Chances are you’ve heard the song, “Who Runs the World (GIRLS)” by Beyonce. Think of that song and then imagine all the incredible women in the world juggling chronic illness, their careers, and their personal lives. It’s no small feat.
Until recently, there wasn’t a group to celebrate and support us. But now that’s changed thanks to the Chronic Boss Collective. It’s the first and only professional membership designed for ambitious businesswomen living with chronic health conditions to help women dream big in their careers while prioritizing their health without tradeoffs. The international networking membership includes monthly in-person and virtual programming rooted in three pillars: professional development, connection, and wellness.
This incredible group is the brainchild of Lilly Stairs, a well-respected patient advocate and entrepreneur. At the age of 19, Lilly was diagnosed with psoriatic arthritis and Crohn’s disease.
Making the concept become reality
The concept for Chronic Boss Collective had been on Lilly’s heart long before everything came into fruition. As an ambitious businesswoman who prioritizes her health and self-care, she had yet to find a space that holds these two statements to be simultaneously true. So, she created it.
“Throughout my career, I’ve met remarkable women whose lives have been turned upside down by a chronic condition, but they choose to keep going. They choose to give back. They choose ambition in the face of adversity. Every time I encountered a new woman who fit this profile, I couldn’t help but wonder how powerful it would be to get them in a network together,” said Lilly.
Because of her unique lens as a driven businesswoman living with chronic conditions and working in healthcare, she identified a gap that most people didn’t realize existed.
“For the past decade, I’ve had the privilege of watching extraordinary women transform their struggle into their strength. There’s an undeniable magic to these women living with chronic conditions who choose ambition. By harnessing that collective power, the Chronic Boss Collective is taking off like a rocketship.”
Currently there are 100 Founding Members. There’s an open enrollment period going on right now and new members are being accepted. Lilly tells me she expects to triple the membership over the course of this year. You can learn more and apply on the CBC website.”
Let’s talk Member Benefits
The Collective Membership is jam packed with benefits designed to help you level up in your health and wealth. Rooted in professional development, connection, and wellness, the Chronic Boss Collective offers the following benefits:
✔ Chronic Boss Mastermind
✔ Boss Boosts: Professional Development
✔ Boss Breaks: Wellness Events
✔ Monthly in Person Meetings (Boston Only)
✔ Private Online Community
✔ Member Directory
✔ Member Feature
✔ Affiliate Program
✔ Exclusive CBC Curated Resources
Detailed Benefits
Private Community
A custom online platform is complete with a private member directory, resource library, and buzzing chat rooms for you to network away with fellow ambitious members.
Chronic Boss Mastermind
Virtual mastermind with the entire membership! This jam-packed event includes:
Kickoff: Led by our Founder designed to amp you up and set intentions to get after your health and career goals this month.
Networking: Expand your reach and visibility and deepen your connections with the Chronic Boss Collective membership
Mastermind: Opportunity to submit a challenge you’re facing ahead of the meeting and then break into small groups to harness the power of the collective and mastermind it.
“Boss Round”: Lightning round of your top “ask” to get support where you need it most!
Boss Boosts: Professional Development
Monthly Boss Boost webinars lead by members and industry leaders presenting in their “Zone of Genius” designed to help you level up in your career. Think building your brand, negotiating your salary, starting a business while living with a chronic condition…and so much more.
Connection
Monthly in-person meet-up for chapter-based members – a mix of networking and fun!
Boss Breaks: Wellness
Quarterly wellness event centered on taking care of you. From mindful movement to gluten-free bake-alongs!
Member Spotlight
Get featured on the CBC social media and have the exclusive opportunity to contribute to media stories.
Resources
Proven methods, tools, and guides to help you level up in your career while maintaining your health.
Affiliate Program
Earn 10% commission when you refer new members to join!”
The priceless power of community
The Collective launched this past January (2023), and it is remarkable the impact it is already making on the lives of members.
“Every day, members are buzzing about the magic happening in Chronic Boss Collective. Women are connecting online and IRL to give each other valuable health support and share their best career and business advice. Our conversations skip the small talk and get straight to a point of vulnerability. The coolest part is that now our members are collaborating on projects that will make a real difference in people’s lives, like mental health resources and patient platforms.”
While CBC is seeking women who are ambitious, high achievers, and making an impact, fitting that description does not mean you have to be working as a full-time professional or running a large-scale business.
“For example, stay at home moms and chronic illness advocates who have monetized their advocacy work or built a side hustle (think Etsy shop, Amazon storefront, social media influencer, etc.) could be fabulous members,” said Lilly.
Requirements and cost to participate
The Collective is an exclusive membership for high achieving career women and all members go through an application and screening process before being accepted.
“Our virtual international membership is $397/year. Our chapter-based membership, which includes a once per month in person meeting, is $497/year. This is currently only available in the Boston area, but we have ambitious plans to scale to new cities in the coming years.”
Hopes and dreams for the future
Lilly says plans are in the works to massively scale the Chronic Boss Collective.
“Not only do we plan to scale the membership, but we plan to scale our offerings. In addition to the membership, we’ve already launched the Chronic Boss Scholarship which has awarded $31,000 to 31 students living with chronic conditions who have persevered and succeeded. We have big plans to usher in impactful programming that will serve the millions of women who choose ambition in the face of living with a chronic condition. Stay tuned…we’re just getting started!”
Feedback from CBC members
“The Chronic Boss Collective has changed my life in many ways. Since becoming a founding member and acknowledging my worth, my life has changed in ways I never could have imagined. The connections, opportunities, and immediate camaraderie amongst intelligent, inspirational, and courageous women has been my biggest blessing in 2024! The degree to which we draw strength from each other is something I have never witnessed in my life and I’m profoundly grateful to share my Chronic Boss journey with so many astonishing women.” – Lisa Z.
“This group is amazing. Thank you for launching this. I feel like this is the sisterhood that I didn’t know I needed whether for my health, business, or career and I’m just so thankful for it especially at this time in my life.” – Erika P.
“I can tell in just a month that I made the right decision to join. The connections I’ve made and leads already generated through the community will help me grow my design business and allow me to work with my people — authentic and adaptable chronically ill women who are changing healthcare.” – Sarah S.
Everybody copes and has their own unique tips and tricks for undergoing an MRE. I received more than 100 messages with recommendations, there was some overlap and similar advice—but I know our community could benefit from this information and find comfort in it. One of the most challenging aspects of undergoing medical scans and procedures is the mental health aspect—the wait, the wondering. Oftentimes these results do not go in our way and may indicate we are in a serious flare or need surgery. So, while the actual process of drinking contrast and dealing with claustrophobia can be intense, the challenges are often amplified by the dread of finding out the story behind our symptoms. Understand you are not alone in that. I try and just prepare myself for the worst, while hoping for the best. Nobody wants “bad” news, but once you go through the scan and have a better idea of what is going on and then you can go after the flare and get to feeling better.
Here’s the link to Part 1 of “Everything You Need to Know Before an MRE with IBD” in case you missed it.
Advice from the community to ease the MRE experience
“Whether it’s laying there saying prayers (like the Rosary) or focusing on doing something (like walking through Sun salutations or walking through doing something you love to do) that has helped me.”
“As a pediatric patient, my mom was allowed into the MRE room, and she held my foot (the only thing she could reach). Just feeling she was physically there helps my anxiety a lot. Ask for goggles that let you watch a movie are gamechangers because you can’t see anything but the movie, even if you tried!”
“I close my eyes and pretend that I’m lying on a beach and listening to country music. I feel comfortable knowing I can see my feet at the other end, and they can communicate with me. Honestly, I close my eyes and sing my heart out!”
“I listen to the loud banging noises and try to find melodies or patterns. Then, I repeat them back in my head and by the time I’ve done it a few times I’m in a meditative state or the test is over.”
“I try to look up/behind me if I start to feel claustrophobic and you can see outside! I also find it almost relaxing to count the loud clips and beeps. It gets your mind distracted.”
“Picture yourself someone you like; use deep breathing to help soothe your vagus nerve.”
“I know it’s not ideal, but if you are extremely overwhelmed you can always get the test under general anesthesia.”
“I focus on my breathing and imagine I’m in my favorite place.”
“Eye mask with no metal clasps and ear plugs (or music) helps to reduce the sensory overload for me.”
“Before you get in the tube, ask for a towel. Put it over your eyes and do not take it off until they let you out.”
“Deep breaths. Visualize you’re in your favorite place and ask for music. Ask your GI if moving forward Intestinal Ultrasound can replace getting an MRE.”
“I’m normally able to tilt my head up to see out the end of the tube. It helps me so much!”
“Breathing exercises can help.”
“Ask if there is a bariatric imaging machine so you have more room.”
“Slow deep breathing helps me prepare for it and calm down.”
“I close my eyes and envision being on a bench or somewhere hard but with open space for me.”
“Gadolinium has a high allergic reaction. Even if you have not had it before. Communicate with your care team and ask about taking Benadryl.”
“Meditation and Guided Imagery.”
“I take deep breaths and remind myself I am going to be ok. It was quicker than I had expected.”
“Take extra Xanax! I take it for flying and always need more than I think.”
“If they let you pick the music, pick it! Having my music really helps me.”
“See if an Open MRI is available. Otherwise, a big dose of benzos.”
“I’ve been Twilight sedated before, it’s the only way to go!”
“I took Zofran. I also wear MRI safe clothes, so I don’t have to change. I make sure there’s no metal in my bra.”
“Focus on breathing. Close your eyes before being rolled in. Think of something like planning a party or a holiday.”
“I hate it. Hate it. Hate it. Someone told me just don’t open your eyes and it worked.”
“I take Ativan and do breathing exercises.”
“Always ask for a towel or wash cloth to cover your eyes.”
“Keep your eyes closed the whole time. Do not peek. And ask for your favorite music to play.”
“I keep my mind focused on other topics and talk to God.”
“Take anxiety meds! If I have to do this again, I will take something.”
“Let your care team know before you enter the room that you’re claustrophobic.”
“Say Affirmations or imagine being on a vacation on a sunny beach. Anything to divert your mind.”
“Last time my nurse gave me an orange smelling strip that helped so much.”
“I close my eyes and pray or sing songs I like the most in my mind.”
“Slow breathing and counting (in for 4 seconds and out for 4 seconds) or listening to music while in the tube.”
“I always have a Life Saver candy between the contrast drinks.”
“I asked them to bring me back far enough so I could tip my head back and see the ceiling.”
“My sister needs to take 3 anxiety pills for the MRE.”
“Try to find your happy place and go to that in the tube.”
“Have all the good and happy plans run through your mind and ponder them. Daydreams! Mantras!”
“I write stories in my head—like manifestations.”
“Think of a beach on a sunny day.”
“Make lists in your head.”
“Definitely have anxiety meds on hand.”
“Bring a personal blanket. This always helps me.”
“Bring ear plugs in case they don’t have some for you.”
“Use a wedge pillow for your legs (ask for it).”
