, so it can be challenging to differentiate if a patient’s symptoms are related to GLP-1RA, active IBD or both. Patients should have their IBD in remission, clinical and endoscopic, and radiographic, if applicable,” explained Dr. Desai.
There is preclinical data suggesting that GLP-1RA can modulate inflammatory responses.
Dr. Desai explained, “Mechanisms include its impact on oxidative stress, immune cell recruitment, cytokine production, and gut microbiota modulation. There is also some clinical data from retrospective studies showing improved IBD outcomes, however we need data from prospective studies to see if these medications can be used as adjuncts with existing IBD therapies.”
He would not recommend starting GLP-1RA for obesity management during a flare/active disease given the risk of drug related GI side effects. This could worsen symptoms which could inadvertently lead to increased dose of steroids, prolonged steroid use or a change in IBD therapy. Additionally, providers prescribing GLP-1RA have a low threshold to discontinue the medication if patients with IBD develop even mild GI symptoms out of potential concern for worsening IBD.
Ongoing research underway
Dr. Desai is working on a study that involves 150 people with IBD who are obese and taking semaglutide.
“We found similar weight loss compared to patients without IBD. We also found higher weight loss with semaglutide compared to other anti-obesity medications except tirzepatide. We did not observe worsened IBD specific outcomes in patients on semaglutide. In another study from a large database, we found that GLP-1RA use for type 2 diabetes in patients with IBD was associated with a lower risk of surgery for ulcerative colitis and Crohn’s disease, but we did not observe a lower risk of steroid use.”
He tells me it’s important to note that this is retrospective observational data. However, Dr. Desai hopes this sets the stage for prospective studies and future randomized controlled trials.
From a safety standpoint, there is limited data, however it appears to be reassuring for serious side effects. Dr. Desai believes until we have more robust data, the key will be disease remission at the time of initiation of GLP1-RA. Keep this in mind if you are dealing with active disease and hope to start this type of medication.
There is no data to suggest that patients on biologics or small molecules cannot be on a GLP-1RA if their disease is in remission. The approach needs to be individualized factoring in clinical characteristics and disease profile.
Scope and Scans and GLP-1s
There seems to be confusion in the patient community about how these weight loss mediations can impact how we prep and undergo scopes and scans. Dr. Desai says there is currently no data supporting stopping GLP-1RA before elective endoscopy – which is a multi-society statement.
“I follow the clinical practice update published by American Gastroenterological Association (AGA) which suggests an individualized approach to each patient. If patients are on GLP-1RA only for weight loss, I think there is little harm in holding the medicine a week before elective endoscopy. An alternative would be to continue the GLP-1RA and place patients on a liquid diet the day before the procedure.”
Dr. Desai says he likes to discuss extended bowel prep (2 days) with his IBD patients.
“Alternatively, I recommend a low fiber low residue diet for 5 days plus 2 days of a clear liquid diet with 1 day of prep. I would encourage patients to discuss management of GLP-1RA and bowel prep with their IBD providers prior to elective endoscopy as institutional protocols especially for anesthesia may vary.”
Hear what an IBD mom has to say about her experience
Emily says she’s been overweight most of her life. She tried everything to lose weight, and nothing seemed to work—or she’d lose weight and gain it right back. She talked with her primary doctor about the weight loss medications and her provider is a big fan of them for the right person and thought they’d be a great fit for her. As an IBD mom of two boys, Emily was worried about what her gastroenterologist would have to say.
“At first, I was nervous about it because I didn’t want him to tell me I couldn’t do it. But he was okay with it. He said if I didn’t have any IBD complications, that I would be fine to be on it. He didn’t have any hesitation since I have been in remission and my colonoscopy and upper endoscopy looked good. I explained that I was followed closely with my primary and that I would let him know if I had any issues that came up. Thankfully, my Crohn’s has stayed in remission!”
Emily started semaglutide in November 2022 and was on that for 7 months and then switched to tirzepatide. She’s now been on that for one year.
“I am starting the process of going into maintenance and will decrease my dose until I find what works for me and plan to stay on this long term.”
Emily’s remarkable transformation from 2022 to now.
She’s currently taking Stelara to manage her Crohn’s. Emily is down 93 pounds, and she feels amazing. She says she has dealt with minimal side effects—some nausea and constipation, but nothing that lasts long. As most of us are, she’s very conscious of her bathroom habits and says if she starts to feel constipated, she takes stool softeners.
Firsthand experience from an ostomate
Elizabeth has perianal Crohn’s and has participated in two clinical trials (stem cells). She has had two gracilis flap surgeries, among others. She says while many IBD patients struggle with keeping weight on, this has not been the case for her.
“I have always been in a larger body (even before my Crohn’s diagnosis 20+ years ago). I workout daily and eat a balanced diet but have, like many, found a natural weight plateau. Since my bloodwork always looks great, I really hadn’t thought about it as it would be seemingly for vanity’s sake.”
With more than a dozen IBD surgeries so far and at least one or two more in the future, she was discussing with her GI wanting to optimize future success post-operatively, when her doctor brought it up.
“Since I carry more weight in my mid-section and currently have a loop ileostomy, which also is poorly placed and with a hernia that causes further projection, addressing those issues was certainly on my mind. I was open to learning more and she was bullish, referring me to a fellow GI doctor who specialized in the area.”
As an ostomate, Elizabeth was concerned about blockages, in addition to insurance not covering the cost.
“My consulting doctor felt confident I was a good candidate, and we both thought it may actually improve my fast GI tract and high-output ostomy (which had been causing daily leaks recently). While insurance denied two different options based on plan carve outs, even after appeals, I decided to try paying out of pocket.”
She started on Zepbound four months ago, in conjunction with her biologic and small molecule medication to manage her IBD. Elizabeth says she was less concerned about adding a medicine but, like many of us, would like to be on fewer longer term.
So far, she has lost 30 pounds or about 12% of her starting weight!
