This blog article is sponsored by Portal Instruments. All opinions and experiences shared are my own.
I’ll always remember how I felt the moment I was told I needed to go on a biologic drug to try and manage and control my Crohn’s disease. It was Fourth of July weekend 2008. My gastroenterologist walked into my hospital room and told me it was time to “break out the big guns,” meaning starting to get medication through an infusion or through a self-injection. I was a morning news anchor at the time in Wisconsin, three years into my patient journey. I knew without a doubt, for privacy reasons, and keeping my chronic health issue under the radar, that doing an injection in the comfort of my apartment was the best choice. As I watched the fireworks reflect off the hospital room window with my mom, tears flowed down my face. I didn’t know how on God’s green Earth I was ever going to be able to give myself an injection for the rest of my life.
I was never a huge fan of needles prior to my diagnosis. Once you have Inflammatory Bowel Disease, needles unfortunately are all part of it. While we may get desensitized, patients would give anything to be able to treat their disease without needles. When I started on my biologic, my mom and I went to my gastroenterologist office and a nurse told me I needed to do four, painful injections in my thighs because at the time I didn’t have enough fat on my stomach. I was shaking like a leaf. I had no idea what to expect, I was about to inflict pain on myself, the injector felt so foreign in my sweaty palms, and I was scared about not only how much it was going to hurt, but also the long-term side effects the medication could cause to my body.
I did the first injection and it felt like liquid fire burning through my skin. I couldn’t believe I had to sit there and do three more, back…to back…to back. The experience was traumatizing. When I finally did all four, my mom and I walked into the hallway and I embraced her, crying because of my reality, and knowing that in two weeks I would need to inject two more needles into my thighs for the final loading dose. Since July 2008, I’ve done a self-injection every other Monday and for a short time weekly, while I was flaring. That’s more than 2,600 shots.
Dreading “shot day”
The first few years I would absolutely dread my “shot day” and deal with the looming dread each week. Early on I would get emotional during the process and feel bad for myself. I was only 25 years old. It made me feel like I was a sickly person. My peers couldn’t relate. It was isolating and overwhelming. Every time I open my fridge, the box of injections is staring back at me as a constant reminder of what’s to come.
Doing my injections as an IBD mom
Fast forward to present day, I’m now a 38-year-old mom of three. Luckily, the formula for the medication was changed in 2018, making the drug virtually “pain-free”, but there are times I still feel the needle. Even though I have my medication process down to a science, I still wish I didn’t have to do it and I usually wait until Monday nights to do it. The timing is moreso out of habit, because when I was a morning news anchor there was no way I was going to deal with an injection at 2 a.m. I started a tradition of doing my injection while watching the Bachelor/Bachelorette, and that’s carried over now that I have three young children, often waiting until after their bedtimes. Each time after I’m done with my shot, I text my mom to let her know how it went. She’s a nurse and has been my greatest support with my IBD since the day I was diagnosed.
Sometimes my 5-year-old and 3-year-old watch me do my injection and each time they are intrigued. I’m sure my 11-month-old will be the same once he starts to gain an understanding of what I’m doing. It makes me sad that they often witness me doing my injection, but they are also my greatest motivation to be strong and smile through it. Watching me doing injections has made my kids incredibly brave at the pediatrician when it’s time for them to get their immunizations. Because I have little ones, I have to be mindful of disposing of my medication properly and keeping the Sharps disposal container out of harm’s way. We keep Sharps Containers up high in a cubby hole in our laundry room and I dispose of the injector pen immediately.
As an IBD mom, my greatest fear is passing along my Crohn’s to my children. While the risk is low, it’s there. I hope and pray my children won’t ever need to receive a biologic medication whether it’s through self-injection or infusion. For me, there’s no end in sight, I’m expected to be on my medication (if it remains therapeutic) for the rest of my life. Thinking of my babies having to deal with needles and being forced to inflict pain on them would be difficult for me and only add to the guilt.
The future holds so much promise when it comes to drug delivery without a needle. My hope is that in the years to come, other people won’t have to succumb to the same anxiety, pain, and worry I’ve had to deal with for more than a decade.
When something traumatic happens—like the mass shooting in Uvalde that left 19 children and two adults dead last week, the stress, sadness, and overwhelming grief can cause IBD to spiral out of control. You are not alone if the heavy nature of what’s happening in the world causes your mind to race and your GI symptoms to be amplified. As May (Maternal Mental Health month) comes to an end, a look at how we can best navigate these emotions and how our thoughts impact the gut-brain connection.
Looming threat of flares and violence
With the constant news cycle that bombards us, added into our reliance on social media, and seeing everyone’s opinions and posts, it’s the perfect storm for feeling suffocated by sadness. Life with IBD, whether you are in remission or not, is living with the looming thought of when your next flare or hospitalization is going to be. You know in your heart of hearts that it’s not a matter of if, but when your IBD is going to rear its ugly head. These days with violence happening left and right, it’s a challenge not to wonder and worry when you’re out in public if you’re going to be in the wrong place at the wrong time or if your children are in harm’s way.
The anxiety of worrying about the “what if” and the pain of grieving can often correlate to actual physical pain in our bodies that are already fighting an uphill battle. It’s difficult to try and make sense of what’s going on in the world. It’s impossible to try and wrap your brain around how people can be so evil. As a mom, I found myself crying putting each of my kids to sleep last week. Snuggling them a little longer. Worrying about their wellbeing and praying as hard as I could over them.
As a former news anchor and journalist, I vividly recall the moment the news of Sandy Hook broke. I was standing in the newsroom, about to head out to the studio to anchor the Midday show, when the heartbreaking news came over the newsfeed. It was incomprehensible then and it’s even worse now as a mom of three. I have only been able to watch the news in short snippets right now because I felt like the sadness of it all was consuming me in an unhealthy way. There’s a guilt that comes with trying to tune out the coverage and feeling like you’re not giving the reality of other peoples’ heartbreak the attention it deserves, while trying to protect your own mental state and heart.
Dr. Lindsay Hallett (Zimmerman), PsyD, is a clinical psychologist in Indiana. Here is her advice for coping:
Give yourself half the grace you give to others. This can make a significant difference in your overall well-being and stress level.
Reach out. If connection feels like what you truly need, enlist a friend or relative. The higher the level of personal connection, the better- seeing a friend is preferable to FaceTime, a phone call is preferable to texting, etc. But also, any connection is better than none.
Make time to move. Time is a premium to everyone and even 15 minutes will do. Listen to your body and give it what it needs – stretching, a walk, an intense workout, gardening… any kind of movement that respects your body’s own capabilities.
Give yourself permission to check out. If everything feels to be “too much,” avoidance can be healthy. Communicate healthy boundaries with others that you can’t talk about topic XYZ right now.
Seek therapy. Your emotional house doesn’t have to be “on fire” to benefit. Ask your primary care doctor, contact your insurance company, or research PsychologyToday.com to find a therapist. In-person with occasional virtual supplementation is best, but online therapy platforms can be helpful if you aren’t having luck otherwise.
Give yourself permission to unplug and stop doom scrolling. While there is no “right way” to cope with traumatic events like what happened in Uvalde and so many times before, give yourself permission to feel whatever complex emotions you are experiencing while also giving yourself space and time to take breaks and turns off screens. When you have IBD, being cognizant of what triggers you and recognizing how your symptoms speak to you, can allow you to stay one step ahead of the game in managing your illness. Focus on what’s tangible, what’s right in front of you, and what you are able to control.
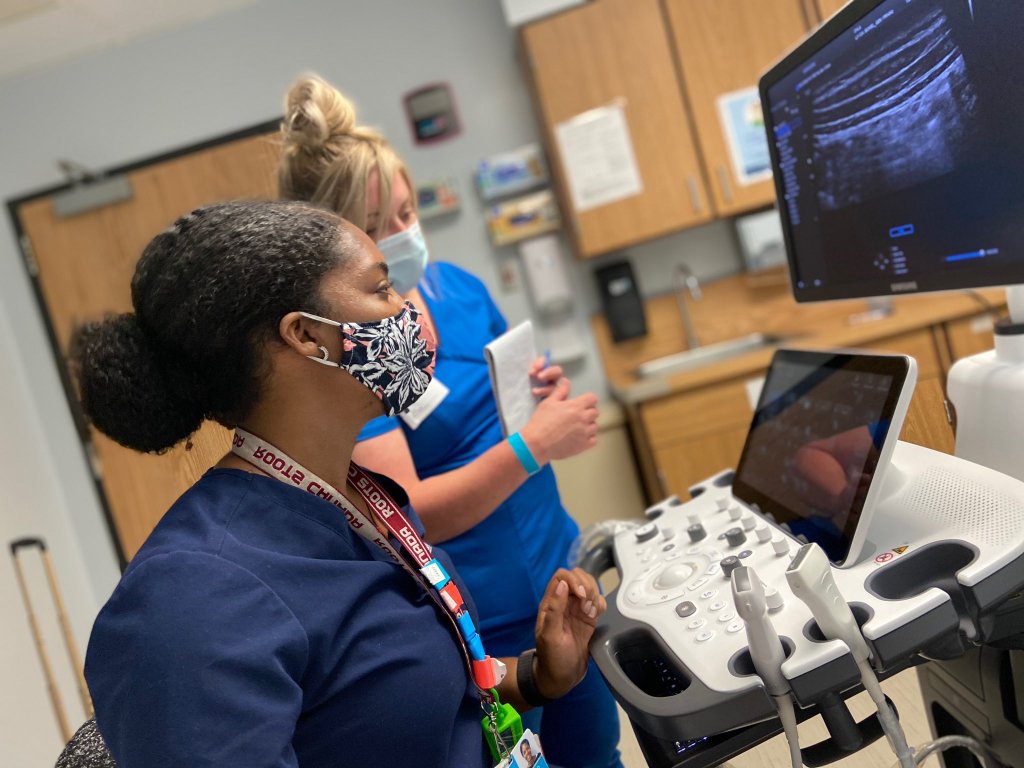
Innovation and changes in healthcare are propelled by patients and caregivers speaking up about improvements that can change the way IBD is treated and managed. This week on Lights, Camera, Crohn’s we hear from pediatric gastroenterologists Dr. Michael Dolinger, MD, MBA, Advanced Pediatric Inflammatory Bowel Disease Fellow, Ichan School of Medicine at Mount Sinai and Dr. Mallory Chavannes, MD, MHSc, FRCPC, Pediatric Gastroenterology, Hepatology and Nutrition, Children’s Hospital Los Angeles about the benefits of Intestinal Ultrasound (IUS) becoming a part of routine care, regardless of age.
The goal of IUS is to utilize a non-invasive method to monitor disease activity over time and it’s considered to be more precise than endoscopy in identifying both disease location and characterizing the severity of IBD. The IBD community—both patients and caregivers—can help fuel the adoption of IUS and gain access to receiving more information about their disease activity than ever before.
What is Intestinal Ultrasound (IUS)?