“Visualize the best vacation, start to finish. Try to remember every detail. Distract your mind!”
“Ask for a heated blanket, it can be chilly in there.”
“When your mind wanders, count. Count breaths in (5) and out (5) and focus on the numbers.”
“Some MRI machines offer a mirror, almost like a periscope. It shows you the outside!”
“Fast paced work out music helps me.”
“I ask before we start that they give me a time update every 15 minutes.”
“It makes me less anxious when I hear the weird and terrible sounds the machine makes if I have NSYNC playing. Have them play music you like that’s also light and funny. (As in 90’s boy bands!)
“My office gives lavender stickers to help calm you to place on the robe. It helped me!”
“I’m SO claustrophobic but I always self-talk “I’m a mother and set the example for my kids.”
“Tell the tech you are nervous. Ask them to check in with you more than they usually would.”
“Remember you can squirm out of the bottom if you need to. Knowing that makes me feel less trapped.”
“Lavender essential oil.”
“I took half a Xanax and enjoyed every second…haha.”
“Take the meds and extra, if possible. I’ve taken up to 4-5 mg of Ativan!”
“They let you choose your radio station or podcast, which can help.”
“I’ve listened to the Hamilton soundtrack. I struggle more with getting the contrast down.”
“Meditation! I always do it before, during, and after.”
“Prepare a playlist or an audiobook and ask if the tech can play it over the speaker.”
“I pray the entire time, so I don’t panic.”
“Try not to investigate too much about the details, it may worry you too much.”
“It’s easier to go in feet first, I don’t know why…but it is.”
“Use the help/panic button and take a break midway through if needed.”
“Be prepared to hold your breath a lot—the tech will guide you.”
“Request a helmet with a mirror. It’ll help you see out of the tube.”
“Try and see how many song lyrics you can remember.”
“Tell them you are nervous. They are more understanding and will talk you through it more.”
“Make sure you give the anxiety meds at least 30 minutes to work their magic.”
“The pills help tremendously, but I also bring an eye mask.”
“Thank you for doing this article, I’ve canceled my MRE twice now out of fear.”
Nearly 19 years of living with Crohn’s disease and this past week I experienced an MRE (Magnetic Resonance Enterography) scan for the second time. I felt nervous, overwhelmed, and scared leading up to the test. The only other time I had an MRE was in July 2015 while hospitalized with a bowel obstruction. The scan was used to determine whether I needed surgery. I was out of it and have little to no recollection of the experience. The results from my MRE in 2015 informed my GI team back then that I needed 18 inches of my intestine removed. Fast forward to the present day, and after being in deep remission since that surgery, I started to experience a worrisome uptick in symptoms beginning in early March 2024.
It took a month to get in for the MRE, but I knew in my heart-of-hearts I needed to get answers. Leading up to the scan, I crowdsourced questions on Instagram and received an outpouring of support that helped make the experience nearly seamless for me. This week on Lights, Camera, Crohn’s I provide a behind-the scenes look at what it’s like to get an MRE and share firsthand advice from a patient advocate who is truly an “MRE pro”. Due to the amount of information, we’re breaking this bad boy up into two parts.
Walking you through the process
I had to arrive at the medical center at 10:15 am and was advised not to eat or drink four hours prior. I set my alarm for 6 a.m. and drank some water. When it was time to get in the car with my husband to head to my MRE, I took a Zofran to help prevent nausea from drinking all the contrast. After arriving at the imaging center, I was brought back to a room where I answered health questions and changed into a hospital gown and pants. I wore a sports bra without metal but was told I couldn’t wear it due to some synthetic fabrics. Then, I received my IV. The nurse took one look at my arms and grabbed a vein finder machine. For those who don’t know, this looks like a wand and puts a light over your arm to highlight veins so the nurse can pick the best option. My husband held the wand for her as she did my IV and she got it on the first try. That was a big win for me.
Once the IV was in, an MRI tech brought me three bottles of contrast (450 ml) to drink, about 46 ounces of fluids. I was told I had 20 minutes for each bottle and hopefully that I would have all three bottles down in an hour. Worst case the tech said I needed two. She told me not to chug too fast as that might make me nauseous. I took it with a straw and scrolled on my phone to distract myself. The contrast tasted like a super flat Sprite with a dull citrus taste. I’ve heard many people must do this in a public waiting room, I was grateful to be in a private room with my husband.
Due to my claustrophobia and anxiety about the test, my GI prescribed pre-meds for me that I picked up from Walgreens prior to the day of my test. He prescribed me four, 0.25 mg Xanax. I had never taken Xanax and did not know how it would make me feel. I called the Radiology center the day before the scan to ask whether I’d be able to get anything in my IV if I was too anxious, and they said if you’re outpatient you can only take anxiety meds orally.
Fellow IBD patients advised I take one Xanax the night before to have an idea of how it made me feel. I followed that advice and I’m so glad I did! Knowing how I responded took a bit of the stress off my shoulders. I took my first Xanax the moment I started the contrast (1 hour prior to the MRE) and then 30 minutes later I took .50 mg (2 pills) because I didn’t feel calm enough. For me, that was the perfect dosage. I felt completely coherent but chill and relaxed.
When I walked into the MRI room I asked if I could have headphones and listen to music. The techs asked me what kind of music I wanted; I said something upbeat like Taylor Swift. Then, I asked for a washcloth to put over my eyes. The scan took 45 minutes, I didn’t have one moment of fear or anxiety. There are lots of loud banging sounds and you hear the tech’s voice instruct you when to hold your breath and when to breathe. I felt very at ease and at the end started to doze off!
Since I had been NPO all day and it was 1 p.m. I was given a bag of pretzels and a bottled water after I changed back into my clothes. My husband had to leave during the scan to pick up our younger two from preschool, but the timing was perfect, and he swung back and grabbed me, so I did not have to drive after the scan. I felt tired afterwards.
After about 3 hours I started to get excruciating abdominal pain that I was not expecting. I’ve since been told by fellow patients that this is a result of the contrast and that it’s not unusual. I was very uncomfortable for about four hours. I spent a long time in the bathroom and on the couch with the heating pad. By about 9 p.m. I felt back to normal.
Guidance from a Veteran IBD Warrior and MRE Pro
Rocio Castrillon has lived with Crohn’s disease for more than 20 years and underwent countless MRIs specific to her IBD, but also for a multitude of other reasons including—Brain, Face/Sinus, Shoulder, Cervical Spine, Lumbar Spine, Legs, and Knee. She’s a true patient advocate in every sense of the word and someone I admire greatly. Through my recent experience, Rocio helped me immensely and even texted me the morning of my scan on her own accord, throughout my test as I drank the contrast, and after when I was stuck in the bathroom in pain. This is a true example of someone who goes out of their way behind the scenes to be a source of comfort and support for others. We have never met in person (yet!) and there’s this level of friendship between us.
“While MREs are specifically used for IBD patients, due to the contrast ingested, as well as injected, they are more complex than the traditional MRI and tend to be lengthier in time. Due to my anxiety and claustrophobia, I’ve had to utilize coping techniques to undergo MRIs and although they are still challenging, it’s yet another aspect of my IBD I’ve overcome. While these recommendations are primarily for IBD patients, many can be considered for a traditional MRI,” explained Rocio.
Check out Rocio’s step-by-step advice as your gear up for your next MRE:
PLANNING
At the time that an MRE is ordered by your gastroenterologist, there are a few considerations to keep in mind. MREs will require prior authorization which may take weeks. Fortunately, this time will allow you to explore options for locations.
In most cases, the MRE is ordered to be performed at the imaging facility that is affiliated with your provider, but you do not have to do your MRE there.
Oftentimes, there are private imaging centers, not affiliated with an academic institution, which can be more cost-effective.
MRI machines are now available in a wider bore design to help reduce anxiety and are recommended for claustrophobic patients. The feeling of a more “open” machine is beneficial. But to locate one, you must call around to determine if your recommended imaging facility has them and/or if you need to seek out an external facility.
At the time of your gastroenterologist appt., and if you have anxiety and/or claustrophobia, Rocio strongly suggests requesting a prescription for a sedative used for panic disorders, such as: Ativan, Klonopin or Xanax, which are short-to-intermediate in duration. While you will only need a prescription for one pill, keep in mind that there are many states that now require identification to pick up controlled substances.
Please note that if you do take a sedative, you will be required to have a driver to accompany you, as you will not be allowed to drive yourself.
Also, at the time of your gastroenterologist appt., and if you have nausea, Rocio strongly suggests requesting a prescription for Zofran to be utilized prophylactically.
Once the prior authorization for your MRE is approved, you will be able to schedule. Request an appt. time that works with your personal eating schedule. Because MREs require fasting, as well as contrast ingestion, patients may find it challenging to drink contrast early in the morning. Rocio tends to have more nausea in the mornings, so she prefers to schedule mid-day scans. While this does mean a longer fasting time, it also allows her to drink more contrast.
DAY BEFORE
Rocio eats a light diet the day before the MRE to prevent nausea as much as possible. While this is not necessary, she’s found it helps with nausea and vomiting.
HYDRATE…before AND after your MRE. While the technicians will explain the need to hydrate following an MRE, hydrating beforehand will allow for easy access to veins for the IV needed to inject the contrast. Hydrating after is crucial to eliminate the contrast from your body.
DAY OF MRE
Before leaving home, be sure to remove all jewelry and/or metal from your body. Because an MRI machine uses a magnetic field, you cannot have any metal on you. Women will be asked to remove their undergarments which have metal.
Additionally, if you continue masking in medical facilities, your mask will be switched out for a mask without metal that the technician will provide you.
An hour prior to the scheduled arrival time, take the prescription Zofran so it has time to kick in before needing to begin the contrast. It will help prevent/reduce the level of nausea and/or vomiting from the contrast.
Upon arrival at the imaging facility, you can take the sedative, as this will allow it time to kick in before you begin the imaging. Because there will be a window of time when you need to consume the contrast and when the imaging begins, this typically works well.
Contrast! While many academic institutions have shifted to a new contrast, Breeza, which is lemon-lime flavored, it is not always available to patients. In the past, Rocio has consumed other contrasts. She wholeheartedly agrees that Breeza is certainly better “tasting” than those in the past. But in full transparency, it still is contrast…haha.
For all her MREs, Rocio has been provided with three bottles of Breeza. Unfortunately, she cannot consume all of them, and at best, she’s drank a maximum of one bottle. While this is certainly not ideal from an imaging perspective, and is NOT medical advice, she’s been fortunate to have been “allowed” to perform the test with just one contrast bottle. The imaging that has resulted has sufficed for the radiologist to review and for her gastroenterologist to see results.
Insider Tip: While this may not be available to all patients at all facilities, Rocio always requests to sit near a bathroom and/or near a trash can if she is in the main waiting area. She says she already has enough anxiety about the MRE, and having people watch her drink contrast tends to make her more anxious. Note this is NOT always readily available, and you will have to adapt to what is available at your facility.