“I wasn’t at my highest all-time weight, but I had gained. The effect was almost immediate for me — with the biggest short-term (and continued) win being the delayed gastric emptying, meaning less liquid output, less rapid output, and less visits to the bathroom to empty. I also stopped having leak issues almost completely and, in conjunction with my IBD meds, my symptoms and inflammation are the best they’ve been in years.”
In terms of the non-IBD effects, the impact on what they call “food noise” was huge and, because food stayed in her stomach for more than an hour or two, her hunger changed dramatically.
“I can’t explain how odd it feels to have to remind yourself to eat and to simply feel full. Fortunately, I have had few side effects as, thanks to my ileostomy, I was already focused on staying hydrated.”
Elizabeth encourages those with IBD to research and consult with a doctor who specializes in obesity medicine (and versed in IBD and/or willing to work with your IBD team). Unlike many of the medications we use to control our disease, antibodies aren’t a concern, and it could be worth a try. Also, she says not to be discouraged if it doesn’t work for you as, just like IBD meds, what works for one person may not work for someone else.
“While the weight loss is great, the impact on my IBD-related quality of life has been just as important. I hope there is more research in this area and potential a path for these medications to be considered as part of a covered treatment plan for patients with IBD and other chronic conditions.”
What other IBD patients have to say
Thank you to those who submitted input for this article—there’s nothing like hearing firsthand perspectives from those living our reality. I have purposefully left all the quotes anonymous.
“I have been on Wegovy for over a year, and I have ulcerative colitis. I’ve had a positive experience and from what my GI told me, there are clinical trials going on for its effect on IBD patients specifically.”
“I started Ozempic last week. My GI approved it. There is lots of research about reducing inflammation, along with other benefits. I am way overweight, and I needed help.”
“I’m on semaglutide, which is the generic compound of Wegovy. My GI approved it and it’s been great. It’s the only way I’ve been able to lose weight in years! It has helped me with cravings, with blood sugar stability, and with my emotional connection to food. The first six weeks, I lost my interest in food and had a weird metal taste in my mouth. But slowly that went away and now I am back to myself but feeling more in control and with a healthier view of food. I have not lost weight as fast as some, more like 1-2 pounds a week with a plateau where we found the dosage needed to be increased. Slow and steady has been fine for me.”
“I have ulcerative colitis and got a jpouch back in 2010. I was on Ozempic last year but got off to get pregnant. Once I’m six months postpartum I was told I could go back on it.”
“My CRP is back to normal, even though my SED rate is still elevated, my IBD is non-existent. My constipation did get worse though. But it’s nothing that daily Miralax can’t help. I had to come off it because it made my anxiety worse. Being on that medicine made me as close to feeling like a normal human being as ever.”
“I have been on Ozempic for the past month. No lie, best I’ve felt in years! It’s taken my 20 bowel movements a day down to 3-4. I have nausea, but it’s tolerable. I don’t have diabetes, so I’m paying out of pocket for it. Those with diabetes get a greater benefit from it. You have to be serious about eating protein and about eating better. Since the food you eat sits in your stomach longer, you’ll feel sicker if you’re just eating junk.”
“I would love to hear more about this as IBD is one of the contra indications for this medication and is not usually prescribed in the UK for people with Crohn’s/ulcerative colitis, as it can cause GI upset. So, I would love to hear more about people’s experiences with this as this is something I have looked into for my weight, and I have Crohn’s.”
“My PCP said in her experience they have helped GI outcomes, but I haven’t talked with my GI to see his response. I will say, as an OR nurse, we have been seeing a lot of exploratory laparoscopic surgeries with patients on these medications.”
“I have UC and they put me on Ozempic last year! One shot and I couldn’t stop vomiting. I lost 35 pounds, but I had to take Zofran daily and used a Scopalamine patch so I would not vomit. I started in April, and I didn’t get better until July or August. I went into the ER and urgent care several times for dehydration. It was mild pancreatis, but my labs were not bad enough for them to admit me.”
“I was on Victoza! My GI symptoms were exacerbated by the medicine, but my A1C went down significantly. Unfortunately, I was throwing up for the first month I was on it and because of that my appetite was not suppressed.”
“I was on Ozempic. It made me nauseous and sick. I had terrible stomach pains and TMI, but super gross mucus-y stools. As soon as I stopped, everything went back to normal. I lost 20 pounds and then gained it all back immediately.”
“I have Crohn’s and I’ve been on Saxenda for 8 months and I’m down 20 pounds. Other than a little nausea in the beginning, it’s been great for me!”
“Started semiglutide injections 2 weeks ago and I’ve been able to stop taking my Loperamide completely (I have ulcerative colitis and a jpouch). Semiglutide wasn’t covered by insurance even with appeals for weight loss and motility, but I got it pretty affordable online through Henry Meds. I’m still on the loading doses but haven’t had side effects so far. It takes about 2-3 months of weekly injections to build up to a full dose.”
“I experience nausea day two after taking the shot. Other than that, I haven’t dealt with anything negative. I lost weight that wasn’t coming off due to hormones being completely screwed from pregnancy and 60 mg of prednisone for almost 9 months. GLP-1s also constipate you, due to your gut not emptying as quickly as it normally would. This is one of the reasons it’s being explored as an IBD option. Taking magnesium, bulking up on fiber or taking fiber helps with this.”
“I am on semeglutide week 6 tomorrow—this is my second time—I did it last summer for about 3 weeks. I went up on my dose last week, I haven’t noticed a difference with anything yet, but I haven’t changed my diet much and that’s on me. There’s no difference in my ulcerative colitis symptoms, I’ve had mild active uc for awhile now. I’m trying to get it under control, but also need to lose a bit of weight.”