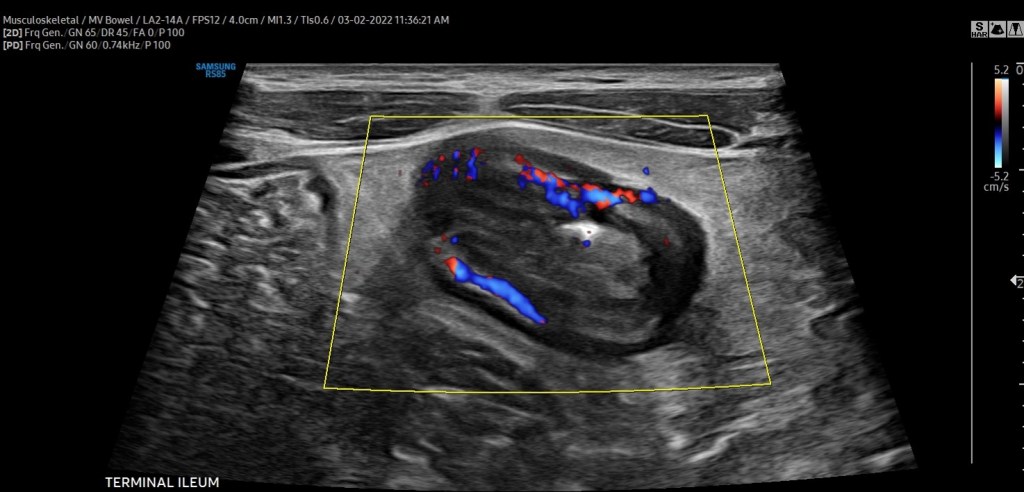
Intestinal Ultrasound (IUS) is an abdominal ultrasound performed during a routine clinic visit without preparation, fasting, or contrast to assess both the colon and the small intestine (terminal ileum most frequently) for the presence of disease activity. Probes are placed over the abdomen and the provider looks at images of the small and large bowel.
“The beauty is that, unlike procedures and other image modalities available to assess disease activity of inflammatory bowel disease, IUS can be performed without any preparation or fasting,” said Dr. Chavannes. “In the setting of active disease, patients can have a thickened appearance of the wall of the bowel (termed increased bowel wall thickness) in both the small intestine and the colon, which can be detected via ultrasound.”
In addition, by using color Doppler, a feature that assesses the velocity of blood flow within and around the bowel wall, gastroenterologists can demonstrate inflammatory activity in the bowel wall. IUS can also detect IBD complications, such as fistulas, abscesses, or strictures (narrowing) of the bowel.
“Our expectation is that, with effective therapies, the aforementioned features of disease activity should improve or even disappear over subsequent clinic visits. If they do not, we now have an objective tool available in the clinic that can assist clinical decisions, such as ordering further investigations or even optimizing or changing therapy. Improvement of bowel wall thickening or decrease in color Doppler signaling is a reassuring sign that treatment is working. Lack of improvement signifies that optimization or changes in therapy should be considered,” explained Dr. Chavannes.
“Intestinal ultrasound is precise, we monitor bowel wall thickness down to the 0.1 mm. We are now able to make informed decisions with patients together, assessing their disease objectively in real-time so we can be aligned with our treatment goals. This reduces misunderstanding and may lead to better treatment adherence and improved outcomes,” said Dr. Dolinger.
Why the delay in the United States?
While IUS isn’t the standard of care across the world, it is used in several Canadian IBD centers and in Europe (Germany, Italy, Norway, the Netherlands, and Australia to name a few). However, there are still many areas of Canada and countries in Europe where this is not used as part of routine IBD care.
“There have been several barriers to adoption in the USA, the biggest of which are reimbursement and the lack of training/expertise. However, that is changing, as there is a tremendous amount of interest from most major academic centers,” said Dr. Dolinger. “Through the International Bowel Ultrasound Group (IBUS) there is now a formal training, while intensive, that can be completed by anyone willing in the USA, which did not exist 5 years ago.”
IUS fits perfectly in the treat-to-target algorithm by adopting a monitoring strategy that helps to prevent flares and bowel damage.
“There is no other test for patients to see their disease dynamically with a gastroenterologist in real-time, which enhances shared understanding and informs decision making like never before. All of this will help break the barrier in the USA and around the rest of the world,” said. Dr. Dolinger.
A study conducted in 2016 explored why IUS is not standard of care in the United States. The
authors surveyed nearly 350 physicians, of which 40% were pediatric gastroenterologists. Although a minority of gastroenterologists were using ultrasound to assess and monitor IBD (either bedside or within the radiology department), over three-quarters expressed interest in using it more.
“The main limitation identified or perceived by gastroenterologists who responded to this survey was a concern for inter-observer variability, a lack of familiarity with ultrasound indications and techniques, and a lack of interest and access to pursuing additional specialized training. In addition, the survey identified a common message that I have received previously from some radiologists; that other modalities are more precise or effective in assessing IBD. All these reasons can hinder interest and implementation,” said Dr. Chavannes.
However, considering the multi-center effort in disseminating training, knowledge, and engagement that has been ongoing in the USA in recent years, Dr. Chavannes is hopeful that IUS will rapidly become the standard of care nationwide.
How Children’s Hospital in LA and Mount Sinai in New York Use the Technology
The Henry and Elaine Kaufman Intestinal Ultrasound Program at Mount Sinai is one of the first in the country to employ the training of gastroenterologists and regular use of intestinal ultrasound for both children and adults routinely in the IBD center for non-invasive disease activity monitoring.
“This would not be possible without the leadership of Dr. Marla Dubinsky, who has worked painstakingly hard to bring this to patients at Mount Sinai, overcoming every barrier to lead the way in the USA. We would like patients everywhere in the USA to be able to have tight control non-invasive monitoring with intestinal ultrasound and in turn, are working with International Bowel Ultrasound Group (IBUS) to host the first hands-on training in the USA at Mount Sinai in the fall. We have faculty from around the country signed up to learn and this will hopefully begin to fuel further adoption,” said Dr. Dolinger.
Intestinal Ultrasound was introduced at Children’s Hospital in LA in the summer of 2020. This was incredibly helpful during the pandemic when access to endoscopy time was difficult, considering cancellations due to active COVID infection and decreased daily procedures to allow for intensive cleaning protocols.
“We integrated using IUS for all patients coming to the pediatric IBD clinic. We have seen an immediate benefit in how we approach patient care and how timely clinical decisions can be made right at the time of the clinical encounter. One example is for patients presenting for a second opinion; these patients usually present with ongoing symptoms of varying degrees, yet incomplete or dated documentation of endoscopy, fecal calprotectin (a stool test helpful in indicating inflammation), and blood work,” said Dr. Chavannes.
During the visit, IUS gives an opportunity to understand the source of the symptoms experienced by patients and the degree of ongoing inflammation. Then, clinical decisions can be made that day, eliminating the need for additional testing. Dr. Chavannes says IUS even helps ease the discussions she has with parents and families.
“Many parents are stunned by the images they see and the changes over time. At the same time, they also notice when there is little difference from one appointment to the next, understanding the reason we are making the changes to the management plan that follows,” said Dr. Chavannes. “IUS has been invaluable for children under 6 years of age. This vulnerable population needs frequent objective reassessments, which is not possible otherwise. Using MR-Enterography would require general anesthesia, and access can be difficult. Similarly, for endoscopy, the prep can be poorly tolerated, and it also requires general anesthesia. IUS is non-invasive, painless, very well tolerated in young children, and available in real-time. Therefore, both parents and children are quite satisfied with their experience with IUS.”
Targeting treatment through IUS
Monitoring symptoms alone is not effective in reaching deep healing of disease in IBD, as many patients feel well despite having ongoing intestinal inflammation. IUS evaluates the inflammation that occurs within the thickness of the bowel wall (transmural inflammation).
“We often find that ultrasound is the only tool that shows continued inflammation when patients are in remission and labs have normalized. Optimizing therapies based on persistent inflammation seen on ultrasound may prevent us from falling into the trap of thinking our medications are working when our patients feel better and thus lead to better outcomes by not missing persistent inflammation that we have continued to miss with traditional monitoring strategies,” said Dr. Dolinger.
Although there are no fully established algorithms for the frequency of monitoring IBD using IUS, the best approach appears to have a baseline IUS at the time of IBD diagnosis or in the context of active symptoms or elevated inflammation markers on blood work (a flare).
“Then, the clinician can understand the features to follow over time. A repeat IUS can be performed at the end of induction treatment to assess how effective the management is. It would represent 6-8 weeks after the treatment was started. Provided that there is a marked improvement, the subsequent evaluations with IUS can be done every 3-6 months unless there are new concerns, with the closer timeline early in the disease course,” explained Dr. Chavannes.
In pediatric patients, this routine ends up matching most routine clinic visits. Therefore, as IUS becomes standard practice, and depending on how a patient is doing, their symptoms, and last assessed disease activity, patients can expect IUS as often as with each clinic visit. This modality would complement blood work and calprotectin stool tests in informing about disease activity and for complications of disease or flares.
What the future holds
Since a few IBD centers in the United States have already implemented regular IUS in their practice and have been disseminating knowledge about this technique, there is growing interest from pediatric providers to join the movement as well.
“Considering the challenges pediatric providers face in access to complementary imaging, operating room time, anesthesia exposure to endoscopy, and even the tolerance drinking contrast for radiology studies, IUS offers a fantastic way to assess disease activity in the pediatric IBD population. I am excited about the number of pediatric centers that have reached out about getting expertise in this field. The key is to promote buy-in from leaders in each institution to get the time and resources required for training and implementation,” said Dr. Chavannes.
Advice for patients and caregivers
It doesn’t hurt to bring up IUS at your next clinic appointment to gauge where your care team stands and if anything is in the works.
“If your provider is unaware of IUS and its benefit, it would be great to talk to them about the International Bowel Ultrasound Group. The curriculum for getting training involves three modules: an introductory module, a 4-week hands-on training at an expert center, and a concluding module and examination part of the European Crohn’s Colitis Congress,” said Dr. Chavannes.
She went on to say that hearing this request from patients may motivate administrators to provide the necessary time clinicians who are interested in getting expertise to implement the tool at their center would need.
Dr. Dolinger believes most major academic IBD centers in the United States will rely on IUS in the next 3-5 years.
“I would like to remind patients to be patient with their providers. Ensuring correct training and standardization is essential for adoption in the USA and this takes time and rigor to be done right and change the monitoring algorithm which has not been done in many years,” said Dr. Dolinger. “I began training in 2019 and it wasn’t until the second half of 2021 that we began using it very routinely for decision making, taking 2 years to become an expert. So, this will happen, but it will take some time.”
Patients and parents are big fans
The safety and efficacy of IUS can’t be matched. It’s also a big-time saver for everyone involved. A bedside ultrasound can be performed in a range of 20 minutes for the first thorough assessment, while an even more focused exam in a known patient can take less than 10 minutes.
“Both parents and children have been quite satisfied after their experience, as children can go back to school after the clinic despite undergoing this examination. Furthermore, the time saved in skipping additional appointments with the radiology department or procedures can be invaluable,” said Dr. Chavannes.
For parents, the imaging provides reassurance when there are improvements or when there are non-specific symptoms, yet the IUS is normal. IUS also bring validation when there are abnormal findings and helps to provide an explanation for why children are feeling a certain way.
“Children appreciate that it does not hurt and takes little time in addition to their clinic visits. In addition, they may not require additional appointments in radiology or endoscopy. Parents who had an opportunity of experiencing an ultrasound often request it afterward as part of their clinic visits. These families are more engaged and participate in shared decision-making. I am pleased and impressed at the engagement that actually “seeing” the disease together brings from families,” said Dr. Chavannes.
While the push is for IUS to be available to all IBD patients, both children and adults, it’s specifically beneficial for the management of pediatrics as it provides the unique opportunity to prevent bowel damage for a person’s entire life and reduce the need for invasive procedures, anesthesia, and sedation. IUS has the potential to alter scoping schedules in the future. While it will not replace the need for colon cancer screening or the assessment of mucosal and histologic healing, IUS can reduce the need for further follow-up scopes once those targets are achieved in between the need for cancer screening.