MRE START
Upon finishing the contrast, the technician will take you back to the MRI machine where you will be laid flat. If you have anxiety and/or claustrophobia, be sure to alert the technician as they can make you more comfortable in a few ways.
Typically, a technician will ask for your music preference as they’re able to control the music that you hear via headphones (provided to you)
Rocio prefers relaxation/spa music as it helps to keep her calm.
Depending on your facility, there are mirrors that can be placed to allow you to “see” the surroundings and not actually have a view of the MRI tube. It enables patients to have the “illusion” that they can see the outside – either images displayed on the ceiling, or the room where the technician is sitting. This has been a lifesaver for her!
During the MRE, the technician will explain everything to the patient through a speaker that you can hear in the machine. You will also be able to respond to the technician and they can always hear you. You will also be provided with an emergency panic button to press, should you need to come out of the machine for any reason.
During the MRE, the technician will advise when they are starting the contrast through your IV. You should not feel anything except a quick sensation of nausea that passes immediately. This doesn’t happen to everyone, but it’s common.
Rocio says for some patients, like herself, who have been unable to consume all the contrast or who have slow motility, sometimes an injection called Glucagon will be utilized. This improves the quality of the images, but it does cause side effects. You will be instructed to ease into resuming eating and avoid any high protein foods due to slow digestion.
At the conclusion of the exam, you will be instructed to hydrate and begin eating slowly. Much like post-colonoscopy, Rocio recommends light meals for a few hours.
Due to Rocio’s extreme nausea and vomiting, she typically does not tolerate the contrast after the exam and tends to get sick shortly after. This is NOT the norm, but she recommends having an emesis bag in your car. As a reminder, if you have taken a sedative, you will not be allowed to drive yourself.
Considerations regarding contrast
While the actual scan experience was more pleasant than I had anticipated, about 3 hours after getting home I started getting terrible stabbing pains in my abdomen and had to run to the bathroom multiple times. At one point my husband came upstairs to check on me because I had been in the bathroom for so long. I was not aware or told that the contrast could cause this type of response. When sharing this on Instagram and after talking with Rocio, I learned how common this is within our community, especially for those who are symptomatic.
An IBD mom whose daughter has Crohn’s shared helpful insight for those who are on special diets or have difficulty tolerating contrast drinks.
Kristen tells me for MRE’s her daughter mixes Miralax in a specific amount of water that the MRI tech recommends, if she had to guess 40-60 oz over an hour. She says this helps prevent stomach cramping and uptick in symptoms. Kristen says some patients on the Specific Carbohydrate Diet (SCD) also drink pineapple juice (Lakewood brand or another organic fresh pressed brand) with Miralax.
“I found through this experience with my daughter that there was not much knowledge about how what you put in your body in the way of contrast, may affect inflamed intestines. Large amounts of sugar alcohol in contrast causes my daughter terrible pains for hours afterwards. Everyone is obviously different, and this disease is unique to each person, but I did a lot of research and we have found that the combo of a biologic plus SCD diet has really helped my daughter maintain remission, for now anyway.”
Kristen’s daughter had bowel resection surgery to remove strictures in her terminal ileum 7 years ago when she was 13 years old. She’s added some food back, but she’s strict with eating only whole foods and great about taking her medication.
Tomorrow on Lights, Camera, Crohn’s hear input and helpful MRE advice from 80 IBD warriors along with how to cope with the mental health aspect of going into a test and not knowing how the results are going to impact your life. As I was working on this article, I found out from my IBD nurse that my MRE results were within normal limits and that there is no evidence of active inflammatory bowel disease. While I’m thrilled and grateful to receive this news, it’s always perplexing when you’re more symptomatic than normal and your labs and scans don’t reflect a reason why.
This post is sponsored by Corra. All thoughts and opinions shared are my own.
For as long as Elya Lane can remember she had signs and symptoms of a health condition. It wasn’t until college that she received her official diagnosis of Ehlers Danlos Syndrome and POTS. She says her poor health started to spiral with other comorbidities popping up, the worst of which was chronic UTIs that left her whole body in crippling, burning pain and weak from the antibiotics. Elya’s personal journey with chronic illness inspired her to create the Corra App. This week on Lights, Camera, Crohn’s we learn about how she made her dream a reality and how she hopes to improve peoples’ lives.
The breaking point
“I was constantly plagued with fears of antibiotic resistance, infection complications, or complications from long term antibiotic use. I got to the point where I was so sick that I wrote letters to my kids and my family in case something happened to me. I started tracking all our passwords and making videos for my husband on where our important files were, how different things were stored, all the kids’ data, etc. While I tried to face this potential outcome bravely, I was devastated imagining my kids growing up without a mom,” said Elya.
As she navigated these dark and daunting days, the despair caused her to think about how she could fight back and regain control of her health.
“I started to religiously track my health in journals before transferring to Excel spreadsheets. I was so frustrated by how exhausting and impossible it felt to crunch that much data, so I turned to searching for a symptom track and correlative software to help me. I downloaded and tried every single one I could find – but none met my needs. Some even gave me back faulty data which made me angry. That’s when I decided to create a solution myself,” she explained.
In 2020, after losing access to all her healthcare management tools, and with her health declining rapidly, she decided to create Corra.
The meaning of Corra
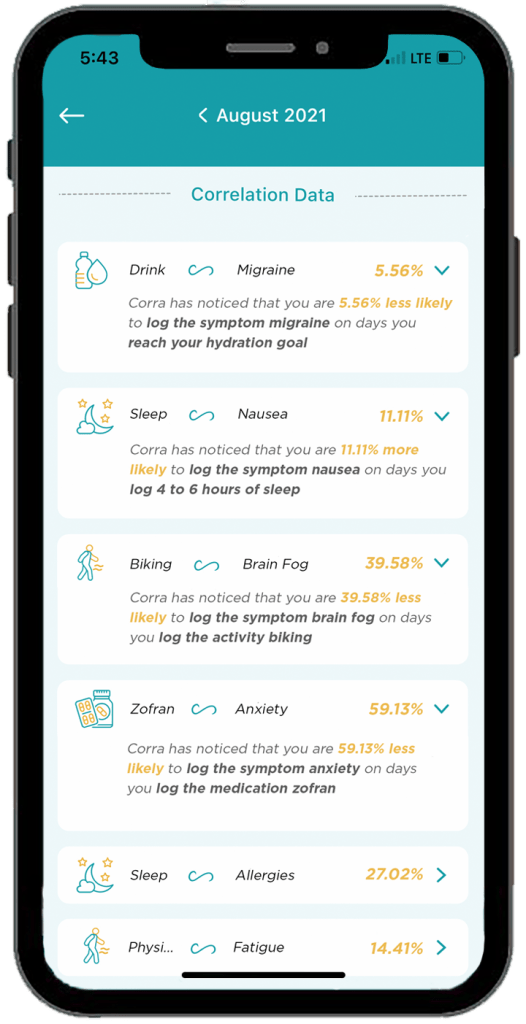
There are quite a few chronic illness apps on the market, some that even attempt to offer correlative insights. Corra is short for correlations. Elya wanted to identify correlations in her health so that she could find her triggers and optimize her lifestyle.
Here’s what sets Corra apart from other chronic illness apps on the market:
The algorithm was custom built by Corra’s chief data scientist, Simeon Wilson, who has a master’s in quantitative economics from UCLA. “We are not aware of any software that exists that compares to what Corra is currently offering with our correlative algorithm.”
Corra was designed by individuals with chronic illness. “Not just me! While the idea and original designs are all mine, we brought on more than 200 beta testers with various chronic illnesses to provide their feedback and help us tailor the app to the needs of the chronic illness community. Even now, we continue to rely on the insights and feedback from the community to enhance and adjust the app. I want Corra to always be designed by and created for our community.”
We correlate with nutrition in an accurate and helpful way. “I believe nutrition plays a massive role in our health so one of our key focuses with our algorithm was to be able to correlate seamlessly with nutrition inputs.”
Corra does not sell user’s data. “We don’t scrape your data from your device or browsing history, we don’t use your data to sell you anything, we don’t share your data with third parties. Your data is yours alone. As an individual with a chronic illness who often feels more like a commodity than a person, making sure people can receive personalized insights into their health without signing away their privacy is incredibly important to me.”
Corra’s bells and whistles to check out
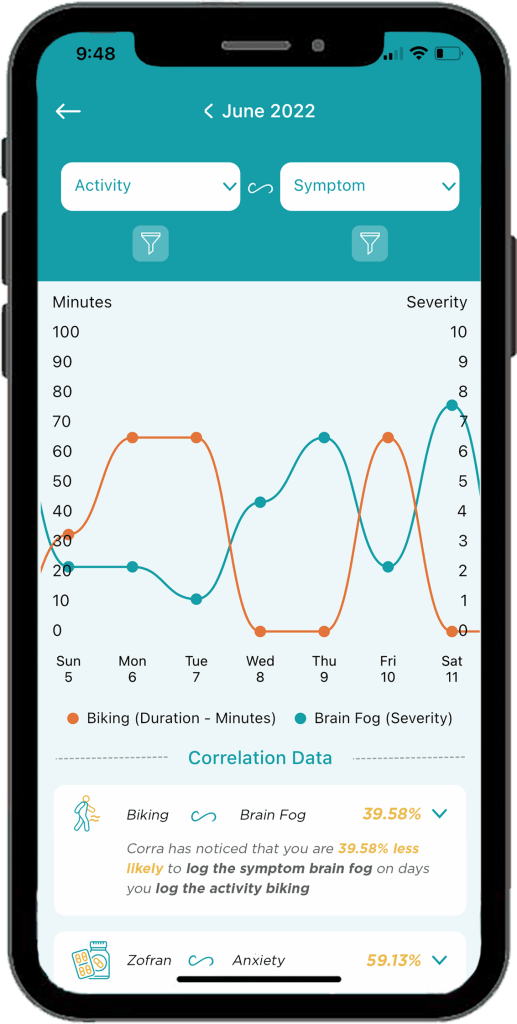
The ability to track health data in one place without having to use five different apps to log information. “My favorite part of Corra is of course the correlations, because getting detailed insights like that about my health is equivalent to having a team of data scientists run extensive tests on my health and provide me reports. It’s life changing to be able to learn about my health overtime and create a custom-built lifestyle that caters to my future.”
Discovering positive and negative correlations. “You may receive insight that something has x% chance of increasing or decreasing a symptom. I think being able to get data on the things that are helping is just as important as being able to identify triggers.”
The ability to log appointments, download PDFs of your data to share with my doctor, track medications and supplements, track mood and stress levels, etc. “I’m also extremely excited about all the upcoming integrations we have in the works! Soon we will be connected to Fitbit and Apple Health with Garmin, Cronometer, Weather data, and hopefully Oura coming shortly after! Over time we will continue to integrate with as many devices and apps as possible so users can have all their data in one location!”
A promising future
Elya says being able to learn what foods, activities, supplements, and medications help or cause symptoms has enabled her to have a much better understanding of how best to manage her health conditions.