“Back in 2022, I was on Mounjaro for about 8 months. I was finally able to lose weight. I am a Crohnie who gains weight because my body has a hard time digesting nutrients. Because of this, my body is in starvation mode a lot. When I was on Mounjaro, I lost about 80 pounds, and my inflammation was well managed. It was the first time I was able to feel energetic and wasn’t tired all the time. It helped with my diarrhea because it made me constipated for the first time in 5 years. It then became regulated. I still had stomach pains and indigestion issues, but overall, the medication improved my quality of life quite a bit. I am pre-diabetic and now my insurance will not cover it. My doctor tried appealing it many times, explaining that Mounjaro was helping to manage my inflammation caused by Crohn’s disease, and they still denied it. I have gained 30 pounds back and have a hard time with energy and my diarrhea has returned on and off.”
“I’m on Mounjaro and taking it specifically to help with my high output ostomy. I have Type 2 diabetes, so I’m able to get it through insurance luckily, since we’re using it “off label”. A friend of mine who has a jpouch was on Saxenda, then Ozempic, for the same reasons. She recently had to go off it because of new insurance and she developed pouchitis within weeks of having to stop it. I have two other friends with ostomies taking it, both with a history of Crohn’s. One is a CEO of a biotech company and has been chatting with the different GLP-1 manufacturers trying to convince them to do trials in patients with short gut or high output ostomies.”
“The first thing I asked my GI doctor is HOW can someone have IBD and be overweight or obese? And he said it’s quite common! When I started to flare, he wanted to blame the diarrhea on GLP-1 (Wegovy). But I asked him for a colonoscopy which showed active ulcerative colitis, unrelated to the medication. I am now on Zepbound. For some reason, these medications don’t help me lose weight. I can’t help but wonder if the inflammation from IBD is preventing successful weight loss. I can have many bowel movements a day and not lose a single pound!”
“I have had a good experience with it. I have a really tough time eating vegetables and some fruits, nuts, etc. because of my Crohn’s. The fact that the medication decreases that hunger helps me maintain a healthy weight. I tell people that all the “food noises” I used to experience are gone.”
“I am researching this for Crohn’s myself. I am interested to see your article and opinion. I’m in the UK and recently heard about the benefits of microdosing and I wanted to see if IBD people had experienced positives.”
“I was originally on Ozempic, and it wrecked my stomach. I had to take a break from it, but I lost weight. I switched to Mounjaro due to insurance and have had way better luck with no GI issues. Altogether, I have lost almost 50 pounds. I should mention that I am pre-diabetic. I have a really hard time losing weight. When I was pregnant, I lost 35 pounds after I gave birth and didn’t gain a pound during. I felt amazing, not sure why I wasn’t hungry when I was pregnant. Mounjaro has allowed me to not think about food 24/7. It’s been a game changer.”
“I’ve Googled it before (because who that’s overweight hasn’t been at least curious) and I remember reading that because it slows digestion it can help IBD patients. I’m still worried about the unknown long-term effects to try to it.”
Final thoughts
It’s important to understand that these are chronic medications for obesity management. GLP-1RAs are not a substitute but should be used in conjunction with lifestyle interventions including diet and exercise. This is necessary for sustained long-term weight loss. This requires a multi-disciplinary team-based approach with nutrition, weight loss specialist, primary care and your IBD provider.
As you heard from the patient community, access and cost for these medications remains a key issue for many. The high cost and complex insurance landscape pose significant barriers for many patients seeking these treatments. The monthly cost of these drugs in the United States can range from several hundred dollars to over one thousand dollars, presenting a substantial financial burden for patients. Many insurance companies require prior authorization for GLP-1RA medications, necessitating extensive documentation and justification from healthcare providers. This process can be time-consuming, and as we’re all too familiar with, may delay treatment.
I’ll leave you with an impactful quote from Emily, “I think for the right person these meds are life changing. I know for me they have been. There is a lot of chatter on both sides, and I have learned to block it out. I work closely with my primary doctor and know that she would never steer me wrong. I also know that my GI is on board and that has helped, too. Don’t let the opinions of others deter you. If this is something you want to do and you have the support from your doctors that is all that matters!”
More than 4 million babies are born in the United States each year, many to mothers who live with chronic illness. Historically, pregnant women are excluded from research, consequently there is limited to no safety data at the time of drug approval. Enormous gaps remain regarding the clinical impact of exposure to biologics and medications when so much is at stake for both mom and baby. July 11-12th the Food and Drug Administration (FDA) hosted a public workshop entitled, “Evaluating Immunosuppressive Effects of In Utero Exposure to Drug and Biologic Products.”
As a patient leader in the IBD community and mom of three children who were all exposed to anti-TNF medication in pregnancy, I was invited to provide the patient voice during this two-day discussion. I spoke on three different panels to share my perspective. This week on Lights, Camera, Crohn’s I’ll share what I learned and what I heard from top researchers and doctors at the workshop. The key overall message—healthy moms lead to healthy babies and a healthy society. Healthy meaning—having disease well-controlled in pregnancy so flares don’t lead to adverse outcomes for both mom and baby.
Pregnant women and lack of research
Often due to ethics, pregnant women have been omitted from research and clinical trials. The absence of human involvement in pharmacology studies can lead to uncertainty about what is deemed “low risk” and “safe” to the fetus, and the impact medications have on the placenta. Women who become pregnant must drop out of clinical studies, even if the drug class has known safety or is deemed low risk (anti-TNF, IL-23s).
It’s clear that reducing or stopping medications can put mothers at risk for flares, which in turn can lead to adverse effects in pregnancy. With my own children, I stayed on Humira until 39 weeks with my oldest (who is now 7), and 37 weeks with my other two children (who are now 5 and 3). All three of my children were a part of pregnancy studies (MotherToBaby and PIANO). My youngest will be followed until age 18! My oldest was followed through kindergarten. The current recommendation, globally (which has changed since I had my children) is to keep women on biologics throughout the entire pregnancy.