Whether you are a parent or not it’s heartbreaking to imagine how it would feel if you found out your child (no matter their age) was diagnosed with a chronic illness like inflammatory bowel disease. Of the more than six million people in the world diagnosed with Crohn’s and ulcerative colitis, approximately 25% of patients are diagnosed during childhood and adolescence, most of which are going through puberty. Impaired growth, pubertal delay, and low bone density are all common in children and teens with IBD. They can occur at diagnosis or at any time during a patient’s IBD journey.
As an IBD mom of three, who was not diagnosed until I was 21 years old, I personally don’t have the experience or perspective to share what it’s like to grow up with IBD or have a child diagnosed with it, so I tapped into several caregivers in our community, along with four leading pediatric gastroenterologists for input.
My hope is this article will serve as a helpful resource as you navigate the challenging waters of puberty with your loved one. Teen years are difficult enough without a chronic disease, taking a close look at how this impacts a young adult physically, emotionally, and mentally is something that deserves much more attention than a blog article.
Concerns from patients and caregivers
Before we get into the medical input, I want to share some of the messages I received this week from young patients and their caregivers so you can see firsthand how complicated this period of life is for everyone involved.
“I’m 14 years old. I was diagnosed with Crohn’s when I was 12, which marked an influential time in my life. It can be hard to cope with being diagnosed and having a chronic illness at that age. That year leading to my Bar Mitzvah, a cultural rights of passage from boyhood to manhood, was really challenging for me. At a time when changes are going on and puberty takes its course, learning to trust your body and that it is working is key. Rather than trusting my body, I had a lot trust issues. If my body could turn itself to work against me in my GI system, what’s to say it wouldn’t turn on me other ways? I am especially worried about my reproductive system. Since I was a little boy, I always knew I wanted to be a father when I grew up. Having kids and being a family man has always been my highest purpose in life. Since my Crohn’s diagnosis, I’ve felt anxious and worried about whether my Crohn’s or my body will stop me from fulfilling that dream.”
“I often worry about whether my son’s hormones will put him into a flare and wonder what the best way to approach the school about his Crohn’s is.”
“My biggest puberty concern is delayed growth or slowed growth and flares. I’ve heard a lot about puberty hormones really causing issues. Is there truth to this?”
“Will my almost 15-year-old son start puberty once his treatment kicks in or will he always look like a 12-year-old child?”
“My 15-year-old lost more than 15 pounds in the last year, we’ve checked all kinds of things, but can’t figure it out. He’s on renflexis (generic Remicade) and his colonoscopy came back clean. He gets full easily and deals with chronic constipation. I hope his IBD doesn’t stunt his growth.”
“The anxiety of managing IBD while combining that with the developmentally normal anxieties of the adolescent years can result in mental health issues that are hard to pinpoint. Body image issues that are normal as their bodies change, mixing with body image and food-related issues associated with IBD (good foods and bad foods, overly focusing on diet, etc.) which can lead into worrisome territory like disordered eating and worse. As children separate from their parents more with each passing year (which is normal), it becomes harder to monitor IBD symptoms and disease progression as a parent. As someone who has always been in the driver’s seat about IBD, this is a scary shift and I worry some symptoms will go unnoticed and become exacerbated.”
“That puberty will stop growth—growth has been severely impacted by Crohn’s before diagnosis and it did—hitting puberty early meant growth stopped and she only reached 4’9”/4’10”. Her periods also add to existing fatigue levels.”
“I worry about medication not working like it used to due to so much change in the body. I also worry about how she may feel about her image comparing herself to others at that age with so many scars or if she ever needs to have an ostomy bag. I worry her IBD will affect her cycles or make them more painful.”
“That my son will go into a flare requiring heavy intervention that goes far beyond our comfort zone, but we’ll feel trapped so he’s able to grow at the right time.”
“My 13-year-old son was diagnosed with Crohn’s a little over a year ago. He is doing ok now and on Humira bi-weekly. I’m mostly concerned about his growth, as he is small for his age. He has gained about 20 pounds in the last year, but he was malnourished as COVID made it difficult to get his diagnosis. Hoping he stays on track and continues growing and that his growth potential isn’t adversely affected by his IBD.”
“As a kid who went through being on high dose steroids while going through puberty, bless my mother!”
“Delayed puberty is a big thing. Also, how, and when is it appropriate to start transitioning responsibly for ultimate transfer of care. Mental health is often a concern for adolescents (anxiety/depression).”
“Flares. Many parents report puberty as being a challenging time for IBD. Imagine all the normal teen/puberty hormonal issues and then add IBD (and I say this as a lucky parent with our teens). I think every parent that makes it out alive should get a very long vacation. The #1 thing I hear from parents of kids with IBD is: “my heart breaks every single day”. Whether in remission or not, the disease is a persistent and heavy burden on patients and families. With all the noise, it’s important not to lose sight of this fact.”
“I was diagnosed with ulcerative colitis at age 13 and it all happened very quickly. I was in eighth grade – my body changed almost immediately after being put on prednisone. Being an early developer, puberty was a challenge for me. I didn’t look like most other girls in my grade. So when I started getting really bad acne and a swollen (moon) face from the meds, it was the icing on the cake. I remember ninth grade consisted of me coming home from school and crying to my mom because I felt what was happening to me was unfair. I’d have to excuse myself during classes to use the bathroom, so everyone knew what was happening. I was mortified. And although I was an “early bloomer”, I can’t help but wonder if I would have grown a bit more if I hadn’t been diagnosed, put on prednisone off and on for the first 3 years, or started on biologic treatment. There’s always the questions and mystery of what IBD has potentially taken away from me. But living with IBD also resulted in me growing up pretty quickly. I was able to navigate the healthcare system by the time I graduated from high school. I learned to talk about my body and my health – things that I don’t believe my peers could articulate by that time. So it came with some benefits – or at least things that I have been able to turn into positives. My experiences have made me a stronger person. And I’m thankful for that.”
Impaired Growth: Why it happens and what to watch out for
According to Dr. Sabina Ali, MD, Associate Clinical Professor, Director of IBD program, UCSF Benioff Children’s Hospitals, the most common extraintestinal manifestation of IBD in children is impaired growth, particularly in Crohn’s disease and that’s also what she hears from patients and their families when it comes to their greatest concern.
“Growth is a dynamic marker of overall health in children and adolescents, which occurs in 10-30% of cases. Short stature and failure to grow can precede IBD symptoms. It is important to monitor nutrition and growth closely and as this can lead to delayed puberty. Make sure the child is routinely getting height, weight and BMI measured. Growth impairment is more common in males than females with Crohn’s disease. It’s important to get disease in remission.”
Dr. Ali went on to explain that growth issues are more frequently seen in children who have never been in remission or for those who have dealt with flare ups in the pre-pubertal period.
“Pubertal delay may potentially decrease bone mineralization and affect quality of life in children who realize that their sexual maturation is different from their peers.”
Dr. Jonathan D. Moses,Assistant Professor of Pediatrics, Director, Pediatric Inflammatory Bowel Disease Program, UH Rainbow Babies and Children’s Hospital, agrees that remission is essential as a first step to ensure normal bone growth and pubertal development. Most of the time the concerns we hear about puberty and IBD is at the initial diagnosis when parents will note that young women have not started their menstrual cycle yet at the expected age or young men have not started their “growth spurt” yet.
“Growth is a key element of children diagnosed prior to puberty. Our goal is to provide the therapy that will allow them to be in continuous remission and achieve their final adult height and avoid any pubertal delays. If there are any concerns with this, we typically place a referral to the pediatric endocrinologist to help co-manage this.”
According to this University of California San Francisco study, boys are three times more likely than girls to deal with one of the conditions most devastating effects: the failure to grow normally. Researchers were surprised by this finding because the study also found girls had a more severe disease course than boys.
Dr. Ali says that a novel finding is that a high proportion of patients with ulcerative colitis exhibited continued growth, suggesting delayed skeletal maturation is also frequent in ulcerative colitis, contrary to common assumptions. For patients exhibiting continued growth, median final adult height was greater in males with ulcerative colitis than males with Crohn’s disease but did not differ significantly in females with ulcerative colitis, compared with females with Crohn’s disease. This finding supports the growing body of literature that statural growth impairment is more common in males than females with Crohn’s disease.”
Dr. Hilary Michel, MD, Assistant Professor of Clinical Pediatrics, Nationwide Children’s Hospital, explains the importance of monitoring pediatric GI patients’ weight, height, and pubertal development over time. She says measuring weight and height and asking about pubertal development helps make sure each patient is tracking along their growth curves and developing at an appropriate rate.
“In addition to monitoring IBD symptoms and checking labs, stool tests, and scopes, monitoring growth and pubertal development is another way to make sure we are treating IBD inflammation completely. If a patient is not going through normal stages of puberty, or is going through puberty more slowly than expected, it’s a hint that we should check on their IBD disease control! And if their disease is in control, then we need to think of other causes for delayed puberty and get them in to see the right experts to help.”
Dr. Sandra Kim, MD, Associate Professor of Pediatrics, Director, Inflammatory Bowel Disease Center, UPMC Children’s Hospital of Pittsburgh, says along with monitoring growth and nutritional status, it’s important to keep a close eye on emotional state and quality of life.
“It’s important children understand their disease, and for families and the care team to understand where the child is not only medically, but psychologically and developmentally. As a pediatric gastroenterologist, who focuses on the care of children and teens living with IBD, I know I have a unique relationship and responsibility as I watch “my kids” grow up.”
Dr. Kim says, “We see growth impairment in children and teens with Crohn’s much more so than with ulcerative colitis, especially with extensive involvement of the small intestine. Active inflammation in the small intestine can impact an individual’s ability to absorb nutrients. IBD also impacts appetite and can lead to inadequate nutrition.”
According to Dr. Kim, studies have shown up to 80% of children (males>females) have some degree of both weight and growth impairment when their Crohn’s is not controlled. While studies do vary in the range affected, it’s clearly a significant issue.
Medication and the pubescent years
In general all pediatric gastroenterologists try to limit and shorten the exposure of steroids in children.
Dr. Ali says, “Recent inception cohort studies in pediatric IBD have highlighted baseline phenotyping of patients to predict the severity of their disease course and help identify who will benefit the most from early biologic treatment. Biologic therapies have improved outcomes in pediatric IBD, including achieving mucosal healing as well as improved growth and pubertal development.”
Prior to this, the goals of treatment in Crohn’s disease were focused on controlling symptoms, enhancing quality of life, minimizing complications to prevent surgery, and restoring growth in pediatric patients. Evidence has shown that mucosal healing is associated with sustained corticosteroid-free clinical remission, reduced hospitalization, and lower surgery rates. According to Dr. Ali, biologics are the most effective in inducing and maintaining mucosal healing in this patient population.
Dr. Moses explains how biologics are decided upon with young patients.
“The age of the patient, in the context of the biologic era, does not seem to play a significant role at our center. If a child, regardless of age, needs a biologic medication, then we will typically proceed with this after shared decision making with the family. As a rule, for all ages, we work very hard to limit steroid exposure, both by planning out their maintenance therapy right away or using exclusive enteral nutrition (EEN) to induce remission in our patient with Crohn’s disease.”
Dr. Michel says it’s important to get IBD under control quickly since the window to achieve the goal of remission is so small.
