By Natalie Hayden and Tina Aswani-Omprakash
**This article has also been published on Tina’s blog: Own Your Crohn’s**
As two bloggers and patient thought leaders in the IBD community, we were thrilled and honored to attend and speak at the Advances in IBD conference in December 2024 in Orlando, Florida. In the article below, we come together to summarize key learnings for our IBD patient and caregiver community.

Management of Crohn’s Disease
Crohn’s can be a very progressive disease, meaning it can worsen over time and cause complications, often leading to fistulae, strictures, and therefore surgery and bowel loss. In a debate between two of the co-chairs, Dr. Miguel Regueiro and Dr. Corey Siegel, as well as throughout AIBD, a key theme was to understand if all Crohn’s patients need advanced therapies (biologics or small molecules) to prevent complications. A good suggestion was to identify those few patients who could be closely monitored but not necessarily put on an advanced therapy. The doctors agreed that almost all patients do need an advanced therapy to prevent progression of the disease. Dr. Siegel brought up an interesting point about risk-stratifying patients via a new blood test called CD-PATH, which allows physicians to better understand if a patient might be low-, medium-, or high-risk for progression of Crohn’s disease.
The conclusion at the conference was that early intervention has made a big difference in terms of improving long-term outcomes for patients. It was shown that there is an optimal time for treatment and missing that window can lead to progression of disease and potentially complications.



From stem cells for perianal Crohn’s to more options for fibrostenotic Crohn’s, many patients are waiting for more therapeutics to gain better quality of life. Patients, however, are also clamoring for more therapies for mild Crohn’s disease. There is a real void in treatment options for mild Crohn’s outside of dietary therapies and occasional use of steroids (< 1-2x a year). As patients ourselves, we advocate for more options whether that’s looking at S1Ps or new therapeutics that can help patients feel safe & comfortable that their disease is being treated.

Management of Ulcerative Colitis
In Dr. Millie Long’s talk on Defining Disease Severity in UC, she shared many pearls. Primary indicators of severity include appearance severity of disease on endoscopy and frequency of use of steroids (more often means another long-term therapy may be needed to quell inflammation). She said to also consider biomarkers (fecal calprotectin, C-reactive protein, etc.) and to keep in mind what prior therapies have been used. Dr. Long emphasized that UC can also progress like Crohn’s, and it is important to use treat to target strategies, including initiating therapy early, monitoring for disease activity using biomarkers and intestinal ultrasound, and aim for mucosal healing.
In Dr. Maia Kayal’s talk on what meds to consider if Mesalamine doesn’t cut it in UC, her key take-home message was, “Your first shot is your best shot.” She said it was important to plan wisely if you have mild to moderate UC and work carefully with your gastroenterologist to identify medication options. Dr. Kayal emphasized that certain biologics may be more effective as a first-line therapy rather than being used after one or two biologics haven’t worked, so to choose carefully. Even if mesalamine doesn’t work, there are multiple biologic options from anti-TNF agents to anti-IL-23 medications, and S1P receptors.



CurQD & IBD
Throughout the conference, CurQD received many notable mentions, which in randomized clinical trials showed efficacy in mild to moderate UC when mesalamine hasn’t cut it. CurQD is a naturally sourced formula. Cura is gut-directed form of curcumin that has been found to reduce inflammatory cytokines, restore barrier function, and positively alter the composition of the gut microbiome. QD (Qing Dai) is an extract of Indigo plants found in clinical trials to relieve bleeding, inhibit inflammation, and promote mucosal regeneration (Naganuma et al, Gastroenterology 2018, Ben-Horin et al, CCFA 2023). Dr. Kayal shared this placebo-controlled trial, that found CurQD was effective for inducing response and remission in active UC patients and has the ability to significantly decrease urgency.
Dr. David Rubin also touted CurQD as an adjunctive IBD therapy option, rather than a singular therapy, much like diet. He said while it may be beneficial, patients need to be cautious about sudden pain or obstructive-like symptoms and communicate how they’re feeling with their doctor.