One of the key areas of discussion is whether animal data from research ever tells us the whole story about the safety and efficacy of medications—the answer is no. There is no substitute for a human placenta, but the challenge and dilemma are what can be done to get this human data. Approaching clinical trials in pregnant women is challenging and takes time to develop. Currently, animals are the best tool we have for educated guesses.
The benefit vs. risk discussion for Mom and Baby
Oftentimes decision making with chronic illness is a risk versus benefit thought process, whether you are pregnant or plan to carry a baby in the future or not. During the FDA workshop, there was an incredible presentation that really resonated with me about the multiple decisions women have to make for both themselves and their unborn children. The discussion highlighted the complexity and why it’s not a black and white decision. These series of decisions are nested in each other and revolve around the decision maker (Mom/Dad) and medical providers.
Key considerations we deal with as IBD moms:
Continue or discontinue medication?
Should we breastfeed on medication?
Should we give an attenuated live vaccine as scheduled or delay?
When making these decisions it’s imperative that patients feel heard and that communication take place between the parents and medical providers (gastroenterologist, maternal fetal medicine, and OBGYN). Knowledge is power and educating yourself going into these conversations and before and during pregnancy can make you feel more empowered in your decisions.
The power of the placenta
There were placentalogists at the workshop—yes, those exist!! And it was amazing to learn how dynamic the placenta is and how it changes throughout pregnancy. The placenta is not just a conduit, its function changes across gestation and with fetal sex and medical condition. It serves as the endocrine function, lungs, pituitary, drug processing center, neuro connections, and growth factors for the baby…to name a few.
For instance, according to this study, there are differing levels of placental chemokines and cytokines and even reduction of placental antibody transfer in male placentas.
Once the placenta is impacted it effects the fetus. There was also discussion about how Inflammatory Bowel Disease impacts placenta—and the possibility of looking at the placenta of an IBD women at delivery to compare them to women without the disease. Even when a woman has well-controlled disease or is in remission, it’s believed our placentas may appear differently at delivery due to the inflammatory nature of our disease. I joked during on one of the speaking panels that I would have gladly given all my placentas to research upon delivery! It’s win-win for researchers and patients alike to do so.
Medication safety in pregnancy
There was also discussion about the importance of developing medications that are safer in pregnancy, much like children’s medications are created with a different formulation.
Prednisone causes minimal fetal exposure. Solumedrol at infusions is fine, and it’s ok to breastfeed on steroids, but high dose daily oral steroid can cause cleft palate and cleft lip.
Azathioprine has also been found to have no impact on breastfeeding, babies born to moms on Azathioprine have normal development and they do not have increased susceptibility to infection.
A graph outlined a study that looked at 107 pregnant women with IBD on Infliximab/Adalimumab:
Detectable anti-TNF levels after birth:
3 months of age—94%
6 months of age—23%
9 months of age—7%
12 months of age—3%
This illustrates why babies exposed to anti-TNF after believed to be immunocompromised until 6 months of age.
Vaccine response and impact of immunosuppressive medications
It is believed that women on immunomodulating medication who get the TDAP vaccination in pregnancy have the same immune response as healthy controls and that the baby receives the same benefits.
The recommendation for Rotavirus (which is the only live vaccine given the first 6 months of a baby’s life), is now to give this vaccine to babies. This updated guidance also applies even when babies are exposed to anti-TNF or immunosuppressive medications in pregnancy.
There’s no difference in vaccine response for babies across different biologics.
Limiting the burden on mom and baby in pregnancy and postpartum studies
Once babies are born and they are part of research studies to measure how their exposure in utero impacts or does not impact their future health, there’s often a burden on the mother about following up. As an IBD mom myself, I wasn’t big on having my babies get blood draws for medical studies—but that data is paramount in helping further that research. And knowing what I know now, I wish I would have been more willing to do so.
So how can studies ease this burden and stress on families?
This can be done by having well-trained phlebotomists who have experience working with children and using techniques to optimize venipuncture success to limit discomfort and pain. By timing blood draws for research at the same time of doctor’s appointments, it reduces the number of needle sticks and blood draws.
Dr. Mahadevan’s Presentation at the workshop
One of my favorite presentations was given by Dr. Uma Mahadevan. She is the key investigator of the PIANO (Pregnancy Inflammatory bowel disease and Neonatal Outcomes), and a well-respected gastroenterologist at UCSF. PIANO started in 2007 and looks at the safety of IBD medications on the pregnancy and short-and-long term outcomes of children. My youngest son is part of PIANO. We participated throughout pregnancy, provided cord blood from delivery, as well as blood draws. I just submitted his 3-year forms online.
I recorded Dr. Mahadevan’s presentation and have transcribed everything she said below so you could hear her expertise firsthand:
“Women of childbearing age—women of reproductive potential are not given JAK inhibitors—even though it may be the most effective medication for them. This is a result of fear—that maybe they’ll get pregnant and maybe there will be some harm. Medications with well-established safety records like anti-TNFs are discontinued in pregnancy now—68% of women who go off their anti-TNF did so from the advice for their rheumatologist, so these are the doctors telling them to do this.
What’s the importance of treating immune mediated disease in pregnancy?
Disease activity is the biggest driver of adverse outcomes in pregnancy. Women with IBD compared to general population have an increased risk of spontaneous abortion, pre-term birth, small for gestational age, hypertensive disorders of pregnancy including preeclampsia , post-partum hemorrhage, and 44% rate of C-section, most of them elective out of fear of disease.
Stopping the biologic which again is out of fear—you’re on a biologic, it’s stopped in pregnancy, still is in many rheumatology and psoriasis cases, less so with IBD, but when you stop it…reducing or stopping leads to an increase of disease flare.
Many of my colleagues who are rheumatologists say “oh many with rheumatoid arthritis get better in pregnancy…there is not a single study that shows that. In fact, this study from The National Inpatient Samples shows women with rheumatoid arthritis were more likely to develop complications of pregnancy both during pregnancy, but also in post-partum and in their neonates.