“Because of this, growth and pubertal delay can be reasons to start a biologic as first line treatment. If steroids are used, they should be short-term (induction therapy only) to prevent negative impacts on growth and bone health. These patients may also be great candidates for exclusive enteral nutrition to treat their IBD, as it can help heal inflammation and address malnutrition without the side effects of steroids. Involving an experienced dietitian is key!”
While research has shown that disease activity may fluctuate with hormonal shifts (like those that happen with puberty, pregnancy, and even menopause), Dr. Michel says she is not aware of any specific data to connect loss of response to therapy because of puberty.
Puberty gets delayed
For pediatric patients in whom remission has never been achieved or for those who have frequent relapses, puberty is often delayed.
“The endocrine-hormonal mechanisms responsible for pubertal delay associated with inflammatory disease are incompletely understood. It is thought to be due to effect by both nutrition and inflammation,” said Dr. Ali.
Delayed puberty or delayed linear growth can be presenting signs of IBD to help clinicians make the diagnosis.
“Once these pre-teens achieve remission, they will begin to progress through puberty again and have improvement in their bone density, if it was low at baseline,” says Dr. Moses.
Dr Michel says, “The best way to ensure normal growth, weight gain, and pubertal development is to make sure their mucosa is healed. It’s also important we address low weight or malnutrition. If we’ve confirmed that IBD inflammation is resolved (through labs, stool tests like calprotectin, and scopes), and that patients are getting the nutrition they need, and we’re still seeing delayed puberty or slow growth or weight gain, this may prompt a referral to an endocrinologist, adolescent medicine doctor, or gynecologist to look for other causes of these problems.”
By adequately treating IBD and achieving mucosal healing, kids have the best chance to grow and develop normally and have healthy bones.
“Inflammation affects hormones important in growth and pubertal development, and delayed pubertal development is closely tied with poor bone health,” explained Dr. Michel. “Active inflammation can also worsen malnutrition and lead to low weight, which can delay puberty. These variables are often closely related; for example, a patient with active IBD may not feel well enough to eat regularly and lose weight or be malnourished. Or they may eat well but not be able to absorb the nutrients from their food. Or they may lose nutrients through stool or vomiting. So, treating inflammation and treating malnutrition are KEY to optimizing outcomes for kids and teens with IBD.”
Causes for the delay in puberty and decreased bone density can be multifactorial.
“Things we consider include nutritional deficiencies (not absorbing enough and/or not getting enough into your body), and the impact of inflammation (though pro-inflammatory cytokines – the “chemicals” produced by activated white blood cells – on sex hormone production, as well as growth hormone),” said Dr. Kim. “Other factors that can specifically impact bone density – decreased physical activity which leads to decreased muscle mass.”
When determining a course of therapy, a child’s quality of life and the impact of active IBD must be taken into consideration.
Dr. Kim explains, “Steroids have a great deal of side effects: external appearance (“moon” facies), psychological (can exacerbate underlying anxiety and depression; can impact sleep), bone health (decrease bone density and increasing risk of fractures), impact on wound healing, increased risk if long term on the GI tract (i.e. perforation), increased blood sugar (hyperglycemia), high blood pressure.”
What’s the deal with birth control and IBD?
Each pediatric gastroenterologist featured in this piece says they have heard from both patients and parents about oral contraceptives aggravating IBD. Dr. Ali says oral contraceptives are consistently linked to an increased risk of IBD.
Dr. Michel says since menstruating is a normal part of development for female patients, active inflammation, low weight, and malnutrition, can all play a role in delaying the onset of it. If a patient is flaring, they might have irregular periods or stop getting their period for some time. Once the problem is addressed—inflammation controlled, normal weight achieved, and malnutrition treated, menses typically resumes. IBD symptoms can also be exacerbated during menses for some women.
When it comes to choosing to go on birth control, and what birth control to choose, Dr. Michel advises patients and parents to be clear about their goals and weigh the risks and benefits.
“Goals for starting birth control can include regulating heavy periods or bad cramps, preventing pregnancy, improving premenstrual symptoms (mood, headache, fatigue), or even managing acne. There are some data about birth control pills increasing the risk of developing IBD, but research is conflicting about whether they increase the risk of flare. I would encourage any patient who is interested in starting birth control to talk with her gastroenterologist about what options might be best for her. An adolescent medicine doctor or gynecologist can also be extremely helpful to have these conversations, weigh pros and cons, and help young women and their families make informed decisions.”
Dr. Kim is no stranger to hearing concerns about the impact of oral contraceptives. She says it’s tough to determine whether birth control specifically aggravates disease.
“Women who have increased diarrhea and cramping around their cycles may have improvement in these symptoms when on birth control. Currently, there is not enough data to suggest birth control directly leads to aggravation of underlying IBD. However, there are other issues to consider when a young woman chooses the type of birth control. There is increased risk of venous thromboembolism (increased risk of forming blood clots) in individuals with IBD. There also is an increased risk for clots associated with combination oral contraceptives whether a young woman has IBD or not. Therefore, a woman who has IBD and goes on oral contraceptives not only has a higher risk of forming significant blood clots, but with more significant consequences from this.”
Dr. Kim’s recommendation? Avoid oral contraceptives with an estrogen component, if possible. Depo-Provera is an alternative, but you need to be aware that it can impact bone density. She says IUDs are safe and highly effective
How best to support young patients
Support groups: Discuss concerns regarding how a patient is coping with the IBD team. A social worker or psychologist on the IBD team can be a great resource.
Psychosocial assessments
Care coordination
Supportive counseling
Connection to resources
“As a pediatric gastroenterologist, my contribution is to manage their therapy as best I can to achieve remission. After that, we rely on our multidisciplinary team to address the psychosocial aspect of the disease and how this affects them at this stage in life,” said Dr. Moses. “Finally, we encourage the families to get involved with the Crohn’s and Colitis Foundation and attend Camp Oasis, if possible, to meet other children their age who also have IBD. This builds up their social support network in a way that can be life changing for them.”
Dr. Michel says, “I try to normalize their feelings, and reassure them that with effective treatment and achieving remission, we are working toward them reaching their full potential. I also think it’s a great time to involve experts like psychologists and child life specialists to help work through these concerns. Parents will often also ask about future fertility (kids and teens usually aren’t thinking of this yet)! It’s always a huge relief for families to learn that we expect normal fertility for our young folks with IBD and that the best way to ensure this is to get good control of disease.”
She advises parents to acknowledge how challenging it can be to go through puberty with IBD.
“Any feelings they’re feeling – frustration, anger, sadness – are ok. Then, I would encourage parents and patients to share these emotional and physical struggles with their healthcare team. Many centers have fantastic psychologists, social workers, and child life specialists that can help young people understand their disease, explore their emotions, and develop healthy coping skills that will serve them now and into adulthood. There are also fantastic resources online through ImproveCareNow and the Crohn’s and Colitis Foundation,” said Dr. Michel.
Dr. Kim advises parents and patients not to be afraid to ask pediatric gastroenterologists and their healthcare team for help.
“I really believe it takes a collective effort to support our children and teens. We are living in an unprecedented time with the COVID 19 pandemic (which has led to social isolation and new stressors with school, peers, and family dynamics),” she said. “Seeking our behavioral health resources (psychology, psychiatry, counseling, social work) is NEVER a sign of weakness – quite the opposite. One thing I would love to see: elimination of any perceived stigma when addressing issues around mental health. It is so crucial to address stress, anxiety, and depression. Besides the obvious impact on quality of life, we know that anxiety and depression can negatively impact an individual’s IBD itself. For the parents out there, I tell them they must check their own guilt at the door. The parents did NOT do anything to cause their child to develop IBD. I always say that you can be mad at the disease but never at themselves.”
Connect with these physicians on Twitter:
Dr. Sabina Ali: @sabpeds
Dr. Hilary Michel: @hilarymichel
Dr. Jonathan Moses: @JonathanMoses77
Dr. Sandra Kim: @SCKimCHP
Let this piece serve as a conversation starter as you discuss your child’s health with their care team. Ask the questions. Get empowered by learning and educating yourself more. As chronic illness patients and parents, it’s a constant learning curve—with each setback and triumph we gain newfound understanding and perspective. Stay tuned for an upcoming article on Lights, Camera, Crohn’s with guidance regarding making the transition from pediatrics to adult doctors.
As she fears for her life each day and every night in her homeland of Ukraine, ElenaSotskova thinks back to when her body started going to war against ulcerative colitis. She was 21 years old. Now, as a 47-year-old IBD mom, she shares firsthand experience of what it’s like to live in absolute chaos and devastation while trying to manage a chronic illness like IBD. Every morning Elena and her family wake up at 6 a.m. to the sound of explosions and gunfire. Oftentimes the internet and electricity go in and out, with repair workers constantly having to restore power.
Before we get into the utter heartbreak and unthinkable sadness, here’s some background. This isn’t the first time Elena has had to run from her home to try and reach safety. Shortly after her ulcerative colitis diagnosis, she fled with her 3-month-old daughter to Kyiv from Crimea, to avoid an abusive husband. At the time, she had the equivalent of 25 U.S. dollars in her pocket. Prior to becoming a mom, Elena worked for one of the largest banks in Ukraine, so she was confident she’d be able to land back on her feet in no time and support herself and her daughter. The stress of the divorce and being forced to start anew exacerbated her IBD.
“My condition was worsened by constant diarrhea, bleeding, low hemoglobin, and as a result, constant fatigue. I tried not to pay attention to it as I needed to work and make money for myself and the baby. My ulcerative colitis limited what I could do and where I could go. I used to be unable to go for walks unless I know where the restrooms were. I always had spare clothes with me and wet wipes, in case I did not make it in time.”
Since then, Elena has managed her ulcerative colitis with Mesalamine, in large doses (6-8 grams per day).
“In Ukraine at that time there was no biological therapy, and even clinical studies of such therapy did not take place. All that was available to patients were hormones and mesalamine. In addition, in Ukraine there is no compulsory insurance medicine (until now), there are no state programs for the treatment of patients with ulcerative colitis and Crohn’s disease, so I and other patients must buy drugs with our own money. And they are, as you know, not cheap. Compared to the level of income in Ukraine, it is expensive.”
How love found its way
Elena says she was working to buy her medicine. It felt like a vicious, never-ending cycle. But Elena’s luck in the love department took an amazing turn.
“I was lucky, I met a wonderful man, named Leonid who has a son. Leonid later became my second husband. I immediately told him about my illness. He accepted me, my IBD, and my child. He wouldn’t turn away from me or be ashamed when I had an accident at an event or in a public place. He helped me and supported me. And as a result, I stopped being nervous about my ulcerative colitis. I stopped worrying, and after I became calmer, the disease slowly began to subside.”
Leonid also started to take care of all the costs associated with her IBD treatments. Elena credits him for reviving her medically and emotionally, allowing her to reach remission after chasing after it for years. She was able to travel comfortably away from home and see the world through a different lens.
Prior to the war with Russia, Elena had big plans for herself. She aspired to begin her MBA and travel to English-speaking countries.
When the explosions hit
“All plans collapsed at 4 a.m. on February 24, 2022. We woke up to the explosions, saw the message “The Russians are bombing Kyiv, the war has begun.” That was more than a month ago, but it seems like we’ve been living in this nightmare for ages.”
Elena’s daughter, Alina, had recently arrived in Poland to study, but she happened to be home in Ukraine with family when the war started. Prior to this happening her travel plans were to fly back on February 27th. Of course, that all changed.