“I’ve been told to go vegan, cut out red meat, don’t eat dairy, sugar, gluten, eat paleo, try a carnivore diet, go vegetarian, and try cutting out leafy greens… what I found with Corra is that I didn’t need to make these drastic nutrition changes, I only needed to cut out some foods in each of those categories. For example, I discovered that I have a high trigger correlation with ground beef. I can eat steak and other red meat, but not ground beef. Similarly, chicken thighs are a trigger for me, but chicken breast is not. Same with gluten, there are some gluten products that are triggering for me, but not all gluten triggers me. Being able to identify exactly which foods to cut out, rather than willy nilly cutting out entire food groups or going on drastic diet changes, has been an absolute game changer.”
Elya has also discovered that cold and flu medications like Mucinex are major triggers for her. This helped her realize why she would get a horrible flare a few days after coming down with a cold or flu.
“Now, I try to manage my colds and flus with other medicine to try to prevent the flare on top of the cold. It’s also important to note that I’m not cured! I have to manage my diet and my activities and my supplements every day. The difference is, I’m no longer throwing shots in the dark, I now have the information I need to manage my condition to the best of my ability.”
Information really is power, and it has given Elya control over her life and reduced her anxiety. Because of Corra, she is now coming up on two years without the need for daily antibiotics. It’s been over 2 years since she visited the emergency room.
“I’ve found that medical providers are far more willing to accept unbiased data from an algorithm than trust my verbal expression of my experience, so in that way Corra becomes my advocate and backs up my statements,” said Elya.
She says her health conditions have caused her to go through depression, isolation, and hopelessness. But her hope for Corra is two-fold.
“First, I believe it can help others identify their triggers and optimize their life so that their conditions can become more manageable, but I also hope that Corra can be a beacon of light for those struggling to see they are not alone. There are so many steps between the start of symptoms and any kind of treatment let alone cure (depending on if your condition is even curable)… and I want to be the one that goes into the trenches and helps people who are suffering the most. So many people in the chronic illness community get forgotten or left with “your test results are normal” when they know there is something wrong with them. I want to create a company that comes alongside them and lifts them up and allows them to have their voices heard.”
Downloading Corra
You can download Corra directly from the App store or the Android playstore. There is a free version as well as premium access. The premium version is $7.99/month or $24.99 if you enroll for a 6-month subscription. Elya is looking for Corra Insiders who are interested in getting free access to the app. By joining the Insiders group, you get a first look at upcoming features. This provides you the opportunity to share feedback on what you do/don’t like or would like to see improved or added in the future. Sign up for the Corra Insiders program here.
An IBD diagnosis is difficult at any age, but even more so when it’s a child who isn’t even two years old yet. Rachel Markovich’s son was diagnosed with VEO (Very Early Onset) IBD at 22 months old. His symptoms started when he was only 9 months. From the onset of his health taking a turn, she did everything in her power to make him feel well and get him the care he needed to get to the root of the problem. He’s now three years old and thriving despite his IBD. Rachel’s own personal struggles and experiences inspired her to create a nonprofit called VEO Guardians. Since her son’s diagnosis, Rachel has experienced difficulties firsthand—everything from insurance denials to the challenge of finding the right specialists, to reaching the right treatment plan.
Now that her son’s IBD is stable, Rachel is on a mission to help other families in similar situations by providing financial coverage, instead of waiting for insurance to approve or deny immediate care. Launched January 1, 2024, VEO Guardians aims to support and assist families with children who’ve been diagnosed with Crohn’s disease or ulcerative colitis, who are six and under. The main mission is to remove the struggle of the wait. We’ve all been there. Whether it’s waiting for approval of a biologic or a certain procedure or test or dealing with insurance denials, it’s a heartbreaking reality that’s far too common.
“We would like to provide financial assistance upfront for biologics and infusions. In addition, we hope to provide emotional support and disease guidance,” said Rachel.
VEO Guardian’s is gearing up for their first fundraiser, Light Up the Night, Friday April 5th in Montana. While there is an in-person event, anyone can participate virtually. Whether you are in person or online, you can join in the paddle raise, the live auction, or donate through the website.
“VEO Guardians is a 100% volunteer-based charity where all funds are placed in a checking account that directly goes to the children diagnosed with IBD to help with necessary medication treatment. This process takes place when the diagnosing pediatric GI specialist contacts the charity with the understanding that there will be a denial or delay from the insurance companies. The charity will begin assisting children 6 years and younger in Montana. As the funds grow, our non-profit will open to 18-year-olds and younger and then adults experiencing the same issues,” said Rachel.
From there, VEO Guardians plans to expand to neighboring states with the same model in place. Ultimately, the hope is to include services, such as mental health counseling for families and children.
Rachel wants caregivers to know they are not alone in this struggle and that there is help and support out there.
“This is bittersweet. When you’ve experienced a trauma like this; watching your child suffer, not being able to fix it immediately or not getting the answers is horrific. Coming together in support of each other and providing that listening ear or just knowing someone understands brings insight and guidance. It’s validating, encouraging and brings hope that we can all help each other,” she said.
Rachel is optimistic VEO Guardians will help ignite interest in supporting families with young children battling IBD.
“It begins with us coming together, finding our voices, and lobbying for changes to best support the children. Our vision is to create a world where all children have access to timely treatment and support. By helping to alleviate the burden of medical costs and allowing for timely treatment, we can help these young children with IBD thrive and live life to the fullest.”
It’s the first of its kind program dedicated to training dietitians about IBD-focused nutrition. Cedars Sinai Hospital in Los Angeles, California launched its IBD Dietitian Apprenticeship in July 2023.
Registered IBD dietitian Stacey Collins was the first registered dietitian to be selected, participate, and complete the program. I’ve been amazed at all she does for our community and been excited to dig deep and learn what her key takeaways have been from this experience. As someone whose lived with ulcerative colitis since 2012, when she was 21-year-old, Stacey has a unique perspective and approach.
This week on Lights, Camera, Crohn’s we’ll hear about her firsthand experience and why this Apprenticeship program is just what our community needs. The hope is that registered dietitians who participate in the program can take their knowledge from the experience and be able to plug themselves into an IBD Center to build and strengthen an IBD program.
Going up against lack of education and funding
Stacey tells me there is little to no education that they receive in dietitian training on how to do nutrition specific to gastroenterology, much-less IBD, and she says this Apprenticeship program fills the gaps and then some.
“So much of what I learned was through self-study before this program. But in the Apprenticeship, whether I was part of the team rounding on patients in the hospital, or seeing a newly diagnosed patient in clinic, or sitting on the floor with a 3-year-old patient asking about their Paw Patrol toys, I left every encounter feeling that special kind of discomfort and gratification that comes with growth and learning. This was truly a hands-on learning experience from many different sides of the IBD rubix cube, and I’m so grateful I wasn’t learning it all by reading slides from a PowerPoint and taking a test- who learns that way anyway?!”
Addressing the unmet needs
Once registered dietitians complete the Apprenticeship they can work in an academic center or a private practice that values IBD nutrition and has the financial backing to justify the need for a dietitian.
“There are institutions and people in places of power who are advocates for the profession of IBD RDs, and this work is simply impossible without them. IBD RDs have the potential to support patients throughout their journey as an accessible, consistent member of their multidisciplinary care team. Unfortunately, a lot of this potential is systemically handicapped by the lack of funds: RDs are investments rather than quick money-makers for a clinic without physician advocates and creativity, and we NEED people at institutions to see our value,” said Stacey.
The main programmatic goals are to provide a structured, supervised training program for dietitians to learn a model wherein dietitians work together with physicians and advanced practice providers for the care of adults and children with IBD.
Places do exist (and many are coming) that support this multidisciplinary model of healthcare delivery, but there’s such an unmet need, especially for people who don’t have access to these IBD centers. The hope is for this Apprenticeship program to fill the gaps of that unmet need by signaling to physician advocates at these institutions that a nutrition professional with intense training and experience DOES exist, ESPECIALLY for more complex patients who have IBD.
So much to be done for patients Registered IBD dietitians can assess people for malnutrition regardless of their stage of IBD, which is common even in remission and linked to poor health outcomes, along with so much more. Stacey says:
We can help catch micronutrient deficiencies or insufficiencies that many other care team members might miss, and we can correct and monitor them.
We can help patients experiencing food insecurity find ways to nourish themselves within their budget constraints with an eye toward prevention of other comorbidities.
We can help nutritionally prepare patients for surgery.
We can help patients in need of a medical or therapeutic diet intervention find a way to make it a sustainable intervention for themselves.
We can help patients nourish themselves using a whole-person approach, whether they are juggling multiple diagnoses, starting a new job, headed off to college, or too tired to eat: we have tools for helping patients feeling like they can handle it all
We can help prevent re-hospitalizations from small bowel obstructions or dehydration by giving patients IBD-specific tools for understanding their body.
We can save physicians time by inheriting questions about nutrition and/or supplementation regimens, and we can personalize these for each patient.
We can even show GI or IBD Fellows what it’s like to feel spoiled working with an IBD dietitian, and hopefully they’ll advocate to hire one of us wherever they make their final clinical stop
She’s confident IBD dietitians can make nutrition an accessible tool when it so often feels inaccessible with IBD!
Stacey’s top apprenticeship moments that left a lasting impression
Six months is a long time to pick up your life, move to another state temporarily, and fine tune your knowledge and expertise on nutrition and IBD. Here are the key takeaways Stacey says she took away from the experience:
1. Patience with patients is key; everyone is on their own timeline.
“I got to see a doctor celebrate with a patient who finally quit smoking cigarettes for good. After that encounter, he told me that he had been pleading with that patient for 20 years to stop, but he never blamed the patient for having a tough time stopping. He really was empathetic to the fact that they had a lot going on, and he knew they’d get around to it once life allowed. That was really enlightening to see: patients really are doing their best. How can I support them, especially if their timeline looks differently than the expectations that I have?”
2. It doesn’t have to be all-or-nothing; don’t let perfection be the enemy of good nutrition.
“One day I was with Erin Feldman, RD (Cedar’s Pediatric GI and IBD RD). She was listening to a worried mom talk about how she didn’t want her kid to eat sugary cereal, but that’s ALL they would eat for breakfast: it was the sugary cereal, or it was nothing at all. The child was exercising their choice autonomy and exploring what that looked like around mealtimes, and it was a challenge for the parents. Erin had a rapport established with the family, and I could see that they really trusted her. Plus, Erin is a mom, too, so she speaks the same first language as parents, and she really empathizes with the fact that many IBD parents are blamed for their child’s symptoms or disease. She truly met the parents right where they were at that moment.”
“Instead of focusing on the PERFECT breakfast with beautifully-balanced macronutrients and color that the child certainly would refuse, she said, “What if you just added PLAIN Cheerios and a couple of raspberries to their sugary cereal, that way they’re getting some antioxidants from the berries and a more diverse source of grains into their breakfast?” It was TOO easy, and the parents were like, “YES. We can do that.” and just like that: not a perfect solution, but a practical intervention that would work for where the child is right now.”