The American College of Rheumatology conditionally recommended continuing anti-TNF during pregnancy despite the available safety data and the voting panel agreed that if the patient’s disease is under control these medicines can be discontinued. This is happening now.
In this article from a prospective registry from Sweden and Denmark that looked at 1700 patients with RA, there was increase in pre-term birth and small for gestational age in RA compared to the general population and that odds ratio increased to three-fold with active disease.
So, there is data that it increases harm in not just IBD but RA as well. We know there’s a strong role for inflammation in pregnancy and in pregnancy outcomes. So, the significant increase in pregnancy and neonatal complications is closely linked to disease activity and inflammation and stopping these low-risk meds and steroid sparing therapies lead to increased suffering for the mother, and post-partum flares and worst outcomes for the infant.
Healthy mother=Healthy Baby
So, what are some of the study designs and limitations-these have been brought up before. Pregnant women are not included in clinical trials. There’s unmeasured confounding in uncontrolled studies. Disease activity impacts the decision to continue or discontinue therapy. It’s not random. The choice of therapy is not random it is linked to their disease severity and what they have.
If you have a series of 100 patients or 1000 patients or 10,000 patients, you may not pick up the signal. The types of studies that are used for the most part are large data sets, so birds eye view and the highest quality study are large population studies from countries in Scandinavia usually where they have longitudinal assessment, parent-child linkage, and a good assessment of diagnosis in pregnancy outcomes. However, these are limited by a fair assessment of medication because they can only measure prescription and not whether the patient is actually taking the medicine. At a very poor assessment of disease activity and very granular data.
People are more likely to report a complication than a healthy pregnancy—incomplete info.
Let me tell you about PIANO—this is a prospective national registry of pregnant women with IBD started in 2007. PIANO divides people into four groups:
The unexposed—which could include people on steroids, 5 ASAS, antibiotics.
We define exposure as anytime within 3 months of conception through pregnancy. We compare the offspring of women exposed to a medication to offspring of women with IBD who have not been exposed. We looked at multiple different outcomes including pregnancy and neonatal outcomes , we administered questionnaires each trimester of pregnancy, three times in the first year of birth and then annually and we continue to follow these patients out to age 18.
So, here’s some of the data that has been published:
Corticosteroids –I often hear from providers, “oh I’ll just stop their medication and if they flare, we’ll give them steroids.” This actually leads to increase rates of pre-term birth, low birth weight, and NICU admission. Of course, the use of steroids is mostly tied to disease activity. It’s hard to separate the two. But the whole point is that you don’t want disease activity, you don’t want steroid use, you want them to be on a steroid sparring effective therapy.
The primary results of PIANO were published in 2021 in Gastro. We looked at 1,400 IBD pregnancies, 379 were not on drugs, 242 were on thiopurine, 642 were on biologics (Primarily anti-TNF), and 227 were on both biologic and thiopurines so about 1,000 biologic exposed pregnancies. We found no increase in birth defects, spontaneous abortion, preterm birth, low birth weight, or infections in the first year of life. We saw an increase in spontaneous abortion with disease activity and we used the Ages and Stages questionnaires to look at developmental milestones and saw no reduction.
We measured placental transfer and we measured maternal and cord blood for inflammation on day of birth. The highest transfer was with infliximab—the lowest was certolizumab, which doesn’t have the FC portion. Vedolizumab had a lower level in the infant than the mother. When this data first came out the first reaction was – “oh we should stop the biologic early”…so in Europe they have more of a glass is half empty look at medications in pregnancy…US tends to be glass is half full. So, they decided to stop at 22 weeks and that was in their official guidance. And it was not until 2 years ago that that was changed to match US recommendations because their own data showed an increase in disease activity and worse outcomes with doing that.
The concern was if you have this placental transfer, if you have therapeutic drug levels in the infant for several months after birth, do they have higher rates of infection? And we showed in PIANO there is no increase in infection at 4 months of age and at 1 year and we looked at if infection rates were relative to the level of drug in the infant at the time of birth, and there was no association to drug level at birth and recent infection.
So based on that now, we don’t stop the biologic at all during pregnancy, we continue it throughout. A systematic review and meta-analysis looking at 8,000 women with IBD who were exposed to biologics showed no increase in infant infections, antibiotic—- showing that biologics do not cause harm.
This data from Antoine Meyer who uses a French patient sample looked at women on anti-TNF and thiopurines and showed no increase in the risk of early life malignancy in children.
We ask about infection—we ask about immune suppression—we ask about malignancy and so far in these 3700 thiopurines and 3400 anti-TNFs from 3 years of age going out to 11 years of age, no increase. Very reassuring data.
PIANO looks at developmental milestones—out to 12 months and up to 4 years—shows no decline, we actually showed patients on TNF had statistically superior developmental milestones in every category compared to the national average and even within PIANO—not to say that TNF’s make your kid smarter…but the whole idea of controlling inflammation is what allows these kids to lay down their neural pathways.
What about the newer biologics?
Ustekinumab and Vedolizumab—again showing no increase in harm for both pregnancy and infant outcomes.
Antoine Meyer again from the French database looked at 398 vedolizumab pregnancies, 464 Ustekinumab pregnancies…again, no increase in harm for all these important outcomes.
It’s not just congenital malformations, what else can happen with these medications?
We’re working with Susan Fisher who is a placental scientist at UCSF, a question was raised about Vedolizumab inhibits alpha 4 beta 7, which can inhibit MAdCAM, which is involved in the process of plasmatation—so if you inhibit MAdCAM are you going to have issues in plasmatation. This was just a pilot study. The first one here the patient also had pulmonary hypertension—this is a normal placental at birth…you can see how this looks distinctly abnormal. The second patient was born 39 weeks, mother was completely healthy with her UC had no other issues during pregnancy. Compared to normal placenta…so are there other things we are missing here?