Insurance barriers
Patients and providers have an uphill climb when dealing with insurance barriers, which makes managing IBD exceptionally challenging and at times frustrating for everyone involved. These proverbial hula hoops we’re all constantly forced to jump through often lead to delays in treatment and unnecessary stress. One key challenge discussed during this session was how to deal with insurance companies denying patients who have not tried 5-ASAs or steroids. Solutions shared included the GI office providing detailed documentation on the following:
- listing previously tried and failed medications including steroids,
- recent objective findings on endoscopy, imaging, blood tests,
- sharing symptoms experienced by the patient,
- referencing guideline recommendations, and
- outlining the risks to the patient and the costs to the insurance company if treatment is not initiated soon.
Patients can also proactively reach out to their insurance company to determine their preferred advanced therapies and pass that intel along to their IBD team.
Another common roadblock discussed was finding out a medication is not covered or no longer covered by insurance—whether it be biologic vs. biosimilar of off-label dosing.
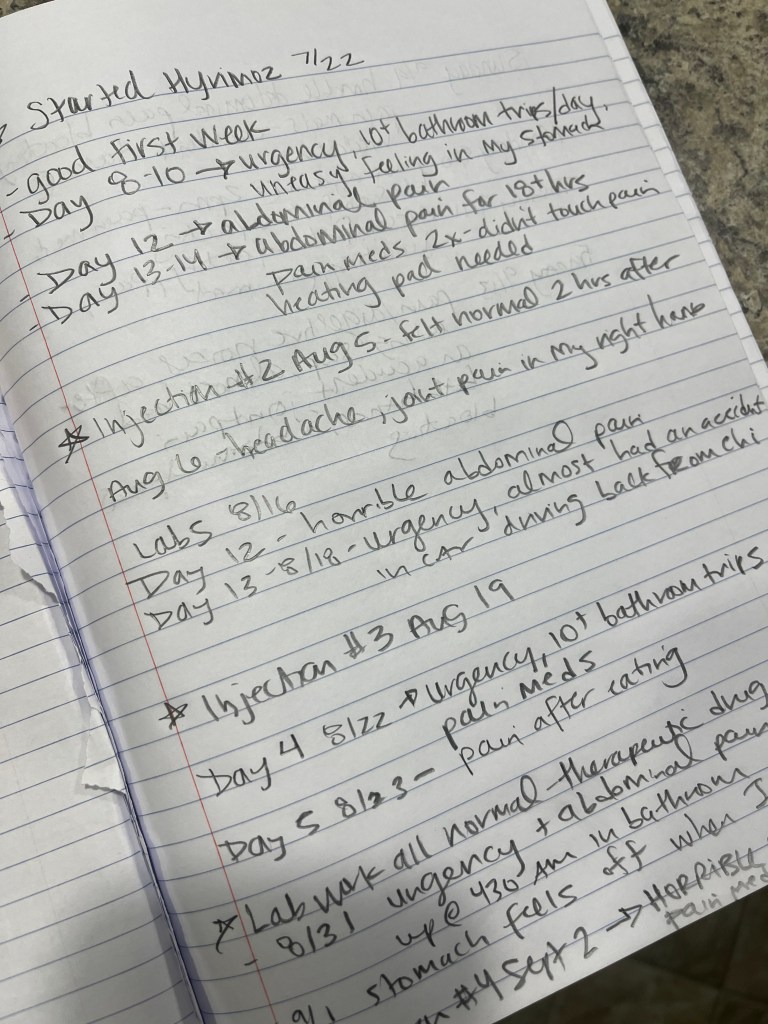
Patients can discuss appealing the decision with their IBD team during clinic appointments, over the Patient Portal, or over the phone. If your first appeal is denied, keep close tabs on your quality of life moving forward. If you are forced to switch, keep a detailed journal of all your symptoms to paint a clear picture of your reality.
Ask about having your GI submit a letter written by you about your patient experience, along with theirs, and make sure a doctor with knowledge of immune-mediated conditions is reviewing the appeal at the insurance company.
Providers can be supportive by showing empathy, following the latest research and including studies within insurance appeal letters. If a person is symptomatic, it would be important to rule out whether it’s active disease or an adverse reaction to medication.
Biosimilars now and in the future
The landscape for IBD therapies has changed immensely in recent years and will continue to do so in the years ahead. Stelara will join Remicade and Humira in 2025 with six biosimilar options for patients (and insurance companies). One of the main areas of improvement lies in patient education. Oftentimes we hear about the switch through a letter from our insurance company or we’re blindsided at an infusion appointment and told by our nurse that we’ll be receiving the biosimilar moving forward. As should be expected, this results in a great deal of uncertainty, skepticism, and pushback from the patient and caregiver population.
Biosimilars are biologic medical products that are highly similar to an already approved reference biologic, with no clinically meaningful differences in terms of safety, potency, or efficacy. Unlike generic drugs, which are chemically synthesized and identical to their branded counterparts, biosimilars are produced using living organisms and exhibit minor natural variability.
Dr. David Choi presented about how important proactive discussions with the patient community area to instill confidence and help educate about how safety and effective biosimilars are. Currently, four adalimumab and two Ustekinumab drugs have interchangeability, which is a designation from the FDA that allows for patients to be automatically switched (originator drug substituted) at the pharmacy level. Dr. Choi shared that providers can avoid this automatic substitution by selecting “dispense as written” on the original prescription. He went on to share that while improving access, there is also a major cost savings. Biosimilars across all disease spaces are expected to save $38-$124 billion from 2021 to 2025. The future of biosimilars is happening right now with exclusivity for golimumab and certolizumab over in 2024 and with more biosimilars in development.

Final thoughts from AIBD 2024
Overall, the main theme throughout all the educational sessions was that IBD needs to be more than just managed, it needs to be overcome with shared patient decision making. More work needs to be done to determine which patient is right for which therapy. There tends to be too much focus on the risk of therapies, rather than the risk of uncontrolled disease. The overarching goal is for providers to identify high-risk patients before we have severe disease and not be hesitant to use surgery as a treatment option when necessary. Emphasis on the importance of re-thinking the role of diet and nutrition and mental health care in conjunction with advanced therapy, looking at biomarkers 10+ years before diagnosis to see if we can prevent or diminish disease severity, utilizing intestinal ultrasound to measure drug response and disease activity in a non-invasive way, and continuing biologics in pregnancy (Healthy mom= healthy baby) were common themes throughout this fantastic conference.
As patients, we remain hopeful for the future of IBD and committed to improving patient outcomes. Lots of work still to be done, but it is impressive to see how far the science has come in the last 19-20 years since our diagnoses!