“She was supposed to fly back to Warsaw on Sunday, but war broke out on Thursday. Immediately, air traffic over Ukraine stopped. And hell began. Kyiv was bombed from the very beginning, we sat in the bathroom during the air raid, went down to the basement or went to the shelter. We did not turn on the lights in the apartment and taped the windows with duct tape so that they would not be knocked out by the explosions. We walked the dog for 5-10 minutes, near the house, so that if the shelling started, we could quickly hide. We live in Kyiv on the 7th floor, and most of all I was afraid that a bomb would hit our house, and we would either be overwhelmed or burned in a fire.”
Elena says for days on end she sat with her husband and daughter in their apartment. Alina would constantly cry. They learned that evacuation trains were leaving Kyiv for western Ukraine. At this point, they decided to send Alina back to Poland.
Nights spent at the railway station
“The most terrible were the three days that Alina and I spent in the basement of the railway station in Kyiv. There is a curfew, you cannot go outside in the evening, in addition, it was dangerous to go outside, because they are constantly shelling. My daughter and I got to the train station and decided to wait here until she could take the train to safety. My husband and son stayed home with the dog.”
The trains to leave Ukraine were like something out of a horror movie. Instead of a train car fitting the usual four people, they were packed with 20-plus people. People were ready to stand for an entire day just to leave Kyiv.
“Alina could not get on the train that was going to Warsaw, and we stayed overnight at the station. At night, the air alarm did not cease, explosions were heard, we went to the shelter (basement) of the station, which for three days turned into a home for us. We tried to sleep on the floor, it was warm, but the main thing was that it was safe. Finally, on the second day, we managed to put Alina on the train to Lviv. She left, and I was standing on the platform crying and praying that the train on the way would not be shelled, and my daughter would reach Lviv intact.”
Elena had to stay alone at the train station for an additional night because of the curfew in Kyiv. She was afraid her IBD would start acting up from the overwhelming stress and worry and terrified she was going to be killed.
“My gut understood me, it “behaved quietly”, and did not give me cause for concern. During the 21 years of illness, I learned to negotiate with him. On the fourth day, when the curfew was lifted, I was finally able to return home, wash myself and clean myself up. And my daughter had already reached Poland and was safe. We thought that somehow, we could adapt to this situation. We had food, water, gas, electricity, and Internet. We thought that we could somehow live in Kyiv. But this turned out to be unrealistic, as soon as dusk came, the city was pierced by an air alarm, it turned on several times during the night.”
Deciding to leave Kyiv
Bombing began each morning between 3 and 4. Elena and her family stayed in their clothes and didn’t sleep. She would take her dog and lock herself in the bathroom while her husband and son were standing in the hallway where there were no windows.
“Then a cruise missile hit a television tower, close to our house. It was afternoon, her son had just gone out to the store for bread, and there was an explosion, a crash, a fire. People who were nearby were killed. My husband said that we needed to leave Kyiv, it was extremely dangerous.”
So that’s what they did. They left for Elena’s mother-in-law’s house who lives in a village outside of Kyiv. There are no military or infrastructure facilities there, so they are hopeful it will not be bombed. As you are reading this, Elena is still there.
“In the village it is calmer, the battles are 30-40 kilometers (20-30 miles) away, we constantly hear artillery shots, gunfire, explosions, and flying missiles. But there is no air raid alarm, which was so exhausting in Kyiv. It’s still impossible to sleep normally. We are afraid that we will be occupied, and we are not where there are active battles.”
Running out of IBD medicine
But, Elena now faces another major issue. She will run out of her IBD medication this week and there is no way to buy it or receive it. Since the war started, she’s heard from countless other patients in the same bind. Doctors have fled, there’s no place to safely receive treatment, and for those who are now refugees or without jobs, they struggle to afford their medications. Elena knew she had to do something.
“I began to write to the European Crohn’s and Colitis Association, manufacturers of drugs, everyone who I could, to find out how to help our patients. Poland and Estonia immediately responded. They understand if Ukraine does not resist, the war will go on, to Poland, and the Baltic countries may also suffer. Now we are in constant contact with our European colleagues and are waiting for humanitarian assistance from them. Packages from Greece are supposed to arrive any day now.”
While Elena’s ulcerative colitis is under control now, she’s been forced to reduce her daily medication dose by half to try and keep medication in her body for as long as she can. She’s starting to feel that reminiscent pain we all know too well when our intestines are making themselves known. The pain, bloating, and diarrhea have been more consistent for her, but she doesn’t feel she’s flaring yet.
“I’m very scared that if I go into a flare, there will be no one and no place to treat me. I am afraid that this war will drag on for a long time, and then it is impossible to predict the condition of either mine or our other Ukrainian patients.”
Her friend was able to find her mesalamine in Kyiv. She bought the medication, but it’s been a week now and the package has not arrived to Elena’s new address. Tomorrow (March 31), Elena’s husband will venture back to Kyiv to try and get Elena the medicine she relies on.
She tells me she no longer cries or has emotions and that every day feels like déjà vu. Sometimes she feels like a robot in an out of body experience. Elena says the Ukrainian people are steadfast, strong, and remain hopeful they will be victorious in the end.
Tomorrow on Lights, Camera, Crohn’s you’ll learn about Elena’s inspiring patient advocacy prior to the Russian invasion, how she co-founded an IBD organization to support the patient community, and how she’s working day and night right now to help the approximate 11,000 Ukrainians who live with IBD and are struggling to manage a disease while living through a war.
Ah, specialty pharmacies. Just hearing those two words probably makes you feel a certain way. I’ve been coordinating my Humira through mail-order shipments since July 2008. Nearly 14 years now. Since that time, I’ve dealt with several different pharmacies. Each job change or insurance shift has resulted in a specialty pharmacy update. Lucky for me, each transition has been seamless. Except for now. My husband’s company switched specialty pharmacy providers at the start of 2022. I went from using Alliance RX Walgreens to Accredo Express Scripts.
The first shipment went well, but my second month was a mess. I’ve ordered Humira monthly—163 times to be exact. This was the FIRST TIME I didn’t have my medication on time and had to do my injection late. This week on Lights, Camera, Crohn’s a look at the literal and proverbial headache countless chronic illness patients are forced to deal with month after month and my advice as a veteran Crohn’s patient for all specialty pharmacies moving forward.
Here’s how it all played out (This ordeal gave me a pounding headache)
I ordered my Humira over the phone like I always do, and I was told it would ship to me on Thursday, February 3 and arrive on my doorstep February 4. That day came and went. Radio silence. Crickets. No communication about a delay due to winter weather. Mind you, the roads were cleared, and the snow had stopped the day prior.
I called Express Scripts on Saturday, February 5th and spoke with 2 call representatives, or as they call themselves “patient care advocate representatives” …insert laugh. Both representatives were incredibly dismissive and told me conflicting information. The first told me the shipment went out FedEx on the 3rd…but that she didn’t have a tracking number. She insisted on giving me the number for FedEx so I could track down the shipment or go to a facility to pick it up. Um, no. I refused and told her she should be able to track it down for me and that this was not my responsibility. She told me I could talk with a pharmacist about my concerns about my temperature-controlled medication being out in the elements during the Midwest winter for five days.
She puts me on hold for 10-minute stretches, and finally after 3 times, I ask to speak to a manager. She tells me she has a manager on the line and that she’ll connect me through, but I end up on hold, again. Finally, she returns and tells me the supervisor can’t receive her call, so I tell her to just call me back directly.
While this is going on, I have another call going through on my husband’s phone in hopes of getting through to someone. That representative was even MORE dismissive. Did not apologize. Acted like I had an attitude and told me there was nothing she could do.
When the “Resolution Team Leader” called me back directly she informed me that shipments go through UPS, not FedEx. Wow. Good to know. Glad I didn’t waste more of my time trying to get through to a FedEx facility on a Saturday. She told me that unfortunately the soonest medication was able to be shipped to St. Louis through their Memphis UPS facility (I learned that’s where my Humira comes from) would be Monday, but most likely Tuesday (Feb. 8).
Here’s why this is so problematic
IBD patients and chronic illness “customers” of specialty pharmacies are on scheduled medications, in my case, a biologic. This isn’t something that you can just delay because ‘oh well, it’s sunny and 45 degrees, it will come in a few days’. Lucky for me, I’m in remission with my Crohn’s disease. What if I was flaring? What if this was a loading dose of the medication that I needed to receive? What if I was traveling and had planned to pack my injection with me? What if I had been off my medication to deliver a baby and needed to start it back up? What if I were pregnant and couldn’t chance missing a dose? There are so many complicated scenarios. This isn’t a pair of leggings I ordered off Amazon that can wait a few days. This is medication that controls a debilitating and unpredictable disease.
Here’s how Express Scripts and pharmacies can do better
Basic business etiquette with customers (aka your patients). Don’t belittle, diminish, or act like you could give two shits about the other person on the line. We are chronically ill people who are juggling a million balls in the air at once to function like the rest of society while managing our health. The last thing we want to do is waste our precious energy going back and forth on the phone and having to stress about getting the medication we depend on to function.
If there is inclement weather or a reason for medicine to be delayed, you should be sending text and email alerts. I was told by the Resolution Team Lead that I was only partially opted in for these—mind you, this was my second re-fill of medication with Express Scripts. The first time a patient sets up an order this should be discussed with a patient over the phone.
I’ve been receiving specialty pharmacy medication in the mail since 2008. This isn’t my first rodeo, but this is the first time I’ve ever had medication delayed. Mind you, I’ve lived in Minnesota, Wisconsin, Illinois, and Missouri this entire time and encountered snowstorms and blizzards each winter without delivery issues. The snow stopped here on a Thursday…but my medicine can’t come until a Tuesday through UPS? Mind-blowing.
Since I was not notified on this delay, I spent all day checking my front porch, anxiously awaiting the delivery so it wouldn’t sit out and freeze on my doorstep. If I wouldn’t have proactively followed up the day after my medication was to arrive, I would have had no way of knowing when my shipment was going to arrive or what happened.
The onus of this should not be on the patient. We’re paying THOUSANDS of dollars for medications. The burden of this should be on the specialty pharmacy who has the job of coordinating prescriptions and making sure they are shipped.
Talk with patient advocates from all disease areas to help you learn how to best communicate and coordinate care. This blog is free advice. If you want invaluable insight like this moving forward, be prepared to compensate patients to share their viewpoints that you wouldn’t otherwise have. Give us a seat at the table to inform you of the shortfalls and the wins so you know where the improvements can be made and where you are successful.
Be kind and understanding when doing these phone calls. Think about the patient who is person on the receiving end who is calling about medication with a laundry list of side effects. It adds salt into the wound when your experience coordinating medication shipments is so negative and unempathetic. We are not just numbers.
As patients our hands are tied. We must go through the specialty pharmacy allocated to us through our insurance. You have that going for you. Now you literally have one job… to do yours.