We are conducting a larger study now with multiple biologics the question is it’s not the Vedolizumab is my hypothesis, it’s more a result of inflammation, having IBD…but it will be interesting to see what these placentas look like when we finish. But maybe this is why these patients have higher rates of preeclampsia, higher rates of hypertensive disorders in pregnancy, and preterm birth. It may be related to the impact of inflammation on the placenta.
Small molecules—I feel very comfortable when a new biologic comes out to continue in pregnancy, I feel reassured by the minimal to lack of transfer in the first 14-16 weeks of gestation, with small molecules—they will transfer and Tofacitinib showed teratogenicity at super therapeutic doses, Upadacitinib showed teratogenicity at the doses we use in humans at 30 mg daily—so that does raise concern. There is now some data, again from clinical programs—no increase in birth defects, in pregnancy loss.
Same for –in press—looking at Upadacitinib …128 maternal exposed pregnancies, 80 of which were in clinical trials…similar rates of live births, spontaneous abortion, compared to what is expected.
What about breastmilk? In PIANO, we do collect samples and found the amount of transfer was really miniscule. But all biologics had transfer—we found no increase rates of infection or impact on developmental milestones with patients who were breastfed while the mother was on an immunomodulator.
We talked about vaccines—if these patients had detectable level of biologics—the first 6 months of life will they have normal response to vaccines? We looked at Tetanus — and found the rates of response were similar to infants of mothers who were not exposed to biologics…that was reassuring. We had 40 inadvertent Rotavirus exposures in our TNF babies, they did just fine. This has also been shown in European data as well. And I want to make sure you are all aware of the study from Lancet looking at Rotavirus vaccine—this was a prospective study looking at infants exposed to biologics, they gave 168 biologic exposed infants Rotavirus vaccine—can only be given the first 3-4 months of life, after 6 months it’s not given—so if you say no in the first 6 months, baby never gets it. They found no harm—at this point, we are letting patients on TNF get Rotavirus vaccine, you can argue the US and most areas because of herd immunity, Rotavirus may not be that important, but in other parts of the world it is—and it’s fine to give to patients exposed.
BCG vaccine is different—especially in an anti-TNF exposed baby, it does have a higher rate of TB, having to do with mechanism. There was one death in a European study given vaccine at 1 month of age. BCG can be given after 6 months of age. So Rotavirus is fine within 6 months, but BCG is still recommended after 6 months.
MMR in high-risk populations can be given at 6 months—why did the Europeans, Asians, and Americans have such different guidelines? This May (2024) we all got together for the Global Consensus Conference to create one standard for pregnant women globally and to help spread the word.
Our recommendations are to continue 5ASA, continue sulfasalazine, continue steroids when necessary, stop methotrexate, and continue thiopurine, continue anti-TNF therapy. The US and Europe agree we will not be stopping TNF early, we will continue it on schedule. We’ll continue vedolizumab and ustekinumabon on schedule, and it’s ok to start these medications in the middle of pregnancy.
Biosimilars have equal safety as originator. The Europeans didn’t understand why we wanted to include this, but this is a common question that comes up in the US. We consider biosimilars safety to be equal to the originator drug.
IL-23 therapies… even though not well studied, we feel based on mechanism they can be continued.
Small molecules should be discontinued—but particularly for the JAKS though, unless there is no effective alternative, they can stay on them. I have had patients where they have to stay on Tofacitinib and Upadacitinib because there was nothing else that worked for them.
Inactive vaccines should be given on schedule. we suggest live rotavirus can be given to children exposed to anti-TNF and recommend BCG be avoided in the first six months.
Final thoughts
A recording of this two-day FDA workshop will be available online in the next two weeks. I will share the link as soon as it becomes available. on my Instagram (natalieannhayden). There were fantastic discussions and as an IBD mom who has gone through pregnancies while on a biologic I am grateful for the consideration and the research that’s going on to help couples feel more confident and at ease about bringing life into this world while juggling complicated health conditions. The conversations and presentations at the workshop were extremely complex, I did my best to translate the information, so the patient community has a better grasp of where we stand about IBD pregnancy research.
If you have IBD and are planning to be a mom or if you are currently pregnant, please consider joining the PIANO study and being a part of this life-changing research for our community.
Living with IBD can be especially challenging in a professional setting. Prior to becoming a stay-at-home mom and freelance/blogger, I worked full-time for 12 years. For 10 of those years, my Crohn’s was not in remission. This week on Lights, Camera, Crohn’s, guidance on how to approach conversations with your boss and co-workers effectively so you can feel supported.
The more they know
Before I became self-employed, I worked at three television stations, a public affairs PR agency, and in Corporate America as a communications specialist for a natural gas utility. With each interview and onboarding process, I waited until I was hired to disclose that I had Crohn’s disease to my boss. The first week of work, in a one-on-one meeting I openly shared about my disease and tried my best to educate my boss and my team about my health. Since I did not start blogging or any patient advocacy work until 2016, there was nothing online about my journey with Crohn’s. If I were trying to get a job nowadays, I wouldn’t have that luxury since my story is publicly shared. Every single boss, all my co-workers, and each employer were extremely understanding and empathetic about my struggles. I was incredibly lucky in that regard.
While working full-time I had several hospitalizations and bowel resection surgery that kept me out of work for 2.5 months. I was grateful for bosses who were generous with sick time and that my corporate job had a solid short-term disability plan I was able to utilize.
Everyone has a different opinion about when and how to best disclose your health or disability status. While some people consider their IBD a “disability,” others do not. I’m often asked how to navigate answering that question on a job application. I personally do not consider my IBD to be a disability, but it’s understandable if you do. Answer as you see best fit and most comfortable.