And that’s the power in having multiple touchpoints to a dietitian: next time they see the doctor again, they’ll see Erin, too, and they can make more adjustments for how life is being lived around food at that stage, too. So often people have the ambitious idea of going from zero to specific carbohydrate diet (SCD) all in one encounter, and the reality is that often multiple conversations and coordination of resources are needed, and meeting patients where they are looks different for everyone.
3. Nutrition interventions can be hard, and multidisciplinary support really is key.
“So often as dietitians, it’s easy to get stuck in the weeds of research and to get excited over interventions that have promising outcomes. This happened with a patient needing Exclusive Enteral Nutrition, but ~5-7 days into it, they were uncomfortable, and they really missed food. I was able to have a conversation with the patient alongside their doctor in the same room, who patiently reiterated our rationale behind the intervention and said, “not if it compromises your mental health. Let’s stop it if your brain is telling you we need to stop- we need to respect that. You should be proud that you tried this, and now you know!” And I could tell the patient was so relieved to have reassurance from their doctor that no matter what THEY chose for THEIR body they’d be supported by their doctor and by their dietitian. It really does take a team.”
4. GI Doctors REALLY do not get exposure to solid nutrition in their training
Kelly Issokson, MS, RD (Clinical Nutrition Coordinator, Course Director: DIET Executive program, Apprenticeship Director) arranged for Stacey to lead a learning session with the GI Fellows at Cedars, and in a room full of some of the smartest and most compassionate clinicians.
“They wanted to know all about the different nutrition interventions that we can recommend for patients. It felt like they had been rewarded for being the best of the best all by themselves their whole lives, and now they had an opportunity to learn more about how to collaborate effectively. They were all so enthusiastic.”
Stacey noticed after that session that the GI Fellows felt comfortable texting her while on rounds if she wasn’t there to ask if she’d stop by a patient’s room, or they’d text to ask about B12 supplementation after remembering to screen for a deficiency.
“They really understood the value that IBD RDs bring, and it’s not because I’m a great public speaker (I’m really not); it’s that they had this additional exposure to working with a dietitian with specialized training. This really made everything click for me: doctors don’t always know the right questions to ask patients about our nutrition needs, because most of them haven’t had the education OR the exposure to team members with the expertise to be truly helpful for patients. Working in silos keeps patients isolated, and I’m hopeful that the GI Fellows, when/if they leave Cedars become physician advocates to ensure that their patients have access to an IBD experienced RD.”
Plans for the future
When Stacey completed her Apprenticeship this winter, she did not envision returning full-time to her online private practice. She thought she’d start working at an academic institution, because the purpose of the program is for the dietitian to seamlessly integrate into a multidisciplinary GI care team.
“I am still holding out on hope that one day I could have both (but I’ll never give up my private practice- I love it so much). Truthfully, I’m thrilled to be back with such a passion for teaching patients how to implement some of the skills that I’ve learned into their own life, plugging it into their existing care teams, even if I’m on my own in private practice. I already helped patients through perioperative nutrition before this program, but now I’ve got some RICH resources to help make IBD surgery and nutrition really make sense for patients now in a much clearer way,” Stacey explained.
She’s able to take the research that they did from the perioperative IBD Nutrition program that exists at Cedars and put it into practice with her patients, and it’s a bit of a full-circle moment for her, having lived through IBD surgery with limited support.
“I’m a much better listener than I was before this program, a skill I learned from Kelly Issokson, MS, RD (Clinical Nutrition Coordinator, Course Director: DIET Executive program, Apprenticeship Director). Additionally, I’m more practical in my approaches and meeting patients where they really are, too, a skill I learned from Erin. I’m working on some ways to expand IBD RD accessibility, too. I’m a much more confident advocate on behalf of my patients now, too.”
Advice for the newly diagnosed
If you’re reading this and you or a loved one was recently diagnosed with IBD, ask your GI doctor to hire an IBD Dietitian. Stacey knows this doesn’t exist in most places, and as a patient, she understands how silly it is to constantly be burdening patients with requests. But the field of IBD Nutrition exists because enough patients asked, “What can I eat?” and enough doctors paid attention to it to be documented research. This is the next piece of the puzzle.
If your care team provides a registered dietitian who doesn’t specialize in IBD, that’s not going to cut it. Be assertive in asking your GI office to hire an IBD Dietitian, or invest in training their Dietitian, if they really want to help their patients.
Stacey advises patients and caregivers to stay off online forums. There’s so much food fear there, and life is bigger than that. Lastly, she advises reaching out for help. Even if Stacey may not be a good fit for you, she’s happy to provide patients with other RDs that she’d enthusiastically see, because an informed decision is a good one.
During her Apprenticeship, Stacey chose to do a research project to examine the effects of malnutrition and perioperative nutrition supplementation on surgical outcomes in people getting IBD surgery, whether that be for j-pouch, permanent ostomy, lysis of adhesions, or a resection.
“We had a small sample size (n=25). Regardless, we found that perioperative nutrition supplementation had a statistically significant impact on decreasing the length of stay, meaning that greater adherence to the nutrition supplementation protocol was associated with a shorter time spent in the hospital. Regardless of nutrition status (malnourished or not), everyone seemed to benefit from the nutrition supplementation protocol that we recommended for before and after surgery.”
Stacey is hopeful that more research with an even larger sample size will help inform these results so that this can be a resource more widely available for patients!
The future is bright
“If I dared to dream about what this could look like in the future, the closest possible model in existence is at UCLA under Dr. Niru Bonthala who is the Director for Women’s Health in IBD. Basically, I see the RD’s role evolving to cover every nutritional aspect of IBD with specialized knowledge to support patients in each life circumstance: from surgical prehabilitation to home nutrition support (TPN or EEN) and transitioning back to eating; to the overlap of eating disorders; to fertility and perimenopause; from anywhere along the spectrum of LGBTQIA+ care and/or transgender care; from peds transitioning to adult care, and even adults to aging adults; even athletics and/or eating disorders.”
There’s a rich opportunity within all these Venn-diagrams for a specialist interest and training to exist in IBD Nutrition, and this learning opportunity exists at Cedars.
“I’d also love to see the RD in an outpatient clinic even able to do community outreach: teaching basic cooking skills, procuring menu items for their medical diet (and beyond), and even showing patients and their families what this could look like by partnering with local food banks. Again, this is just me dreaming here in a world that I think should exist for people who have IBD and for RDs who are trained in IBD Nutrition,” said Stacey.
The current IBD Apprentice Yi Min Teo (@herbsandfood) came from both clinical and private practice backgrounds like Stacey. Yi Min will finish her training in July 2024. The program is supported by a grant from Leona M. and Harry B. Helmsley Charitable Trust.
In addition to dietitians wanting more IBD nutrition education, there’s also an Executive Program for MDs/DOs, APPS, and includes both virtual and in-person learning opportunities. You can apply here.
This blog post is sponsored by the Alliance for Access to Care. All thoughts and opinions are my own.
Going head-to-head with insurance companies goes hand in hand with managing chronic illness. The amount of time wasted, and energy exhausted over the course of a patient’s journey is incomprehensible. But the Alliance for Access to Care is looking to change that with the help of its latest campaign known as Healthcare Here. This coalition of healthcare associations has shared concerns about the way that insurance companies have adopted and implemented practices and policies that impede timely decisions related to treatment coverage at the expense of patient care. The burden of these practices, as we know all too well, not only falls on patients, but also on local hospitals that make up the backbone of community care that so many people rely on.
This week on Lights, Camera, Crohn’s we hear from Sr. Mary Haddad, RSM, President and Chief Executive Officer, Catholic Health Association, about the key issues and how she’s leading the charge.
The mission of Healthcare Here
Sr. Mary says the mission of the Catholic Health Association of the United States (CHA) is to advance Catholic health in caring for people and communities. Recently they also adopted a new vision statement that highlights why they are so passionate about health care reform: We Will Empower Bold Change to Elevate Human Flourishing.
“We are keenly aware that the United States’ health care system is in dire need of bold change, and this needed change is long overdue. Commercial insurance companies that profit from the delay and denial of health care stand in direct opposition to our mission of caring for people. How can a person flourish, or even survive, if their basic health care needs are not being met?”
As a faith-based organization, they believe that their ministry echoes that of Jesus Christ, who spent his time on earth providing compassion care for those in need.
“This cause is not only central to our mission and vision; it’s core to who we are,” she said.
Local hospitals in financial distress
When commercial insurance companies continually delay or deny coverage for care to those who need it, the cost of that care is passed to local hospitals. Not-for-profit hospitals have policies in place to ensure that those burdened by financial challenges receive either free or discounted care.
“As an example, on average, members of CHA provide free care to individuals and families who are under 200 percent of the federal poverty level guidelines. They also provide discounted care for those making up to 350 percent of the federal poverty level guidelines,” explained Sr. Mary.
The role of AI and medical decisions made by insurance companies
The CHA has seen several examples of commercial insurers utilizing automated systems to quickly process claims that may require greater scrutiny.
“For example, a recent ProPublica article found that Cigna spent an average of 1.2 seconds per individual case to deny more than 300,000 claims. They used an automated system to do this and, in doing so, saved millions of dollars for themselves. NaviHealth, which is a UnitedHealth Group subsidiary, is currently being investigated for trying to align rehab stays for Medicare Advantage patients to within 1% of days projected by an algorithm,” she said.
There are other examples, but the overall trend is telling enough. According to Change Healthcare, denial rates increased by 23 percent from 2016 to 2020. Meanwhile, profits from commercial insurance companies continue to rise.
A call to action for patients and caregivers
It can feel helpless as a patient, feeling as though your health and well-being is in the hands of your insurance company. I relate to this on many levels. Since my Crohn’s disease diagnosis in 2005, I’ve had to deal with everything from insurance telling me I’m too young for my annual colonoscopy to deciding the biologic injection I’ve been on since 2008 needs to switch to a biosimilar, not for medical reasons, but because of insurance coverage.
“We must advocate for change in the health care system, specifically as it relates to commercial insurers. On Healthcarehere.org, the CHA has pre-written a message that patients and advocates can send to their local, state and federal elected officials that gets the message across loud and clear: local hospitals are important and need to be protected,” said Sr. Mary.
Rural hospitals at risk
Not-for-profit hospitals are experiencing dire financial straits. More than 30 percent of the United States’ rural hospitals are at risk of closing. Per-patient hospital expenses have increased. At the same time, commercial insurance premiums are increasing at twice the rate as the annual rise in hospital prices.
“We’re approaching a point where a dam is going to break. And the ones left dealing with the shortfall of coverage will be patients and the local hospitals that they rely on for care. Ideally, all sectors of the healthcare system should be working together to deliver affordable, accessible, and high-quality care for patients. Through this campaign, we want the public and the policymakers they elect to understand how profit-driven actors are manipulating the health care system, which in turn is harming patients and the local hospitals that care for them,” she said.
Sr. Mary went on to say chronic illness patients need to know they are safe and welcome at their local hospitals.