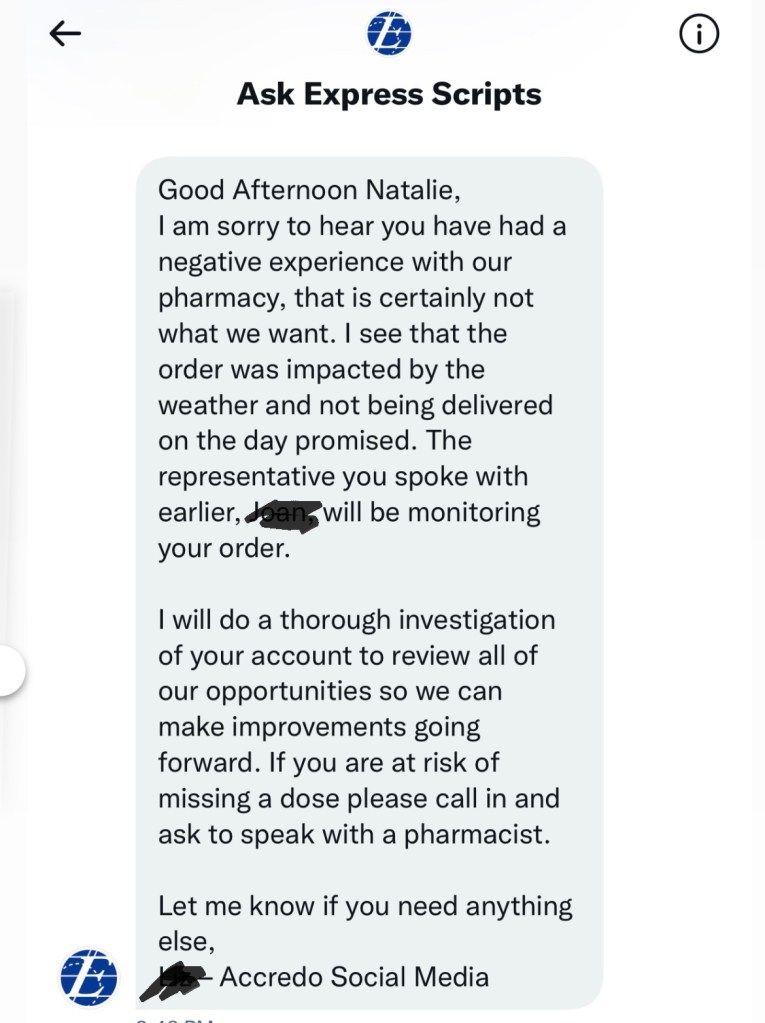
“Sincerely” want to help, yet never reached out as they claimed they would over tweets and direct message. That “empathy” is clearly all for show.
I tapped into the IBD community on Instagram and was blown away by the number of direct messages and comments from those who have struggled to get their critical medication through specialty pharmacies. This is unacceptable and eye-opening. Here are *some* of the stories.
“I will never use Express Scripts for my Humira, again. When I started it, I couldn’t walk or stand or do anything really because of my ankylosing spondylitis. They had the audacity to tell me I can expect my first shipment of medication in 1-2 months because there’s a lot of “processing involved.” They were acting like they were making the drug themselves. It had nothing to do with pre-certification. Everything was already processed and approved through insurance. Luckily, I was able to get my injections from a local specialty pharmacy the same day I called.”
“The number of issues I’ve had over the years with specialty pharmacies is ridiculous. My GI has an unlimited expiration/refills for my prescriptions, yet every year we must “renew” and it’s never at the start of the year. It’s always some random time when my shipment doesn’t go out as scheduled and the only reason, I find out is because I call and question the delay. They’re NEVER proactive. One of my most frustrating situations was a delayed delivery. It was supposed to arrive via UPS per tracking. The driver never showed. I called repeatedly and no one could tell me where the driver was. Eventually the next day I learned the driver left it in the truck and brought it back to the warehouse where I was told by the pharmacy to go and pick it up myself. Mind you it had already exceeded refrigeration time so there was no way it was safe for me to use. I then spent the next two days trying to get a new shipment processed.”
“From personal experience with Express Scripts and their specialty pharmacy Accredo, my Stelara is delayed every time. It’s gotten to the point that if they are going to make me late on it, I make them do same day delivery. They can make this happen if it’s not a holiday. Insist the medication gets delivered and don’t back down, demand for a private courier service.”
“I have to use CVS Specialty Pharmacy for Humira, they are absolute trash. I confirmed twice that my Humira would ship, and then it never arrived. I called and they took my insurance information, again, and told me it would take three days to process before I could re-order my medication. I waited and called again and then they told me my insurance had been denied. I was on the phone for six hours trying to figure out what was wrong. They finally re-shipped the medication only for it to be delayed by UPS and 8 injectable pens got too warm and had to be discarded…so I had to start again with another shipment! By the time I got the package, my dose was a week late.”
“I recently switched from my hospital’s special pharmacy to CVS Specialty Pharmacy due to my insurance changing and I didn’t get my Humira until 10 days after I was due for my injection. It was such a frustrating process and anxiety provoking.”
“Express Scripts issue with Humira. I spent 30 minutes trying to work out a $1,000 billing error on their part. After a half hour, they told me that they couldn’t fix billing issue the same day and that I would need to call back the following day and have the same conversation all over again.”
“Optium RX makes me cry at least once a year. Every year I try and beat the pre-authorization loopholes to get my medication on time and there’s always something new. Having to push my medication schedule is so defeating.”
“It’s a mess trying to work with a specialty pharmacy. I have never had a pleasant, easy experience with them. I’ve had four medications (IV and self-administered) sent to Accredo within Express Scripts over the last nine years. To this day, I have to spend at least an hour on the phone so they can run the co-pay assistance information…so for a bit, my co-pay was $2,000!”
“I have been on biologics for about a decade, and I think I could write a book about specialty pharmacy debacles. The latest being that as I was checking out on the phone, the rep commented on my insurance because it had my husband’s company (a popular brand). Thing is, he left the company 18 months ago and at that time I contact the pharmacy with my new insurance, went through the run around of changing insurance getting pre-authorizations, etc. They had been charging the old insurance the entire time. They attempted billing me $18,000 which I am still fighting. I’ve spent over 50 hours on the phone dealing with this and had many sleepless nights.”
“I went without my biologic for nine months because my insurance company through John Hopkins Hospital said I required prior authorization, when in fact I had prior authorization for the 277 refills that my prescription had. I had to advocate for myself to both my GI and primary care physician and they sent 378 pages of my medical records along with a 3-page email about my medication for it to be approved. To this day, I still have issues processing my orders.”
“At the end of the year, I received an email from Express Scripts that said Remicade would no longer be covered, and I would need to switch to the biosimilar, Inflectra. I called to confirm this, and no one could help me. I spent 8 hours over the next two weeks trying to determine if this was really the case. I had to call Blue Cross Blue Shield who then said I should speak to Express Scripts…who then transferred me to the Specialty Pharmacy, Accredo. I was then told by Accredo that I should talk to Blue Cross. It was the most frustrating thing. All I wanted to do was confirm if Remicade was not going to be covered and if it wasn’t what the cost of the biosimilar was going to be for me. Finally, a pharmacist assistant at the infusion center was able to help me.”
“My specialty pharmacy was late with my FIRST maintenance dose of Humira by 3 weeks. The pharmacy said they could only find the prior authorization for the loading doses and not the doses after. Then, my doctor sent me the copy of what they sent the first time, and my maintenance doses were clearly part of the prior auth. The pharmacy argued with me that my doctor didn’t fill it out correctly. They finally sent it, but accidentally sent it FedEx ground in July…and had to re-send it.”
“When I first switched to Humira, Express Scripts, said it wasn’t on their preferred list unless there was a good reason. I told the call rep I had gone into anaphylaxis. She said that I was going to need an actual reason or something serious. I told her I was going to need to speak with her manager because last I checked…not being able to breathe was serious.”
“My workplace changed insurance carriers and promised me that coverage would remain the same through Cigna and Caremark, with the specialty pharmacy being Accredo. Suddenly, I got a call that the Entyvio I take every 4 weeks is not covered at that frequency and also not covered at the Family Health Center where I’ve always received it. Naturally, I raised hell. Had to submit a new pre-certification which took almost 28 days to get approved, switched to a new private infusion center and abandoned my tried-and-true site, and spent more than 8 hours on the phone to do one simple thing: be able to receive the medicine I’ve taken for years. It’s unreal how insurance and specialty pharmacies just make decisions without considering the inconvenience and stress it puts on patients.”
“Specialty pharmacies are just an additional hurdle between a patient and their medicine. It’s like you’re playing a game of telephone and more players are added to the circle and increasing the odds of a miscommunication. When a problem arises you now have to make sure you smooth it out with health insurance, your doctor’s office, and your pharmacy. Oftentimes you don’t know where the problem arises in the first place because of all the finger pointing. I haven’t had a Remicade infusion since December 16th…even though I’m due every 4 weeks.”
“I had a specialty pharmacy send me my Stelara injections without ANY cold packs. Just in a cardboard box. I had not refilled it in 4 months because I was on Entyvio at the time so luckily, I wasn’t going to use it, but it was a mess. The company was so accusatory when I asked to return it until I told them there were no cold packs…shut them up real quick.”
“I called Accredo weeks ago to make sure my medication was going to arrive because my GI sent in a renewed script. I followed up daily the week I wanted to place the order, but they kept saying it was in processing and delayed. My prior authorization goes to 2024, my doctor did everything he could, yet Accredo still couldn’t tell me what the hold up was. I’m 33 weeks pregnant and I really don’t want to mess up the timing of my doses. Person after person says they have it handled, but it’s never the case. I feel like they just give the runaround to get you off the phone. It’s unbelievable how much time gets spent dealing with this. It feels like phone call roulette. It gives me serious anxiety every month.”
“When the new year started my specialty pharmacy would not accept my new Humira Savings Card. It took 10 phone calls and all parties, and it ended with an hour and a half call trying to get $5,000 reimbursed. The provider laughed when I asked then I had him call AbbVie and within 10 minutes the guy did a complete 180 and I was reimbursed. It’s scary to think what would happen if a patient didn’t fight back or speak up.”
“Your post about Express Scripts is triggering. My daughter, age 25, was diagnosed with UC at age 17. She is on our insurance a few more months. Express Scripts became our new online pharmacy a year ago. They’ve been horrific to deal with. She’s only on basic medications—mesalamine, Canasa suppositories and enemas. I dread the thought of what it might be like with them for more complex medications.”
…and there were SO many more messages that I received. Are you seeing a pattern here? This is ridiculous. It’s heartbreaking, frustrating, and sad. The incompetence and lack of care is comical. DO BETTER. I spoke with five different call reps/managers at Accredo and each time it was like I was calling for the first time. Take notes when you’re talking to patients/customers, so you don’t sound clueless on the other line and waste everyone’s time. You can at least pretend to care.
Advice for handling specialty pharmacy issues
Document, document, document! If you are having trouble with your specialty pharmacy, you should document each call and issue. Take note of the date, time, and describe what went down. Then, send a log of all the issues you’ve had to your employer and whoever oversees insurance so that they are aware. If HR gets enough complaints, they’ll look into a new pharmacy for employees.
Advocate for yourself and don’t back down. Be a thorn in their side. Tell them like it is and always ask to escalate the issue and speak to a manager. Get your GI involved and have them go to bat for you, too.
Check with your GI if you’re in a pinch. Oftentimes GI offices carry a couple of injections. You may be able to go and pick one up at the office if you need one. Always worth an ask if you’re in a tough position and don’t know when your medicine is going to arrive.
Contact the pharmaceutical company who makes your drug. One of my IBD friends manages a large practice in Boston. She advised me to contact the AbbVie Ambassador, which is a program available to patients for situations like this. They can overnight you a Humira pen to bridge the gap while companies like Express Scripts figure out their mess.
“The AbbVie ambassador program is a lifesaver for many of our patients when the specialty pharmacies fail! It is soooo frustrating. We see it all the time in our patients, and I’ve experienced it personally, too.”
Utilize social media. Having an issue with your specialty pharmacy? Head to social media (Twitter is best for this) and tag them publicly with your complaint.