Why It’s Important to Share
Accommodation Needs: Explaining your condition can help you receive necessary accommodations, such as flexible work hours or the ability to work from home during flare-ups. One of the major benefits of the pandemic is how it altered how we work. Back when I was in the workforce, working from home wasn’t utilized as much as an option. I had high symptom days where I worked from home once or twice every few months, but it wasn’t a weekly occurrence. Hybrid working environments or remote jobs are ideal for those with chronic illness.
The flexibility work from home jobs provide is huge—whether it’s being able to work from your couch if you’re dealing with abdominal pain and it hurts to sit at a desk, being able to work in comfortable clothes or pajamas if the fatigue makes showering a challenge, or worrying about the commute and being able to travel without a bathroom mishap or having to go multiple times in a public employee bathroom…the list can go on and on.
Understanding: Colleagues aware of your condition are more likely to be supportive and understanding during challenging times. One of the most important aspects of IBD to share with others who do not have our disease is the unpredictability of our health. Since we’re able to look perfectly normal on the outside, it can be difficult for an average person to fully grasp or believe the pain we’re dealing with. I remember countless days in Corporate America having to unbutton my work pants and having to tell my co-workers I was on the struggle bus. I can still envision myself on the news desk when the camera shifted to a weather segment and slumping over in pain. Everyone I worked with was aware of when I was having an “off” day. I’ve had co-workers drive me to the emergency room during the workday. I always felt supported and was never made to feel like I was less than because of my Crohn’s and for that I am still grateful.
Reduced Stigma: Talking openly about Crohn’s and ulcerative colitis can help reduce the stigma associated with chronic illnesses and foster a more inclusive workplace. People may question or wonder why you may have unique work accommodations, while it’s none of their business, being transparent, and really stepping up to the plate and going above and beyond when you’re able will show others that you never use your disease as an ”excuse”. If you have an infusion or a doctor’s appointment that makes you arrive late, it’s helpful to inform your boss and co-workers so they know why you may be strolling in during the middle of the day.
Preparing for the Conversation
Know Your Rights: Familiarize yourself with your workplace’s policies on medical conditions and accommodations. Understanding your rights under laws such as the Americans with Disabilities Act (ADA) can provide a framework for your discussion. Check out these tips from the Crohn’s and Colitis Foundation.
Plan Ahead and Explain Your Needs: Choose an appropriate time and setting for the conversation. Ensure privacy and sufficient time to discuss your needs without interruptions. I always had a face-to-face conversation with my bosses, and they were appreciative of knowing. Clearly state what accommodations you need to manage your condition effectively. This could include flexible hours, a work-from-home arrangement, or having a desk closer to the restroom. Emphasize your dedication to your job and how these accommodations will help you remain productive. For example, “Having the ability to adjust my work schedule during flare-ups will help me stay on top of my responsibilities.” If I was prepping for a colonoscopy or having a scan, I let my team know.
Gather Information: Be ready to explain what IBD is, how it affects you, and what accommodations or support you might need. A high-level explanation is often sufficient.Your boss doesn’t need to know your entire patient journey. For example, “I have a chronic condition called Crohn’s disease/ulcerative colitis that affects my digestive system. This can sometimes cause severe abdominal pain and fatigue.”
Offer Solutions: Suggest practical ways to implement accommodations. For example, “During flare-ups, I could work from home and communicate via video calls and emails to stay connected with the team.” Your boss may have questions or concerns. Be prepared to address them calmly and provide any necessary documentation from your healthcare provider.
Communicating with Coworkers
You don’t need to share all the details. A brief explanation like, “I have a medical condition called Crohn’s disease/ulcerative colitis, which sometimes causes me to feel unwell,” can suffice. Explain how your condition might impact your work or interactions. For example, “There may be times when I need to step away from my desk more frequently.”
Reassure coworkers that while you have a chronic condition, you are still capable of performing your job. For example, “Most days, it doesn’t affect my work, but there might be times when I need a bit of flexibility.”
Encourage an open dialogue. Let them know they can ask questions if they want to understand better, but also respect your privacy. While I was hospitalized, I would often send an email to my team at work to provide them with a high-level update, so they heard the information from me versus someone else. For example, “Hi team! I appreciate all your well wishes. It’s been a difficult few days, but I’m hanging in there. I hope to be discharged from the hospital by the weekend and look forward to seeing you soon.”
Final Thoughts
Talking about IBD with your boss and coworkers can seem daunting, but it is a crucial step toward ensuring you have the support you need in the workplace. By being honest, clear, and proactive, you can foster a more understanding and accommodating work environment. Remember, your health and well-being are paramount, and having open discussions can help you maintain your health, while staying on top of your professional responsibilities. When interviewing for jobs, pay close attention to how an employer manages insurance benefits, short-term/long-term disability, and whether you feel like your boss and co-workers would be people you feel comfortable sharing your health struggles with. You aren’t married to your job, if you ever feel unsupported, seek employment elsewhere. Along with your boss, it’s helpful to talk with Human Resources, so you’re aware of all the medical benefits and support that is available for employees.
While IBD complicates life, I hope you continue to go after your dreams. Sure, there are going to be setbacks and roadblocks along the way, but you are worthy of whatever job or career you want to set out and do. Less than 3 months after my diagnosis, while on 22 pills a day, I landed a job 8 hours away from all friends and family and went after my dream of working in TV news. I’m proud of that and it’s a reminder that this disease doesn’t need to rob you of all you hope to be and all you hope to do. You are not a burden on employers and the sky is the limit for you.
When you live with a disease like Crohn’s or ulcerative colitis, family planning takes thought and special consideration. The first-ever Global Consensus Conference on Pregnancy and IBD was held during Digestive Disease Week (May 2024) and part of the discussion focused on the latest recommendations for pre-conception counseling and family planning. This week on Lights, Camera, Crohn’s hear from Dr. Uma Mahadevan who co-chaired the conference, along with Dr. Christopher Robinson, a maternal fetal medicine specialist. As an IBD mom of three kids and the patient lead for the United States on this initiative, I’m excited to start sharing the latest guidance for our community.