“We want patients to understand that they have a voice which needs to be heard. Coupled with the advocacy efforts of the Alliance for Access to Care, patient testimonials are a powerful tool in standing up to the commercial insurance industry that would profit off their illnesses. Too many have been victimized by this broken system of care. The stories need to be told and change must happen now.”
If you have a story of denials to care through commercial insurers, send them to story@healthcarehere.org. We want policymakers to understand that this isn’t a battle between hospitals and insurers. This is an issue that affects real people. Your stories and experiences matter and deserve to be heard. Lives are at stake.
Kids are more intuitive than we tend to give them credit for. They are always watching us and even before they’re able to speak in sentences they have an innate sense of empathy and understanding. As an IBD mom of three, whose kids are almost 7, 5, and 2.5, I’ve started to think more lately about how to explain my Crohn’s disease to them in a way that will educate them, without scaring them. It can be a difficult balance.
I know my older two know mama gives herself shots, often needs to run to the bathroom, and gets “tummy aches” but I haven’t yet dropped the term “Crohn’s” or “disease” to them quite yet. It can be hard to explain and sometimes when I start trying to share more, I feel like it’s still going over their heads. Their concerned eyes when I’m in pain and how they watch me do my Humira injections is a reminder to me that they are aware something is going on. As we potty train my youngest, he commends himself for going on the potty by saying he’s “just like mama” …ah, what a great analogy!
This week on Lights, Camera, Crohn’s hear from several IBD parents about how they transparently communicate their experiences with Crohn’s disease and ulcerative colitis. It can be a fine line educating and being open, while also trying not to overwhelm and scare kids. I’ve found it extremely helpful tapping into the community and gaining input from others and I hope you do, too!
Helpful Guidelines for Navigating the conversation with your kids
Choose the right time. Pick a time when you won’t be interrupted and can focus on the conversation. Ensure it’s a moment when you and your children are feeling calm, at ease, and open to discussion. My recommendation as an IBD mom would be to have this conversation on a “feel good” day—rather than when you’re flaring or in the hospital.
Prepare yourself. Decide in advance how much detail you want to share based on your child’s age and maturity level. IBD is complicated, be ready for a range of emotions including sadness, fear, and even anger.
Use age-appropriate language. Explain your IBD in a way that is understandable to your child. Avoid using confusing or technical terms. For younger kids, it might be helpful to compare your illness to something they already understand.
Be honest but reassuring. You can be transparent and truthful, but also reassure them about all you do to manage and control your IBD. Empathize with the aspects of your daily life that won’t change, to provide them with a sense of stability and comfort.
Focus on practical impacts. Explain how your IBD might affect your daily routine or activities with them in a straightforward way. Use examples such as—“Mommy’s Crohn’s can be unpredictable, I may say we’re going to the park, but then I don’t feel well so we have a movie date and snuggle instead and plan to go to the park another day.”
Encourage questions. Allow your children to ask questions and express their feelings and know this will be an ongoing conversation throughout life. Go into the conversation without expectations. It’s ok to admit if you don’t have all the answers. You can explore some of the questions together.
Provide continuous support. Let your kids know that it’s okay to have and express their feelings about your IBD. Offer them ongoing support and reassurance. Let them know they can always come to you with questions or concerns at any time.
Seek support when needed. Consider enlisting the help of a therapist or a counselor, especially if you or your children are struggling to cope. Joining support groups and tapping into the online patient community and connecting with fellow IBD families in similar situations can be beneficial.
Keep the conversation going. Check in with your children regularly about your IBD and how you’re feeling. Be casual about it. Share when you see an opportunity to teach or calm fears that your kids may be internalizing.
Highlight the positives. While acknowledging the challenges, also focus on the positive aspects, such as the strength of your family unit or the support you have from friends and community. I always tell my kids when I’m doing my injection that mommy is strong, and we can all do hard things.
By approaching the conversation with honesty, sensitivity, and openness, you can help your children understand and cope with your chronic illness in a healthy way.
My 2-year-old trying to make me smile during a rough day in the bathroom.
IBD as a family disease
There’s a common saying in our community that IBD is a family disease, in that whether you have Crohn’s or ulcerative colitis or not, if someone in your nuclear family has it, the disease impacts your living experience in some way.
Emily and her husband have IBD and so do their three daughters, so discussions about IBD are frequent in their home since it’s a living reality for all five of them. She tells me the conversations tend to fall in one of the following categories:
1) Explanations of IBD details, procedures, surgeries, or diet needs for a member (or members) of the family.
2) Discussions to calm anxieties in one child about the presentation of IBD in themselves or in another family member.
She says the second category tends to be the more challenging conversations, by far.
“In the first category, we tend to stick to factual, age-appropriate explanations. For example, when our five-year-old needed to know about scopes and surgeries, we explained that a specific family member has “belly problems” and the doctor is helping by taking pictures of their belly and fixing the parts that were causing trouble,” explained Emily.
As the girls have gotten older, Emily says they add details about how the doctors do different procedures – always led by their child’s level of interest and desire for the knowledge.
“We are always honest about pain or discomfort related to medical procedures. Many things are NOT painful, and we want them to trust us that something does not hurt if we tell them. This has served us well. When surgery was needed for one daughter, we discussed how she would be sore afterwards, but we had ways to help the pain until it would subside. This was undoubtedly a challenging time for us, but our daughter did amazing,” Emily said.
As Emily’s girls have gotten older, as a preteen and teen, they understand more about their parents,’ and their own, IBD. They have lived through surgeries and many medical procedures in their family. Emily says now the more challenging conversations have started, related to knowing the possibilities around IBD.
“For example, I had a colon perforation following a routine monitoring scope for my IBD. It was a rare event that we are all warned about prior to a colonoscopy. It resulted in a more significant repair surgery and several days in the hospital. My daughters are old enough to realize that they also have scopes regularly and we had to have some discussions about the chance that the same thing could happen to them. It was challenging for our family for a few rounds of scopes!”
Emily says they addressed this topic mostly by focusing on the “helpers” as the iconic Mr. Rogers would! Yes, bad things can happen, but she reminded her daughters that they are so lucky to have doctors and medical professionals to “fix” these problems. She reminds them that they are lucky to have family and friends to help when they are not feeling well. She also talks about how they are lucky to have each other – who understand the ups and downs of this disease.
“This narrative has gotten our family through many challenges! I talk with my oldest daughter much more now about the details of her IBD. She is a teen and has had more than her fair share of IBD troubles. She has watched me deal with my challenges too. We are open with each other about the negative parts, and our frustrations having to deal with IBD. It is a double-edged sword to have her growing up! On the one hand – I hate that she is old enough to really understand the negatives. But she is also turning into an amazing young woman who is one of my closest confidants with this disease. We understand each other’s highs and lows like most cannot. We supported each other in challenging times and celebrate together for each win!”
Sari says she bought a couple of children’s books that feature a caregiver with chronic illness.
“One of them is titled ‘Some days’…it’s about a mom with multiple sclerosis, but it works for IBD, too. It goes over how some days are more exciting and others are simpler more restful days. If there are other kids’ books people have found, I’d love to hear about them!”
Kate also has a book by someone with Crohn’s, but says they’ve also always been very honest and open about it with her son.
“I always worried he would tell people too much, but I’ve found he’s incredibly respectful and it has made me feel less shame in my body because I talk to him so positively about it. Especially the perianal disease, which has been really hard to talk about with people. My son is six and understands my immune system attacks my digestive tract. We also have a puzzle of the body we have played with for years and he knows the colon, intestines, rectum, etc. because of that.”
Becca says one of her favorite memories as an IBD mom is when her daughter was learning body parts and said, “Mommy and I have vulvas, Daddy has a penis, Daddy and I have butts, and mommy has a bag!” She also often asks to see her “cut” on my belly (c-section scar), but I constantly remind her that she shares her “cut” with a lot of intestine.”
Becca also says for the longest time her daughter thought that EVERY mom gets an ostomy bag when they’ve had a baby.
“She didn’t realize I had mine for four years before she was born!”
As an IBD Dad, Brandon said he stumbled upon a video series when his son was around age five that provided a solid explanation. At the time his son had a broken arm.
“The video explained people have booboos you can’t see. I explained that I had what the girl in the video has. Nowadays, I show both my boys’ photos from my colonoscopies.”
You can watch the video Brandon showed his son here.
Here are additional books about chronic illness that others have recommended:
When you’re diagnosed with Crohn’s disease or ulcerative colitis it’s a lot to process. When I started this blog in 2016 and after living with Crohn’s for nearly 19 years, my focus has always been to be the voice I needed to hear upon diagnosis and what it was like to experience young adulthood with a chronic illness. As a 21-year-old, fresh out of college, I had to navigate my career, finding love, and becoming a mom with IBD on my own. The first decade I wasn’t publicly sharing my story and didn’t know there was a patient community to tap into online for support.
The first week I started experiencing Crohn’s symptoms-March 2005, Senior Spring Break in the Bahamas
Often as the years go by and we get beyond the initial shock of hearing the news and what this means for our lives, we tend to forget the challenges we faced to gain our footing. This week on Lights, Camera, Crohn’s I share some tokens of knowledge I’ve gained along the way that I hope will help you on your own journey, no matter where you find yourself at this moment.
Healing—physically, mentally, and emotionally is not linear. We all experience IBD uniquely—some people’s disease course is milder, others have it severe. We all cope differently with knowing and living with a chronic illness. Give yourself grace in the difficult moments. It’s ok to feel resentment or anger. It’s understandable to wonder at times “why me.” It’s “normal” to feel scared and anxious whether you’re a few weeks or a few decades in. Sometimes it’s taking things one hour at a time, other times it’s taking them one day at a time. Because of how quickly a flare up can strike, I try to live in the now and not worry about tomorrow.
You didn’t have control of getting your chronic illness, but you can control how you react and choose to heal from it. It’s easy to feel like you may be to blame if your health takes a turn for the worse. But understand this is not your fault. The unpredictability of IBD makes it feel like we’re often in the passenger seat and spiraling in circles, but this disease cannot control how you react, respond, and choose to heal from it. No matter what, you’re in control of the healing process. Whether it’s finding support through fellow patients and caregivers or through professional therapy, you won’t look back and you’ll be setting yourself up to take this on to the best of your ability.
There is no comparison game. Since the majority of people are diagnosed with IBD in their teens and into their 30s, it can be easy to try and measure your timeline and accomplishments to that of your peers who do not have chronic illness. It can also be tempting to look at people in the patient community who seem to have the world by the tail, when you’re struggling to get out of bed each day. This isn’t a competition of the sickest or a ploy to see who can smile through the pain and get more done. The only person you need to answer to, is who you see looking back in the mirror. You determine what you’re capable of and what you want in life. Your roadmap is yours and you’re right where you’re meant to be.