Coordinating medication through specialty pharmacies is somewhat of an artform for chronic illness patients. Unless you deal with managing this monthly, you may be unaware of the endless time and energy that goes into making sure all the ducks are in a row to keep everything on schedule with your gastroenterologist, insurance, and pharmacy.
A few weeks back, I received a letter in the mail explaining that beginning January 1, 2022, my Humira would be handled through a different specialty pharmacy. As soon as I saw the letter my first gut reaction was that I was being switched to a biosimilar. Upon further reading, I learned that Alliance RX Walgreens, my specialty pharmacy, will now be Accredo (through Express Scripts).
Letter I received from my previous specialty pharmacy.
What now?
As a patient who has been on Humira since July 2008, this is the fifth time I have had to switch specialty pharmacies. Previously, it was because I switched employers and had different insurance. This time around my husband’s insurance switched specialty pharmacies. And even though this is far from my first rodeo—as a person who depends on a biologic every 2 weeks, I worry about a lapse in my medication, so I’m being proactive by communicating the change with my care team.
The letter stating the change said everything for my Humira would automatically be switched over, as long as there were refills remaining. I wasn’t sure if I had refills.
Communicating with your care team
With the New Year holiday being this past week, I went ahead and wrote my GI on the Patient Portal. Here’s the correspondence so you see how it all played out from the back end (no pun intended!)
Hi Dr. G and team,
Wanted to give you a heads up that I received a letter that beginning Jan. 1 my specialty pharmacy that I go through for my Humira prescription will switch from Alliance RX Walgreens to Accredo (Express Scripts).
The letter states that my prescription will transfer automatically as long as I had refills on file with Alliance. I just wanted to make sure that was the case and that there was nothing we needed to do on our end to ensure a smooth transfer.
My next Humira injection is Monday, Jan 10–so I’ll be scheduling a delivery next week.
Thanks!
Natalie
Good morning, Natalie,
I updated your chart (removed Alliance Rx and put in Accredo) as your specialty pharmacy. I did send in a new prescription for your Humira to Accredo this morning that way they would have it. It does look like your prior authorization previously expired. I have notified Lori so that she is aware that a new auth may be required. I did want to verify with you that your insurance coverage will remain the same going into the new year?
Thank you for the heads up, we always appreciate it.
Thanks SO much. Yes, my insurance coverage is the same (has not changed). Appreciate your follow up!
Natalie
You’re very welcome. That sounds great, I have notified Lori so that she is aware that your insurance will remain the same, that way she can work on that new prior auth if it’s needed.
Perfect, thanks so much! Do you know if Accredo will contact me next week to schedule delivery or if I contact them the first go-around?
Natalie,
I would suggest contacting them. Lori is aware that we will likely need a new prior auth but you contacting them to schedule delivery will also initiate that process (if needed).
Will do– that’s helpful to know. I’ll plan to call them on Monday to get the ball rolling. Thanks for all your help, have a Happy New Year!
When someone receives medication from a specialty pharmacy know they are on the phone coordinating delivery every month, making sure prior authorizations, insurance, and drug savings cards are all in check. It’s like a never-ending homework assignment that’s constantly looming. Many specialty pharmacies have apps to help “simplify” the process for patients, but I’ve found that the times I’ve tried to use apps in the past, I still receive a phone call about ordering my Humira and never know if my online order even went through. Call me “old school” but I still prefer to order my medication over the phone each month for the past 13-plus years. Find what works best for you and stick with it!
As you can see, it’s helpful to have a care team that responds promptly on the Patient Portal and helps you navigate the ins and outs of ordering your biologic. Rather than being unsure and worried about when and how I’ll receive my next Humira delivery, I now feel confident that it will be a seamless transition. I highly recommend grabbing the reins and checking so you don’t end up in a situation where you’re scrambling to get your medicine on time. Being proactive saves everyone involved a lot of headaches.
Overwhelmed. Terrified. Unsure. When Heather Hausenblas’ son, Tommy, was diagnosed with Crohn’s disease December 6, 2018 at age 16, she didn’t even know what IBD stood for. She knew she had a lot to learn and was on a mission to get her son healthy. Fast forward three years and now she’s a published author on the topic.
“Invisible Illness” chronicles how it feels from a parent’s perspective when your teenage child is diagnosed with a chronic illness for which there is no cure. The book provides an inside look at a mother struggling to find her way forward and how she turned despair into hope not only for herself, but for her entire family.
Heather Hausenblas, PhD, is a mother of three boys, health psychology expert, and award-winning researcher. She says when her eldest son was diagnosed with Crohn’s, her personal and professional roles collided. Not only was she going to battle for her child, but she also began her mission to help those with chronic illness eliminate the overwhelm and (re)discover health.
Dealing with the words chronic and incurable
“I kept hearing there was no cure, no known cause, no one treatment, and no one symptom. No. No. No. No. He will always have it. It’s never going away,” writes Hausenblas in her book.
Chronic and incurable-these two words were exploding in Heather’s mind on repeat. Tommy went from being on the high school baseball team, with lots of friends, doing well in school, and being very active…to living with a complicated and often debilitating disease. Everything in their life came to an abrupt halt. She explains how the illusion of youthful invincibility began to fade. Something anyone in our community can relate to. Health is often taken for granted until it is robbed away from you.
Feeling helpless through the struggles
She writes, “I could hear the pain in Tommy’s voice. But I was helpless. To put his excruciating pain in perspective, one Crohn’s patient described it as, “I’ve given birth without an epidural twice in my life, and the pain of Crohn’s disease was far worse than that.” “Tommy’s physical agony was accompanied by the unending frustration involved in trying to diagnose this complex disease. His symptoms and complaints had been overlooked—even dismissed.”
When a child or parent is diagnosed with IBD it impacts not only the person with Crohn’s or ulcerative colitis, but each family member in a unique way. It’s often said that IBD is a “family” disease.
“Torture was seeing my child wasting away to a skeleton, dropping nearly twenty pounds on his already lean frame, constantly running to the bathroom, and having excruciating pain. Torture was watching him leave the house only to run back seconds later for the bathroom while his friends went to the party.”
As a mom with Crohn’s myself, reading Heather’s perspective as the parent watching her son endure pain and hardships struck a chord with me because when you’re a young patient and are diagnosed before becoming a parent yourself, you often don’t take the time to think about how your disease and struggles are impacting the people who love you most. Not out of disregard, but simply because you are dealing with so much internally and externally it can be difficult to think outside of yourself.
Healing with food
While Heather shares a great deal of insight about the importance of diet and nutrition as it relates to IBD throughout the book, she also talks about the challenges Crohn’s presents since each person tolerates food differently. She explains how it’s impossible to find a one-size-fits-all diet but advises patients to journal everything from what they eat to how often they go to the bathroom to try and tailor a personal diet that works for you. Discovering your own triggers and knowing which foods are risky or tend to cause pain is a huge step in managing your illness.
“After a few weeks of strictly following the SCD (Specific Carbohydrate) diet, Tommy said that gluten wasn’t his issue. He somehow knew. He knew his body. He now eats gluten when he wants…Tommy’s liberalization of the SCD highlights the practical concern of adhering to a very restrictive diet.”
“Invisible Illness” includes 30 pages of helpful inflammation-fighting recipes. Throughout the book Heather talks about how she “detoxed and decluttered” her home and the cathartic effect journaling had on her coping process then and now.
Now, as a sophomore at Clemson University studying engineering, Tommy is in remission and does not take medication. He manages his Crohn’s by eating a healthy diet made up of organic, whole food, has an active lifestyle, and says his Crohn’s disease does not define who he is.
Forming connections and offering hope
Heather hopes that by candidly sharing her family’s journey with IBD that she opens the door for connections between other parents and families living the same reality. She recommends fellow parents to get involved with local organizations, so you recognize from the get-go that you are not alone.
Her main goal with publishing “Invisible Illness” was to “to help others navigate through the storm of medical and health information to figure out the right wellness path.”
How to purchase “Invisible Illness”
You can get your hands on a book by ordering a copy on Amazon.
‘Hello darkness, my old friend. I’ve come to talk with you again’. Ahh, the dreaded annual, routine, colonoscopy. I got a little spoiled because my last scope was July 2019. I decided to hold off in the thick of the pandemic out of safety concerns and did a fecal calprotectin test instead. Then, I got pregnant…so I had quite the enjoyable hiatus.
This time around, I decided to try SUTAB, a 24-pill prep + Magnesium citrate, rather than my typical Miralax-Dulcolax-Magnesium citrate. Without insurance and utilizing the patient savings card that’s online, SUTAB can be costly. I went here and printed out a coupon, I was able to get it from the CVS Pharmacy in Target for $50. While it’s more expensive than most preps, to me, it was worth the try.
Thoughts on doing a pill prep
So, this entire experience was a bit complicated for me. The night before my scope, I was miserable from the Magnesium citrate and the initial 12 pills. First off, I’ve come to learn that most GI’s do not make you take magnesium citrate on top of the typical prep. I’m just one of the lucky ones. Magnesium Citrate has always made me vomit, even if I take Zofran before. Prior to this prep, I always did the lemon flavor. I switched to the cherry flavor this time, GAME CHANGER. I had no problem getting it down…but it only stayed down for about an hour or so.
I threw up an unbelievable amount multiple times and never had a bowel movement. After not eating a solid meal for three days I was anxious and worried that I wouldn’t be cleaned out enough and that I was going through this hell for nothing. Sadly, Reid and Sophia witnessed it all go down and it broke my heart that they had to see me so sick and weak on the bathroom floor.
I relied on many members of the IBD community and medical professionals on social media to help guide me through the unknown. I took a Zofran and went to bed. I never woke to use the bathroom. I set my alarm for 3 a.m., took another Zofran, did NOT take the second 10 ounces of Magnesium citrate, and timed the remaining 12 pills every 3 minutes (rather than taking them back-to-back). I found that tip on Twitter and it made a huge difference! I decided not to take the second bottle of Magnesium citrate because in the medical instructions from the SUTAB box it says *not* to take any additional laxatives.
My scope was scheduled for 8:30 in the morning. I finished the pill prep at 4 a.m. and between then and 6:45 a.m. when we got on the road to hospital, I got completely cleaned out. I didn’t get nauseas, and everything fell into place. Now, I credit this with the fact I barely had anything in my body, which makes the prep much easier in my opinion.
If you would have asked me my thoughts on SUTAB vs. my typical go-to, Miralax + Dulcolax + Magnesium citrate the eve of the scope, I would have told you I would never do a pill prep, again. But once I took the Zofran, didn’t take the Magnesium citrate, and timed out the pills, only having to chase with pure water was amazing and very simple. All you have to do is drink 16 ounces of water with the 12 pills, and then an additional 32 ounces of water spaced out after. You can have more water if you want it.
My mom was laughing because she was watching me do multiple loads of laundry, make my son’s school lunch, pump milk for my 4-month-old, shower and get dressed…all on 4 hours of sleep, while in the middle of colonoscopy prep. As an IBD mom, I felt empowered in that moment of all I was capable of doing in the midst of what previously had been a nightmare.
Unfortunately, what is generally the “easy” part of the process—the hospital portion and the actual scope was very emotional and painful for me. My GI had ordered my usual routine labs to be drawn through my IV (to try and save me a trip) but I was so dehydrated from the prep and breastfeeding that the nurses could not get any blood. It took sticking me 8 different times. I felt like a human pin cushion. The IV was placed in a very tiny vein in my hand and the Propofol burned SO badly going in that I almost couldn’t handle it.