The latest recommendations for IBD women
Couples should get pre-conception counseling.
Remission prior to conception for at least 3-6 months with objective evidence of remission.
All women with IBD should be followed as high-risk pregnancies (however that monitoring works in each country)
Pregnant women should take low dose aspirin daily by 12-16 weeks gestation to avoid preterm pre-eclampsia.
These recommendations were voted on and determined by more than 50 medical providers and IBD patient advocates from around the world. They are the gold standard, and the hope is that the recommendations help clear up the gray area and bring clarity to couples who are planning to grow their family and wanting to conceive.
“Our goal was to have a universal guideline that was the same worldwide. This would reduce confusion and avoid the default of just not giving women appropriate therapy. The Consensus really tried to advise what we, as pregnancy in IBD experts, do with our patients, so that women everywhere can have the same high level of care,” said Dr. Mahadevan.
Considerations for women prior to conception
Dr. Mahadevan says when a woman starts medication, she generally tells her whether it is a compatible with pregnancy or not.
“I also tell them when they are ready to consider conception to meet with me first. So generally – the education and family planning discussions should start before you are even ready to consider pregnancy. For couples, they should give their GI a 6-month window ideally to make sure there is remission, a chance to optimize medication, and get any testing done that is needed.”
Personally, I had bowel resection surgery in August 2015 while I was engaged. We knew our wedding was in June 2016, and following the surgery I reached remission for the first time in a decade, so timing was of the essence. I told my GI at a post-op appointment in November 2015 that we were planning to start trying for a baby right after our wedding. Knowing that, she put me on a prescription prenatal and folic acid to start prepping my body for pregnancy, I also had a colonoscopy the month prior to my wedding to confirm I was in remission.
Recovering in the hospital after my bowel resection surgery, with hopes of one day being a mom.
Dr. Mahadevan recommends patients start 1 mg of folic acid daily when she learns they are considering conception.
“The prenatal with iron can be bothersome to some patients so I wait for the OB to start that. I check Vitamin D, B12, and iron labs to make sure those are all good.”
Dr. Christopher Robinson, MD, MSCR, Charleston Maternal Fetal Medicine says preconception care is an excellent way to plan out a pregnancy path.
He went on to say, “We recognize that the best outcomes are achieved when preconception care is employed prior to conception for optimization of disease management. This is especially true of IBD where there can be a number of misconceptions about safety of medications and goals for nutrition and surveillance of the pregnancy. Thus, I would recommend preconception counseling and establishing a care plan with Maternal Fetal Medicine early in pregnancy (first trimester).”
What does pre-conception counseling entail
Preconception counseling can be extensive. You should expect to go through an entire healthcare maintenance checklist of the following:
Checking labs—vitamin levels, sometimes drug levels
Updating vaccines
Cancer screenings—pap smear, colonoscopy if appropriate
Ensuring the patient is in remission which may require a colonoscopy, intestinal ultrasound or other imaging
Making sure medications are compatible with pregnancy
Reviewing prior pregnancy and if there were complications
Discussing mode of delivery, referring to a Maternal Fetal Medicine doctor prior to pregnancy if prior complications or if a woman is extremely high risk (for example, prior blood clots), has an ostomy, or if there is evidence of malnutrition or difficulty with weight gain.
Discuss starting aspirin at week 12 and set up a visit schedule with your GI, as you’ll generally see them once per trimester.
I had four pregnancies—three healthy, full-term babies and one miscarriage. As soon as I found out I was pregnant I alerted my GI. From there I set up an appointment with my “regular” OB for the initial ultrasound at 8-10 weeks, and then moving forward I had monthly ultrasounds with a maternal fetal medicine doctor, appointments with my GI each trimester, and the regularly scheduled in-office visits with my OB. Even though I had flawless pregnancies each time (aside from the baby I lost around 7 weeks), I was considered “high risk” because of my history of Crohn’s disease and prior surgery.
I had three scheduled c-sections, not because I had perianal Crohn’s, but because my care team allowed me to decide what I felt most comfortable given my health history. If I could do it all over again, I’d do it all the same. I appreciated the extra surveillance for my children and for me, healed beautifully after each abdominal surgery, and was grateful that by staying on Humira until 39 weeks with my first child and 37 weeks with my younger children, I maintained my remission throughout pregnancy and after.
Dr. Robinson said while each pregnancy has specific needs, in general he also follows pregnancy with serial growth checks every 4 weeks across pregnancy (following the targeted anatomic scan).
“It is possible, if a patient has longstanding, well controlled disease, and an optimum prior pregnancy outcome history, to check a 32- and 36-week ultrasound for growth. However, in the first pregnancy, I agree with serial growth scans.”
What remission before pregnancy really looks like
Remission is often a difficult word to define when it comes to living with IBD. As Dr. Mahadevan tells me, “Not everyone can achieve complete remission.” So, what are doctors looking for and what should your target be?
“We are looking to give moms-to-be the best chance at conceiving, keeping the pregnancy, and having a health pregnancy. I like to see normal labs, normal calprotectin, normal colonoscopy, and imaging without visible inflammation. Not everyone can achieve this, but that is the ideal three to six months prior to conception,” explained Dr. Mahadevan.
“IBD has both genetic and autoimmune underlying components that can interfere with development of the placenta and affect maternal nutrition across pregnancy. In these cases, optimization of disease management can improve care and reduce risk for both mother and fetus. The goal of interventions is to reduce the risk for mother and infant through coordinated care with GI, MFM and OB/Gyn in pregnancy,” said Dr. Robinson.
Stay tuned to Lights, Camera, Crohn’s next week when the latest recommendations for IBD medication in pregnancy and lactation is disclosed. A full manuscript with all the recommendations and guidance is in the works, with hopes of the information being publicly available by the end of this year. I’ll be working on the companion piece for the manuscript dedicated specifically to the patient community.