You set the benchmark for what’s possible. Your IBD is part of you, but it’s not your entire identity. Remember that even patient advocates are posting somewhat of a highlight reel. Even those who are working, in love, and parenting are dealing with their own struggles, too. My best advice would be to think about what you hope for in life (don’t even think of your IBD as part of the equation) and go after it. Yes, your health may cause some detours and roadblocks, but you won’t find your way unless you try.
No one knows your body better than you. I don’t care how many letters someone has after their name, they aren’t living in your body and experiencing what you feel each moment of every day. Be vocal when you need to be. Communicate as much as you can with your care team and paint the clearest picture of your reality. If you keep parts of your struggles to yourself or dumb down the severity of your day-to-day life, the only person you’re hurting is yourself. Learn about nutritional bloodwork and advocate for yourself to be tested for a full iron panel with Ferritin and Vitamin D. Get labs every 3-4 months so you can keep a finger on the pulse of what’s going on with your body. If you feel like your provider is being lackadaisical, don’t hesitate to get a second opinion. Take ownership of your health and find a provider who in your darkest moments you would feel most comfortable by your bedside in the hospital.
Make sure your GI specializes in IBD. There are gastroenterologists and there are gastroenterologists who specialize in Crohn’s and ulcerative colitis. Once you’re diagnosed with IBD, it’s imperative you try to find a GI who is an IBDologist. This can be tricky if you live in a rural area, it may mean you need to travel several hours to find a provider who fits the bill. If you move or are unsure of a good GI to check out, it’s helpful to reach out to your local Crohn’s and Colitis Foundation chapter and often they can help point you in the right direction.
Diet and stress levels matter. Read that again. Any doctor who tells you diet, and stress doesn’t impact your disease process is wrong. There are incredible registered dietitians throughout the US who specialize in IBD, and many of them have IBD themselves! Before you start restricting yourself or your child, make an appointment—most provide virtual options and this will help you get educated on what works best for you. What is a trigger for one person, isn’t necessarily a trigger for another. There isn’t a one-size-fits-all diet or else we would all do it.
Emotions will strike when you least expect them. Even almost 19 years in, I’ll sometimes break down and cry when I think about my Crohn’s or how it makes me feel. Just because you become a veteran patient doesn’t necessarily mean you fully ever heal from the hurt life with a chronic illness causes. It’s ok to have these moments where you may feel like you’re allowing your disease to control your emotions, you’re not. You’re human. It’s healthy to feel frustrated and to get emotional about what your life is like because you have IBD.
You’ve endured more than you give yourself credit for. As chronic illness patients we go through so much that often we don’t even bat an eye over experiences that would be extremely painful or stressful to the average person. Think about what a bad ass you are and how that carries over into each and everything you do in life. If you’re newly diagnosed you will get there—but even those initial weeks and months, you’re enduring more than the people who have their IBD under control and have a good handle on their body. No matter how many surgeries, scopes, scans, and IVs I’ve had, I always get a little teary eyed because it brings me back to 21-year-old me and then all the trauma that comes along with living with Crohn’s for 19 years. While those tears are sad, they also come from the strength of reflecting on what I’ve gone through to bring me to now.
Stay in tune with how your body is speaking to you through symptoms, do not ignore them. It can be challenging to communicate what you’re feeling to someone who does not have IBD. I get that. But by protecting loved ones, friends, and doctors from what you’re experiencing you’re preventing them from stepping in before it’s too late and before you know it your flare has gotten out of control and requires hospitalization. I used to be that person all the time. I would always internalize the pain, silently fighting through each day, doing anything possible to stay out of the hospital until the symptoms were simply unavoidable and required medical intervention. One hospitalization always sticks out in my mind. It was May 2009. I was a 25-year-old morning news anchor in Wisconsin. I was solo producing a 2-hour morning show dealing with horrible abdominal pain that kept making me throw up in the garbage can next to my desk in the newsroom as I struggled to put together the show. Finally, I couldn’t take it anymore and I had to call my co-anchor, who rushed me to the hospital. I was released from the ER hours later after my parents had driven from Chicago in the middle of the night only to return to the hospital that afternoon and have my dad carry me in his arms through the automatic doors. I was finally admitted and given the medical intervention I needed. Take it from me, you’re creating even more of an uphill climb for yourself if you don’t start speaking up when you initially notice something is awry.
The worst moments are just that, moments. When you hit your breaking point, when the pain seems overwhelming, and you can’t see the forest through the trees try to breathe. Go to your happy place. Recognize this is one day, one moment, I always tell myself “This too shall pass.” Go to your happy place mentally. Do mindfulness exercises. Shut out the outside world and focus on your breath. Detach from your body as best you can. Think of people who inspire you and bring you joy. Everything is fleeting. Each flare, each recovery, each prep, procedure, and surgery…it has a start and a finish. One day it will be a memory you talk about.
Pay attention to who is there when you when are quiet and when you’re going through the thick of it. IBD is too big to deal with alone. Lean on people you can trust, who you genuinely feel safe sharing your health woes with. This will be fewer people than you’d ever imagine. Be prepared to realize that many of the people you thought would be front and center to support you will be non-existent. It’s fine to mourn those friendships or relationships, but don’t waste your time or energy on them. Your disease will give you the ability to see who loves you and who wants to be present in not only the good times, but the bad. You can’t change people. Hold on tightly to the people who show up consistently, expecting nothing in return. Those are your people.
Emmanuel Acho shared a reel on Instagram recently that really hit home for me and caused me to reflect a bit on the people in my life and their roles. In the video he explains that friendship is like a house. You have your window, door, and floor friends. Window friends are outside looking in, they don’t know what’s going on in your house. They don’t have intimate access to what’s going on in your life. You can only let so many people into your house. Door friends come in and out of your life depending on the season. When life gets too hard or when your world turns cold, they might exit. Your friends might not be equipped for that season. Floor friends—aren’t going anywhere. You might track mud, but they will last regardless of the season. They are there to catch your tears and hear your fears. Remember—a house has more windows than it has doors and more doors than it does floors…if it has one good floor, you’re set.
Just because you need medication does not mean you’re taking the easy way out. I’ve been where you are. I remember lying helpless in a hospital bed and what it felt like to be told I needed to “break out the big guns” and start a biologic medication back in 2008 when there were only two options on the market for those with IBD. In that moment, we all naturally want to learn about side effects and what this could possibly mean for the long term. But please try and focus on the actual risk versus the benefit. As someone who has been on Humira since July 2008, I’m so grateful for my medication for allowing me to live a full life, bring babies into this world, and be a present, able-bodied, and active mom. It’s not all medicine, or all diet and lifestyle, often for many of us who have moderate to severe IBD we need a mix of both, and that’s ok. You can still thrive and be healthy, despite being on a medication with a black box label.
You are not a burden, and you deserve love. Any romantic partner who makes you feel less than, isn’t present when you need them most, or doesn’t show any empathy or interest in your daily reality isn’t going to stand the test of time. Use your IBD to your advantage to see your partner’s true colors. Be honest and upfront when you start dating and if you ever feel like you need to defend their actions or make excuses consider that a major red flag. Dating and marrying a person with a chronic illness isn’t for everyone, and that’s fine—but when it comes to people like you and me, we need a partner who is willing to take the challenge on beside us every step of the way. Find someone who you feel comfortable communicating openly with, who sees you for more than your disease.
IBD is not a battle to be “won” or “lost.” One of my pet peeves with any health condition or disease is when people say “so and so lost their battle”…they didn’t lose shit. Diseases are not a game. Oftentimes reaching remission is due to luck, disease severity, or surgery. I spent a decade of my life with active disease and have been in remission (thanks to surgery) for almost nine years. I don’t give myself credit for that, I’m not “winning.” It’s because of my efforts to stay diligent with my biologic, vitamins, safety labs, daily decisions, and check-ins with multiple specialists, but I also don’t think I’m at this point because of something special I’m doing compared to someone else. We’re all dealt a different hand of cards in life. Your IBD isn’t a win or lose situation—you’ll celebrate big victories and small ones, too, your disease can rob you at times, it’s a never-ending exchange and game of back and forth. You are not less than because you are flaring. You are not lazy for taking medication or failing because you struggle to follow a strict, regimented diet that may or may not help you. Once you stop thinking of everything as a “fight” it takes a bit of the stress, anger, and onus off your shoulders. IBD is a chronic illness, until there’s a cure, we’re in this situation until the day we die…that’s simply too long to be “fighting” anything.
Get ready to be extra proactive with your health. Due to the nature of our IBD and the medications many of us take, we are at greater risk for additional health problems. It’s important to get annual skin checks at the dermatologist. Make sure whether you have good vision or not that you’re seeing an eye doctor. Get cleanings at the dentist at least every six months. If you’re a female, make sure you get your well woman visits. We are greater risk for cervical cancer because many biologics don’t allow our bodies to fight off HPV, this may mean annual Pap smears. We’re also at an increased risk for breast cancer, so don’t delay your mammogram. Get a bone scan every 3-4 years, get one as close to diagnosis as you can so you have a baseline. Your GI may say it’s not necessary, it is. Steroids put us at risk for osteopenia and osteoporosis from an early age, this may mean you need to see a bone health doctor (yes, those exist). Those of us with IBD are at greater risk for pelvic pain, it can be helpful to see a Pelvic Floor Therapist who addresses those unique needs.
Faith can give you added strength and comfort. I understand faith is very individualized and looks different for each of us, but I can tell you as someone who is Greek Orthodox who has always been a faithful and prayerful person that I rely on my faith to guide me through my IBD each and every day. There’s a sense of comfort and hope that comes with believing God is watching over you through the good, the bad, and everywhere in between. When you’re diagnosed or flaring, it can test your faith. Hold on tightly to what you believe and lean on that (however it looks for you). I truly believe God gives his toughest lessons to his greatest teachers. One of my biggest fears as an IBD mom of 3 is that one of my children will get my disease one day. Each night before bed, I always pray with them and say, “keep my babies healthy, safe, and strong.”
My why. My motivation to push through each and every day.
Family planning takes time and effort. Just because you have IBD does not mean you can’t be a biological mom or dad one day. The journey will look a bit different, but this disease does not necessarily need to rob you of the experience if that’s what you want in your life. Communicate these desires with your GI so they can help prep your body for a baby. This can mean starting a prenatal vitamin and folic acid several months before trying. I had a colonoscopy before every pregnancy so that I could be given the ‘green light’ by my GI that we were cleared to try for a baby. When I was pregnant, my care was overseen by my OB, a maternal fetal medicine OB (high risk), and my GI. Unless you have perianal disease, you can have a vaginal birth, but oftentimes this is a discussion left to you and your care team. I personally chose to have 3 scheduled c-sections, because while I don’t have perianal Crohn’s, I didn’t want to risk tearing or causing a fistula to form. I would make the same choice if I had to do it all over again. I also stayed on my biologic through conception, pregnancy, and breastfeeding. These are all personal choices but there are many, many research studies available that show the safety and efficacy of doing so. If you feel you could have internal scarring due to past surgeries that could hinder your fertility, check in with a fertility specialist and have them help you investigate if there could be issues.