I kept asking for my husband Bobby to be allowed in recovery and felt like no one was listening to me. The nurse was gruff and kept poking me, even after I told her I would just go to a lab this week once I was hydrated. The blood pressure cuff even bruised my arm. I cried a lot of tears and the experience brought me back to a traumatic 2008 hospitalization for an abscess in my small intestine that involved 8 tries to get an IV.
My recommendation—do NOT allow labs to be drawn after you are done prepping for a scope. Save yourself the pain and the prodding. I overhead the nurses talking (outside the curtain) of my “room” saying they refuse to ever do this again to a patient and that we should all just go to labs to get bloodwork, rather than trying to get it done when we’re all terribly dehydrated. I had so many band-aids and gauze all over both my hands and arms, the nurses even sent me home with more gauze and band-aids in case I bled in the car. Fun times.
The best news
Luckily, the heaviness of this entire ordeal lifted a bit when my GI walked into the recovery room and said, “your small bowel and colon could not be more gorgeous. It was so pretty in there!” Best compliment you can give a gal with IBD!
She said even my anastomosis site (where my large and small intestine were reattached in 2015) …looked perfect. She explained how ulcers develop and indicate lack of blood flow. No ulcers, mucosal healing, and no biopsies needed. I feel incredibly fortunate that I have been lucky enough to hold onto my remission that came about because of my bowel resection surgery in August 2015.
I understand that “remission” is a complicated term in the IBD world. It doesn’t mean symptom-free, it doesn’t mean a cure…to me, it means I have many more days that I feel well than when I don’t. It means my Crohn’s disease doesn’t have to dictate or rule my life and that I’m able to be present for my family and for myself. It’s knowing that remission can go away in the blink of an eye. It’s happened to me before, and I know it will happen again. But for now, I’ll take a deep breath and enjoy this reprieve from the havoc I know my disease is capable of causing and continue to do all I can to stay well by staying on my biologic, keeping tabs on my lab work, and checking in with my GI whenever I feel like something may be starting to go awry. Remission is not something to be taken for granted. I often get asked what I do to “stay” in remission, I honestly don’t feel like I deserve much of the credit other than being a compliant patient and being very in-tune to how my body speaks to me through symptoms.
Moments that helped me get through
When my kids kept bringing me play food to help me feel better when they realized I couldn’t eat “real food” all week.
How my mom flew in from Chicago to help with the kids and to be an added support (like she does for every scope, procedure, and hospitalization).
When my husband, Bobby, came home late from work and rather than sitting at the kitchen table to eat, I caught him standing at the sink with his dinner plate and back turned so he wouldn’t be eating in front of me.
Knowing I was going to have a breakfast date with Bobby at our favorite spot and keeping my eye on the prize after going so many days without eating solid food.
Using my frozen breastmilk stash the day before and day-of the procedure to ease the burden of having to use energy and my body to feed Connor.
Reading all the comments on Instagram and hearing from friends and family near and far over text message and through phone calls really helped lift my spirits and conquer this as an exclusively breastfeeding mama.
Long story short—Aside from checking with your GI and getting a prescription for SUTAB, I would recommend trying the pill prep and from a patient perspective remind you to do the following:
Have your GI provide you with a prescription of Zofran (if you don’t have one already).
Take Zofran 30 minutes prior to taking the pills.
Set a timer on your phone and take one pill every three minutes.
While the pills are large, they are no bigger than a Prenatal vitamin and are doable.
For my self-imposed liquid diet this is how I plan it out for a Friday morning scope:
Last solid meal Monday evening
Tuesday-Wednesday full liquids
Thursday-Friday am clear liquids…and don’t forget my favorite tip of all…GUMMY BEARS! They are considered clear liquids, just steer clear from the red and purple ones.
Over the weekend (Saturday, November 6) I received my third dose of the Pfizer vaccine. When I had my second vaccine on August 11, I never dreamed I would be getting another jab so soon. But here we are. In talking with several IBDologists and patients I felt the need to expound on this topic, as misinformation is driving quite a bit of confusion about what additional doses and boosters mean for the IBD community and how we can best sort through all the information being thrown our way.
What’s the difference between an additional dose (3-part vaccine series) vs. a booster?
Dr. Meenakshi Bewtra, MD, MPH, PhD, Penn Medicine,helped me better understand this by explaining, “a 3rd dose implies that you had a less-than ok response to two doses and need a “3-dose regimen” to get the same response that someone else would get with two doses.”
The 3-dose regimen caters to those who are severely immunocompromised—those on chemotherapy and organ transplant recipients.
“Most IBD patients do NOT have this problem. Some small studies have shown varying responses; the largest is PREVENT-COVID which was over 3,000 patients. The study found that those on monotherapy TNF had similar response to the COVID vaccines as the general population. It was only in the setting of combination therapy (anti-TNF plus azathioprine or methotrexate) that you had a blunted antibody response (again–this was a research study),” said Dr. Bewtra.
She went on to say she has not been recommending that all her patients get a 3rd dose—rather, reserving that for patients who are on combination therapies. At the same time, this is a very fluid discussion, and the decision needs to be made on a case-by-case basis between each patient and their physician.
A booster is if you had an adequate response to the first 2 doses and are now 6 months past your primary series and fall into the recommended categories (over 65 years old or age 50+ with high-risk medical conditions), if you are part of a younger age group with high-risk medical conditions, or for those who work in occupations that put them at high risk for COVID. Booster shots are most effective 6 months after your initial series for Pfizer and Moderna and 2+ months after J&J, although the data really supports waiting until at least 6 months for best response. Age is the biggest determinant of needing a booster, whether you have IBD or not.
Dr. Peter Higgins, MD, PhD, M.Sc., University of Michigan Health, explained this clearly on Twitter. He tweeted, “It is a catch-up dose for folks who for various reasons (anti-TNF’s, steroids, chemo) will not have a great response to two doses. To catch-up to everyone else. Then a booster dose later to keep pace.”
I’m *only* 38 years old. I’m *only* on Humira. Why am I getting a 3rd dose two months after my 2nd vaccine?
I saw my gastroenterologist for a check up last week and she ordered a SARS-Cov-Z Antibody (IgG) Spike Semi Quantitative test at Quest Labs. My results came back and from a range of 0-20, I was at 4.42. My GI was surprised my response had dwindled so quickly and recommended I receive a third dose to help mount a more robust response.
Dr. David Rubin, MD, Professor of Medicine, University of Chicago, and Chairof the National Scientific Advisory Committee of the Crohn’s & Colitis Foundation told me that multiple studies on antibody response in patients with IBD have shown that after two doses the titers are similar to that of the general population. So, my result, is an aberrancy compared to the data. He said getting a 3rd dose seems right for me, given my personal results.
“We have suggested the booster for everyone and think of the COVID vaccines as part of a 3-dose series. When it comes to true protection from the infection, memory B cells (cellular immunity) are more important than antibodies. There is not a commercial test for that yet, but we are studying it.”
In a recent talk Dr. Rubin gave about COVID, vaccines, and the updated recommendations for additional doses and boosters, he discussed how IBD is a condition of an abnormal immune response. Therapies to manage IBD are predominately immune-based and immune-modifying. The information shared by the CDC and FDA is not specific to IBD and is confusing (for everyone).
“CDC recommends individuals should get a third vaccine if:
Previously received two doses of an mRNA vaccine
Currently taking select therapies, including anti-TNF and anti-metabolites
“Other biologic agents that are immunosuppressive or immunomodulatory”
High dose steroids (prednisone ≥20 mg/d or equivalent for ≥2 weeks)
All other individuals are recommended to get a booster 6-8 months after second mRNA vaccination.”
But wait, what’s the recommendation on antibody tests? Are they valid?!
This is where I get confused too, folks. Prior to receiving my antibody test and following my doctor’s orders I was not aware that the FDA and CDC both strongly recommend NOT checking or acting on antibody levels, as the tests outside of research studies are unreliable and unvalidated. Antibody tests do not paint a full picture of our immune system.
“There are strong recommendations from the CDC, FDA and ACIP (Advisory Committee on Immunization Practices) that patients NOT check antibodies nor use them in decision making. The only time they should be used is in the setting of research studies,” said Dr. Bewtra.
The reason for this is multifold:
-Antibody tests are not validated.
-Since they are not validated, there is no comparison for values. For example, my 4.42 on one test may be completely different in a different test.
-We know that antibodies are testing only one aspect of the immune system—there is a LOT more to immunity than an antibody level.
Dr. Jami Kinnucan, MD, University of Michigan Health advises all her IBD patients to receive a third dose, or a booster vaccination based on their risk factors and immunosuppression medications.
Dr. Kinnucan says, “Overall the current recommendations are to get a dose #3 on certain immunosuppressive therapy, which is different than a true booster dose. In addition, it is hard right now to understand what the true threshold of immunity is with antibody testing so I would not put too much into antibody test results. I do not recommend that patient’s routinely have their antibody status checked (unless they are involved in current studies). I would recommend getting dose #3 or booster dose for IBD patients.”
Vaccinated diverse people presenting shoulder
During the holidays we should all continue to follow CDC recommendations when it comes to social gatherings, social distancing, wearing masks, and properly washing our hands. Everyone that you spend time with should be fully vaccinated so the only thing being spread is holiday cheer. If you plan to spend time with anyone who is not from your immediate bubble, it’s recommended they take a rapid test before coming over.
Key Reminders as We Head into the Holidays
Vaccines are not 100% protective and Dr. Bewtra says “no one is fully vaccinated.”
“No one should think that just because they’ve had two vaccines, or 3 or 4, that they are safe. Protection is a function of the community: when community levels are high, even if you just got your vaccine, you need to wear a mask and practice all the recommendations from the CDC.”
What are the studies saying about the IBD Community
The data from science is highly variable. Studies looking at Rheumatoid Arthritis are not translatable to IBD, even when patients are on the same drugs. We have the real-world data from IBD, and it shows that the vast majority of IBD patients respond to vaccines appropriately. So not everyone needs to rush out to get a 3rd dose.
“We are doing a lot of vaccinating “the worried well” in this country. That may be fine because we are in a rich enough place to do that over and over, but it should not infer a feeling of false protection and it may be unnecessary,” said Dr. Bewtra.
Closing Thoughts
On the fence about receiving a 3rd dose and/or a booster dose? Have a discussion with your physician who specializes in caring for your IBD and prescribes your medications. Much like how IBD and COVID manifest differently in each person, it’s not fair to make blanket decisions about the entire patient population.
Dr. Rubin wants to reassure those with IBD that they are not at increased risk of bad COVID outcomes (but not at decreased risk either). He says most patients with IBD on therapy beyond 5-ASA or budesonide are eligible to get a third dose now. For patients on combination therapy with anti-TNF and thiopurine, methotrexate or high dose steroids, it’s reasonable to get the third dose/booster early.
Stay tuned for the evolving research. As the months go by and more research studies are completed, we’ll have a clearer picture of how to tackle this as well as additional guidance.
Save the Date: Facebook Live Event on Global Perspectives on COVID + IBD
The South Asian IBD Alliance (SAIA) is hosting a Facebook Live event Saturday, November 20 at 10 am EST. Patients and physicians will share their perspectives on COVID from the United States, United Kingdom, and India. Doctors will explain study data on serocoversion (development of specific antibodies in blood serum as a result of infection or immunization) in IBD patients and what their thoughts are on boosters and a 3-dose regimen, along with their viewpoints on mixing and matching vaccines. Patients will share their experiences from each respective country and discuss the challenges the pandemic has caused in terms of care.