Educate yourself on insurance, prior authorizations, specialty pharmacies, and Pharmacy Benefit Managers (PBMS). Unfortunately, with IBD we are forced to do so much behind-the-scenes work to simply receive treatment and medication. You will waste countless hours and endless energy on the phone as these people give you the run around. Nobody ever seems to want to take ownership. Work with your gastroenterologist if you are denied a medication so they can write an appeal letter to insurance and go to bat for you. Stay on top of everything, don’t worry about annoying anybody. You gotta hustle. You gotta be frank and assertive. It’s not about hurting feelings; it’s about making sure people are doing their jobs and ensuring your course of treatment doesn’t get delayed because someone fumbles some paperwork. Our medications are time sensitive. Light a fire under people’s ass if you’re not getting responses you deserve. One of my friends on social media posted this over the weekend, “Managing specialty medications in January is an annual slap in the face to chronically ill people.” It sure is. This week will mark the first time I’ve ever received my injections late in the mail, due to a misstep in my GI office that I had to follow up on for over a week. Be extra proactive at the start of each year. Make sure your GI informs you about all the patient savings programs available, these can help you not only emotionally, but also financially.
You get the final say. No one but you gets to say what you do with your body. If a doctor wants you to do an enema before a scope and you don’t want to, don’t. If you don’t feel comfortable with taking a certain medication and your care provider keeps pushing it, they can’t physically make you pop a pill, take an injection, or receive an infusion. You must do your research, educate yourself every day, feel empowered by all you know and be ready to deal with the ramifications if you go against the grain or determine you want to try something differently. There’s not one “right” way to live with IBD. Be honest with your provider. Don’t say you’re taking a medication and then not take it, that’s not helping anyone or anything. Be a compliant patient, but an educated and empowered one at the same time. Measure all the risks and benefits and what your hopes and dreams are for your present life and for your future. Don’t ever feel like someone else can or should dictate what path your journey takes. Just because one biologic is a magic bullet for one person doesn’t mean it will be for you. You never fail treatments, they fail you. If a provider says “oh, you failed Remicade” … please correct them. “No, Remicade failed me.”
I write this as a 40-year-old mom of three—ages 6, 5, and 2.5 years old, married for almost 8 years, who has been on a biologic since 2008, who was diagnosed at age 21 in 2005. So much has changed for the better regarding the patient experience since that time. My perspective has come a long way. I used to be right where you are, so many are living your current reality. Instagram is the bread and butter for the patient community, that’s where you’ll find the most patients and caregivers transparently sharing. Follow the accounts, send a DM, comment on reels and posts, get engaged. Never hestitate to connect and reach out to me–natalieannhayden. Educate yourself through lived experiences and people who have paved the way for you, rather than Google. You don’t need to recreate the wheel, but this is your experience and your story. You get the final word on how you want each chapter to play out. Know each time you fall you will bounce back and that there’s a massive community of support here to catch you and cheer you on every step of the way as you rise once again.
It’s not surprising there’s stigma that surrounds gut health. Even though “everybody poops” it’s still a bit of a taboo topic, and don’t even get the general population to think about getting the dreaded colonoscopy. This is where the GH Foundation comes into play. Co-Founders, Dacia Heck and Kristin Lynn Grubehave both been personally impacted by gastro health in unique ways and their journeys inspired them to create a non-profit to help break down barriers and start critical, life-saving conversations.
According to the Crohn’s and Colitis Foundation, “patients with IBD appear to be at notably increased risk of colorectal cancer compared to the general population, with one recent study demonstrating a 7% colorectal cancer risk after 30 years of the disease. I had my first colonoscopy at age 21, which confirmed my Crohn’s disease diagnosis. Since 2005, I’ve had more scopes than I can count. I typically get a colonoscopy every year. While it’s not an enjoyable experience, it gives me peace of mind that I’m being proactive about my health. I’ll be getting my next scope in the coming months.
This week on Lights, Camera, Crohn’s we hear from Dacia and Kristin to learn more about their mission, the difference they hope to make, and how you can get involved and feel supported.
The personal connection
Until your gut starts causing health problems, chances are you don’t often think about it. Kristin was diagnosed at age 27 with Serrated Polyposis Syndrome (SPS), which is characterized by the occurrence of multiple polyps throughout the colon and/or rectum that can develop into colorectal cancer (CRC). She discovered this through a colonoscopy.
Kristin Lynn Grube, co-Founder of the GH Foundation
“My diagnosis has taught me to be my own relentless health advocate and speak up for myself. I continue to learn how to cope with SPS’s ongoing effects – emotionally, physically, and spiritually. Some days are easier than other days.”
Dacia lost her healthy, active sister from Stage IV colon cancer. Her sister was diagnosed at age 43 and passed away less than 4 months later.
Dacia Heck, co-founder of the GH Foundation.
“My sister’s diagnosis was a complete shock, as we didn’t have a family history of colorectal cancer and she was well below the screening age of 50 at the time of her diagnosis.”
The inspiration behind the GH Foundation
While Dacia and Kristin have different stories and experiences, they are both passionate about bringing important resources to the general public and are adamant about making gastrointestinal (GI) conversations not only more accessible, but also more mainstream, in order make the path to GI wellness and cancer prevention easier for others.
“We truly believe we can make a difference – one conversation at a time. As Kristin and I discussed where we wanted to focus our time and energy, we kept circling back to the “stigma” associated with GI diseases. That stigma often delays people talking to their family or medical provider about GI-related conditions. We decided the way we could make the biggest impact was to create GH Foundation and focus our mission on breaking that stigma,” said Dacia.
The GH Foundation’s main mission is to destigmatize conversations around GI, or gastro, health issues. 1 in 16 people in America will get CRC and 0 in 16 like talking about it. The GH Foundation encourages everyone to start the conversation. True prevention starts with educating the public on what is normal GI health and when to speak with a medical provider.
Discovering the loopholes in gastro health
As Dacia and Kristin did their research and spoke with different folks from all walks of life, they kept noticing that the conversations around gastro health have to start with a younger audience. Young adults in their late twenties to early forties are not discussing the importance of gastro health with their medical providers.
“We believe this is mostly due to the deeply rooted societal stigma surrounding gastro health. Given the uptick in early age onset (EAO) CRC, it may be too late to prevent a late-stage diagnosis once they qualify for screening. We want to focus on the very beginning and origin of it all – the conversation, whether it is with your family, friends, or network. Take that first step and reach out to someone, ask questions, make that list of symptoms you are experiencing, find out if you have a family history of GI diseases,” said Kristin.
While it’s intimidating, Dacia and Kristin guarantee that the first step will go a long way and may improve your quality of life, or even save your or someone else’s life.
“Our goal is to bridge the gap between the medical terminology and the general public’s knowledge about GI health. We are finding ways to make medical terminology and information accessible to the public. We encourage everyone to listen to their body, and to get the tools to empower them to speak up if they have issues,” said Dacia.
Taking their mission into action
The GH Foundation works to meet people where they are and find different ways to overcome the stigma. For some people, it’s learning about the basics of gastro health through an educational webinar, for others, it is hearing a survivor’s story and becoming inspired to take that first step.
“It’s connecting at a social gathering and finding a space where you can share your day-to-day challenges that you thought you were experiencing alone. Other times, we just want to have fun – we play GI trivia games and entertain each other with the Poo Squad mascots (more on that later in this interview). With all our events, we create an environment where it is safe to ask any questions. There is never TMI; we can talk about poop all day if you like,” said Kristin.
The Three Main Pillars of the GH Foundation’s Advocacy
Gastro Health
Inform and educate the public about the importance of GI health. So far, the GH Foundation has focused on the human GI anatomy, common myths and facts about GI health, ostomy facts, and CRC-related information. You can find out more about resources and past events on the GH Foundation website.
Proactive Advocacy
Proactively provide information and strategies to create positive shifts in how we communicate and influence others. Using what they’ve learn from other organizations, medical providers, patients, and cancer survivors, the GH Foundation has created educational content to then share with the public. Be on the lookout, you may just see their Mascots or Bristol Stool Charts popping up more and more near you!
Impact/Prevention
Educate and inspire people to take action to live a healthier life by fostering an open environment where no topic or question is off limits. Kristin and Dacia lead by example by first sharing something about themselves or asking someone at an event if they would like to share their experiences. They want to help people become as comfortable as possible about talking with their medical providers so they can get the most accurate information about their symptoms and find the best treatment for them.
Making a Difference
Since launching the GH Foundation, Kristin and Dacia have heard from many people that they scheduled their colonoscopy after attending one of their events or receiving one of their resources.
“People have also spoken with family members about their family history to get genetic testing and have said they felt more prepared about what to ask their medical provider at their next visit. People have approached us and expressed a sense of relief that we are creating an environment where they can ask any question, as uncomfortable or personal as it may be. Our mascots have received positive feedback as well. Seeing Sir Colon has taught them what the “colon” looks like,” said Dacia.
Through their initiative “GHF on Campus” they bring gastro health conversations to the forefront of young adult minds through a series of captivating events exclusively tailored to undergraduate students.
“One of our main approaches at the GH Foundation is targeting who we call the “pre-screening community”. Young adults under the age of 45 need to be made aware of common myths and facts on GI health, CRC signs and symptoms to keep watch, and what to ask if CRC symptoms emerge. GHF on Campus has a dual impact: Not only are they learning for themselves, but they can go back home and share what they have learned with family and friends. They can ask about their family history and encourage their family members to act, like scheduling a colonoscopy,” said Kristin.
So far, the GH Foundation has collaborated with the vibrant student communities at the University of Iowa and Northwestern University. Kristin and Dacia are looking to expand campus programming—if you’re reading this and would like to learn more, click here.
Finding humor through the message
You must meet people where they are. One of the ways they are doing that is with a sense of humor.
“We have designed our GHF mascots that bring some fun and lightness to topics that can be very overwhelming and serious,” said Kristin.
The GH Foundation’s mascot crew features: The Poo Squad (from left to right)—Ms. TP, Plungy, Mr. Poo and Sir Colon.
They will show up in different ways. One of the ways is our “Check your Colon” t-shirt with our very own Sir Colon. You can purchase a shirt here.
You can register now for a virtual webinar panel discussion entitled, “Destigmatizing Ostomy 101” taking place Tuesday, February 20th, 2023 at 6:30 pm CT. The discussion will feature Wound Ostomy RNs Jennifer Bart, MSN, RN, CWOCN, and Aimee Sheddan, BSN, RN, CWOCN.
Getting Involved with the GH Foundation
Talk – Initiate the conversation with your family, friends, and colleagues. Educate your loved ones about the risk of neglecting their gastro health. It may seem like a small step but can change the trajectory of life.
Volunteer – Help connect your community to life-saving resources about GI health.
Donate – Your donation directly funds our efforts to distribute educational materials and health guidance to the public.
Engage – Reach out to us! We welcome new ideas on how we can break the stigma.
Follow us on our socials so we continue to reach more and more people.
Connect with the GH Foundation on social media and follow the amazing work they’re doing: